evaluation of mobile health and nutrition teams in … · mobile health and nutrition teams f ......
TRANSCRIPT

2
EVALUATION OF MOBILE HEALTH AND NUTRITION
TEAMS IN AFAR AND SOMALI REGIONS
Final Report
DECEMBER 15, 2015

3 Evaluation of Mobile Health and Nutrition Teams: Final Report
3
Acronyms ................................................................................................................................... 4
Executive Summary ................................................................................................................... 6 Objectives and Methodology .................................................................................................... 6 Major findings ........................................................................................................................... 6 Recommendations..................................................................................................................... 8
Government ........................................................................................................................... 8 Development partners including UNICEF ............................................................................... 9
1. Background ................................................................................................................... 11 1.1. Context ......................................................................................................................... 11 1.2. Objective and scope of work ........................................................................................ 13 1.3. Methodology ................................................................................................................ 13 1.4. Limitation ...................................................................................................................... 19 1.5. Organization of the report ............................................................................................ 19
2. Description of the MHNTs in the two Regions ............................................................. 20 2.1. Why MHNT? ................................................................................................................. 20 2.2. Objectives and strategies ............................................................................................. 20 2.3. Design differences and peculiarities of MHNTs in Afar and Somali ............................. 20 3. Achievements of the MHNTs ........................................................................................ 24 3.1. Increasing access to services ........................................................................................ 24 3.2. Improving quality of services ........................................................................................ 31 3.3. Responding to health emergencies .............................................................................. 31 3.4. Capacity building .......................................................................................................... 32 3.5. Operation and management of MHNTs ....................................................................... 34 4. MHNTs relevance, effectiveness and sustainability ..................................................... 36 4.1. Relevance...................................................................................................................... 36 4.2. Effectiveness ................................................................................................................. 38 4.3. Efficiency ....................................................................................................................... 40 4.4. Cost effectiveness and Sustainability ........................................................................... 42 5. Financing of the MHNTs ............................................................................................... 44 6. Major findings and recommendation ........................................................................... 46 6.1. Findings ......................................................................................................................... 46 6.2. Recommendations ........................................................................................................ 48
7. Annexes: ....................................................................................................................... 51 Annex 1: Semi-structured Interview Guide for national level KII ............................................ 51 Annex 2: Semi-structured Interview Guide for Development and Implementing Partners ... 55 Annex 3: Semi-structured Interview Guide for regional and Woreda health offices .............. 59 Annex 4: MHNT Observation Checklist ................................................................................... 63 Annex 5: Focus Group Discussion Guide at Community Level ................................................ 66 Annex 6: Secondary information from RHB and WoHo and health facilities .......................... 68

4 Evaluation of Mobile Health and Nutrition Teams: Final Report
4
Acronyms ANC AWD
Antenatal Care Acute watery Diarrhoea
C-IMCI Community Integrated Management of Childhood Illnesses
CSOs DPs DSA
Civil Society Organizations Development Partners Daily Subsistence allowance
ECHO EPI FGDs
European Commission for Humanitarian Aid Expanded Program on Immunization Focus Group Discussions
HEP Health Extension Programme
HEWs Health Extension Workers
HSDP Health Sector Development Programme
ICCM iMHNT KII
Integrated Community Case Management Integrated Mobile health and nutrition team Key Informant interview
IMNCI MHNTs
Integrated Management of New-born and Childhood Illnesses Mobile health and nutrition teams
F(MOH) Federal (Ministry of Health)
I(NGO) OECD-DAC OFDA OCHA OPV
International (Non-Governmental Organization) Organization for Economic Cooperation and Development-Development Assistance Committee The Office of U.S. Foreign Disaster Assistance UN Office for the Coordination of Humanitarian Affairs Oral polio Vaccination
PCV Pneumococcal conjugate vaccine
PHC Primary Health Care
PHCU Primary Health Care Unit
PHEM PHEW
Public Health Emergency Management Pastoralist Health extension program
RHBs RUTF
Regional Health Bureaus Ready to use therapeutic Food
SBA Skilled Birth Attendants
TT Tetanus Toxoid
UNICEF United Nations Children’s Fund
USAID WASH WoHO
United States Agency for International Development Water, sanitation and hygiene Woreda Health Office

5 Evaluation of Mobile Health and Nutrition Teams: Final Report
5
Acknowledgement The authors would like to acknowledge the support and inputs of many colleagues in Ethiopia’s Federal Ministry of Health. We would like to acknowledge the the two regional health bureaus and partners that have reviewed the tools and assisting in sample selection as well as providing valuable comments on the draft report. We are also grateful for key informant interviews at the federal, regional, woreda and MHNTs levels as well as communities we have talk for their views and support during the evaluation process. Development partners that were interviewed including OCHA/HRF, OFDA, ECHO, Australia National Committee for their views and suggestions. We would like to thank UNICEF for guiding and steering the whole evaluation process both at the regional and national levels. We would like to acknowledge the contribution of Ato Getachew Haile, Beshir Sheik Mohammed and Mohammed who have been actively engaged during the whole evaluation process.
The evaluation Team
6 Evaluation of Mobile Health and Nutrition Teams: Final Report
6
Executive Summary
Objectives and Methodology The overall objectives of this study is to evaluate the current and future contributions of
MHNT in Afar and Somali regions with answering (i) what is the effectiveness and efficiency
of MHNT for providing emergency health and nutrition services ; (ii) what is the perception of
the community accessibility, availability, completeness of quality of service provided by
MHNTs?; (iii) what is the current and unrealized potential contributions and/or challenges of
MHNTs towards the development of effective pastoralist health care delivery services and (iv)
what are the major recommendations that will help guide the evolution of the MHNT in the
medium term?. The evaluation used OECD DAC evaluation criteria as a methodology. The
evidences used to reach on the conclusions and recommendations were collected through
key informant interviews of DPs, RHBs, and active implementing partners as well as actual
visit is selected MHNTs. The evaluation team had also a chance to undertake FGDs with
communities that were found using the MHNTs during the the visit.
Major findings Overall the MHNTs are relevant to the pastoralist and weak health infrastructure context of
Somali and Afar regions and could be considered as a transitional alternative strategy for
health service delivery in these two regions. MHNTs were effective as compared to the static
facilities in creating access to previously unreached population groups for health services.
They MHNTs were able to provide:
158,758 and about 1.7 million consultations in Afar and Somali regions with 3 and 24 MHNTs respectively over the last 4 years
3042 referrals in Somali region and 386 in Afar between 2010-2014
OTP to a good number of pastoralist children, with the recovery rate rate of more than 80%; mortality rate of about 1% and a defaulter rate of less than 8%;
around 33,000 children with Penta 3 and OPV 3; around 21,000 children with PCV-3; and more than 18,000 children were fully vaccinated between 2011-2014;
But the investment of MHNT is investing on is on maternal health- ANC, PNC family planning and delivery services is not effective due to deep-rooted cultural barriers that hindered utilization. Service uptake rate is not as good as other services. MHNTs reached in Somali region about 46,000 pregnant women with TT vaccination in the last four years, of which only 4400 pregnant women took TT4, and 2042 mother have been assisted with delivery services showing the inefficiency of the systems as 90% of mothers dropped out from ANC 1 to ANC 4 and delivery.
The MHNTs has also been effective in responding to health emergencies and saving lives.
However, clear triggers of entry and exit from the emergencies are not always clear. MHNTs
has been also effective in capacity building of Pastoralist HEWs in Somali region, while this is
not the case in Afar and IMHNT in Somali region. The IMHNTs objective to strengthen health
posts and woredas in Somali regions is good initiative, but the the environment within which
7 Evaluation of Mobile Health and Nutrition Teams: Final Report
7
it is operating (inadequate woreda health staff and health extension workers and frequent
turn over) hamper the realization of its objective of graduating woredas and health facilities
after building their capacities.
The services provided by the MHNTs to the community by and large remain adequate in terms
of scope and address priority health services especially in Somali region. The perception of
the community about the effectiveness and reach of the MHNTs is quite positive. There is
universal acknowledgement of the value of MHNTs in reaching the unreached by the RHBs,
woreda health officials, facility heads, community discussions and and their role in some cases
in introducing modern health care services. It has started influencing health seeking
behaviors. The FDGs with the community members revealed that the community is willing to
contribute a goat per year per household rather than seeing the MHNTs discontinue their
operation due to lack of finance.
The evaluation team was unable to compare the efficiency of the MHNTs and static facilities
in the same woreda, due to lack of disaggregate outcome and financing data. Overall, the unit
cost for providing consultation and treatment by MHNTs increased from $1.41 to $3.55 in
2014 and of which the unit running cost was $1.3 and $1.9 respectively in these years. This
clearly shows that non running costs are contributing more in increased costs recently. There
are also inefficiencies as evidenced by the fact that only 8% of the MHNTs were able to
operate the full 12 months while all the rest were unable to do so.
There are some success and constraining factors in the functioning of MHNTs. The success
factors include:
There is ownership of MHNTs by RHBs and the community: they are being managed
and run by the RHBs. The RHBs instituted its own review and supportive supervision
visits. In Somali region, MHNTs are politically supported to provide service in insecure
woredas. The community perception and values on MHNTs services is quite positive
and in our discussions with leaders, they have expressed willingness to contribute at
least a goat to finance their operation rather than seeing it discontinued due to lack
of financing. They are also aware of their schedules and report to the woreda office
when MHNTs do not show up.
Both regions take care in selecting health professionals that are deployed in MHNTs.
In the majority of cases, heath professionals with better skills and capacity as well as
commitment are recruited and deployed. When skill gaps are observed, training is
provided before deployment.
The regions carry out regular performance reviews. The achievements, challenges as
well as actions to be taken are presented and discussed in the presence of the MHNTs,
woreda officials and the regional bureau. There is more active follow up of actions
agreed upon in the subsequent review meetings in Somali region.
There is regular availability of kits and supplies for MHNTs. The availability of supplies
is reported to be much better in MHNTs than static facilities. When there are
occasional shortages, mechanism is in place to fill the gaps either from Woredas or
UNICEF.

8 Evaluation of Mobile Health and Nutrition Teams: Final Report
8
MHNTs is serving as alternative service delivery modality to pastoralist community at the
moment. Its potential however has not been fully exploited as it has not been classified as so
either by the RHBs or the FMOH. Although their value in terms of relevance, effectiveness of
reaching the unreached and efficiency of resource use and commitment of the team members
is well appreciated by all, it has not been seen or reflected as a major priority and as alterative
service delivery strategy by the regional government’s strategies and and hence are not well
resourced from the regular government allocation. There is Inadequate political buy in by
Federal and regional levels as an alternative service delivery strategy. While the MOH is
exploring innovative mechanisms to deliver services to pastoralist community, it is yet to
approve and support it as an alternative model. Even when one explores the regional health
strategic plans, MHNTs are considered as emergency response mechanism rather than
alternative service delivery model. As a result of these, the FMOH isn’t contributing to the
financing of the MHNTs and the RHBs are not able to mobilize adequate funding from the
regional allocations. As a result, the functionality and operation of the MHNTs is highly
dependent on the external funding. Given the number of years that some of the DPs are
financing MHNTs, their continued commitment and financing is not certain. Unless
sustainability and exit plan are agreed and implemented, a sudden withdrawal is likely to
erode the gains made by the MHNTs. The woredas being supported by the MHNTs have
developed dependency syndrome and are not willing to allow MHNTs to exit. Some woredas
have managed to reverse decisions to exit politically. The vehicles used for MHNTs are
becoming older and the cost of maintenance is increasing. So far, there is no vehicle
replacement strategy in place as the case is with ambulances deployed by the FMOH. The
quality and availability of maintenance service in the regions is inadequate and very long time
is required for maintenance, with long service disruption time. There are no standby cars or
resources to rent additional cars to ensure continuity of service when needed.
Recommendations
Government
Consider MHNTs as an alternative PHC service delivery strategy for medium term in the next
regional health sector transformation plan. Currently the government’s main strategy is to
encourage pastoralists to voluntarily settle and provide facility-based services. This is a correct
priority over the long term. However, there will be people that are moving from place to place
and will not access services in the short and medium term. There is also a need to work with
the FMOH and generate evidences of different modalities of alternative service delivery for
the pastoralist context. If MHNTs is found the best options available, MHNTs could evolve as
a transitional alternative service delivery strategy for pastoralist areas to reach the
underserved population. This calls to clearly put it as one of the priorities to enhance access
to PHC rather than emergency response. This may include development of the strategies on
how to integrate other PHC services with the MHNTs services. It also calls for ensuring that it
is led and managed by the PHC unit rather than PHEM. The RHBs should develop a clear
strategy on how they are going to use MHNTs as an alternative strategy.

9 Evaluation of Mobile Health and Nutrition Teams: Final Report
9
Ensure buy-in of the alternative service delivery strategy by the regional cabinet and FMOH.
Given MHNTs are credible and politically driven starting from the president of the Somali
region, it may be important to get the alternative strategy approved by the regional cabinet.
The strategy should also provide evidence and justification on why and how much the
government should finance MHNTs as transitional service delivery model. This will help the
RHB negotiate and budget a reasonable share of government resources to MHNTs.
Consider innovative mechanisms to mobilize additional external resources for MHNTs. Once
the region has endorsed MHNTs as alternative strategy and budget for it, the RHBs can use
the budget as ‘’pooled fund’ or ‘matching fund’ to mobilize additional funding from interested
partners. This will also include the development sustainability plan for MHNTs in the long term
and how the region will transit from MHNTs to static facilities. Given that these regions are
often characterized by frequent health emergencies; it may also be necessary to consider
financing MHNTs as a one of the strategies for exiting emergencies by international agencies.
If FMOH is convinced about its ability to serve as alternative strategy, RHBs should leverage
the equity agenda of the Heath Sector Transformation Plan to mobilize additional predictable
resources through the FMOH.
Look for alternative strategies for strengthening woreda and HP systems instead of using
iMHNTs: Indeed, the iMHNTs have strengthened health service delivery at the HP and
supportive supervision at the woreda levels. The potential for iMHNTs to enable facilities and
woredas to graduate is constrained by weak environment/context at the woreda level.
Strengthening the health systems is very important and critical but it may be also important
to re-look whether the iMHNT is the right strategy for continued capacity development.
Revise the MHNTs Package based on the visions and directions of the FMoH as alternative
service delivery strategy: there is evolution in service delivery in the Ethiopian Heath care
delivery system as more of the curative services are being provided at the heath post levels in
the agrarian context. The MHNTs is bridging such a system in the pastoralist context. If the
MHNT model is accepted as an alternative service delivery strategy, it is necessary to revisit
the MHNTs service package, its human resource requirements as well as the implementation
guidelines and make it more affordable.
Exit strategy: the RHBs should work with the main partners to develop an exit strategy that
will outline on how government will take increasing responsibility of financing MHNTs and
allow some partners either to exit from the financing and reduce the scale of their investment
in the medium and long term.
Development partners including UNICEF
Responsible withdrawal: The MHNTs were effective in saving lives and reach marginalized
population groups. Immediate reductions of external resources are like to reduce the gains
made so far in providing OTP, immunization and consultation services. The support given to
the MHNTs should continue until its status, as an alternative model of service delivery is
known. Partners that have been investing on MHNTs should develop with the RHBs on exit

10 Evaluation of Mobile Health and Nutrition Teams: Final Report
10
strategy that clearly outlines the responsibilities of the RHBs and DPs, which will allow
responsible withdrawal.
Continue ensuring the regular Essential Drug Kit and nutrition supplies: UNICEF has been
able to ensure that the needed kits and nutrition supplies are available for MHNTs. All MHNTs
stated that the supplies are by and large available to run the services. It is therefore necessary
for UNICEF to continue investing on ensuring the availability of kits and supplies. The move
towards integrating it to government supply system will not work at the moment, given the
high stock out rates in static facilities.
Advocate and negotiate with RHBs to make MHNTs as transitional strategy and for more
resource allocations: UNICEF and other DPs supporting MHNTs should enhance their
engagement and advocacy with the FMOH and regional RHB to help MHNTs evolve as an
alternative strategy for service delivery.

