exercise management cabg and ptca chapter 07. cabg – coronary artery bypass graft surgery ptca –...
TRANSCRIPT

Exercise ManagementExercise Management
CABG and PTCACABG and PTCAChapter 07Chapter 07
CABG – Coronary Artery Bypass Graft SurgeryCABG – Coronary Artery Bypass Graft SurgeryPTCA – Percutaneous Transluminal Coronary PTCA – Percutaneous Transluminal Coronary Angioplasty, aka. Percutaneous Coronary Angioplasty, aka. Percutaneous Coronary InterventionIntervention
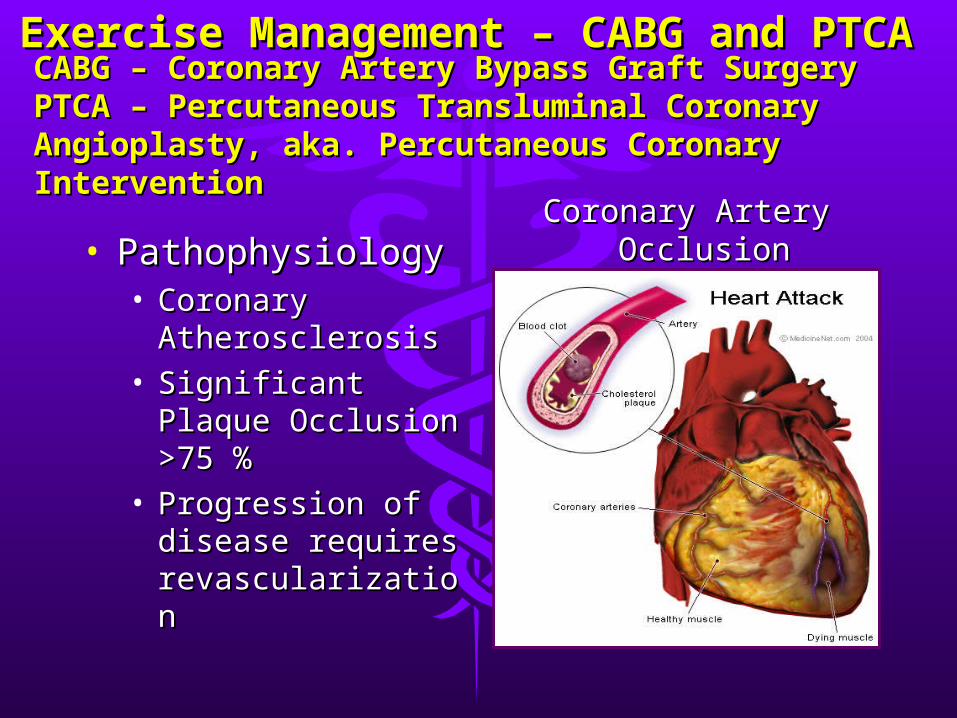
• PathophysiologyPathophysiology• Coronary Coronary
AtherosclerosisAtherosclerosis• Significant Plaque Significant Plaque
Occlusion >75 %Occlusion >75 %• Progression of Progression of
disease requires disease requires revascularizationrevascularization
Coronary Artery Coronary Artery OcclusionOcclusion
Exercise Management – CABG and Exercise Management – CABG and PTCA PTCA
Exercise Management – CABG and Exercise Management – CABG and PTCAPTCA
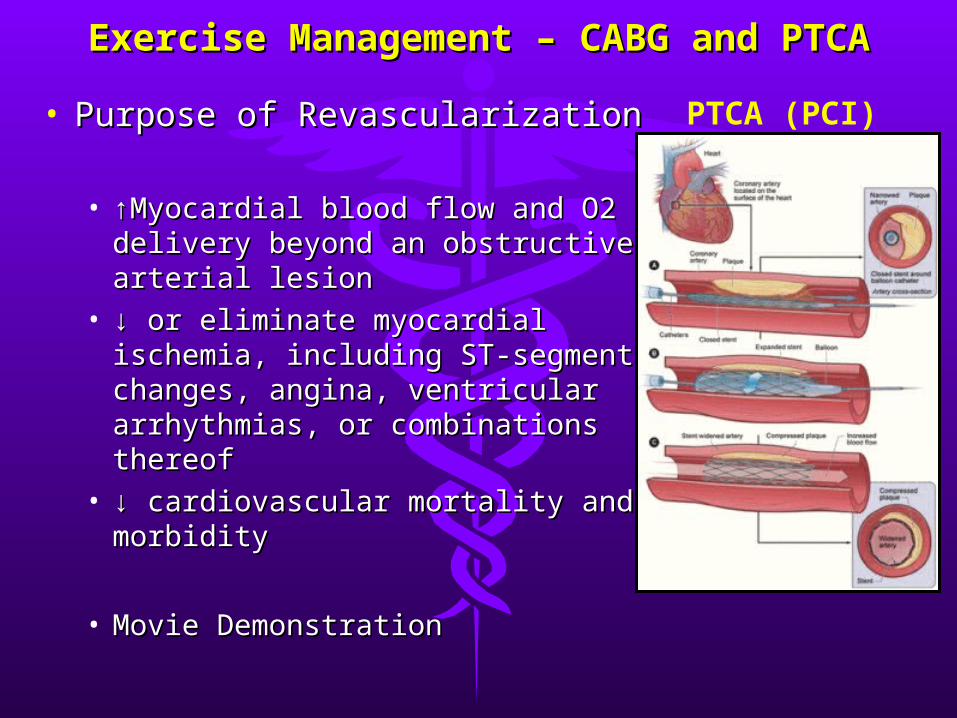
• Purpose of RevascularizationPurpose of Revascularization
• ↑↑Myocardial blood flow and O2 Myocardial blood flow and O2 delivery beyond an obstructive delivery beyond an obstructive arterial lesionarterial lesion
• ↓ ↓ or eliminate myocardial or eliminate myocardial ischemia, including ST-segment ischemia, including ST-segment changes, angina, ventricular changes, angina, ventricular arrhythmias, or combinations arrhythmias, or combinations thereofthereof
• ↓ ↓ cardiovascular mortality and cardiovascular mortality and morbiditymorbidity
• Movie DemonstrationMovie Demonstration
PTCA (PCI)
Exercise Management – CABG and Exercise Management – CABG and PTCAPTCA
• Indications for CABG Indications for CABG (follows cardiac cath.)(follows cardiac cath.)
• Relief of angina when pharmacologic Relief of angina when pharmacologic therapy is ineffectivetherapy is ineffective
• When PTCA is contraindicatedWhen PTCA is contraindicated• Prolong life in patient with multiple artery, Prolong life in patient with multiple artery,
or main artery disease, in patient with or main artery disease, in patient with ventricular dysfunction due to vascular ventricular dysfunction due to vascular diseasedisease
