exploring homoeopathy in cystic ovarian diseases
TRANSCRIPT

EXPLORING HOMOEOPATHY IN CYSTIC OVARIAN DISEASES
Dr. Smita Brahmachari,Dr. Smita Brahmachari,M.D. (Repertory) from N.I.H., Kolkata.M.D. (Repertory) from N.I.H., Kolkata.
M.O., Dept. of AYUSH, M.O., Dept. of AYUSH, Govt. of NCT Delhi.Govt. of NCT Delhi.

INTRODUCTIONOvarian enlargements, cystic or solid
may occur at any age.The ovary is complex in its embrology,
histology, steroidogenesis, and has the potential to develop malignancy.
Therefore ovarian diseases exhibit a wide variation in structure and biological behaviour

Unlike the cervix and uterus, the ovaries are not clinically accessible, and therefore easy screening methods for detecting ovarian neoplasms are unavailable.
The ovary, after the uterus, is the second most common site for development of gynaecological malignancy, and the prognosis remains poor.

Ovarian functionOvarian functionOvaries produces an ovum monthly.Produce hormones responsible for maturation of the
graffian follicle, ovulation, menstruation and maintenance of pregnancy in the early weeks of gestation.
The steroidal hormones are oestrogen and progesterone.The other hormones which ovary produces in small
amount are testosterone and androstenedione (secreted by stromal cells stimulated by LH, gets converted peripherally into oestrone through aromatization in the fat tissue).
Ovarian functionOvarian function• After menopause, ovarian oestrogen level falls as
graafian follicles disappear, and progesterone fails to be produced.
• The increased stromal cells of the menopausal ovary continue to produce androstenedione which gets converted into oestrone.
• Though a weak oestrogen, oestrone is capable of exerting oestrogenic effect on the target tissues.
• Obese women have therefore more oestrone than a lean woman and hence a greater tendency to endometrial hyperplasia and malignancy.
In majority of women, oestrogen withdrawal at menopause causes endometrial atrophy, thus post menopausal endometrium measuring more than 4 mm is considered abnormal. Endometrial thickness of 8-12 mm is considered normal in the premenstrual phase.
Ovarian disorders may be benign or malignant.In this presentation I will be concentrating on non-
neoplastic enlargements of the ovary and benign ovarian tumours.
In a daily Homoeopathic OPD the commonest ovarian disorder encountered are Ovarian cysts and Polycystic Ovarian Disorder.
Non-neoplastic enlargements of the ovaryNon-neoplastic enlargements of the ovarySuch an ovarian enlargement may be the result of
ovarian congestion due to adnexal inflammatory states, ovarian endometriosis causing a chocolate cyst or persistence and enlargement of physiological structures in the ovary like the graafian follicle or corpus luteum.
The discussion will be restricted to non-neoplastic functional distension cysts of the ovary, benign tumours.

OVARIAN CYSTSOVARIAN CYSTSFollicular cysts: results from the growth of a follicle. A follicle is the
normal fluid-filled sac that contains an egg. Follicular cysts form when the follicle grows larger than normal during the menstrual cycle and does not open to release the egg. Does not exceed 5 cm in diameter, asymptomatic unless haemorrhage, rupture or torsion supervenes in which acute abdomen develop, large and multiple cysts may cause pelvic pain, dyspareunia and irregular bleeding. The enlarged ovary is visualized by USG. Most disappear spontaneously within few weeks to months.
Follicular haematomas / Haemorrhagic cysts : old ovarian cysts contain tarry material and likely to be mistaken for endometriosis. Contain blood from leakage of blood into the egg sac. Asymptomatic, unless bursts into peritoneal cavity causing acute abdomen.

OVARIAN CYSTSOVARIAN CYSTS• Corpus luteum cysts are functional cysts. The corpus luteum is an
area of tissue within the ovary that occurs after an egg has been released from a follicle. If a pregnancy doesn't occur, the corpus luteum usually breaks down and disappears. It may, however, fill with fluid or blood and persist as a cyst on the ovary. Usually, this cyst is found on only one side, cause local pain, tenderness and delayed menses, palpable clinically, resolve in due course of time.
• Functional cysts are recognized from neoplastic cyst by the fact they never grow more than 7 cm in size, are unilocular with clear fluid and regress after some time. These cysts occur as a result of ovulation.
• Multiple functional cysts….Polycystic ovarian syndrome characterized by multiple small cysts less than 1 cm; LH is raised and LH/FSH ratio is >6. Occur as a result of failed ovulation.
OVARIAN CYSTSOVARIAN CYSTSChocolate cyst : Endometriosis is a condition in which cells that
normally grow inside as a lining of the uterus, instead grow outside of the uterus in other locations. The ovary is a common site for endometriosis. When endometriosis involves the ovary, the area of endometrial tissue may grow and bleed over time, forming a blood-filled cyst with red or brown-colored contents called an endometrioma, sometimes referred to as a chocolate cyst.
Most ovarian cysts are never noticed and resolve spontaneously. When a cyst causes symptoms, pain in the abdomen or pelvis is the most common one. The pain can be caused from rupture of the cyst, rapid growth and stretching, bleeding into the cyst, or torsion.