11 Evaluation of Mobile Health and Nutrition Teams: Final Report
11
1. Background
1.1. Context
The repeated emergencies related to droughts, floods, diseases outbreaks as well as conflicts
and increasingly weakened resilience to such threats make many of the pastoralists
vulnerable. The health systems were not ready and suited to meet such demands in terms of
providing adequate access and quality especially for pastoralist communities. There was a
need to introduce innovative health service delivery mechanisms to respond to these crises.
The need to increase access and utilisation of service especially through free outreach service
and strengthen disease & nutrition surveillance became one of the major priorities in the
Somali and Afar regions. Mobile health and nutrition teams (MHNTs) were initiated to
respond to and meet the growing challenges of meeting the health needs of the pastoralist
community. It started in the Somali region on a small scale in 2004. Since its initiation, the
number of MHNT deployed in Ethiopia has continued to rise in response to each emergency.
By 2009, there were 20 government-run teams in Somali region expanded and by 2011 it again
increased 24. Alongside government run MHNTs, international NGOs (INGOs) working in
Somali have deployed additional MHNTs, generally operating in a similar manner, but often
with specific project defined variations. During the HOA crisis of late 2011, the total number
of deployed MHNTs reached over 50 teams in Somali region alone. In Afar, 4 MHNTs started
in March 2009, including 2 camel run teams that were disbanded in 2010. In 2010 the number
of vehicle-run MHNT increased to 3 then to 4 teams in 2011.
The importance of mobile health teams in pastoralist context has been an agenda of research
for some time globally. Imperato [1969] had to learn that, while he was reaching nomadic
men for vaccination against small pox in villages on market days, he did not reach children
and women who stayed behind in the camps. MHUs are a strategy (which is sometimes
effective but rarely has lasting effects) to be used as a last resort to reach population groups
cut off from health services. The main objective of the use of MHUs is to improve the access
of these population groups to the health system. MHUs are popular and flexible. They are
deployed on a temporary basis, before the opening (or reopening) of permanent health
facilities (health posts or centers) to refer isolated population groups to existing health
facilities. Many articles stress the importance of there being a fixed health facility on which
the MHU can depend (for example, a health center or a hospital offering specialized services).
This fixed facility has a dual role selection of patients and follow-up of patients after the
departure of the MHU. However, mobile services had higher costs than static facility services
[Brenzel and Claquin 1994] - particularly if operating independently from static health facilities
[Aliou 1992]. A combined system of mobile (outreach services) and static health services can
make better use of existing infrastructure and human resources and avoid that communities
can only access mobile services that are limited in time and space. Animal health can be a
gateway to mobile pastoralist communities for the public health. Complementary to any
health care is the provision of appropriate information. Indeed, pastoral communities with
their perceived exclusion from planning often ask for sufficient information on health topics.
Good and widespread knowledge on animal health – often with perceived more
straightforward concepts than for human illnesses – can be used for human health
information.

12 Evaluation of Mobile Health and Nutrition Teams: Final Report
12
Although data on effectiveness were not available, both the Regional Health Bureaux and
UNICEF staff argued that mobile health teams provide better services for pastoralists, and
have lower recurrent costs, than fixed facilities, although this would need to be empirically
tested. Both stated that MHTs have played key roles in reaching previously unreached
populations in 20 of the 53 Woredas in Somali and three Woredas in Afar (DFID, Peace and
Development Program-options for service delivery, 2011). In Afar camel based MHTs
providing curative services and assisting HEWs have been piloted. These MHTs maintain
regular weekly outreach services to communities. The same report indicated that MHTs are
better managed and operated by non-government actors, and that UNICEF managed MHTs
are less costly than those managed by NGOs. The report indicated that an assessment carried
out by Somali Regional Health Bureau reported the need to establish 65 MHTs in Somali
region. Major issues associated with scaling up include: (i) the cost (ii) a tendency to operate
outside the referral system, and (iii) a tendency to move from Woreda to Woreda for the sake
of equity rather than need. Furthermore, the funding of these services comes in the form of
emergency support, and through channel 3 for some of the NGOs, raising questions of
sustainability.
The context in which MHNTs operate is changing. The static health service provision has
continued to expand with more health workers training and deployed, more health centers
and health posts equipped and made operational. Integrated Community Case Management
(iCCM) has recently started that will increase the curative capacity of pHEWs. Accordingly,
there is a strong desire to better define the ways in which MHNTs can meaningfully work
closely with the rapidly evolving static health system while maintaining its core function as
emergency health responders.
We understood that the regional government, UNICEF and several other partners have made
considerable investments in the MHNT strategy. Although there is a general appreciation of
the live-saving contribution of such teams in times of crises and admiration for their
dedication to providing life-saving emergency health services, there has been no formal
evaluation of the impact of MHNTs on reducing excess mortality and morbidity in times of
crises since 2009. This evaluation is expected to appraise the rapidly evolving context in which
MHNT works, including the development of the health system, and explore what has worked
in its design and what may require modifications.

13 Evaluation of Mobile Health and Nutrition Teams: Final Report
13
1.2. Objective and scope of work
According to the RFP the overall objectives of the study is to evaluate the current and future
contributions of MHNT with answering the following evaluation questions:
1. What is the effectiveness and efficiency of MHNT for providing emergency health and
nutrition services in the pastoralist regions of Somali and Afar?
2. What is the perception of the community accessibility, availability, completeness of
quality of service provided by MHNTs?
3. What is the current and unrealized potential contributions and/or challenges of
MHNTs towards the development of effective pastoralist health care delivery
services;
4. What are the major recommendations that will help guide the evolution of the MHNT
in the medium term?
In the course of answering these questions, the study needs to produce the following
deliverables:
Inception report: including final, detailed evaluation plan as well as the evaluation
data collection tools
Hard and electronic copies of all secondary reference materials obtained during the
evaluation in a reference binder
Note summarizing general stakeholder’s consultation meeting
Hard and electronic copies of all primary data collected
Preliminary report and presentation (5 hard copies)
Final, bound report and accompanying presentation (20 copies)
1.3. Methodology
1.4.1 Evaluation framework
The evaluation used the OECD DAC evaluation criteria of relevance, effectiveness, efficiency,
and sustainability to evaluate the MHNT in Somali and Afar regions. We documented the
relevance of the MHNT not only to the needs of the community but also its linkage with
government policies and strategies. The study documented its achievement in terms of
reaching the unreached and improving quality of care in the difficult service delivery
environments. Our evaluation questions helped us review what worked well and what hasn’t
in terms of design, and implementation. The lessons learnt has been identified and
recommendations on how the MHNT should evolve in the coming few years are provided.
Table 1 presents the evaluation framework for the study.

14
Table 1: MHNT evaluation framework
Themes Evaluation Issues Methods and sources of information
Rel
evan
ce
Did the MHNT planning and implementation meet the needs of community - Focus Group Discussion, Interviews with facility
To what extent, and in what ways, did Mobile health teams demonstrate clear linkages to major health sector strategies and objectives?
- Desk review of results chain - Plot and examine programme logic in terms of major process
activities /outputs against sought outcomes - Interviews
DES
IGN
& IM
PLE
MEN
TATI
ON
To what extent were RHBs and other stakeholders actively involved in the design of the application? - Document review - Interviews
Implementation of planned activities (quality, quantity, ways and means)? Availability of qualified Health workers
a. Availability of formal package of training & protocols provided b. Resources and support for transportation and movement & supplies c. Availability of Medical supplies & consumables d. Tools and focus for monitoring and supervision work
- Desk review of documents - Interviews - Field visits (Regional / Woreda/facility Level) Note: Different data sources triangulated
Activities, resources and results coordination, monitoring and reporting - Challenges associate with monitoring and reporting of the MHNT performance - Existence of feedback - Actions taking based M&E reporting appropriate actions
- Annual reports against guidelines and plans - Interviews
Use of findings/ recommendations from 2009 evaluation and other field monitoring reports to inform actions for the current design MHT design?
- Document review and comparison - Interviews
EFFI
CIE
NC
Y
Use of the funds allocated for MHNT against as planned - Review of financial data
Exploring factors explain the utilization of the funds received - Field visits and interviews
Complementarity of MHNT and facility based service delivery mechanisms - Comparative mapping of areas of resource allocation
Integration with the expanding static facilities in terms of: Planning; service delivery; monitoring and supervision; human resource management and motivation and supplies procurement and distribution
- Review of documents - Key interviews - FGDs
Eff
ect
ive
ne
ss To what extent did the MHNT achieve the objectives and targets as described in its project objectives? - Review of programme log frame (end point versus baseline
review of indicators)
15 Evaluation of Mobile Health and Nutrition Teams: Final Report
15
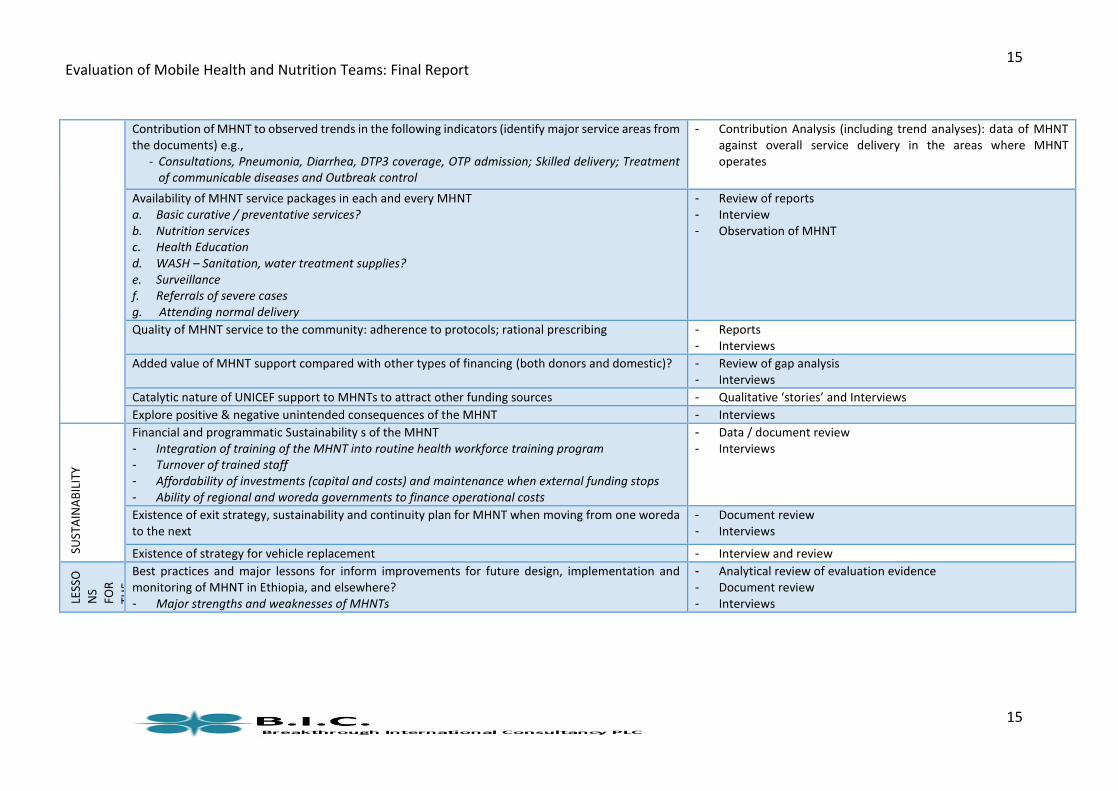
Contribution of MHNT to observed trends in the following indicators (identify major service areas from the documents) e.g.,
- Consultations, Pneumonia, Diarrhea, DTP3 coverage, OTP admission; Skilled delivery; Treatment of communicable diseases and Outbreak control
- Contribution Analysis (including trend analyses): data of MHNT against overall service delivery in the areas where MHNT operates
Availability of MHNT service packages in each and every MHNT a. Basic curative / preventative services? b. Nutrition services c. Health Education d. WASH – Sanitation, water treatment supplies? e. Surveillance f. Referrals of severe cases g. Attending normal delivery
- Review of reports - Interview - Observation of MHNT
Quality of MHNT service to the community: adherence to protocols; rational prescribing - Reports - Interviews
Added value of MHNT support compared with other types of financing (both donors and domestic)? - Review of gap analysis - Interviews
Catalytic nature of UNICEF support to MHNTs to attract other funding sources - Qualitative ‘stories’ and Interviews
Explore positive & negative unintended consequences of the MHNT - Interviews
SUST
AIN
AB
ILIT
Y
Financial and programmatic Sustainability s of the MHNT - Integration of training of the MHNT into routine health workforce training program - Turnover of trained staff - Affordability of investments (capital and costs) and maintenance when external funding stops - Ability of regional and woreda governments to finance operational costs
- Data / document review - Interviews
Existence of exit strategy, sustainability and continuity plan for MHNT when moving from one woreda to the next
- Document review - Interviews
Existence of strategy for vehicle replacement - Interview and review
LESS
O
NS
FOR
THE
FUTU
RE
Best practices and major lessons for inform improvements for future design, implementation and monitoring of MHNT in Ethiopia, and elsewhere? - Major strengths and weaknesses of MHNTs
- Analytical review of evaluation evidence - Document review - Interviews

16
1.4.2 Data Collection methods
The evaluation team used four different methods of data collection to generate information that was
necessary to reach to some kind of conclusions on what works and what doesn’t and to provide some
overall conclusions and recommendations. These data collection methods are the following:
Document review: The MHNT implementation guidelines, its concept note was reviewed. Any
documentation (regional sector plans, targets, performance reports, review findings etc., produced by the
two regions) of its contribution to the reach of services and quality was also reviewed and synthesized.
Any documentation both in-country and from experience of other countries on the challenges of MHNT
implementation and possible recommendations for short term and long term sustainability were
assessed. The evaluation team also collected the necessary information that helped to estimate the unit
cost of the providing services by the MHNTs and static facilities.
Key Informant Interview guides: We undertook in-depth interviews with key national officials and
implementing partners/stakeholders, including donors to explore their perception on the relevance,
effectiveness, efficiency and sustainability of the MHNT. We did also undertake in-depth interviews with
the regional and woreda managers to understand the success and the challenges of implementing MHNT
with changing landscape of service delivery in these two regions. We explored how effectively regions
are provided with the necessary inputs and system for the implementation of the MHNT operation. (See
annex 1-3)
MHNT Check List: The MHNT checklist was used to assess quality of the services in MHNTs. The assessment
was carried out while the teams were in the field. The evaluation team observed the extent to MHNTs were
effective in reaching the underserved population and carry out proper service delivery, treatment and
referral. The assessment reviewed the availability of the necessary human resource, equipment and
supplies, to carry out quality services as per regional guidelines (see annex 4). The observation and
interview at MHNTs level also helped to understand the extent to which the health workers are
capacitated/ trained to undertake the activities as per the guidelines.
Focus Group Discussion guide for Community level: The evaluation team has also undertaken some focus
group discussions of MHNTs to understand the perception of the beneficiaries, HEWs, on the
performance, relevance and effectiveness to meet their needs and expectation. It helped to generate
some ideas on what should be done to make the MHNTs formulation and implementation more
responsive (see annex 5). Focus group discussions were carried out in each of the visited MHNTs.

Evaluation of Mobile Health and Nutrition Teams: Final Report
17
Table 2: participants of the FGDs
Level Targets
Community Keble administration/ Community leaders
Beneficiaries of MHNTs
MHNT workers
1.4.3 Sampling frame
The overall contribution of the MHNTs to the service delivery of the regions was evaluated based on the
secondary time serious data generated from the MHNTs database and other secondary information on
woredas with MHNTs and those provided by the fixed facilities in other areas (see secondary information
collection tools). The determinants of what makes the MHNTs works and does not work were generated
from the data generated from the samples visits and key informant interviews. According the latest
information available, there are up to 24 MHNTs in Somali and 4 in Afar regions. The purposive sampling
frame was used to identify best performing and weak performing MHNTs to learn from the successes and
challenges of MHNTs in the two regions. The MHNTs was selected by the RHBs based on their strength
and weaknesses. The evaluation was conducted 9 MHNTs in Afar and Somali regions. The woredas and
health facilities visited were those that MHNTs were operating from and linked with and managed from.
Table 3 presents the sample woredas and MHNTs.
Table 3: Sampled MHNTs, woredas and health facilities
MHNTs Woredas Health facilities
Population
Afar 4
Somali 24
Sample
Afar 3 3 where MHNTs operate
(Kori; Buremodaitu, Dupti-
sekoita and kutibila Kebeles
3 health facilities where
MHNTs refer to
Somali 5 5 where MHNTs operate.
1 integrated MHNT
5 Health facilities MHNTs refer
to
Sample implementing partners: According to the latest available information, there are 6 and 11
implementing partners in Afar and Somali respectively supporting or were supporting the implementation
of MHNTs. Of these, in consultation with the two regional steering committees 4 were selected for KIIs.
Implementing partners providing high technical and financial support were selected as a sample (see Table
4).