• Preserve LV function, especially following Preserve LV function, especially following an MI that has already compromised LV an MI that has already compromised LV functionfunction
Exercise Management – CABG and Exercise Management – CABG and PTCAPTCA
• CABG are performed on patients who have CABG are performed on patients who have multiple vessel disease and poor ventricular multiple vessel disease and poor ventricular function, and poor LV ejection fraction.function, and poor LV ejection fraction.
• Complications include infarction following Complications include infarction following surgery and (saphenous) grafts tend to surgery and (saphenous) grafts tend to remain open 90% at 1 year, 80% at 5 years, remain open 90% at 1 year, 80% at 5 years, and 60% at 11 years post surgery. and 60% at 11 years post surgery.
• Mammary grafts have 93%, 10 yr patency Mammary grafts have 93%, 10 yr patency (remain open) (remain open)
• The greatest incidence of graft occlusion The greatest incidence of graft occlusion occurs between 5-8 years post surgeryoccurs between 5-8 years post surgery
• Total relief of angina is typically 70% at 5 Total relief of angina is typically 70% at 5 years, approx. 50% are asymptomatic at 10 years, approx. 50% are asymptomatic at 10 yearsyears
Exercise Management – CABG and Exercise Management – CABG and PTCAPTCA
• Indications and Concerns for PTCAIndications and Concerns for PTCA• Originally the choice for single vessel Originally the choice for single vessel
diseasedisease• Now used to treat multiple vessel disease, Now used to treat multiple vessel disease,
impaired LV function, and to open an acute impaired LV function, and to open an acute occlusion during an MIocclusion during an MI
• If PTCA fails then CABG is used during If PTCA fails then CABG is used during surgerysurgery
• PTCA is less invasive and requires a shorter PTCA is less invasive and requires a shorter hospital stayhospital stay
• Arterial injury, thrombosis, and restenosis Arterial injury, thrombosis, and restenosis are the major complications of PTCAare the major complications of PTCA
• PTCA stints can now be coated with anti-PTCA stints can now be coated with anti-thrombic agents to help prevent restenosis.thrombic agents to help prevent restenosis.