OVARIAN CYSTSIf the cyst has reaches a large size, symptoms may arise as a result of
pressure or distortion of adjacent anatomical structures. These symptoms can include abdominal bloating, dyspepsia, feeling full after eating only a small amount (early satiety), frequency of urination, feeling an urge to defecate or having difficult bowel movements, or dyspareunia.
Most cysts are diagnosed by ultrasound, which is the best imaging technique for detecting them. It is useful to determine if the cyst is simple (just fluid with no solid tissue, suggesting a benign condition) or compound (with solid components that often requires surgical resection).
The tumor can be surgically removed either with laparoscopy or if needed, an open abdominal incision (laparotomy) if it is causing severe pain, not resolving, or if it is suspicious in any way. Once the cyst is removed, the growth is sent to a pathologist who examines the tissue under a microscope to make the final diagnosis as to the type of cyst present.
POLY CYSTIC OVARIAN SYNDROMEPOLY CYSTIC OVARIAN SYNDROME Polycystic ovarian syndrome (PCOS) or disease (PCOD) is a multisystem
endocrinopathy in women of reproductive age with the ovarian expression of various metabolic disturbances
The current incidence of PCOS (5 -6 %)1 is fast increasing lately. It is also becoming a common problem amongst adolescents, developing soon after puberty.
Two main reasons responsible for young girls being diagnosed with PCOS are "Girls with no siblings tend to be pampered from an early age with their diet comprising heavily of junk food. Secondly, the tremendous academic load in schools leaves children with no time to play or exercise, resulting in them gaining weight”. India, is undergoing rapid nutritional transitions due to westernized diets and lifestyle indicate prevalence (9.13%)2
The characteristic clinical features of PCOS are menstrual irregularity, such as amenorrhoea, oligomenorrhoea, or other irregular uterine bleeding, and signs of excessive androgen production, such as hirsutism, greasy skin, acne, acanthosis nigra and obesity.
Oligoamenorrhoea is defined as the absence of menstruation for ≥35 days or <8 cycles/year and amenorrhea as no menstruation for >6 months.

PCOSPCOS The cause is traced to insulin resistance with resultant
hyperinsulinaemia as the central key point in the genesis of PCOS in 70% cases1.
Also hypothalamic – pituitary – ovarian axis and adrenal glands (hyperandrogenism with resultant increased free testosterone leading to hirustism) are involved.
Obesity is another important cause of insulin resistance and hyperinsulinaemia occurring in 40 – 50% patients with PCOS.
For the diagnosis of PCOS, Rotterdam criteria (2003)1 suggest that at least two out of three criteria should be present. These criteria are oligo/amenorrhoea (absence of menstruation for 45 days or more and/or ≤8 menses per year), anovulation, infertility; hirustism and ultrasoundfindings (enlarged ovaries with increased stroma, 12 or more small follicles, each of 2 – 9 mm in size placed peripherally) should be performed in early follicular phase.
With irregular cycles in young girls, hormonal assays will identify hypothalamic – pituitary – ovarian dysfunction.
PREVALENCE OF PCOSPREVALENCE OF PCOS33
The prevalence of PCOS is increased in overweight and obese women when compared to their lean counterparts.
The prevalence rates of PCOS in underweight, normal-weight, overweight, and obese women are 8.2, 9.8, 9.9, and 9.0%, respectively.
Prevalence rates reaches 12.4 and 11.5% in women with BMI 35-40 kg/m 2 and greater than 40 kg/m 2 .
SEQUELAE OF PCOS
DiabetesCVS disorderHyperlipidaemiaHypertensionEndometrial cancerBreast cancerPremature ovarian failure following
surgery

It has been scientifically established that PCOS arises due to imbalance of hormones and thus responds well to suitable hormonal therapy. Their recurrence however cannot be checked because ovarian hormones are under the control of FSH and LH which are secreted by Pituitary gland and regulated by Gonadotropin Releasing Hormone (GnRH) which is released by Hypothalamus.