Evaluation of Mobile Health and Nutrition Teams: Final Report
18
Table 4 Sample implementing partners
All MHNT Implementing Partners in Afar
regional state
All MHNT Implementing Partners in Somali
regional state
International Rescue Committee*
Samples
Save the Children, GOAL and Afar
Pastoralist Association
7 with higher involvement (technically and
financially). To be selected with RHB
* To be meet in Addis Ababa, others (no-star) in capital of region.
Development partners are critical providers of funding for the MHNTs. Of these all the major ones
including OCHA/HRF, OFDA, ECHO, Japan, and AUSTRALIA National Committee were included as part of
KIIs to hear their views on the achievements and challenges and lessons learnt from MHNTs experience.
UNICEF as a main technical assistance provider to these two regions was also interviewed at regional and
federal levels. The major KIIs that interviewed at national, regional woreda and facility levels are shown
in table 5.
Table 5 Key Informant interviewees at all levels
Level Targets
National Government: FMOH special support directorate; pastoralist directorate)
UN Agencies: UNICEF: WHO (EHR)
Donors: OCHA/HRF, OFDA, ECHO, Japan, Australia National Committee, U
Regional/Zonal RHB heads and service delivery focal persons/ process owner-responsible
for MHNTs, HEP focal person; PHEM focal person; RHB finance focal person
BOFED-UNDAF finance’ Water bureaus
Other MHNT providers/organizers
Woreda Woreda Administrator; Woreda health office head, Person responsible for
HEP, service delivery-MHNTs; woreda women, youth and children office;
WASH focal person in the water bureau
Health facilities
(Zonal/rural hospital, Health
center and Health posts)
Health facility heads and Health workers currently providing referral
services to the sample MHNTs
Team leaders of MHNTs 5 MHNTs in Somali and 3 MHNTs in Afar

Evaluation of Mobile Health and Nutrition Teams: Final Report
19
1.4. Limitation
The evaluation team was not able to get the necessary secondary information from the Somali RHB.
Further more, due to the commencement of rains, the evaluation team was only able to visit 5 of the
MHNTs in Somali and 3 of the MHNTs in Afar regions. The inability of the team to visit all the sample
MHNTs have limited the coverage and could have also confined the insight of the team on identifying
successes and challenges.
1.5. Organization of the report
Chapter two will present the description of the MHNTs in the two regions. Chapter three presents the
highlights of the achievements of the MHNTs. Chapter four presents the evaluation of MHNTs using the
OECD evaluation criteria (relevance, effectiveness, efficiency and sustainability). Chapter 5 shows the
financing of MHNTs in the two regions while chapter six presents the conclusions and recommendations.

Evaluation of Mobile Health and Nutrition Teams: Final Report
20
2. Description of the MHNTs in the two Regions
2.1. Why MHNT?
These two regions faced with repeated emergencies and increasingly weakened resilience to threats of
drought, floods, disease outbreaks and conflicts. These conditions affect the vulnerable population,
mainly pastoralist and agro-pastoralists. There is poor or limited health system for service delivery that fit
well to the living style of the pastoralist population. The need to increase access and utilization of service
is identified is one of the major system challenges that needs to be worked on.
2.2. Objectives and strategies
The main objectives of the mobile heath and nutrition teams are to:
Address repeated, regular emergency needs and increasingly weakened resilience due to shocks
such as drought, floods, disease outbreaks, and conflict (emergency response),
Address susceptible, mobile livelihoods profile (mainly pastoralist and agro-pastoralist) and poor
or limited basic infrastructures for service delivery that can meet public demand even in normal
times, (gap-filling)
Increase access and utilization through the provision of free outreach/mobile health and nutrition
services with a focus on women and children, (service performance), and
Increase disease surveillance to identify risk factors and monitor malnutrition pattern.
2.3. Design differences and peculiarities of MHNTs in Afar and Somali
The MHNT started in Somali region in 2004 to ensure that basic health and nutritional needs of
children and women are met at least in times of humanitarian emergencies1. These mobile teams
have indeed made basic health care services available to the un-reached during the difficult times.
Initially it was driven by UNICEF and later on by some NGOs, but it evolved into one of the innovative
service delivery modalities that is owned and led by the regional health bureau. The lessons from
Somali region are also being used in Afar, although at a reduced scale. In Somali there are currently
24 MHNTs while in Afar this is limited to four.
1 Somali Regional State Health Bureau Emergency Health and Nutrition Program Comprehensive Mobile Teams Performance Review Report -1st Quarter 2008

Evaluation of Mobile Health and Nutrition Teams: Final Report
21
There are two types of MHNTs in Somali. The first one is the regular MHNTs whose primary objective
is the service delivery to the community with secondary objective of building capacities of the health
facilities. The second type of MHNTs is the integrated MHNTs whose primary objective is to build the
capacity of health posts to provide services with its secondary focus on reaching the community. But
these integrated mobile health teams are limited to four.
All the four Mobile health teams in Afar are regular MHNTs. There was a camel driven MHNT in Afar
some time back. It was designed to provide services to areas where access to vehicle driven mobile
health teams was difficult. Unfortunately, this was discontinued due to the fact that the RHB and
woredas were not able to confirm whether they are operating as per guidelines due their inability to
provide regular supportive supervision on the ground.
The MHNT services have evolved in both regions from response to natural disaster and relief response
into one that provides routine and regular services for a limited time period in a woreda. The two
regions have slightly different design of this scheme (see table 6)

Evaluation of Mobile Health and Nutrition Teams: Final Report
22
Table 6 Design of MHNTs in Somali and Afar Regions
MHNT design
Elements
Somali Region Afar Region
1 Models of MHNTs Two: regular and integrated MHNTs Regular MHNTs. Had a camel MHNTs, but
stopped
2 Service package Regular MHNT: Consultation and treatment; Child health services; Maternal
Health Services; Nutrition; Referral and transport of all emergency cases; and
response emergencies
IMHNT: providing support for supervision, supply management and logistics,
on-the-job training in priority facilities, and facilitate report compilation and
analysis; provision of standard MHNT “gap-filling” support to provide health
services to un-served or migrant communities outside the catchment of
existing health posts, but this should not exceed 50% of their working time);
also respond to sudden emergencies (e.g. AWD outbreak)
Curative and preventive services and referral
services. The guidelines does not specify the
details of the services to be provided
3 Types of Human
resources
deployed
2 Health Professionals (clinical nurse and midwife)
3 Health Extension Workers
1 Social mobilizer
1 Driver
Composed of 4 clinical Nurses
(Diploma/Degree) or Health officers and one
Environmental health technician (Public nurse)
4 EDL and supplies Standard essential drugs and supplies for the regular MHNT services have
been identified and packages
IMHNTs also support the supplies of health posts whose capacities are being
built
Will be supplied with Essential Drug kits
(EDKs). The guideline does not have a package
as the case is in Somali region
5 Working time and
arrangement
6 days per week with a movement plan 6 days per week with a movement plan
6 Scope of
movement
Support six operational sites including one health post for three weeks and
move to the next. The team will assist in functionalizing and strengthening the
health post by visiting one day per week for three weeks.
6 kebeles or 5 depending on the sizes of the
kebeles in a week time and should also move
depending on the movement of the
population
7 Entry and exist
criteria
Entry of regular MHNT: woredas with either or combination of disease
outbreaks and/or other health related hazards (flood, drought, internal
displacement, clan conflict, etc.) or Woredas with major access problems
and/or Woredas with relatively very low service coverage as per the RHB
categorization.
Entry for IMHNT: Better functioning woredas
Exit for Regular MHNT: If operational limitations limit the functioning of for
the MHNT the service provisions; or if the health condition of the woreda
improves and/or if the condition of another woreda worsens than a woreda
having MHNT
Exit for IHMNT: no clear criteria
No explicit entry and exit criteria

Evaluation of Mobile Health and Nutrition Teams: Final Report
23
The services have reached the unreached population of these two pastoralist regions. There has been
some growing interest and commitment to get these services rollout to the community by the two
regional health bureaus. This is evidenced by the development of the standards for MHNTs and
establishment of the teams within the RHBs. It is also evidenced by the commitment of the RHBs to
assign human resources and undertake regular monitoring meetings. However, most of the non-salary
resources required are still financed through external funding.
Service composition: many of types of services provided through MHNTs are similar in both regions.
However, there is much more focus on health education in Afar than Somali region. On the other
hand, maternal delivery service is part of the Somali MHNTs and there is a midwife as part of the team
to carry out this function. In Afar, there are no midwives as part of the team and MHNTs do not
provide maternal delivery services.
There is also difference in focus on capacity building between the two regions. One of the objectives
of the MHNTs in Somali region is to strengthen the capacity of the HEWs by working with them as part
of the team. In addition, the region is also implementing the IMHNTs whose primary objective is test
the mechanisms of strengthening HPs and woredas. In contrast, in Afar, there is no clear objective of
capacity building for the mobile health teams and HEWs are not working with them.
Evaluation of Mobile Health and Nutrition Teams: Final Report
24
3. Achievements of the MHNTs
3.1. Increasing access to services
Overall there is clear consensus among the various key stakeholders interviewed at the regional, woreda
and facility levels that the MHNTs has contributed to the improvement in the health status of the Somali
population. The following are the major achievements as perceived by stakeholders in the two regions:
MHNTs averted death of many thousands of population by providing primary health care service (consultation and treatment) and early referral services care
They introduced the concept of modern health care including immunization of children that
positively influenced early health seeking behaviors,
Helped to contain health emergencies when disease outbreak occurs, as one appropriate disaster
risk management approaches- preparedness, response, and rehabilitation of people affected;
Increased access to care by reaching the mobile community in both regions; it also helped to
provide health services to conflict prone and no go areas in Somali region; and
In Somali region contributed to capacity building of the health extension workers and woreda
health offices.
Indeed, MHNTs have reached the hitherto unreached segment of the pastoralist population. The MHNTs
are deployed in areas where the facility level services cannot reach the community. It is generally
deployed to areas that are hard to reach, even in some cases where there is security related challenges.
Its ability to move with the community and respond to their needs makes it more important in reaching
them. Although there are areas far, in the majority of cases, the MHNTs travel between 10-70 kms to
reach the community.
Regular availability of services once a week is one of the strengths of MHNTs compared to static facilities
that are affected by the frequent breakdowns of services mainly due to staff turnover and stock out of
supplies. In comparison, the MHNTs are reported to maintain the service provision at an acceptable level.
One of the team leaders of MHNTs in Somali region who served for three years in different places stated
that in the MHNTs ‘never seen any stock out of medical supplies’. If it happened, the woredas are also
ready to fill the gap.
MHNT has contributed to the increasing uptake of services by the pastoralist community: Stakeholders
(RHBs, health workers, implementing partners and beneficiaries) all agree that MHNTs in both regions
have reached population groups (kebeles and woredas) that have not been beneficiaries of the static
health systems. They are deployed in areas where there is no or very limited number of facilities, and
where delivering health services is particularly challenging. MHNTs helped to change the mindset of the

Evaluation of Mobile Health and Nutrition Teams: Final Report
25
community to seek care when feel seek. Poor health care seeking behavior is one of the major barrier to
care and that is why there is programs that aimed at reducing demand side barriers in the region: the
RMNCH innovative Fund financed through DFID. According to the head of the Somali RHB, the MHNTs is
changing that attitude and they are seeking more care than before. Although show some decline in 2014
and about 554908 in Somali and 32815 people consulted MHNTs in 2013. The MHNTs were able to provide
158,758 and about 1.7 million consultations in Afar and Somali regions with 3 and 24 MHNTs respectively
over the last 4 years (see Table 7).
Table 7: Consultation services provided
Afar Somali
<5yr <15 yr ≥15 yr Total <5yr <15 yr ≥15 yr Total
2014 5,226 3,486 3,354 30,336 129,433 74,071 144,282 347,786
2013 13,838 9,267 9,710 32,815 204,033 100,828 250,047 554,908
2012 13,087 6,436 10,886 30,409 149,280 70,231 192,363 411,874
2011 23,937 8,480 11,470 43,887 57,295 27,153 75,685 160,133
2010 10,600 3,579 7,132 21,311 79,255 36,364 92,994 208,613
Total 66,688 31,248 42,552 158,758 619,296 308,647 755,371 1,683,314
Note; the data for 2014 is not a full year
Source: MHNT Database
Associated with the consultation and treatment, is the ability of the MHNTs to provide a referral service
for those patients that are beyond their capacity to treat. In this regard, the team provided 3042 referrals
in Somali region and 386 in Afar between 2010-2014 (see table 8). MHNTs are acting as a very good link
to health facilities and ensure there is proper referral for the required higher level services). They are
responsible to bring the patients from their site to the ambulance of the woreda. Although the MHNT
vehicles are not supposed to provide referral services when the woreda ambulance is available, they
continue to provide important referral services to the community. This is reported to be one of the cost
drivers of the mobile health teams. The vehicles cover a very long distance to take the patients, which
disrupts their other services.

Evaluation of Mobile Health and Nutrition Teams: Final Report
26
Table 8: referral services provided Afar Somali
2013 284 547
2012 12 1209
2011 2 657
2010 0 319
Total 386 3042
The OTP services made impressive achievements as it has reached good number of pastoralist children,
which would have not been the case without it. Regarding the program quality, the recovery rate
increased over time and reached by 2014, in both regions, more than 80%; while mortality rate of about
1% and a defaulter rate of less than 8% maintained (Table 9). Given the operational context of the MHNT,
these quality indicators are in line with the acceptable quality performance based on the revised national
TFP guideline.
Table 9: OTP services
Total at the
beginning of
the month
New
Admission
Cured Death Referred Defaulter Death
Rate
Defaulting
rate
Afar Region
2014 1295 372 329 0 0 24 0% 1%
2013 2070 1089 680 0 3 54 0% 2%
2012 89 936 15 0 0 0 0% 0%
2011 719 779 232 74 0 120 9% 8%
2010 761 577 317 12 0 92 2% 7%
Somali Region
2014 1770 2093 1780 5 19 240 0% 6%
2013 10763 7209 5970 12 56 536 0% 3%
2012 16054 11631 9288 37 19 697 0% 3%
2011 4306 4810 3251 36 0 581 1% 6%
2010 945 2112 761 13 0 177 1% 6%
Source: MHNT Database

Evaluation of Mobile Health and Nutrition Teams: Final Report
27
Providing immunization services through MHNTs started in 2013 in Afar and in 2011 in Somali Regions.
The performance in Somali region is more visible than Afar. MHNTs reached around 33,000 children with
Penta 3 and OPV 3; around 21,000 children with PCV-3; and more than 18,000 children were fully
vaccinated between 2011-2014 (see table 10).
Table 10: Trend of immunization through MHNTs
Penta-3 OPV-3 PCV-3 Fully vaccinated Vitamin A
0-11 12-24 0-11 12-24 0-11 12-24 0-11 12-24 6-11 12-24
Afar
2014 212 44 212 44 129 24 49 0 0 160
2013 214 251 214 251 47 30 35 0 205 166
2012 0 0 0 0 0 0 0 0 0 0
2011 0 0 0 0 0 0 0 0 0 0
2010 0 0 0 0 0 0 0 0 0 0
426 295 426 295 176 54 290 159 205 326
Somali
2014 7117 2329 7140 2308 7108 2200 3361 1126 2588 2243
2013 8939 2960 8542 3359 7608 2670 4523 1422 3374 2885
2012 5580 2395 5369 2655 1506 424 3701 1961 2685 3907
2011 2305 1324 2014 1176 0 0 2024 1341 1882 2509
2010 0 0 0 0 0 0 0 0 0 0
23,941 9,008 23,065 9,498 16,222 5,294 13,609 5,850 10,529 11,544
Another area of service that MHNT is investing on is on maternal health- ANC, PNC family planning and
delivery services. For these services, there are culturally deep-rooted barriers that hindered utilization;
and service uptake rate is not as good as other services. When we look at trends of TT vaccination again
Somali region managed to reach about 46,000 pregnant women in the last four years, of which only 4400
pregnant women took TT4, showing the inefficiency of the systems as 90% of mothers dropped out from
ANC 1 to ANC 4.

Evaluation of Mobile Health and Nutrition Teams: Final Report
28
Table11: Trend of TT vaccination in Somali and Afar regions
TT Pregnant Women
TT-1 TT-2 TT-3 TT-4
Afar
2014 30 13 22 0
2013 98 89 85 0
2012 0 0 0 0
2011 0 0 0 0
2010 0 0 0 0
128 102 107 0
Somali
2014 11921 8989 5684 1804
2013 17483 13147 5659 1712
2012 10630 7038 3221 526
2011 6027 3737 1550 391
2010 0 0 0 0
46,061 32,911 16,114 4,433
What is also very apparent is that, of those that have gone for TT4, only few mothers come for delivery
services. The fact that MHNTs are only available once in a week in the area have reduced their
performance in delivery. The MHNTs in Afar are not providing maternal delivery services while in Somali
the trend particularly in 2013 and 2014 does seem below what was achieved in 2011 and 2012 (see table
12). The performance also varies from one MHNT to the other. In the best case, the midwife has managed
to assisted 36 mothers deliver over the last three months while also providing delivery services in the
referral health center when called during the night.
Table 12 Delivery Services in Somali Region
Normal Deliveries
through MHNTs
2014 187
2013 386
2012 618
2011 526
2010 325

Evaluation of Mobile Health and Nutrition Teams: Final Report
29
Another important contribution of the MHNTs in this regard is assisting the woredas they are operating
from and help in strengthening and restructuring the community mobilization committees at the kebele
level in Somali region. This is not the case in Afar.
MHNTs services operating six days per week. Our discussion with the woredas and MHNTs clearly stated
that team is working as schedules 6 days per week. The woreda and the community share information on
the provision of services. The community complaints are mostly that in some distance places, the teams
do not arrive on time. But, there are instances where MHNTs for some reason or another leave their site
and do not return back immediately. This was a discussion point in the quarterly review in Afar. It is
therefore necessary to establish punitive sanctions or penalties for the team leaders of MHNTs if they
leave without notification and without circumstances forcing them to stay out. This also calls for
strengthening the supportive supervision and monitoring mechanisms of MHNTs.
Build the capacity of the HEWs: although not their primary objective, they also provide on job training on
case definition, classification (iCCM) and treatment to health extension workers. The HEWs also call the
team when they found cases beyond their skills.
Challenges:
There are many different challenges that compromise the effectiveness of MHNTs, which are well
documented in the quarterly review reports. The most common challenges that have been reported in
the last twenty quarterly review meetings is summarized in Table 13 The most frequent one is the
inadequacy and delay of the different types of supplies (drug kits, nutrition supplies etc.) to MHNTs,
mainly from the regions to the teams, in both regions. This is followed by the lack of functioning cold
chain to provide EPI services and weak and poor reporting by the MHNTs. The other fact that hampers
MNHNTs’ service delivery is movement restriction due to issues related to security in Somali region.

