explaining attendance at a breast-screening clinic
TRANSCRIPT

Patient Education and Counseling, 7 (1985) 87-96 Elsevier Scientific Publishers Ireland Ltd.
EXPLAINING ATTENDANCE AT A BREAST-SCREENING CLINIC
M.W. CALNANa’*, S. MOSSb and JOCELYN CHAMBERLAINb
%ealth Seruices Research Unit, University of Kent at Canterbury, Canterbury, Kent CT2 7NX and bSection of Epidemiology, Institute of Cancer Research, University of London, London (U.K.)
(Received May 22nd, 1984) (Accepted September llth, 1984)
ABSTRACT
This paper describes an analysis of the social, psychological and demo- graphic factors associated with attendance/non-attendance at a clinic provid- ing mammography and an examination carried out by medically-trained staff. Six hundred and fifty-four women aged 45-64 were interviewed approx. 1 month before they received an invitation to attend for breast screening. Seventy-two percent of these women subsequently attended the clinic. In all 30 different variables were measured. The attender could best be character- ised as someone who previously used other types of preventive health service, felt vulnerable to breast cancer and saw breast screening as being beneficial. The implications of these and other findings are discussed.
Key words: Breast screening - Health beliefs - Use of preventative services - Patient compliance
INTRODUCTION
A comparative multi-centre trial is currently being carried out in the U.K. [l] which is evaluating different methods for the early detection of breast cancer in well women. The two methods being evaluated are mammography with physical examination and breast self-examination (BSE). An analysis reported previously [2] examined the social, psychological and demographic factors which are associated with attendance at a class teaching BSE. A parallel analysis is presented in the following paper examining factors associated with attendance at a screening clinic.
*To whom correspondence should be sent at: Health Services Research Unit, University of Kent at Canterbury, Cornwallis Building, George Allen Wing, Canterbury, Kent, U.K.
0738-3991/85/$03.30 0 1985 Elsevier Scientific Publishers Ireland Ltd. Printed and Published in Ireland 87

Previous research has shown that the participant in programmes providing mammography has both distinctive sociodemographic characteristics [ 33 and health beliefs [4,5]. However, since then a wide range of different types of factor have been shown to be associated with decisions to use preventive health services. One of these factors is the availability of social networks [6] and studies have shown that those women with a strong network of support are more likely to participate in preventive health programmes than those who have less social support. In addition, health status [7] self-esteem [8] and social pressure [ 91 have each been shown to be associated with preventive health behaviour. Social pressure can involve direct pressure by friends, rela- tives or neighbours, or ‘normative’ pressure [lo]. The latter might be illus- trated by an individual feeling that they ‘ought’ to do something even though they might not feel that it will be particularly valuable for them.
In the area of health beliefs, three major dimensions [ll] (general health motivation, value of illness threat reduction and probability that compliant behaviour will reduce the threat) are said to be important in understanding health behaviour. These dimensions are said to act together to influence an individual’s decision to adopt preventive behaviour. Locus of control [12] is also believed to be an important factor in explaining health behavior. How- ever, more recently this general concept has been questioned and it has been suggested that an individual’s specific feeling of control over getting the disease in question is a more sensitive measure of personal control over health v31.
The aim of the study described here is to examine which, if any, of the factors described previously best explain attendance at a breast-screening clinic. However, another type of factor will be included which is previous experience of programmes for the early detection of breast cancer. Not only is it important to know if attendance is influenced by previous use of breast- screening services but also if attendance is associated with the use of possible alternatives such as BSE.
METHOD
The study was carried out in a health district included in the main trial [l] and was situated in a city in southern England. All women aged between 45 and 64 who are registered with general practitioners serving the district are included in the trial. Each woman was invited to attend a clinic situated either in the city or for those women living in outlying areas in a mobile clinic. Each woman attending the clinic was given a physical examination by a medically trained member of staff and mammography.
By the time this study had started all but six practices had received their first invitation to attend for screening and thus a 1 in 3 random sample was taken from the remaining population (3,660) giving a sample size of 1,180. However, due mainly to greater than predicted inaccuracies on the age/sex register this sample was reduced to 854 women eligible for interview.
The sample of women were interviewed in their own homes at least 1
88

