exercise in advanced disease: benefit or burden?
TRANSCRIPT

Exercise in advanced disease: benefit or burden?
Matthew Maddocks MSCP FHEA PhD
Reader in Health Services Research
Specialist Physiotherapist
@MTMaddocks

Terminology
• Physical activity: any bodily movement produced by the skeletal muscles that results in energy expenditure
• Exercise: a sub-set of physical activity that is planned, structured and repetitive and has as a final or an intermediate objective the improvement or maintenance of physical fitness
• Rehabilitation: a set of interventions designed to optimize functioning and reduce disability in individuals with health conditions in interaction with their environment.
Caspersen. Public Health Reports 100(2) (1985) 126-131WHO, 2021 www.who.int/news-room/fact-sheets/detail/rehabilitation

Jones et al. Lancet Oncol 2009;10:598-605.
Cardiorespiratory fitness

Jones et al. Lancet Oncol 2009;10:598-605.
Chemotherapy induced anaemia
radiation induced pneumonitis
resection-related impairment
Age, comorbidities (cardiovascular), sedentary lifestyle
Cardiorespiratory fitness: effects of cancer

Activities of Daily Living (ADLs)
Basic Activities of Daily Living
(BADLs)
Instrumental Activities of Daily Living
(IADLs)
Feeding/eatingDressingBathing/showeringToiletingTransfers e.g. bed/chairAmbulation
Preparing foodHousekeepingShoppingDoing laundryUsing transportationHandling medicationsHandling finances
Activities of Daily Living
Essential activities that an individual needs to perform to live independently
Neo et al. Cancer Treat Rev 2017:61:94-1061/2
1/3
Reffin et al. JAGS 2018 doi.org/10.1111/jgs.15664

Gill et al. NEJM 2010;362:1173-80
Functional loss toward end of life

Cancer cachexia accelerates the loss of function
Fearon et al. Lancet Oncol 2011:12;489-95
LeBlanc et al. JPSM 2015:49;680-9Gibney ER. Proc Nutr Soc 2000:59;199–207
REE
PAEE
Naito et al. BMC Cancer 2017:17:800

What matters to people with advanced disease?
• Usual routines
• Continuing with important roles
• No longer feeling ‘who I once was’
• Being able to perform daily activities
• Adequate symptom control
• A sense of control
• Relieving burden
• Strengthen relationships with loved ones
• Maintaining dignity
• Sharing time with friends and family
• Not being a burden
Singer et al. JAMA 1999;Chochinov et al JPSM 2009; Steinhausse et al. JAMA 2000

GENERAL EVIDENCE FOREXERCISE IN CANCER

• >700 trials
• >50,000 pts
• ✓ safe
• ✓ feasible
• ✓ physical function
• ✓ psychosocial function
• ? disease progression
• ? survival
• ? treatment toxicity
• ? treatment efficacy
Current state of ‘exercise oncology’ science
Christensen et al. Compr Physiol 9:165-205, 2019.
69 national and international guidelines (2009-19) with rehabilitation guidance. All endorse, many provide population / treatment specific recommendations
Stout et al. CA Cancer J Clin 2021;71:149-75

Moderate-intensitys
aerobic training≥30 min, 3x /week,
resistance training2 sets, 8-15 repetitions,
2x /week
Campbell et al. Med Sci Sports Ex 2019
Scmitz et al. CA Cancer J Clin 2019

Sasso et al. J Cachexia Sarcopenia Muscle 2015.
Exercise prescription

Exercise safety and monitoring
ACS 2017; ACSM 2016
Considerations
• Monitor vital signs regularly
• Exercise with a partner
• Avoid public facilities with increased risk of viral/bacterial infection (e.g. swimming)
• Stop exercise if sudden:– dizziness, blurred vision, faint– nausea, vomiting– unusual shortness of breath– palpitations, chest pain– leg/calf, bone or unusual pain
Precautions
• Anaemia (“low”) - scale back or avoid
• Neutropenia (>100°F / 38°C) - avoid
• Thrombocytopenia (“low”) - avoid contact sports or activities with high risk of injury
• Catheter / line – avoid exposure to infection or exercises that may disturb
Mina et al. Lancet Oncol 2018;19e433-6
Bone metastases?
• 17 trials, n=1489 (43% bone mets, 57% allocated to exercise)
• Exercise screening criteria ± prescription modification (to reduce loading) + supervision
• 4 SAEs related to exercise (0.5% of pts allocated to exercise) (3 football intervention)
Campbell et al. Crit Rev Oncol Haem 2021