Evaluation of Mobile Health and Nutrition Teams: Final Report
30
Table 13 frequently raised challenges for the performance of the MHNTs in Somali and Afar Regions
#
Challenges Reported in the
Quarterly Review Meetings
Somali Afar
# of times reported
out of 20 RM and
from 24 MHNTs
Comments # of times
reported
out of 12 RM and
4 MHNTs
Comments
1 Inadequate availability of
supplies, drugs, nutrition
supplements etc.)
11 5 EDK Kit sometimes
contains near expiry
drugs; there are times
where amoxicillin syrup,
and paracitamol were not
included in the kit.
2 Lack of functioning cold chain
affecting service delivery
7 3
3 Weak reporting (timeliness,
quality, completeness)
7 Difficult for
communication
4 Movement restrictions due to
security concerns
7 2
5 Services discontinued due
breakdown of vehicles
3 5
6 Lack of skills of the MHNTs to
provide some of the services
within the package
2 Both of them at the
earlier stages of
implementation
2
7 Inadequate supervision 2 3
The service package is defined some time back. The utilization of the services from the mobile team is
improving and in some instances, there is overburden of MHNTs especially due to the overflow of people
that are not within the target woreda due to movement. In such instances, the number of human
resources within the team is reported to be not adequate enough, which sometimes end of in
compromising the quality of care. Given the evolution and maturity of the MHNTs, it is timely to relook at
the service package and revise the MHNT guideline. The revision should relook at the service packages
being offered and the human resources requirement and the accompanying medical supplies. There are
still some service interruptions, as the MHNTs do not always work per schedule. There is frequent
variation of the # of reporting MHNTs sites for different services. This is exacerbated by the fact that there
is a challenge in getting the vehicles maintained on time.

Evaluation of Mobile Health and Nutrition Teams: Final Report
31
3.2. Improving quality of services
One of the major challenges that the MHNTs reported in Afar is that there is a financial barrier at hospital
level for some of the referred patients since the introduction of retention of user fees at the facility level.
This is mainly due to the fact that the regions haven’t developed effective waiver program, as is the case
with other regions that implement health care financing. There is a need to look at the how best this can
be addressed given that MHNTs has spent their time and resources to bring the patient to the hospital.
3.3. Responding to health emergencies
The role of the MHNTs in responding to health emergencies, particularly given the fragile nature of the
health system in pastoralist areas, is reported/observed to be fundamental. They are flexible to move and
help the region to respond in timely fashion. The number of days required for the MHNTs to shift to
emergencies from their regular activity is reported to be only a maximum two days provided there is no
problem of tire for the vehicle and shortage of fuel. Although there is now a shift by the RHBs to look at
it as alternative service delivery modality, the long held view has been that is primarily related to PHEM
services. Indeed, the regions have been using the MHNTs as an instrument to contain health emergencies.
Although the deployment of these teams has offered invaluable services to the communities that were
affected by these emergencies, the evaluation team did not access the evidence and data on the average
annual number of population served with emergency response. One of the major success stories was that
when 9 polio cases was found in one of the woredas, the MHNTs were deployed for three months to work
on polio campaign and contain the outbreak.
Entry into and Exit Strategy from Health emergencies: the evaluation team didn’t find a clear entry and
exit strategy spelt out in the two regions. In Somali region, there are two approaches used to help decide
into emergencies. First, when there is big emergency response decided by multi-sector coordination
mechanisms, MHNTs would also be deployed. Second, when a woreda reported to have emergences-
AWD, malaria, drought or flood- that is above emergency threshold, the MHNTs nearby the affected area
are deployed to investigate and provide evidence on the existence of the emergency. Based on the
findings of the investigation, decisions will be made whether MHNTs should respond to the health
/nutrition emergency. Overall, it is reported that the MHNTs will respond to health emergencies between
a minimums of 15 days to a maximum of 2 months. During these times, the regular services expected from
the team are usually discontinued. In Afar, there are instances that the WoHO reports emergencies that
might have been controlled within the capacity of the woreda. It is therefore necessary to establish an
entry and exit strategy from emergencies to ensure that there is responsible entry and exit.

Evaluation of Mobile Health and Nutrition Teams: Final Report
32
In Somali region, there are a few NGOs that are involved in providing health emergency services in very
limited geographic focus - one or two woredas - with significant levels of funding. The interviews with the
RHBs and Woredas health offices confirmed the fact that it is generally difficult to sustain these services
after the withdrawal of the NGO supported projects. Given that the RHB is viewing MHNTs as an
alternative service delivery strategy, it may be important to consider that strengthening mobile team
should be considered as a mechanism for ensuring sustainability of services after their withdrawal. This
call for the development of a guideline that ensures that NGOs funding health emergencies also invest on
‘responsible withdrawal or exit strategy’ through investing in strengthening MHNTs.
3.4. Capacity building
There is a difference in Somali and Afar regions in using MHNTs as means to build capacity of the health
system. In Afar, MHNTs are only used as service delivery mechanism without having a clear target of
strengthening health posts. On the other hand, MHNTs in Somali region are used to create capacity in
three ways: (i) Pastoralist HEWs are assigned with the MHNTs for a fixed time (three months) to work with
and acquire skills that will be used in the health posts; (ii) 4 integrated MHNTs have been established and
deployed in woredas with primary objective of building the capacities of HPs and woredas; (iii) MHNTs are
used to establish social mobilization groups in the kebeles to help them access to the community.
Overall attaching the PHEWs to mobile health teams is found effective as it builds the skills and capacities
of the HEWs to work in their health posts when their attachment period is finished. The Woreda offices
play an active role in selecting and deploying these PHEWs. It is also reported to have motivated the
PHEWs.
Capacity building Integrated MHNTs (iMNTs) in Somali Region
The primary objective of the iMHTs in building the capacities of the health posts to provide service and
help them and the woreda to manage the services better. IMHNT support to the woreda includes,
development of the annual woreda based plan, especially determining the target population for each of
the services; provision of transport services when for supportive supervision, especially the HEW
supervisor (2 rounds each month), collet and bring data from the health posts, assist in the compilation
process and also support the woreda when there is a shortages of supplies.
The support to the health posts include development of actions plans, documentation and reporting,
provision of on-job training for identified skill gaps in screening, record keeping and some essential
diagnosis and treatment (e.g. on EPI, Malaria, Treatment of emergencies, safe delivery, social
mobilization, etc.); train and provide delivery kits to TBA, provide essential drugs and supplies (all the

Evaluation of Mobile Health and Nutrition Teams: Final Report
33
medications, and nutrition supplements, RUTF); provision of fridges when there isn’t in the health post;
training on how maintain fridges; provision of registers and documentation and referrals of the emergency
cases from the health posts to the referral health center. The team also provides EPI outreach services if
they were not able to access and deploy fridges.
The Woreda offices, the IMHNT teams and interviewed HEWs being supported by these teams all stated
that they have built their capacity, which is reflected in the form of:
Health posts being able to expand their services due to enhanced skills and confidence of HEWs.
In Babile for instances the HPs were not functional before and they have now started providing
services like EPI, ANC and clean delivery; early initiation of breastfeeding. One glaring finding is
that in spite of the efforts made, the uptake of family planning is disappointing due demand side
barriers. In one of the visited health posts, Kora in Babile, there is evidence of increasing interest
in sanitation and construction of latrines.
Table 14: Functionalizing HPs before and after team deployment by woreda, April- June’14
Type of service Functionality before and after team deployment by woreda
Hargelle Shilabo Babili Galadi
Before team
deployment
After team
deployment
Before
deploy
After
deploy
Before
deploy
After
deploy
Before
deploy
After
deploy
Functional HPs 8 8 5 8 9 11 8 11
HPs with EPI 6 8 2 8 6 8 0 7
HPs with ANC 8 8 0 4 8 9 0 7
HPs with timely HMIS
report
1 8 0 7 1 9 0 7
HPs with OTP 8 16 1 4 0 6 0 7
Source: ETHIOPIA SOMALI REGION, HEALTH BUREAU THE 19TH MHNTs QUARTER PERFORMANCE REVIEW
MEETING REPORT (April-June, 2014)
There is regular supply of medicines and other necessary supplies and the stock out rates are very
rare. They have two kits (one for the gap filling-services provided as regular MHNTs) and another
one for supporting health posts.
The referral they provide and their support to the HEWs enable the community to establish and
build trust and confidence on the HEWs.
The major drivers of these successes are reported be explained careful recruitment of members of the
team. Respondents at the regional level stipulated that team members will never been candidate unless

Evaluation of Mobile Health and Nutrition Teams: Final Report
34
they are trained in the basic packages that are provided by the MHNTs, with few exceptions. There are
also clear evidences, unless there are referral cases, the team operates at least once a week in each of the
supported health posts.
IMHNTs started in 2013 and it was expected that facilities would graduate in two years. However, there
is no facility that has graduated from such support so far. The major reason for not getting health facilities
graduate is mainly due to the fact that the basic conditions are not yet met in the region. This is mainly
related to shortage, motivation and retention of HEWs. Most of the HPs have one HEW. There is frequent
turner turnover HEWs for various reasons, mainly upgrades. There are now instances that the HEWs are
moving towards the agriculture sector. Because they know the shortage, some consider themselves
indispensable and very difficult to be influenced and managed by the IMHNTs. Despite the support and
reported improvements in data management, the evaluation team was not able to get the data on
improvements at the woreda and health facility levels. In Babile for instances, of the 4 health posts
supported, three of them are not going to graduate for sometime to come. The IMHNTs also reported
that their incentive is about 40% lower than the MHNTs.
3.5. Operation and management of MHNTs
RHB and UNICEF regularly carry out performance review of the teams through quarterly reviews. The
quarterly MHNTs report (achievements by different categories of services, challenges and lessons learnt)
informs the review meeting. In Somali a total of 20 quarterly review meetings were held which the
evaluation team has gone through. In Afar, about 14 review meetings have been carried out as well. In
Somali, more recently, the reviews have started reporting at the performance of the action points taken
last quarter. While these review meeting have helped to understand the opportunities and challenges and
take action on challenges and constraints, these MHNTs has not set targets as part of the woreda based
plan against which their performance is evaluated. In some woredas, they reported that they have annual
plans but have not used it for performance reviews. This could be due to the difficult circumstances that
they are working under. But it is essential to set some indicative targets for each of the MHNTs as part of
the annual woreda plan to ensure that there is value for money for the investments made.
Our interviews with woreda and health facilities clearly show that they are too reliant and dependent on
these teams that they don’t want them to exit. One of the woredas stated that they might need another
two years of their support. The health extension workers stated that immediate exit from support will
result in:
Stock out of drugs and medical supplies and hence discontinuity of the services being provided to
the community at the moment; Emergency treatment and nutrition may suffer the most;
Evaluation of Mobile Health and Nutrition Teams: Final Report
35
Treatment of emergency cases and referral will suffer;
Community’s confidence on the health posts services and on the HEWs might be eroded as they
have a positive perception to the IMHNTs.
From the above analysis, the RHB should consider introducing IMHNTs only to areas where the minimum
condition is met (two HEW per HP and likely stay due to social commitments in the kebele) and develop
a clear time table and exit strategy by establishing a cut-off point for service coverage for exit at health
post levels. There is also a need to relook as the overall mechanisms of retention of health extension
workers.
The achievements of MHNTs are reported to have influenced the Somali regional government to scale up
this type of initiative in the agriculture and WASH sectors, mainly through government funding. The WASH
mobile maintenance teams contributed increased deep wells functionality and reduction of frequent
borehole dysfunction that costed huge resources for water trucking over the past 2 years in the Somali
region. The health sector should also explore how the Agriculture Bureau managed the regional
government to advocate for government funding.
Evaluation of Mobile Health and Nutrition Teams: Final Report
36
4. MHNTs relevance, effectiveness and sustainability
4.1. Relevance
As is known, the Somali and Afar regions are populated by the pastoralist community whose way of life
characterized by seasonal movement from place to place. Providing PHC services through static facilities
therefore does not fit well to the life style of the community as reported by one of the key informant
interviews in Somali regions, which is also reinforced by many in regional, woreda and community
discussions (see box 1). The pastoralist mother clearly recommended immunization services to follow
their movement.
All the KII and FGDs revealed that
the mobile health teams are able to
reach areas that have not been
reached before by modern health
services due to distance, security
and movement of people. It fits well
with the pastoralist way of life-
movement of the people. It is also
able to work to some degree with
conflict situations. In Afar, some of
the woredas and Kebeles where MHNTs are deployed are places where the woredas are either unable to
attract health professionals for employment or to retain them due to lack of water and other necessities
for attracting human resources for static facilities. There are also documented cases where the MHNTs
reached mothers and other critical patients that have complications and managed to refer them to
nearest health facilities and delivered safely (see box 2)
Box 2: Effective in saving lives A mother was having complications in delivering her child. The community has tried all the means available in their surrounding to save her life and found it difficult to get both the mother and the child safe. So they decided to save the mother at the expense of new born. But before they carry out their decision, the MHNTs arrived in the spot and take her to the nearest facility to deliver. Both the mother the newborn survived. The father of the Son is report have given as a token of appreciation his six goats to the MHNTs.
BOX 1: Views of pastoralist mother on immunizing her child
You are well aware that we are a pastoralist community that we move from place to place to survive. The health facilities are too far and not appropriate for us for getting our children immunized. Unless your immunization programs follow our movement, how do you expect us to immunize our children?

Evaluation of Mobile Health and Nutrition Teams: Final Report
37
One of the measures of relevance is that if communities find it the services of MHNT that important, they
would be willing to cover some part of its costs. Although we have not done a through ‘willingness and
ability to pay’ analysis, the community dialogue clearly show that beneficiaries are willing to contribute a
goat or two per year per household rather than see the discontinuation of the MHNTs services. The first
overall conclusion is that the MHNTS are relevant and reasonably cover the needs of the pastoralist
communities in both regions, more so Somali region.
The evaluation team reviewed the regional HSDP IV and regional performance reports. While there is a
reference to mobile health team as a mechanism to respond to emergencies, there is limited evidence
that clearly stated that it is a priority service delivery modality in the pastoralist context. In this regard,
the finding of this evaluation report reaffirms the finding of the FMOH 2011 assessment, which stated
that
… The Mobile health team in Somali is not considered and presented as an alternative to the
conventional healthcare system, much of the components of which are believed to be
incompatible with the pastoral life style. Rather it appears to be a way of temporarily responding
to a crisis, be it conflict, flood or drought.
Yet, there is adequate evidence demonstrating the fact that the Mobile Health team has registered
encouraging results and has definitely been positively viewed by beneficiary communities. First the Team
took the services to the beneficiaries instead of waiting for them to come to get it, considering their
patterns of movement both routine (seasonal) as well as crisis induced ones. Secondly the service
components included curative treatment, nutrition, education, and distribution of preventive are well
aligned to the services that the heath service has to deliver.
Because the RHBs in both regions were not able to prioritize MHNTs as one of the core service delivery
strategy in the pastoralist region and advocate for it, there is very little political commitment and support
from the FMOH for this innovative service delivery modality. This is mainly associated with the overall
government interest and policy directions to transform the lives of the pastoralist communities through
voluntary resettlement. Second, although there is recognition that it is effectives and relevant to reach
the unreached, given its additional costs related to fuel and per diems, there are justifiable questions
about its cost effectiveness. These two factors are likely to be the main reasons why there is lack of formal
policy on MHNTs as alternative innovative service modality by the two regions and consequently
commitment to allocate more funding from government resources for its functioning.

