e.w. - 83 yof -...
TRANSCRIPT



� E.W. - 83 YOF
� Caucasian, Catholic, widowed, resides in Queens, lives alone (for 33 years), her 2 nieces are main people involved w/ her care
� Retired secretary (12 years ago), walked 13 blocks to and from her church to volunteer everyday after retirement up until her illness.
� Smoked 3 cigarettes/day for 20 years (quit many years ago), has alcohol 1x/month
� Admission: 3/21/12
� Admitting DX: Ampullary CA

� Cooks all of her own meals
� Sample day (before illness): � Breakfast- oatmeal, blueberry muffin, Ensure � AM Snack- Ensure � Lunch: Turkey sandwich on rye, potato salad, Pepsi, Ensure � PM Snack: Ensure � Dinner: rice pudding, jello, Pepsi, Ensure
� Meds/Vits: amlodipine (antihypertensive), MVI
� No Food Allergies

� No significant past medical problems � Mild HTN- treated years ago and stopped medication
� Prior to dx, no previous hospitalizations
� Jan 2012: First sign of symptoms � 1/14: Presents w/jaundice, excoriation from severe pruritus,
dysguesia, B/L LE weeping edema, tea-colored urine and clay-colored stools � Abdominal CAT scan è suggested periampullary neoplasm
� 1/16: EUS è ampullary mass w/ lesion, dilatation of CBD and pancreatic duct (c/w cholestasis)
� 1/18: ERCP è Ampullary CA confirmed, balloon stent was placed in bile duct SURGERY PLANNED

� Surgery planned for 3/21/12
� Admitting symptoms: jaundice subsided, 30# wt loss, nausea, LE vascular lesions, NPO for surgery
*Staging Laparoscopy w/ US, Whipple, Omenectomy, and J-tube insertion
� Surgical Pathology RESULTS:
*No luminal stones in gallbladder
*No mass lesions identified in omentum
*No malignancy in liver
*No malignancy in surrounding lymph nodes

T2 N0
M0
*T2: Tumor limited to the pancreas, >2cm in greatest dimension *N0: No regional lymph node metastasis
*M0: No distant metastasis

� 3/22
� NG tube placed to suction serosanguineous fluid � Epidural given for pain � Leg dressings changed daily � Meds given: heparin, metoprolol, protonix, narcan
� 3/23
� Low urine output noted è IV LR @100cc/hr � *NUTRITION ASSESSMENT

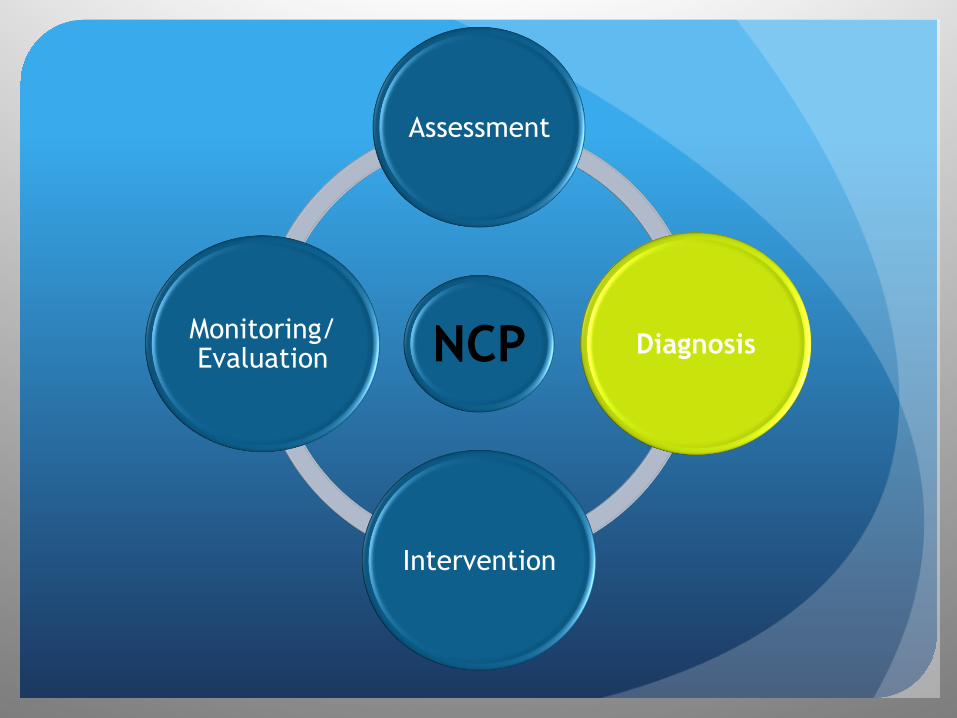
NCP
Assessment
Diagnosis
Intervention
Monitoring/Evaluation
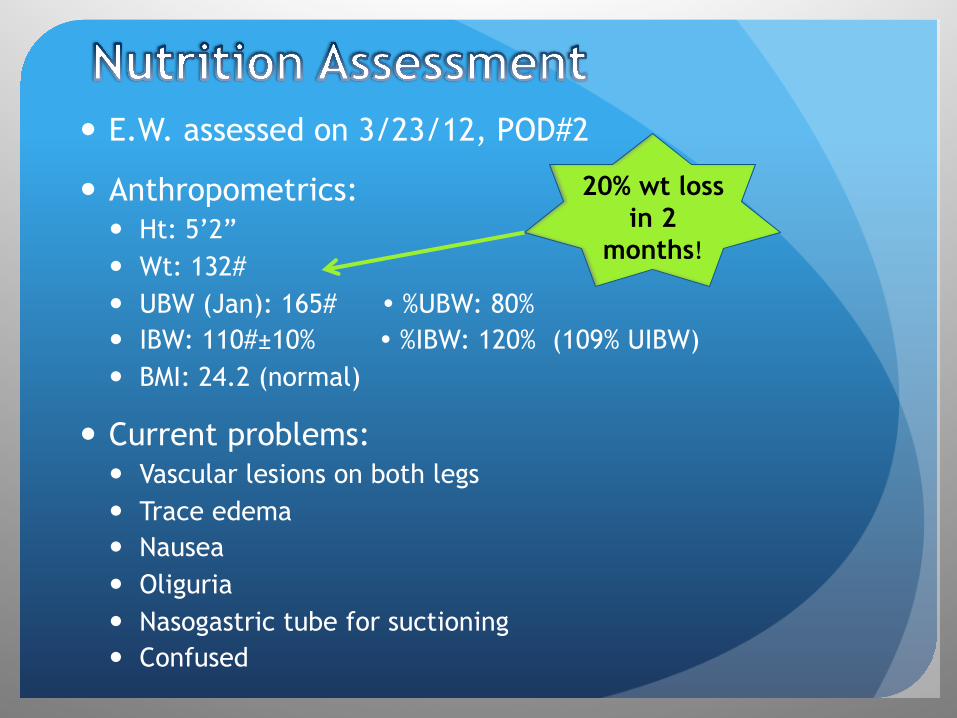
� E.W. assessed on 3/23/12, POD#2
� Anthropometrics: � Ht: 5’2” � Wt: 132# � UBW (Jan): 165# � %UBW: 80% � IBW: 110#±10% � %IBW: 120% (109% UIBW) � BMI: 24.2 (normal)
� Current problems: � Vascular lesions on both legs � Trace edema � Nausea � Oliguria � Nasogastric tube for suctioning � Confused
20% wt loss in 2
months!

