evidence-based prenatal care parts 1 & 2 afp 1 st and 15 th july 2005 oguchi nwosu m.d. asst....
TRANSCRIPT

Evidence-Based Prenatal careEvidence-Based Prenatal careParts 1 & 2Parts 1 & 2
AFP 1AFP 1stst and 15 and 15thth July 2005 July 2005
Oguchi Nwosu M.D.Oguchi Nwosu M.D.
Asst. Prof.Asst. Prof.
Emory Family MedicineEmory Family Medicine
January 10January 10thth 2008 2008
Evidence-Based Prenatal Care: Part 1Evidence-Based Prenatal Care: Part 1General Prenatal care and counselling issuesGeneral Prenatal care and counselling issues
AFP , April 1, 2005AFP , April 1, 2005
Systematic approachSystematic approach
Best evidenceBest evidence
Model of informed, shared decision makingModel of informed, shared decision making
-Reduced visit schedule- No adverse outcomes-Reduced visit schedule- No adverse outcomes
- Decreased patient satisfaction- Decreased patient satisfaction
-Caregiver continuity- Decreased interventions in labor &-Caregiver continuity- Decreased interventions in labor &
improved maternal satisfactionimproved maternal satisfaction
-Care by midwives/FM/OB- Equally effective, more-Care by midwives/FM/OB- Equally effective, more
satisfaction with MW and FMsatisfaction with MW and FM
Prenatal carePrenatal careFirst VisitFirst Visit
Ideally 1Ideally 1stst trimester trimester
Appropriate counseling : Table 1Appropriate counseling : Table 1
- First 12 weeks organogenesis- First 12 weeks organogenesis
Accurate EDDAccurate EDD
Recommendations for routine prenatal Recommendations for routine prenatal care: Table 2care: Table 2
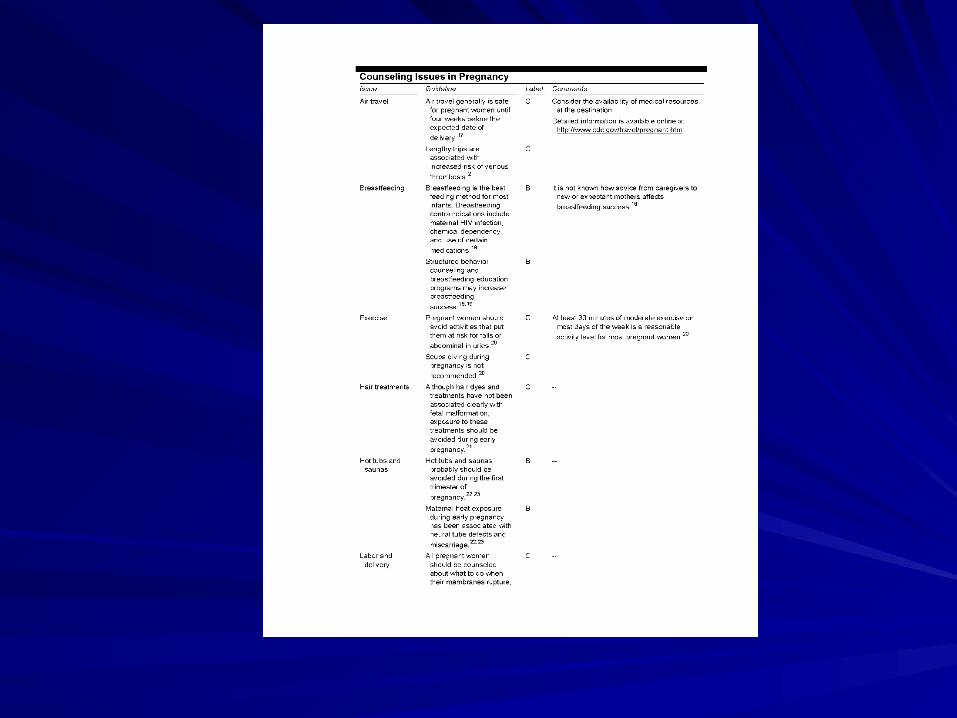
Table 1Table 1