Evaluation of Mobile Health and Nutrition Teams: Final Report
38
However, although not considered as alternative strategy, there are clear evidences in both regions that
the MHNTs are provided focus and some prioritization during implementation. Table 15 presents the
different reflections of commitment at woreda, RHB and higher levels of government in the two regions.
Table 15: some indicators of government commitment for MHNTs by levels
Levels Commitment measures
Woreda level Have not used the vehicle outside the intended purposes
MHNTs are allowed to work without any restrictions in Somali unless there is a
challenge of their safety. They can move from site to site. The woreda have only
a say during site selection
Support the MHNTs if there are shortages of supplies in both regions
Follow up and change the HEWs every three months in Somali
Monitor their performance and provide supportive supervision in both regions
RHBs Managed and led by PHEM unit within he RHB in both regions
Consistency in undertaking quarterly review meetings
Established own database.
Undertake quarter supportive supervision to MHNTs
Follow up of the MHNTs every week by phone from PHEM
Top
Government
The Somali regional president is reported to be very much supportive of the
MHNTs
Both region has started to put budgets for vehicle maintenance from
government budget and is looking to negotiate more for the coming financial
year
4.2. Effectiveness
Effectiveness is about reaching the meeting the targets set for MHNTs: reaching the unreached through
routine service delivery and while responding to health emergencies when they occur. As clearly outlined
in chapter 3, they were by and large effective in reaching the unreached, maintain provision of service at
their site on regular basis, carried out acceptable level of community mobilization to access services and
respond to emergencies when called up on. One of the major reasons for being effective is the availability
of drugs and medical supplies for the services provided in MHNTs. Even where there is shortage of
delivery, a mechanism is in place to take these supplies either from RHB or from UNICEF’s emergency
reserves, UNICEF field office, prepositions at Jijiga level. The commitment of the human resources

Evaluation of Mobile Health and Nutrition Teams: Final Report
39
deployed and the incentives provided to them help the MHNTs work effectively. Although there is a
standard stating that the MHNTs should provide 800 consultations per moth, this is not well translated
into annual targets for the different services provided by MHNTs (EPI, delivery, FP, OTP etc.) to compare
their performance with. As a result, the evaluation team found it difficult to provide value judgment on
their effectiveness to meet targets. There is also variation around effectiveness of MHNTs and
composition of packages between Afar and Somali regions. The composition services and human
resources are more complete in Somali. They provide delivery services with midwives deployed as part of
the team while this is not the case in Afar. In Afar, delivery is not considered as part of the MHNTs services,
the MHNTs mainly provide referral services.
But effectiveness of iMHNTs in Somali regions, while innovative in thinking, its effectiveness to build the
capacities of woredas and health posts is questionable. This is mainly due to the enabling environment
for attracting and retaining health professional at HP and woreda levels is yet to be put in place.
The MHNTs in Somali region also provided systematic capacity building for pastoralist HEWs as they are
part and parcel of the team for three months while this is not the case in Afar. In Somali region, MHNTs
are capacitating pHEWs through providing opportunities to work with and learn from them. This so fat
seems effective in skill transfer in some of the core functions of the pHEWs. Afar MHNTs should learn
from best practices in Somali in terms of improving service composition and mix of human resources
deployed. In both cases there is a need to re-look at the MHNTs guidelines and revise it to the current
context to make them more effective and efficient.
The MHNTs could have achieved more if some of the limitations and challenges for their functioning are
addressed. Some of the challenges are the following:
The capacity of the PHEWs and the capacity of the woreda to provide supportive supervision
have compromised the effectiveness of the MHNTs.
As the vehicles used for MHNTs served more years, they are requiring frequent maintenance.
The first consequence of this is frequent breakdown of service delivery and some time a longer
period of MHNTs staying out of service. According to the KII at the regional levels, the frequency
and cost of maintenance is increasing. The long process of procurement of maintenance service
using government procedures often exacerbate the delay of getting back to service provision.
The effective way to provide sustainable and efficient services to the population is through the static
facilities. Currently such service provision is much relevant in few woredas. But with the implementation
of voluntary resettlement program, this is expected to be more the mode than the exception in the future.

Evaluation of Mobile Health and Nutrition Teams: Final Report
40
But this will be achieved in the long than in the medium term. MHNTs will continue to be one of the
effective modes of reaching the unreached community in the medium term.
4.3. Efficiency
Efficiency in this context is considered as the use of inputs and processes in delivering MHNT services.
This is therefore related to how communities are mobilized during service provision days, deployment
and utilization of team members, availability of medicines and supplies and integration towards
government health systems (PHC, planning and M&E systems and Supply management systems). The
following highlights the successes and challenges in enhancing efficiency.
The efficiency of MHNTs varies. Two (8%) out of 24 teams in Somali operate for 12 months , while 11
(46%) of the teams operate 11 months of the year while 11 others (46%) only operate between 2 -10
months. The main reason being sited in the review meetings is the non-functionality of vehicles for
providing the service.
Table 16 # of months each of the MHNTs was working, 2011-2014
S.N. Woreda (Zone) 2011 2012 2013 2014 Total
1 Maymuluko (Fik) 11 11 10 11 43
2 Danot (Warder) 11 9 10 12 42
3 Duhun (Fik) 12 10 11 9 42
4 Gunagedo (Degehabur) 9 11 10 11 41
5 Segage (Fik) 9 11 10 11 41
6 Shilabo (Korahe) 11 9 10 11 41
7 Hamero (Fik) 5 11 11 11 38
8 Degahmado
(Degehabur)
5 10 11 11 37
9 Dobawen (Korahe) 12 9 5 11 37
10 Galadi (Warder) 5 11 8 12 36
11 Selahad (Fik) 6 10 11 9 36
12 Legahida (Fik) 5 11 10 7 33
13 Marsin (Korahe) 5 10 7 9 31
14 Mustahil (Gode) 12 - 8 11 31

Evaluation of Mobile Health and Nutrition Teams: Final Report
41
15 Kubbi (Fik) 5 11 5 9 30
16 Daratole (Warder) - 8 10 11 29
17 Goljano (Jijiga) - 8 10 11 29
18 Birkot (Degehabur) - 8 10 10 28
19 Babile/Dhandhamane
(Jijiga)
- 6 10 11 27
20 Kelafo (Gode) 6 - 7 10 23
Raaso (Afder) 1 7 9 4 21
21 Ferfer (Gode) 11 3 - 2 16
22 West-Ime (Afder) 10 - - 2 12
23 East-Ime (Gode) - - - 2 2
Garbo (Fik) 11 9 10 9 39
Fik (Fik) 5 9 10 9 33
24 Hargele (Afder) - 2 9 9 20
Parallel systems: One of the mechanisms of enhancing efficiency is through enhancing integration of the
MHNTs into routine system. Given the nature of the MHNTs, service delivery remains parallel, as it has to
reach mobile community. Although there are cases that some of the MHNTs staff (midwifes) are serving
in heath facilities at night, the human resource deployment follows the service delivery model. They are
using their own social mobilization strategy to reach the community. The planning and M&E systems are
aligned to the regional timelines but use data collection tools, including the establishment of own data
base that this evaluation benefitted from. However, there are technical support supervision and own
database to ensure that MHNTs are followed properly.
Strong monitoring and evaluation: the MHNTs are closely monitored and followed up by the health bureau
in both regions. There are quarterly review meetings, where the woreda Administrator, head of the
woreda health office and MHNTs as well as UNICEF attend. The challenges are raised and actions are
agreed up on. However, although the MHNTs in the two regions reported to have annual plans, they are
not used to use it to compare their achievements against. Given that they know the estimated population
of the woreda, it is essential they develop an annual plan for services they are offering to the population.
The Somali regions do have social mobilizers as part of the MHNTs while this is not the case in Afar. While
the MHNTs do follow the population in Somali, there are isolated challenges related to tracking the
movement of people in some cases in Afar.
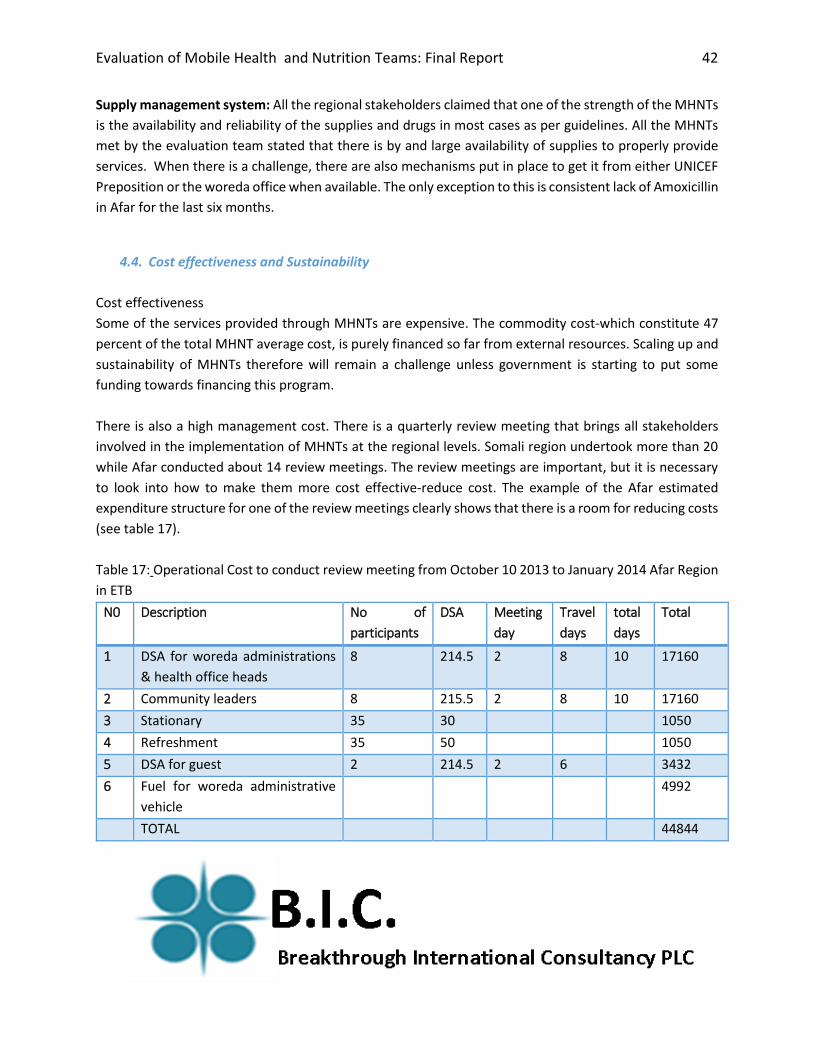
Evaluation of Mobile Health and Nutrition Teams: Final Report
42
Supply management system: All the regional stakeholders claimed that one of the strength of the MHNTs
is the availability and reliability of the supplies and drugs in most cases as per guidelines. All the MHNTs
met by the evaluation team stated that there is by and large availability of supplies to properly provide
services. When there is a challenge, there are also mechanisms put in place to get it from either UNICEF
Preposition or the woreda office when available. The only exception to this is consistent lack of Amoxicillin
in Afar for the last six months.
4.4. Cost effectiveness and Sustainability
Cost effectiveness
Some of the services provided through MHNTs are expensive. The commodity cost-which constitute 47
percent of the total MHNT average cost, is purely financed so far from external resources. Scaling up and
sustainability of MHNTs therefore will remain a challenge unless government is starting to put some
funding towards financing this program.
There is also a high management cost. There is a quarterly review meeting that brings all stakeholders
involved in the implementation of MHNTs at the regional levels. Somali region undertook more than 20
while Afar conducted about 14 review meetings. The review meetings are important, but it is necessary
to look into how to make them more cost effective-reduce cost. The example of the Afar estimated
expenditure structure for one of the review meetings clearly shows that there is a room for reducing costs
(see table 17).
Table 17: Operational Cost to conduct review meeting from October 10 2013 to January 2014 Afar Region
in ETB
N0 Description No of
participants
DSA Meeting
day
Travel
days
total
days
Total
1 DSA for woreda administrations
& health office heads
8 214.5 2 8 10 17160
2 Community leaders 8 215.5 2 8 10 17160
3 Stationary 35 30 1050
4 Refreshment 35 50 1050
5 DSA for guest 2 214.5 2 6 3432
6 Fuel for woreda administrative
vehicle
4992
TOTAL 44844

Evaluation of Mobile Health and Nutrition Teams: Final Report
43
The total expenditure for the MHNTs in Somali region supported by UNICEF between 2012-2014 was $
3,946,410.48. Of this, 47% was used for supplies, 29% for operation cost (per diems) and 24% for costs
related to transport (see table 20).
Table18: supplies distributed in the last two years by UNICEF
Unit Annual Qt. In two year
EDK Kit 212 424
IEHK 2006, kit, 3-renewable
medical supplies
Kit 106 212
RUTF 150 sachet per carton
Carton 4480 8960
If we take only the running cost (operations and transport)2, the unit cost for each consultation ranges
from $1.13 in 2012 to $1.93 in 2014. We don’t have the details of the supplies on which service type they
were used and cannot allocate it to different services (EPI, OTP, etc.) in each year. The information we
obtained only shows quantities in two years, which cannot be used for unit costs calculations. However,
part of the reason for the increasing unit costs over time is changes from the DSA /fuel rates over time.
DSA changed increased from150 ETB in 2012 to 210 ETB in 2014. Fuel costs have also increased over time
during this period.
But if we used the consultations as a proxy for all services and estimate the total unit cost including
commodities, the unit cost is estimated from $1.41 in 2012 to $3.55 in 2014. The cost of maintaining and
managing older vehicles as means to deliver services could have contributed to increased unit costs.
Table 19: estimated unit costs per consultation
2012 2013 2014
Total unit cost per consultation 1.41 3.82 3.55
Unit running cost/consultation 1.13 1.73 1.93
2 While operational cost include the capacity building training, DSA for HWs, monitoring and
evaluation transport cost include rented vehicles cost , maintenance and fuel for RHB vehicles, transport of MHNT supplies . Both costs are transferred to and managed by regions

Evaluation of Mobile Health and Nutrition Teams: Final Report
44
One of the issues that contribute to sustainability is the ability of the RHBs to motivate and retain health
workers especially the PHEWs in the area after being supported and the capacity built by the MHNTs.
There is variation between Afar ad Somali regions in terms of using resources effectively. The Afar MHNTs
seem to be less cost effective for the following reasons: (i) the MHNTs are staffed by more qualified human
resources (4 in Afar 2 in Somali); (ii) their service packages are less (e.g. does not include delivery); and
(iii) they do not have an in-built capacity building objective to sustain the service through the health posts.
Some of the DPs we have talk to stated that they are committed to support this program for a maximum
of medium term (3-5 Years); but are considering to work towards ‘responsible exiting’ from MHNTs after
three to five years. Our discussion with the RHBs and partners at the regional level especially in Somali
stated that if there were withdrawal of funding for MHNTs, government would be forced to finance some
of the MHNTs as it is accepted as effective strategy. This clearly shows that the RHBs will need to develop
health systems strengthening and sustainability plan towards MHNTs.
5. Financing of the MHNTs
The MHNTS is financed through two major funding sources. First government in both regions covers the
costs of salaries of the MHNT members. It has also started, especially in Somali region, to allocate some
maintenance costs for vehicles. Second, external resources cover the costs of DSA, fuels, supplies and
procurement of vehicles. Although different INGOs were financing MHNTs in both regions, currently, the
external financing is being mobilized and financed through UNICEF.
UNICEF mobilized the resources required for MHNTs from different sources and in different mechanisms
based on the number of MHNTs operational. The total resources mobilized and used from UNICEF varies
from $508 108 to $2.12 million in 2013 (see table 20).
Table 20: UNICEF’s funding of MHNTs by different categories
2012 2013 2014 Total %
Supply 114,239.96 1,159,906.53 575,311.32 1,849,457.81 47
Operational 187,816.29 507,823.16 447,566.16 1,143,205.61 29
Transport 278,052.36 452,173.04 223,521.66 953,747.06 24
Total 580108.61 2,119,902.73 1,246,399.14 3,946,410.48 100
Source: UNICEF.

Evaluation of Mobile Health and Nutrition Teams: Final Report
45
We requested the Somali RHB to give us data on the amount of resources allocated and used for salaries
and maintenance but so far the evaluation team has not received information and we are unable to
calculate the share of external and domestic financing in total MHNT financing. However, from the
discussion we had in both regions, the share of government financing is not that significant reflecting the
fact MHNTs are not considered as an alternative service delivery strategy and hence are not a priority as
other programs in terms of financing.
Table 21: Financing of MHNTs in Afar
Expenditure Items 2012 2013 2014
Salary of health workers 688,560.00 841,074.00 922,074.00
Per diem of health
workers
499,050.00 978,923.00 896,100.00
Cost for commodities and
supplies
806,060.00 877,080.00 892,845.47
Car Fuel 257,350.00 921,932.00 233,300.00
Maintenance Cost 868,090.00 - 1,102,616.67
Car rent 2,664,000 2,664,000 3,420,000
Total 3,119,110.00 3,619,009.00 4,046,936.14
Source: Afar RHB
One of the major issues raised by all sources of UNICEF funding (Australia, USAID and EU) is that while
they are convinced that MHNTs are relevant to the community needs and will continue to contribute to
its financing for some time to come, there is a need for some responsible withdrawal as it cannot be
financed indefinitely. This could be facilitated if RHBs and UNICEF develop and implement a clear exit
strategy that will show either government is taking it as alternative strategy and start financing it, or
replace it with static facilities. This requires for the RHBs and their regional cabinet to examine and decide
if and how to make the MHNTs as one of priorities for increasingly taking share of the cost of their
financing.

