evaluation of the allied health brief therapies (ahbt) clinics
TRANSCRIPT
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 1 of 86
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics Final Report December 2019
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 2 of 86
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics Final Report December 2019
Published by the State of Queensland (Queensland Health), March 2019
This document is licensed under a Creative Commons Attribution 3.0 Australia licence.
To view a copy of this licence, visit creativecommons.org/licenses/by/3.0/au
© State of Queensland (Queensland Health) 2019
You are free to copy, communicate and adapt the work, as long as you attribute the State of Queensland (Queensland Health).
For more information on the evaluation report contact:
Service Evaluation and Research Unit (SERU) Mental Health & Specialised Services West Moreton Health Ph: 07 3271 8647 Email: [email protected] For more information on the Clinics contact the Executive Director, Mental Health at each of the pilot sites: Darling Downs Health: [email protected]
Metro South Health: [email protected]
West Moreton Health: [email protected] Disclaimer:
The content presented in this publication is distributed by the Queensland Government as an information source only. The State of Queensland makes no statements, representations or warranties about the accuracy, completeness or reliability of any information contained in this publication. The State of Queensland disclaims all responsibility and all liability (including without limitation for liability in negligence) for all expenses, losses, damages and costs you might incur as a result of the information being inaccurate or incomplete in any way, and for any reason reliance was placed on such information.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 3 of 86
Evaluation report prepared by: Ms Yolanda Mansfield Service Evaluation & Research Unit (SERU), Mental Health & Specialised Services, West Moreton Health
Dr Tom Meehan Service Evaluation & Research Unit (SERU), Mental Health & Specialised Services, West Moreton Health
Dr Marianne Wyder Research & Learning Network, Addiction & Mental Health Services, Metro South Health
Ms Julie Argus Rehab & Recovery Centre, Divisions of Mental Health & Allied Health, Darling Downs Health
Acknowledgements The evaluation team would like to acknowledge the support of the following people and organisations: AHBT Clinics Research Group Representatives Ms Sarah Hamilton (MSH) Mr Geoff Lau (MSH) Ms Michelle Giles (WMH) Ms Marea Webb (DDH) Ms Bridie James (WMH) Ms Julie Argus (DDH) Ms Coralie Stewart (MSH) Ms Stacey Agar (WMH) Ms Rachel Macready (DDH) Dr Marianne Wyder (MSH) Mr Ossi Beck (MHAODB) Mr Jason Monk (MHAODB)
Management and clinicians within the Darling Downs, Metro South and West Moreton Hospital and Health Services
Aftercare
Financial contributions of:
• Strategic Planning and Partnerships Unit, Mental Health, Alcohol and Other Drugs Branch (MHAODB)
• Allied Health Professions Office for Queensland (AHPOQ), Clinical Excellence Queensland
• Clinical Governance, Mental Health, Alcohol and Other Drugs Branch (MHAODB)
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 4 of 86
Contents Executive Summary 7
Allied Health Brief Therapies Clinics 7 Evaluation 8 Major Findings 8 Conclusions 9 Recommendations 9
1 Introduction 12
1.1 Previous Research 13 1.2 Allied Health Brief Therapies (AHBT) Clinics 16 1.3 Evaluation Aims and Objectives 21
2 Evaluation Framework 22
2.1 Study Design 22 2.2 Study Locations 22 2.3 Data Collection 23
3 AHBT Clinic Implementation Process Findings 28
3.1 AHBT Clinic Model of Service 28 3.2 Consumer Demographics 31 3.3 Clinic Activity 32 3.4 Workforce Development 36 3.5 Staff perceptions of implementation 38 3.6 Summary 43
4 AHBT Clinic Impact Findings 44
4.1 Consumer Clinical Impacts 44 4.2 Consumer Satisfaction Ratings 52 4.3 Staff Perceptions of Clinic Impact 57 4.4 Summary 61
5 AHBT Clinic Outcome Findings 62
5.1 Patient safety 62 5.2 Staff perceptions of Clinic outcomes 65 5.3 Summary 69
6 Discussion 70
6.1 AHBT Clinic Implementation, Feasibility & Scalability 70 6.2 Impact Consumer Presenting Problems & Satisfaction 71 6.3 Impact on Clinicians 73 6.4 Impact on Mental health Services 73
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 5 of 86
6.5 Limitations 74 6.6 Conclusions 74
7 Recommendations 76
7.1 Continue to embed Clinics within existing and emerging service models 76 7.2 Ensure Clinic infrastructure supports efficient and effective service delivery 76 7.3 Expand the workforce providing therapy in the Clinics 76 7.4 Streamline consumer referrals to Clinics 76 7.5 Provide brief ‘aftercare’ interventions 77 7.6 Ensure ongoing training for staff 77 7.7 Conduct more comprehensive evaluation 77
8 References 78
9 Appendices 85
Appendix A: Consumer Measures 85

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 6 of 86
List of Tables
Table 1 Consumer Clinical Measures ............................................................................................................. 25
Table 2 Age Category of Consumers ............................................................................................................. 31
Table 3 Consumer Diagnosis Category ........................................................................................................... 32
Table 4 Compliance with MoS Timeframe for 1st Appointment ...................................................................... 33
Table 5 Consumer Attendance Initial Appointment ....................................................................................... 33
Table 6 Consumer AHBT Clinic Session Attendance........................................................................................34
Table 7 AHBT Clinic Consumer Referral Outcomes ........................................................................................ 35
Table 8 Consumer Discharge Destination ..................................................................................................... 36
Table 9 AHBT Clinic Training Program ............................................................................................................ 37
Table 10 Pre / Post DASS Mean Scores & Severity Level (n54) ...................................................................... 44
Table 11 Pre / Post DASS Mean Scores & Severity Level - Consumers Completed Treatment (n45) ................. 45
Table 12 Pre / Post DASS Mean Scores & Severity - Consumers Disengaged Treatment (n9) .......................... 45
Table 13 Comparison of AHBT Clinic DASS Scores with similar Australian Initiatives........................................ 47
Table 14 Presence of suicidal ideation .......................................................................................................... 48
Table 15 Frequency of Suicidal Ideation ........................................................................................................ 48
Table 16 Intensity of Suicidal Ideation ........................................................................................................... 49
Table 17 Likelihood To Act ............................................................................................................................. 49
Table 18 Confidence to Maintain Safety over Next Week ............................................................................. 49
Table 19 ORS Pre and Post Results ............................................................................................................... 50
Table 20 ORS Reliable Change Index Categories............................................................................................. 51
Table 21 ORS Comparative - disengaged vs completed ................................................................................... 51
Table 22 ORS Comparative – Previous MH contact vs new presentation ....................................................... 52
Table 23 SRS Pre and Post Results ................................................................................................................. 53
Table 24 SRS Comparative - disengaged vs completed .................................................................................. 53
Table 25 SRS Comparative – Previous MH contact vs new presentation ........................................................54
Table 26 Consumer Feedback Survey Results................................................................................................. 55
Table 27 Consumer Contacts with MH Services - 3 months pre and post Clinic Attendance ........................... 62
Table 28 Number of ED presentations 3 months pre and post by Clinic attendance status ............................ 63
Table 29 Number of ED presentations 3 months post Clinic Attendance by number of sessions attended ..... 64
Table 30 Number of ED presentations 3 months pre and post Clinic Attendance by Previous MH Service Contact ........................................................................................................................................................ 64
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 7 of 86
“What works well from my perspective is that it [the Clinic] fills a gap for consumers who need help straight away. And by help I mean therapy, crisis support, rather than just repeated assessment” (Clinic Clinician)
Executive Summary Many people at risk for suicide attend a hospital emergency department (ED) seeking help for their distress. However, most recent reviews highlight the difficulty of meeting the complex needs of those presenting with suicidality within the ‘acute’ care approach of the ED. While consumers can be referred to community-based support services (such as the ‘Better Access’ program), they generally have to wait protracted periods to access such programs and a large proportion fail to make connect with these providers. As a result, many people return to the ED which has been found to exacerbate their distress, frustrate and divert emergency clinicians, paramedics and police, and is an expensive treatment option. It is now clear that more assertive follow-up and therapy are required following discharge from the ED. A recent report by the Australian Centre for Research Excellence in Suicide Prevention (2014) concluded that “failure to provide follow-up care after suicide attempts is associated with increased risk of re-attempt and death by suicide” (p.2). There is an urgent need to develop and evaluate ‘aftercare’ interventions that support people with suicidality following their assessment in the ED.
A key factor in service provision is the presence of a highly skilled mental health workforce with the confidence and capacity to work with those presenting in suicidal crisis (Queensland Health, 2016a; Queensland Health, 2016b; Leggat, 2014). However, recent studies have highlighted concerns around clinical workforce capacity to provide therapeutic interventions and services beyond assessment and referral, particularly for clinicians in allied health disciplines (Queensland Health, 2017a; Queensland Health, 2015). Within the mental health field, opportunities for allied health professionals to work to full practice scope are limited resulting in de-skilling and a lack of confidence in managing complex mental health issues (Philip, 2015).
Allied Health Brief Therapies Clinics During 2018, three Allied Health Brief Therapies (AHBT) Clinics were established on a trial basis in three health services in Queensland; Darling Downs, West Moreton and Metro South. The clinics are located in the community (at Community Health Centres and NGO facilities) to provide an immediate, more accessible and coordinated treatment approach for those presenting to emergency departments with suicidality. Having been assessed in the ED, consumers are referred to the Clinics where allied health mental health staff work collaboratively with them, their families and carers to provide personalised psychotherapeutic support. Most consumers are seen in a Clinic within 3 business days of referral from the Emergency Department. The overall aim of the Clinics is to ensure consumers remain engaged and safe during their time of crisis and support their transition, as required, to a range of community, private and primary care-based service providers.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 8 of 86
Evaluation This report describes the evaluation of the AHBT Clinics that was carried out across the three health services. A broad range of data was collected from staff, consumers and from consumer records /databases to provide detailed information concerning the process, impact and outcomes of establishing the Clinics. In designing the evaluation, we tried to reach a compromise between the burden placed on staff to administer measures and the time taken by consumers to complete the measures (time that could be devoted to therapy). A randomised control trial was considered but this proved to be too disruptive to the establishment of the Clinics.
Major Findings The findings from the evaluation indicate the introduction of AHBT Clinics does not appear to duplicate existing services but complements service provision by addressing an important gap in service provision to those with suicidality. Other key findings include:
• 149 consumers were referred to the 3 clinics over the six-month study period – receiving a median of 2 therapy sessions (range 1 to 6 sessions) with one-fifth attending 4 sessions.
• Just over half (57.7%) had previous contact with a mental health service (86/149) while the current presentation was the first presentation to mental health for 42.3% of those referred to the clinics (63/149).
• Psychological distress in the study group was high. The score for depression on initial presentation to the Clinics places the sample in the ‘extremely severe’ category for depression.
• There was significant improvement in psychological distress for those attending the clinics between initial visit and follow-up as demonstrated by large effects on depression (Cohen’s d = 0.98), anxiety (Cohen’s d = 0.73) and stress (Cohen’s d = 0.78).
• There was a significant improvement between baseline and follow-up in consumer confidence in being able to maintain their safety over the next week (p = 0.004).
• Over three-quarters of consumers (76%) were seen in clinic within 72 hours of initial presentation to the emergency department.
• High levels of consumer satisfaction were found. Over 90% of consumers indicated that they would ‘use the clinic again if they were experiencing similar issues’ while 91% indicated that they would ‘recommend the Clinic to a friend or family member’.
• In the 3 months prior to the Clinic, 143 consumers had 177 presentations to an ED. This is compared to 26 presentations by 18 consumers in the 3 months following referral to the Clinic.
• Clinic staff felt that the introduction of the clinics enabled them (allied health staff) to refine and develop new skills and deliver therapies in keeping with scope of practice.
• Perception of increased capacity among clinic staff in their ability to manage suicidality
• Feedback from staff suggests that provision of timely, accessible, evidence based therapeutic interventions through the AHBT Clinics: validates the consumer as a person, reducing stigma; enables collaborative engagement between consumer and clinician to address the immediate crisis; provides

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 9 of 86
consumers with skills and techniques to better manage similar situations; and instils hope that continued recovery is achievable through ongoing engagement with suitable support services
Conclusions The purpose of the report was to provide the evaluation findings from the piloting of the AHBT Clinics concept across the three implementation sites. It must be acknowledged that the Clinics continue to be supported and operate post pilot within existing service funding and resourcing constraints.
Findings from the evaluation indicate that the introduction of AHBT Clinics does not duplicate existing services but complements service provision by addressing an important gap in current services for those presenting with suicidality. The AHBT Clinic model provides prompt treatment and support for people at the time of their greatest need and ensures safe transition from one service provider to the next.
Delivering the right care to consumers, their families and carers at the initial contact point or crisis also benefits the system through potential reduction in future use of limited system resources (such as ED and mental health services). Our findings point to a significant reduction in ED usage following Clinic intervention. This enables the system greater flexibility and capacity to meet other competing demands.
The AHBT Clinics are positioned to enhance communication, clinical management pathways and service linkages. Within each HHS, the Clinics have been integrated with existing service and clinical governance structures to optimise consumer transition between ED, mental health and alcohol and other drug service components. The position of the clinics within current service provision supports the implementation of the Zero Suicide Framework.
In addition to better meeting consumer needs, the Clinics assist allied health staff to practice to full scope. Working in the clinics has enabled allied health staff to refine current skills, develop new skills and acquire confidence in delivering therapeutic interventions in a clinic environment. It is likely that staff will rotate through the clinics, bringing with them the new skills that they have acquired. As such, the Clinics are likely to act as a training environment for mental health staff, thereby increasing the pool of staff with advanced skills within each service.
In summary, the AHBT Clinic model is based on existing evidence, fulfils an identified gap in current service provision and enables a range of therapeutic approaches based on consumer needs. For consumers (and carers), the provision of early intervention through the Clinics results in higher levels of satisfaction with the mental health system and a perception that consumer concerns are being addressed.
Recommendations 1. Continue to embed the Clinics within current and emerging service models.
Findings from the evaluation indicate that the introduction of AHBT Clinics does not duplicate existing services but complements current service provision by addressing a gap in services for those presenting with suicidality. The AHBT Clinic model provides prompt treatment and support for people at the time of their greatest need and ensures safe transition from one service provider to the next. Moreover, the position of the clinics within current service provision supports the implementation of the Zero Suicide Framework. As such, it is recommended that service managers explore options to further integrate the clinics into existing service models as well as emerging service delivery initiatives. This is likely to require some consideration of the endorsed AHBT Clinic Model of Service (MoS) and localised operational and governance frameworks,
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 10 of 86
how the clinics will be funded as well as physical location and accessibility (for both consumers and clinical staff).
2. Ensure Clinic infrastructure supports efficient and effective service delivery
A key component to the successful implementation of the Clinics is availability of and access to infrastructure that supports therapeutic service delivery. It is recommended that co located Clinics have sufficient access to appropriate physical, human and communication / information system resourcing and infrastructure.
3. Expand the workforce providing therapy in the Clinics
It is recommended that service managers consider recruiting other mental health professionals (in addition to Allied Health) to work in the Clinics such as mental health nurses, psychiatric trainees, etc. In addition to providing a larger pool of staff available to work in the Clinics, clinic exposure is likely to increase staff skill and confidence in providing therapeutic interventions (similar to the experience of allied health staff described in this study).
4. Streamline consumer referrals to the Clinics.
One of the advantages of the Clinic model is access to prompt treatment for those at risk. It is noted that the services in our study have taken different approaches to providing access to the Clinics – some provide direct access from the ED while others refer consumers to the Acute Care Team for review and subsequent referral to the Clinic (based on assessment by ACT). While different approaches arise from local service requirements, it is recommended that services continue to review their procedures so that consumer access to the Clinic is as efficient and prompt as it can be.
5. Provide brief ‘aftercare’ interventions
It is recommended that services consider supplementing the current Clinic sessions with outreach contact after discharge. This can include phone calls, voice messages, text messages, and possibly home visits, etc. It has been noted in previous research that this type of follow-up ‘aftercare’ can decrease suicide risk. Where possible, this follow-up should be carried out by the clinician who treated the consumer in the Clinic.
6. Ensure ongoing training for staff
It was noted in interviews with clinic clinicians that they valued the additional training provided to increase their confidence in working in a clinic environment. In the present project, the AHBT clinicians were supported in this regard through the provision of targeted professional development and training in brief interventions and suicide risk management. A program of ongoing clinical supervision was also provided to assist staff in translating learning into practice. Services will need to consider the level of training and support required by new staff who wish to work in the Clinics.
7. Conduct more comprehensive evaluation
The present evaluation followed a single group pre/post-test design which has a number of known limitations. Given that the Clinics are now established and the process for care delivery refined, a more comprehensive evaluation of the initiative should be considered. While an RCT may be feasible, it would involve denying some consumers access to the Clinics for the sake of the evaluation (i.e. those in the control group). Moreover, a future evaluation should consider the inclusion of an economic evaluation to determine

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 11 of 86
the cost-effectiveness of the Clinic model. This and a range of other issues would need to be considered in developing a more comprehensive evaluation.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 12 of 86
1 Introduction People at risk for suicide are likely to attend a hospital emergency department (ED) seeking help for their distress (Silk, 2016; Morphet, Innes, Munro, O’Brien, Gaskin, Reed & Kudinoff, 2012). However, treatment of those at risk of suicide in EDs presents a significant challenge in providing timely and appropriate health care. Presentations for suicidality can be complex due to a combination of co-morbidities such as adverse life events, substance misuse and a range of social factors (Leske, Crompton & Kolves, 2019; Morphet et al, 2012; Hert, Correll, Bobes, Cohen, Asai, & Leucht, 2011;). While health staff who work in EDs and with mental health services are committed to providing a high level of care, they work within a system where staff are expected to do more in the face of increasing demand and dwindling resources (Black Dog Institute, 2015)
People presenting with suicidality are assessed in the ED and provided with some brief interventions and usually referred to another arm of the mental health service. However, there tends to be lack of service coordination and integration within the health care system and consumers must ‘navigate a fragmented service system’ to obtain the services they need (National Mental Health Commission, 2018). A recent Australian review found that patients attending ED for suicidality reported that their “emotional distress was not attended to: many believed that they had been discharged too rapidly and were left to seek their own options for ongoing care” (Jelinek, Weiland, Gerdtz & Hill, 2013; p.2).
The mental health system is ‘risk averse’ and people presenting to emergency departments with suicidality are frequently subjected to excessive review and assessment with limited therapeutic intervention (Black Dog Institute, 2015; Queensland Mental Health Commission, 2018). There is a major focus on clinical diagnosis which often results in other ‘non-clinical’ factors being overlooked including the importance of carers and providers of social support services (Productivity Commission, 2019). In the absence of alternate service options, consumers make multiple presentations to the emergency department in search of appropriate treatment for their distress (Casey, 2015; Meehan, Mansfield, Neillie & O’Gorman, 2016; Bugeja, Milner & Pirkis, 2015). Over the past 15 years, the rate of mental health presentations at emergency departments in Australia has increased by around 70% (AIHW 2019).
A key factor in service provision is the presence of a highly skilled mental health workforce with the confidence and capacity to work with those presenting in suicidal crisis (Queensland Health, 2017b; Leggat, 2014). However, recent studies have highlighted concerns around clinical workforce capacity to provide therapeutic interventions and services beyond assessment and referral, particularly for clinicians in allied health disciplines (Queensland Health, 2017a; Queensland Health, 2016a). Within the mental health field, opportunities for allied health professionals to work to full practice scope are limited resulting in de-skilling and a lack of confidence in managing complex mental health issues (Philip, 2015).
A recent review of mental health care in Australia by the Productivity Commission (2019) highlighted the lack of appropriate aftercare for those presenting to emergency departments with suicidality. It was noted that adequate aftercare following a suicide attempt could reduce emergency department presentations by up to 20% and deaths by 1%. This is equivalent to preventing 34 people per year from dying by suicide and around 6000 people per year from attempting suicide. The Commission recommended that “a program to provide access to timely, effective aftercare for every person who presents to a hospital, GP or other service following a suicide attempt or in suicide distress should be provided as soon as possible” (p.15).

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 13 of 86
Given the limitations around the treatment of those with suicidality in emergency departments and the lack of appropriate aftercare, there is a need to develop and evaluate options that are brief, focused, and capable of providing personalised support immediately following discharge from the ED.
1.1 Previous Research
1.1.1 Suicidality Suicide rates in Australia have continued to rise in recent years despite significant investment in suicide prevention. In 2017, there were 3128 deaths attributed to suicide, an increase of 9.1% on the previous year(Leske et al. 2019). Suicide is now the leading cause of death for Australians aged 15–44 years. While suicide rates in Queensland decreased in the 2018 year, Queensland continues to have the second highest rate of suicide in Australia (Queensland Mental Health Commission, 2019). However, reducing suicide is complex as suicidality is underpinned by a dynamic interaction of biological, psychological, social, cultural, and spiritual factors. This complexity is evident in the recent report on Suicide in Queensland (Leske et al. 2019). The authors noted that of the 2085 deaths by suicide in Queensland between 2013 -15, the most frequent adverse events prior to suicide included relationship separation (27.7% of all deaths by suicide); financial problems (17.3%); relationship conflict (16.0%); risk of unemployment (12.5%); pending legal matters (11.1%); and family conflict (10.5%). It was also noted that almost half (49.2%) had no known mental health condition while a further 32.2% had an untreated mental health condition. For every death by suicide, as many as 30 people attempt suicide and many of these are hospitalised due to intentional self-harm. However, up to 25% of people who attempt suicide will re-attempt it, with the risk being significantly higher in the first week following discharge from hospital after an attempt.
There have been several recent reviews of interventions that are likely to be effective in managing suicidality (Gysin-Maillart, Schwab, Soravia, Megert & Michel, 2016; Beautrais, 2014; Fleischmann et al, 2008; Brown et al, 2005). Individual one-to-one therapy using cognitive behavioural approaches has been widely evaluated and has demonstrated positive outcomes. In their study with 152 active-duty soldiers, Rudd and colleagues (2015) found that a brief cognitive-behavioural therapy with 12 to 16 sessions plus usual mental health care (from case managers) was associated with a 60% lower risk of attempting suicide in the 24 months following treatment.
One-to-one therapy with the addition of ‘brief’ follow up contact (letters, text messages, and phone calls, etc) has also been evaluated. In Ireland, Surgoner and colleagues (2015) provided up to 13 therapy sessions and follow up contact after the therapy had ended. Participants in the program received a text message two weeks after therapy to serve as a brief reminder that the service was available if required. Four weeks after therapy they received a letter and information about local support services that they may find useful in dealing with more specific stressors (e.g., relationship or financial issues). The final contact was six weeks after therapy concluded and was in the form of a telephone call to check on the consumer’s progress and suicidal ideation. This contact asked about current depression, hopelessness and suicidal ideation. The findings pointed to a significant improvement in depression, suicidal ideation and self-esteem at follow-up.
More recently, Gysin-Maillart and colleagues (2016) carried out an evaluation of the Attempted Suicide Short Intervention Program (ASSIP) using a randomised controlled trail. ASSIP is a manualised brief therapy
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 14 of 86
program (3 sessions) with brief follow-up comprising standardised letters sent to participants every 3 months in the first year and every 6 months in the second year. The study found no significant differences between ASSIP and control participants on the number of inpatient admissions and use of other services (e.g. ED) at 12 months follow-up. However, over the entire study period (24 months), only 5 ASSIP patients attempted suicide while 41 TAU patients attempted suicide.
Interestingly, brief contact, on its own, after attempted suicide, such as contacting patients with regular postcards or letters, has been found to reduce the risk of suicide (Carter, Clover, Whyte, Dawson, & D’Este, 2013; Motto & Bostrom, 2001). However, findings have not been consistent with some studies finding no effect (Kapur, Gunnell, Hawton, Nadeem, Khalil, Longson & Cooper, 2013; Beautrais, Gibb, Faulkner, Fergusson, Mulder, 2010). It is possible that this contact needs to be more extensive to have a clinical impact. Fleischmann and colleagues (2008) offered 1,867 individuals who had attempted suicide a brief psychoeducation session and more long-term contact with phone calls or visits over a period of 18 months. The intervention group had significantly fewer deaths from suicide than the group with usual treatment.
A small number of Australian initiatives are worthy of mention since the consumers in these studies are similar to the target group in the present evaluation. The first of these commenced in July 2008 with the aim of assisting GPs to improve the treatment of people presenting with suicide risk. Under the initiative (known as ATAPS-SP), Divisions of General Practice were funded (through the Commonwealth Government) to provide specialist services to consumers at risk of suicide. This enabled GPs to refer ‘at risk’ consumers to mental health professionals (mostly psychologists following additional training) for an unlimited number of sessions of the initial two months (average sessions provided = 5.2). Of the initial 2312 consumers referred to the program, 2070 attended at last one session. Of these 271 were referred directly from emergency departments. An evaluation of the initiative showed that consumers had “significant improvement in outcomes (including a reduction in suicidality) over the course of their care” (King, Bassilios, Reifels, Fletcher, Ftanou, Blashki, Burgess & Pirkis, 2013).
In Queensland, Meehan and colleagues (2015) evaluated the Mental Health Nurse Incentive Program (MHNIP). The Program was established to provide a non-MBS incentive payment to general practices, private psychiatrists and other appropriate community providers (including general practice networks) to engage or retain mental health nurses to assist in the provision of coordinated clinical care for people with severe mental health disorders. Patient contact with the programme ranged from 3 weeks to 38 weeks, and the study group demonstrated significant improvement on all the self-report and clinician-rated measures employed. Effect sizes ranged from 0.59 to 0.74. The findings suggest that the MHNIP had a medium-to-large impact on the mental health and general functioning of individuals supported through the programme.
A more recent initiative in Melbourne describes the establishment of a brief therapy ‘psychology’ clinic, co-located with General Practitioners (GPs) and in partnership with the public mental health services (Casey, 2015). Potential consumers are assessed in the Emergency Department or other arms of the mental health service and referred to the Agile Psychological Medicine Clinic. An evaluation of the initiative identified positive outcomes for 222 consumers referred to the Clinic over a 12-month period (Feb. 2014 to Jan. 2015). Complete data sets were available for 59 of these consumers and show that assessments significantly improved on a range of standardised clinical measures following intervention at the clinic. Consumer satisfaction was also high with an average satisfaction score of 97.5% (out of a possible 100%). System activity data were also collected and showed there were substantially less clinicians involved in each consumer’s care following the implementation of the Clinic. The study concluded that:

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 15 of 86
“The clinic’s systems activity data combined with the improvements in clinical outcomes challenges the ‘triage and handover’ approach that often dominates acute mental health service delivery. The data emerging from the Clinic is very promising and indicates that the Agile Psychological Medicine Clinic assists many consumers to achieve good clinical outcomes as well as providing a more satisfactory consumer interaction with public
adult mental health services” (p28).
Despite the benefits of psychological support for those at risk of suicide, a large proportion of those referred to support services do not attend their initial appointment. In an Irish study by Surgenor and colleagues (2016) found that up to half of the referred clients failed to present at therapy despite having made an appointment to do so. Clients who remained in therapy beyond the second session were more likely to be in contact with a health care provider, have family support and know someone who had died by suicide (Surgenor, Meehan, & Moore, 2016). Other studies suggest that anywhere from 30% to 60% of all clients drop out of treatment following initial engagement (Swift & Greenberg, 2012; Garfield, 1994).
In summary, a review of the literature demonstrates that access to high quality crisis and follow-up aftercare is protective against further suicidal behaviour. Evidence-based options for the provision of aftercare have been isolated by the Black Dog Institute (2015) and include: (i) Brief contact interventions such as phone calls, voice messages, text messages, (ii) Coordinated assertive aftercare with assertive follow up with solution focused counselling following ED presentation (iii) Brief therapy combined with brief contact interventions, and (iv) and Intensive longer-term follow up. While positive results have emerged from intensive follow up (up to 20 therapy sessions) in conjunction with ongoing contact (phone calls, texts, etc), there is less information available on the effectiveness of ‘brief’ interventions comprising 3 – 5 sessions.
1.1.2 Allied Health Mental Health Workforce and Practice Scope The National Practice Standards for the Mental Health Workforce (2013) clearly articulate the practice standards relevant to the five main disciplines working in mental health settings, which include the allied health disciplines of occupational therapy, psychology and social work. The standards make explicit the shared knowledge, skills and capabilities that mental health professionals hold that complement discipline specific practice standards and competencies of each professional group. However, the rise of ‘generic’ mental health clinician positions within public mental health services and a culture focused on the assessment and management of risk has resulted in allied health mental health clinicians suffering a loss of ‘professional identity’ (Porter & Wilton, 2018; Nancarrow, 2015; Philip, 2015).
The 2016 the State-wide Mental Health Allied Health Scope of Practice Project was undertaken to identify the current scope of practice of allied health professionals working in Adult Community Mental Health Services (Queensland Health 2017a). This study along with the findings from the Community Mental Health Services Time and Motion Study (Queensland Health, 2015) concluded that allied health mental health services hold a strong focus on generic tasks with the constraints of care coordination functions limiting the use of therapeutic interventions. CIMHA activity data of teams who participated in the State-wide Mental Health Allied Health Scope of Practice Project support these claims with Provision of Service data showing only 11.5% of the recorded activity assigned to the delivery of interventions while care coordination and assessment were assigned 55.5% and 21.2% respectively. The focus on care coordination and assessment has resulted in a de-skilled and underutilised workforce with poor use of allied health expertise and resources.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 16 of 86
Opportunities for the allied health mental health workforce to work to full practice scope have been identified as key priorities within a number of recent Queensland Health strategic documents, including Connecting Care to Recovery – 2016 – 2021 (Queensland health, 2016a); Allied Health Expanded Scope Strategy 2016 – 2021 (Queensland Health, 2016c) and the Mental Health Alcohol and Other Drugs Workforce Development Framework 2016-2021 (Queensland Health, 2017b). Central to this is the development and implementation of service models of care which ‘optimise the expertise and scope of practice of mental health, alcohol and other drug workforce and increase therapeutic, psychosocial and rehabilitative outcomes for individuals’ (Queensland Health, 2016a).
A number of studies have provided evidence to support models of service involving allied health clinicians in a range of settings and sectors. These include allied health primary contact outpatient models of care (Stute, Moreetto, Raymer, Banks, Buttrum, Sam, Bhagwat & Comans, 2018; Philip, 2015), within emergency departments (Barrett, 2019; Kinsella, Collins, Shaw, Sayer, Cary, Walby & Cowan, 2017) as well as within general practice (McDonald, Ward, Lane, Kearns, Powell Davies, Fuller, Dennis, Spooner & Russell, 2017). The State-wide Mental Health Allied Health Scope of Practice Project Report (2017) also recommended trialling alternate service delivery models, including co-located models, which support allied health clinicians to deliver therapeutic interventions in partnership with Non-Government Organisations and the private sector.
The mental health allied health workforce requires both confidence and capacity to operate successfully within these new models of service. To achieve this, clinicians must be supported via a range of measures including targeted professional development and training (Jackson, Purdy, & Cooper Thomas, 2018; Nancarrow, 2015), individual clinical and peer group supervision opportunities (Snowdon, Millard & Taylor, 2015; Saxby, Wilson & Newcombe, 2015) and the opportunity to translate these skills and knowledge into their clinical practice (Mallidou, Atherton, Chan, Frisch, Glegg & Scarrow, 2018).
With all these elements in place, there is opportunity to develop a service model that optimises the expertise and scope of practice of the allied health mental health workforce that improves linkages with the primary health sector and ultimately therapeutic outcomes.
1.2 Allied Health Brief Therapies (AHBT) Clinics Towards the end of 2018, AHBT clinics were established on a trial basis in three health services in Queensland (Darling Downs, West Moreton and Metro South) – one clinic in each health service. These clinics are co-located in the community and operate in collaboration with existing Queensland Health, NGO and primary health services to support improved care integration across services. The intended outcomes of establishing AHBT Clinics included:
• development of clear referral pathways for people at risk of suicide;
• improved delivery of evidenced-based, brief interventions to people at risk of suicide presenting to Queensland Health Emergency Departments and Hospitals at a time of distress or crisis;
• enhanced clinical management pathways for those at risk of suicide;
• enhanced service partnerships between public mental health services and primary health; and
• provision of a workforce model that allows allied health staff to practice at their full scope

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 17 of 86
Key considerations to developing the AHBT Clinic service model included:
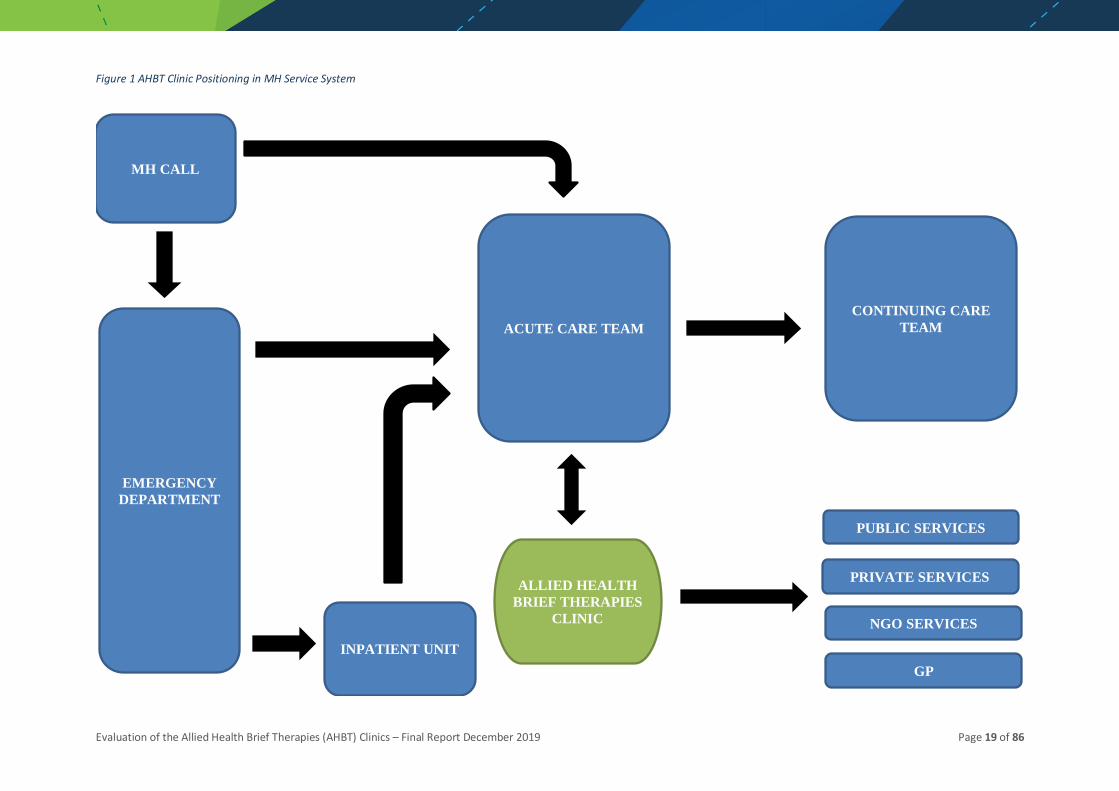
• provision of an ‘add on’ model of service that could be incorporated into and complement existing mental health clinical governance and service delivery systems targeting suicidality (e.g. Zero Suicide initiatives and mental health co responder programs with Queensland police and ambulance services), avoiding duplication (refer Figure 1)
• service provision that was achievable within existing HHS staffing and resources to ensure ongoing sustainability past the pilot
• collaboration with community-based co-location partners to strengthen and embed linkages between clinicians and the sectors that would support consumer, carer and family continuity of care
The operation of the clinic at each site is directed by the model of service (MoS). Eligibility criteria to access AHBT Clinic services included:
• aged over 18 years
• reside in the local catchment area for the Acute Care Team
• presented to the Emergency Department with identified risk factors for suicidality
• willing to engage in a short-term therapeutic intervention
• have the capacity to engage in a short-term therapeutic intervention
• willing and / or motivated to attend sessions at the clinic
• clinical advice supports the referral (e.g. ACT Consultant, ACT Team review)
• clinic attendance will not interfere with other current treatment / management providers
Consumers were deemed ineligible for the Clinic management pathway if they:
• had symptoms severe enough to meet requirements for inpatient admission
• were currently under Mental Health Act
• did not reside in local ACT catchment area
• were not willing to engage in a short-term therapeutic intervention
• did not have the capacity to engage in short term therapeutic intervention
• had other risk factors such that attendance at a clinic is likely to place staff at risk (e.g. violence, current drug use, etc)
In line with best practice evidence, consumers attended between 1 to 6 brief therapy sessions (usually weekly, unless more intense support was required) with the option to also access single session family interventions if agreed to by consumer and family members. Access to a 24-hour support line (MHCALL) and monitoring by the Acute Care Team (ACT) was available if initial appointment not within the 3-business day timeframe or the consumer was identified as being at elevated risk.
The therapeutic interventions offered via the AHBT Clinics seek to address the current crisis and accompanying levels of suicidality and distress. The initial session follows a ‘listen, understand, validate’ approach where the clinician and consumer work together to explore protective factors and solutions for the

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 18 of 86
current issue (Echterling, Presbury & McKee, 2005). Clinic clinicians are encouraged to work with each consumer to determine the therapeutic approach that is likely to be most effective for that individual.
A diagram of the AHBT Clinic consumer management pathway is provided in Figure 2.
Clinic staff did receive significant training in Solution Focused Brief Therapy (SFBT) and most rely on SFBT to structure their therapy sessions. SFBT provides a flexible framework to enable the delivery of brief therapeutic interventions. Its ‘strengths’ and solutions-based approach shifts the focus away from pathology and illness onto skills that promote resilience and independence (Wand, Acret & D’Abrew, 2017). There is strong evidence for the effectiveness of SFBT for a wide variety of behavioural and psychological conditions including suicidality (Hendon, 2008).
SFBT is supported by several principles, all of which are underpinned by the premise that the solution to the consumer’s problems is within the consumers capability and each consumer has the capacity to achieve their desired goals or changes (Ferraz & Wellman, 2009; Wand, 2010). SFBT has the can be delivered in a flexible mode and is not constrained by the traditional therapist role or setting (Ferraz & Wellman, 2009).
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics – Final Report December 2019 Page 19 of 86
Figure 1 AHBT Clinic Positioning in MH Service System
MH CALL
EMERGENCY DEPARTMENT
INPATIENT UNIT
ACUTE CARE TEAM
ALLIED HEALTH BRIEF THERAPIES
CLINIC
CONTINUING CARE TEAM
PUBLIC SERVICES
PRIVATE SERVICES
NGO SERVICES
GP

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 20 of 86
Figure 2 AHBT Clinic Consumer Pathway
Consumer presents to Emergency Department
Does consumer meet eligibility criteria for referral to AHBTC?
YES
NO Follow usual ED protocols
Does consumer accept referral to AHBTC?
YES
NO Follow usual ED protocols
Refer consumer to AHBTC
Does AHBTC accept referral
YES
Does consumer attend AHBTC appointment(s)?
NO Follow usual Acute Care Team protocols
AHBTC clinician attempts follow up of consumer
YES
AHBTC intervention completed. Consumer offered appropriate referrals and
service episode closes
Follow up contact of consumer successful?
YES
NO
Consumer lost to service and service episode closed
NO

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 21 of 86
1.3 Evaluation Aims and Objectives The aim of this study was to evaluate the introduction and effectiveness of the three clinics in terms of process, impact and outcome from the perspective of the consumers and service providers involved. The specific objectives of the evaluation included:
1. Examine the implementation of the AHBT Clinic Model of Service (MoS) at each of the three sites to determine feasibility of implementation, adherence to the MoS and scalability.
2. Examine the impact of the clinics on consumer presenting problems and satisfaction levels
3. Examine the impact on clinicians involved in the clinics in relation to:
• providing referrals to the clinic
• providing interventions within the clinic
• receipt of referrals from the clinic post intervention
4. Examine the impact of the clinic on mental health services at each of the three sites
5. Examine the outcomes for consumers post-clinic intervention in terms of contact with and use of mental health services
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 22 of 86
2 Evaluation Framework
2.1 Study Design The evaluation employed a multi-site repeated measures, mixed methods approach using standardised clinical measures, service data, clinical / patient data, consumer surveys and semi-structured interviews with mental health clinicians and managers and NGO staff. The evaluation focused on three key elements of program implementation as described by Owen & Rogers (1999): process, impact and outcome.
• ‘Process’ evaluation aims to assess how well the Clinics have been established at each site, given consideration to the Model of Service (MoS) developed to guide implementation. In addition, process evaluation considers the robustness of planning and governance processes.
• ‘Impact’ evaluation considers the effectiveness of identified interventions provided through the Clinics - the ability of the interventions to change psychological wellbeing and suicidal thoughts.
• ‘Outcome’ evaluation assesses the ability of the Clinic interventions to keep people safe and assist them to better manage their distress. As such, consumers will be followed for 3 months post-clinic intervention to assess suicide attempts and suicide crisis, visits to ED, inpatient admissions including any unintended consequences of establishing the clinics.
2.2 Study Locations As outlined, one AHBT clinic was established on a trial basis in each of the three health services. During the trial these clinics were located at:
• Wynnum-Manly Community Health Centre, Gundu Pa (Metro South Health)
• Floresco Centre (Aftercare) – Ipswich (West Moreton Health)
• Floresco Centre (Aftercare) – Toowoomba (Darling Downs Health)
The Wynnum-Manly Community Health Centre, Gundu Pa, is a health hub located in Wynnum West to provide a range of primary health services including: 24-hour Primary Care Centre, Breast Screen Queensland, Oral Health (Dental Clinic), Specialist Outpatient Clinics, Addiction and Mental Health, Allied Health, Child Development Services and Chronic Disease Services. The name Gundu Pa is a combination of two words in the local Jandai language meaning ‘medicine stones place’ and was suggested by Winnam Aboriginal and Torres Strait Islander Corporation.
‘Floresco’ is a ‘one-stop’ mental health service provided by the NGO, ‘Aftercare’, for adults in both Ipswich and Toowoomba. The Floresco ‘hub’ provides non-clinical, community-based mental health services through: personalised support, mutual support and self-help, group support activities, and family and carer support. In addition, the hub is designed to simplify access to a range of other services for people with mental illness and their families and carers -for example, general practitioners, psychology, and mental health social work services. Floresco’s integrated service model aims to overcome many of the challenges caused by the fragmentation of mental health services.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 23 of 86
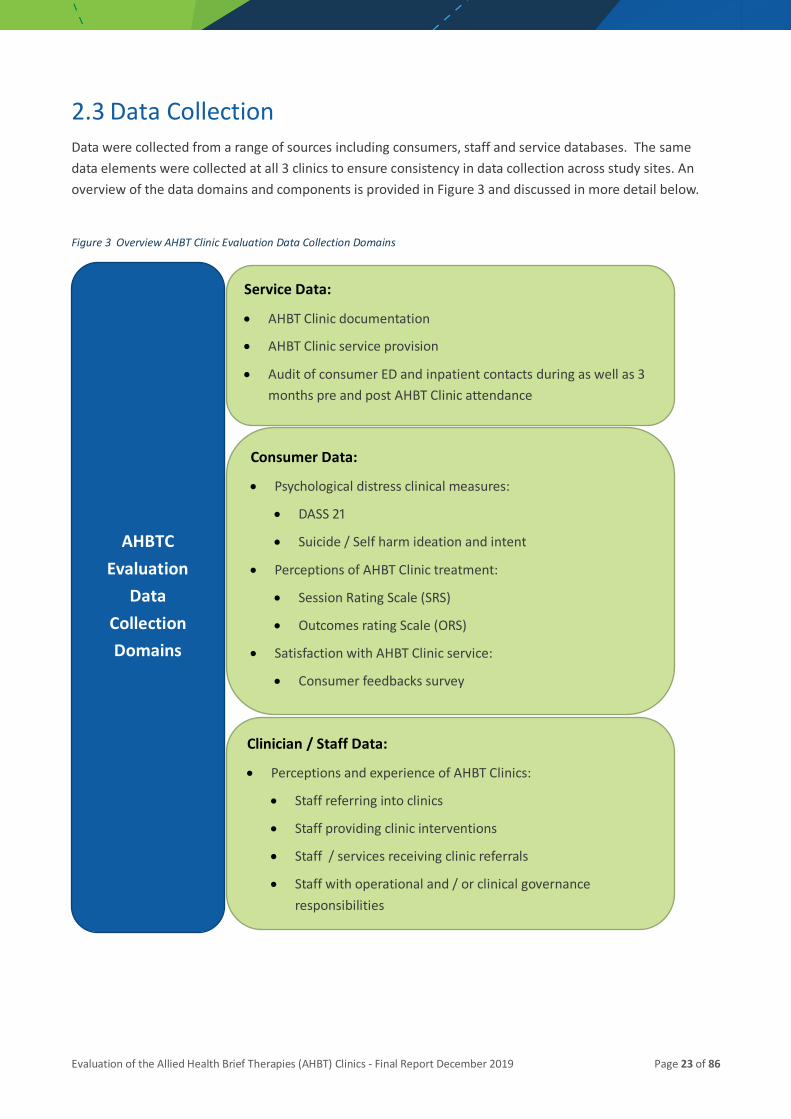
2.3 Data Collection Data were collected from a range of sources including consumers, staff and service databases. The same data elements were collected at all 3 clinics to ensure consistency in data collection across study sites. An overview of the data domains and components is provided in Figure 3 and discussed in more detail below.
Figure 3 Overview AHBT Clinic Evaluation Data Collection Domains
AHBTC Evaluation
Data Collection Domains
Service Data:
• AHBT Clinic documentation
• AHBT Clinic service provision
• Audit of consumer ED and inpatient contacts during as well as 3 months pre and post AHBT Clinic attendance
Consumer Data:
• Psychological distress clinical measures:
• DASS 21
• Suicide / Self harm ideation and intent
• Perceptions of AHBT Clinic treatment:
• Session Rating Scale (SRS)
• Outcomes rating Scale (ORS)
• Satisfaction with AHBT Clinic service:
• Consumer feedbacks survey
Clinician / Staff Data:
• Perceptions and experience of AHBT Clinics:
• Staff referring into clinics
• Staff providing clinic interventions
• Staff / services receiving clinic referrals
• Staff with operational and / or clinical governance responsibilities