EVIDENCE IN ADVANCED DISEASE / KEY TRIALS

Evidence reviews in advanced cancer
• Rehabilitation advanced cancer (13 RCTs, n=1169). 7 RCTs (n=596) on exercise “associated with a significant improvement in general well being and quality of life”
Salakari et al, Acta Oncol 2015;54:618-28
• Exercise advanced cancer (15 RCTs, n=1208). Improved QoL, fatigue, insomnia, physical function, social function, breathlessness
Chen et al, JPSM 2020:59:734-49
• Rehabilitation cancer cachexia. (4 RCTs, n=178). Uncertain effect on lean body mass, physical performance, fatigue, QoL
Grande et al, Cochrane DSR, 2021;CDO10804
• Exercise and nutrition in incurable cancer. (8 studies, n=685). Improved physical endurance and depression.
Hall et al, Support Care Cancer 2019;27:2371-84
Overall positive accounts. Small studies. Mixing of terminology / populations. Methodological limitations studies and reviews.

• ↓ fatigue• ↑ exercise capacity• ↑ muscle strength• ↑ physical activity• ↑ SF-36 scores• Global QoL EORTC-C30
unchanged
Adamsen et al. BMJ 2009;339:b3410
n=269120 min, 4x/wkHigh intensity
Aerobic + Resistance 6 wks
• Large but select group

n=23160 min, 2x/wk
Modrate intensity, resistance >
aerobic, 8wks
Oldervoll et al. Oncologist 2010;89:611-6
• Loss to follow up 36% exercise vs. 23% usual care (death, disease progression)
• Survival markedly different in non-completers
• Fatigue unchanged, physical capacity improved

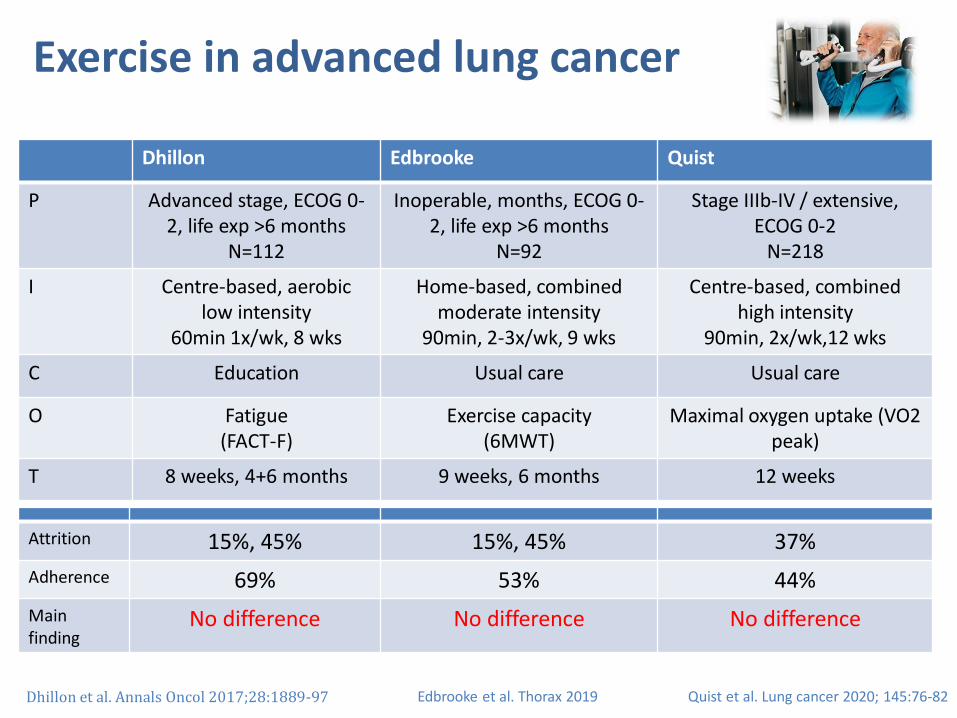
Exercise in advanced lung cancer
Edbrooke et al. Thorax 2019
Dhillon Edbrooke Quist
P Advanced stage, ECOG 0-2, life exp >6 months
N=112
Inoperable, months, ECOG 0-2, life exp >6 months
N=92
Stage IIIb-IV / extensive, ECOG 0-2
N=218
I Centre-based, aerobic low intensity
60min 1x/wk, 8 wks
Home-based, combined moderate intensity
90min, 2-3x/wk, 9 wks
Centre-based, combined high intensity
90min, 2x/wk,12 wks
C Education Usual care Usual care
O Fatigue (FACT-F)
Exercise capacity (6MWT)
Maximal oxygen uptake (VO2 peak)
T 8 weeks, 4+6 months 9 weeks, 6 months 12 weeks
Dhillon et al. Annals Oncol 2017;28:1889-97 Quist et al. Lung cancer 2020; 145:76-82
Exercise in advanced lung cancer
Edbrooke et al. Thorax 2019
Dhillon Edbrooke Quist
P Advanced stage, ECOG 0-2, life exp >6 months
N=112
Inoperable, months, ECOG 0-2, life exp >6 months
N=92
Stage IIIb-IV / extensive, ECOG 0-2
N=218
I Centre-based, aerobic low intensity
60min 1x/wk, 8 wks
Home-based, combined moderate intensity
90min, 2-3x/wk, 9 wks
Centre-based, combined high intensity
90min, 2x/wk,12 wks
C Education Usual care Usual care
O Fatigue (FACT-F)
Exercise capacity (6MWT)
Maximal oxygen uptake (VO2 peak)
T 8 weeks, 4+6 months 9 weeks, 6 months 12 weeks
Dhillon et al. Annals Oncol 2017;28:1889-97 Quist et al. Lung cancer 2020; 145:76-82
Attrition 15%, 45% 15%, 45% 37%
Adherence 69% 53% 44%
Main finding
No difference No difference No difference

