ew part ii - department of internal medicine -...
TRANSCRIPT

1

NEW HOUSESTAFF MEETING PART II MONDAY JUNE 10, 2013
HASSAN DOUMIATI ,MD MEDICAL CHIEF RESIDENT
DEPARTMENT OF INTERNAL MEDICINE

OUTLINE
→1-Professionalism and Behaviors
→2-Intern’s responsibilities
→3-Dress Code
→4-Chart work
→5-Teaching activities
→6-Evaluation/ ACGME core competencies
3

PROFFESSIONALISM AND BEHAVIORS

→Primacy of patient welfare
Placing the interests of patients above those of the physician
PROFESSIONALISM/ BASIC PRINCIPLES

→Patient autonomy
Patients’ decisions about their care must be paramount
→Honesty with patients
Physicians must ensure that patients are completely & honestly informed before the patient has consented to treatment & after treatment has occurred
TALK TO YOUR PATIENTS
PROFESSIONALISM/ BASIC PRINCIPLES

→Social justice
No discrimination in health care, whether based on race, gender, socioeconomic status, ethnicity, religion, or any other social category
→Professional competence
Physicians must be committed to lifelong learning & be responsible for maintaining the medical knowledge & clinical skills necessary for the provision of high quality care
PROFESSIONALISM/ BASIC PRINCIPLES

DEPARTMENTAL POLICIES
Departmental policies can be accessed online through the department’s website

→The intern has the responsibility of:
Patient care
Teaching medical students
Improve his own knowledge
INTERN’S RESPONSIBILITIES

CHART WORK
→
“The most feared stationery item a physician can receive is the envelope with the return address of a lawyer. Good documentation in the medical record is a key factor in helping to allay some of this fear”
“Jerome Greenberg, M. D.”

12
→The main reason for maintaining medical records is to ensure continuity of care for the patient

CHART WORK
→Integral part of patient care (the only evidence)
→Includes/not limited to
↘Problem list
↘Admission note
↘Progress note
↘Laboratory flow sheets
↘On call note
↘On/Off service
↘Discharge summary
↘Procedure note etc.

Routine checking of the medical record and notes will be performed by the medical chief resident and during chairman rounds
Update your problems list everyday !!!

DRESS CODE
→ Clean and closely shaved
→ Neckties (preferred)
→ Jeans, shorts, t-shirts, sweat-shirts, sweatpants, jackets/vest or crop tops/low cut tops, polo shirts are NOT TOLERATED
→ Scrubs accepted ONLY on duty hours (1700-0700)
→ A clean white physician coat at ALL TIMES
→ Sports shoes are not tolerated / open shoes neither
→ Identification BADGES should be visible and worn above the waist at ALL TIMES


PRE-ROUND CHECKLIST

Pre-round checklists will be provided and will include all relevant information to be addressed during morning assessment and evaluation


FRONT SHEET
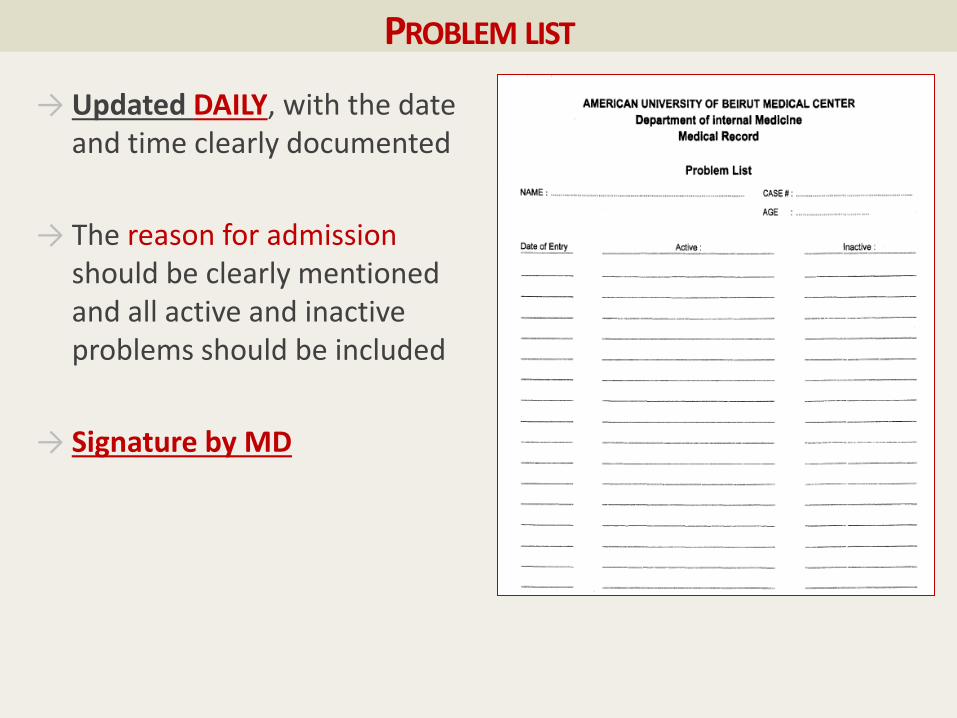
PROBLEM LIST
→ Updated DAILY, with the date and time clearly documented
→ The reason for admission should be clearly mentioned and all active and inactive problems should be included
→ Signature by MD