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 24 of 86
2.3.1 Service Data AHBT Clinic Documentation
As desktop review of documentation relating to the establishment and implementation of the Clinics at each pilot site was undertaken. Key identified documents included:
• Endorsed AHBT Clinic Model of Service (MoS) document
• Site specific operational and clinical guidelines, protocols, templates and other supporting documentation
AHBT Clinic Service Provision
Monthly service provision data was collected at each site to assess the establishment and implementation of the AHBT Clinic Model of Service for the pilot period. Key data areas included:
• Clinic staffing and availability (e.g. number of clinicians working in the clinic0
• Clinic capacity (number of consumers, number of sessions available)
• Referrals made, accepted and declined
• Compliance with 72-hour (3 business day) timeframe for first session appointment
• Services provided (number of sessions completed, types of interventions, number of consumers seen for all sessions)
• Drop outs (consumers lost to follow up)
Consumer ED and Mental Health Service Contacts
An audit of Consumer Integrated Mental Health Application (CIMHA) data was undertaken to determine the extent of consumer contact with mental health services in the 3 months pre and post their referral to the AHBT Clinic. Identified key contact points included:
• Emergency Department (ED) presentations
• Inpatient Admissions
• Mental Health Co – Responder (where applicable)
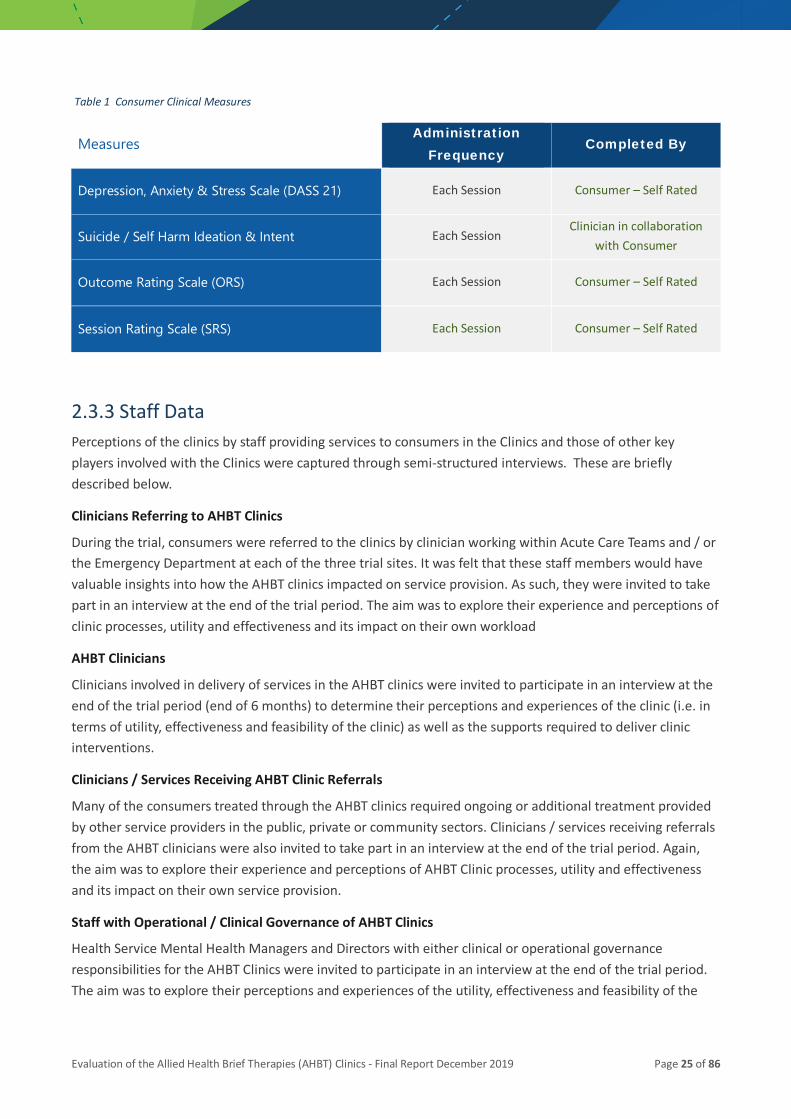
2.3.2 Consumer Data Consumers presenting to each clinic were required to complete several brief clinical measures as part of routine service provision at the AHBT Clinics. These measures focused on psychological wellbeing, suicidal ideation and intent and ratings of each session and perceived outcomes (see Table below). An additional measure, focusing on consumer satisfaction with and perceptions of the services provided at AHBT Clinics was also completed at the end of treatment. A more detailed description of each measure is provided in Appendix A.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 25 of 86
Table 1 Consumer Clinical Measures
Measures Administration
Frequency Completed By
Depression, Anxiety & Stress Scale (DASS 21) Each Session Consumer – Self Rated
Suicide / Self Harm Ideation & Intent Each Session Clinician in collaboration
with Consumer
Outcome Rating Scale (ORS) Each Session Consumer – Self Rated
Session Rating Scale (SRS) Each Session Consumer – Self Rated
2.3.3 Staff Data Perceptions of the clinics by staff providing services to consumers in the Clinics and those of other key players involved with the Clinics were captured through semi-structured interviews. These are briefly described below.
Clinicians Referring to AHBT Clinics
During the trial, consumers were referred to the clinics by clinician working within Acute Care Teams and / or the Emergency Department at each of the three trial sites. It was felt that these staff members would have valuable insights into how the AHBT clinics impacted on service provision. As such, they were invited to take part in an interview at the end of the trial period. The aim was to explore their experience and perceptions of clinic processes, utility and effectiveness and its impact on their own workload
AHBT Clinicians
Clinicians involved in delivery of services in the AHBT clinics were invited to participate in an interview at the end of the trial period (end of 6 months) to determine their perceptions and experiences of the clinic (i.e. in terms of utility, effectiveness and feasibility of the clinic) as well as the supports required to deliver clinic interventions.
Clinicians / Services Receiving AHBT Clinic Referrals
Many of the consumers treated through the AHBT clinics required ongoing or additional treatment provided by other service providers in the public, private or community sectors. Clinicians / services receiving referrals from the AHBT clinicians were also invited to take part in an interview at the end of the trial period. Again, the aim was to explore their experience and perceptions of AHBT Clinic processes, utility and effectiveness and its impact on their own service provision.
Staff with Operational / Clinical Governance of AHBT Clinics
Health Service Mental Health Managers and Directors with either clinical or operational governance responsibilities for the AHBT Clinics were invited to participate in an interview at the end of the trial period. The aim was to explore their perceptions and experiences of the utility, effectiveness and feasibility of the
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 26 of 86
clinic, ongoing supports and resourcing requirements and opportunities for future scalability within and outside of their respective HHS.
2.3.4 Data Management and Analysis Individual clinic sites were responsible for the collection and collation of site-specific data. An Evaluation Co-Investigator was nominated from the staff at each site to work with the AHBT Clinic Co-ordinator and the Evaluation Coordinator to manage the transfer of de-identified data to the Evaluation Team.
Service Data
De-identified consumer service contact data was obtained from CIMHA by staff at each site and entered on a spreadsheet for comparison of mental health service contact for the 3 months pre- and post-attendance at each AHBT Clinic. Descriptive statistics (means, medians, standard deviations, etc) were used to summarise the data while chi-square and t-tests analyses were employed to assess difference in service contacts pre, during and post AHBT Clinic attendance.
Scale Data
The quantitative data derived from the standardised measures completed by consumers (DASS, ORS, SRS, suicidal intent, etc) was provided to the evaluation team in de-identified format. Individual data was combined with that of others to yield sub-scale and total scale scores. Descriptive statistics (means, standard deviations, etc) were used to summarise the data for each time point. Repeated measures analyses of variance (ANOVA) was then employed to explore change on the different scales over the study period. Given that a large number of tests were performed, Bonferroni correction of the alpha level was carried out to adjust for risk of Type I error (ie. declaring a difference when one does not exist). In addition to statistical significance, ‘clinical’ significance was assessed using effect sizes (i.e. Cohen’s d and Hedges g).
Interview Data
Qualitative (interview) data was collected from clinicians working in or providing consumer referrals to the clinics. Clinicians and services receiving referrals were also interviewed as well as management staff with oversight responsibilities for the clinics. While most of these interviews were conducted in person, a small number were conducted via telephone. The topics for discussion were driven by a list of questions set out in a semi-structured interview schedule. The questions focused on clinician and management experiences and perceptions of:
• Training and clinical support provided
• Referral processes and client suitability
• Interventions / services within the clinic
• Referral to other providers
• Staff satisfaction and perceptions of ability to work to their full practice scope
• Possible improvements to clinic services / structures
• Effectiveness and future sustainability / scalability
Interviews were conducted by a co-investigator (not directly associated with the establishment of the Clinics) and digitally recorded with the permission of the participant. Interview recordings were then transcribed verbatim for analysis and checked for errors against the recorded version to ensure an accurate and
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 27 of 86
authentic reproduction. Content analysis (Berg, 2009) was employed to guide analysis of the data contained in each transcript. The transcripts were reviewed several times to generate units of information that refer to common themes. The findings were then discussed with other members of the study team to reach agreement on the final set of themes.
These semi-structured individual interviews allowed participants to express their views and thoughts in a safe and private context without the pressure of how their experiences may be viewed by other participants. Thus, the interview data add depth to the clinical / scale data provided by consumers.
In total 26 staff across the 3 sites participated. These included staff who provided therapy in the Clinics (i.e. clinic staff, n=13), staff who referred consumers to the Clinics (n= 6), senior managers at each site who had responsibility for overseeing the establishment of the Clinics (n= 6), and services who received consumers from the clinics (n=1).
2.3.5 Ethics Approval The evaluation protocol was reviewed and approved by the Darling Downs HHS Human Research Ethics Committee (LNR/19/QTDD/52228) on behalf of all sites through a process of mutual recognition. The evaluation was undertaken in accordance with NH&MRC guidelines.
Although informed consent is the gold standard in research and evaluation studies to ensure consumer autonomy, a waiver of consent was sought for the present study from the relevant ethics committee and granted. It was felt that consumers attending the AHBT Clinics were likely to be in a state of psychological distress. The impost of participating in an informed consent procedure at the initial meeting was likely to escalate what already is a stressful or anxious situation for consumers (Rebers, Aaronson, van Leeuwen & Schmidt, 2016). The implications of this could adversely impact on:
• the development of therapeutic relationships
• the limited time clinicians have to deliver therapeutic interventions
• the ongoing engagement of consumers in therapeutic interventions at the AHBT clinics, potentially increasing risk / presenting issue
• clinician responsibility to determine capacity of consumer to provide informed consent for study participation during heightened distress states
Informed consent processes can also impact on the quality and validity of available data through selection bias. Restricting data to those who consent may compromise external validity as any inferences drawn will be based on a subset of ‘consenting’ participants which may not be representative of the broader population group. Evidence from the literature also supports the argument that there are key differences between those that provide consent and those that do not (Porsdam Mann, Savulescu & Sahakian, 2016; Rebers et al, 2016; Kho, Duffett, Willison, Cook & Brouwers, 2009; Woolf, Rothemich, Johnson & Marsland, 2000). Consequently, study outcomes address the efficacy of the intervention among those who consent, whilst of greater importance and interest is evaluating the effectiveness of the clinics for all possible users.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 28 of 86
3 AHBT Clinic Implementation Process Findings Process evaluation examines the ‘processes’ around the day-to-day operation of the Clinics. As such, process evaluation examines factors such as referral pathways, hours of operation, number of sessions offered, session and clinical documentation, clinic governance and a description of the consumers accessing the Clinics.
3.1 AHBT Clinic Model of Service An endorsed Model of Service (MoS) document was developed with key stakeholders across the three sites to guide overarching implementation of the clinics (Appendix B). In addition to this, sites also developed and formalised operational guidelines and other supporting documentation specific to their local context.
3.1.1 Clinical Governance The AHBT Clinics were an add-on model of service that included service elements linked to acute care teams (ACT), primary care and general practice, private sector specialist services and non-government organisations that operated in alignment with the endorsed ACT model of service in each of the trial sites. During the trial, referrals to the AHBT clinics were made from AHBT clinic trial site ACT Teams only. Local acute care mental health teams remained as the Treating Unit in CIMHA while consumers were attending the clinics, which were provided by staff allocated to the AHBTC Treating Team in CIMHA. Clinical governance of the AHBT clinics therefore remained with the ACT Team.
The local ACT was identified on CIMHA as a ‘Treating Unit’ and the AHBT clinic as ‘Treating Team’. For all clients of the AHBT clinic, the Principal Service Provider was an ACT staff member and the AHBT clinic clinician listed as an Other Services Provider in CIMHA. Routine liaison between the local ACT and the AHBT clinic clinician was ongoing.
3.1.2 Clinic Operation and Staffing All clinics operated within business hours and provided services between 3 to 5 days per week. Sites had some flexibility regarding the days and times appointments were scheduled based on demand for service, consumer preferences / availability and clinician availability. No sessions were able to be provided after hours or on weekends.
Two of the clinics were located with a community non-government organisation with the remaining site utilising a Queensland Health Community Health centre. Near the end of the pilot, uncertainty around the continued funding of the NGO’s arose, with sites having to look at potential relocation and/ or other partnerships for the clinics to continue operation. Whilst one site was able to continue with the existing partnership arrangement, the other had to halt referrals until alternate arrangements could be put in place.
Clinics typically operated out of a single office and were provided with varying levels of infrastructure and support from staff at the co-location site (e.g. such as reception, waiting areas and storage facilities). Clinicians regularly had to either travel by car or walk to the co-location site, depending upon its proximity to their usual work base.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 29 of 86
During the pilot, a total of 18 clinicians worked across the three clinic sites. As there were no funded positions attached to the clinics, staff rotated through the clinics in a part time capacity whilst retaining their substantive roles and workloads. Whilst the majority of clinicians were based within the respective Acute Care Teams, a smaller number of staff worked in other mental health services / units. This resulted in some clinicians completing limited block placements within the clinics (e.g. 5 weeks). Clinician workload ranged from a few sessions per week to a couple of days based on a number of factors including clinician capacity and good will from service team leaders, as supported backfill was not available.
The clinics were predominantly staffed by psychologists (14 out of the 18), with the remaining allied health staff comprising of social workers (3) and a sole occupational therapist. A staff member at each of the sites was also nominated to take on the responsibility of coordinating and managing local clinic operation, activity (including new clinician orientation, service provision, clinic staff support) and stakeholder liaison during the pilot. As this position was also non funded, staff managed this responsibility on top of their substantive position workload.
3.1.3 Referral Process As outlined in the MoS, referral to the clinics was made via the Acute Care Teams. Consumers who had presented to Emergency Departments that met the eligibility criteria for the clinics were offered a referral to the clinic. Operational guidelines at each site documented the specific referral protocol and processes to be followed. Whilst these had many commonalities, for example a generic email account for referrals and appointment setting and the clinic coordinator being the first point of contact, there was a key difference in the management process and timing of referrals.
At one site, the ACT ED clinician booked the consumer’s first session into the clinic outlook calendar and provided the consumer with this information prior to them leaving the ED. The remaining two sites referred eligible consumers presenting to ED onto the respective acute care teams, who then made the decision to offer referral onto the clinics. This resulted in different starting points for the measurement of the 3-business day rule (outlined in the MoS) for consumers to be seen at the clinics from the point of referral as opposed to their ED presentation. It may also have had implications on consumer uptake of referral and attendance at their first clinic session.
Planning for onward referrals from the clinics to other service providers was instigated at the initial session, due to the brief timing of the clinic intervention and to minimise the risk of consumers being placed on a wait list for a receiving service. Written and / or phone referrals were made to the relevant services and warm handovers, involving the clinician, consumer and receiving service were completed when possible.
3.1.4 Clinical Information Management & Access Clinicians across the three sites used all psychometric measures outlined in the MoS that were designated as part of standardised clinic service provision. Good completion rates of psychological measures were found at initial appointment, but this dropped off over consecutive consumer appointments. This can be attributed to a number of possible factors including consumer completion of measures was not compulsory, possible consumer drop out past the first session, or the consumer not being well enough to complete the measures. Of the measures used, DASS 21 (consumer completed) rated highest in terms of both initial and subsequent completion by consumers with the Suicide Ideation & Intent measure (completed by clinician in collaboration with consumer in interview format) being the least utilised.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 30 of 86
All measures were available in hard copy formats only, which then had to be stored securely either at the clinic co location site or back at the clinician’s substantive work location until they could be uploaded to CIMHA as part of the clinical documentation of the session. All measures also had to be manually scored as electronic / application-based versions of the measures were not approved for use during the pilot.
As two of the three clinics were located at non-Queensland Health facilities, clinicians at these sites did not initially have readily available access to or capacity to upload or refer to important clinical information management systems during clinic sessions, such as CIMHA. Laptops with external QH clinical information system capability and IT support were to be provided, but differences in procurement and IT / computing infrastructure policies resulted in delayed approvals until near the end of the pilot. Clinicians worked around this by either reviewing consumer clinical information or completing clinical documentation whilst they had access to the systems, either prior to or after clinic sessions (usually back in their substantive positions).
3.1.5 Therapeutic Interventions A range of brief, evidence based therapeutic interventions were used across the clinics. Clinicians generally had experience in using a number of approaches and were also supported through training, provision of resources and supervision to further expand their clinical skill and practice base. Rather than being prescriptive, clinicians used their clinical judgement to determine which approaches provided ‘best fit’ for individual consumers, whether this was use of a single therapy or combination of approaches.
The main therapeutic approaches / interventions offered across the three clinic sites included:
• Acceptance and Commitment Therapy (ACT)
• Attempted Suicide Short Intervention Program (ASSIP)
• Brief Intervention for Personality Disorder (Project AIR Strategy)
• Heart rate variability biofeedback (HRVB) / biofeedback
• Cognitive Behavioural Therapy (CBT)
• Cognitive Behavioural Therapy – Suicide Prevention (CBT – SP)
• Dialectical Behavioural Therapy (DBT)
• Feedback Informed Therapy (FIT)
• Motivational Interviewing (MI)
• Sensory Modulation
• Solution Focused Brief Therapy (SFBT)
• Single Session Family Consultation (SSFC) – offered as an adjunct to clinic
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 31 of 86
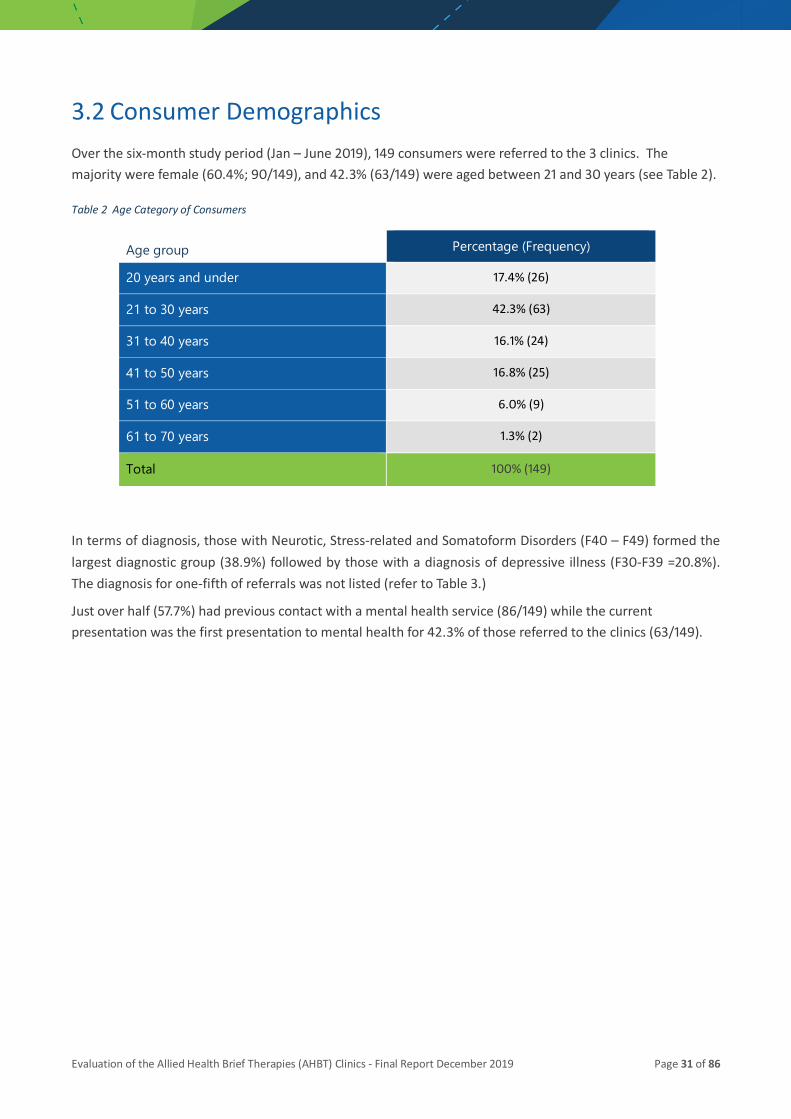
3.2 Consumer Demographics Over the six-month study period (Jan – June 2019), 149 consumers were referred to the 3 clinics. The majority were female (60.4%; 90/149), and 42.3% (63/149) were aged between 21 and 30 years (see Table 2).
Table 2 Age Category of Consumers
Age group Percentage (Frequency)
20 years and under 17.4% (26)
21 to 30 years 42.3% (63)
31 to 40 years 16.1% (24)
41 to 50 years 16.8% (25)
51 to 60 years 6.0% (9)
61 to 70 years 1.3% (2)
Total 100% (149)
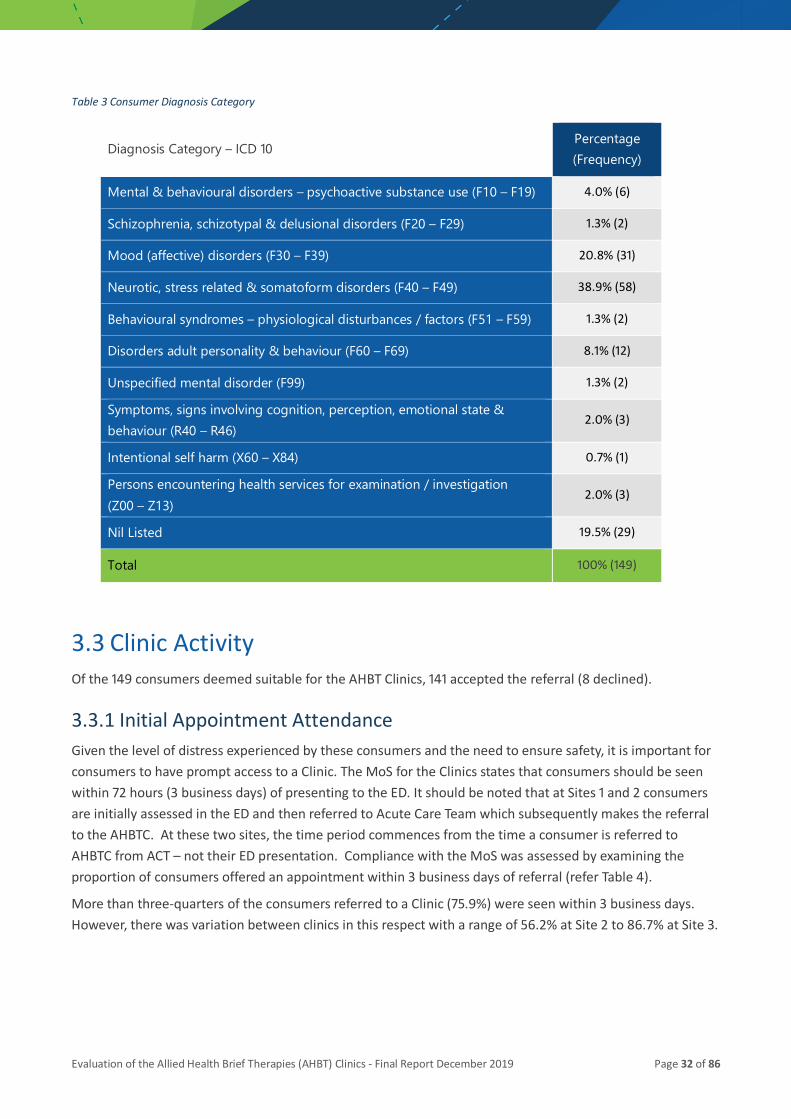
In terms of diagnosis, those with Neurotic, Stress-related and Somatoform Disorders (F40 – F49) formed the largest diagnostic group (38.9%) followed by those with a diagnosis of depressive illness (F30-F39 =20.8%). The diagnosis for one-fifth of referrals was not listed (refer to Table 3.)
Just over half (57.7%) had previous contact with a mental health service (86/149) while the current presentation was the first presentation to mental health for 42.3% of those referred to the clinics (63/149).
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 32 of 86
Table 3 Consumer Diagnosis Category
Diagnosis Category – ICD 10 Percentage (Frequency)
Mental & behavioural disorders – psychoactive substance use (F10 – F19) 4.0% (6)
Schizophrenia, schizotypal & delusional disorders (F20 – F29) 1.3% (2)
Mood (affective) disorders (F30 – F39) 20.8% (31)
Neurotic, stress related & somatoform disorders (F40 – F49) 38.9% (58)
Behavioural syndromes – physiological disturbances / factors (F51 – F59) 1.3% (2)
Disorders adult personality & behaviour (F60 – F69) 8.1% (12)
Unspecified mental disorder (F99) 1.3% (2)
Symptoms, signs involving cognition, perception, emotional state & behaviour (R40 – R46)
2.0% (3)
Intentional self harm (X60 – X84) 0.7% (1)
Persons encountering health services for examination / investigation (Z00 – Z13)
2.0% (3)
Nil Listed 19.5% (29)
Total 100% (149)
3.3 Clinic Activity Of the 149 consumers deemed suitable for the AHBT Clinics, 141 accepted the referral (8 declined).
3.3.1 Initial Appointment Attendance Given the level of distress experienced by these consumers and the need to ensure safety, it is important for consumers to have prompt access to a Clinic. The MoS for the Clinics states that consumers should be seen within 72 hours (3 business days) of presenting to the ED. It should be noted that at Sites 1 and 2 consumers are initially assessed in the ED and then referred to Acute Care Team which subsequently makes the referral to the AHBTC. At these two sites, the time period commences from the time a consumer is referred to AHBTC from ACT – not their ED presentation. Compliance with the MoS was assessed by examining the proportion of consumers offered an appointment within 3 business days of referral (refer Table 4).
More than three-quarters of the consumers referred to a Clinic (75.9%) were seen within 3 business days. However, there was variation between clinics in this respect with a range of 56.2% at Site 2 to 86.7% at Site 3.
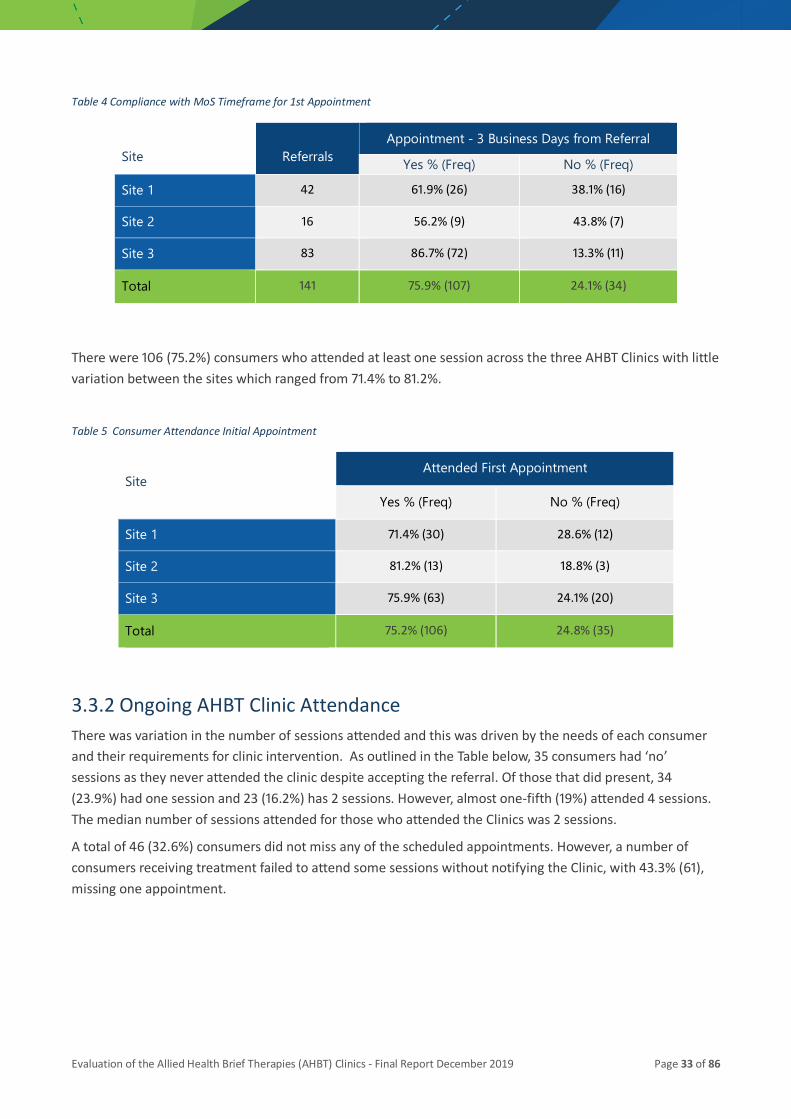
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 33 of 86
Table 4 Compliance with MoS Timeframe for 1st Appointment
Site Referrals Appointment - 3 Business Days from Referral
Yes % (Freq) No % (Freq)
Site 1 42 61.9% (26) 38.1% (16)
Site 2 16 56.2% (9) 43.8% (7)
Site 3 83 86.7% (72) 13.3% (11)
Total 141 75.9% (107) 24.1% (34)
There were 106 (75.2%) consumers who attended at least one session across the three AHBT Clinics with little variation between the sites which ranged from 71.4% to 81.2%.
Table 5 Consumer Attendance Initial Appointment
Site Attended First Appointment
Yes % (Freq) No % (Freq)
Site 1 71.4% (30) 28.6% (12)
Site 2 81.2% (13) 18.8% (3)
Site 3 75.9% (63) 24.1% (20)
Total 75.2% (106) 24.8% (35)
3.3.2 Ongoing AHBT Clinic Attendance There was variation in the number of sessions attended and this was driven by the needs of each consumer and their requirements for clinic intervention. As outlined in the Table below, 35 consumers had ‘no’ sessions as they never attended the clinic despite accepting the referral. Of those that did present, 34 (23.9%) had one session and 23 (16.2%) has 2 sessions. However, almost one-fifth (19%) attended 4 sessions. The median number of sessions attended for those who attended the Clinics was 2 sessions.
A total of 46 (32.6%) consumers did not miss any of the scheduled appointments. However, a number of consumers receiving treatment failed to attend some sessions without notifying the Clinic, with 43.3% (61), missing one appointment.

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 34 of 86
Table 6 Consumer AHBT Clinic Session Attendance
Number of Sessions Consumers - Sessions Attended
% (Freq)
Consumers - Sessions DNA
% (Freq)
0 sessions 24.8% (35) 32.6% (46)
1 session 23.9% (34) 43.3% (61)
2 sessions 16.2% (23) 13.4% (19)
3 sessions 12.0% (17) 9.2% (13)
4 sessions 19.0% (27) 1.4% (2)
5+ sessions 3.5% (5) -
Total 100% (141) 100% (141)
3.3.3 Consumer Referral Outcome Of the 149 consumers referred to the Clinics, 43% (64) completed all sessions agreed to by both the clinician and consumer. A further 36 consumers (24.2%) attended some sessions but disengaged prior to completion of planned sessions. Just over one-fifth (20.8%) did not attend the initial session that was booked for them. While attempts to contact these by phone usually proved unsuccessful, it is likely that the initial crisis had resolved between the time of referral the clinic appointment. Finally, a small group of the consumers (6.7%) were deemed no longer eligible as they were either admitted to hospital or had other / private service providers in the community (e.g. psychiatrists, psychologists). Refer to Table 7 below.
The data for two of the groups requires additional exploration. These include:
• those that did not start (DNS) and
• those that disengaged prior to treatment being completed.

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 35 of 86
Table 7 AHBT Clinic Consumer Referral Outcomes
Referral Outcome Definition Percentage (Frequency)
Declined by Consumer Consumer declined referral 5.4% (8)
Did not Start at Clinic (DNS) Consumer accepted referral but never attended
20.8% (31)
Disengaged Consumer attended clinic but was lost to follow up before completing all sessions
24.2% (36)
Completed Consumer attended all sessions agreed in consultation with clinician
43.0% (64)
No Longer Eligible Consumer no longer met eligibility criteria during clinic attendance
6.7% (10)
Total 100% (149)
Consumers - Did Not Start (DNS)
As outlined in the table above, 20.8% of consumers (n=31) did not present for their initial appointment at the Clinic despite an expressed desire by the consumer to do so. There was no significant difference in male (22.8%) and female (21.4%) consumers who did not start. However, a greater proportion of those in the 21 – 30 age group (54.8%) did not attend compared to those that did attend (39.1%).
While there was a greater proportion of those with previous contact (58.1%) with mental health services compared to those with no previous contact (41.9%) who did not present to their first appointment, the difference was not statistically significant (χ2= 0.67, p= 0.796).
Consumers Disengaged with Clinic
As outlined previously, 36 consumers (36/149) did not complete treatment as planned. In relation to gender, 44.4% of males and 55.6% of females disengaged from treatment and did not attend all sessions. Also, those that disengaged were more likely to be in the 21 – 30 age group (52.8%) compared to those that did engage (29.7%).
Finally, 54.7% of those with previous contact with mental health services completed treatment compared to 45.3% of those that were new to mental health. However, the difference was not statistically significant (χ2=0.007, p=0.93). Of those who disengaged, 21 (58.3%) attended 1 session, 11 (30.6%) attended 2 sessions and 3 (8.3%) attended 3 sessions.
3.3.4 Discharge Destination The discharge destination for all 106 consumers who attended at least one session at the Clinics is provided in the Table below. The largest group (23.6%) were referred to their GP for further treatment while 15.1% were referred to a Non-Government Organisation (NGO), or a combination of these service providers (9.4%).
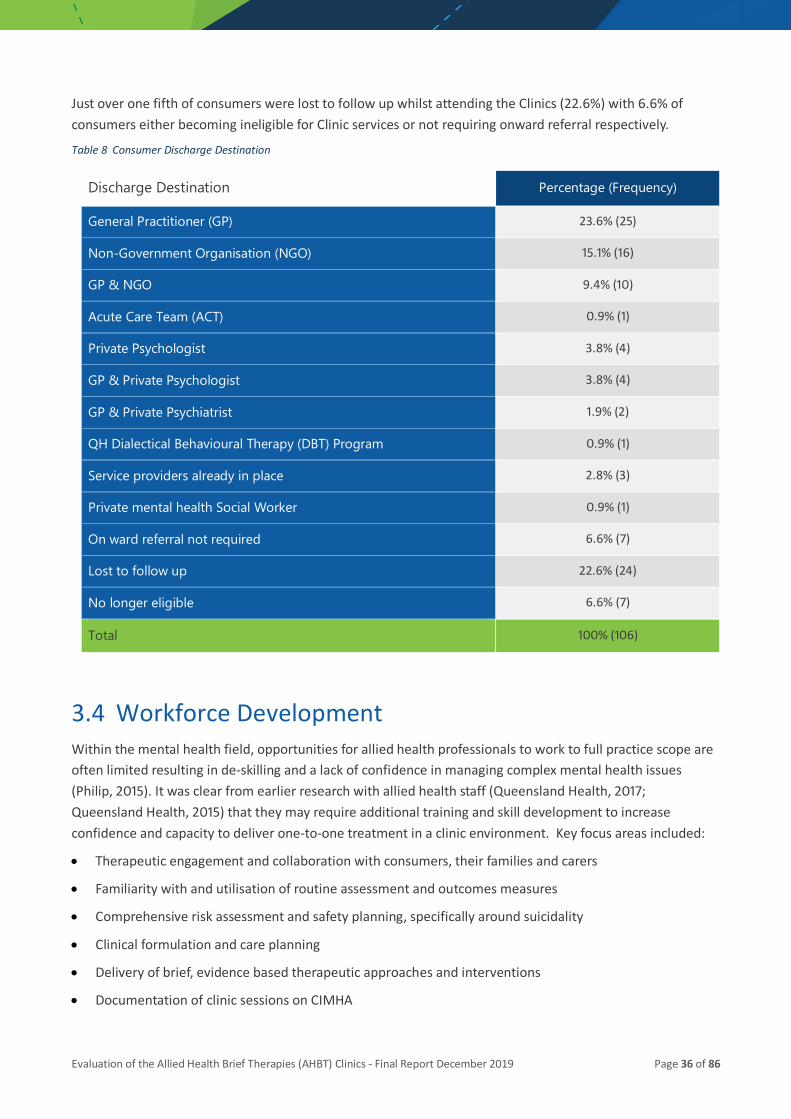
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 36 of 86
Just over one fifth of consumers were lost to follow up whilst attending the Clinics (22.6%) with 6.6% of consumers either becoming ineligible for Clinic services or not requiring onward referral respectively.
Table 8 Consumer Discharge Destination
Discharge Destination Percentage (Frequency)
General Practitioner (GP) 23.6% (25)
Non-Government Organisation (NGO) 15.1% (16)
GP & NGO 9.4% (10)
Acute Care Team (ACT) 0.9% (1)
Private Psychologist 3.8% (4)
GP & Private Psychologist 3.8% (4)
GP & Private Psychiatrist 1.9% (2)
QH Dialectical Behavioural Therapy (DBT) Program 0.9% (1)
Service providers already in place 2.8% (3)
Private mental health Social Worker 0.9% (1)
On ward referral not required 6.6% (7)
Lost to follow up 22.6% (24)
No longer eligible 6.6% (7)
Total 100% (106)
3.4 Workforce Development Within the mental health field, opportunities for allied health professionals to work to full practice scope are often limited resulting in de-skilling and a lack of confidence in managing complex mental health issues (Philip, 2015). It was clear from earlier research with allied health staff (Queensland Health, 2017; Queensland Health, 2015) that they may require additional training and skill development to increase confidence and capacity to deliver one-to-one treatment in a clinic environment. Key focus areas included:
• Therapeutic engagement and collaboration with consumers, their families and carers
• Familiarity with and utilisation of routine assessment and outcomes measures
• Comprehensive risk assessment and safety planning, specifically around suicidality
• Clinical formulation and care planning
• Delivery of brief, evidence based therapeutic approaches and interventions
• Documentation of clinic sessions on CIMHA
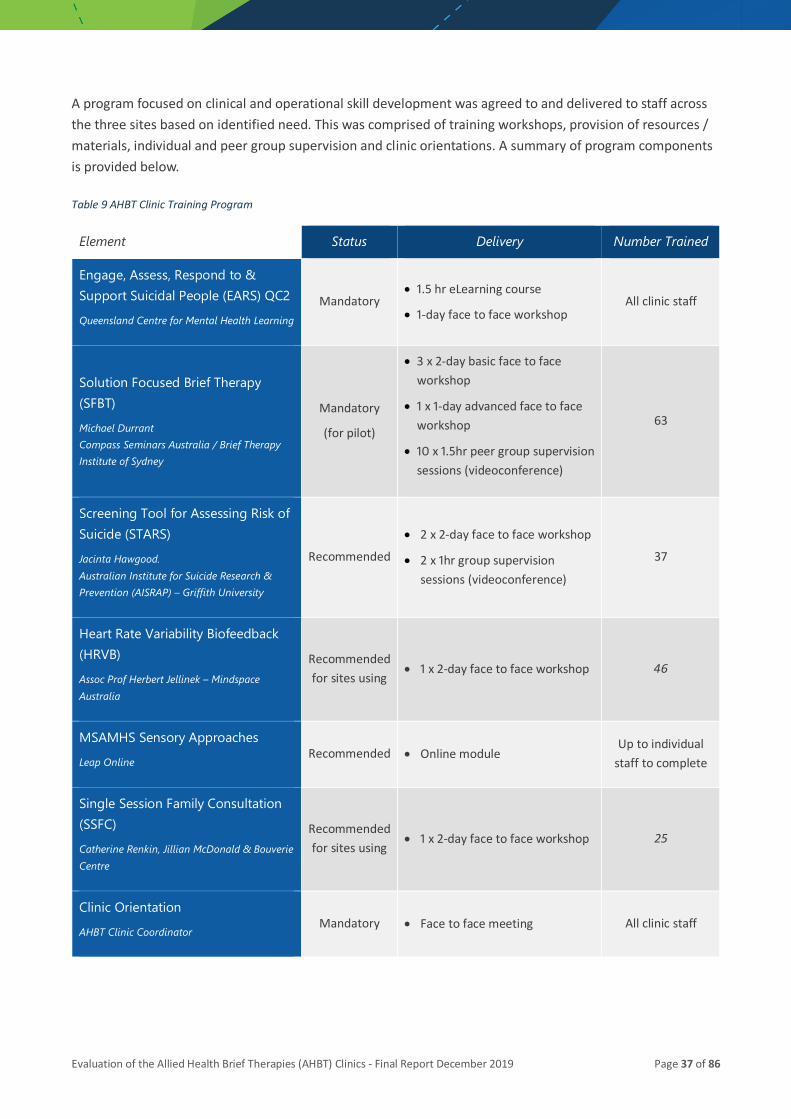
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 37 of 86
A program focused on clinical and operational skill development was agreed to and delivered to staff across the three sites based on identified need. This was comprised of training workshops, provision of resources / materials, individual and peer group supervision and clinic orientations. A summary of program components is provided below.
Table 9 AHBT Clinic Training Program
Element Status Delivery Number Trained
Engage, Assess, Respond to & Support Suicidal People (EARS) QC2 Queensland Centre for Mental Health Learning
Mandatory • 1.5 hr eLearning course
• 1-day face to face workshop All clinic staff
Solution Focused Brief Therapy (SFBT) Michael Durrant Compass Seminars Australia / Brief Therapy Institute of Sydney
Mandatory
(for pilot)
• 3 x 2-day basic face to face workshop
• 1 x 1-day advanced face to face workshop
• 10 x 1.5hr peer group supervision sessions (videoconference)
63
Screening Tool for Assessing Risk of Suicide (STARS) Jacinta Hawgood. Australian Institute for Suicide Research & Prevention (AISRAP) – Griffith University
Recommended
• 2 x 2-day face to face workshop
• 2 x 1hr group supervision sessions (videoconference)
37
Heart Rate Variability Biofeedback (HRVB) Assoc Prof Herbert Jellinek – Mindspace Australia
Recommended for sites using
• 1 x 2-day face to face workshop 46
MSAMHS Sensory Approaches Leap Online
Recommended • Online module Up to individual
staff to complete
Single Session Family Consultation (SSFC) Catherine Renkin, Jillian McDonald & Bouverie Centre
Recommended for sites using
• 1 x 2-day face to face workshop 25
Clinic Orientation AHBT Clinic Coordinator
Mandatory • Face to face meeting All clinic staff
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 38 of 86
3.5 Staff perceptions of implementation As outlined previously, the mental health staff (clinicians and managers) directly involved with the initiative were invited to participate in individual interviews. The aim of these interviews was to enable those involved to describe, in their own words, their perceptions of a range of issues around the establishment of the Clinics. In total 26 staff across the 3 sites participated. Themes related to the ‘process’ of providing therapy at the Clinics are discussed below.
3.5.1 Filling an important gap All clinicians interviewed felt that the AHBT Clinics were a good fit within existing service delivery structures as it filled an important emergent gap within current service provision for consumers as well as clinicians.
What works well from my perspective is that it, I think, fills a gap for consumers who need help straight away. And by help I mean therapy, crisis support, rather than just repeated
assessment. And that seems to be a gap in our district, and I think a lot of districts. So the way the service – the clinic – was structured worked really well in meeting that need. And certainly we had that feedback from consumers that it was what they were wanting and
needing at the time. (Clinic Clinician)
And
Acute care teams, prior to this amazing pressure that they see coming through EDs and so forth … I think the definition was that they provide like brief intervention in teams that I’ve
worked in before, it was sort of up to three months. So I think it’s a return really to an element of acute care that previously was there… that it’s not just about assessment and managing the risk after a presentation, it’s actually providing some sort of intervention as
well. So I think it’s more back to that but the reason why that stopped is more the pressure, not that they don’t want to. (Clinic Clinician)
While community service options are available for those with suicidality, these can be difficult to access and have long wait times. The Clinics enabled consumers to receive a more intensive intervention than what may have been otherwise provided:
They're [ACT] really motivated to refer people. They're seeing a benefit of it and it does…. because that was one of…. one of the difficulties we had is we had a wait list for private
psychologists. We were having people on our journey board for long periods of time anyway. So at least with the clinic they're not getting assessed, assessed and assessed, and having a risk assessment…they're getting some therapeutic intervention. So, I think
for the consumers’ journey and the consumers’ experience of what they're being exposed to it's much better. And they're going to get a lot more gains from that than our team
[ACT]. They're getting a therapeutic intervention rather than just re-screened until they're…. until they link with someone else. By the time they get to see a private
psychologist, if they're not already engaged, it's over, it's done and dusted. (Referring Clinician)