Dhillon2,4,6 months
Edbrooke9 weeks
Edbrooke6 months
Quist12 weeks
Fatigue (FACT-F score) Exercise capacity (6MWT) Exercise capacity (6MWT) VO2 peak (L/min)
Fatigue (FACT-F cut off) Steps per day Steps per day VO2peak (mL/min/kg)
QoL (EORTC-C30) MVPA per day MVPA per day Leg press, 1RM (kg)
EORTC emotional Self-reported PA Self-reported PA Chest press, 1RM (kg)
EORTC physical Quadriceps strength Quadriceps strength Lat. machine, 1RM (kg)
EORTC role Hand grip strength Hand grip strength Leg extension, 1RM (kg)
EORTC social FACT-L total FACT-L total 6-min walk distance (m)
Anxiety / depression (GHQ) FACT-L LCS FACT-L LCS FEV1 (L/sec)
Distress thermometer FACT-L TOI FACT-L TOI FACT physical well-being
Sleep (Pittsburgh) AQoL utility AQoL utility FACT social well-being
Dyspnoea (SDSBQ) MDASI-LC—symptom severity MDASI-LC—symptom severity FACT emotional well-being
Basic ADLs MDASI-LC—symptom distress MDASI-LC—symptom distress FACT functional well-being
Extended ADLs HADS anxiety HADS anxiety FACT lung cancer
Social cognitive determinants HADS depression HADS depression FACT trial outcome Index
BREQ-2—amotivation BREQ-2—amotivation FACT general
BREQ-2—external regulation BREQ-2—external regulation FACT-L total score
BREQ-2—introjected regulation BREQ-2—introjected regulation HADS anxiety
BREQ-2—identified regulation BREQ-2—identified regulation HADS depression
BREQ-2—intrinsic regulation BREQ-2—intrinsic regulation
PAAI PAAI
CD-RISC CD-RISC

✓Well controlled trials in difficult populations
• Exercise prescription and/or adherence not always sufficient to measurably improve physical capacity
• Physical capacity ≠ quality of life
• Selective attrition and variation in physical trajectory
• Rehabilitation challenges in population:
– ? more ‘biographical disruption’
– ? higher treatment demands
– ? sub-optimal integration with oncology
Interpretation

• P: stage IIIC-IV solid or haematological cancer, life expectancy >6 months (n=516)
• I: physio- and physician-led rehabilitation (step counts and indoor resistance exercises) 90 min, four times weekly, 8 weeks ± nurse-led pharmacological pain management
• C: usual care• O: function, pain, QoL, hospital days, cost
Cheville et al. JAMA Oncol 2019

All 6 month duration
Usual care
• automated monthly monitoring (telephone or web) for pain and function
• summary reports to team coordinating the patient’s care
Intervention
Cheville et al. JAMA Oncol 2019

Telerehabilitation
• Individualised exercise programme delivered by phone
• Experienced physical therapist
• Pedometer-based walking
• Resistance exercise using bodyweight and TheraBand™
• Non-drug strategies to manage pain
• Patient report of exercise adherence
• Option to request a physical therapist phone call
• Weekly team review meetings (PT, physician) to track reporting
• Referral to local outpatient physical therapists with support to individualise to cancer population
Cheville et al. JAMA Oncol 2019
Intervention

Pharmacological pain management
• Stepped care approach to optimizing analgesics
• Nurse pain care manager, call on report of moderate pain
• Structured algorithm based on patient history, presentation, preference, response, side effects
Cheville et al. JAMA Oncol 2019
Intervention

Usual care
RehabRehab + pharm
Findings
Relative to usual care:
Rehabilitation group:↑ function↑ quality of lifeBoth groups↓ pain intensity↓ pain interference
Cheville et al. JAMA Oncol 2019