ADMISSION NOTE
→ It should be written within 4 hours of the patient’s arrival to the floor
→ The POMR form should be filled on all new admissions
→ A readmission note can be written for the patients readmitted within one month
→ A special admission form exists for chemotherapy/biologics one day admissions. These admissions are fully taken care of by the attending or fellow concerned.
→ (1 day adm for blood transfusion are seen by interns)


ADMISSION NOTE
→The admission note should include
Chief complaint / reason for admission
History of present illness
Past medical + past surgical history with dates
Medications (doses, frequency, duration)
Family history (detailed)
Social history
Allergies
System review

ADMISSION NOTE
→The admission note should include
Detailed physical examination
Assessment and plan:
Brief summary of the case
Appropriate differential diagnosis
Tests and justification for ordering them
Response to any abnormal results
Discussion of treatment chosen

27
POMR


THROMBOEMBOLISM PROPHYLAXIS SHEET

ORDERS
→Should be written
↘Within the first hour of the patient’s arrival to the floor
↘Promptly after evaluation of the patient
↘By the PGY1 or student
↘Under the supervision of the senior resident

ORDERS
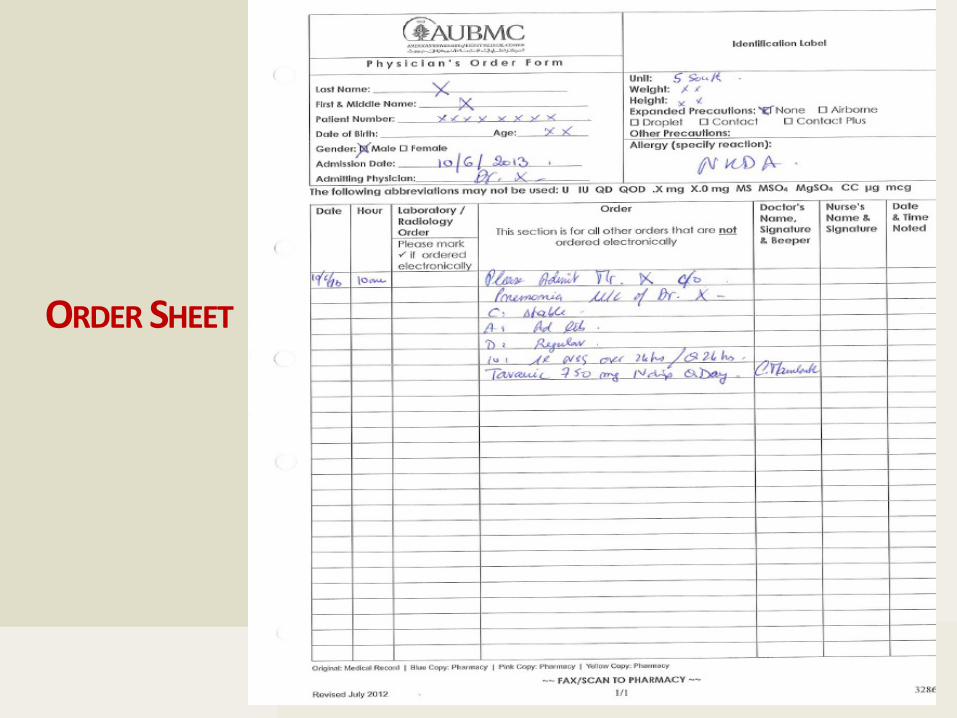
→All orders should
↘Have date and time
↘Clear, concise, organized and legible
↘Be signed and the name should be clear and written in FULL or stamped
↘Be always written
↘Be communicated orally to responsible RN when STAT

ORDERS
→All orders should
↘BE COUNTER SIGNED by an MD latest by the next morning during the morning round (when written by students)
↘Color indicators on the medical record folder:
↘RED Stat order
↘YELLOW all other orders

ORDERS
→Some orders are written only by attendings and fellows (e.g. chemotherapy)
→NO over-writing is allowed
→In changing an order, the old order must be specifically cancelled before a new one is written
→Only the abbreviations approved by the AUB-MC should be used
→Order revision every week responsibility of PGY1/student
34
ORDER SHEET
BLOOD SAMPLING AND EKG
→ Phlebotomy rounds: 0700, 1100, 1300, 1600 and 1900
→ Requests done ahead
→ Urgent blood draws taken by the student/PGY1
→ Blood cultures should always be drawn by housestaff (at any time)
→ ABGs: inhalation team; any time
→ EKG team on weekdays until 1800 and Sunday afternoon
→ EKGs to be done by medical team after hours, on weekends and when needed urgently

→All EKGs should be labeled and sent for reading
→Flagging of blood transfusions on the red laboratory sheet is done in red ink as detailed on the sheet
→Flagging of body cultures taken with appropriate date and time on the green laboratory sheet, ASAP
→Documenting studies that are taken and needs time to be out