Exercise Management – CABG and Exercise Management – CABG and PTCAPTCA
• Indications and Concerns for PTCA (PCI)Indications and Concerns for PTCA (PCI)• Risks and Complications:Risks and Complications:• Low risk symptomatic patients may not Low risk symptomatic patients may not
benefit any more from PCI than with benefit any more from PCI than with conservative treatmentsconservative treatments
• PCI may involve:PCI may involve:• Bleeding at the catheter insertion siteBleeding at the catheter insertion site• Blood clot or damage to the blood vessel at the Blood clot or damage to the blood vessel at the
insertion siteinsertion site• Blood clot within the vessel treated with PCI Blood clot within the vessel treated with PCI • Infection at the catheter insertion siteInfection at the catheter insertion site• Cardiac dysrhythmias /arrhythmiasCardiac dysrhythmias /arrhythmias• MIMI• Rupture of Coronary ArteryRupture of Coronary Artery
Exercise Management – CABG and Exercise Management – CABG and PTCAPTCA
• Benefits of PTCA (PCI)Benefits of PTCA (PCI)• Increases myocardial blood flow, thus:Increases myocardial blood flow, thus:
• Correct ischemic complications reflected in Correct ischemic complications reflected in exercise ECG response (T wave inversion and exercise ECG response (T wave inversion and ST-depression)ST-depression)
• Reduce angina on exertionReduce angina on exertion• Increase PWC (physical work capacity)Increase PWC (physical work capacity)• Improve Oxygen supply and demand (MVOImprove Oxygen supply and demand (MVO22) )
and improve contractility and hemodynamic and improve contractility and hemodynamic functionfunction
• May improve post-exercise chronotropic May improve post-exercise chronotropic impairment, and reduce the risk of impairment, and reduce the risk of hypotensive response (reducing likelihood of hypotensive response (reducing likelihood of pre-syncope)pre-syncope)
• Effects of Exercise TrainingEffects of Exercise Training• Many results are similar to those with post MIMany results are similar to those with post MI
• ↑ ↑ Max VoMax Vo22 (mean 20%) (mean 20%)
• ↓ ↓ myocardial demand (myocardial demand (↓ Submax HR and SBP for given workload↓ Submax HR and SBP for given workload))• ↑ ↑ glucose metabolism, ↓ insulin resistance, and glucose metabolism, ↓ insulin resistance, and
other typical changes in blood lipid profiles.other typical changes in blood lipid profiles.• In patients with stable CAD, PTCA (PCI) who In patients with stable CAD, PTCA (PCI) who
undertook a 12 month training program resulted undertook a 12 month training program resulted in a higher (event-free) survival rate. Each 1 in a higher (event-free) survival rate. Each 1 MET increase in exercise appears to confer 8-MET increase in exercise appears to confer 8-17% reduction in mortality.17% reduction in mortality.
Exercise Management – CABG and Exercise Management – CABG and PTCAPTCA
• Management and MedicationsManagement and Medications• Attempt to slow, halt, or reverse the Attempt to slow, halt, or reverse the
progression of atherosclerosis through progression of atherosclerosis through medication and health behavior medication and health behavior management (diet, exercise, stress management (diet, exercise, stress management), while maintaining the management), while maintaining the integrity of the vasculature addressed integrity of the vasculature addressed during surgery.during surgery.
• Poor prognosis includes: 1) recurrent Poor prognosis includes: 1) recurrent angina, 2) pre-syncope, syncope, and 3) angina, 2) pre-syncope, syncope, and 3) threatening forms of ventricular ectopy threatening forms of ventricular ectopy (multiform PVC, couplets, V-tach )(multiform PVC, couplets, V-tach )
• Repeat PTCA is the usual treatment for Repeat PTCA is the usual treatment for restenosis.restenosis.
Exercise Management – CABG and Exercise Management – CABG and PTCAPTCA
• Recommendations for Exercise TestingRecommendations for Exercise Testing• Exercise testing may begin earlier than for post Exercise testing may begin earlier than for post
MI patients (CABG = 3-5 weeks, PTCA 2-5 weeks)MI patients (CABG = 3-5 weeks, PTCA 2-5 weeks)• Cycle and Treadmill Tests commonly used with Cycle and Treadmill Tests commonly used with
CABG due to incision pain in the sternum areaCABG due to incision pain in the sternum area• Retest procedures should follow for any patients Retest procedures should follow for any patients
who are symptomatic within 5 years, and all who are symptomatic within 5 years, and all patients after five years.patients after five years.
• The combination of perfusion and exercise testing The combination of perfusion and exercise testing can detect ischemia and restenosis.can detect ischemia and restenosis.
Exercise Management – CABG and Exercise Management – CABG and PTCAPTCA
• Recommendations for Exercise TestingRecommendations for Exercise Testing• Supine cycle ergometry and echocardiography Supine cycle ergometry and echocardiography
may be used to dectect wall function may be used to dectect wall function abnormalities and provide prognostic information abnormalities and provide prognostic information for risk assessment if clinical restenosis.for risk assessment if clinical restenosis.