month before the women received their invitation to attend the clinic. The interview schedules were administered by trained interviewers unconnected with the breast-screening team. Respondents had no prior knowledge that they were to be interviewed. While there was no media publicity about the breast-screening programme, in the local area women may have learnt infor- mally through friends and neighbours that they were to be invited to partici- pate particularly as the programme has been in existence for over a year. Data on whether the women attended the clinic or not were subsequently derived from information collected in the main trial.
Six hundred fifty-four (77%) of the 854 women were successfully inter- viewed. Of the 654, 471 women (72%) subsequently attended the clinic, which was higher than the attendance rate for the whole cohort (69%) and 139 (21%) did not. There was no information on attendance for 44 women (7%) who had been interviewed. The analysis was carried out on the 610 where there was information on attendance. There was a difference in partici- pation rates in the survey between attenders (84%) and non-attenders (64%). Thus, there is some evidence to suggest that the interview may have provided an additional cue (the invitation provided the other cue) to attend for breast screening.
Thirty independent variables were included in the study and each is de- scribed in Tables I, II, III and IV. The relationships between each of the vari- ables and attendance were examined independently using a chi-square test (see Tables I-IV)*. Then the 30 variables were analysed in combination using linear discriminant analysis to identify the strongest predictors of attendance at the screening clinic.
RESULTS
Socio-demographic characteristics Of the five socio-demographic characteristics only marital status was statis-
tically significantly associated with attendance at the screening clinic (see Table I). Women who were married were more likely to have attended than
TABLE I
SOCIO-DEMOGRAPHIC CHARACTERISTICS AND ATTENDANCE/ NON-ATTENDANCE AT THE BREAST SCREENING CLINIC
)i ’ -value d.f.
1 Social class 2.5 4 2 School leaving age 3.7 4 3 Age 7.3 3 4 Marital status 13.2** 3 5 Employment status 6.5 4
- *P < 0.05; **p < 0.01; ***p < 0.001.
*Detail of the tabulations can be obtained on request to M. Calnan.
89

TABLE II
HEALTH BELIEFS AND ATTENDANCE/NON-ATTENDANCE AT THE BREAST SCREENING CLINIC
x 2-value d.f.
Health motivation 6 Concern about health I Willingness to seek medical care 8 Previous use of cervical smear 9 Regular use of dentist for check-up
10 Pattern of personal health behaviour
5.4 1.7
22.5*** 19.5*** 24.7**
Value of illness threat reduction 11 Perceived vulnerability to breast cancer 12 Perceived vulnerability to illness in genera1 13 Concern about breast cancer 14 Past experience with breast symptoms 15 Previous experience of someone who had
had breast cancer
12.9** 10.6* 12.0*
2.3 0.2
Probability that compliant behaviour will reduce the threat 16 Perceived costs and benefits of breast
screening 17 Faith in medicine 18 Control over health (i) genera1 19 Control over health (ii) specific
8.0*
0.8 3.4
0.6
3
2 4 1
*p < 0.05; **p < 0.01; ***p < 0.001.
single women or women who were divorced, widowed or separated. Women aged over 60 were less likely to attend than younger women although the overall differences were not significant. Variations in attendance by social class and length of full-time education were small. Women who were working or who were housewives were more likely to attend than those who were retired or actively seeking work. These differences were not statistically significant.
Health beliefs (i) Health motivation. Of the three dimensions of health motivation, Table
II :hows that only the different elements measuring preventive health activities showed marked statistically significant variations in attendance. Women who had had a cervical smear test whether they deliberately sought it or not, were more likely to have attended. Similarly, women who reported going to the dentist for regular check-ups were more likely to have attended than those who did not.
Table II also shows that those who had adopted patterns of personal health behaviour which comply with recommended health actions (high scorers on health behaviour index) were more likely to have attended than those who were less compliant.
90