TREATMENT OF PCOSTREATMENT OF PCOS
Allopathic treatment: symptomatic, includes oral contraceptives to regulate menstrual cycles and reduce male hormone levels; glycaemic control medications, synthetic hormones to stimulate ovulation and regulate the levels of androgens.
General management: Maintaining optimum weight is a part of the treatment plan as a loss of 10% of body weight can regularize the patient’s menstrual cycle. Diet modifications in form of consumption of foods of low glycemic index and limiting carbohydrates and foods high in PUFA is advocated. Aerobic exercises like walking, jogging, swimming for at least 30 minutes for at least 5 days a week.

Homoeopathic mode of treatment follows a constitutional approach.
It stresses upon an integrated collection of the relevant alternations in the psychic and somatic field, along with the past medical; iatrogenic; obstetric; sexual; and family histories. Here the footnote of Aph. 94 of Organon of medicine4 should be accounted which emphasizes on case taking of chronic diseases of female.
Homoeopathy stresses on individuality above nosological diagnosis [‘no real cure can take place without a strict particular treatment, individualization of a case of disease’….Aph.82, Organon of Medicine4].
So search for individuality among the individuals are more important for prescription point of view. The totality of signs and symptoms is the most vital part to draw the individuality in the portrait of the disease.
Proper case taking, analysis and evaluation of symptoms followed repertorisation is the ideal homoeopathic approach.

Homoeopathy believes in the concept of miasms, various fundamental causes of chronic diseases.
In case of PCOS, it is the psoric miasm which initially brings about the functional changes followed by involvement of sycotic miasm which leads to cystic changes in the ovary.
PCOS is therefore the result of combination of psoric and sycotic miasms in the sick individual.
It has been observed that there is a possible link of hormonal imbalance with adult happiness, psychological health and general well being including mood dysfunction which is consistent with literature linking women with PCOS having anxiety, depression, psychosocial disturbances and disturbed stress responses. Infertility and obesity have been reported as source of depression in PCOS patients5.
Homoeopathy believes that emotions Homoeopathy believes that emotions initiate, precipitate and aggravate the initiate, precipitate and aggravate the illnesses. In illnesses. In Aph. 225 of Organon Aph. 225 of Organon of medicineof medicine4, Hahnemann says there , Hahnemann says there are few diseases which originate and are few diseases which originate and progress due to emotional causes progress due to emotional causes such as continued anxiety, worry, such as continued anxiety, worry, vexation etc. Here the physical health vexation etc. Here the physical health is slightly affected in the beginning is slightly affected in the beginning but in course of time these negative but in course of time these negative emotions destroy the health to a emotions destroy the health to a great degreegreat degree44. PCOS can be . PCOS can be categorized under psychosomatic categorized under psychosomatic illness.illness.
Psychological causes like anxiety, Psychological causes like anxiety, depression, mortification, vexation depression, mortification, vexation suppression of anger, emotions affect the suppression of anger, emotions affect the limbic system leading to disturbance in limbic system leading to disturbance in psycho-neuro-hormonal axis and psycho-neuro-hormonal axis and ultimately leading to imbalance in ultimately leading to imbalance in pituitary and ovarian hormones…..FSH, pituitary and ovarian hormones…..FSH, LH, Estrogen and Progesterone. LH, Estrogen and Progesterone.
The neurotransmitters produced in higher The neurotransmitters produced in higher centre of the brain due to psychological centre of the brain due to psychological reasons are passed on to hypothalamus reasons are passed on to hypothalamus and to pituitary gland through and to pituitary gland through hypothalamic hypophyseal axis resulting hypothalamic hypophyseal axis resulting in pathological changes in the uterus and in pathological changes in the uterus and ovary.ovary.

There is no specific medicine for the treatment of PCOS/ Ovarian cyst.
Each prescription plan is unique and designed according to the individual patient.
Only constitutional homoeopathic treatment approach of a case of PCOS/ ovarian cyst can cater the aim of treatment.
A constitutional medicine works not only on ovaries but also the entire neuro-endocrine system.
Homoeopathic repertories list a large group of medicines acting on ovaries and thus act a valuable aid in medicine selection.