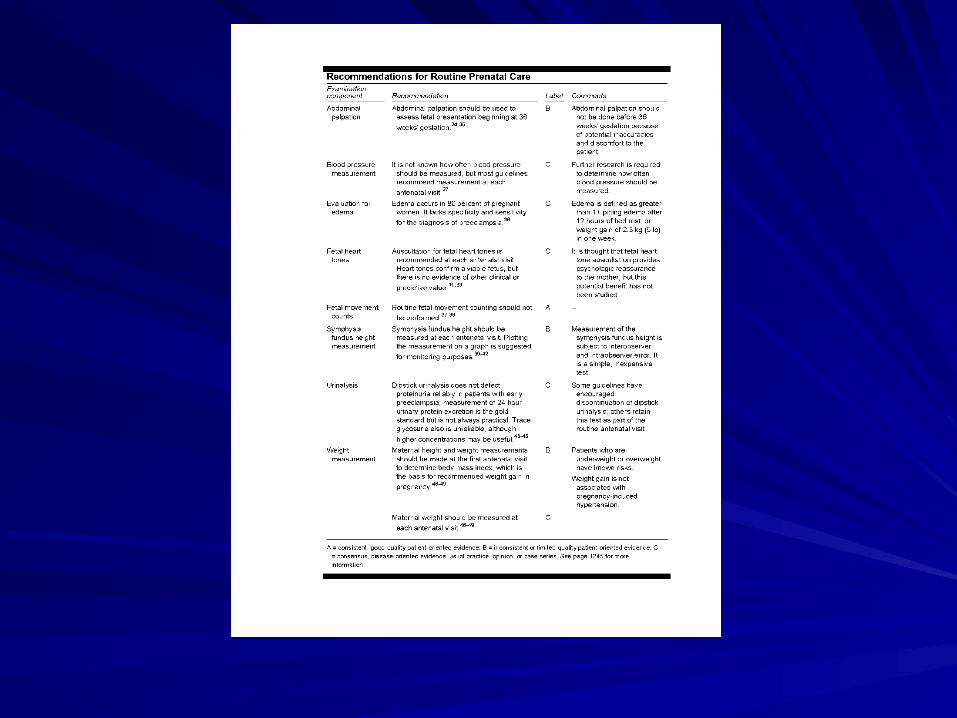
Table 2Table 2

Prenatal carePrenatal careOther issuesOther issues
Prenatal education- especially 1Prenatal education- especially 1stst preg. preg.
Domestic violence screen- 3 questionsDomestic violence screen- 3 questions
Blood typing- Ab screen & rhogam at 28 Blood typing- Ab screen & rhogam at 28 weeks if Rhesus negweeks if Rhesus neg
Other indications for rhogam ?Other indications for rhogam ?

Prenatal carePrenatal careGenetic screeningGenetic screening
Ideally preconceptionIdeally preconception
-FH of genetic disorder-FH of genetic disorder
-Previous fetus/child with GD-Previous fetus/child with GD
-Recurrent miscariages-Recurrent miscariages
-Ethnic grp. disease specific screening (CF, SCA, -Ethnic grp. disease specific screening (CF, SCA, Tay Sachs, ThalTay Sachs, Thal
Offer all women triple screen. 16 to 18 weeks Offer all women triple screen. 16 to 18 weeks (15 t0 20)(15 t0 20)
Women at increased risk offer Amnio/CVSWomen at increased risk offer Amnio/CVS

Prenatal carePrenatal careUltrasoundUltrasound
No evidence directly linked to improved No evidence directly linked to improved fetal outcomesfetal outcomes
Early USS (b/4 14 weeks) accurately Early USS (b/4 14 weeks) accurately determines gest. – when in doubt.determines gest. – when in doubt.
Indications for 1Indications for 1stst trim USS? trim USS?
Offer USS b/w 18 – 20 weeks for fetal Offer USS b/w 18 – 20 weeks for fetal anomaly searchanomaly search

