evaluation of anticancer agents final
TRANSCRIPT

Evaluation of anticancer agents
- Dr Anup Thorat- Guide : Dr Sandhya Kamat

Evaluation of anticancer agents - Dr. Anup Thorat 2
History
5/4/2014

Evaluation of anticancer agents - Dr. Anup Thorat 3
History
5/4/2014
Louise Goodman Sidney FarberFather of modern
chemotherapy
Alfred Gilman

Evaluation of anticancer agents - Dr. Anup Thorat 4
Need for Novel Anticancer Agents
• Multidrug resistance.
• Long-term treatment with cancer drugs a/w severe side effects.
• Cytotoxic drugs have the potential to be very harmful to the body unless they are very specific to cancer cells.
• New drugs - more selective for tumour cells.
5/4/2014

5
Pre clinical evaluation
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat
IN VITRO IN VIVO
6
In vitro cytotoxicity studies:
• 1990 : NCI-60 screen• Cytotoxicity assays on panel of human cancer cell lines – MTT-assay– SRB- assay – 3H-thymidine uptake assay – Fluorescence Dye exclusion tests – Clonogenic assays – Cell counting assay
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

7
In vitro cytotoxicity studies:
Advantages• Reduce the usage of animals. • Less time consuming, • Cost effective & • Easy to manage • Able to process a larger number of
compounds quickly with minimum quantity.
• Range of concentrations used are comparable to that expected for in vivo studies
Disadvantages: • Difficulty in maintaining of cultures. • Show negative results for the
compounds which gets activated after body metabolism and vice versa.
• Impossible to ascertain the Pharmacokinetics .
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

8
Cell lines• Tumor cell lines derived from several cancer types – lung, colon, melanoma, renal, ovarian, brain, and leukemia.
• The lines are prepared and cryopreserved using DMSO(di methyl sulfoxide )
• THAWING OF THE CELLS : Rapid thawing of frozen ampoule in water bath until it gets liquefied.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

9
Cell lines
• The solution is centrifuged with saline for 10 mins to remove the DMSO
• The saline is discarded and aliquot is taken for cell counting, cell viability and for sub culturing.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat
10
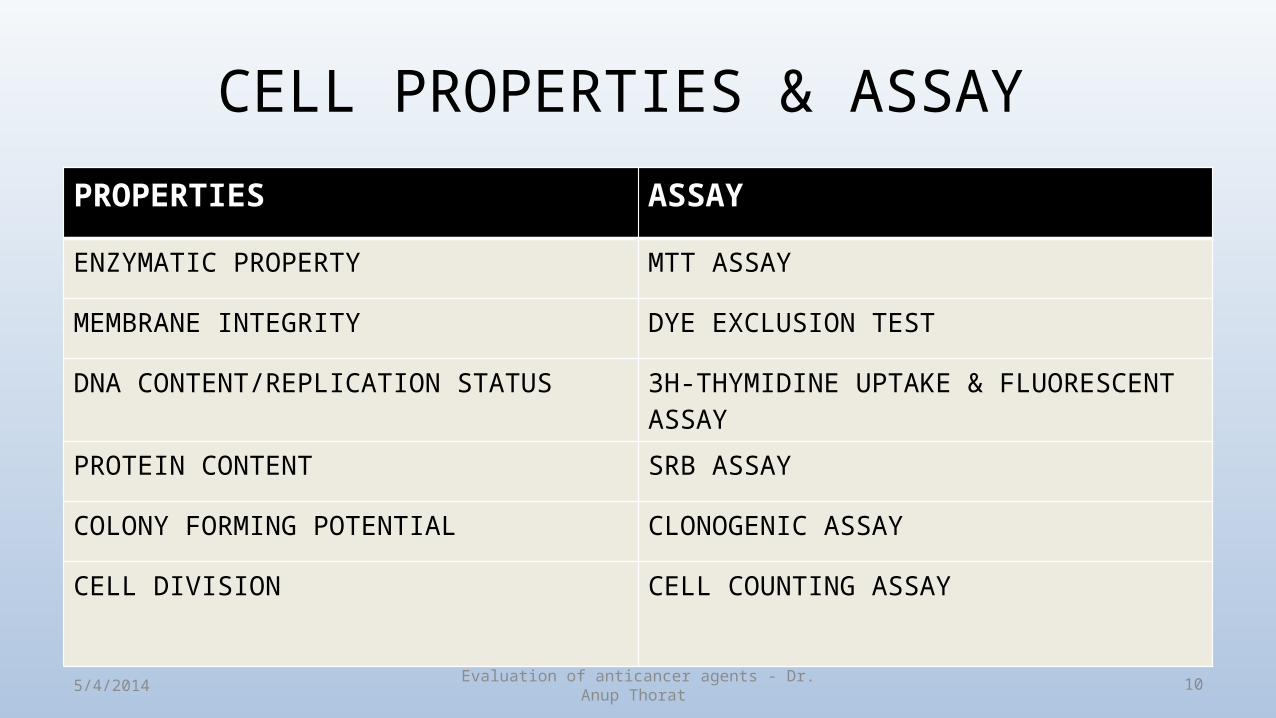
CELL PROPERTIES & ASSAY PROPERTIES ASSAY
ENZYMATIC PROPERTY MTT ASSAY
MEMBRANE INTEGRITY DYE EXCLUSION TEST
DNA CONTENT/REPLICATION STATUS 3H-THYMIDINE UPTAKE & FLUORESCENT ASSAY
PROTEIN CONTENT SRB ASSAY
COLONY FORMING POTENTIAL CLONOGENIC ASSAY
CELL DIVISION CELL COUNTING ASSAY
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