� Nutrient Requirements:
� 1500-1800 kcal (25-30 kcal/kg) � 72-90 gm protein (1.2-1.5 gm/kg) � 40-60 gm fat � 213-225 gm carbohydrate � ~1500 ml H20 (25ml/kg) *Based on her actual body weight
� Current diet order per MD: � NPO � Jevity 1.5 @ 20cc/hr via J-tube (goal rate of 40cc/hr)
� Providing 720kcal, 31gm pro, 365 cc H20
20%
53%
27% PRO
CHO
FAT
PES Guess???
NCP
Assessment
Diagnosis
Intervention
Monitoring/Evaluation
� PES Statement
Inadequate oral intake (NI-2.1) related to physiological causes increasing nutrient needs due to dx of Ampullary CA as evidenced by 30# wt loss, nausea, emesis, dysguesia, decreased appetite, and NPO status 2° Whipple procedure.

NCP
Assessment
Diagnosis
Intervention
Monitoring/Evaluation
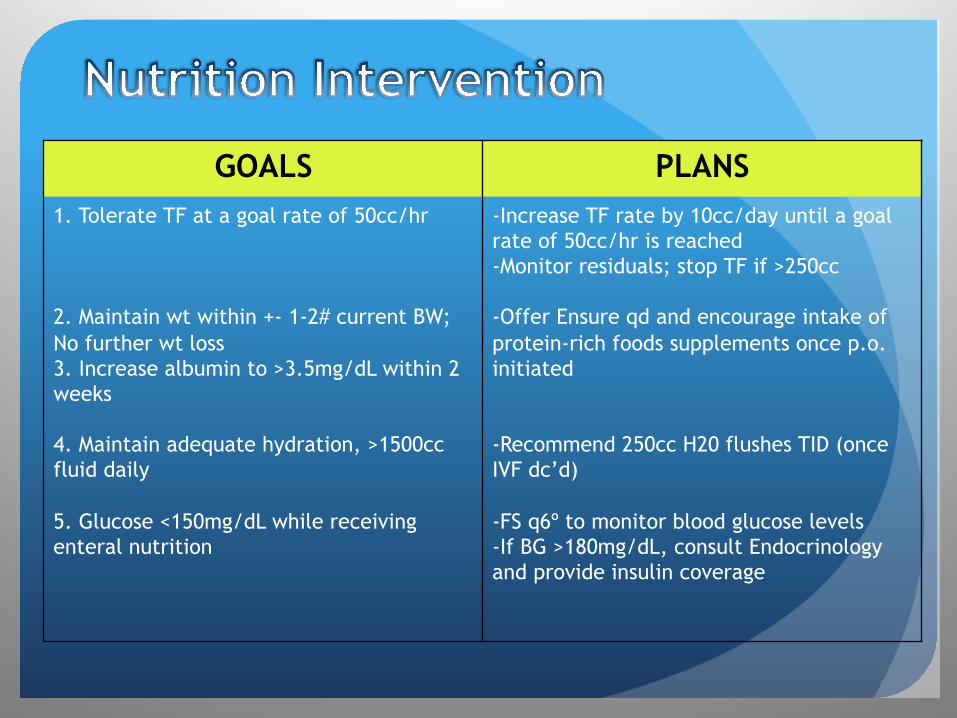
GOALS PLANS 1. Tolerate TF at a goal rate of 50cc/hr 2. Maintain wt within +- 1-2# current BW; No further wt loss 3. Increase albumin to >3.5mg/dL within 2 weeks 4. Maintain adequate hydration, >1500cc fluid daily 5. Glucose <150mg/dL while receiving enteral nutrition
-Increase TF rate by 10cc/day until a goal rate of 50cc/hr is reached -Monitor residuals; stop TF if >250cc -Offer Ensure qd and encourage intake of protein-rich foods supplements once p.o. initiated -Recommend 250cc H20 flushes TID (once IVF dc’d) -FS q6º to monitor blood glucose levels -If BG >180mg/dL, consult Endocrinology and provide insulin coverage