eyes - stem · pdf fileparts of the eye we depend on our eyes to provide us with information...
TRANSCRIPT
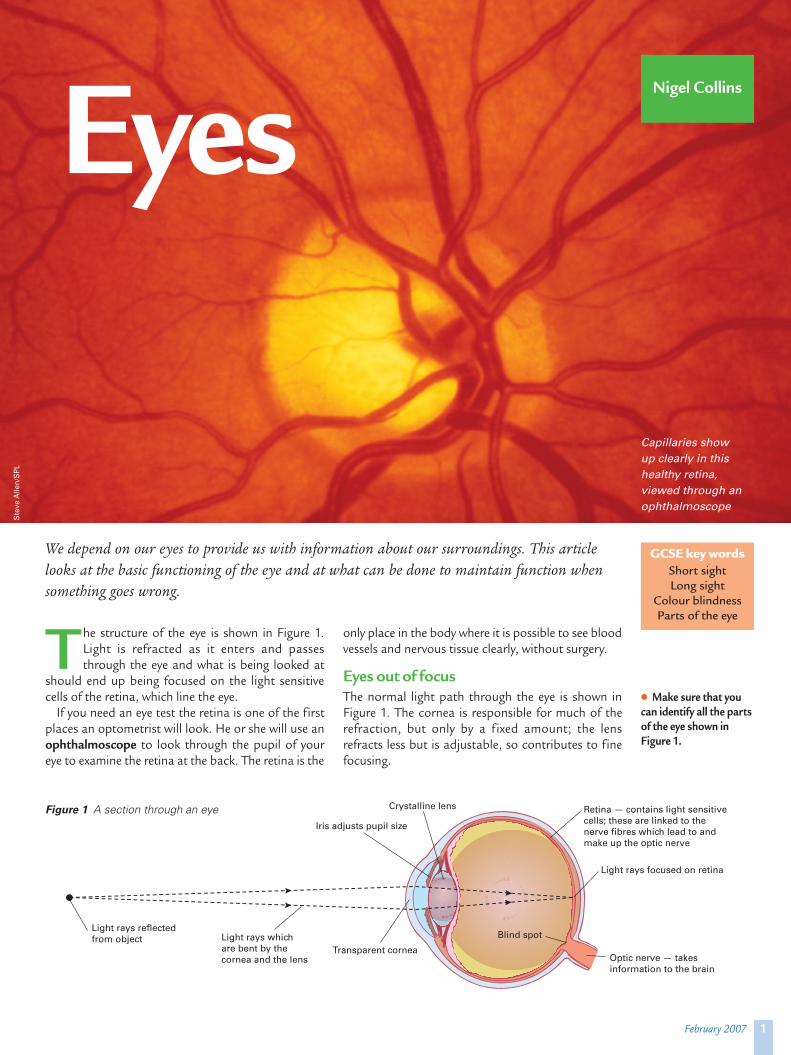
T he structure of the eye is shown in Figure 1.Light is refracted as it enters and passesthrough the eye and what is being looked at
should end up being focused on the light sensitivecells of the retina, which line the eye.
If you need an eye test the retina is one of the firstplaces an optometrist will look. He or she will use anophthalmoscope to look through the pupil of youreye to examine the retina at the back. The retina is the
only place in the body where it is possible to see bloodvessels and nervous tissue clearly, without surgery.
Eyes out of focusThe normal light path through the eye is shown inFigure 1. The cornea is responsible for much of therefraction, but only by a f ixed amount; the lensrefracts less but is adjustable, so contributes to finefocusing.
1February 2007
EyesNigel Collins
GCSE key wordsShort sightLong sight
Colour blindnessParts of the eye
We depend on our eyes to provide us with information about our surroundings. This articlelooks at the basic functioning of the eye and at what can be done to maintain function whensomething goes wrong.
Optic nerve — takesinformation to the brain
Crystalline lens
Iris adjusts pupil size
Transparent corneaLight rays which are bent by thecornea and the lens
Light rays reflectedfrom object
Retina — contains light sensitivecells; these are linked to the nerve fibres which lead to and make up the optic nerve
Light rays focused on retina
Blind spot
Figure 1 A section through an eye
Capillaries show up clearly in thishealthy retina,viewed through anophthalmoscope
l Make sure that youcan identify all the partsof the eye shown inFigure 1.
Ste
veA
llen/
SPL
Problems with focusingThe following three conditions make it impossible to focus unaided: myopia, hypermetropia and astigmatism.
Myopia (short- or near-sightedness) is a defect ofthe eye in which the image is focused in front of theretina. People with myopia can normally see nearbyobjects clearly, but distant objects appear blurred.This is because the eye is too long or its focusingpower is too great.