Evaluation of Mobile Health and Nutrition Teams: Final Report
46
6. Major findings and recommendation
6.1. Findings
Overall the MHNTs are relevant to the pastoralist and weak health infrastructure context of Somali and
Afar regions and could be considered as a transitional alternative strategy for health service delivery in
these two regions. MHNTs were effective as compared to the static facilities in creating access to
previously unreached population groups for health services. They MHNTs were able to provide:
158,758 and about 1.7 million consultations in Afar and Somali regions with 3 and 24 MHNTs respectively over the last 4 years
3042 referrals in Somali region and 386 in Afar between 2010-2014
OTP to a good number of pastoralist children, with the recovery rate rate of more than 80%; mortality rate of about 1% and a defaulter rate of less than 8%;
around 33,000 children with Penta 3 and OPV 3; around 21,000 children with PCV-3; and more than 18,000 children were fully vaccinated between 2011-2014;
But the investment of MHNT is investing on is on maternal health- ANC, PNC family planning and delivery services is not effective due to deep-rooted cultural barriers that hindered utilization. Service uptake rate is not as good as other services. MHNTs reached in Somali region about 46,000 pregnant women with TT vaccination in the last four years, of which only 4400 pregnant women took TT4, and 2042 mother have been assisted with delivery services showing the inefficiency of the systems as 90% of mothers dropped out from ANC 1 to ANC 4 and delivery.
The MHNTs has also been effective in responding to health emergencies and saving lives. However, clear
triggers of entry and exit from the emergencies are not always clear. MHNTs has been also effective in
capacity building of Pastoralist HEWs in Somali region, while this is not the case in Afar and IMHNT in
Somali region. The IMHNTs objective to strengthen health posts and woredas in Somali regions is good
initiative, but the the environment within which it is operating (inadequate woreda health staff and health
extension workers and frequent turn over) hamper the realization of its objective of graduating woredas
and health facilities after building their capacities.
The services provided by the MHNTs to the community by and large remain adequate in terms of scope
and address priority health services especially in Somali region. The perception of the community about
the effectiveness and reach of the MHNTs is quite positive. There is universal acknowledgement of the
value of MHNTs in reaching the unreached by the RHBs, woreda health officials, facility heads, community
discussions and and their role in some cases in introducing modern health care services. It has started
influencing health seeking behaviors. The FDGs with the community members revealed that the
community is willing to contribute a goat per year per household rather than seeing the MHNTs
discontinue their operation due to lack of finance.

Evaluation of Mobile Health and Nutrition Teams: Final Report
47
The evaluation team was unable to compare the efficiency of the MHNTs and static facilities in the same
woreda, due to lack of disaggregate outcome and financing data. Overall, the unit cost for providing
consultation and treatment by MHNTs increased from $1.41 to $3.55 in 2014 and of which the unit
running cost was $1.3 and $1.9 respectively in these years. This clearly shows that non running costs are
contributing more in increased costs recently. There are also inefficiencies as evidenced by the fact that
only 8% of the MHNTs were able to operate the full 12 months while all the rest were unable to do so.
There are some success and constraining factors in the functioning of MHNTs. The success factors include:
There is ownership of MHNTs by RHBs and the community: they are being managed and run by
the RHBs. The RHBs instituted its own review and supportive supervision visits. In Somali region,
MHNTs are politically supported to provide service in insecure woredas. The community
perception and values on MHNTs services is quite positive and in our discussions with leaders,
they have expressed willingness to contribute at least a goat to finance their operation rather
than seeing it discontinued due to lack of financing. They are also aware of their schedules and
report to the woreda office when MHNTs do not show up.
Both regions take care in selecting health professionals that are deployed in MHNTs. In the
majority of cases, heath professionals with better skills and capacity as well as commitment are
recruited and deployed. When skill gaps are observed, training is provided before deployment.
The regions carry out regular performance reviews. The achievements, challenges as well as
actions to be taken are presented and discussed in the presence of the MHNTs, woreda officials
and the regional bureau. There is more active follow up of actions agreed upon in the subsequent
review meetings in Somali region.
There is regular availability of kits and supplies for MHNTs. The availability of supplies is reported
to be much better in MHNTs than static facilities. When there are occasional shortages,
mechanism is in place to fill the gaps either from Woredas or UNICEF.
MHNTs is serving as alternative service delivery modality to pastoralist community at the moment. Its
potential however has not been fully exploited as it has not been classified as so either by the RHBs or the
FMOH. Although their value in terms of relevance, effectiveness of reaching the unreached and efficiency
of resource use and commitment of the team members is well appreciated by all, it has not been seen or
reflected as a major priority and as alterative service delivery strategy by the regional government’s
strategies and and hence are not well resourced from the regular government allocation. There is
Inadequate political buy in by Federal and regional levels as an alternative service delivery strategy. While
the MOH is exploring innovative mechanisms to deliver services to pastoralist community, it is yet to
approve and support it as an alternative model. Even when one explores the regional health strategic
plans, MHNTs are considered as emergency response mechanism rather than alternative service delivery

Evaluation of Mobile Health and Nutrition Teams: Final Report
48
model. As a result of these, the FMOH isn’t contributing to the financing of the MHNTs and the RHBs are
not able to mobilize adequate funding from the regional allocations. As a result, the functionality and
operation of the MHNTs is highly dependent on the external funding. Given the number of years that
some of the DPs are financing MHNTs, their continued commitment and financing is not certain. Unless
sustainability and exit plan are agreed and implemented, a sudden withdrawal is likely to erode the gains
made by the MHNTs. The woredas being supported by the MHNTs have developed dependency syndrome
and are not willing to allow MHNTs to exit. Some woredas have managed to reverse decisions to exit
politically. The vehicles used for MHNTs are becoming older and the cost of maintenance is increasing. So
far, there is no vehicle replacement strategy in place as the case is with ambulances deployed by the
FMOH. The quality and availability of maintenance service in the regions is inadequate and very long time
is required for maintenance, with long service disruption time. There are no standby cars or resources to
rent additional cars to ensure continuity of service when needed.
6.2. Recommendations
Government
Consider MHNTs as an alternative PHC service delivery strategy for medium term in the next regional
health sector transformation plan. Currently the government’s main strategy is to encourage pastoralists
to voluntarily settle and provide facility-based services. This is a correct priority over the long term.
However, there will be people that are moving from place to place and will not access services in the short
and medium term. There is also a need to work with the FMOH and generate evidences of different
modalities of alternative service delivery for the pastoralist context. If MHNTs is found the best options
available, MHNTs could evolve as a transitional alternative service delivery strategy for pastoralist areas
to reach the underserved. This calls to clearly put it as one of the priorities to enhance access to PHC
rather than emergency response. This may include development of the strategies on how to integrate
other PHC services with the MHNTs services. It also calls for ensuring that it is led and managed by the
PHC unit rather than PHEM. The RHBs should develop a clear strategy on how they are going to use MHNTs
as an alternative strategy.
Ensure buy-in of the alternative service delivery strategy by the regional cabinet and FMOH. Given
MHNTs are credible and politically driven starting from the president, it may be important to get the
alternative strategy approved by the regional cabinet. The strategy should also provide evidence and
justification on why and how much government should finance MHNTs as transitional service delivery
model. This will help the RHB to negotiate and budget a reasonable share of government resources to
MHNTs.

Evaluation of Mobile Health and Nutrition Teams: Final Report
49
Consider innovative mechanisms to mobilize additional external resources for MHNTs. Once the region
has endorsed MHNTs as alternative strategy and budget for it, the RHBs can use the budget as ‘’pooled
fund’ or ‘matching fund’ to mobilize additional funding from interested partners. This will also include the
development sustainability plan for MHNTs in the long term and how the region will transit from MHNTs
to static facilities. Given that these regions are often characterized by frequent health emergencies, it may
also necessary to consider financing MHNTs as a one of the strategies for exiting emergencies by
international agencies. If FMOH is convinced about its ability to serve as alternative strategy, RHBs should
leverage the equity agenda of the Heath Sector Transformation Plan to mobilize additional predictable
resources through the FMOH.
Look for alternative strategies for strengthening woreda and HP systems instead of the using IMHNTs:
Indeed, the IMHNTs have strengthened health service delivery at the HP and supportive supervision at
the woreda levels. The potential for IMHTs to enable facilities and woredas to graduate is constrained by
the enabling environment. Strengthening the health systems is very important and critical but it may be
also important to re-look at whether the IMHNT is the right strategy for capacity development.
Revise the Package based on the visions and directions as alternative service delivery strategy: there is
evolution in service delivery in the Ethiopian Heath care delivery system as more of the curative services
are being provided at the heath post levels in the agrarian context. The MHNTs is replacing such a system
in the pastoralist context. If the MHNT model is accepted as an alternative service delivery strategy, it is
necessary to revisit the package and its human resource requirements and make it more affordable.
Exit strategy: the RHBs should work with the main partners to develop an Exit strategy that will outline
on how government will take increasing responsibility of financing MHNTs and allow some partners either
to exit from the financing and reduce the scale of their investment in the medium and long term.
Development partners including UNICEF
Responsible withdrawal: The MHNTs were effective in saving lives and reach marginalized population
groups. Immediate reductions of external resources are like to reduce the gains made so far in providing
OTP, immunization and consultation services. The support given to the MHNTs should continue until its
status, as an alternative model of service delivery is known. Partners that have been investing on MHNTs
should develop with the RHBs on exit strategy that clearly outlines the responsibilities of the RHBs and
DPs, which will allow responsible withdrawal.
Evaluation of Mobile Health and Nutrition Teams: Final Report
50
Continue ensuring the regular supplies EDK and supplies: UNICEF has been able to ensure that the
needed kits and supplies are available for MHNTs. All MHNTs stated that the supplies are by and large
available to run the services. It is there necessary for UNICEF to continue investing on ensuring he
availability of kits and supplies. The move towards integrating it to government supply system will not
work at the moment given the high stock out rates in static facilities.
Advocate and negotiate with RHBs to make MHNTs as transitional strategy and for more resource
allocations: UNICEF and other DPs supporting MHNTs should enhance their engagement and advocacy
with the FMOH and regional RHB to help MHNTs evolve as an alternative strategy for service delivery.

Evaluation of Mobile Health and Nutrition Teams: Final Report
51
1. Annexes:
Annex 1: Semi-structured Interview Guide for national level KII
Brief: We are an independent team evaluating the MHNTs an innovative approach for reaching
the underserved. RHBs and UNICEF wishes to know about the progress thus far and extract
lessons and good practices for the future of the program. We would like to learn your opinions on
the program, what worked and what did not work, and we assure you of our confidentiality.
1. Name of interviewee
2. Organization__________________________
3. Position in the organization? ___________________________________
4. How long have you participated in the program? ___________________
(For the evaluator – Please read relevant documents before the interview and customize the
questions.) What was their role supposed to be? Were they involved in planning and how? Were
they involved in the implementation and monitoring? Then include the questions on the list below
as possible.
Example:
2. What are the policy context and place of MHNTs in particular in Somali and Afar
Regions? Please describe the commitment of the government in leading and managing
the MHNT services? Please support evidence for this in terms of:
MHNTs and regional HSDP IV and service delivery strategy
Adopting policies and strategies
Linking MHNTs with other intervention
Allocating resources (human resources, budget)
Taking leadership and coordinating of partners
Integrating MHNTs in the overall government systems and procedures
Putting strategies for future sustainability
3. What are the major accomplishments of the program? What worked well?
Social mobilization and behavioral change
Screening and case finding
Evaluation of Mobile Health and Nutrition Teams: Final Report
52
Access to care
Quality of care
Integration with other programs and overall health systems management
Planning, management and M&E including HMIS
How did it work? What factors played a role? What are the good practices?
Enabling environments (policy, commitment, organization and management, resource
mobilization, etc.)
(For the evaluator: Probe more deeply according to the information offered by the interviewee:
What was the evidence of success? Why was it a success? What contributed to the success?
Who was instrumental in promoting success? Who else should we interview regarding the
successes?)
1. What are the major problems? What did not work well, what needs improvement? What
lessons would you like to share?
Community mobilization
Quality of care in the face of movement from one place to another
Challenges in the referral facilities
Availability of commodities and supplies in the MHNTs
Sustainability
Government resource allocation
(For the evaluator: Probe more deeply according to the information offered by the interviewee:
What was the evidence of things not working properly? What were the constraints that caused
the problem? What standards and agreements were not followed? What exactly prevented them
from being followed? Who else should we interview regarding these issues?)
5. What are your recommendations for improvement of the functioning of the MHNTs in
the future? What are your recommendations for its scaling up and expansion of the in the
regions?
On the relevant issues raised under 2 and 3
(For the evaluator: Get as much detail as possible on the recommendations and their rationale.)
Do you have any documents that are useful for this evaluation? __________________
Specific Questions to bring up to probe more deeply

Evaluation of Mobile Health and Nutrition Teams: Final Report
53
Relevance
Did the MHNT services and their provision meet the needs of community?
Number and type of emergency response events (hazards) have been addressed in recent
years (2004, 2005, 2006)
Were the planned and implemented technical and organization support activities relevant
to the planning, implementation and management of MHNTs?
How relevant are the MHNTs service delivery models for the pastoralist contexts in
Ethiopia? What are major challenges of reaching the most vulnerable groups in these
different contexts?
Effectiveness:
Were the outcome and output targets planned in MHNTs programming achieved (regional
coverage)? What are the lessons learnt from the MHNTs-balance between access and
quality?
Did the program receive the technical/organizational assistance planned? How adequate
was the quality and quantity?
How was the quality of the services (meeting the guidelines) of MHNTs? Were MHNT
standards respected? How well the MHNTs meets the standards set in the regional
guidelines? What needs to be done to improve the quality of MHNTs?
Do you think that there are enough trained health workers for MHNT? What should be done
to strengthen the capacity of health workers?
How well is the referral link functioning? What are the challenges and what can be done to
strengthen the linkage and synergy between these two programs?
What factors contributed to the achievement (successes or lack of success) desired and
planned outcomes? What issues constrained the achievement of outcomes; were they
addressed satisfactorily did the MHNTs confront any management issues? What
improvements were made over time and how did they affect results? Did all involved know
their roles?
What, in your view, is the counter-factual? What would things look like without MHNTs in
terms of emergency response and health service delivery?
What is the overall of impact of MHNTs in strengthening government health service delivery
mechanisms? How much are your plans and program implementation is:
o Using government systems (planning, fund management, monitoring and
evaluation)
o Delivering through the support of public health facilities (hospitals, health
centers and health posts)

Evaluation of Mobile Health and Nutrition Teams: Final Report
54
o Using human resources, infrastructure, referral pathways, and procurement
and logistics management system?
What are the sources of funding for MHNT activities? To what extent are the resource
mobilized to support to an effective implementation? What do think level of funding by the
government? What is the contribution of your agency? How well were they used? Do you
feel there is adequate funding to scale up MHNTs? Are there any specific plans or ideas
for increasing funding?
Access to financial and technical support
Who are the major financiers of the MHNTs in terms of:
o Vehicles
o Equipment for treatment
o Drugs and medical supplies used in the MHNTs
o Cost of human resources
o Training and capacity building (get the quantitative data)
Efficiency
Where do you think cost efficiency could be improved? How could funds be saved with the
same result?
Coordination: what was the development and implementation partners support mechanisms
at regional levels, and what effects have they had in the scaling up process? What do you
perceive as the major strengths of the current system/mechanism for coordinating MHNT?
And how could they be done better? Was coordination worth doing given its associated
transaction cost? What are the opportunities to link MHNT with other health service delivery
and veterinary services?
How much is the planning, resource allocation, management and supervision of MHNT is
integrated in the overall government systems and process?
MHNT and supply systems: How far the MHNT supplies are procured through the use of
government procurement and distribution systems? What are the type of MHNT supplies
(capital equipment, drugs,) that are being procured through the use PFSA procurement
processes and procedures? What are the major supplies that are being procured outside
the procurement procedure of PFSA? What are the main reasons for doing so? Has MHNT
contributed in any way for strengthening the procurement and distribution process? If not,
what do you think are the major reasons? What do you thing MHNT partners shall do to
work with and strengthen the country’s procurement and distribution system? If yes, what
is its contribution in terms of

Evaluation of Mobile Health and Nutrition Teams: Final Report
55
o Strengthening procurement and distribution systems
o Availability of health commodities
o Quality of drugs and medical supplies
o Strengthening accountability and transparency
What are the major achievements in MHNT information system and reporting? Has it been
integrated into the routine health information systems? What needs to be done to improve
the MHNT information system or its integration?
Sustainability
How has scale-up been planned and implemented? What do you perceive as the major
success factor and barriers for MHNT? What needs to be done to improve the scale up with
quality? What do you think the ownership of MHNT by the government at different levels?
o Integration with overall government wide management process including
resource allocation
o Integration with government service delivery mechanisms
o Capacity building in the public sector for planning, and managing
implementation
What is the trend of government and DP allocation to MHNT? Is the government and
community increasingly taking care more of the financing of MHNT? If not what do you think
should be done by government, development partners and communities to ensure that they
(government and communities) take more of the responsibility of financing the MHNT?
Annex 2: Semi-structured Interview Guide for Development and Implementing Partners
Brief: We are an independent team evaluating the MHNT program in Somali and Afar regions.
We would like to learn your opinions on the program, what worked and what did not work, and we
assure you of our confidentiality
Name of interviewee
Organization__________________________
Position in the organization? ___________________________________
How long have you participated in the program? ___________________
(For the evaluator – Please read relevant documents before the interview and customize the
questions.) What was their role supposed to be? Were they involved in planning and how? Were
they involved in the implementation and monitoring? Then include the questions on the list below
as possible.
Example:
2. What are the major accomplishments of the program? What worked well?