RIGHT OVARY Apis Bell Bryonia Carbo animalis Iodum Lycopodium Palladium Platina Thea
LEFT OVARY Actea racemosa Eup purp Graphites Kali brom Lachesis Sepia Thuja Vespa crabro Wyethia

Apis: suppressed menses with cerebral and head symptoms in young girls, stinging pain in right ovary with great tenderness in the abdomen.
Aur mur natonatrum: enormous induration of ovary, cystic enlargement of ovary, sterility from ovarian disease. Has more power over uterine tumors than any other remedy (Burnett). Dose: 3x
Aurum iod: ovarian cysts Cantharis: burning, extremely sensitive pain in ovaries
with urinary complaints. Carbo animalis: useful in scrofulous constitutions. Right
ovary seems like a heavy ball. Valuable remedy for ovarian cysts.
Cimicifuga: amenorrhoea, pain in ovarian region shooting to anterior surface of thighs, backache and facial blemishes
Conium: with suppressed menses and sterility. Oophorinum: ovarian cysts
Homoeopathic constitutional treatment: Helps to balance hyperactivity of the glands. Regulate hormonal balance. Dissolve the cysts in the ovaries. Enhance the normal functioning of ovaries. Eliminating the need for hormonal therapies
and surgery. Early intervention with this treatment can assist
in preventing complications.

CASE PRESENTATIONCASE PRESENTATION
A CASE OF FUNCTIONAL OVARIAN CYSTA CASE OF FUNCTIONAL OVARIAN CYST
A female of 33 years (dt. of 1st visit: 18.8.11) presented with pain in hypogastrium radiating to lower back and extremities <10 -12 days before menses, since 3-4 months. Her menses were regular, early onset; lasted for 3-4 days, bright-red, with clots, she felt better after menses. Also she had frequent urination < before menses. Regular pelvic pain disturbed her daily activities. Pt. was unable to conceive after 3yrs of marriage.
USG of Pelvis (11.8.11): A functional cyst measuring 33*30 mm in left ovary

Other complaints: Recurrent tendency to coryza, sneezing
< rising from sleep < morning < summer till onset of rainy weather since 10 – 12 yrs with crusts formation in eyelid.
Generalized weakness; backache and pain in extremities < exertion.
Pain in nape of neck <change of weather, <rainy weather; <rising from sleep – 6 months.
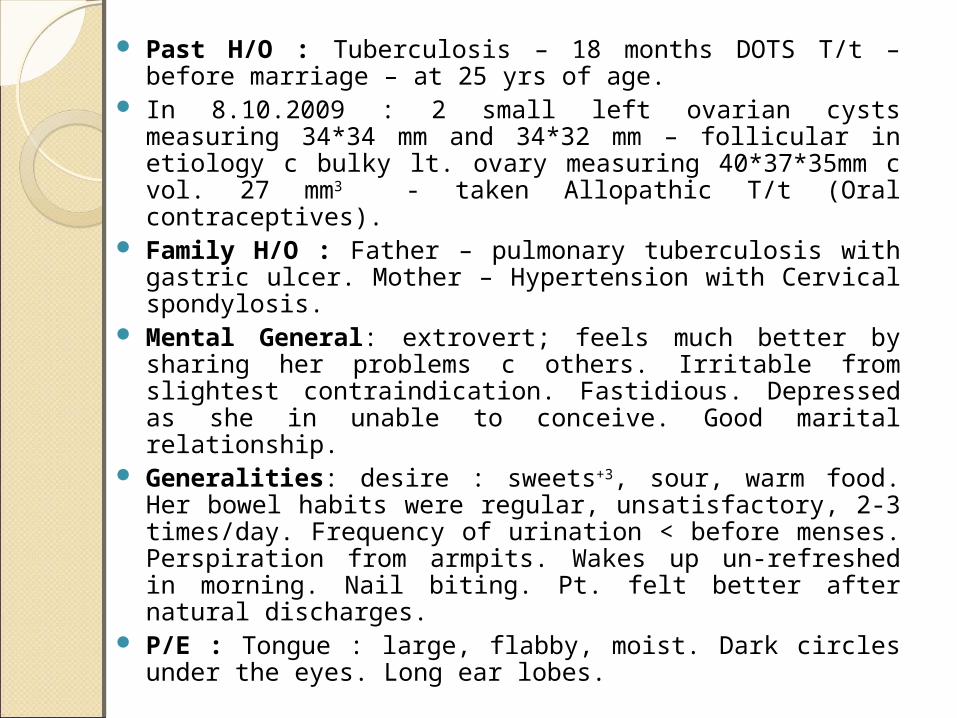
Past H/O : Tuberculosis – 18 months DOTS T/t – before marriage – at 25 yrs of age.
In 8.10.2009 : 2 small left ovarian cysts measuring 34*34 mm and 34*32 mm – follicular in etiology c bulky lt. ovary measuring 40*37*35mm c vol. 27 mm3 - taken Allopathic T/t (Oral contraceptives).
Family H/O : Father – pulmonary tuberculosis with gastric ulcer. Mother – Hypertension with Cervical spondylosis.
Mental General: extrovert; feels much better by sharing her problems c others. Irritable from slightest contraindication. Fastidious. Depressed as she in unable to conceive. Good marital relationship.
Generalities: desire : sweets+3, sour, warm food. Her bowel habits were regular, unsatisfactory, 2-3 times/day. Frequency of urination < before menses. Perspiration from armpits. Wakes up un-refreshed in morning. Nail biting. Pt. felt better after natural discharges.
P/E : Tongue : large, flabby, moist. Dark circles under the eyes. Long ear lobes.