TABLE III
VARIABLES ASSOCIATED WITH THE EARLY DETECTION OF.BREAST CANCER AND ATTENDANCE/NON-ATTENDANCE AT BREAST SCREENING
20 21 22
23
24 25
Ever had breast screening Time since last breast screening Should have breasts examined more
often than do at present Ever discussed breast screening with
friends or family Practice of BSE (frequency) Practice of BSE (technique)
x ‘-value d.f.
1.1 2 6.3* 2
24.6*** 2
0.7 1
15.4** 3 5.9* 1
*P < 0.05; **P <’ 0.01; ***p < 0.001.
(ii) Value of illness threat reduction. Table III shows that women who felt vulnerable to breast cancer (moderately, high) or felt concerned about getting breast cancer (moderately, high) were more likely to attend than those who were assessed as having a low vulnerability to breast cancer or were not concerned about getting it. Both of these differences were signifi- cant. By contrast, on a more general level, those women who said they were more likely than other people to become ill were less likely to attend than those who said their vulnerability was the same or less than other people.
There was little variation in attendance according to whether the women had had direct or indirect experience of breast disease or not.
(iii) Probability that compliant behaviour will reduce the threat. Of the variables measuring this dimension of health beliefs (see Table III) the only marked variations in attendance were found in the perceived costs and bene- fits of breast screening. Women who though breast screening was beneficial were significantly more likely to attend than those who did not.
Previous involvement with programmes for the early detection of breast cancer
Women who had previously had mammography were less likely to attend than those who had no previous knowledge or experience of breast screening or those who had been screened previously but only by physical examination, although the difference was not significant (see Table III). Similarly, those who reported having breast screening in the last 2 years were less likely to have attended than those who had never been screened or had been screened over 2 years prior to the interview. However, women who felt that they should have their breasts examined more often than they did at the time of the interview were more likely to attend than those who felt they were examined often enough. There was little variation in attendance according to whether the respondent said she had discussed breast screening with others or not.
91

TABLE IV
ADDITIONAL VARIABLES AND ATTENDANCE/NON-ATTENDANCE AT BREAST SCREENING
Health 26 27
Health status Presence of an impairment that restricts
activity
x ‘-value d.f.
14.3** 4 9.4** 2
Social network and social support 28 Presence of confiding relationship 29 Number of close friends 30 Self-esteem
9.4* 3 11.3* 3 6.1* 2
*p < 0.05; **p < 0.01; ***p < 0.001.
Women who said that they had carried out BSE at least once in the past year (see Table III) were more likely to attend than those who said that they had not practiced it. However, women who said that they practised BSE at least once a month were less likely to attend than those who said that they had done it more than once every 6 months but not as much as once a month. Women whose reported practice complied with the recommended BSE tech- nique (see Table III) were more likely to have attended than those who did not.
Health status Both elements of health status were found to be statistically significantly
associated with attendance. Women who rated their health as good or very good were more likely to have attended than those who rated their health as fair or poor. Women who did not have any health problems that limited their activities or who had a problem which limited them in only certain things that they can do were more likely to have attended than those who said that they had a problem which kept them from doing a lot of things that they wished they could do (Table IV).
Social support Women who reported having a confiding relationship with their husband
boy-friend (see Table IV) were more likely to have attended than those who had no confiding relationship or had a confiding relationship with someone other than a husband or boy-friend such as a female confidante. Similarly, women who reported having at least one close friend were more likely to attend than those who said that they had no close friends.
Self-esteem Women who said that they were not a confident type of person (see Table
92
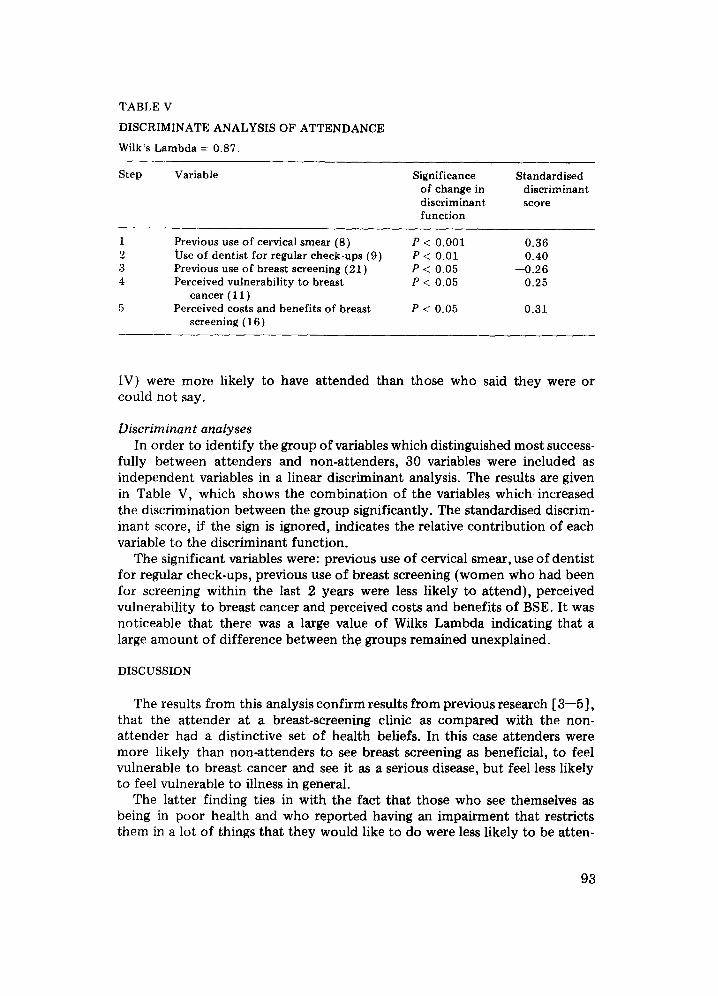
TABLE V
DISCRIMINATE ANALYSIS OF ATTENDANCE
Wilk’s Lambda = 0.87.
Step Variable
1 Previous use of cervical smear (8) 2 Use of dentist for regular check-ups (9) 3 Previous use of breast screening (21) 4 Perceived vulnerability to breast
cancer ( 11) 5 Perceived costs and benefits of breast
screening (16)
Significance of change in discriminant function
Standardised discriminant score
P < 0.001 0.36 P < 0.01 0.40 P <: 0.05 -0.26 P < 0.05 0.25
P <: 0.05 0.31
IV) were more likely to have attended than those who said they were or could not say.
Discriminan t analyses In order to identify the group of variables which distinguished most success-
fully between attenders and non-attenders, 30 variables were included as independent variables in a linear discriminant analysis. The results are given in Table V, which shows the combination of the variables which increased the discrimination between the group significantly. The standardised discrim- inant score, if the sign is ignored, indicates the relative contribution of each variable to the discriminant function.
The significant variables were: previous use of cervical smear, use of dentist for regular check-ups, previous use of breast screening (women who had been for screening within the last 2 years were less likely to attend), perceived vulnerability to breast cancer and perceived costs and benefits of BSE. It was noticeable that there was a large value of Wilks Lambda indicating that a large amount of difference between the groups remained unexplained.
DISCUSSION
The results from this analysis confirm results from previous research [ 3-51, that the attender at a breast-screening clinic as compared with the non- attender had a distinctive set of health beliefs. In this case attenders were more likely than non-attenders to see breast screening as beneficial, to feel vulnerable to breast cancer and see it as a serious disease, but feel less likely to feel vulnerable to illness in general.
The latter finding ties in with the fact that those who see themselves as being in poor health and who reported having an impairment that restricts them in a lot of things that they would like to do were less likely to be atten-
93