11
Microculture Tetrazolium Test(MTT Assay)
• A quantitative colorimetric assay • Measures cellular growth, cell survival and cell proliferation
based on the ability of living cells.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat
MTT (3-(4,5-
Dimethylthiazol-2-yl)-2,5-
diphenyltetrazolium bromide)
Formazan
mitochondrial dehydrogenasein living cells only

12
MTT Assay - Procedure• Cells from particular cell lines in log phase of growth are trypsinised.
Check the cell viability through haemocytometer .
• Adjust to appropriate density in suitable medium and inoculate in multiwell plates.
• Cells are treated with various conc. of test compounds & the plate incubated at 37 °C in 5% CO2 /95% humidified air (1-4 d)
• Cultures are taken out and 10 μl of MTT dye is added (5 mg/ml) into each well and incubated for 4hrs
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

13
MTT Assay
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

14
MTT Assay - Procedure
• The plate is centrifuged, supernatant discarded & precipitated formazan salt is dissolved in 100 μl of isopropanol/DMSO
• The plate samples are read at 570 nm microtiter plate reader
IC50 of drugs can be determined by counting the viable cells
% Cell viability = Absorbance of treated cells x 100 (%MTT reduction) Absorbance of untreated cells
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

15
Microtiter plate reader
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

16
SRB (SULPHORHADAMINE B) ASSAY
• Measures whole protein content which is proportional to the cell number.
• SRB – a bright pink anionic protein staining dye that binds to the basic amino acids of the cellular proteins.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

17
SRB ASSAY - Procedure • Cell lines are counted, cultured & inoculated in 96 well plates.
• After incubation with different concentrations of test compounds, the cell cultures are stained with SRB dye.
• Washing with acetic acid removes the unbound dye and the protein bounded dye is extracted using triss base
• Optical density is determined by 96-well plate reader5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

18
3H-Thymidine uptake assay
• Provides information about tumour kinetics, ploidy status of the cells.
Procedure:1. Tumor cell suspensions are exposed to the drug for 5 days. 2. Radio-labeled 3H-thymidine is added 3. Replicating cells will incorporate 3H-thymidine into their DNA 4. Determined by autoradiography or liquid scintillation.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