Prenatal carePrenatal careNutrition/Food safetyNutrition/Food safety
25 to 35ib weight gain ideal25 to 35ib weight gain idealFolic @ from 4 weeks preconceptionFolic @ from 4 weeks preconceptionUSPSTF – insufficient evidence for or against fe USPSTF – insufficient evidence for or against fe supplementationsupplementationCaffeineCaffeineDairy productsDairy productsDelicatessen foodsDelicatessen foodsMeatMeatRaw eggsRaw eggsSeafoodSeafood

Evidence-Based prenatal care: Part 1Evidence-Based prenatal care: Part 133rdrd Trim care & prevention of infectious diseases Trim care & prevention of infectious diseases
AFP, April 15, 2005AFP, April 15, 2005
Infectious diseasesInfectious diseases
Gestational diabetesGestational diabetes
Post-term pregnancyPost-term pregnancy
Prenatal carePrenatal careInfectious diseasesInfectious diseases
HIVHIVRecommend to allRecommend to all
Retest high risk in 3Retest high risk in 3rdrd trimestertrimester
Informed consent Informed consent requiredrequired
SYPHILLISSYPHILLISScreen allScreen all
Retest high risk at 28 Retest high risk at 28 weeks & at deliveryweeks & at delivery
Prenatal carePrenatal careInfectious diseasesInfectious diseases
HERPES SIMPLEXHERPES SIMPLEXAsk patients and partners re hx of genital or Ask patients and partners re hx of genital or orolabial HSVorolabial HSVVertical transmission -- 50% prim, 33% non Vertical transmission -- 50% prim, 33% non prim & 0 – 3% recurrentprim & 0 – 3% recurrentAcquired during passage through birth canalAcquired during passage through birth canalHSV +ve partner- Abstinence, ? Condom use, HSV +ve partner- Abstinence, ? Condom use, Antiviral rx for partnerAntiviral rx for partnerRecurrent HSV counsel re acyclovir at term, role Recurrent HSV counsel re acyclovir at term, role of C/S, & avoiding post partum transmissionof C/S, & avoiding post partum transmission
Prenatal carePrenatal careInfectious diseasesInfectious diseases
CHLAMYDIA/GCCHLAMYDIA/GCScreen women < 25 and Screen women < 25 and high riskhigh riskEFM- universal screening EFM- universal screening at 1at 1stst visit visit11stst & 3 & 3rdrd trim trim
High risk groupsHigh risk groups< 25< 25Unmarried womenUnmarried womenBlack womenBlack womenHx of STD’sHx of STD’sNew or multiple sexual New or multiple sexual partnerspartnersCervical ectropionCervical ectropionInconsistent use of barrier Inconsistent use of barrier contraceptioncontraceptionWomen living in comm. Women living in comm. with high infection rateswith high infection rates

Prenatal carePrenatal careInfectious diseasesInfectious diseases
BVBVScreen symptomatic Screen symptomatic womenwomen
Screen women at Screen women at increased risk for increased risk for preterm laborpreterm labor
RUBELLARUBELLAUniversal screeningUniversal screening
Offer vaccination in Offer vaccination in the immediate post the immediate post partum period if non partum period if non immuneimmune

Prenatal carePrenatal careInfectious diseasesInfectious diseases
VARICELLA ZOSTERVARICELLA ZOSTERNone immune preg. None immune preg. Women exposed- VZ Women exposed- VZ immune globulinimmune globulin
None immune- offer post None immune- offer post partum vaccination.partum vaccination.
-Safe while breastfeeding-Safe while breastfeeding
-Delay for 3/12 if rhogam-Delay for 3/12 if rhogam
HEP B & CHEP B & CHbHbssAg at 1Ag at 1stst visit. If + visit. If + post natal interventionpost natal intervention
Women at increased Women at increased risk of acquiring- can risk of acquiring- can vaccinate while preg.vaccinate while preg.
Hep C testing only in Hep C testing only in women with risk women with risk factors factors