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 39 of 86
The managers interviewed also held positive views of the Clinics. There was a perception that the introduction of the Clinics could break the assess and refer approach:
My perceptions are that it [introduction of AHBT Clinics] is an innovation. For some people it might not seem as different as what other services might be doing, but the way that it is set up within a system … I think it’s still very early days, but it has even more potential to have benefits for consumers, breaking that cycle of assessment, admission, assessment,
discharge, assessment, admission. (Manager)
The AHBT clinic approach provided staff with sufficient time to properly assess the consumer, provide initial support and link them into the most appropriate care options for ongoing treatment. This was not always possible under the current ‘treatment as usual’ approach:
I’m seeing the same clientele. The difference is we’re giving them [consumers] a different service. They [consumers] would have been discharged and referred to their GP or
referred to a place that we nominated as being a beneficial one that might meet their service needs but there wasn’t that time taken to get them to process why it would be good adjusting to this change or to consider it, whereas this process allows you a few
weeks to do that. (Clinic Clinician)
The ‘brief’ focus of the therapy was also noted. Some of those interviewed welcomed the short-term approach to patient therapy within the model of service for the Clinics. Staff were clear that the focus was on treating the primary issue for the consumer and not dealing with all the concerns a consumer may have:
The issue of being brief has always been the key element of it for me to be honest, just knowing that it’s only four sessions, and this has been in the work instructions and you tell
them [consumers] that you’re not going to stay with this clinic for a long, long time. It allowed us to be quite specific in terms of the treatment targets, what we’re targeting, even in the way that we are communicating or talking to our clients, and say, “Hey, you might have other issues that need ongoing therapy, but we need to look at something quite practical and specific,” so that really helped a lot for clients who have listened to
that and say, “okay, maybe I have to really explore some things that are quite tangible, it’s quite a specific timeframe…..realistic,” and I think that’s what I love about this brief
interventions; it’s quite targeted about something really specific.(Clinic Clinician)
3.5.2 Clinic integration with community co-location partner An integral part of the AHBT Clinic implementation was the selection and location of co-location partners. Location of the Clinics in a non-clinical setting was viewed as a core component of the service model in terms of increasing consumer comfort, uptake of clinic services and onward referral:
Because I don't think it's so much about being based at that non-government organisation specifically, but it's about being based somewhere away from the rather unpleasant
environment of public mental health facilities that usually aren't very welcoming (Clinic Clinician)
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 40 of 86
However, uncertainty around continued funding at two of the three sites created some challenges regarding clinic implementation and delivery. Both sites had to reduce / halt referrals until the situation resolved with one site being able to continue operation whilst the other had to source an alternate location for the clinic:
It has been difficult to sustain and the numbers of referrals has been difficult to sustain. Our location of clinics is at risk, if we’ve got clinic bookings where we currently have them. If we can't maintain them, we’re at risk of losing those bookings. (Manager)
Co -location partners provided the physical infrastructure to support clinic implementation. This covered things such as office / consulting room space, reception / waiting areas, storage and telephone and internet facilities. There was however an issue with clinicians being able to access and manage consumer clinical information externally at two of the three sites due to the clinics being in non-Queensland health facilities.
We didn't have access to CIMHA through the computer that we had, we did have access to the internet. I don't know where that came from so I guess it was just the Wi-Fi in the
building, but it did have some implications on accessing things like CIMHA, but we could access our emails through the work email portal. Printers we had access to, photocopiers
we had access to, phones we had access to and so I think the only other thing that would've been nice had we had it … was having like an iPad or a laptop with external
access (Clinic Clinician)
A lack of formalised communication channels between clinic staff and staff at the co -location sites also had implications for service implementation, particularly between site reception and visiting clinicians:
Where someone wasn’t able to attend … they used to call them [co located clinic] in the morning. We would be going, attending, and then all of a sudden the [clinic] reception
would say, “Oh, hang on a minute. We’ve received a few phone calls about your clients,”…. So that’s why it caused some issues, especially if you had one client, perhaps, or one no-show, so basically you would go in there and no one is there, and you’ve got to
come back (Clinic Clinician)
And
Particularly if it’s a first appointment with someone, you don’t know what they look like, and you have to keep coming out the front and calling the name over and over…. and then
I’ve had times when I’ve assumed someone’s not come because they’ve been late and then they’ve come in and they’ve just waited there for an hour and left(Clinic Clinician)
3.5.3 Clinic integration with ACT Those interviewed identified the integration of the AHBT Clinics within local Acute Care Teams (ACT) as a major strength of the service model. A clear understanding of the purpose of the Clinics and the services provided by services referring in and consumers was essential to the success of implementation:

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 41 of 86
Probably one of the bigger challenges was that often people who I saw haven’t really been informed what the Clinic was, or the purpose of it. I don’t know that actually that it
wasn’t explained well, or if it was actually, they were at such a heightened state of distress when they presented to ED that they weren’t taking on that information. It’s all a lot to go through. I am assuming that it would have been discussed, because they had to consent to it, so I would say it is more around, maybe at the point of referral, if there’s a
flyer they can take away and have access to review, it might be beneficial. (Clinic Clinician)
The Clinic Coordinator position, although not funded was viewed as an essential lynchpin between ACT and the Clinics:
Just having a clinic coordinator is really helpful as well … having someone oversee the whole processes and the ACT team involvement. So that’s a really, really big one. They do
a lot of the follow up phone calls with the consumers in between sessions and just even small things like sending an SMS message so then our community clinician does that and
that does improve the chances of them coming in the next day. (Clinic Clinician)
Clinic staff felt that they were part of a ‘team’ and not solely responsible for the consumers treated in the Clinics:
So it sits very comfortably under ACT. So rather than I guess being kind of like a satellite service or clinic that's operated really independently it is very much under the umbrella of
ACT and I think that helps because it promotes a feeling of ownership within the team. And so I think that sense of ownership is that it was led by people within the acute care
team, the cases are all discussed at the acute care team team review meetings. It's mainly staffed by clinicians from ACT, not wholly, but largely staffed by clinicians from ACT.
(Clinic Clinician)
This integration enabled the clinic clinicians to received support and practical assistance when issues emerged with the clients. They felt that having ACT involved provided a safety net when they had concerns about a consumer:
I’ll ring them up [ACT staff] and be, like, hey, I’ve just seen this person, here’s where they’re at in terms of the risk….. and sometimes where there’s been individuals that I
wanted them to monitor and how they would accept that and then engage in that monitoring (Clinic Clinician)
3.5.4 Need for documented systems and processes The importance of documented processes and systems to support the implementation of the clinics was noted, particularly in relation to the current staffing arrangements operating across the sites:
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 42 of 86
I think having clear processes that are written down will be really key for keeping it going. Because then if staffing changes and people move in and out someone new can come in
and they'll know how it operates … We have had clinicians from other teams kind of rotate into the clinic and do a set period and then go back to their own teams. And that's worked quite well. But I think that would be something that would probably fluctuate as to, yes, if we have the interest and kind of rely on the goodwill of team leaders to release
people from their roles. (Clinic Clinician).
Documented eligibility criteria were useful in ensuring that referrals to the Clinics were appropriate.
So, we kind of worked out that we would discuss it in an MDTR and flag someone that might be a candidate for allied health brief therapies. So, in the assessment the clinician would kind of be thinking about that, whether they fit that kind of criteria and whether they have capacity. One of the things that I was keen about when we were first having discussions about it, that we referred people that would actually get good benefit from
them [Clinics]…. that they [consumers] would have that level of engagement and motivation to continue on with things. (Referring Clinician)
As mentioned previously, there was some differences in the referral pathways and process utilised at each of the sites. Some clinicians felt that making the referral at the time of ED presentation had the potential to increase attendance at initial appointments and provide a more timely and effective service response:
The process is, if we’ve done an intake and assessment of a client in the ED and they meet some of the criteria that’s been provided by the psychologist, then we ascertain if the consumer’s interested and if they are then we progress to make an appointment on a
calendar with the vacancies that are all highlighted with the various clinicians that provide that service. (Referring Clinician)
And
If there is some way the ACT could make the referrals at the time when they have seen the person rather than doing it the next day or a few days later, I think that that would be
more effective so that we could actually see someone face-to-face the day or two days after they presented to emergency department. I think one of the issues that we are
having is, often by the time we got a referral and got to see someone, the crisis was well and truly passed and they didn’t really want or need the intervention. (Clinic Clinician)
3.5.5 Training All staff were more than satisfied with the training provided to prepare them to work in the clinic environment. A key focus of the training program was on solution focused therapy as this has been found to be a useful approach in previous research (Gingerich & Peterson, 2012; Fiske, 2008; Hendon, 2008; Sharry, Darmody & Madden, 2002). All clinic staff had participated in training in Solution Focused Brief Therapy
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 43 of 86
(SFBT) and many spoke about the challenges in changing their approach to using SFBT. They noted that SFBT was strengths based and useful in that it has less of a focus on consumer problems:
I have found that experience really valuable using the solution focused therapy because it uses a different approach and it is very much strength based and it is focusing less on the consumer’s problems and allowing them to think of helpful corrective strategies for them.
So, I definitely found it really valuable and it is just a different way of thinking. (Clinic Clinician)
Ongoing concerns about the ongoing training will need to be addressed locally and innovatively in order to ensure that Clinics have a suitably skilled and sustainable workforce pool to deliver services:
But the thing I have a question over is … what the plan is from an internal service perspective to continue to train people and prep them to be able to provide those services adequately for them. So at the moment we’re taking on a bit of a mentor model but that model is actually really intensive in and of itself. So it's selecting the right staff who are
going to be around in the service for a while and mentoring them in. (Manager)
3.6 Summary This section of the Report provides an overview of the ‘processes’ that were required to support the introduction of the Clinics. The importance of having clear documentation and processes around the operation of the Clinics was considered paramount given that the Clinics involved a new service component treating a high-risk cohort. As such, the initiative was underpinned by a Model of Service (MoS) delivery document which was considered integral to the implementation process. However, despite the MoS, the three services took a slightly different approach to implementation in keeping with local policies and service structures.
All 3 clinics were managed through the local Acute Care Team (ACT). As such, the Principal Service Provider for AHBT clients was an ACT staff member and the AHBT clinic clinician listed as an Other Services Provider in CIMHA.
During the pilot, a total of 18 clinicians worked across the three clinic sites. As there were no funded positions attached to the clinics, staff rotated through the clinics in a part time capacity whilst retaining their substantive roles and workloads. The need for staff training for those volunteering to work in the Clinics was also identified. AHBT clinicians were supported in this regard through the provision of targeted professional development and training in brief interventions and suicide risk management. A program of ongoing clinical supervision is currently being provided to assist staff in translating learning into practice.
Our findings indicate that the AHBT Clinic model provides prompt treatment and support for people at the time of their greatest need and ensures safe transition from one service provider to the next. This approach supports the current roll-out of the Zero Suicide Framework.
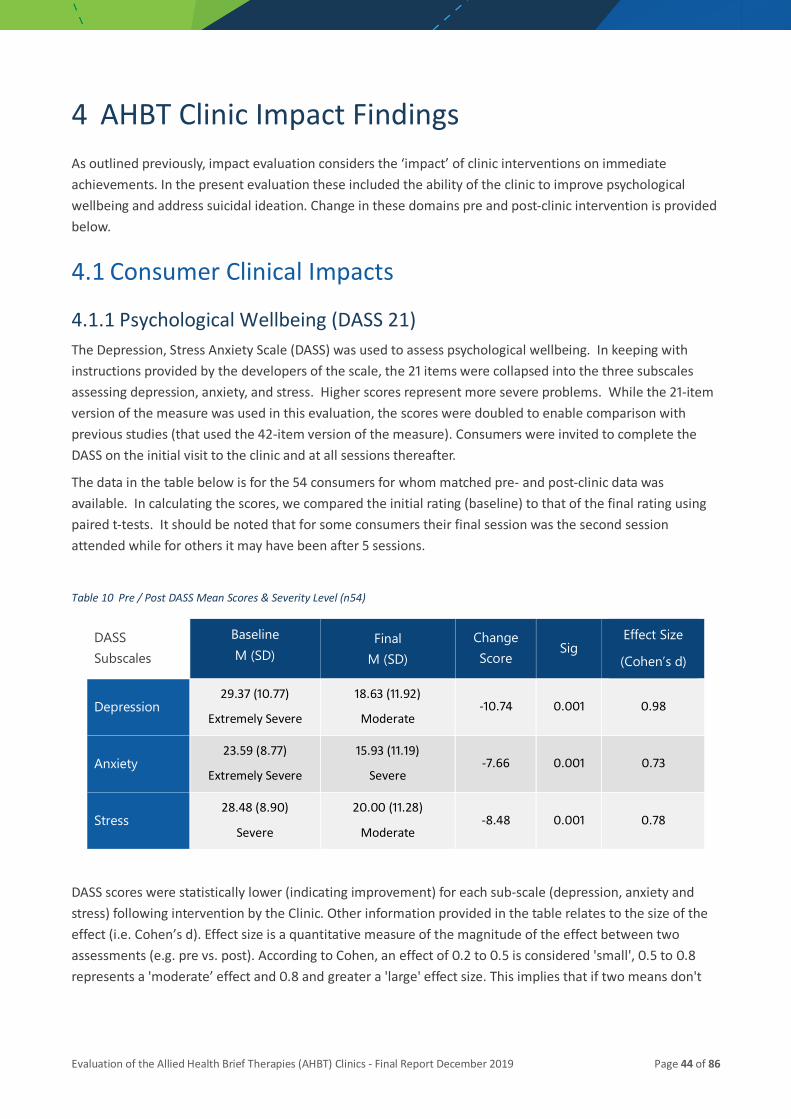
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 44 of 86
4 AHBT Clinic Impact Findings As outlined previously, impact evaluation considers the ‘impact’ of clinic interventions on immediate achievements. In the present evaluation these included the ability of the clinic to improve psychological wellbeing and address suicidal ideation. Change in these domains pre and post-clinic intervention is provided below.
4.1 Consumer Clinical Impacts
4.1.1 Psychological Wellbeing (DASS 21) The Depression, Stress Anxiety Scale (DASS) was used to assess psychological wellbeing. In keeping with instructions provided by the developers of the scale, the 21 items were collapsed into the three subscales assessing depression, anxiety, and stress. Higher scores represent more severe problems. While the 21-item version of the measure was used in this evaluation, the scores were doubled to enable comparison with previous studies (that used the 42-item version of the measure). Consumers were invited to complete the DASS on the initial visit to the clinic and at all sessions thereafter.
The data in the table below is for the 54 consumers for whom matched pre- and post-clinic data was available. In calculating the scores, we compared the initial rating (baseline) to that of the final rating using paired t-tests. It should be noted that for some consumers their final session was the second session attended while for others it may have been after 5 sessions.
Table 10 Pre / Post DASS Mean Scores & Severity Level (n54)
DASS Subscales
Baseline M (SD)
Final M (SD)
Change Score
Sig Effect Size
(Cohen’s d)
Depression 29.37 (10.77)
Extremely Severe
18.63 (11.92)
Moderate -10.74 0.001 0.98
Anxiety 23.59 (8.77)
Extremely Severe
15.93 (11.19)
Severe -7.66 0.001 0.73
Stress 28.48 (8.90)
Severe
20.00 (11.28)
Moderate -8.48 0.001 0.78
DASS scores were statistically lower (indicating improvement) for each sub-scale (depression, anxiety and stress) following intervention by the Clinic. Other information provided in the table relates to the size of the effect (i.e. Cohen’s d). Effect size is a quantitative measure of the magnitude of the effect between two assessments (e.g. pre vs. post). According to Cohen, an effect of 0.2 to 0.5 is considered 'small', 0.5 to 0.8 represents a 'moderate’ effect and 0.8 and greater a 'large' effect size. This implies that if two means don't
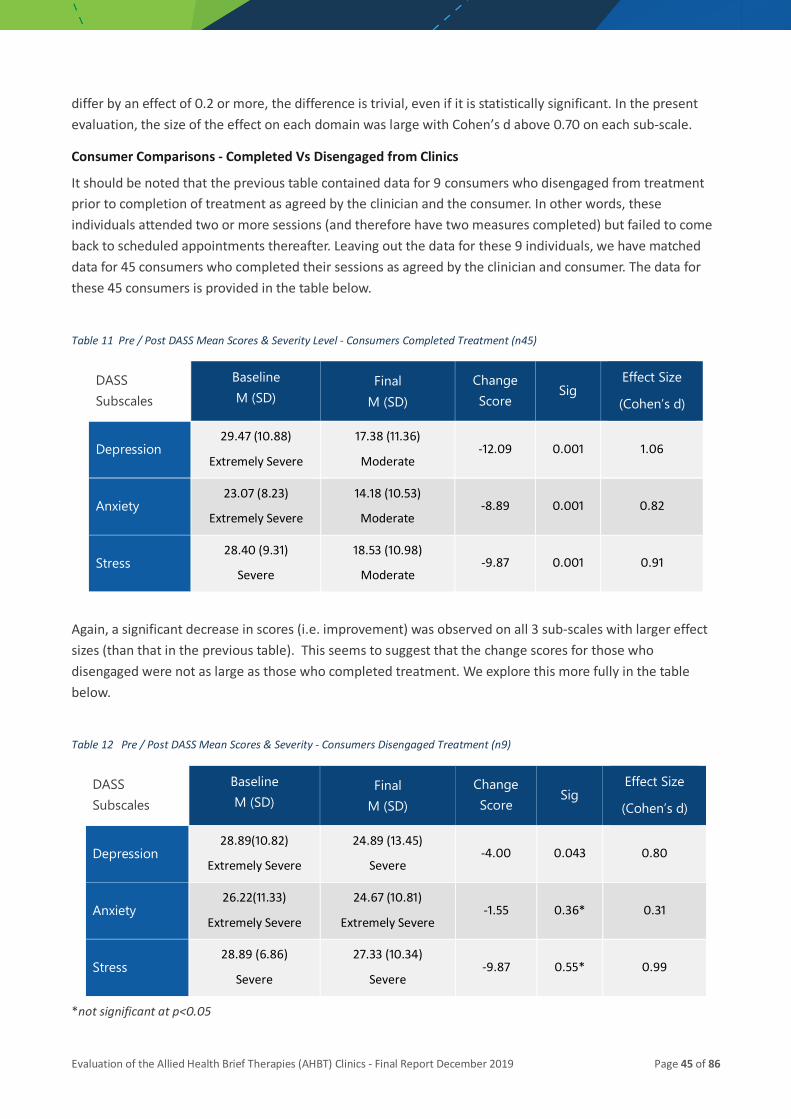
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 45 of 86
differ by an effect of 0.2 or more, the difference is trivial, even if it is statistically significant. In the present evaluation, the size of the effect on each domain was large with Cohen’s d above 0.70 on each sub-scale.
Consumer Comparisons - Completed Vs Disengaged from Clinics
It should be noted that the previous table contained data for 9 consumers who disengaged from treatment prior to completion of treatment as agreed by the clinician and the consumer. In other words, these individuals attended two or more sessions (and therefore have two measures completed) but failed to come back to scheduled appointments thereafter. Leaving out the data for these 9 individuals, we have matched data for 45 consumers who completed their sessions as agreed by the clinician and consumer. The data for these 45 consumers is provided in the table below.
Table 11 Pre / Post DASS Mean Scores & Severity Level - Consumers Completed Treatment (n45)
DASS Subscales
Baseline M (SD)
Final M (SD)
Change Score
Sig Effect Size
(Cohen’s d)
Depression 29.47 (10.88)
Extremely Severe
17.38 (11.36)
Moderate -12.09 0.001 1.06
Anxiety 23.07 (8.23)
Extremely Severe
14.18 (10.53)
Moderate -8.89 0.001 0.82
Stress 28.40 (9.31)
Severe
18.53 (10.98)
Moderate -9.87 0.001 0.91
Again, a significant decrease in scores (i.e. improvement) was observed on all 3 sub-scales with larger effect sizes (than that in the previous table). This seems to suggest that the change scores for those who disengaged were not as large as those who completed treatment. We explore this more fully in the table below.
Table 12 Pre / Post DASS Mean Scores & Severity - Consumers Disengaged Treatment (n9)
DASS Subscales
Baseline M (SD)
Final M (SD)
Change Score
Sig Effect Size
(Cohen’s d)
Depression 28.89(10.82)
Extremely Severe
24.89 (13.45)
Severe -4.00 0.043 0.80
Anxiety 26.22(11.33)
Extremely Severe
24.67 (10.81)
Extremely Severe -1.55 0.36* 0.31
Stress 28.89 (6.86)
Severe
27.33 (10.34)
Severe -9.87 0.55* 0.99
*not significant at p<0.05
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 46 of 86
It is clear from the data provided above that those who disengaged from treatment had lower change scores and lower effect sizes than those who remained in treatment. Nonetheless, the depression score decreased significantly with a Cohen’s d of 0.80 which indicates positive effect. An independent samples t – test was conducted to determine if the differences between the two cohorts in terms of their baseline and final scores was significant. No significant differences were found for the baseline scores for each of the subscales as well as the depression subscale pre and post (t (52) = -1.756, p=0.085). There were however significant differences between the two groups at final review for both the anxiety (t (52) = -2.716, p=0.009) and stress (t (52) = -2.214), p= 0.031) subscales respectively.
4.1.2 Comparing AHBT Clinic DASS Outcomes to Similar Initiatives As outlined in the literature summary for this evaluation, there are a number of similar initiatives that have been established in Australia to support those with suicidality. These include the Mental Health Nurse Incentive program (MHNIP), Access to Allied Psychological Services (ATAPS) and Access to Psychological Services – Suicide Prevention (ATAPS – SP).
Table 13 provides comparative DASS outcomes data for these initiatives against those of the AHBT Clinics. It is clear that all of the programs were capable of promoting significant improvements as measured by the DASS subscales. The consumers accessing the AHBT Clinics had higher mean scores on the baseline for all DASS subscales when compared to those in other programs. While this was not significantly different from other programs, it does indicate the condition severity in the consumers presenting to the AHBT Clinics. It is also clear that the extent of improvement on the 3 sub-scales for consumers accessing the AHBT Clinics (as demonstrated by the effect sizes) is similar to improvement achieved by more extensive interventions such as ATAPS and ATAPS-SP.
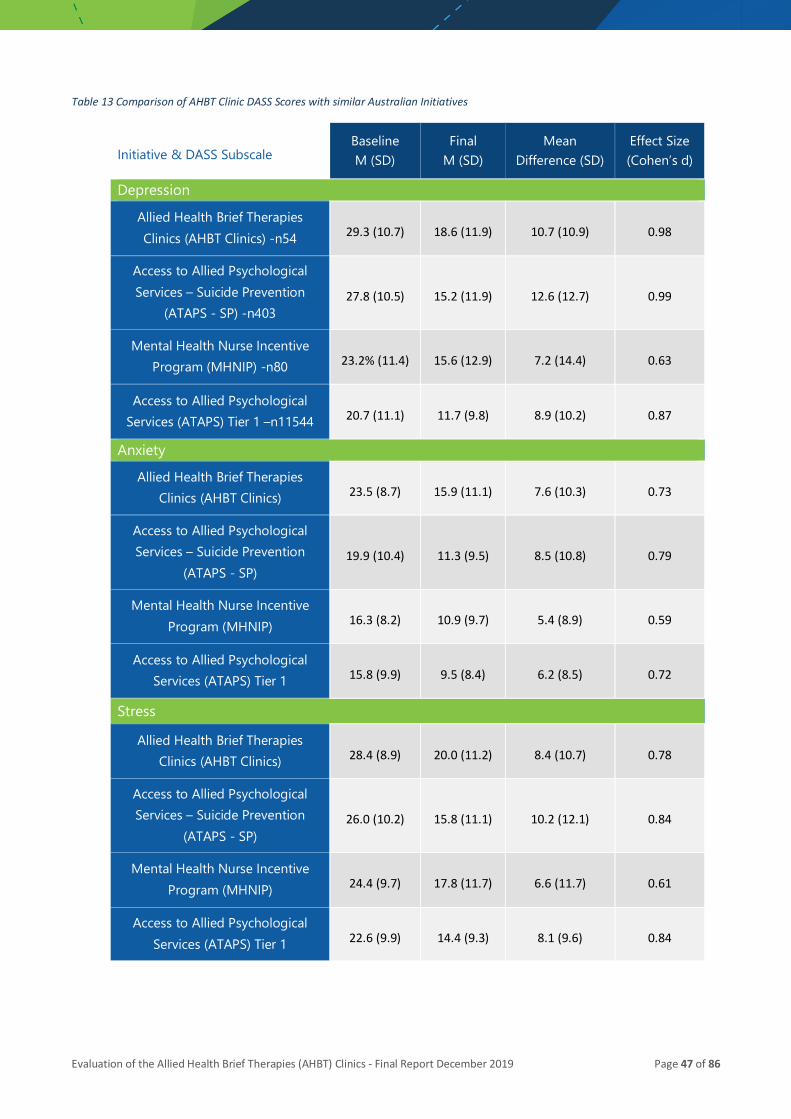
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 47 of 86
Table 13 Comparison of AHBT Clinic DASS Scores with similar Australian Initiatives
Initiative & DASS Subscale Baseline M (SD)
Final M (SD)
Mean Difference (SD)
Effect Size (Cohen’s d)
Depression Allied Health Brief Therapies Clinics (AHBT Clinics) -n54 29.3 (10.7) 18.6 (11.9) 10.7 (10.9) 0.98
Access to Allied Psychological Services – Suicide Prevention
(ATAPS - SP) -n403 27.8 (10.5) 15.2 (11.9) 12.6 (12.7) 0.99
Mental Health Nurse Incentive Program (MHNIP) -n80 23.2% (11.4) 15.6 (12.9) 7.2 (14.4) 0.63
Access to Allied Psychological Services (ATAPS) Tier 1 –n11544 20.7 (11.1) 11.7 (9.8) 8.9 (10.2) 0.87
Anxiety
Allied Health Brief Therapies Clinics (AHBT Clinics) 23.5 (8.7) 15.9 (11.1) 7.6 (10.3) 0.73
Access to Allied Psychological Services – Suicide Prevention
(ATAPS - SP) 19.9 (10.4) 11.3 (9.5) 8.5 (10.8) 0.79
Mental Health Nurse Incentive Program (MHNIP) 16.3 (8.2) 10.9 (9.7) 5.4 (8.9) 0.59
Access to Allied Psychological Services (ATAPS) Tier 1 15.8 (9.9) 9.5 (8.4) 6.2 (8.5) 0.72
Stress
Allied Health Brief Therapies Clinics (AHBT Clinics) 28.4 (8.9) 20.0 (11.2) 8.4 (10.7) 0.78
Access to Allied Psychological Services – Suicide Prevention
(ATAPS - SP) 26.0 (10.2) 15.8 (11.1) 10.2 (12.1) 0.84
Mental Health Nurse Incentive Program (MHNIP) 24.4 (9.7) 17.8 (11.7) 6.6 (11.7) 0.61
Access to Allied Psychological Services (ATAPS) Tier 1 22.6 (9.9) 14.4 (9.3) 8.1 (9.6) 0.84
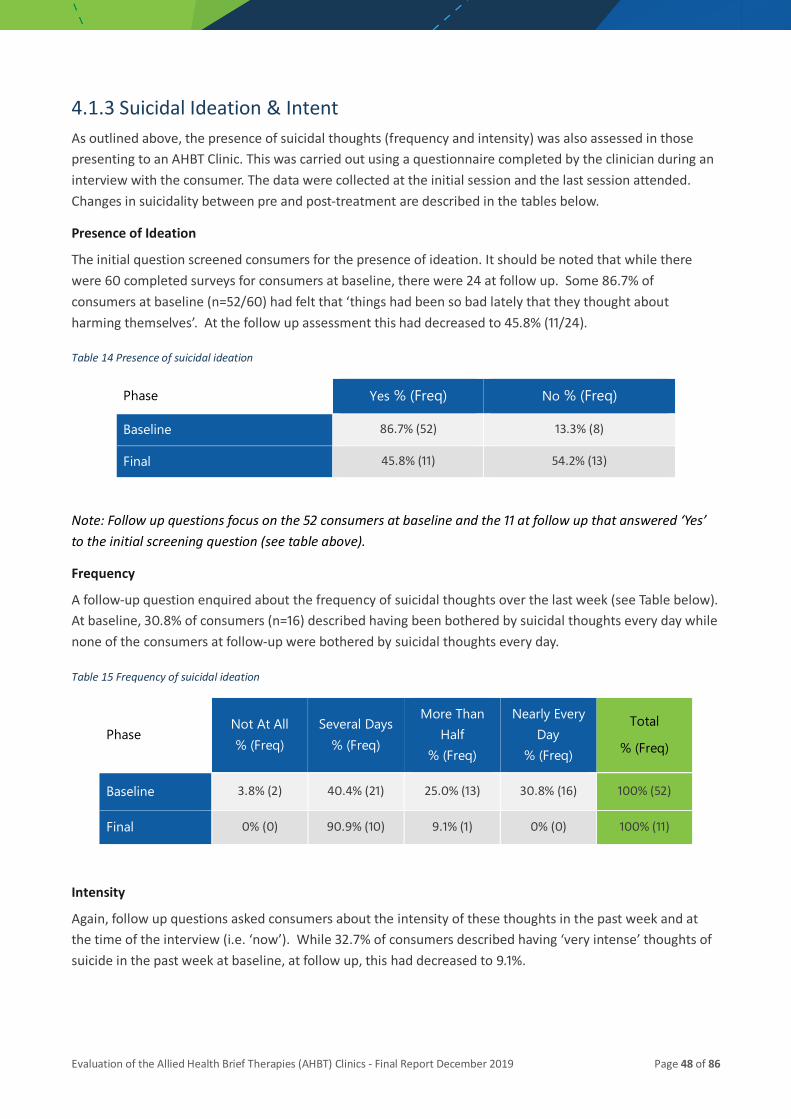
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 48 of 86
4.1.3 Suicidal Ideation & Intent As outlined above, the presence of suicidal thoughts (frequency and intensity) was also assessed in those presenting to an AHBT Clinic. This was carried out using a questionnaire completed by the clinician during an interview with the consumer. The data were collected at the initial session and the last session attended. Changes in suicidality between pre and post-treatment are described in the tables below.
Presence of Ideation
The initial question screened consumers for the presence of ideation. It should be noted that while there were 60 completed surveys for consumers at baseline, there were 24 at follow up. Some 86.7% of consumers at baseline (n=52/60) had felt that ‘things had been so bad lately that they thought about harming themselves’. At the follow up assessment this had decreased to 45.8% (11/24).
Table 14 Presence of suicidal ideation
Phase Yes % (Freq) No % (Freq)
Baseline 86.7% (52) 13.3% (8)
Final 45.8% (11) 54.2% (13)
Note: Follow up questions focus on the 52 consumers at baseline and the 11 at follow up that answered ‘Yes’ to the initial screening question (see table above).
Frequency
A follow-up question enquired about the frequency of suicidal thoughts over the last week (see Table below). At baseline, 30.8% of consumers (n=16) described having been bothered by suicidal thoughts every day while none of the consumers at follow-up were bothered by suicidal thoughts every day.
Table 15 Frequency of suicidal ideation
Phase Not At All % (Freq)
Several Days % (Freq)
More Than Half
% (Freq)
Nearly Every Day
% (Freq)
Total
% (Freq)
Baseline 3.8% (2) 40.4% (21) 25.0% (13) 30.8% (16) 100% (52)
Final 0% (0) 90.9% (10) 9.1% (1) 0% (0) 100% (11)
Intensity
Again, follow up questions asked consumers about the intensity of these thoughts in the past week and at the time of the interview (i.e. ‘now’). While 32.7% of consumers described having ‘very intense’ thoughts of suicide in the past week at baseline, at follow up, this had decreased to 9.1%.
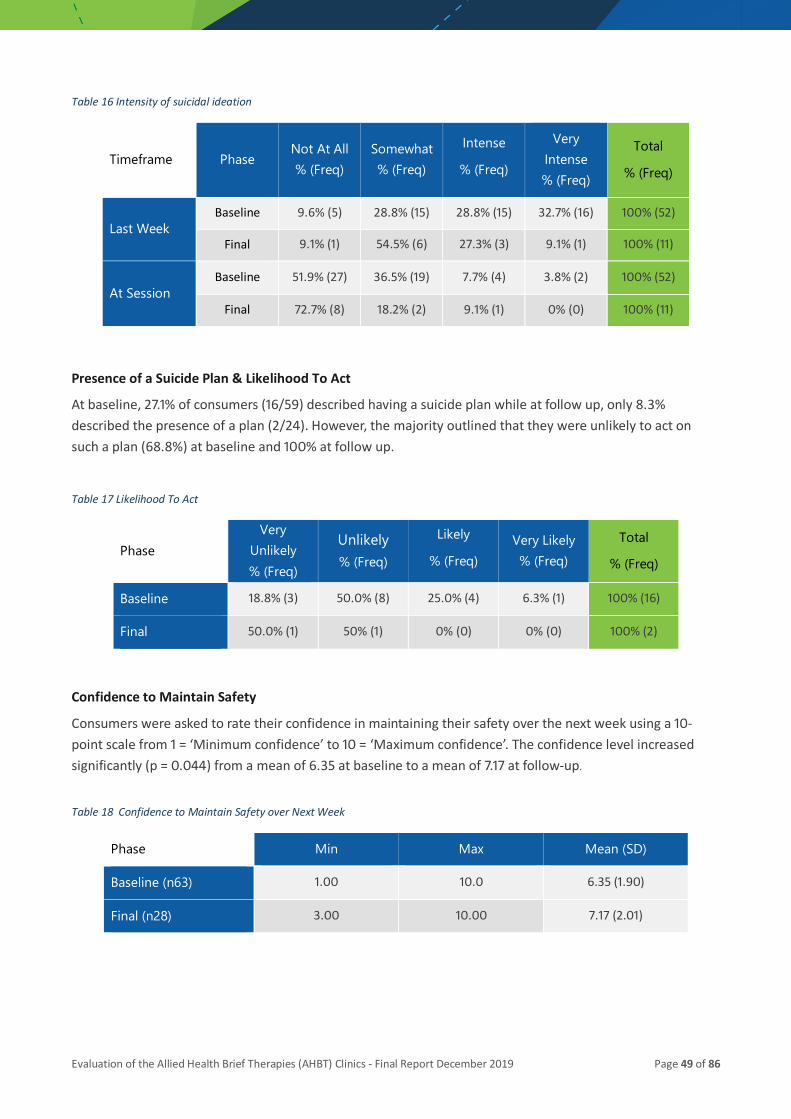
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 49 of 86
Table 16 Intensity of suicidal ideation
Timeframe Phase Not At All % (Freq)
Somewhat % (Freq)
Intense
% (Freq)
Very Intense % (Freq)
Total
% (Freq)
Last Week Baseline 9.6% (5) 28.8% (15) 28.8% (15) 32.7% (16) 100% (52)
Final 9.1% (1) 54.5% (6) 27.3% (3) 9.1% (1) 100% (11)
At Session Baseline 51.9% (27) 36.5% (19) 7.7% (4) 3.8% (2) 100% (52)
Final 72.7% (8) 18.2% (2) 9.1% (1) 0% (0) 100% (11)
Presence of a Suicide Plan & Likelihood To Act
At baseline, 27.1% of consumers (16/59) described having a suicide plan while at follow up, only 8.3% described the presence of a plan (2/24). However, the majority outlined that they were unlikely to act on such a plan (68.8%) at baseline and 100% at follow up.
Table 17 Likelihood To Act
Phase Very
Unlikely % (Freq)
Unlikely % (Freq)
Likely
% (Freq) Very Likely % (Freq)
Total
% (Freq)
Baseline 18.8% (3) 50.0% (8) 25.0% (4) 6.3% (1) 100% (16)
Final 50.0% (1) 50% (1) 0% (0) 0% (0) 100% (2)
Confidence to Maintain Safety
Consumers were asked to rate their confidence in maintaining their safety over the next week using a 10-point scale from 1 = ‘Minimum confidence’ to 10 = ‘Maximum confidence’. The confidence level increased significantly (p = 0.044) from a mean of 6.35 at baseline to a mean of 7.17 at follow-up.
Table 18 Confidence to Maintain Safety over Next Week
Phase Min Max Mean (SD)
Baseline (n63) 1.00 10.0 6.35 (1.90)
Final (n28) 3.00 10.00 7.17 (2.01)