The opposite condition is hypermetropia (far- orlong-sightedness). This occurs when the cornea is tooflat or the eye is too short, causing the image to formbehind the retina. A person suffering from this cannotfocus on near objects; in extreme cases, a sufferer maybe unable to focus on objects at any distance.
Both of these defects may be complicated by astigmatism. This occurs when the eye has unevencurvatures, so that, for example, horizontal lines mayappear in sharper focus than vertical ones.
Figure 2 shows the ray patterns and the correctinglenses for each of these conditions.
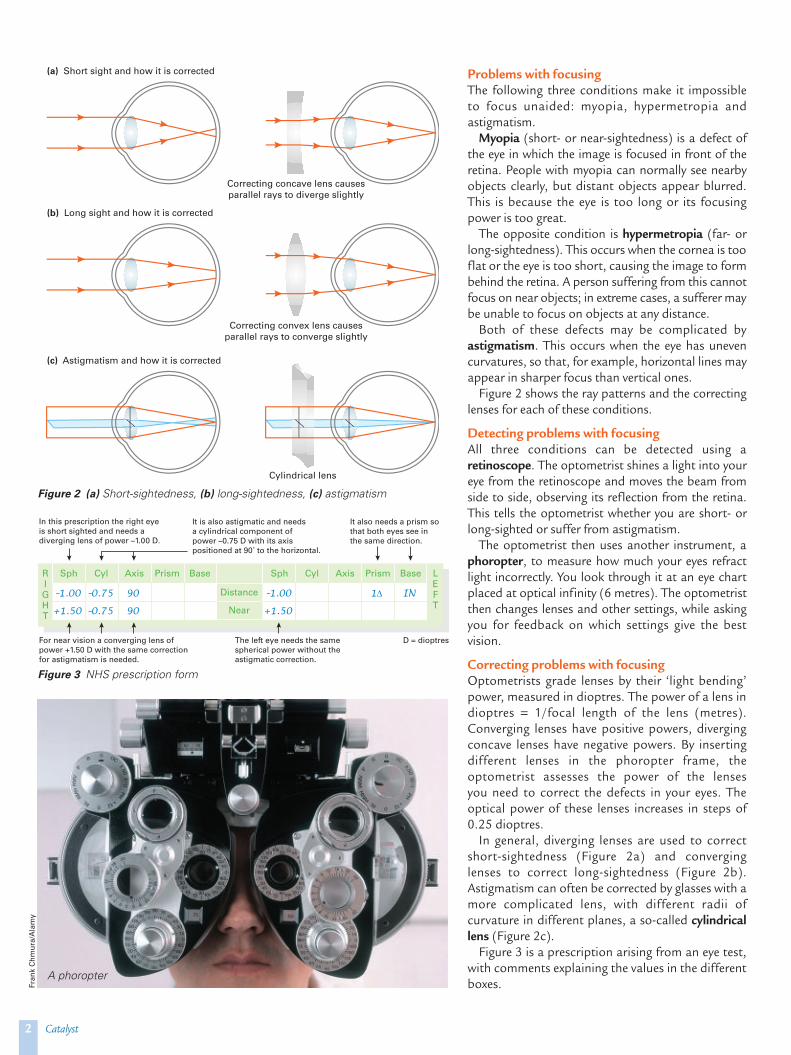
Detecting problems with focusingAll three conditions can be detected using aretinoscope. The optometrist shines a light into youreye from the retinoscope and moves the beam fromside to side, observing its reflection from the retina.This tells the optometrist whether you are short- orlong-sighted or suffer from astigmatism.
The optometrist then uses another instrument, aphoropter, to measure how much your eyes refractlight incorrectly. You look through it at an eye chartplaced at optical infinity (6 metres). The optometristthen changes lenses and other settings, while askingyou for feedback on which settings give the bestvision.
Correcting problems with focusingOptometrists grade lenses by their ‘light bending’power, measured in dioptres. The power of a lens indioptres = 1/focal length of the lens (metres).Converging lenses have positive powers, divergingconcave lenses have negative powers. By insertingdifferent lenses in the phoropter frame, theoptometrist assesses the power of the lenses you need to correct the defects in your eyes. Theoptical power of these lenses increases in steps of0.25 dioptres.
In general, diverging lenses are used to correctshort-sightedness (Figure 2a) and converging lenses to correct long-sightedness (Figure 2b). Astigmatism can often be corrected by glasses with amore complicated lens, with different radii ofcurvature in different planes, a so-called cylindricallens (Figure 2c).
Figure 3 is a prescription arising from an eye test,with comments explaining the values in the differentboxes.