MEDICAL RECORDS SHEETS

PROGRESS NOTES
→ Written DAILY by the first year resident or student including weekends and holidays
→ For chronic cases, it can be written once weekly if no active problems arise (no new orders written) in agreement and after approval of the team leader
→ Written in the SOAP format and should include:
↘Date and time
↘Appropriate title (PGY1, Med IV)
↘Signature and co-signature of the senior resident

PROGRESS NOTES
→S: Subjective
↘Address events over interval since last note
↘Documentation of patient concerns
→O: Objective
↘Vital signs (HR, BP, RR, Sat)
↘Pertinent physical exam tailored to the clinical problem and any change in the exam
↘X-rays + labs: Any abnormal labs or important normal labs

PROGRESS NOTES
→A/P: Assessment & Plan
↘Briefing of the current patient’s status
↘Address abnormal labs (interpretation and management)
↘Ongoing diagnostic testing plans
↘Discussion and justification of treatment chosen
↘Response to initiated treatment
↘Discussion with patient and family
↘Discharge planning

ON CALL NOTE
→If any problem or event occurs during the call time, a clear, precise and adequately dated note should be written in order to keep everything documented.
→Done ASAP
→Medico-legal

CONSULTATIONS
→ ASSESS the patient
→ Write the consultation order
→ Fill out the consultation sheet
↘Specify the service and the attending requested
↘Specify type of consultation (urgent, regular etc.)
→ Call the consultant physician or the fellow:
↘Give him/her a concise and focused presentation and ASSESSMENT including the REASON FOR CONSULTATION
→ Request to be called to discuss the case upon consultation
→ Should be done as early as possible during the day
→ Mark “informed” when informed

43

→All procedure notes should be flagged (red) →Should include:
↘Date and time ↘Procedure performed - Reasons for performing
procedure ↘Risk and benefit discussion with family/patient – ↘Consent obtained (verbal vs. written)
→Should add procedure log in myevaluations.com
PROCEDURE NOTES

45
INFORMED CONSENT
→ Before procedures, blood transfusion etc.
→ Should be INFORMED

PROCEDURE NOTES

MY EVALUATIONS - PROCEDURES
47

TRANSFER/ACCEPTANCE NOTE
→ Detailed summary of the history of present illness
→ Past medical history
→ Social history, allergies, family history etc.
→ Events since admission
→ Full same day physical exam
→ Comprehensive, clear problem oriented plan

DISCHARGE SUMMARY
→ This is the note the patient will take home or to his other care providers/legal document
→ Sums up the admission note and all hospital events
→ The first page of the discharge summary is to be written by the admitting first year resident/medical student
→ This page will include a brief summary of the history of present illness, pertinent physical exam findings, in addition to the results of the pertinent labs and imaging studies.
→ The second page will be completed by the senior resident or attending physician
→ Discharges should be made as early as possible (before 10 am)

DISCHARGE SUMMARY

ON-SERVICE, OFF-SERVICE
→The on-service note is written by the PGY1 or student who will start taking care of the patient
→The off-service note is written by the PGY1 or student who was the last taking care of the patient and now delegating his care to others
→Similar to transfer notes
→This will be the first note you write next Monday !!

SIGN IN AND SIGN OUT
→Sign out should be complete, clear, systematic
→Integral part of patient care
→Affects quality of care and patient outcome

TEACHING ACTIVITIES

MORNING REPORTS
→Four morning reports per week
→Attended by all inpatient housestaff
→and the float team once a week
NOON CONFERENCE
→Daily MANDATORY noon conference:
↘Core curriculum
↘Grand rounds
↘Journal clubs / Ambulatory reports
↘Board review sessions
↘Morbidity and Mortality conferences
↘EKG/Radiology rounds
→Meetings with residency program

ATTENDANCE LOG
AT LEAST 60% of assigned activities for a passing motion

→Weekly divisional activity
↘Case presentation
↘Journal club
→Schedule sent weekly by the department including all departmental activities
SUBSPECIALTY CONFERENCES

→First year residents are responsible for:
↘Close supervision of the performance of the medIII students (Team 5S and 10)
↘Providing help and assistance as a second call for medIV students (Inpatients)
TEACHING RESPONSIBILITIES
AMBULATORY CARE CURRICULUM

JOHNS HOPKINS IM AMBULATORY CARE CURRICULUM
→case-based modules covering the commonly encountered ambulatory medicine topics
→49 modules (23 mandatory)
→Follow up on your progress on completing these modules will be reviewed by the Program Director
61

62

EVALUATION/ ACGME CORE COMPETENCIES
→Interpersonal and communication skills
→Medical Knowledge
→Patient care
→Practice based learning
→Professionalism
→System based practices




ABSENTEEISM AND SICK LEAVES
→ Housestaff should NOT leave the hospital without notice
→ Any first year resident who needs to leave for a short period of time for any VALID reason should inform his/her senior resident and leave the pager with a covering colleague to whom his/her patients will be signed out
→ All illnesses should be reported, in a timely fashion, to the the program director or associates and to the MCRs who should decide about the need for a formal medical evaluation by an attending physician (ER)

EMAIL ACCESS
Daily email checking is essential – important messages

THANK YOU