DISCUSSIONDISCUSSIONThe case is multimiasmatic with sycotic dominant and of
tubercular diathesis. The case was prescribed Lachesis starting with 200 potency and gradually increased to 1M, 10M with intercurrent dose of Tuberculinum.
Reason for selection of Lachesis : left sided predominant complaint – lt. ovarian cyst; feels better after menses; cannot tolerate tight clothing around waist; extrovertedness and Tub. was prescribed intercurrently on the basis of family and personal history of tuberculosis. With Lachesis her generalities improved along with decrease in presenting complaints of pain in nape of neck and hay fever and recurrent tendency of cough and coryza
USG of Pelvis (25.2.12): Sonographic study within normal limits.
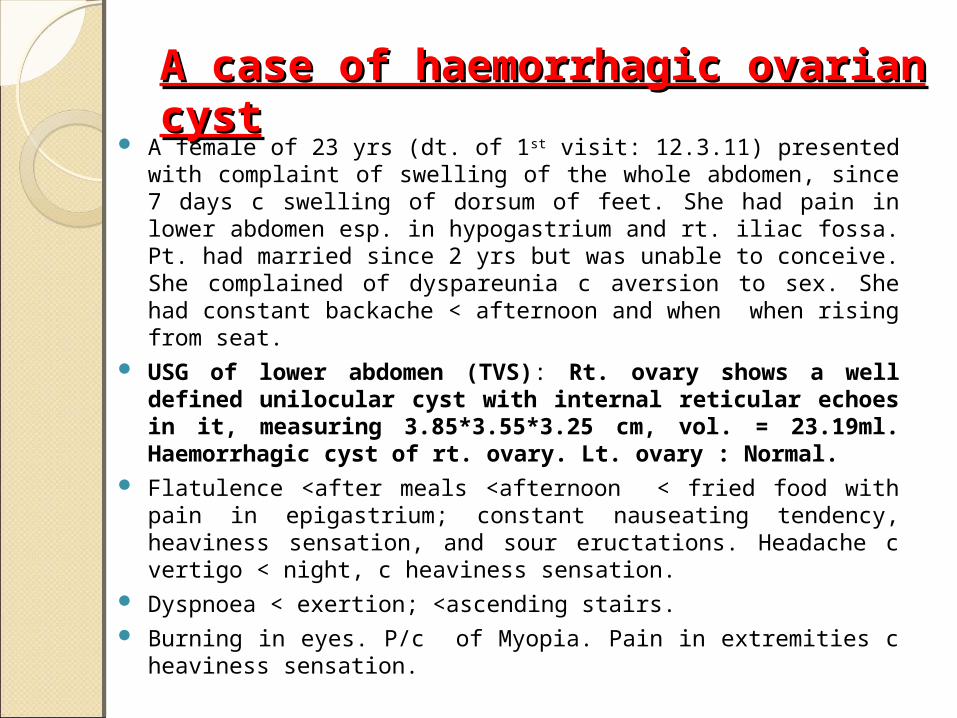
A case of haemorrhagic ovarian cystA case of haemorrhagic ovarian cyst A female of 23 yrs (dt. of 1st visit: 12.3.11) presented with complaint of
swelling of the whole abdomen, since 7 days c swelling of dorsum of feet. She had pain in lower abdomen esp. in hypogastrium and rt. iliac fossa. Pt. had married since 2 yrs but was unable to conceive. She complained of dyspareunia c aversion to sex. She had constant backache < afternoon and when when rising from seat.
USG of lower abdomen (TVS): Rt. ovary shows a well defined unilocular cyst with internal reticular echoes in it, measuring 3.85*3.55*3.25 cm, vol. = 23.19ml. Haemorrhagic cyst of rt. ovary. Lt. ovary : Normal.