• ST-segment changes, CP, or both present in the ST-segment changes, CP, or both present in the follow-up exercise test (2-5 weeks) may be follow-up exercise test (2-5 weeks) may be indicative or restenosis .indicative or restenosis .
Exercise Management – CABG and Exercise Management – CABG and PTCAPTCA
Exercise Management – CABG and Exercise Management – CABG and PTCAPTCA
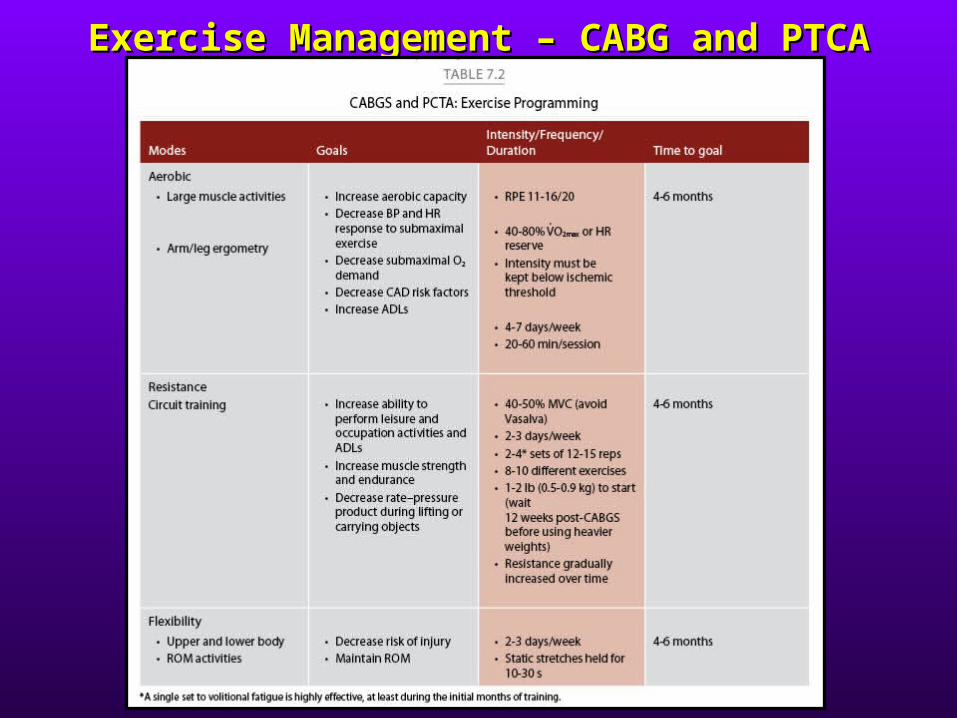
Recommendations for Programming Recommendations for Programming (see chart p. (see chart p. 63, also below)63, also below)
• Significant increases in functional capacity and ADL Significant increases in functional capacity and ADL will occur in the weeks following CABG and PTCA will occur in the weeks following CABG and PTCA ( improved myocardial supply)( improved myocardial supply)
• CABG and PTCA patients can typically begin CABG and PTCA patients can typically begin exercise programming sooner and at a more exercise programming sooner and at a more accelerated rate than post MI patients.accelerated rate than post MI patients.
• ROM exercises are indicated for CABG patients and ROM exercises are indicated for CABG patients and contraindicated with excessive sternal movements.contraindicated with excessive sternal movements.
• Individuals with > 4 MET capacity and who complete Individuals with > 4 MET capacity and who complete 12 week programs have less mortality risk12 week programs have less mortality risk
Exercise Management – CABG and Exercise Management – CABG and PTCAPTCA
Recommendations for Programming Recommendations for Programming (see chart p. (see chart p. 63)63)
• CABG and PTCA may begin inpatient exercise CABG and PTCA may begin inpatient exercise rehabilitation sooner than post MI and;rehabilitation sooner than post MI and;• Progress at a more accelerated rate, andProgress at a more accelerated rate, and• Devote more attention to upper extremity ROMDevote more attention to upper extremity ROM
• CABG focused ROM - 1) Shoulder ROM exercises; 2) Hip CABG focused ROM - 1) Shoulder ROM exercises; 2) Hip ROM exercises; Ankle ROM exercises.ROM exercises; Ankle ROM exercises.
Exercise Management – CABG and Exercise Management – CABG and PTCAPTCA
Exercise Management – CABG and Exercise Management – CABG and PTCAPTCA
End of PresentationEnd of Presentation
Exercise Management – CABG and Exercise Management – CABG and PTCAPTCA