extending preventive care to pediatric urgent care a partnership between: university of california,...
TRANSCRIPT

Extending Preventive Care to Pediatric Urgent Care
A Partnership Between:University of California, San Francisco
& Kaiser Permanente Northern California
Mary-Ann Shafer MD & Kathleen Tebb PhD
Presentation to STD Prevention ConferenceMarch 10, 2004
Funded by the Centers for Disease Control and Prevention & The Agency for Health Care Research and Quality

BackgroundBackgroundFacts About Facts About Chlamydia Trachomatis (CT)Chlamydia Trachomatis (CT)
• Rate is 6-12% in teen females
• 70-80% are asymptomatic
• 10-20% untreated PID infertility
• NAATs 90-95% sensitivity/specificity
• Nat’l Guidelines annual CT screen

Background cont.Background cont.
• Clinical Practice Improvement intervention (CPI) increased CT screening of sexually active teens at pediatric well care visits (WCVs)
• Yet, over 50% of adolescents are seen only for urgent care visits (UCVs), in any given year

JAMA December 11, 2002

Learning ObjectivesLearning Objectives
• Review the development, implementation and evaluation of a systems-based intervention for CT screening
• Understand utilization patterns of teens seen in well versus urgent care
• Discuss the translation of the CPI model to different clinical settings

Study ObjectivesStudy Objectives
• Develop a modified CPI (clinical practice improvement) intervention to address barriers to CT screening during UCVs
• Examine feasibility of CT screening attending pediatric UCVs in a large HMO

MethodsMethods
Setting
Large HMO in Northern California: KPMG
• 2 Pediatric clinics participating in the previous well-care CPI intervention
• 14-18 yo females seen for UCVs
• ~4,000 enrolled 14-18 yo adolescent females in 2 sites

Methods
Urgent-Care Visit
• Same/ next day visit
• Sick/ non-ER visit
• 10 minute visit
• Same physical setting as WCV
• Same providers & staff as WCV
KP Pediatric Setting cont.
Well-Care Visit
• Appointment required
• Physical exam (every 2-3 yrs)
• 20 minute visit

MethodsMethods
Design
Pre-Post test study
• Provider survey (anonymous) to assess attitudes toward screening in UCV
• Teen survey (anonymous) for sex active rate
• Comparison of baseline CT screening rates to 6 month post-test rates

Engage
Team Building
Re-Design Clinical Practice
Sustain the Gain
Clinical Practice Improvement Model

Clinical Practice Improvement Model
Engage
Team Building
Re-Design Clinical Practice
Sustain the Gain
•Leadership
•Best practices
•Define gap
•Raise Awareness

Engage
Team Building
Re-Design Clinical Practice
Sustain the Gain
•ACTeam•Skill building•Tool Kit
Clinical Practice Improvement Model

Engage
Team Building
Re-Design Clinical Practice
Sustain the Gain
•Customize•Measure success
Clinical Practice Improvement Model