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 50 of 86
4.1.4 Consumer Functioning – Outcomes Rating Scale (ORS) The ORS is a visual analogue measure designed to monitor consumer satisfaction in 4 domains during treatment. These include:
• Individually (personal wellbeing);
• Interpersonally (family, close relationships);
• Socially (work, school, friendships); and
• Overall (general sense of well-being).
Each domain is rated on a 10-point scale with a higher score on a sub-scale or total scale representing a more favourable outcome.
The information in the table below is for any consumer with at least one session at an AHBT clinic (and had the ORS completed). As such, there is information for 84 consumers at baseline and 49 at follow-up. As outlined in the Table, there were significant improvements on all subscales between baseline and follow up. The size of the effect size for the overall scores between baseline and final measure was also large (Cohen’s d=-1.231).
Table 19 ORS Pre and Post Results
ORS Subscales Phase Min Score Max Score Mean (SD) Sig (p)*
Individually (Personal Wellbeing)
Baseline (n84) 0.00 10.00 2.82 (2.34) 0.001
Final (n49) 0.40 10.00 5.80 (2.86)
Interpersonally (Family / Friends)
Baseline (n84) 0.00 10.00 3.63 (2.75) 0.001
Final (n49) 0.90 10.00 6.36 (20.51)
Socially (Work / School)
Baseline (n84) 0.00 10.00 3.47 (2.85) 0.001
Final (n48) 0.10 10.00 5.99 (2.67)
Overall (General Wellbeing)
Baseline (n84) 0.00 10.00 3.00 (2.47) 0.001
Final (n49) 0.70 10.00 6.04 (2.55)
Total ORS Score Baseline (n84) 0.00 40.00 12.93 (8.60)
0.000 Final (n48) 6.00 40.00 24.45 (9.58)
*Sig (p) calculated using paired samples t test for consumers with matched data (n48)
The ‘Reliable Change Index’ was also examined to determine the ‘amount’ of change for the 48 consumers with matched data. Based on this approach (see Table below), three quarters (75%) of patients had either reliable change (33.3%) or clinically significant change (41.7%). None of the patients had deterioration.
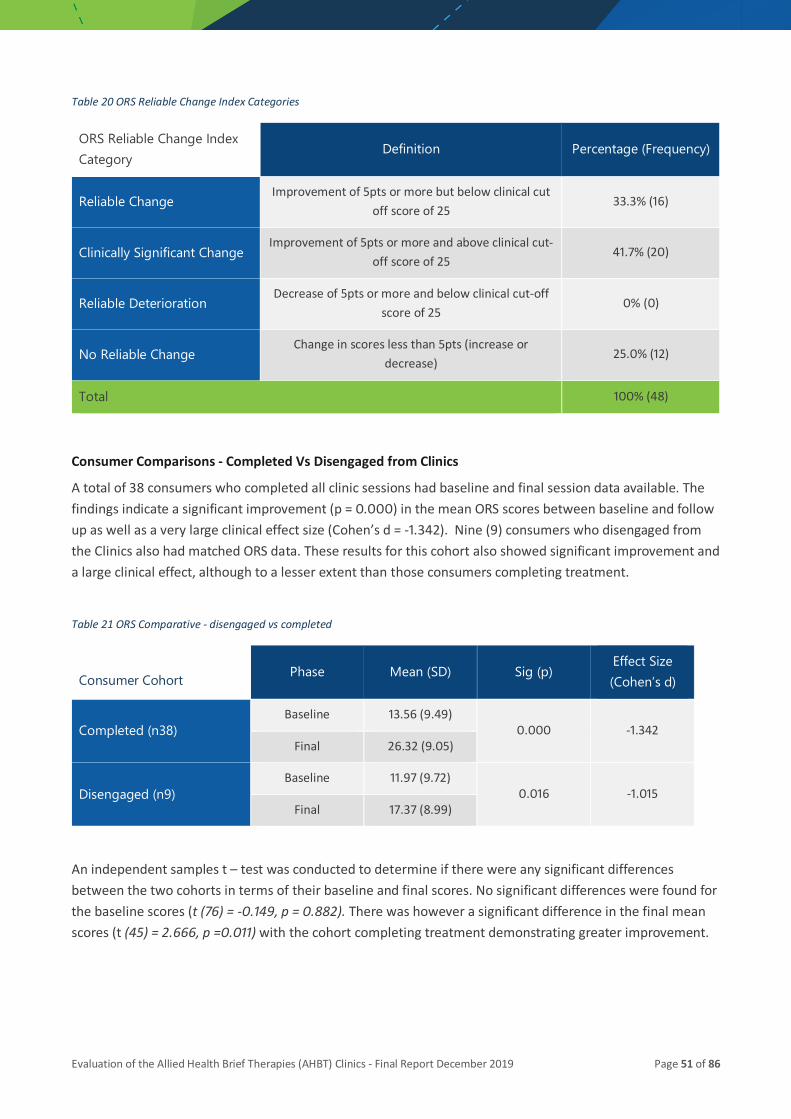
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 51 of 86
Table 20 ORS Reliable Change Index Categories
ORS Reliable Change Index Category
Definition Percentage (Frequency)
Reliable Change Improvement of 5pts or more but below clinical cut
off score of 25 33.3% (16)
Clinically Significant Change Improvement of 5pts or more and above clinical cut-
off score of 25 41.7% (20)
Reliable Deterioration Decrease of 5pts or more and below clinical cut-off
score of 25 0% (0)
No Reliable Change Change in scores less than 5pts (increase or
decrease) 25.0% (12)
Total 100% (48)
Consumer Comparisons - Completed Vs Disengaged from Clinics
A total of 38 consumers who completed all clinic sessions had baseline and final session data available. The findings indicate a significant improvement (p = 0.000) in the mean ORS scores between baseline and follow up as well as a very large clinical effect size (Cohen’s d = -1.342). Nine (9) consumers who disengaged from the Clinics also had matched ORS data. These results for this cohort also showed significant improvement and a large clinical effect, although to a lesser extent than those consumers completing treatment.
Table 21 ORS Comparative - disengaged vs completed
Consumer Cohort Phase Mean (SD) Sig (p) Effect Size (Cohen’s d)
Completed (n38) Baseline 13.56 (9.49)
0.000 -1.342 Final 26.32 (9.05)
Disengaged (n9) Baseline 11.97 (9.72)
0.016 -1.015 Final 17.37 (8.99)
An independent samples t – test was conducted to determine if there were any significant differences between the two cohorts in terms of their baseline and final scores. No significant differences were found for the baseline scores (t (76) = -0.149, p = 0.882). There was however a significant difference in the final mean scores (t (45) = 2.666, p =0.011) with the cohort completing treatment demonstrating greater improvement.
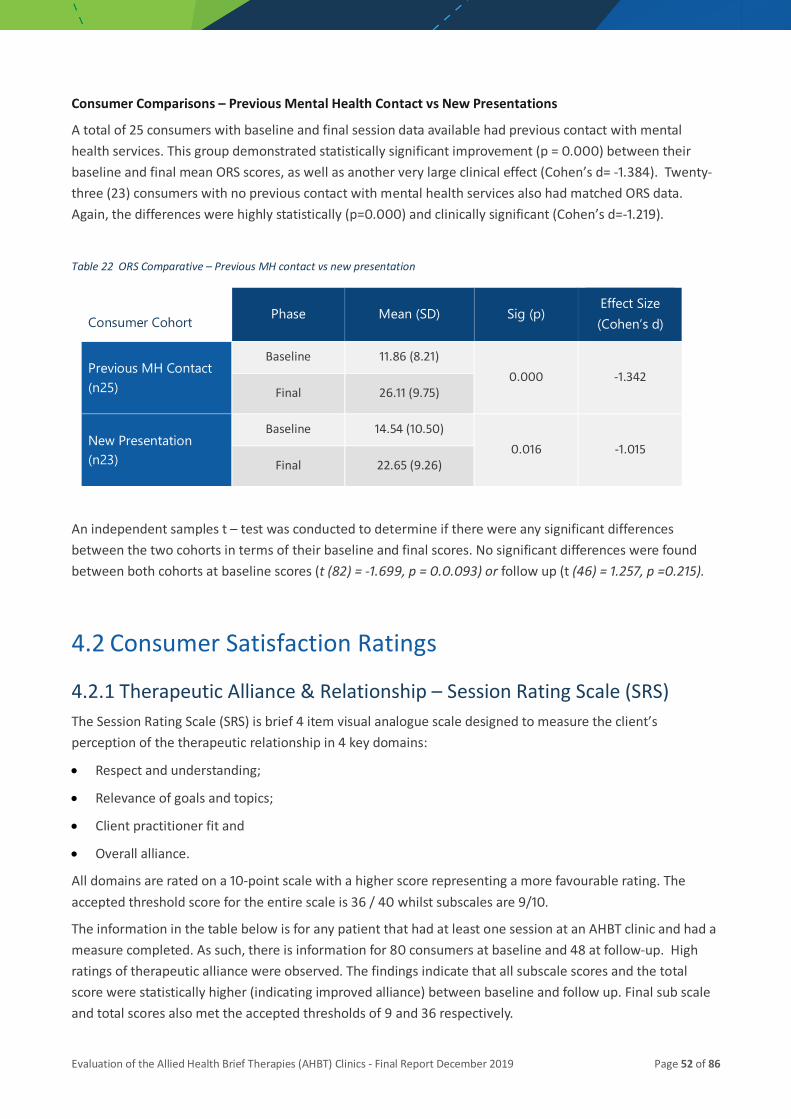
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 52 of 86
Consumer Comparisons – Previous Mental Health Contact vs New Presentations
A total of 25 consumers with baseline and final session data available had previous contact with mental health services. This group demonstrated statistically significant improvement (p = 0.000) between their baseline and final mean ORS scores, as well as another very large clinical effect (Cohen’s d= -1.384). Twenty-three (23) consumers with no previous contact with mental health services also had matched ORS data. Again, the differences were highly statistically (p=0.000) and clinically significant (Cohen’s d=-1.219).
Table 22 ORS Comparative – Previous MH contact vs new presentation
Consumer Cohort Phase Mean (SD) Sig (p) Effect Size (Cohen’s d)
Previous MH Contact (n25)
Baseline 11.86 (8.21) 0.000 -1.342
Final 26.11 (9.75)
New Presentation (n23)
Baseline 14.54 (10.50) 0.016 -1.015
Final 22.65 (9.26)
An independent samples t – test was conducted to determine if there were any significant differences between the two cohorts in terms of their baseline and final scores. No significant differences were found between both cohorts at baseline scores (t (82) = -1.699, p = 0.0.093) or follow up (t (46) = 1.257, p =0.215).
4.2 Consumer Satisfaction Ratings
4.2.1 Therapeutic Alliance & Relationship – Session Rating Scale (SRS) The Session Rating Scale (SRS) is brief 4 item visual analogue scale designed to measure the client’s perception of the therapeutic relationship in 4 key domains:
• Respect and understanding;
• Relevance of goals and topics;
• Client practitioner fit and
• Overall alliance.
All domains are rated on a 10-point scale with a higher score representing a more favourable rating. The accepted threshold score for the entire scale is 36 / 40 whilst subscales are 9/10.
The information in the table below is for any patient that had at least one session at an AHBT clinic and had a measure completed. As such, there is information for 80 consumers at baseline and 48 at follow-up. High ratings of therapeutic alliance were observed. The findings indicate that all subscale scores and the total score were statistically higher (indicating improved alliance) between baseline and follow up. Final sub scale and total scores also met the accepted thresholds of 9 and 36 respectively.
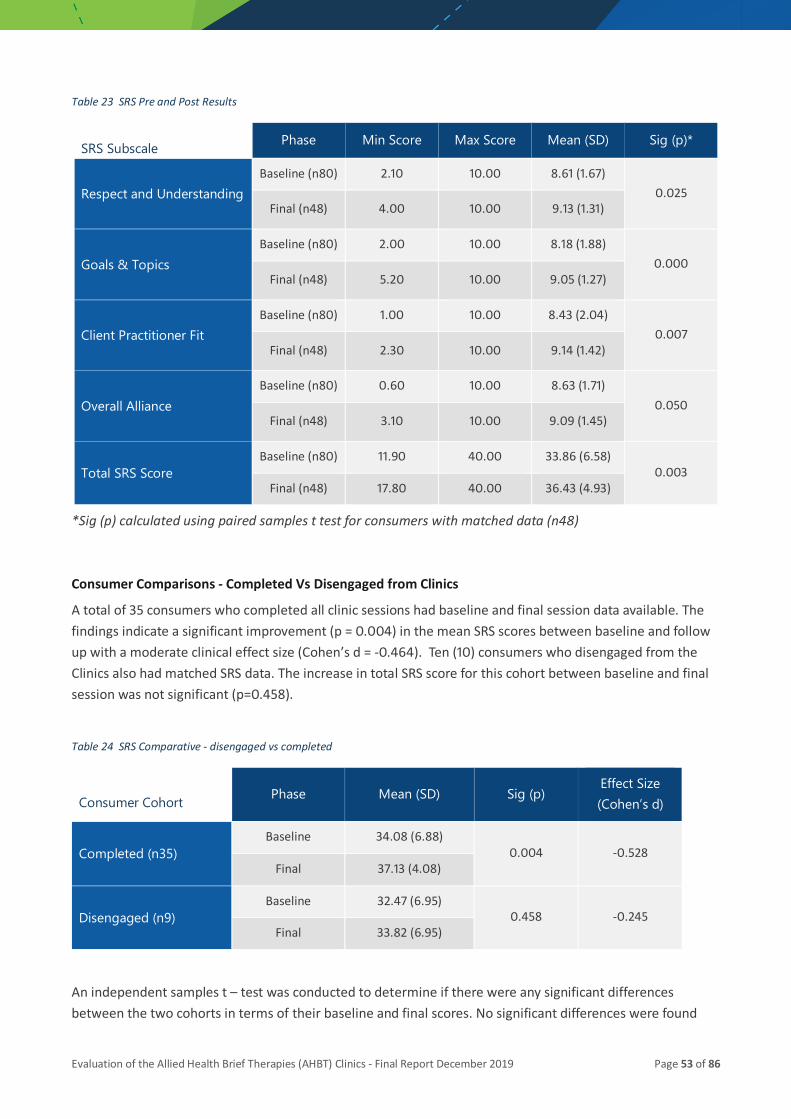
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 53 of 86
Table 23 SRS Pre and Post Results
SRS Subscale Phase Min Score Max Score Mean (SD) Sig (p)*
Respect and Understanding Baseline (n80) 2.10 10.00 8.61 (1.67)
0.025 Final (n48) 4.00 10.00 9.13 (1.31)
Goals & Topics Baseline (n80) 2.00 10.00 8.18 (1.88)
0.000 Final (n48) 5.20 10.00 9.05 (1.27)
Client Practitioner Fit Baseline (n80) 1.00 10.00 8.43 (2.04)
0.007 Final (n48) 2.30 10.00 9.14 (1.42)
Overall Alliance Baseline (n80) 0.60 10.00 8.63 (1.71)
0.050 Final (n48) 3.10 10.00 9.09 (1.45)
Total SRS Score Baseline (n80) 11.90 40.00 33.86 (6.58)
0.003 Final (n48) 17.80 40.00 36.43 (4.93)
*Sig (p) calculated using paired samples t test for consumers with matched data (n48)
Consumer Comparisons - Completed Vs Disengaged from Clinics
A total of 35 consumers who completed all clinic sessions had baseline and final session data available. The findings indicate a significant improvement (p = 0.004) in the mean SRS scores between baseline and follow up with a moderate clinical effect size (Cohen’s d = -0.464). Ten (10) consumers who disengaged from the Clinics also had matched SRS data. The increase in total SRS score for this cohort between baseline and final session was not significant (p=0.458).
Table 24 SRS Comparative - disengaged vs completed
Consumer Cohort Phase Mean (SD) Sig (p) Effect Size (Cohen’s d)
Completed (n35) Baseline 34.08 (6.88)
0.004 -0.528 Final 37.13 (4.08)
Disengaged (n9) Baseline 32.47 (6.95)
0.458 -0.245 Final 33.82 (6.95)
An independent samples t – test was conducted to determine if there were any significant differences between the two cohorts in terms of their baseline and final scores. No significant differences were found
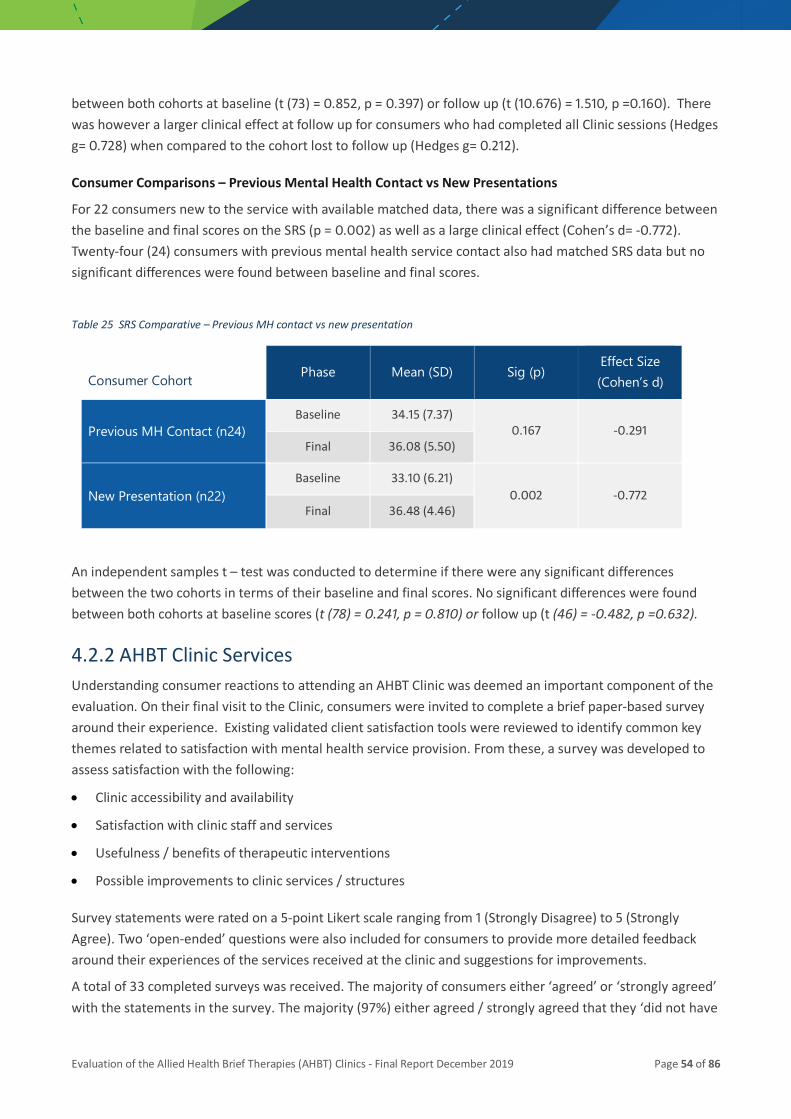
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 54 of 86
between both cohorts at baseline (t (73) = 0.852, p = 0.397) or follow up (t (10.676) = 1.510, p =0.160). There was however a larger clinical effect at follow up for consumers who had completed all Clinic sessions (Hedges g= 0.728) when compared to the cohort lost to follow up (Hedges g= 0.212).
Consumer Comparisons – Previous Mental Health Contact vs New Presentations
For 22 consumers new to the service with available matched data, there was a significant difference between the baseline and final scores on the SRS (p = 0.002) as well as a large clinical effect (Cohen’s d= -0.772). Twenty-four (24) consumers with previous mental health service contact also had matched SRS data but no significant differences were found between baseline and final scores.
Table 25 SRS Comparative – Previous MH contact vs new presentation
Consumer Cohort Phase Mean (SD) Sig (p) Effect Size (Cohen’s d)
Previous MH Contact (n24) Baseline 34.15 (7.37)
0.167 -0.291 Final 36.08 (5.50)
New Presentation (n22) Baseline 33.10 (6.21)
0.002 -0.772 Final 36.48 (4.46)
An independent samples t – test was conducted to determine if there were any significant differences between the two cohorts in terms of their baseline and final scores. No significant differences were found between both cohorts at baseline scores (t (78) = 0.241, p = 0.810) or follow up (t (46) = -0.482, p =0.632).
4.2.2 AHBT Clinic Services Understanding consumer reactions to attending an AHBT Clinic was deemed an important component of the evaluation. On their final visit to the Clinic, consumers were invited to complete a brief paper-based survey around their experience. Existing validated client satisfaction tools were reviewed to identify common key themes related to satisfaction with mental health service provision. From these, a survey was developed to assess satisfaction with the following:
• Clinic accessibility and availability
• Satisfaction with clinic staff and services
• Usefulness / benefits of therapeutic interventions
• Possible improvements to clinic services / structures
Survey statements were rated on a 5-point Likert scale ranging from 1 (Strongly Disagree) to 5 (Strongly Agree). Two ‘open-ended’ questions were also included for consumers to provide more detailed feedback around their experiences of the services received at the clinic and suggestions for improvements.
A total of 33 completed surveys was received. The majority of consumers either ‘agreed’ or ‘strongly agreed’ with the statements in the survey. The majority (97%) either agreed / strongly agreed that they ‘did not have
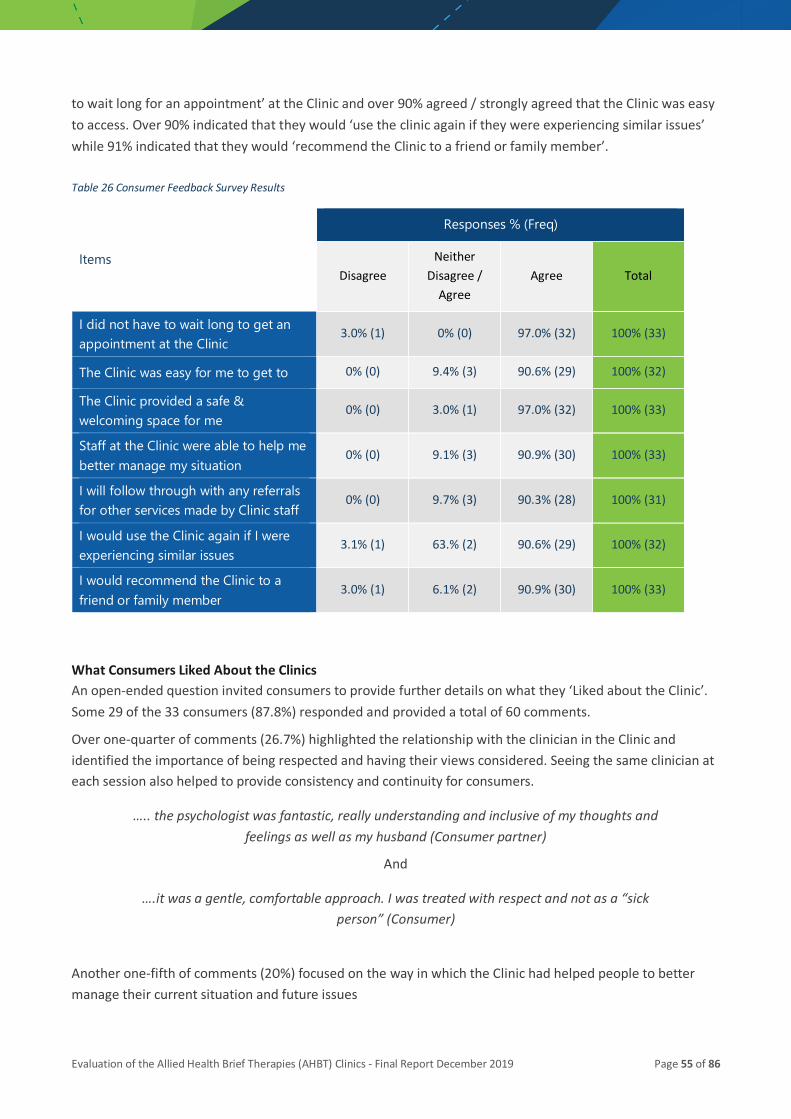
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 55 of 86
to wait long for an appointment’ at the Clinic and over 90% agreed / strongly agreed that the Clinic was easy to access. Over 90% indicated that they would ‘use the clinic again if they were experiencing similar issues’ while 91% indicated that they would ‘recommend the Clinic to a friend or family member’. Table 26 Consumer Feedback Survey Results
Items
Responses % (Freq)
Disagree Neither
Disagree / Agree
Agree Total
I did not have to wait long to get an appointment at the Clinic
3.0% (1) 0% (0) 97.0% (32) 100% (33)
The Clinic was easy for me to get to 0% (0) 9.4% (3) 90.6% (29) 100% (32)
The Clinic provided a safe & welcoming space for me
0% (0) 3.0% (1) 97.0% (32) 100% (33)
Staff at the Clinic were able to help me better manage my situation
0% (0) 9.1% (3) 90.9% (30) 100% (33)
I will follow through with any referrals for other services made by Clinic staff
0% (0) 9.7% (3) 90.3% (28) 100% (31)
I would use the Clinic again if I were experiencing similar issues
3.1% (1) 63.% (2) 90.6% (29) 100% (32)
I would recommend the Clinic to a friend or family member
3.0% (1) 6.1% (2) 90.9% (30) 100% (33)
What Consumers Liked About the Clinics An open-ended question invited consumers to provide further details on what they ‘Liked about the Clinic’. Some 29 of the 33 consumers (87.8%) responded and provided a total of 60 comments.
Over one-quarter of comments (26.7%) highlighted the relationship with the clinician in the Clinic and identified the importance of being respected and having their views considered. Seeing the same clinician at each session also helped to provide consistency and continuity for consumers.
….. the psychologist was fantastic, really understanding and inclusive of my thoughts and feelings as well as my husband (Consumer partner)
And
….it was a gentle, comfortable approach. I was treated with respect and not as a “sick person” (Consumer)
Another one-fifth of comments (20%) focused on the way in which the Clinic had helped people to better manage their current situation and future issues