ders. This suggests that those in poor health may be less likely to see the value of engaging in preventive health behaviour than those in good health. Alternatively, the restrictions on those particularly with serious impairments may limit the extent to which the screening service is accessible to them.
No variations in attendance by social class or educational background were found although attenders were more likely to be married than non- attenders. This variation by marital status may be linked with the finding that those with a confiding relationship with a male were more likely to attend than those who did not have one suggesting that social support may be more likely to promote health behaviour. This is further supported by the evidence that those with a network of close friends were more likely to attend than those without close friends. However, the fact that those with a confid- ing relationship with a femaie only were less likely to attend than those with a confiding relationship with a male one suggests that the social support may not be the full explanation. It might be that those with a confiding relationship with a female only may also be more likely to be the sole parent and the explanation for a lower attendance rate may be due to circumstantial factors such as lack of time, energy or finance to pay transport costs.
The relationship between attendance at the screening clinic and the prac- tice of BSE as reported by the respondent was not as expected. Those who reported practicing BSE more than once a month were less likely to attend than those who practiced it once a month or less. This finding suggests that those who practice BSE regularly and more often than is officially recom- mended might see breast screening as unnecessary and see regular BSE as a preferable alternative to breast screening.
This study also provided a strong test of the Health Belief Model (HBM) in that the study design was prospective and that behaviour in relation to previous use of breast screening was taken into account. The evidence showed some, if only limited, support for the HBM in that four of the five best discriminators were elements contained in the three health dimensions of the HBM. However, the overall variance explained by the health belief dimensions was low as was the variance explained by the remainder of the variables. Pre- vious use of other preventive health services were the best predictors of attendance suggesting that once women begin to use one type of preventive health service they will see the value of attending breast screening.
The results of this analysis are different to those found in the parallel analysis [ 2 3 of attendance at a class teaching BSE. In the latter study, the best predictors of attendance were beliefs about vulnerability to breast cancer and previous pattern of personal health behaviour. These differences may be due to the differences in the social composition of the two samples [14]. Alternatively, it may be that different influences are involved in the decision making about attendance at the two different services. The familiarity and acceptability of screening services, at least relative to other preventive services, suggests that the invitation may be sufficient to prompt a decision to attend in the case of breast screening. However, in the case of attendance at the class teaching BSE the evidence suggested that decisions to attend were less
94