Engage
Team Building
Re-Design Clinical Practice
Sustain the Gain
•Monitor performance•Time series analysis•Continuous improvement
Clinical Practice Improvement Model
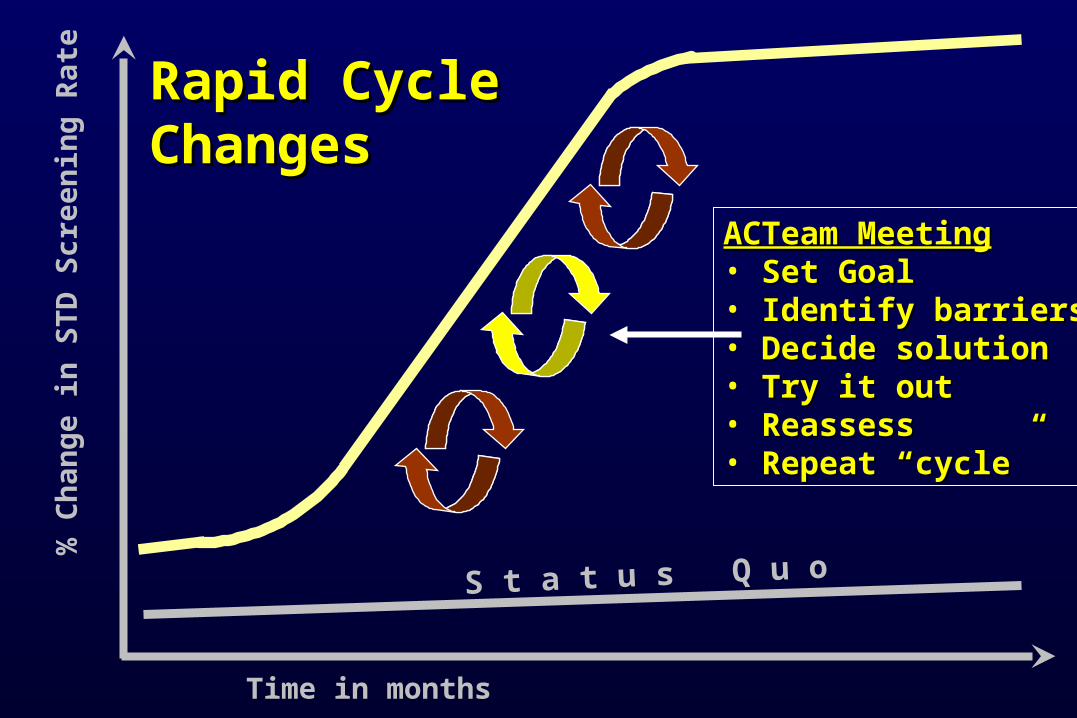
ACTeam MeetingACTeam Meeting• Set GoalSet Goal• Identify barriersIdentify barriers• Decide solutionDecide solution• Try it outTry it out• ReassessReassess• Repeat “cycle”Repeat “cycle”
Time in months
% C
han
ge in
STD
Scre
en
ing
Rate
S t a t u s Q u o
Rapid CycleRapid CycleChangesChanges

Urines To Lab
MD/NPVISIT
RoomPatient
MA refrigerates FVUs A enters teen name, confidential # in clinic log book LRunner takes FVU to lab
MD/NP obtains sex hx
If sexually active, MD completes CT lab slip WWWrites confid. # on chart
MA collects FVU on all 14-18 yo F TTeen takes FVU sample to exam room
CueCharts
ID eligible teensC
Charts are stamped with cue
Follow-Up
RN contacts CT + teen: confid. #
Teen comes to clinic for Rx
RN enters Rx in STD log book
Site Specific Flow Chart

Data Bases and Analysis
Data Bases
• Registration + lab + anonymous survey of teens for clinic specific screening rates
Data Analysis
• Mann-Whitney/T-test

Data Analyses: CT Screening Rate
Screening Rate = No. of CT tests
Sexually active teen females*
*Site specific sexual activity rates determined by anonymous survey

RESULTS

Urgent Care vs Well Care PopulationUrgent Care vs Well Care Population
Teen girls who utilize urgent care compared to well care visits have a higher STD risk profile:
• Older (15.7 vs 15.4 years)*
• More ethnically diverse (Cauc/Asian vs. Oth)*
• Higher sexual activity rates (42% vs 26%)*
*p<0.05

Pediatrician Survey ResultsCT Screening Likelihood during UCV: (1=not likely, 4=very likely)
Teen Chief Complaint MD Mean Rank SD Asthma 1.26 0.52
URI 1.30 0.57
Minor trauma 1.31 0.58
Non-reproductive visit 1.64 0.74
Abdominal pain 2.84 0.90
Vaginal bleeding 2.98 1.12
Pregnancy test 3.45 0.86
Requested by patient 3.87 0.58
STD symptoms 3.91 0.44

MD’s Top 3 Barriers to UCV Screening
1. Parents in room/confidentiality
2. Competing priorities
3. Discomfort in taking sexual history

RESULTS: Female CT Screening Rate in Urgent Care Pilot Sites
0
10
20
30
40
50
60
70
2000 2001 2002 2003
Year Clinic AClinic B
% S
A F
emal
es
Scre
ened
for C
T
A
A
B
B
B

Conclusions
• CT screening in pediatric UCVs is feasible
• Significantly more teens screened for CT
• Clinic differences different results
• More research needed (e.g., RCT, more clinics)

Implications
• CT epidemic universal screening recommended
• Most teens seen only in UCVs and they have a higher STD risk profile screen for CT in well and urgent care
“Do Today’s Work Today”
• The CPI model (rapid-cycle change) may be generalizable to other services & clinic settings

Implications cont.
• Rapid cycle quick, dramatic & sustained
• Effective in different settings- well & urgent and likely others as well
• Capitalizes upon existing resources & staff
• Small changes LARGE effects
• Gives chronically over-worked staff sense of importance, success & control over workplace