Flatulence <after meals <afternoon < fried food with pain in epigastrium; constant nauseating tendency, heaviness sensation, and sour eructations. Headache c vertigo < night, c heaviness sensation.
Dyspnoea < exertion; <ascending stairs. Burning in eyes. P/c of Myopia. Pain in extremities c heaviness
sensation.
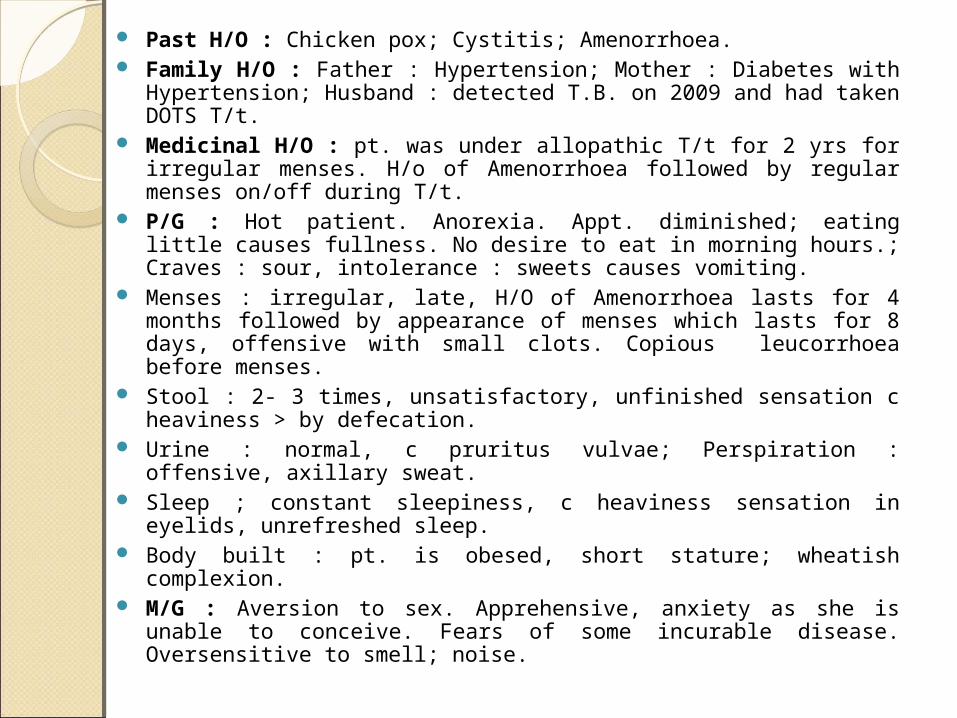
Past H/O : Chicken pox; Cystitis; Amenorrhoea. Family H/O : Father : Hypertension; Mother : Diabetes with
Hypertension; Husband : detected T.B. on 2009 and had taken DOTS T/t. Medicinal H/O : pt. was under allopathic T/t for 2 yrs for irregular
menses. H/o of Amenorrhoea followed by regular menses on/off during T/t.
P/G : Hot patient. Anorexia. Appt. diminished; eating little causes fullness. No desire to eat in morning hours.; Craves : sour, intolerance : sweets causes vomiting.
Menses : irregular, late, H/O of Amenorrhoea lasts for 4 months followed by appearance of menses which lasts for 8 days, offensive with small clots. Copious leucorrhoea before menses.
Stool : 2- 3 times, unsatisfactory, unfinished sensation c heaviness > by defecation.
Urine : normal, c pruritus vulvae; Perspiration : offensive, axillary sweat. Sleep ; constant sleepiness, c heaviness sensation in eyelids, unrefreshed
sleep. Body built : pt. is obesed, short stature; wheatish complexion. M/G : Aversion to sex. Apprehensive, anxiety as she is unable to
conceive. Fears of some incurable disease. Oversensitive to smell; noise.