to do with ‘normative’ pressure (the service and the principles involved were relatively novel) and more to do with women’s beliefs about their vulnerability to breast cancer. Those women who were assessed as having a high vulner- ability to breast cancer were more likely to attend than those who had lesser feelings of vulnerability [ 21. Women do prefer the prospect [ 141 of attending breast screening to that of attending classes teaching BSE mainly because they have more confidence in medical screening and prefer the private setting of the consultation in the breast-screening clinic compared with the class. Thus, they may need additional influences other than general normative pressures to attend a service which is not altogether attractive. Perceptions of being ‘at risk’ may be the major motivating forces in these circumstances.
If the results from the trial [l] indicate that mammography in combination with a medical examination is a valuable method of detecting breast cancer early then there may be pressure to provide-a comprehensive breast-screening service in the U.K. One difficulty may lie in gaining a high rate of participa- tion. At the moment approx. 7 out of every 10 women in the population being studied accepted the first invitation to attend for breast screening. However, this attendance rate would have been considerably lower without the invitation. For example, a sample of those who attended were asked if they had not been invited would they have attended for breast screening if it was available. Sixty-six per cent of the attenders said that they would have attended, 31% said that they would not have and 3% gave no answer [ 151.
REFERENCES
1 U.K. Trial of Early Detection of Breast Cancer Group. Trial of early detection of breast cancer: description of method. Br J Cancer 1981; 44:618.
2 Calnan M, Moss S, Chamberlain H. Explaining attendance at a class teaching breast self examination. Patient Educ Corms 1984, in press.
3 Fink R, Shapiro S, Lewison R. The reluctant participant in a breast screening pro- gramme. Public Health Rep 1968; 83:479.
4 French K, Porter A, Robinson S, McCallum F, Howie J, Roberts M. Attendance at a breast screening clinic: a problem of administration or attitudes. Br Med J 1982; 285: 617.
5 Hobbs P, Eardly A, Wakefield J. Motivation and education in breast cancer screening. Public Health 1977; 91:221.
6 Langlie JK. Social Networks, health beliefs and preventive health behaviour. J Health Sot Behav 1977; 18:244.
7 Schwoom DR, Schmoll JH. Motivation to participate in cancer screening programmes. Sot Sci Med 1979; 13A:283.
8 Van Den Heuvel WJA. Participants and non-participants in a mammography mass screening: who is who? in Brand PC, van Keep PA (Ed.), Breast Cancer, MTP Press, London, 1978, pp. 97-104.
9 Vermost L. Factors affecting participation in screening programmes, in Brand PC, van Keep PA (Ed.), Breast Cancer, MTP Press, London, 1978, pp. 91-96.
10 Fishbein M, Ajzen I. Attitude, Intention and Behaviour. An Introduction to Theory and Research. Addison-Western, Boston, 1975.
11 Becker MH, Maiman LM. Socio behavioural determinants of compliance with health and medical care recommendations. Med Care 1975; 13:lO.
95

12 Wallston K, Wallston B. Locus of control and health: a review of the literature. Health Educ Monogr 1978; 6(2):107.
13 King J. The impact of patients perceptions of high blood pressure on attendance at screening. Sot Sci Med 1982; 16:1074.
14 Calnan M. Women and medicalisation: an empirical examination of the extent of womens’ dependence on medical technology in the early detection of breast cancer. Sot Sci Med 1984; 18(7):561.
15 Calnan M: Explaining womens’ participation in programmes for the early detection of breast cancer. Community Med 1984; 6( 3): 204.
96