Evaluation of Mobile Health and Nutrition Teams: Final Report
56
Social mobilization and behavioral change
Nutrition screening and case finding
Access to care
Quality of care
Integration with other programs and overall health systems management
Planning, management and M&E including HMIS
How did it work? What factors played a role? What are the good practices?
Enabling environments (commitment, organization and management, resource
mobilization, etc.)
(For the evaluator: Probe more deeply according to the information offered by the interviewee:
What was the evidence of success? Why was it a success? What contributed to the success?
Who was instrumental in promoting success? Who else should we interview regarding the
successes?)
3. What are the major problems? What did not work well, what needs improvement? What
lessons would you like to share?
o Quality of care
o Sustainability
o Government resource allocation
o Community involvement and ownership/gaps in community social protection
mechanisms
(For the evaluator: Probe more deeply according to the information offered by the interviewee:
What was the evidence of things not working properly? What were the constraints that caused
the problem? What standards and agreements were not followed? What exactly prevented them
from being followed? Who else should we interview regarding these issues?)
4. What are your recommendations for improvement of the program? What are your
recommendations for scale up and expansion of the program?
On the relevant issues raised under 2 and 3
(For the evaluator: Get as much detail as possible on the recommendations and their rationale.)
Do you have any documents that are useful for this evaluation? __________________
Questions to bring up as appropriate and to probe more deeply.
Relevance
Did the service delivery meet the needs in the community?
Evaluation of Mobile Health and Nutrition Teams: Final Report
57
Were the planned and implemented technical and organization support activities relevant
to the planning, implementation and management of MHNT?
How available and responsive are the MHNTs during health emergencies?
Effectiveness:
Were the outcome and output targets planned in MHNT programming achieved (national
or regional coverage)? What are the lessons learnt from the rapid scaling up of MHNT-
balance between access and quality?
Did the program receive the technical/organizational assistance planned? How
adequate was the quality and quantity?
How was the quality of the services (meeting the MHNT guidelines)? Were MHNT
standards respected? How well the program achieves the standards? What needs to be
done to improve the quality of MHNT?
Do you think that there are enough trained health workers at the different levels
(regional, woreda, and MHNT teams) to implement MHNT? What should be done to
strengthen the capacity in the country? What support does your agency provide to build
the national capacity for MHNT?
How effective are the MHNTs in responding to health emergencies?
o Flexibility to be mobilized during emergencies
o Trends and magnitude of emergency services provided through MHNTs as
against static facilities
o Existence of entry and exit strategies to enter and exit emergencies
o Impact of emergency deployment on the regular services of MHNTs
How well is the referral link functioning? What are the challenges and what can be done
to strengthen the linkage and synergy between the MHNTs and their immediate referral
facilities?
What factors contributed to the achievement (successes or lack of success) desired and
planned outcomes? What issues constrained the achievement of outcomes; were they
addressed satisfactorily did the program confront any management issues? What
improvements were made over time and how did they effect results? Did all involved
know their roles?
What is the overall of impact of MHNT in strengthening government health service
delivery mechanisms? How much are your plans and program implementation is:
o using government systems (planning, fund management, monitoring and
evaluation)
o Delivering through the support of public health facilities (hospitals, health
centers and health posts)

Evaluation of Mobile Health and Nutrition Teams: Final Report
58
o Using human resources, infrastructure, referral pathways, and procurement
and logistics management system?
What are the sources of funding for MHNT activities? To what extent are the resource
mobilized to support to an effective MHNT implementation? What do think level of
funding by the government? What is the contribution of your agency? How adequately
have the funds been distributed among activities? How well were they used? Do you
feel there is adequate funding to scale up MHNT? Are there any specific plans or ideas
for increasing funding?
Provision financial and technical support
What type of financial support do you provide for MHNT program in terms of:
o Vehicles
o Drugs and other supplies procurement and distribution (get the quantitative data)
o Equipment (get Quantitative data)
o Paying for salaried and DSA
o Training and capacity building (get the quantitative data)
Do you provide technical assistance to the MHNT program implementation? How do you
value your support in terms of its relevance, quality and adequacy? What do you comment
on the technical and financial support provided by UNICEF?
Efficiency
Where do you think cost efficiency could be improved? How could funds be saved with
the same result?
Coordination: What do you perceive as the major strengths of the current
system/mechanism for coordinating MHNTs? What do you perceive as the major aspects
of the coordination of MHNT that should be improved?
How much is the planning, resource allocation, management and supervision of MHNT is
integrated in the overall government systems?
What are the major achievements in MHNT information system and reporting? Has it
been integrated into the routine health information systems? What needs to be done to
improve the MHNT information system or its integration?
Sustainability
Given the expansion of the PHC facilities, do you think there is a need to scale up MHNTs?
If yes, how should the scale-up be planned and implemented? What do you perceive as
the major barriers for scaling-up MHNT? What needs to be done to improve the scale up
with quality? What do you think the ownership of MHNT by the government at regional
and woreda levels?

Evaluation of Mobile Health and Nutrition Teams: Final Report
59
o Integration with overall government wide management process including resource
allocation
o Integration with government service delivery mechanisms
o Capacity building in the public sector for planning, and managing implementation
What is the trend of government and DP allocation to MHNT? Is the government and
community increasingly taking care more of the financing of MHNT? If not what do you
think should be done by government, development partners and communities to ensure
that they (government and communities) take more of the responsibility of financing the
MHNT?
Annex 3: Semi-structured Interview Guide for regional and Woreda health offices
Brief: We are an independent team evaluating the MHNT in Somali and Afar regions. We would
like to learn your opinions on the program, what worked and what did not work, and we assure
you of our confidentiality
2. Name of interviewee
3. Organization__________________________
4. What is your role in MHNT? ___________________________________
5. How long have you participated in the program? ___________________
(For the evaluator – Please read relevant documents before the interview and customize the
questions.) What was their role supposed to be? Were they involved in planning and how? Were
they involved in the implementation and monitoring? Then include the questions on the list below
as possible.
Relevance
Did the MHNT services and their delivery models meet the needs in the community and their
ways of life region? Is it aligned with the HSDP IV? How it was reflected in the RHB’s plans like
Health Sector annual and five-year plan?
Did the program receive the technical/organizational assistance planned? Please describe the
federal or regional support for MHNT to the lower levels? How adequate was the quality and
quantity?

Evaluation of Mobile Health and Nutrition Teams: Final Report
60
Does the RHB has the capacity to manage MHNT like in terms of competencies, planning, and
managing and skill and handling the logistic?
Coverage
Who are benefiting from MHNT services? Ask about boys/men and girls/women, who benefited
more? Why? Who were not benefited? Why?
What were the main criteria to select woredas to initiate MHNT? Are there any biases?
Effectiveness
Do you think that there are enough trained health workers at regional level to implement MHNT?
What should be done to strengthen the capacity in the regions and woredas? How well did the
training and capacity development meet the needs?
What are the major accomplishments of the program? What worked well? How did it
work? what factors played a role? What are the good practices?
How effective are the MHNTs in responding to health emergencies?
o Flexibility to be mobilized during emergencies
o Trends and magnitude of emergency services provided through MHNTs as
against static facilities
o Existence of entry and exit strategies to enter and exit emergencies
o Impact of emergency deployment on the regular services of MHNTs
(For the evaluator: Probe more deeply according to the information offered by the interviewee:
What was the evidence of success? Why was it a success? What contributed to the success?
Who was instrumental in promoting success? Who else should we interview regarding the
successes?)
What are the major problems? What did not work well, what needs improvement? What
lessons would you like to share?
(For the evaluator: Probe more deeply according to the information offered by the interviewee:
What was the evidence of things not working properly? What were the constraints that caused
the problem? What standards and agreements were not followed? What exactly prevented them
from being followed? Who else should we interview regarding these issues?)
Do you get MHNT drugs and medical supplies timely? Why and why not?
Do you get direct financial support? Who are the major providers of this support? If yes, what type
of financial support do you get for MHNT program and its components in terms of:

Evaluation of Mobile Health and Nutrition Teams: Final Report
61
o Procurement of vehicles
o Drugs and medical supplies procurement and distribution (get the quantitative
data)
o Equipment (get Quantitative data)
o Human resource cost (salary and DSA)
o Training and capacity building (get the quantitative data)
Do you get technical assistance to the MHNT program implementation? If yes, who are
these implementing partners that provided you with technical support? How do you value
the relevance, quality and adequacy of this technical support? What is your comment on
the relevance, quality and adequacy of the technical support provided by UNICEF?
Efficiency and Quality
What are the sources of funding for MHNT activities? What is the contribution of the government?
How adequately have the funds been distributed among components of MHNT? How well were
they used? Do you feel there is adequate funding to scale up MHNT in the region? Is there any
specific plans or ideas for increasing funding?
Where do you think cost efficiency could be improved? How could funds be saved with the same
result?
Did the program confront any management issues? What improvements were made over time
and how did they effect results? Did all involved know their roles?
What do you perceive as the major strengths of the current system/mechanism for coordinating
MHNT at the regional level? What were the main constraints and supports to coordination? What
do you perceive as the major aspects of the coordination of MHNT that should be improved?
What are the major achievements in MHNT information system and reporting? What needs to be
done to improve the MHNT information system?
Were MHNT standards respected? How well the program achieves the standards? What needs
to be done to improve the quality of MHNT?
What management lessons would you like to share?
Sustainability
How has scale-up been planned and implemented? What do you perceive as the major barriers
for scaling-up MHNT? What needs to be done to improve the scale up with quality? What do you
think the ownership of MHNT by the government at different levels? How can it be improved?

Evaluation of Mobile Health and Nutrition Teams: Final Report
62
What medium and long-term plan is there to sustain the achievement with decreasing donor
funding and partner’s technical assistance?
(For the evaluator: Get as much detail as possible on the recommendations and their rationale.)
Do you have any documents that are useful for this evaluation? __________________

Evaluation of Mobile Health and Nutrition Teams: Final Report
63
Annex 4: MHNT Observation Checklist
Region___________________________ Woreda______________________ Name of the
Site__________________
Distance from town in kms_____________________ Referral Health Cente_________referral
Hospital____________
Respondent: Profession___________________ Responsibility in
MHNT___________________________
4.1 Availability of Human resources
Type Standard
Availability
Reasons for not availability Yes No
1.1 Clinical Nurse
1.2 midwife 1
1.3 Nurse 1
1.4 HEWs 2
social mobilizer 1
Driver 1
4.2 Availability of Services in the sample MHNTs against the standards of service that they are
expected to provide
Type Standard
Availability
Reasons for not availability Yes No
2.1 Consultation and treatment
2.2 Child health services
Immunization
Vitamin A supplementation
Deworming
IMNCI treatment
ICCM
2.3 Maternal Health Services
ANC services

Evaluation of Mobile Health and Nutrition Teams: Final Report
64
Distribution of delivery kit
Identification and referral of
high risk mothers
Family planning
Safe delivery
PNC
2.4 Nutrition
Screening under 5 children,
pregnant women
Essential Nutrition Action
Outpatient Therapeutic
service
2.5
Referral and transport of all
emergency cases to the
nearest facility
2.6
Response to Emergency
conditions

Evaluation of Mobile Health and Nutrition Teams: Final Report
65
4.3 . Availability of supplies in the MHNTs
Type Standard
Availability
Reasons for not availability Yes No
3.1 Medical Supplies
Emergency Drug Kit
Malaria Supplies
Medical supplies and
equipment
Guidelines, charts and
booklets
BP apparatus and
thermometer
3.2 Nutrition Supplies
Vitamin A capsule
Multi-micronutrient
supplements
MUAC tapes
Weighing scales
RUTF
Amoxicillin
Folic acid
Registers, Reporting papers for
EPI service, TT vaccination
and Contraceptives services;
OTP record card, posters, TFP
screening and charts
4.4 Training of Health workers on MHNT skills
Training of Health workers, including HEWS
Types of Training
Expected
Trainings to
meet the
standards
Trained
on
Reasons for not being trained Yes No
ICCM and IMNCI
Evaluation of Mobile Health and Nutrition Teams: Final Report
66
Micro nutrient supplementation
Screening for malnutrition
Management of SAM
WASH; Sanitation, hygiene and
emergency water treatment
Health education on
Prevention of acute diarrheal diseases
including AWD
Malaria control and utilization of ITN
Family planning, HTPs
Essential nutrition action
ANC
Immunization
Cold Chain management
Disease and nutrition surveillance, and
use of HMIS reporting tools
Annex 5: Focus Group Discussion Guide at Community Level
1. For Community leaders and care givers, and social protection groups
Please describe the health and nutrition situation in your community?
How do you traditionally provide care for when you do not have access to care in the community?
What is the major difference that the establishment MHNT made in your community?
Behavioral change
Access
Quality
How often are MHNTS offer services to your community? What are the interventions you are
advised to do? Do you get drugs and medical supplies when you go to MHNT sites?

Evaluation of Mobile Health and Nutrition Teams: Final Report
67
What is the role of the HEWs and community volunteer/development army in the community
mobilization? How effective are they? Do you think all community members in the area are
informed about the MHNT services?
What do you suggest to improve access and quality of services through MHNTs?
2. Pastoralist Health Extension Worker
How do you plan to work with MHNT in your kebele? Are you involved and plan for the deployment
of the MHNTs as part of the overall annual planning process?
Does the MHNT meet the needs in the village? Are there areas and population groups that have
not accesses this service? If yes, what are the barriers (socio- cultural, financial, geographic or
otherwise)?
Has MHNT being implemented as planned? If not what are the challenges, you face in community
mobilization?
Have you been trained on MHNT guidelines and protocols? What are the challenges of
implementing the protocol?
Do you think MHNTs have adequate equipment, drugs and supplies and recording and reporting
formats when working with you? if not what are the major challenges? What do you think are the
effect on the quality of the services?
How is the monitoring and supportive supervision done? Are there regular supervision from the
health centers and the woreda? Do you get feedbacks to you reports?
3. Community volunteers /Development army or VCHW
What is your role in community mobilization of the community to access and utilize MHNT
services? Do you think all What are you successes and challenges in this regard?
Are you trained on community mobilization?
What are your challenges of working as the volunteer in the health sector? what do you think
should be changed to make your more effective?

Evaluation of Mobile Health and Nutrition Teams: Final Report
68
Annex 6: Secondary information from RHB and WoHo and health facilities
6.1. General Population
2003 EFY (2011/12)
2004 EFY /2012/13)
2005 EFY /2012/13
2006 (1013/14)
Regional Population
# of woredas
# of mobile health and nutrition teams
# of woredas where MHNTs were deployed
Estimated population of woredas with MHNTs
# of health posts in woredas with MHNTs
# of health centers in woredas with MHNTs
# of health centres in the region
# of health posts in the region
# of Health professionals in the region
General Practitioners Health officers Nurses Midwifes Pastoralist HEWs

69
6.2 Services offered by MHNTs
Types of services Offered
2003 EFY (2011/12) 2004 EFY /2012/13) 2005 EFY /2012/13 2006 (1013/14)
Target population
# accessing services
% covered through MHNTs
Target population
# accessing services
% covered through MHNTs
Target population
# accessing services
% covered through MHNTs
Target population
# accessing services
% covered through MHNTs
Consultation and treatment
Child health services
Penta 3
Vitamin A supplementation
Deworming
Maternal Health Services
ANC services
Distribution of delivery kit
Identification and referral of high risk mothers
Family planning
Safe delivery
PNC
Nutrition
Screening under 5 children, pregnant women
Outpatient Therapeutic service
Referral and transport of all emergency cases to the nearest facility
Response to Emergency conditions
Evaluation of Mobile Health and Nutrition Teams: Final Report
70
6.3 Services offered by static health facilities (health centres and health posts)
Types of services Offered
2003 EFY (2011/12) 2004 EFY /2012/13) 2005 EFY /2012/13 2006 (1013/14)
Target population
# accessing services
% covered in health facilities
Target population
# accessing services
% covered through health facilities
Target population
# accessing services
% covered through health facilities
Target population
# accessing services
% covered through health facilities
Consultation and treatment
Child health services
Penta 3
Vitamin A supplementation
Deworming
IMNCI treatment
ICCM
Maternal Health Services
ANC services
Distribution of delivery kit
Identification and referral of high risk mothers
Family planning
Safe delivery
Evaluation of Mobile Health and Nutrition Teams: Final Report
71
Types of services Offered
2003 EFY (2011/12) 2004 EFY /2012/13) 2005 EFY /2012/13 2006 (1013/14)
Target population
# accessing services
% covered in health facilities
Target population
# accessing services
% covered through health facilities
Target population
# accessing services
% covered through health facilities
Target population
# accessing services
% covered through health facilities
PNC
Nutrition
Screening under 5 children, pregnant women
Essential Nutrition Action
Outpatient Therapeutic service
Referral and transport of all emergency cases to the nearest facility
Response to Emergency conditions