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 56 of 86
…really listened to me … gave me the perfect tools to take home and use to help myself….even went through them with me. I feel 100% better to my first session here
(Consumer)
And
…..two lovely staff members went above and beyond to help with compassion [sic] and haist [sic]. Without them, I would have been – finalizing in some way (Consumer)
Other comments pointed to the Clinic and how this was a friendly and welcoming space with non-judgemental staff.
I liked that the staff were friendly and welcoming. They made me feel a lot more safe and better about my situation (Consumer)
And
I like it not feeling clinical. More like just chatting but with the confidence on going on and using the methods of coping suggested … (Consumer)
The ability to get an appointment quickly and the capacity to access community-based support services that consumers perceived that they would not otherwise be able to were also appreciated.
The fact that this is actually here for people and so handy (Consumer)
And
That I could talk to someone / get in to talking to someone (Consumer)
Suggested Improvements
The second open ended question asked consumers if they had any suggestions for improvement in relation to clinic service provision. Eight consumers (24.2%) made suggestions (n=10) for improvement. Some 50% of comments indicated that the duration and / or number of sessions should be increased and that an option to access extended services provided by the clinics after the initial session block would be welcomed.
I wish I had more sessions and I hope I can experience similar if not continued services like this one / or this one as an extension (Consumer)
Although back up support outside business hours was available via ACT and MH CALL, better access to clinic services after hours and weekends was also suggested.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 57 of 86
4.3 Staff Perceptions of Clinic Impact During interviews, staff were asked to describe how the introduction of the AHBT Clinics had impacted on their role. Comments were generally positive. Key themes are provided below.
4.3.1 Provides another option Staff employed in the ED have limited options when they need to refer patients for aftercare. It was also noted that the introduction of the AHBT clinics provide staff in ED (and ACT) with another treatment pathway:
So, it gave the acute care staff another option, a different option when the consumers needed treatment, particularly psychosocial or psychological treatments.
(Referring Clinician)
While managers had to make a strong case to support the introduction of the AHBT Clinics, there is now a perception that the Clinics are gaining acceptance. This is due in part to the implementation of Zero Suicide Framework as the AHBT Clinics have become an integral component of the Zero Suicide:
At first we had to help the system – or translate the benefits of the clinic to the system, but now it’s actually under a very – it’s under a concept that’s gaining more and more momentum, it’s quite a strong profile which is under the Zero Suicide Implementation Framework, so the clinic is actually on the new protocol for people who present with suicidal ideation, or intent, and so it’s actually part of the referral pathway and it’s considered as one of the innovations around zero suicide implementation, which is
fantastic. (Manager)
4.3.2 Ability to work to scope Introduction of the clinics enabled allied health staff to deliver therapies in keeping with discipline specific work. The Clinics provided an opportunity to engage in more intensive face to face work with clients which is not always possible in busy mental health services. The work in the clinic allowed allied health staff to refine current skills, develop new skills and acquire confidence in working in a clinic environment. Furthermore, the focus on short-term therapies was appealing as staff could observe rapid improvement in consumers which was rewarding for staff. Some also commented that they enjoyed working with consumers who were really motivated to change.
I really appreciate the ability to actually practice my profession as a psychologist that involves therapy, and so that was one key element that was exciting to me …. was that
opportunity (Clinic Clinician)
And….
I do enjoy the work and I was telling someone the other day that it’s really the most satisfying mental health work I’ve done in Queensland Health, and I’ve worked in
Queensland Health for nearly 20 years (Clinic Clinician)
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 58 of 86
Another positive factor for clinic staff was being able to devote uninterrupted time to each consumer. This enabled a greater depth of problem exploration and working to support consumers:
Having the time to just sit with somebody and to talk through what’s gone on for them and the difficulties that they’re facing, and what they'd like to be different about where
they are in their current situation. (Clinic Clinician)
And….
I think the clinic is a really wonderful opportunity for clinicians to be able to have the experience of working with people through a crisis and seeing them improve because
that's something that often when you're working in an acute care team you don't get to see because you see people when then they're at the height of their distress, and then usually they're referred on somewhere else. So with this service you get to travel with
people on that journey and see them improve, and I think that's good for our professional development as clinicians, but also good for our sense of wellbeing and the sense of our
work being meaningful and useful (Clinic Clinician).
It was identified that the AHBT Clinic approach could enable staff to gain skills in therapeutic interventions in a ‘safe’ environment. It was recognised that staff in other arms of the service were asking to have time in the Clinics:
In the last few months we’ve had requests from a few other staff working in other parts of the service to do sessions in the clinic because they see it as a way to develop their
therapeutic skills under guidance and under a structure where it’s focused on providing that treatment (Manager)
However, trying to balance the delivery of therapeutic interventions against service reporting key performance indicators and the prioritisation of assessment could be difficult:
I really struggled at times to keep the therapy focus, to keep the intervention focus working within a team that really prioritises assessment and all the documentation and
processes within the team are really focused on assessment. (Clinic Clinician)
4.3.3 Workload The clinicians did not believe that the clinic had greatly increased their workload in the ACT team. Some identified that the introduction of the Clinics did add some additional work around arranging appointments:
I wouldn’t say it had a big impact on the workload. Probably … in some ways it increased the workload a bit because of that to-ing and fro-ing and negotiating and booking
appointments and then re-ringing and that triple handling (Referring Clinician).
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 59 of 86
Others noted that the introduction of the Clinics took staff away from the Acute Care Teams. While this was considered useful in up-skilling staff, they felt that the provision of the Clinics requires separate resources (while remaining under ACT):
Well I actually think it can work really well within the existing service model. Even with the governance under ACT, I think that it actually can work and does work quite well… as long
as it is resourced and I think that’s the biggest issue. Resourcing it properly and not just simply taking ACT clinicians to fulfil the Clinics roster, because all you do is leave that short or the other problem could be that some services might pull people out of the Clinic to do it, so I think it needs to be a separate team within ACT that is actually staffed separately
and also resourced separately as well. (Referring Clinician)
Staff rotating into the clinics had varying views as to the impact of this on their substantive roles. For some it was seen as a trade-off for the opportunity to work to their clinical scope:
I don't think it creates any extra work for anyone except the person that is putting their hand up to say, “I want to come into this clinic to deliver this kind of work, because I want to increase my scope of practice as a clinician,” so they acknowledge what’s required to
do that. It takes it out of our service if we provide the bulk of those clinicians. (Clinic Clinician)
Whereas for others, it didn’t appear to have been that big of a concern:
I guess if management is supportive of it and willing to accommodate for it and accommodate our workloads with that, that would be great. At the same time I also feel
like it didn’t add a huge amount to my workload in that I only had one or two sessions available per week. If they are supporting it in that they can accommodate for us then
that’s great. (Clinic Clinician)
Managers from teams that had staff rotating into the clinic had more concerns about the impact on individual clinicians, overall team functioning and broader service delivery:
So for the clinicians who are providing services actually into the clinic, for them, I think it greatly increased their workload. So, yeah, it was an additional thing that they had to do, every week on top of the other tasks and duties that they have. Yes … so it's an additional
thing on top of. There isn’t any concession made for those staff to have reduced workloads in any other way or form within our service. Broader workload, that’s a little bit of a tricky one in that it is more just around where the workload actually sits. If have that nicely distributed a little bit off of multiple different teams, it's not such an issue. But if it
ends up being where the person has all of the staff come out of the one work area because they're doing it in addition to, the weight becomes really heavy. (Manager)
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 60 of 86
The allocation of KPI’s around the clinic was seen as one way of addressing this concern going forward:
Ultimately if it [Clinic] became a KPI, and it became a part of a service that the hospital and health service provides, and it's an expected, then resources are going to be supplied
and it would be much more effective. At the moment it is really run on a, almost like a clinician volunteer basis (Manager)
4.3.4 Improved Care Transitions When consumers had been assessed and treated in the AHBT Clinics, they were frequently referred by Clinic staff to an NGO provider for additional support. Having the Clinic co-located within the NGO service enabled a smooth transition of the consumer. In particular, there was a sense that communication between both providers was enhanced via a ‘warm handover’ process:
They do a referral form, they send it to us. But we also did have a really good warm, soft handover with referrals as well. So, if they were seeing a person that they were going to refer to us then they would often have a chat to the team and have a chat to my intake workers who would then meet with the person, even briefly, and go through the referral process that way. So that's how that happened…. it worked incredibly well. Especially
with the warm handover (Receiving Service)
And
I feel that it’s the difference between just referral and a warm handover. So you’re preparing the other side that you’re going to get a referral and then that agency is able to
just say we’ve got the referral, this is really good and the reason why you didn’t get it before is this, this and this but now you’ve sorted that out it’s actually really good and I’m
actually referring to a particular case I’m talking about where she couldn’t understand why she could never link in but there were things that she just wasn’t navigating it
properly and it only took a few minutes extra. We figured it out and that person was able to stand there and talk to the receptionist which she wouldn’t have been able to do a few
weeks beforehand. It was very empowering for them, I think. (Clinic Clinician)
The co-location of services also meant that both Health staff and NGO staff had a greater awareness of what services the consumer required and what services NGOs could provide. Having a better understanding of the consumer’s goals resulted in the timely provision of services to the consumer:
And the clinic [AHBT clinic staff] had a really good understanding of what we could provide to them. So, there was no unrealistic expectations set, which is fantastic as well.
And I found that it worked really well. We got a lot more information than what we do on some other referrals that we get from Q Health. And even on the ways that they were
working with the people, we had a good understanding of what the person's goals would be, so we could do our triage and intake a lot quicker. And wouldn't have to explore and
investigate as much, because the information was there, which I think was fantastic. (Receiving Service)

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 61 of 86
4.4 Summary This section of the Report considers the ‘impact’ of establishing the Clinics on consumers, staff and the services more broadly. A significant amount of data was collected in each of these 3 key areas while reaching a compromise between the burden placed on staff and consumers to collect data. While the collection of consumer related data (i.e. DASS, Suicidality, SRS and ORS) was used to provide a measure of Clinic effectiveness, it was used by the clinic clinicians in decision making around consumer progress and safety plans. It is now clear that these measures will be used by the Clinics going forward.
Consumers painted a positive picture of their experience of the Clinics in ‘free-hand’ comments provided through a satisfaction survey. These comments highlighted the positive relationship they had with the clinician in the Clinics and identified the importance of being respected and having their views validated. Seeing the same clinician at each session also helped to provide consistency and continuity for consumers. Over 90% of consumers indicated that they would ‘use the clinic again if they were experiencing similar issues’ while 91% indicated that they would ‘recommend the Clinic to a friend or family member’.
Staff feedback indicates that the Clinics provided them with an opportunity to engage in more intensive face to face work with clients which is not always possible in busy mental health services. Working in the clinic allowed allied health staff to refine current skills, develop new skills and acquire confidence in working in a clinic environment. Furthermore, the focus on short-term therapies was appealing as staff could observe rapid improvement in consumers which was rewarding for staff.
At the service level, the introduction of AHBT Clinics does not appear to duplicate existing services but complements existing service provision by addressing an important gap in services for those presenting with suicidality.

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 62 of 86
5 AHBT Clinic Outcome Findings
5.1 Patient safety One of the key outcomes of the AHBT Clinics was ensuring the safety of those consumers referred to the Clinics. Since the Clinics began in early 2019, none of the patients treated at the clinics went on to end their life through suicide. Information concerning other outcomes such as inpatient admissions and ED presentations is provided below.
5.1.1 Service Use: Pre-and post-AHBT Clinic One measure of Clinic effectiveness is the use of services following intervention by the AHBT Clinic. Data for the 3 months pre and post-intervention were compared to determine changes in the need for mental health services. It should be noted, we do not have data on access to services such as those provided by private sector (such as Psychologists, GPs, etc).
In the 3 months prior to the Clinic, 6 of the consumers had contact with the Co-responder Program on 6 occasions. None of those referred to the Clinic had contact with the Co-responder in the 3 months following (see Table below). The second outcome indicator examined contact with the emergency department. In the 3 months prior to the Clinic, 143 consumers had 177 presentations to an ED. This is compared to 26 presentations by 18 consumers in the 3 months following referral to the Clinic. A small number of 9 consumers had 9 admission (one admission each) to an inpatient unit at one of the 3 sites in the 3 months prior to the Clinics. In the 3 months that followed, 8 consumers had been admitted to an inpatient unit.
Table 27 Consumer Contacts with MH Services - 3 months pre and post Clinic Attendance
Service 3 months pre AHBT Clinic
Occasions of Service (People)
3 months post AHBT Clinic
Occasions of Service (People)
MH Co-Responder 6 (6) 0 (0)
Emergency Department 177 (143) 26 (18)
Inpatient Unit 9 (9) 9 (8)
5.1.2 Emergency presentations by Clinic Status The finding suggests that while the Clinic intervention was instrumental in reducing service utilisation for those who attended the clinic, those who disengaged or did not start were also less likely to use mental health services following their presentation to the ED. Whilst It was beyond the scope of this evaluation to further investigate these trends for the disengaged and did not start cohorts, it is possible that the crisis may have self resolved by the time of the first clinic appointment or during clinic attendance.
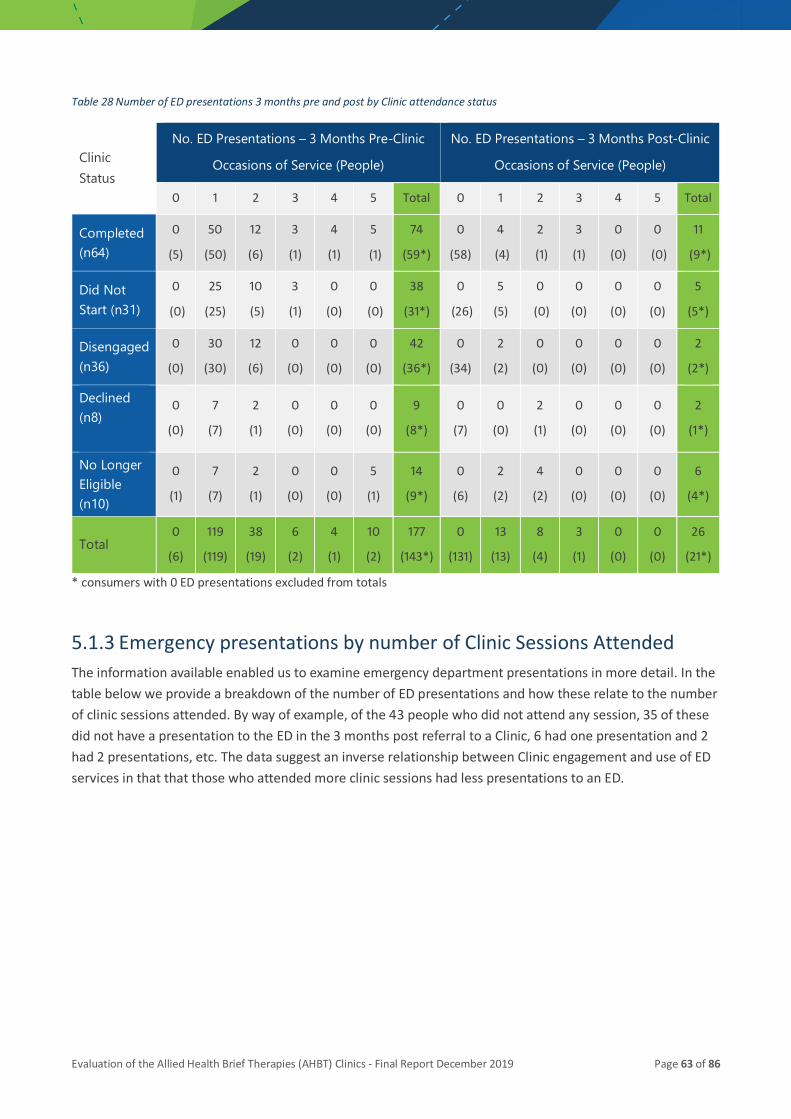
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 63 of 86
Table 28 Number of ED presentations 3 months pre and post by Clinic attendance status
Clinic Status
No. ED Presentations – 3 Months Pre-Clinic
Occasions of Service (People)
No. ED Presentations – 3 Months Post-Clinic
Occasions of Service (People)
0 1 2 3 4 5 Total 0 1 2 3 4 5 Total
Completed (n64)
0
(5)
50
(50)
12
(6)
3
(1)
4
(1)
5
(1)
74
(59*)
0
(58)
4
(4)
2
(1)
3
(1)
0
(0)
0
(0)
11
(9*)
Did Not Start (n31)
0
(0)
25
(25)
10
(5)
3
(1)
0
(0)
0
(0)
38
(31*)
0
(26)
5
(5)
0
(0)
0
(0)
0
(0)
0
(0)
5
(5*)
Disengaged (n36)
0
(0)
30
(30)
12
(6)
0
(0)
0
(0)
0
(0)
42
(36*)
0
(34)
2
(2)
0
(0)
0
(0)
0
(0)
0
(0)
2
(2*)
Declined (n8)
0
(0)
7
(7)
2
(1)
0
(0)
0
(0)
0
(0)
9
(8*)
0
(7)
0
(0)
2
(1)
0
(0)
0
(0)
0
(0)
2
(1*)
No Longer Eligible (n10)
0
(1)
7
(7)
2
(1)
0
(0)
0
(0)
5
(1)
14
(9*)
0
(6)
2
(2)
4
(2)
0
(0)
0
(0)
0
(0)
6
(4*)
Total 0
(6)
119
(119)
38
(19)
6
(2)
4
(1)
10
(2)
177
(143*)
0
(131)
13
(13)
8
(4)
3
(1)
0
(0)
0
(0)
26
(21*)
* consumers with 0 ED presentations excluded from totals
5.1.3 Emergency presentations by number of Clinic Sessions Attended The information available enabled us to examine emergency department presentations in more detail. In the table below we provide a breakdown of the number of ED presentations and how these relate to the number of clinic sessions attended. By way of example, of the 43 people who did not attend any session, 35 of these did not have a presentation to the ED in the 3 months post referral to a Clinic, 6 had one presentation and 2 had 2 presentations, etc. The data suggest an inverse relationship between Clinic engagement and use of ED services in that that those who attended more clinic sessions had less presentations to an ED.
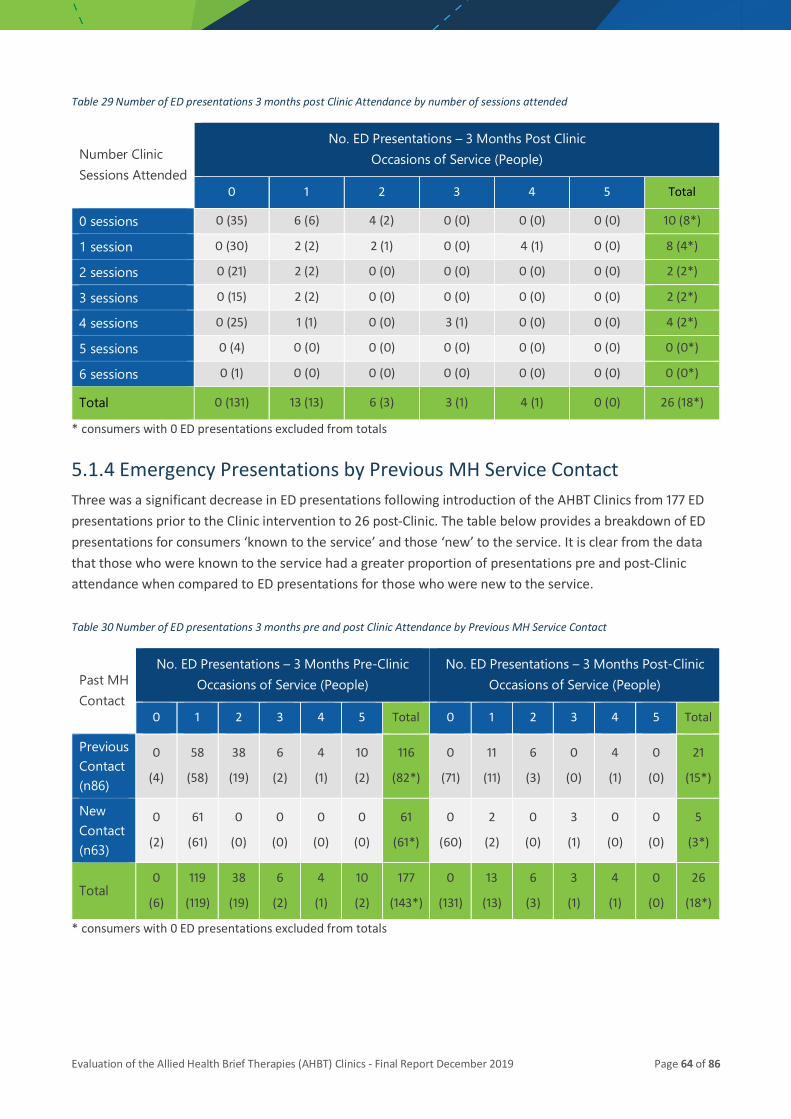
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 64 of 86
Table 29 Number of ED presentations 3 months post Clinic Attendance by number of sessions attended
Number Clinic Sessions Attended
No. ED Presentations – 3 Months Post Clinic Occasions of Service (People)
0 1 2 3 4 5 Total
0 sessions 0 (35) 6 (6) 4 (2) 0 (0) 0 (0) 0 (0) 10 (8*)
1 session 0 (30) 2 (2) 2 (1) 0 (0) 4 (1) 0 (0) 8 (4*)
2 sessions 0 (21) 2 (2) 0 (0) 0 (0) 0 (0) 0 (0) 2 (2*)
3 sessions 0 (15) 2 (2) 0 (0) 0 (0) 0 (0) 0 (0) 2 (2*)
4 sessions 0 (25) 1 (1) 0 (0) 3 (1) 0 (0) 0 (0) 4 (2*)
5 sessions 0 (4) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0*)
6 sessions 0 (1) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0*)
Total 0 (131) 13 (13) 6 (3) 3 (1) 4 (1) 0 (0) 26 (18*)
* consumers with 0 ED presentations excluded from totals
5.1.4 Emergency Presentations by Previous MH Service Contact Three was a significant decrease in ED presentations following introduction of the AHBT Clinics from 177 ED presentations prior to the Clinic intervention to 26 post-Clinic. The table below provides a breakdown of ED presentations for consumers ‘known to the service’ and those ‘new’ to the service. It is clear from the data that those who were known to the service had a greater proportion of presentations pre and post-Clinic attendance when compared to ED presentations for those who were new to the service.
Table 30 Number of ED presentations 3 months pre and post Clinic Attendance by Previous MH Service Contact
Past MH Contact
No. ED Presentations – 3 Months Pre-Clinic Occasions of Service (People)
No. ED Presentations – 3 Months Post-Clinic Occasions of Service (People)
0 1 2 3 4 5 Total 0 1 2 3 4 5 Total
Previous Contact (n86)
0
(4)
58
(58)
38
(19)
6
(2)
4
(1)
10
(2)
116
(82*)
0
(71)
11
(11)
6
(3)
0
(0)
4
(1)
0
(0)
21
(15*)
New Contact (n63)
0
(2)
61
(61)
0
(0)
0
(0)
0
(0)
0
(0)
61
(61*)
0
(60)
2
(2)
0
(0)
3
(1)
0
(0)
0
(0)
5
(3*)
Total 0
(6)
119
(119)
38
(19)
6
(2)
4
(1)
10
(2)
177
(143*)
0
(131)
13
(13)
6
(3)
3
(1)
4
(1)
0
(0)
26
(18*)
* consumers with 0 ED presentations excluded from totals
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 65 of 86
5.2 Staff perceptions of Clinic outcomes
5.2.1 The role of the Clinic Many of those interviewed (managers and clinic staff) identified that the primary role of the clinic was providing support and therapy to keep consumers safe during their time of crisis. Most importantly, this support could be provided immediately and seemed to address the issue of assessing people and referring them on to another service:
What works well from my perspective is that it, I think, fills a gap for consumers who need help straight away. And by help I mean therapy, crisis support, rather than just repeated
assessment (Refering Clinician)
However, staff identified that the Clinics were not for all patients presenting with suicidality. They recognised that the support provided through the Clinic, while brief, was sufficient for many consumers who require one or two sessions to support them through their time of crisis:
So, there are a massive amount of people that go back out and don't have access to anyone if they don't follow through with the recommendations, which they probably
wouldn’t and that takes time as well. So, I think whilst this might not capture all of those people, I think it would help with the high end ones that actually just want one session or just a contact with somebody or something that’s affirming and, yeah, provides that hope
and just eases that process more. (Clinic Clinician)
Many of the staff interviewed felt that the Clinics were an important adjunct to the Zero Suicide pathway. They noted that the presence of the Clinics provided mental health staff (working in the ED) with an avenue to refer at risk consumers to the Clinics:
I do think that that’s a good idea, because one of the limitations with the [Zero Suicide] pathway was that there wasn’t any resources to refer people to, and so by doing that it actually really filled that gap that that was lacking. It was actually where am I going to
refer someone to, and because it’s only brief, I just thought it was perfect, a perfect match. (Referring Clinician)
Many staff saw the Clinics as providing another option for those presenting to the ED with suicidality. However, the capacity of mental health staff in the ED to be able to offer consumers an immediate appointment was considered a key factor in the success of the Clinics. Staff felt that the fact that consumers left the ED knowing that they could get to see a mental health professional on a one-to-one basis within a day or so was instrumental in keeping them safe:

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 66 of 86
If a person is suicidal, they just need another option, and if you can provide them that and that’s why I think the ED providing an appointment is such an important part of that
because then they have a goal, they at least can see an option or a light at the end of the tunnel. It may not fix everything, but at least it gives them another 24 hours for them to settle down a little bit, and I think that’s why the results are going to be so good. It gives
them another option without undergoing intense long-term therapies because most people don’t need that, they just need one or two counselling sessions to get them over the crisis and get them back on track and link them in with other services. That’s why I
think this is so useful and is probably one of the most effective interventions that we can offer in Health. (Clinic Clinician)
There was overwhelming support for the clinic approach and all of those interviewed (managers, ACT and clinic staff) felt that the Clinics should continue. There was a perception that while the Clinics required additional time and input from staff, they were instrumental in meeting the needs of those more severe problems to remain safe and connected to the service.
It is a really good service and we’re really actually meeting some people’s needs who would have otherwise been in awful situations. They would have represented. They
would have gone through difficult situations. This has actually been for some very, very seriously compromised clients that we’ve taken through the clinic. So from my perspective I’m very enthusiastic that it would continue. I think it’s worth all the extra work because
it’s a really good way to go. Seamless service provision. That’s it. (Manager)
5.2.2 Referrals Good referral criteria and explanation to the consumers about the purpose of the clinic was also important. Similarly, it was critical to ensure that people were committed to the process or were able to engage in therapy as for some consumers their lives maybe too chaotic:
What isn’t good is when someone just hasn’t got a commitment in the first place. So perhaps that comes down to possibly not a sufficiently placed or appropriately placed
referral. They just were not ready yet or their life is too scattered for this and I don’t know that another referral would have suited their needs either. Their life was too chaotic.
(Clinic Clinician)
The clinicians also noted that the referrals from ACT were very appropriate and that the interventions provided through the clinics were able to have a positive impact:
I’ve had a few really nice situations where I’ve felt like it was absolutely a brilliant referral, like the referral suited the need and that the outcome was good. That’s very, very
pleasing. It’s very empowering and you watch that person go from that situation to in four weeks they’re really getting settled into a track. They’re getting to navigate a track
that will set them up for success (Clinic Clinician)

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 67 of 86
The co-location of services provided health staff with a better understanding of the services offered through the NGO sector. While this resulted in more referrals to the NGO, the referrals seemed to be more appropriate for their service:
From our perspective, I suppose it's opened doors for people that may not have had the opportunity or known what we do and who we are. And I suppose – so in a way I think it
increased our workload I suppose a little bit, in that we were getting, but at the same time they were appropriate referrals. So, while it may have increased people coming through the doors, they are a lot more appropriate than, say, some other ones that were coming
through at that time. I think in terms of having that warm handover, once again, enhanced the transition over from their clinic [AHBTC) to our service, to have that
continuity of care coming through as well. I think that was an incredible big positive. (Receiving Service)
One of the issues for clinic staff was the difficulty of finding the right support after the clinic sessions had been completed. It was critical to start looking for referral pathways at the start of the therapy as many clients stated that they had a GP or were linked in with a psychologist this was not always the case.
I would normally negotiate with the consumer what their needs were, what their support preferences were. And if we were able identify an appropriate service that they were
happy with, then I would usually do like a verbal handover to the receiving service, often by phone. But it really depended on which service they were going to. If they were going
to a private psychologist I would usually do a verbal handover and that worked well on most occasions. (Clinic Clinician)
And….
One of them [consumer] continued onto a private psychologist that they had seen before, it’s just they had to wait to see them. And the other was happy just to get referred back to GP although, I mean, I pushed more for continuing to see at least somebody, but he
was happy with what he had received already (Clinic Clinician)
5.2.3 Clinic- positive for consumers There was a perception that the Clinics had a positive impact on consumer outcomes in that the Clinics provided a more personalised intervention. This was perceived to assist consumers to better manage their distress and prevent the need for consumers to return to the service again for support:
If you track the consumer journey pre the allied health clinic, those consumers would have either ended up returning because there wasn’t a successful referral out to another
service, or they would have been referred into a team that most likely wouldn’t have had the capacity to work with them and provide intervention when they needed it. So, from
that instance, yes… it works (Manager)
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 68 of 86
The immediate response to consumers at risk was considered a key component of the clinics and a major improvement on usual service provision:
They [consumers] didn’t need to wait for four weeks and they actually had somewhere to go, rather than just being given this magical off you go to your GP and you’ll get a mental
health care plan. So, yes, I think that they definitely had that. (Clinic Clinician)
It was also noted that the AHBT clinic model offered something more than assessment. The clinician participants identified that while risk assessment was important and was considered, they were also able to focus on providing therapy and moving away from the ‘assess and refer’ mentality:
I also think that it was an opportunity for them [consumers] to experience interventions from a different perspective; so rather than risk, whilst that was something, we obviously
were aware of and assessed, but it wasn’t mainstream diagnosis (Clinic Clinician)
The ACT clinicians referring to the Clinic felt that the Clinics provided consumers with an opportunity to learn new skills to cope with future crises. As such, there was a perception that the therapy provided through the Clinics was instrumental in breaking the cycle of having one crisis after another:
And there's a lot of opportunities for that consumer to not have to re-present later. That they can learn those skills there and then while they're motivated, while the captured
audience. […] If he crisis is gone…they’ve left it behind. They don’t want to know about it and go on until the next crisis happens. And then they're in the same place again. So
yeah… I think when you're looking at a purely clinical perspective for them, it's providing a service that’s going to give them tools at the time that they need it. Not six weeks down
the track on a waiting list (Referring Clinician)
However, they felt that the best time to provide the intervention was soon after the crisis as consumers were less motivated to engage when the crisis has passed:
I think it fits in, because early intervention, preventing that cycle of self-harm, self-abuse, suicidality and getting the person to see what sort of changes they need to make,
encouraging them to make those changes, but also that therapy is not so confronting when you started off immediately from the discharge because they’re ready for change at that point in time. […] Yes. Rather than just telling them to go out and get a GP referral to mental health here, we can actually make an appointment for them. (Referring Clinician)
5.2.4 Variety of Approaches It was important for clinicians to utilise their clinical judgement, have an eclectic approach in delivering therapies and to focus on the issues the person would bring to the session:
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 69 of 86
My approach and certainly what I heard from other clinicians is that we were flexible in our approach, so if we started out doing solution-focused therapy and that really didn't
seem to be a good fit then we would be flexible and try another approach. So maybe motivational interviewing or teaching some skills from DBT or CBT to try and be
responsive to client need. So people responded well and in part I think that's because we were being flexible (Clinic Clinician)
And…..
We used a variety of models. I think we were open about offering them a wide range of models of therapy, but I have to say that it was, at times, quite useful, at times quite challenging; I’ve got to get things done really fast and quick, and I don’t have time to
discuss everything, so I think it was just even helping them to know that I’ve got to get something out of these four sessions (Clinic Clinician)
5.2.5 Enhanced Cross Sector Working Relationships The NGO service identified a number of factors that may enhance working relationship between the Clinic staff and the NGO staff.
Definitely a continuation of a good partnership with us and with them. And then just having them [Clinic] here on a daily basis and being able to talk to clinicians has been
really good. I think having open communication around referrals is another really important thing. Being able to have that open communication between the two services
and what we do, what we don't do, and things like that. (Receiving Service)
The NGO service was happy to have the AHBT Clinics co-located within their service and was hoping that the current arrangement could continue. There was a perception that the new arrangement enhanced the delivery of therapy as the NGO service was less clinical:
Like I said, I think it's a really good project. I do definitely hope to see it continue. And we've really enjoyed having them working out of the centre. I think that's just such a nice way of combining Queensland Health with a community NGO. And I think it's been good for the people that have here as well, because the feeling here in our service is quite nice.
It's not as clinical as others. So, they can feel a little bit more comfortable, which hopefully the clinicians are recognising that as well, that their people are recognising any
benefits from having that feeling as well. (Receiving Service)
5.3 Summary In relation to outcomes, we have strong evidence to suggest that the AHBT clinic model addresses an important gap in current service provision for those presenting with suicidality. Both staff and consumers felt that the clinics were beneficial in assisting consumers to manage their current stress and in providing them with the skills to better manage future crises. Moreover, the clinic model reduces the need for emergency department visits and improves consumer satisfaction with services.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 70 of 86
6 Discussion The findings reported here represent the culmination of several pieces of work designed to assess the efficacy of providing Allied Health Brief Therapy Clinics. The combination of rich qualitative data from interviews with staff, survey data from consumers, standardised consumer assessments and service utilisation enabled us to evaluate the study objectives which included:
1. Examine the implementation of the AHBT Clinic Model of Service (MoS) at each of the three sites to determine feasibility of implementation, adherence to the MoS and scalability.
2. Examine the impact of the clinics on consumer presenting problems and satisfaction levels
3. Examine the impact on clinicians involved in the clinics in relation to:
• providing referrals to the clinic
• providing interventions within the clinic
• receipt of referrals from the clinic post intervention
4. Examine the impact of the clinic on mental health services at each of the three sites
5. Examine the outcomes for consumers post-clinic intervention in terms of contact with and use of mental health services.
6.1 AHBT Clinic Implementation, Feasibility & Scalability After considerable discussion and negotiation over about 12 months, AHBT Clinics were established in each of the 3 health services. The ‘roll-out’ of the Clinics at each site was driven by a Model of Service document which provided guidelines for the establishment and operation of the clinics. While it was initially planned to have the clinics located within local GP clinics, this proved too difficult and costly (for room rent). As such, two of the Clinics were located with the ‘Floresco’ service and one at a Community Health Centre. Being located within Floresco meant that consumers with social and non-clinical concerns could be linked into the services offered through Floresco. Other options could include locating the clinics within GP practices. This would place AHBT Clinics within the primary care sector, with improved access to GP services and access to ongoing care through a mental health plan (via the Better Access program). Previous research has demonstrated that people with mental health issues prefer to receive services from GP practices due to the stigma associated with mental health services (Meehan et al. 2013). Linkages with emerging service delivery initiatives and models should also be considered (for example, Safe Haven Cafes).
In selecting partner or ‘co location’ sites, both the physical location and available infrastructure to effectively and efficiently operate the clinics need to be taken into consideration (Myers, Breuer, Lund, Petersen Williams, van der Westhuizen, Brooke – Summer, Naledi, Stein & Sorsdahl, 2019). Clinic sites must support both consumer attendance (e.g. good transport links, availability of parking, easy to locate within building) and clinician delivery of therapeutic interventions (comfortable, private office space, reception and waiting room facilities, travel time / modality from substantive base and access to IT and other clinical information systems).
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 71 of 86
The clinics at all 3 sites are managed on a daily basis through the local Acute Care Team (ACT). Consumers would, in the absence of the Clinics, be most likely referred to ACT. As such, ensuring the Clinics remain a component of ACT makes for a more coordinated approach to treatment provision. Indeed, findings from the interviews with Clinic staff identified that the integration of the AHBT Clinics within local Acute Care Teams (ACT) was a major strength of the service model. Clinic staff felt that they were part of a ‘team’ and not solely responsible for the consumers treated in the Clinics. This integration enabled the clinic clinicians to receive support and practical assistance when issues emerged with the clients. They felt that having ACT involved provided a safety net when they had concerns about consumers. It was also noted that the transfer of consumers in to the Clinics and from the Clinics back to ACT was facilitated through the integration of the Clinics with ACT.
More than three-quarters of the consumers referred to the Clinics (75.9%) were seen within 72 hours. However, there was variation within clinics in this respect with a range of 56.2% at Site 2 to 86.7% at Site 3. The variation arises from the availability of staff at some clinics. It should also be noted that there were no additional staff provided at the 3 services to support the Clinics and the staffing of the Clinics is mostly from within ACT. As such, some sites had difficulty rostering staff to the Clinics in the initial stages of implementation
For right care to be delivered, clinicians require both capacity and confidence in delivering therapeutic interventions. AHBT clinicians were supported in this regard through the provision of targeted professional development and training in brief interventions and suicide risk management. A program of ongoing clinical supervision is being provided to assist staff in translating learnings into practice. Finally, the Service Managers at each site noted the difficulty of relieving staff for training and then providing services through the Clinics. Having sufficient staff trained and willing to work in the Clinics was also an issue for Managers. The level of training and support required to establish such Clinics should not be underestimated and needs to be considered by those intending to replicate the introduction of Allied Health Clinics.
6.2 Impact Consumer Presenting Problems & Satisfaction Over the 6-month trial, 149 consumers were referred to one of the AHBT Clinics. Of these 106 attended at least one session and 64 (43%) completed all planned / agreed sessions (typically 4 sessions). However, 36 consumers (24.2%) attended some sessions but disengaged prior to completion of all planned sessions. Another one-fifth (20.8%) did not attend the initial session that was booked for them. While the rates of ‘no show’ and disengagement seem high, they are in keeping with similar studies overseas. In a similar initiative in Ireland, Surgenor and colleagues (2016) found that up to half of the referred clients with suicidality failed to present at the clinic despite having made an appointment to do so. Other studies suggest that anywhere from 30% to 60% of all clients drop out of treatment following initial engagement (Garfield, 1994; Swift and Greenberg, 2012). The main reason cited by participants in these studies for not presenting and disengagement following the initial session is that they had progressed beyond their suicidal crisis and were reluctant to revisit that aspect of their life. Other studies found that those who refused treatment or disengaged gave circumstantial reasons, such as work commitments and lack of child care (Gysin-Maillart et al. 2016).
We have matched data for 45 consumers who completed all sessions as agreed by the clinician and the consumer. The improvement in functioning was statistically significant with large effect sizes (Depression = 1.06, Anxiety = 0.82, and Stress 0.91). The extent of improvement in these domains for consumers accessing
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 72 of 86
the AHBT Clinics is similar to that achieved by more extensive interventions such as MHNIP, ATAPS and ATAPS-SP. This is despite consumers attending the AHBT Clinics having higher scores on the depression subscale at baseline. Moreover, the number of sessions offered through the AHBT Clinics was considerably less than the number of sessions offered in these other suicide prevention programs.
With around 4 sessions, the therapy provided through the AHBT clinics is considerably shorter than other programs for individuals who have attempted suicide. An exception is the study by Fleischmann and colleagues (2008) in which individuals who had attempted suicide were offered a single session of psychoeducation. However, this was supplemented with regular outreach contact after discharge including phone calls, home visits, etc. In their study, Surgoner and colleagues (2015) sent consumers a text message two weeks after therapy to serve as a brief reminder that the service was available if required. Four weeks after therapy they received a letter and information about local support services that they may find useful in dealing with more specific stressors (e.g., relationship or financial issues). The final contact was six weeks after therapy concluded and was in the form of a telephone call to check on the consumer’s progress and suicidal ideation. It has been noted that this ‘aftercare’, when based on a therapeutic relationship, is likely to decrease suicide risk (Hepp, Wittman, Schnyder & Michel, 2004). In the present study, clinic clinicians did not provide aftercare contact. However, it should be noted that consumers requiring ongoing support were referred to other supports such as their GP or NGO service. Given the research evidence for outreach contact, it is suggested that the leadership group for the ongoing development of the Allied Health Brief Therapies Clinics consider the provision of this additional support.
Therapeutic alliance is an important factor as it tends to be a consistent predictor of outcome form psychotherapy (Hovarth, Del Re, Flückiger & Symonds, 2011). In the present study, there were high ratings of therapeutic alliance (average 8.5 / 10) as assessed by the consumers using the Session Rating Scale. The findings indicate that all subscale scores and the total score were statistically higher (indicating improved alliance) at follow up. While the SRS scores for those new to the service were statistically significant between baseline and follow up (p=0.002), those for repeat presentations did not reach significance (p = 0.167). The finding indicates that those new to the service were significantly more likely to rate the alliance between themselves and their clinician as being higher at follow up than those with previous contact with the service. It is possible that those with previous contact did not have a good experience with support following their previous presentations to the service. This is likely to have had a negative impact on their perceptions of the Clinics. (Black Dog Institute, 2015).
A small group of consumers disengaged prior to completion of treatment. It should be noted that the baseline scores for those who disengaged and those who remained in treatment were not significantly different on depression (p = 0.88), anxiety (p = 0.33) and stress (p =0.88). However, follow up data for those who disengaged (who had two completed measures) showed lower effect sizes at follow up than those who remained in treatment. This goes some way towards supporting the effectiveness of the Clinics and “a dose-response effect” whereby more sessions equate to greater improvement.
It was noted that those who did not present to the Clinic for treatment or who disengaged prior to completion of treatment did not seem to have a greater number of ED presentations in the 3-month follow up period. For example, 6 of the 64 consumers that completed treatment (9.3%) had presentations to ED post clinic. This is compared to 14.1% of those who did ‘not show’ or disengaged prior to completion of treatment had a presentation to the ED. The finding indicates that while the Clinic intervention was instrumental in reducing service utilisation for those who attended the clinic, those who did not attend were also less likely to use mental health services following their presentation to the ED. While the reasons for this
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 73 of 86
are unclear, it is possible that the issue that brought the consumer to the ED in the first place may have been resolved between the time they were assessed in the ED and their initial appointment in the Clinic. As such, these individuals would not need to represent to the ED despite having minimal or no contact with a Clinic. Indeed, it is possible that the needs of those who are less likely to attend a Clinic are best met through brief follow up contact such as telephone calls, voice messages, text messages, etc. Future research should explore more fully the reasons for disengagement and how the needs of this group can be effectively addressed.
6.3 Impact on Clinicians Clinicians interviewed in all three sites expressed great enthusiasm for the AHBT Clinics. All believed that the clinic filled an important gap in current service provision and that the clinics were instrumental in supporting consumers to better manage their distress and maintain their safety. A key factor noted by staff was the capacity of the Clinics to provide prompt treatment to individuals in crisis. All of those interviewed were of the belief that the Clinics filled an important gap in current service provision.
The State-wide Mental Health Allied Health Scope of Practice Project recommended trialling alternate service delivery models where allied health professionals could have opportunity to practice at their full scope. Introduction of the AHBT clinics appears to meet this objective. Working in the Clinics has enabled allied health staff to refine current skills, develop new skills and acquire confidence in working in a clinic environment. Being able to deliver personalised therapies in a clinic environment allows allied health staff to work towards full scope of their practice.
While the Clinic staff were initially restricted to those from Allied Health backgrounds, it is worth considering staff from other disciplines such as medicine and nursing. This is likely to provide a larger pool of staff within each health service to work in the Clinics going forward. Moreover, clinic exposure is likely to increase skill and confidence in providing therapeutic interventions similar to the experience of allied health staff described in this study. Indeed, the recent Productivity Commission Report (2019) recommends that “the number of mental health nurses practicing in Australia — in GP clinics, community health services, and aged care facilities — should be significantly increased.”
6.4 Impact on Mental health Services The findings from the evaluation indicate the introduction of AHBT Clinics does not appear to duplicate existing services but complements service provision by addressing an important gap in the services for those with suicidality. The AHBT Clinic model provides prompt treatment and support to people at the time of their greatest need and ensures safe transition from one service provider to the next. For example, those who meet criteria for the Better Access Program may be referred to a GP to receive additional treatment through a ‘mental health plan’. As such, AHBT Clinics could be considered an ‘add-on’ service component that links service provision across acute care mental health (ACT) teams, primary care and general practice, private sector specialist services and non-government organisations.
The introduction of the clinics is likely to benefit mental health services. As outlined above, clinic exposure has enabled allied health staff to refine current skills, develop new skills and acquire confidence in delivering therapeutic interventions in a clinic environment. It is likely that staff will rotate through the clinics, bringing with them the new skills that they have acquired. As such, the Clinics are likely to act as a training

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 74 of 86
environment for mental health staff, thereby increasing the pool of staff with advanced therapeutic skills within each service.
6.5 Limitations The present evaluation followed a single group pre/post-test design which has a number of known limitations. In the absence of a control group, one cannot be completely confident that the clinic interventions resulted in the positive changes observed. A randomised controlled trial (RCT) was contemplated for this evaluation but this was not feasible as staff would have to select and manage treatment and control consumers and focus on establishing the Clinics. Given that the clinics have now been established, an RCT may be feasible and should be considered. However, this would involve denying some consumers of the therapy programme provided through the Clinics (i.e. those in the control group). This runs contrary to the principle of beneficence as outlined in ethical guidelines and it may prove difficult to have an RCT approved by an ethics committee.
It is possible that some of the consumers in our sample commenced antidepressant medication following their initial assessment in the ED. This may have had a positive impact on consumer depression levels at follow up. Future research should consider the impact of antidepressant medication on consumer outcomes. Finally, it would be useful to have some record of suicide attempts pre and post intervention as this would provide a measure of suicide risk and the impact of the clinic on suicide attempts following intervention. While the effect sizes for some of the variables are large, small sample sizes can act to increase effect sizes.
Missing data on some of the measures caused by consumers disengaging from treatment and others lost to follow up is a common problem in longitudinal studies. We considered using the Last Observation Carried Forward (LOCF) method as this allows the researcher to impute results for missing observations / data. While this provides a larger and more ‘complete’ data set, it tends to underestimate the variability of results, in this case the DASS scores. The difficulty of obtaining complete data sets in in-vivo studies such as the one reported here needs to be considered in future evaluations.
Despite these limitations, we believe this study provides useful insights into the provision of aftercare for those presenting to ED with suicidality.
6.6 Conclusions A recent report by the Centre for Research Excellence in Suicide Prevention (2014) concluded that “failure to provide follow-up care after suicide attempts is associated with increased risk of re-attempt and death by suicide” (p.2). The introduction of Allied Health Brief Clinics goes some way towards addressing this concern around aftercare. The Clinic model is based on existing evidence, fulfils an identified gap in current service provision and enables a range of therapeutic approaches based on consumer needs. For consumers (and carers), the provision of appropriate, evidence-based care results in better care outcomes and higher levels of satisfaction with the mental health system.
Findings from the evaluation indicate the introduction of AHBT Clinics does not duplicate existing services but complements service provision by addressing an important gap in current services for those presenting with suicidality. The AHBT Clinic model provides prompt treatment and support for people at the time of their greatest need and ensures safe transition from one service provider to the next. This approach supports the current roll-out of the Zero Suicide Framework.