The case was repertorized using RADAR. Rubrics selected : Female Genitalia – Tumors – Ovaries – right. Female Genitalia – Sterility. Female Genitalia – coition – painful. Sleep – Sleepiness – eyes – opening, difficult. Female Genitalia – Menses – clotted – offensive. Female Genitalia – Pain – ovaries – right. Chest – perspiration – axilla – offensive. Medicines (Repertorization) : Apis, Lyco; Sep; Bell; Sulph;
Calc; Iod; Plat.; Sil. and Lach. Medicines used during T/t : Nux vom – Sepia –
Lycopodium (Following the remedy relationship).

DISCUSSIONDISCUSSION The case is multimiasmatic with tubercular miasm dominance
(Haemorrhagic ovarian cyst; sterility with F/h of tuberculosis). It cannot be cured with a single medicine; change of symptom
picture (also taking lurking miasm into consideration ) during course of treatment invites for the change of the remedy.
The case was started with Nux vom given in 30th potency as the pt. had a history of use of allopathic medicines for prolonged time.
With predominance of uterine symptoms like irregularity of menses, leucorrhoea before menses; sterility with accompanying constant backache; dyspareunia; constant heaviness in eyelids; mental generals like oversensitiveness and aversion to sex; desire for sour; offensive axillary sweat and chronic of Nux vom.; Sepia was the medicine selected. The medicine was started in 200th potency and gradually increased to 1M, 10M with improvement of complaints.

DISCUSSIONDISCUSSIONWith Sepia the regularity of menstrual cycle was
established; generalities improved. But the dyspeptic troubles remained and it was < esp. in afternoon hours.
Following the drug relationship the remedy that follows Sepia well covering the P/c along with the tubercular diathesis, Lycopodium was prescribed in 200th and 1M potency. The pt. improved much after Lyco. 1M. and advised for USG which revealed Normal study.
The remedies used during the course of treatment also came during Repertorization.
USG of lower abdomen (TVS): Sonographic study within Normal limits. Both ovaries are normal in size and echo.

A CASE OF PCOSA CASE OF PCOSA female of 32 yrs (dt. of 1st visit: 1.12.10) presented with complaints: Amenorrhoea since 4 months; L.M.P.: August 2011. Menses: dark – red,
offensive, with clots and backache. Pt. felt better after menses. USG of Lower Abdomen : Endometrial thickness measures 8.5mm.
Rt Ovary measures 3.8*2.1*2.0 cm, Vol. 8.7cc; Lt. Ovary measures 2.8*2.6*2.2cm, Vol. 8.6cc. Both Ovaries show evidence of multiple small follicles ranging from 3 – 8 mm in size arranged mainly peripherally. No dominant follicle is noted.
OPINION : Findings consistent with POLYCYSTIC PATTERN OF OVARIES.
Leucorrhoea: copious, yellowish, offensive and before menses since 1 yr. Generalized weakness; constant backache in LS region and pain in
hypogastrium since 6 months. Severe pain in extremities esp. lower with subjective sensation of burning in
soles < night, washes them at least twice with water waking up in night and numbness in left lower extremity since 2 yrs.
Tendency to catch cold easily followed by severe headache esp. left sided from slightest draft of air since 2 yrs.