Prenatal carePrenatal careInfectious diseasesInfectious diseases
Risk factors for Hepatitis CRisk factors for Hepatitis C1.1. Prison inmatesPrison inmates
2.2. Injection drug usersInjection drug users
3.3. Exposure to blood or blood productsExposure to blood or blood products
4.4. HIV +HIV +
5.5. Elevated AST levelsElevated AST levels
6.6. Multiple sexual partnersMultiple sexual partners
7.7. TattoosTattoos
Prenatal carePrenatal careInfectious diseasesInfectious diseases
UTIUTIUniversal screening by Universal screening by urine culture (12 – 16 urine culture (12 – 16 weeks)weeks)
EFM 1EFM 1stst visit visit
INFLUENZAINFLUENZAOffer all women with med Offer all women with med conditions that increase conditions that increase risk of complications. risk of complications. (Vac.)(Vac.)
Others- offer women who Others- offer women who will be in their 2will be in their 2ndnd or 3 or 3rdrd trim during influenza trim during influenza season.season.
No evidence of risk with No evidence of risk with 11stst trim vaccination trim vaccination

Prenatal carePrenatal careInfectious diseasesInfectious diseases
GBSGBSSignificant cause on neonatal M & MSignificant cause on neonatal M & M
10 to 30 % colonization in women10 to 30 % colonization in women
Risk factors for neonatal infection x 3Risk factors for neonatal infection x 3
Universal screening with vaginorectal culture at Universal screening with vaginorectal culture at 35 to 37 weeks35 to 37 weeks
Women with GBS bacteuria or previous infant Women with GBS bacteuria or previous infant with GBS infection do not need screening – rxwith GBS infection do not need screening – rx
Pen or Clinda in Labor or ROMPen or Clinda in Labor or ROM

Prenatal carePrenatal careGestational diabetesGestational diabetes
2 to 5%2 to 5%
Associated withAssociated with
- Hypertensive disorders- Hypertensive disorders
- Macrosomia- Macrosomia
- Shoulder dystocia- Shoulder dystocia
- Increased C/S rates- Increased C/S rates
- DM later in life - DM later in life

Prenatal carePrenatal careGestational diabetes (Screening)Gestational diabetes (Screening)Controversial- no studies showing improved Controversial- no studies showing improved perinatal outcomesperinatal outcomesACOG/ADA recommends at 24 to 28 weeks ACOG/ADA recommends at 24 to 28 weeks except ‘low risk’except ‘low risk’94% physicians including EFM- universal 94% physicians including EFM- universal screeningscreeningI hour 50g GCT followed if positive by 3 hour I hour 50g GCT followed if positive by 3 hour 100g GTT100g GTTBritish guidelines recommend against screeningBritish guidelines recommend against screeningA randomized trial of 2,400 women ongoing in A randomized trial of 2,400 women ongoing in US should provide some answersUS should provide some answers

Prenatal carePrenatal careGestational diabetes (Low risk)Gestational diabetes (Low risk)
<25<25
Low risk ethnic groupLow risk ethnic group
Normal pre-pregnancy weightNormal pre-pregnancy weight
No hx of abnormal glucose metabolismNo hx of abnormal glucose metabolism
No hx of poor obstetric outcomesNo hx of poor obstetric outcomes
No hx of 1No hx of 1stst degree relatives with DM degree relatives with DM

Prenatal carePrenatal carePost-term pregnancyPost-term pregnancy
Risk of stillbirth- 37 weeks 1/3000 Risk of stillbirth- 37 weeks 1/3000 - 42 weeks 3/3000- 42 weeks 3/3000 - 43 weeks 6/3000- 43 weeks 6/3000
In a meta-analysis, routine induction at 41 weeks In a meta-analysis, routine induction at 41 weeks reduced perinatal death without increase in C/S ratereduced perinatal death without increase in C/S rateMost guidelines recommend routine induction after 41 Most guidelines recommend routine induction after 41 weeksweeksBeyond 42 weeks, assess fetal well being with NST and Beyond 42 weeks, assess fetal well being with NST and AFVAFVSweeping membranes reduces need for labor induction Sweeping membranes reduces need for labor induction