Evaluation of Mobile Health and Nutrition Teams: Final Report
72
6.4. Financing of MHNTs
2003 EFY (2011/12) 2004 EFY /2012/13) 2005 EFY /2012/13 2006 (1013/14)
Regional
Gov’t
UNCE
F
Other
DPs
Other
INGOs
Regional
Gov’t
UNCE
F
Other
DPs
Other
INGOs
Regional
Gov’t
UNCE
F
Other
DPs
Other
INGOs
Regional
Gov’t
UNCE
F
Other
DPs
Other
INGOs
Investment
Vehicle (4 WDs )
Training
Sub total
Operational cost
Salary of health
workers
Per diem of health
workers
Cost for supplies
Fuel
Maintenance Cost
Sub total
Total

Evaluation of Mobile Health and Nutrition Teams: Final Report
73
6.5 Financing of health posts and health centers in woredas with MHNTs
2003 EFY (2011/12) 2004 EFY /2012/13) 2005 EFY /2012/13 2006 (1013/14)
Regional
Gov’t UNCEF
Other
DPs
Other
INGOs
Regional
Gov’t
UNCE
F
Other
DPs
Other
INGOs
Regional
Gov’t
UNCE
F
Other
DPs
Other
INGOs
Regional
Gov’t
UNCE
F
Other
DPs
Other
INGOs
Capital budget
Construction
Equipment
Furniture
Sub total
Recurrent
expenditure
Salary of health
workers
Non salary
operational budget
Sub total
Total

74
Annex X MHNT service provision in Afar and Somali
Data Items Sex
Afar Somali
2014 2013 2012 2011 2010 Total 2014 2013 2012 2011 2010 2009 Total
Severe Complicated
Malnutrition
M 39 41 7 204 65 356 125 213 190 245 84 158 1015
F 37 48 14 104 85 288 129 269 231 258 68 172 1127
Total 76 89 21 308 150 644 254 482 421 503 152 330 2142
Severe
Uncomplicated
Malnutrition
M 165 465 393 316 331 1670 968 1944 3333 2526 912 1495 11178
F 191 521 417 294 365 1788 1078 2230 3904 2975 1139 1680 13006
Total 356 986 810 610 696 3458 2046 4174 7237 5501 2051 3175 24184
Children screened
with MUAC 11 -
11.9
M 1025 2189 1284 3099 736 8333 5284 11969 20681 13394 4492 8333 64153
F 978 2079 1362 3159 806 8384 5853 13926 23005 16458 5152 8916 73310
Total 2003 4268 2646 6258 1542 16717 11137 25895 43686 29852 9644 17249 137463
Children screened
with MUAC >12
M 1130 2936 2719 2490 837 10112 17163 40636 68495 46850 20678 26512 220334
F 1090 3018 2385 3156 927 10576 19570 47119 77001 54510 23599 30607 252406
Total 2220 5954 5104 5646 1764 20688 36733 87755 145496 101360 44277 57119 472740
Number of children
who received Vit A
M 744 1495 490 346 33 3108 3095 4483 14917 5251 3986 6524 38256
F 673 1441 555 382 0 3051 3292 4833 17264 6499 4550 7558 43996
Total 1417 2936 1045 728 33 6159 6387 9316 32181 11750 8536 14082 82252
Number of PLW
with MUAC <21
M 0 0 0 0 0 0 0 0 0 0 0 0 0
F 698 1637 1246 112 314 4007 4264 9059 18615 14799 6345 8123 61205
Total 698 1637 1246 112 314 4007 4264 9059 18615 14799 6345 8123 61205
Number of PLW
with MUAC >21
M 0 0 0 0 31 31 0 0 0 0 0 0 0
F 868 2234 1573 439 487 5601 13507 32399 52134 49387 29708 43149 220284
Total 868 2234 1573 439 518 5632 13507 32399 52134 49387 29708 43149 220284
Number of Children
admitted in OTP
M 176 525 460 398 272 1831 1014 1919 3323 2542 954 1763 11515
F 196 564 476 381 305 1922 1156 2214 3959 3094 1158 1972 13553
Total 372 1089 936 779 577 3753 2170 4133 7282 5636 2112 3735 25068

Evaluation of Mobile Health and Nutrition Teams: Final Report
75
Data Items Sex
Afar Somali
2014 2013 2012 2011 2010 Total 2014 2013 2012 2011 2010 2009 Total
Injuries caused by
land mines/UXO
M 4 0 12 1 19 36 51 239 848 293 81 924 2436
F 12 0 1 0 9 22 60 266 918 362 154 1022 2782
Total 16 0 13 1 28 58 111 505 1766 655 235 1946 5218
Intestinal Parasite
M 1 0 0 0 0 1 0 323 293 509 1264 0 2389
F 1 0 0 0 0 1 0 355 326 649 1467 0 2797
T 2 0 0 0 0 2 0 678 619 1158 2731 0 5186
Visible signs of
Trauma
M 31 116 75 77 22 321 303 972 1937 2178 706 590 6686
F 28 121 74 84 14 321 386 1032 1928 2354 784 600 7084
T 59 237 149 161 36 642 689 2004 3865 4532 1490 1190 13770
Injuries caused by
physical violence*
M 34 38 5 0 51 128 73 426 984 367 267 336 2453
F 22 21 0 0 54 97 74 461 934 393 241 356 2459
T 56 59 5 0 105 225 147 887 1918 760 508 692 4912
Others
M 502 1521 871 886 700 4480 7766 21597 40911 27262 10732 14456 122724
F 506 1398 948 966 707 4525 9369 27146 52453 37196 14530 19534 160228
T 1008 2919 1819 1852 1407 9005 17135 48743 93364 64458 25262 33990 282952
No. of Cases
referred
M 40 125 10 1 0 176 135 211 463 254 108 168 1339
F 48 159 2 1 0 210 175 336 746 403 211 379 2250
T 88 284 12 2 0 386 310 547 1209 657 319 547 3589
No. of Normal
Deliveries attended
M 3 13 0 0 0 16 1 4 3 13 0 15 36
F 4 19 14 3 0 40 178 395 630 523 325 261 2312
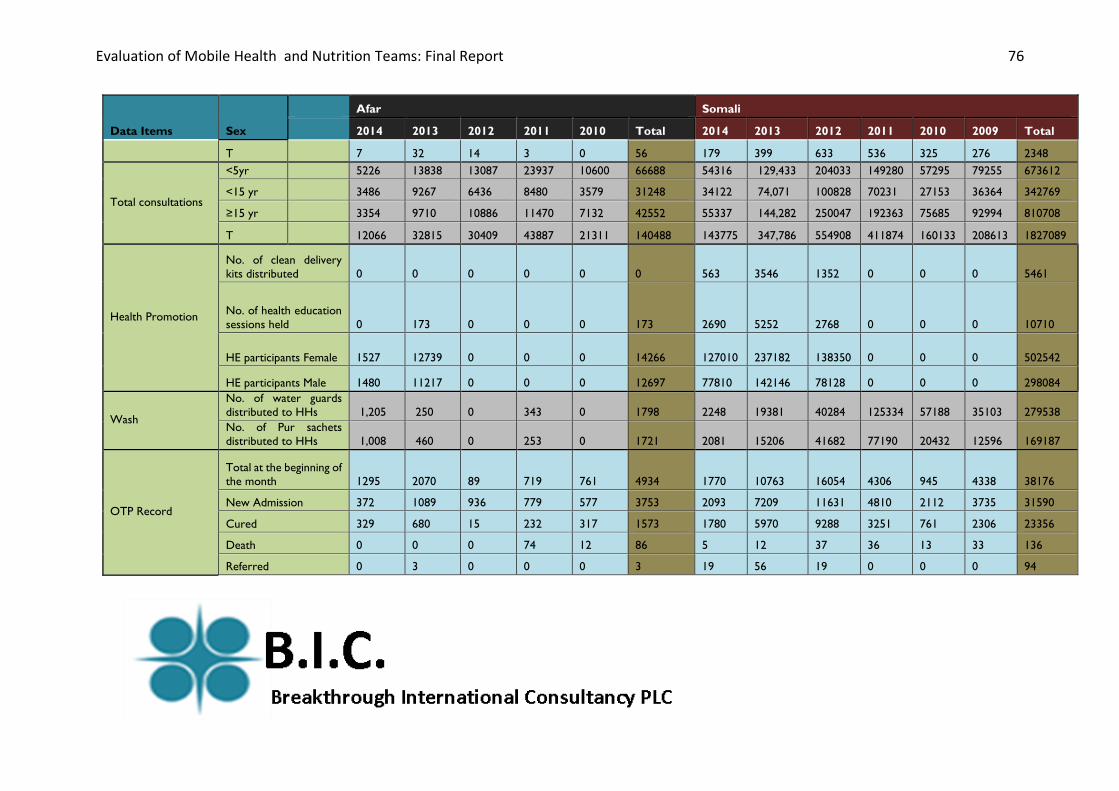
Evaluation of Mobile Health and Nutrition Teams: Final Report
76
Data Items Sex
Afar Somali
2014 2013 2012 2011 2010 Total 2014 2013 2012 2011 2010 2009 Total
T 7 32 14 3 0 56 179 399 633 536 325 276 2348
Total consultations
<5yr 5226 13838 13087 23937 10600 66688 54316 129,433 204033 149280 57295 79255 673612
<15 yr 3486 9267 6436 8480 3579 31248 34122 74,071 100828 70231 27153 36364 342769
≥15 yr 3354 9710 10886 11470 7132 42552 55337 144,282 250047 192363 75685 92994 810708
T 12066 32815 30409 43887 21311 140488 143775 347,786 554908 411874 160133 208613 1827089
Health Promotion
No. of clean delivery
kits distributed 0 0 0 0 0 0 563 3546 1352 0 0 0 5461
No. of health education
sessions held 0 173 0 0 0 173 2690 5252 2768 0 0 0 10710
HE participants Female 1527 12739 0 0 0 14266 127010 237182 138350 0 0 0 502542
HE participants Male 1480 11217 0 0 0 12697 77810 142146 78128 0 0 0 298084
Wash
No. of water guards
distributed to HHs 1,205 250 0 343 0 1798 2248 19381 40284 125334 57188 35103 279538
No. of Pur sachets
distributed to HHs 1,008 460 0 253 0 1721 2081 15206 41682 77190 20432 12596 169187
OTP Record
Total at the beginning of
the month 1295 2070 89 719 761 4934 1770 10763 16054 4306 945 4338 38176
New Admission 372 1089 936 779 577 3753 2093 7209 11631 4810 2112 3735 31590
Cured 329 680 15 232 317 1573 1780 5970 9288 3251 761 2306 23356
Death 0 0 0 74 12 86 5 12 37 36 13 33 136
Referred 0 3 0 0 0 3 19 56 19 0 0 0 94

Evaluation of Mobile Health and Nutrition Teams: Final Report
77
Data Items Sex
Afar Somali
2014 2013 2012 2011 2010 Total 2014 2013 2012 2011 2010 2009 Total
Defaulter 24 54 0 120 92 290 240 536 697 581 177 470 2701
Total Exits 349 655 15 389 433 1841 2044 6574 10041 3868 951 2809 26287
Total End of the month 1286 1991 97 740 905 5019 1819 11398 17644 5351 1355 3124 40691
Nutrition screening 0 0
Children screened with MUAC
>12
No. 2220 5954 5104 5646 1764 20688 36733 87755 145496 101360 44277 57119 472740
% 48% 53% 59% 44% 42% 50% 73% 74% 74% 74% 79% 73% 74%
Children screened with MUAC 11
- 11.9
No. 2003 4268 2646 6258 1542 16717 11137 25895 43686 29852 9644 17249 137463
% 43% 38% 31% 49% 37% 40% 22% 22% 22% 22% 17% 22% 22%
Children screened with MUAC <
11 and no complication
No. 356 986 810 610 696 3458 2046 4174 7237 5501 2051 3175 24184
% 8% 9% 9% 5% 17% 8% 4% 4% 4% 4% 4% 4% 4%
Children screened with MUAC <
11 and medical complications
No. 76 89 21 308 150 644 254 482 421 503 152 330 2142
% 2% 1% 0% 2% 4% 2% 1% 0% 0% 0% 0% 0% 0%
Total number of children screened 4655 11297 8581 12822 4152 41507 50170 118306 196840 137216 56124 77873 636529
PLW screened with MUAC >21
No. 868 2234 1573 439 487 5601 13507 32399 52134 49387 29708 43149 220284
% 55% 58% 56% 80% 61% 58% 76% 78% 74% 77% 82% 84% 78%
PLW screened with MUAC <21
No. 698 1637 1246 112 314 4007 4264 9059 18615 14799 6345 8123 61205
% 45% 42% 44% 20% 39% 42% 24% 22% 26% 23% 18% 16% 22%
Total number of PLW screened 1566 3871 2819 551 801 9608 17771 41458 70749 64186 36053 51272 281489
Total number children & PLW screened 6221 15168 11400 13373 4953 51115 67941 159764 267589 201402 92177 129145 918018
Children screened with MUAC<
11 and no complication admitted
and treated in OTP
No. 372 1089 936 779 577 3753 2170 4133 7282 5636 2112 3735 25068
% 96% 91% 87% 78% 121% 92% 94% 101% 99% 98% 97% 85% 96%

Evaluation of Mobile Health and Nutrition Teams: Final Report
78
Data Items Sex
Afar Somali
2014 2013 2012 2011 2010 Total 2014 2013 2012 2011 2010 2009 Total
Number of children screened who
received one dose of Vit A
No. 1417 2936 1045 728 33 6159 6387 9316 32181 11750 8536 14082 82252
% 30% 26% 12% 6% 1% 15% 13% 8% 16% 9% 15% 18% 13%
BCG
0-11 117 135 0 0 0 252 4931 8449 8410 3421 0 2391 27602
12-24 0 0 0 0 0 0 355 1408 1053 660 0 0 3476
Measles
0-11 236 181 0 0 0 417 7742 13115 8698 3619 0 4099 37273
12-24 101 325 0 0 0 426 4199 6407 5579 2468 0 0 18653
>24m 0 0 0 0 0 0 0 0 14 21 0 0 35
Penta-1 0-11 166 284 0 0 0 450 12914 20234 13255 6503 0 3175 56081
Penta-2
0-11 182 251 0 0 0 433 9755 13664 7951 4078 0 2753 38201
12-24 45 229 0 0 0 274 3696 4173 3776 1820 0 0 13465
Penta-3
0-11 212 214 0 0 0 426 7117 8939 5580 2305 0 2246 26187
12-24 44 251 0 0 0 295 2329 2960 2395 1324 0 0 9008
OPV 0 0-11 8 0 0 0 0 8 1219 1102 917 761 0 694 4693
OPV-1 0-11 166 284 0 0 0 450 12433 19581 13565 4618 0 3175 53372
OPV-2
0-11 182 258 0 0 0 440 9900 13538 7887 2951 0 2753 37029
12-24 45 229 0 0 0 274 4075 5008 3637 1475 0 0 14195
OPV-3
0-11 212 214 0 0 0 426 7140 8542 5369 2014 0 2246 25311
12-24 44 251 0 0 0 295 2308 3359 2655 1176 0 0 9498
PCV-1 0-11 126 57 0 0 0 183 12450 18414 3404 0 0 0 34268
PVC-2
0-11 109 73 0 0 0 182 9660 11755 2428 0 0 0 23843
12-24 45 41 0 0 0 86 3781 3827 823 0 0 0 8431

Evaluation of Mobile Health and Nutrition Teams: Final Report
79
Data Items Sex
Afar Somali
2014 2013 2012 2011 2010 Total 2014 2013 2012 2011 2010 2009 Total
PVC-3
0-11 129 47 0 0 0 176 7108 7608 1506 0 0 0 16222
12-24 24 30 0 0 0 54 2200 2670 424 0 0 0 5294
Fully vaccinated
0-11 49 214 0 0 0 290 3361 4523 3701 2024 0 2246 15855
12-24 0 159 0 0 0 159 1126 1422 1961 1341 0 0 5850
Vitamin A
6-11 0 205 0 0 0 205 2588 3374 2685 1882 0 4384 14913
12-24 160 166 0 0 0 326 2243 2885 3907 2509 0 0 11544
TT Pregnant
Women
TT-1 30 98 0 0 0 128 11921 17483 10630 6027 0 6441 52502
TT-2 13 89 0 0 0 102 8989 13147 7038 3737 0 0 32911
TT-3 22 85 0 0 0 107 5684 5659 3221 1550 0 0 16114
TT-4 0 0 0 0 0 0 1804 1712 526 391 0 0 4433
TT-5 0 0 0 0 0 0 828 462 137 61 0 0 1488
TT Non-Pregnant
Women
TT-1 40 224 0 0 0 264 14210 18136 12131 7565 0 6441 58483
TT-2 24 207 0 0 0 231 10716 13206 7054 4127 0 0 35103
TT-3 25 182 0 0 0 207 6434 5658 3119 1890 0 0 17101
TT-4 0 0 0 0 0 0 2255 1725 482 201 0 0 4663
TT-5 0 0 0 0 0 0 1021 592 115 29 0 0 1757
OPV Vials used 0 0 0 0 0 0 0 127 0 55 0 1194 1376
Penta Vials 0 0 0 0 0 0 0 99 0 171 0 3438 3708
Measles Vials 0 0 0 0 0 0 0 0 0 0 0 183 183
TT Vials 0 0 0 0 0 0 0 0 0 0 0 333 333