2 Catalyst
Figure 2 (a) Short-sightedness, (b) long-sightedness, (c) astigmatism
Correcting concave lens causesparallel rays to diverge slightly
(a) Short sight and how it is corrected
Correcting convex lens causesparallel rays to converge slightly
(b) Long sight and how it is corrected
Cylindrical lens
(c) Astigmatism and how it is corrected
Sph
–1.00
+1.50
–0.75
–0.75
90
90
–1.00 1∆ IN
+1.50
In this prescription the right eyeis short sighted and needs a diverging lens of power –1.00 D.
For near vision a converging lens ofpower +1.50 D with the same correctionfor astigmatism is needed.
The left eye needs the samespherical power without theastigmatic correction.
D = dioptres
It is also astigmatic and needs a cylindrical component ofpower –0.75 D with its axispositioned at 90˚ to the horizontal.
It also needs a prism sothat both eyes see inthe same direction.
RIGHT
LEFT
Cyl Axis Prism Base Sph
Distance
Near
Cyl Axis Prism Base
A phoropter
Figure 3 NHS prescription form
Fran
kC
hmur
a/A
lam
y

Colour blindness The most common cause of colour blindness is aninherited disorder which affects some of the receptorsin the retina. Other causes include damage to theretina, to the optic nerve or to visual centres in thebrain. Few people are completely colour blind —seeing only in black and white and all the shades ofgrey in between. Most suffer from a condition inwhich they have trouble telling red from green.
DiagnosisDiagnosis of basic colour blindness is often done withIshihara cards (Figure 4). Colour blindness (ordeficiency) is caused by recessive alleles. It is muchmore common in men, as the recessive allele is carriedon the X chromosome. A single copy of the recessiveallele is expressed, as there is no dominant allele onthe small Y chromosome to mask its presence.
Cone cellsThe retina includes two types of cell: rod cells (activein low light intensities) and cone cells (active in broaddaylight). There are three types of cone cell and eachtype contains a pigment which absorbs light across adifferent and overlapping range of wavelengths.Between the three, with overlap, they cover the visiblespectrum. Nevertheless, they are often referred to as‘blue’, ‘green’ and ‘red’ receptors. Light across alimited range of wavelengths will stimulate some orall of them to a greater or lesser extent, so that the eye can discriminate between subtly differentcolour hues.
Colour blindness arises from partial or completedefects in particular types of cone. The commonestdefect leads to difficulty in discriminating betweenreds, yellows and greens — so called red-green colourblindness.
GlaucomaThe fluid inside the eye is slightly pressurised. Becausethe eye is a very tough structure it cannot expand if thepressure increases for any reason — as a result, increas-ing pressure is exerted on the lining of the eye. Thiscondition is called glaucoma. The weakest point in thelining is where the optical nerve leaves the eye and asthis becomes damaged peripheral vision is reduced.This causes the area of effective vision to shrink. If leftuntreated, glaucoma can cause blindness.
High blood pressure (see ‘Blood pressure’, CATALYST
Vol. 17, No. 1) can cause glaucoma. Optometristsroutinely check the pressure in the eyes of patientsover the age of 40 using a tonometer. There are twomain methods. One uses a sterile probe which ispressed against the surface of the cornea. The forceneeded to flatten a particular area of the cornea ismeasured and this correlates with the pressure insidethe eye. Before the test, anaesthetic drops are placedin the eye, followed a short while later by a drop ofyellow fluorescein dye, which, used with a blue filtermakes it easier for the optometrist to check theflattened area. Another method places a nozzle closeto the cornea and the deflection of the cornea surfaceis measured when a puff of air is blown at it. Althoughnot as accurate as the first method it is useful forscreening and with young children.
CataractsThe lens in the eye is completely transparent. In olderpeople it may become progressively more cloudy.Clouding causes vision to become more and moreblurry and often more yellowish or brownish overtime. This can have a huge impact on people’s lives,preventing them from reading or driving. The clouding(cataract) cannot be reduced, but the lens can beremoved and replaced with a plastic lens (or a trans-planted one), which can improve vision greatly.
Nigel Collins is a myopic and an editor of CATALYST.
3February 2007
Figure 4 Ishihara card. A person with normal vision willbe able to see an image of an eye. A person who iscolour blind will not see the eye
Left: Damage causedinside the eye byglaucoma
l Find out more aboutcolour blindness atwww.VisionSimulations.com/Color.htm
Paul
Park
er/S
PL
Dav
idN
icho
lls/S
PL
l Find out more aboutthe effects of glaucomaat www.VisionSimulations.com/Glaucoma.htm
Some visual problemsare caused by faults inbrain processing, not inthe eye.
The rows of letters onan eye test chart arenumbered. The rowlabelled ‘20’ should belegible at a distance of20 feet (6 metres) ifyour eyesight is good;hence ‘20/20 vision’.
l Find out more aboutcataracts atwww.VisionSimulations.com/Cataract.htm