Past H/O : UTI (Cystitis); 2 Spontaneous Abortion at 3 months. Acne before the appearance of menses > with flow. 1 son and 1 daughter – FTNVD.
Family H/O : Mother : Renal calculi.P/G : Desire : salt, warm food, Aversion : sweet;
Perspiration from face, upper lip and tip of nose. Recurrent dreams of dead grand mother which disturbs her sleep and feels un-refreshed on waking up.
P/E : Coldness of palms and thick hair growth on upper lip and chin. Pt. was average built with fair complexion.
M/G : Likes company. Good marital relationship.
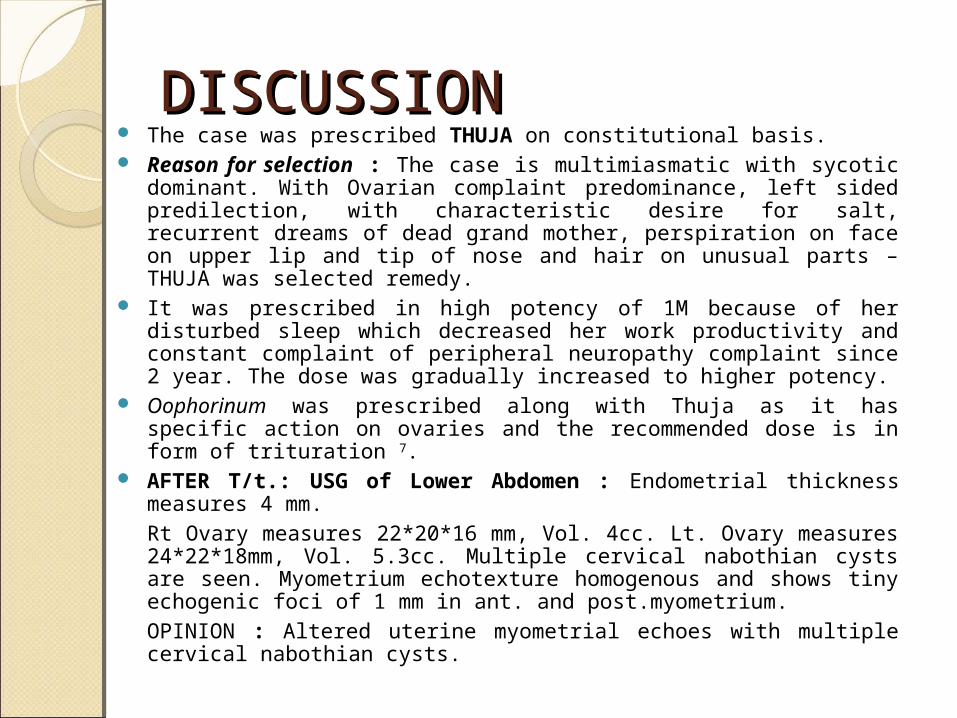
DISCUSSIONDISCUSSION The case was prescribed THUJA on constitutional basis. Reason for selection : The case is multimiasmatic with sycotic dominant.
With Ovarian complaint predominance, left sided predilection, with characteristic desire for salt, recurrent dreams of dead grand mother, perspiration on face on upper lip and tip of nose and hair on unusual parts – THUJA was selected remedy.
It was prescribed in high potency of 1M because of her disturbed sleep which decreased her work productivity and constant complaint of peripheral neuropathy complaint since 2 year. The dose was gradually increased to higher potency.
Oophorinum was prescribed along with Thuja as it has specific action on ovaries and the recommended dose is in form of trituration 7.
AFTER T/t.: USG of Lower Abdomen : Endometrial thickness measures 4 mm.
Rt Ovary measures 22*20*16 mm, Vol. 4cc. Lt. Ovary measures 24*22*18mm, Vol. 5.3cc. Multiple cervical nabothian cysts are seen. Myometrium echotexture homogenous and shows tiny echogenic foci of 1 mm in ant. and post.myometrium.
OPINION : Altered uterine myometrial echoes with multiple cervical nabothian cysts.

CONCLUSION Every woman suffering from PCOS/ Ovarian cyst
presents with different set of symptoms and hence differs evaluation and analysis of case in each sick individual.
The patient with PCOS if young are mostly concerned about their personal appearance and irregular menses.
The results of the presented cases of ovarian diseases is encouraging i.e., symptomatic improvement and disappearance of ovarian pathology, but these cases require long term follow ups with constant reassurance to patient to prevent drop out.
Whether it is treatment of hormonal imbalances, or regulating menstrual cycles, seeking relief from the side effects of prescribed medications or support in dealing with the stress and frustration associated with complications or the emotional turmoil of being diagnosed with PCOS/ Ovarian cyst, Homoeopathy helps to restore health on both the physical and emotional plane.

Homoeopathic medicines are cost effective, gentle and free from any side effects.
Various studies conducted till date establish a positive role in treating ovarian diseases5.
The need of the hour are well documented cases on ovarian diseases to achieve the target of evidence based medicine for Homoeopathy.
REFERENCES1. Howkins and Bourne. Disorders of the Ovary and Benign tumours: Non-
neoplastic enlargements of the ovary. Shaw’s Textbook of Gynaecology, 15th ed.Elsevier Publication; 2012. p. 369 -72.
2. Nidhi R, Padmalatha V, Nagarathna R, Amritanshu R. Prevalence of polycystic ovarian syndrome in Indian adolescents. J Pediatric Adolesc Gynecol 2011; 24; 223-7.
3. Yildiz BO, Knochenhauer ES, Azziz R. Impact of obesity on the risk for polycystic ovary syndrome. J Clin Endocrinol Metab 2008;93:162-8.
4. Hahnemann S. Organon of Medicine, 5thed. New Delhi: Pratap Medical Publishers (P) Ltd, Indian edition; 1994.
5. Gupta G, Gupta N, Singh R. Ultrasonographic case series study in cases of PCOS in response to Homoeopathic drugs. Homoeopathic Heritage March 2015; 40: 39-50.
6. Thomas R. Theft of womanhood – PCOS: Role of Homoeopathy. Homoeopathic Heritage August 2014; 40: 41-45.
7. Boericke W. Boericke’sNew Manual of Homoeopathic Materia Medica with Repertory, 3rd revised and augmented edition based on 9th edition.New Delhi :B.Jain Publishers (P) Ltd; 2008.