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 75 of 86
Delivering the right care to consumers, their families and carers at the initial contact point or crisis also benefits the system through potential reduction in future use of limited system resources (such as ED and mental health services). Our findings point to a significant reduction in ED usage following Clinic intervention. This enables the system greater flexibility and capacity to meet other competing demands.
The AHBT Clinics are positioned to enhance communication, clinical management pathways and service linkages. Within each HHS, the Clinics have been integrated with existing service and clinical governance structures to optimise consumer transition between ED, mental health and alcohol and other drug service components.
Co-location of the AHBT Clinics at the public and community mental health sector interface and in-kind contributions (public health clinicians and community physical space) from both partners demonstrates commitment to an innovative way of working collaboratively across the system and provides clinicians and consumers with efficient, effective and appropriate referral pathways.
The immediacy of care provided to consumers through AHBT Clinics ensures that consumers are supported during their highest period of risk. Addressing the initial suicidal ideation or crisis within 3 business days of referral serves to keep consumers actively engaged, reducing the potential for further escalation. The current program with 3-4 sessions of aftercare is considered brief when compared to similar programs described in the literature. However, there is evidence that the provision of minimal outreach interventions after therapy has been completed could enhance brief therapy interventions. This outreach includes contacting patients with regular text messages, or standardized letters. It is suggested that strategies are developed that would allow clinic clinicians to be able to follow up their consumers following clinic treatment.
Feedback from staff suggests that provision of timely, accessible, evidence based therapeutic interventions through the AHBT Clinics:
• validates the consumer as a person, thereby reducing stigma
• enables collaborative engagement between consumer and clinician to address the immediate crisis
• provides consumers with skills and techniques to better manage similar situations in the future
• instils hope that continued recovery is achievable through ongoing engagement with suitable support services
Finally, in addition to better meeting consumer needs, the Clinics assist allied health staff to practice to full scope. Working in the clinics has enabled allied health staff to refine current skills, develop new skills and acquire confidence in delivering therapeutic interventions in a clinic environment. It is likely that staff will rotate through the clinics, bringing with them the new skills that they have acquired. As such, the Clinics are likely to act as a training environment for mental health staff, thereby increasing the pool of staff with advanced skills within each service.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 76 of 86
7 Recommendations
7.1 Continue to embed Clinics within existing and emerging service models
Findings from the evaluation indicate that the introduction of AHBT Clinics does not duplicate existing services but complements current service provision by addressing a gap in services for those presenting with suicidality. The AHBT Clinic model provides prompt treatment and support for people at the time of their greatest need and ensures safe transition from one service provider to the next. Moreover, the position of the clinics within current service provision supports the implementation of the Zero Suicide Framework. As such, it is recommended that service managers explore options to further integrate the clinics into existing service models as well as emerging service delivery initiatives. This is likely to require some consideration of the endorsed AHBT Clinic Model of Service (MoS) and localised operational and governance frameworks, how the clinics will be funded as well as physical location and accessibility (for both consumers and clinical staff).
7.2 Ensure Clinic infrastructure supports efficient and effective service delivery
A key component to the successful implementation of the Clinics is availability of and access to infrastructure that supports therapeutic service delivery. It is recommended that co located Clinics have sufficient access to appropriate physical, human and communication / information system resourcing and infrastructure.
7.3 Expand the workforce providing therapy in the Clinics It is recommended that service managers consider recruiting other mental health professionals (in addition to Allied Health) to work in the Clinics such as mental health nurses, psychiatric trainees, etc. In addition to providing a larger pool of staff available to work in the Clinics, clinic exposure is likely to increase staff skill and confidence in providing therapeutic interventions (similar to the experience of allied health staff described in this study).
7.4 Streamline consumer referrals to Clinics One of the advantages of the Clinic model is access to prompt treatment for those at risk. It is noted that the services in our study have taken different approaches to providing access to the Clinics – some provide direct access from the ED while others refer consumers to the Acute Care Team for review and subsequent referral to the Clinic (based on assessment by ACT). While different approaches arise from local service requirements, it is recommended that services continue to review their procedures so that consumer access to the Clinic is as efficient and prompt as it can be.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 77 of 86
7.5 Provide brief ‘aftercare’ interventions It is recommended that services consider supplementing the current Clinic sessions with outreach contact after discharge. This can include phone calls, voice messages, text messages, and possibly home visits, etc. It has been noted in previous research that this type of follow-up ‘aftercare’ can decrease suicide risk. Where possible, this follow-up should be carried out by the clinician who treated the consumer in the Clinic.
7.6 Ensure ongoing training for staff It was noted in interviews with clinic clinicians that they valued the additional training provided to increase their confidence in working in a clinic environment. In the present project, the AHBT clinicians were supported in this regard through the provision of targeted professional development and training in brief interventions and suicide risk management. A program of ongoing clinical supervision was also provided to assist staff in translating learning into practice. Services will need to consider the level of training and support required by new staff who wish to work in the Clinics.
7.7 Conduct more comprehensive evaluation The present evaluation followed a single group pre/post-test design which has a number of known limitations. Given that the Clinics are now established and the process for care delivery refined, a more comprehensive evaluation of the initiative should be considered. While an RCT may be feasible, it would involve denying some consumers access to the Clinics for the sake of the evaluation (i.e. those in the control group). Moreover, a future evaluation should consider the inclusion of an economic evaluation to determine the cost-effectiveness of the Clinic model. This and a range of other issues would need to be considered in developing a more comprehensive evaluation.

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 78 of 86
8 References Australian Bureau of Statistics. (2015). Causes of Death Australia 2013. Australian Bureau of Statistics: Canberra.
Australian Government Productivity Commission. (2019). Mental Health Draft Reports 1 & 2. Productivity Commission; Canberra.
Barrett, R. (2019). Patients’ and healthcare professionals’ experiences and perceptions of physiotherapy services in the emergency department: a qualitative systematic review. Physiotherapy, 105(S1), e134.
Berg, B. (2009). Qualitative Research Methods for the Social Sciences, 7th Ed. Allyn & Bacon. Boston, Mass.
Black Dog Institute (2015) Care after a Suicide Attempt: A report prepared for the National Mental Health Commission by the Centre for Research Excellence in Suicide Prevention; University of NSW. Sydney.
Australian Government Department of Health. (2009) Suicidality. Downloaded from: https://www1.health.gov.au/internet/publications/publishing.nsf/Content/mental-pubs-m-mhaust2-toc~mental-pubs-m-mhaust2-hig~mental-pubs-m-mhaust2-hig-sui 22 Oct 2019.
Australian Institute of Health and Welfare (AIHW). (2019). Mental Health Services in Australia. Australian Institute of Health and Welfare. Canberra.
Bassilios, B., Nicholas, A., Reifels, L., Machlin, A., Ftanou, M., King, K., Fletcher, J., Blashki, G., Burgess, P., & Pirkis, J. (2013). Evaluating the Access to Allied Psychological Services (ATAPS) Program: Ten-year consolidated ATAPS evaluation report. Centre for Mental Health, University of Melbourne. Melbourne.
Beautrais, A.L., Gibb, S.J., Faulkner, A., Fergusson, D.M., & Mulder, R.T. (2010). Postcard intervention for repeat self harm: randomised controlled trial. British Journal of Psychiatry, 197(1), 55-60.
Beautrais, A.L. (2014). Intervening to prevent suicide. Lancet Psychiatry; 1:165-166.
Brown, G.K., & Jager-Hyman, S. (2014). Evidence based psychotherapies for suicide prevention: future directions. American Journal of Preventive Medicine, 47(3S2), S186-S194.
Brown, L.A., Wiley, J.F., Wolitzky – Taylor, K., Roy – Byrne, P., Sherbourne, C., Stein, M.B., Sullivan, G., Rose, R.D., Bystritsky, A., & Craske, M.G. (2014). Changes in self efficacy and outcome expectancy as predictors of anxiryu outcomes from the CALm Study. Depression and Anxiety, 31(*), 678-689.
Brown, G.K., Ten Have, T., Henriques, G.R., Xie, S.X., Hollander, J.E., & Beck, A.T. (2005). Cognitive therapy for the prevention of suicide attempts: a randomized controlled trial. JAMA. 294:563-570.
Bugeja, L., Milner, A., & Pirkis, J (2015). Identification and analysis of health service use and pathways to health service contact amongst persons who died from suicide in Victoria, 2009-2010: Final Report. Beyond Blue: Melbourne.

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 79 of 86
Campbell, A., & Hemsley, S. (2011). Outcome Rating Scale and Session Rating Scale in psychological practice: clinical utility of ultra brief measures. Clinical Psychologist, 13(1), 1-9.
Carter, G.L., Clover, K., Whyte, I.M., Dawson, A.H., & D'Este, C. (2013). Postcards from the Edge: 5-year outcomes of a randomised controlled trial for hospital-treated self-poisoning. British Journal of Psychiatry. 2013;202:372-380
Casey, M. (2015). Agile psychologists designing and delivering change in adult public mental health. InPsych. Available: www.psychology.org.au/inpsych/2015/april/casey
Cedergren, C. (2012). The Effectiveness of the Patient Health Questionnaire 9 cross cultures. All Theses, Dissertations, and Other Capstone projects. 549. https://cornerstone.lib.mnsu.edu/etds/549
Deady, M., Ross, J., & Darke, S. (2015). Suicide Assessment Kit (SAK): A comprehensive assessment and policy development package. National Drug and Alcohol Research Centre. Sydney.
Duncan, B.L., Miller, D.S., Sparks, J.A., Claud, D.A., Reynolds, L.R., Brown, J., & Johnson, L.D. (2003). The Single Session Rating Scale: Preliminary psychometric properties of a ‘working’ alliance measure. Journal of Breif Therapy, 3(1), 3-12.
Echterling, L.G., Presbury, J., & McKee, J.E. (2005). Crisis intervention: Promoting resilience and resolution in troubled times. Prentice Hall. Colombus, OH.
Evans, N., & Evans, A. (2013). Solution- focused approach therapy for mental health nursing students. British Journal of Nursing, 22(21), pp. 1222-1226.
Ferraz, H. & Wellman, N., (2009). Fostering a culture of engagement: an evaluation of a 2-day training in solution-focused brief therapy for mental health workers. Journal of Psychiatric and Mental Health Nursing, Volume 16, pp. 326-334.
Fiske, H. (2008). Solution Focused Approach to Crisis. In Hope in Action: Solution Focused Conversations about suicide (H. Fiske Ed.). Taylor & Francis Ltd: New York.
Fleischmann, A., Bertolote, J.M., Wasserman, D., De Leo, D., Bolhari, J., & Botega, N., De Silva, D., Phillips, M., Vijayakumar, L., Vämik, A., Schlebusch, L., & Thanh, H.T. (2008.) Effectiveness of brief intervention and contact for suicide attempters: a randomized controlled trial in five countries. Bull World Health Organ. 2008; 86:703-709.
Gingerich, W. J. & Peterson, L. T., (2012). Effectiveness of SFBT: A systematic Qualitative Review of Controlled Outcome Studies. Research on Social Work Practice, 23(3), pp. 266-283.
Gysin-Maillart, A., Schwab, S., Soravia, L., Megert, M., & Michel, K. (2016). A novel brief therapy for patient who attempt suicide: as 24 months follow up randomized controlled study of the Attempted Suicide Short Intervention program (ASSIP). PLoS Med, 13(3): e1001968.
Hendon, J. (2008). Preventing Suicide: The Solution Focused Approach. John Wiley & Sons Inc. Chichester, England.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 80 of 86
Hepp, U., Wittmann, L., Schnyder, U., & Michel, K. (2004). Psychological and psychosocial interventions after attempted suicide: an overview of treatment studies. Crisis; 25:108-117.
Hoeppner, B.B., Kelly, J.F., Urbanoski, K.A., & Slaymaker, V. (2011). Comparative utility of a single item versus multiple item measure of self efficacy in predicting relapse among young adults. Journal of Substance Abuse Treatment, 41(3), 305-312.
Hogan, M. (2016). Better suicide screening and prevention are possible. JAMA Psychiatry, 73, 1111-1112.
Horvath, A.O., Del Re, A.C., Flückiger, C., & Symonds, D. (2011). Alliance in individual psychotherapy. Psychotherapy; 48:9-16.
Jackson, B.N., Purdy, S., & Cooper Thomas, H.D. (2018). Role of Professional Confidence in the development of Expert Allied health Professionals. Journal of Allied Health, 48(3), 226-232.
Jelinek, G., Weiland, T., Gerdtz, M., & Hill. N. (2013). Knowledge and confidence of Australian emergency department clinicians in managing patients with mental health related presentations: findings from a National qualitative study. International Journal of Emergency Medicine, 6:2.
Kapur, N., Gunnell, D., Hawton, K., Nadeem, S., Khalil, S., Longson, D.& Cooper, J. (2013). Messages from Manchester: Pilot randomised controlled trial following self-harm. British Journal of Psychiatry, 203(1), 73–74.
Kho, M.E., Duffett, M., Willison, D.J., Cook, D.J., & Brouwers, M.C. (2009). Written informed consent and selection bias in observational studies using medical records : systematic review
King, K., Bassilios, B., Reifels, L., Fletcher, J., Ftanou, M., Blashki, G., Burgess, P., & Pirkis, J. (2013). Suicide prevention: Evaluation of a pilot intervention in a primary care context. Journal of Mental Health, 22)5), 439-448.
Kinsella, R., Collins, T., Shaw, B., Sayer, J., Cary, B., Walby, A., & Cowan, S. (2017). Management of patients brought in by ambulance to the Emergency Department : Role of the Advanced Musculo-skeletal Physiotherapist. Australian Health Review, 42(3), 309-315.
Kõlves, K., Potts, B., & De Leo, D. (2015). Suicides in Queensland 2002-2011. Australian Institute for Suicide Research and Prevention: Brisbane.
Kroenke, K., Spitzer, R.L., & Williams, J.B.W. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606-613.
Lambert, M.J., Harmon, C., Slade, K., Whipple, J.L. & Hawkins, E.J. (2005). Providing feedback to psychotherapists on their patients’ progress: clinical results and practice suggestions. Journal of Clinical psychology, 61(2), 165-174.
Leggat, S.G. (2014). Changing health professionals’ scope of practice: how do we continue to make progress? Deeble Institute Issues Brief (NLCG-4). Deeble Institute for Health Policy Research. Australian Healthcare and Hospitals Association. Canberra.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 81 of 86
Leske, S., Crompton, D., & Kolves, K. (2019). Suicide in Queensland: Annual Report 2019. Brisbane, Queensland, Australia: Australian Institute for Suicide Research and Prevention, Griffith University. Brisbane.
Louzon, S.A., Bossarte, R., McCarthy, J.F., & Katz, I.R. (2016). Does suicidal ideation as measured by the PHQ-9 predict suicide among VA patients? Psychiatric Services, 76(5), 517-522.
Lovibond, P.F., & Lovibond, S.H. (1995). The structure of negative emotional states: comparison of the Depression, Anxiety and Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behaviour Research and Therapy, 33(3), 335-343.
Lovibond, P.F. (1998). Long term stability of depression, anxiety and stress syndromes. Journal of Abnormal Psychology, 107(3), 520-526.
Luty, S., & Scalia, S. (2018). Can interpersonal psychotherapy be delivered by a community agency? Australasian Psychiatry, 1-6.
McDonald, J., Ward, B., Lane, R., Kearns, R., Powell Davies, G., Fuller, J., Dennis, S., Spooner, C., & Russell, G. (2017). How are co-located primary health care centres integrating care for people with chronic conditions? International Journal of Integrated Care, I
Mallidou, A.A., Atherton, P., Chan, L., Frisch, N., Glegg, S., & Scarrow, G. (2018). Core knowledge translation competencies: a scoping review. BMC Health Services Research, 18: 502.
Martin, A., Rief, W., Klaiberg, A & Braehler, E. (2006). Validity of the Brief Patient health Questionnaire Mood Scale (PHQ-9) in the general population. General Hospital Psychiatry, 28(1), 71-77.
Meehan, T., Mansfield, Y., Neillie, D., & O’Gorman, J. (2016). Mental health presentations at Queensland Hospital Emergency Departments. Final Report to Queensland Health and the Mental Health Clinical Network.
Meehan, T., & Robertson, S. (2013). The Mental Health Nurse Incentive Program: reactions of general practitioners and their patients. Australian Health Review, 37, 337-340.
Meehan, T., & Robertson, S. (2015). Impact of the Mental Health Nurse Incentive Programme on patient functioning. International Journal of Mental Health Nursing, 24, 7581.
Miller, S.D., Duncan, B.L., Brown, J., Sparks, J.A., & Calud, D.A. (2003). The Outcome Rating Scale: a preliminary study of the reliability, validity and feasibility of a brief visual analogue measure. Journal of brief Therapy, 2(2), 91-100.
Morphet, J., Innes, K., Munro, I., O’Brien, A., Gaskin, C.J., Reed, F., & Kudinoff, T. (2012). Managing people with mental health presetnations in emergency departments: a service exploration of the issues surrounding responsiveness from a mental health care consumer and carer perspective. Australasian Emergency Nursing Journal, 15(3), 148-155.
Motto, J. A., & Bostrom, A. G. (2001). A randomized controlled trial of post crisis suicide prevention. Psychiatric Services, 52(6), 828–833.

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 82 of 86
Myers, B., Breuer, E., Lund, C., Petersen Williams, P., van der Westhuizen, C., Brooke – Summer, C., Naledi, T., Stein, D.J., & Sorsdahl, K. (2019). Assessing capability for implementing mental health counselling within primary care facilities in a middle income country: a feasibility study. J Psychiatr Ment Health Nur, 00:1, 1-12.
Nancarrow, S.A. (2015). Six principles to enhance health workforce flexibility. Human Resources for Health, 13(9).
Olfson, M., Marcus, S.C., & Bridge, J.A. (2014). Focusing suicide prevention on periods of high risk. The Journal of the American Medical Association, 311(11):1107-8.
Oman, D. & Bormann, J.E. (2015). Mantram repetition fosters self efficacy in veterans for managing PTSD: a randomised controlled trial. Psychology of Religion and Spirituality, 7, 34-45.
Owen, J., & Rogers, P. (1999). Program evaluation: Forms and approaches. Allen and Unwin. Sydney.
Pearson, A., Saini, P., Da Cruz, D., Miles, C., While, D., Swinson, N., Williams, A., Shaw, J., Appleby, L., & Kapur, N. (2009). Primary care contact prior to suicide in individuals with mental illness. The British Journal of General Practice, 59(568): 825-32.
Philip, K. (2015). Allied Health: untapped potential in the Australian health system. Australian Health Review, 39, 244-247.
Porsdam Mann, S., Savulescu, J., & Sahakian, B.J. (2016). Facilitating the ethical use of health data for the benefit of society: electronic health records, consent and the duty of easy rescue. Phil. Trans R. Soc A 374:20160130. http://dx.doi.org/10.1098/rsta.2016.0130
Porter, J., & Wilton, A. (2018). Professional Identity of Allied health Staff. Journal of Allied Health, 48(1), 11-17.
Potts, B., Kõlves, K., O’Gorman, J., & De Leo, D. (2016): Suicide in Queensland, 2011-2013: Mortality Rates and Related Data, Brisbane.
Queensland Health. (2015). Community mental health services in Queensland Time and Motion Study: Summary Findings. Queensland Health. Brisbane.
Queensland Health. (2016a). Connecting Care to Recovery 2016 – 2021: A plan for Queensland’s state funded mental health, alcohol and other drug services. Queensland Health. Brisbane.
Queensland Health (2016b). Suicide Prevention Health Taskforce: Phase 1 Action Plan. Queensland Health. Brisbane.
Queensland Health. (2016c). Allied Health Expanded Scope Strategy 2016 – 2021. Queensland Health. Brisbane.
Queensland Health (2017a). State-wide Mental Health Allied Health Scope of Practice Project: Community Adult Mental Health Final Report. Allied Health Professions Office of Queensland. Brisbane.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 83 of 86
Queensland Health. (2017b). Mental Health Alcohol and Other Drugs Workforce Development Framework 2016-2021. Queensland Health. Brisbane.
Queensland Mental Health Commission (2015). Queensland Suicide Prevention Action Plan 2015-2017. Queensland Mental Health Commission: Brisbane.
Queensland Mental Health Commission (2019). Every Life: The Queensland Suicide Prevention Plan 2019-2029 (Phase One). Queensland Mental Health Commission. Brisbane.
Rebers, S., Aaronson, N.K., van Leeuwen, F., & Schmidt, M.K. (2016). Exceptions to the rule of informed consent for research with an intervention. BMC Medical Ethics, 17(9). Doi:10.1186/s12910-016-0092-6
Rudd, M., Bryan, C., Wertenberger, E., Peterson, A., Young-McCaughan, S., Mintz, J., Williams, S.R., Arne, K.A., Breitbach, J., Delano, K., Wilkinson, E., & Bruce, T.O. (2015). Brief cognitive-behavioral therapy effects on post-treatment suicide attempts in a military sample: results of a randomized clinical trial with 2-year follow-up. American Journal of Psychiatry, 172:441-449.
Saxby, C., Wilson, J., & Newcombe, P. (2015). Can clinical supervision sustain our workforce in the current healthcare landscape? Findings from a Queensland study of allied health professionals. Australian health Review, 39, 476-482.
Sharry, J,. Darmody, M., & Madden, B. (2002). A solution-focused approach to working with clients who are suicidal, British Journal of Guidance & Counselling, 30:4, 383-399.
Simon, G.E., Rutter, C.M., Peterson, D., Oliver, M., Whiteside, U., Operskalski, B., & Ludman, E.J. (2013). Does response on the PHQ-9 Depression Questionnaire predict subsequent suicide attempt or suicide death? Psychiatric Services, 64(12), 1195-1202.
Stanley, B., & Brown, G. (2012). Safety planning intervention: A brief intervention to mitigate suicide risk. Cognitive and Behavioural Practice, 19, 256-264.
Stute, M., Moretto, N., Raymer, M., Banks, M., Buttrum, P., Sam, S., Bhagwat, M., & Comans, T. (2018). Process to establish 11 primary contact allied health pathways in a public health service. Australian Health Review, 42, 258-265.
Surgenor, P., Freeman, J., and O’Connor, C. (2015). Developing the Pieta House Suicide Intervention Model: a quasi-experimental, repeated measures design. BMC Psychology, 3, 14.
Surgoner, P., Meehan, V., & Moore, A. (2016). Early attrition among suicidal clients. British Journal of Guidance and Counselling, 44:5, 589-597.
Swift, J. K., & Greenberg, R. P. (2012). Premature discontinuation in adult psychotherapy: A meta-analysis. Journal of Consulting and Clinical Psychology, 80, 547-559.
Victorian Government Department of health. (2013). The National Practice Standards for the Mental Health Workforce 2013. Safety and Quality partnership Standing Committee, Melbourne.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 84 of 86
Wand, T., (2010). Mental health nursing from a solution focused perspective. International Journal of Mental Health Nursing, Volume 19, pp. 210-219.
Wand, T., Acret, L. & D'Abrew, N., (2017). Introducing solution-focussed brief therapy to mental health nurses across a local health district in Australia. International Journal of Mental Health Nursing, pp. 1-9.
Woolf, S.H., Rothemich, S.F., Johnson, R.E & Marsland, D.W. (2000). Selection bias from requiring patients to give consent to examine data for health services research. Arch Fam Med, 9, 1111-1118.
Evaluation of the Allied Health Brief Therapies (AHBT) Clinics - Final Report December 2019 Page 85 of 86
9 Appendices
Appendix A: Consumer Measures
Depression, Anxiety and Stress Scale (DASS 21) The DASS was developed in Australia (Lovibond & Lovibond 1995; Lovibond, 1998). The brief 21-item version of the measure will be used in this evaluation. The 21 items can be collapsed into three separate but related subscales that assess; depression, anxiety, and stress. Response options focus on the amount of time in the past week that an individual experiences a given problem, such as ‘I couldn't seem to experience any positive feeling at all.’ This and other items are rated on a 4-point scale ranging from ‘Did not apply to me at all’ to ‘Applied to me very much or most of the time’. Higher scores represent more severe problems. In Australia, the DASS is widely used as a screening tool by General Practitioners and other clinicians.
Suicide / Self Harm Ideation and Intent (SSHII) This brief measure allows clinicians to collaboratively document ideation and intent around suicide with clients. It is comprised from the following existing measures:
a) Primary Health Questionnaire 9 – Depression (PHQ-9)
The PHQ 9 is a brief, reliable and validated measure of depression severity based on the nine diagnostic criteria for major depression identified in the Diagnostic and Statistical Manual of Mental Disorders, DSM – IV (Kroenke, Spitzer & Williams, 2001; Martin, Rief, Klaiberg & Braehler, 2006; Cedergren, 2012). Question 9 in the measure screens for the presence and duration of suicide ideation and has been found to be a strong predictor of suicide attempt and death over the following 12 months (Simon, Rutter, Peterson, Oliver, Whiteside, Operskalski & Ludman, 2013; Louzon, Bossarte, McCarthy & Katz, 2016)
b) Suicide Risk Screener
The Suicide Risk Screener was developed in Australia as a component of a broader Suicide Assessment Kit (SAK) initially to provide alcohol and other drug workers with evidence based resources to assist them in the assessment and management of suicide risk (Deady, Ross & Darke, 2015). It is a simple tool designed for use at set time points in treatment (e.g. admission, transition points, discharge) or at times where client crisis is clearly visible or suspected. Question 8 from the Suicide Risk Screener has been included in the clinic measure as a brief, simple but effective question that specially targets suicidal intent.
c) Single Item Self Efficacy Measure (SEM)
The SEM is used to measure perceived self-efficacy of recovery and has been adapted for use in a range of areas including alcohol abstinence (Hoeppner, Kelly, Urbanoski & Slaymaker, 2011), engagement in anxiety treatment (Brown et al, 2014) and PTSD symptom management (Oman & Bormann, 2015). Respondents are asked to rate their confidence in terms of maintaining their recovery and staying well over a period of time on a 10-point scale (1- not confident, 5-6 somewhat

Evaluation of the Allied Health Brief Therapies (AHBT) Clinics — Final Report December 2019 Page 86 of 86
confident and 10 – very confident). The original SEM has been found to be a statistically significant predictor of alcohol use relapse at one month and has shown convergent validity with the longer 20 item Alcohol and Drug Abstinence Self Efficacy Scale (Hoeppner, Kelly, Urbanoski & Slaymaker, 2011).
Session Rating Scale (SRS) The SRS is brief 4 item visual analogue scale designed to measure the client’s perception of four domains of the therapeutic relationship: respect and understanding; relevance of goals and topics; client practitioner fit and overall alliance (Duncan, Miller, Sparks, Claud, Reynolds, Brown & Johnson, 2003). Designed to be administered every session, the SRS allows practitioners to predict with a high degree of certainty the value of therapy as well as real time feedback on the therapeutic alliance including: empowering clients, promoting collaboration, making necessary adjustments to therapy and enhancing outcomes (Lambert, Harmon, Slade, Whipple & Hawkins, 2005). It has been found to have significant and consistent moderate correlation with the Working Alliance Inventory – Short (WAI-Short) and is also positive correlated with outcome measures, such as the Outcome Rating Scale (ORS) (Campbell & Hemsley, 2009).
Outcome Rating Scale (SRS) The ORS is a brief 4 item visual analogue outcome measure designed for tracking client progress in every session (Miller, Duncan, Brown, Sparks & Claud, 2003). Clients are asked to rate their satisfaction on the following items: individual (personal wellbeing); interpersonal (family, close relationships); Social (work, school, friendships); and overall (general sense of well-being). Moderately strong correlation with The Outcome Questionnaire 45 (OQ-45) (Miller et al, 2003); moderate to strong correlations with self-esteem and self-efficacy measures and significantly correlated to the DASS 21(Campbell & Hemsley, 2009). Provides rapid and valid information about patient functioning and wellbeing that is more feasible than longer alternatives.
Consumer Feedback Survey A number of existing validated client satisfaction tools were reviewed to identify common key themes around mental health service provision. Measures included Your Experience of Service Survey (YES), the Client Satisfaction Questionnaire – 8 (CSQ-8) and the Consumer Perceptions of Care (CPoC) survey. From these, a survey was developed based on these themes to gauge broad consumer experiences and perceptions of the clinic including:
• Clinic accessibility and availability
• Satisfaction with clinic staff and services
• Usefulness / benefits of therapeutic interventions
• Possible improvements to clinic services / structures
The survey contains 7 statements rated on a 5-point likert scale ranging from 1 (Strongly Disagree) to 5 (Strongly Agree). There are also 2 open response questions for consumers to provide more detailed feedback around their experiences of services received at the clinic and suggestions for improvements.