• Total hospital days in usual care group 57% more than rehabilitation group and 18% more than combined rehab and pharm group.
• Rehabilitation led to shorter not fewer hospitalisations
• Incremental cost-effectiveness ratio $15 494/QALY and cost saving once downstream hospital costs accounted
* < 0.05 Usual care Rehabilitation Rehab + pharm
Hospitalizations 45 61 57
Total hospital days 335 213* 284
Length of stay 7.4 (9.3) 3.5 (4.3)* 5.0 (7.2)
Discharge home (n,%) 20 (44) 45 (74)* 41 (72)*
Planned admission (n,%) 8 (18) 24 (39) 17 (30)
Cheville et al. JAMA Oncol 2019; Cheville et al Cancer Med 2020;9:2723-31
Findings

✓ Collaborative rehabilitation improved self-reported function and pain, and reduced hospital length of stay
✓ Large trial sample size, low attrition, high data reporting
✓ Excellent use of limited specialist expertise to enrich community rehabilitation provision
• Unexpected finding that addition of drugs had no additive effect on pain control and reduced impact on function
• Modest effect sizes for health outcomes in keeping with remote ‘light touch’ delivery
• Missing objective measures of physical performance
Interpretation
Patel JAMA Oncol 2019; Cheville et al. JAMA Oncol 2019


Contextual factors influencing behaviour
Granger et al. Annals ATS 2016;13:2215-22Granger et al. Support Care Cancer 2017;25:983-99

Patient experiences of exercise
• Sense of group belonging and commitment
• Group security, caring, empowerment
• Supportive relationships, camaraderie
• Change of focus, from sickness to health
• Deeper appreciation of own abilities
• Sense of achievement and work
• Source of positivity and focus, uplifting, calming
• Promotion of self-management, space to reflect
• Reclaiming control / not giving up hope
Paltiel et al. Pall Supp Care 2009;7:459-67
Malcom et al. BMC Pall Care 2016;15:97 Turner et al. Prog Pall Care 2016;24:204-12
Krishna et al. BMJ Case Repoer 2014;

• In public gyms, focus on high performance, not compatible with current health
• Comparison with others ability
• Noticing decline linked to measurement
• Sense of loss when others stop attending or die
Paltiel et al. Pall Supp Care 2009;7:459-67
Turner et al. Prog Pall Care 2016;24:204-12
Patient experiences of exercise

Patient and family views on exercise
Advanced lung / GI cancer and cachexia
• Low self‐efficacy, mismatch between ‘ask’ and perceived abilities
• Low confidence exercise would reduce effects of cancer
• Concerns exercise could worsen symptoms and cause harm
• Low feeling of control over choice to exercise, strong need for approvaland lack of direction staff (e.g. oncologist)
• Weather, premorbid fitness and exercise participation
Family ambivalent about promoting exercise
• Aware of potential value, but constrained in willingness to promote
– established boundaries of relationships
– support of individual autonomy
• General focus on ‘staying active’ as source of exercise
Wasley et al Psych-Oncol 2018:27:458-64Cheville et al JPSM 2012:44:84-95
Rhudy et al Comm Supp Oncol 2015;2015:392-99

Why were patients not receptive?
• Too busy for rehabilitation treatment demands, appointment conflicts
• Rehabilitation not necessary can manage myself, have done before, no need
• Waiting for a better time after treatment, test result, symptom improvement, worsening of disease
• Rehabilitation not beneficialalready tired it, don’t believe, fatalism about disease
• Rehabilitation is burdensome symptoms, limitations, transport, affordability
Sources of resistance to exercise
Cheville et al Arch Phys Med Rehab 2017;98:203-10
Advanced lung cancer n=311

IMPLICATIONS

Take a broad approach to screening and referral
Stout et al, Cancer 2020:2750-58

Goal setting can be used to:
• understand what patients want to achieve
• direct treatment in a manner that values their priorities (and benefit / burden of exercise)
Understand patient priorities and values
Rank ICF domain Frequency
N (%)
1 Mobility (e.g. walking, carrying objects, driving, transportation) 114 (18)
2 General tasks and demands (e.g. transfers, stairs) 100 (16)
3 Mental functions (e.g. confidence, anxiety, energy, fatigue) 100 (16)
4 Community, social and civic life
(e.g. to go home, to go out with family, partaking in hobbies)
99 (15)
5 Self-care (e.g. washing, dressing, toileting, eating, drinking) 68 (11)
Median (range) timescale of 28 (4-56) days

Consider exercise as part of a wider approach
Rehabilitation should go beyond exercise training with education, behaviour change, self-management, empowerment, nutrition, symptom control, social networking etc.

• Exercise interventions should be considered for people with advanced cancer (and other diseases)
• Changes in exercise capacity often require intensive, supervised programmes, which are not always acceptable or practical
• Time (prognosis) and identity are important to patients when considering their ‘trade-off’ for exercise
• We should encourage and support physical activity, but be realistic about the evidence for effects
Exercise in advanced disease:Benefit or burden?