19
FLUORESCENCE ASSAY
• Cells are exposed to fluorescent labeled precursors after drug exposure.
• Replicating cells will incorporate the dye into their DNA.
• Resulting fluorescence is measured by flow cytometry / fluorescent microscopy .
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

20
Dye Exclusion Test
• This assay is relayed on the structural integrity of the cells.
• Dyes used : Trypan blue, Eosin, or Nigrosin
• Live cells possess intact cell membranes that exclude the dye, whereas dead cells having lost membrane integrity take up the dyes.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

21
Dye Exclusion Test - Procedure • Cells are incubated with different concentrations of test compounds for 4
days.
• Dead cells are stained with dye colour.
• Specimen is centrifuged & collected in microscopic slides.
• Live cells – stained with hematoxylin eosin.
• Tumor cell cytotoxicity is compared with control – duck erythrocytes.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

22
Trypan blue dye exclusion test
Live cell
Dead cell
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

23
CLONOGENIC ASSAY • Measures the growth inhibition.• Important for the drugs that act by arresting the cells at checkpoints in the
cell cycle
Procedure:1. Single cell suspensions are exposed to anticancer agents to be tested. 2. Suspensions are rinsed and plated in a semisolid medium.3. After 14 to 28 days, some cells will having undergone several division
form tumour colonies which can be quantified in a visual or semi-automated fashion.
4. No of colonies from treated cells is compared with untreated colonies.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

24
CLONOGENIC ASSAY
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat


26
Preclinical Toxicity Studies• Aimed at predicting
(a) Safe starting dose & dosage regimen for human clinical trials(P1)(b) The toxicities of the compound, &(c) The likely severity and reversibility of drug toxicities.
• Regulatory requirement : Two acute preclinical toxicity studies1. Rodent (mice) - single- and multiple-dose lethality studies.2. Non rodent (dogs) - single- and multiple-dose confirmatory toxicity.
• Cytotoxic & non cyotoxic drugs5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

27
Acute Toxicity Studies• First mouse given a single injection (IP, IV, SC, IM or PO) of 400 mg/kg (or
lower if the compound is extremely potent)
• Second mouse - 200 mg/kg &• Third mouse - 100 mg/kg
• The mice are observed for a period of 2 weeks & sacrificed if there are signs of significant toxicity
• If all 3 mice must be sacrificed, the next 3 dose levels (50, 35 and 12.5 mg/kg) are tested in a similar manner
• This process is repeated until a tolerated dose is found designated as MTD.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

28
Preclinical Toxicity Studies• To determine the phase I entry dose of a cytotoxic anticancer
agent, the dose levels that are lethal to 10, 50, and 90% of mice (LD10, LD50, & LD90) is determined by the same route of administration.
The projected phase I entry dose is usually 1/10th of the LD10
• A robust toxicity study needed to avoid lengthy phase I trials as well as severe drug toxicities.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

29
Why Mice?• Mice are small, easy to handle.• Short generation time & accelerated lifespan,manageable
costs, space, and time.• Striking similarity to humans in anatomy, physiology, and
genetics.• Over 95% of the mouse genome is similar to humans.• Many of the genes responsible for complex diseases are shared
between mice and humans.• Mouse genome can be directly manipulated.5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

30
Tumour Models 1. Carcinogen induced models2. Viral infection models3. Transplantation Models– Murine – Human
4. Genetically Engineered Mouse Models5. In vivo hollow fibre assay
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

31
CHEMICAL CARCINOGEN MODELDMBA induced mouse skin papillomas • Two stage experimental carcinogenesis – Initiator – DMBA (dimethylbenz[a]anthracene),– Promotor – TPA. (12-O-tetradecanoyl-phorbol-13-acetate)
• Mice : Single dose – 2.5 µg of DMBA f/b 5 to 10 μg of TPA in 0.2 ml of acetone twice weekly.
• Papilloma begins to appear after 8 to 10 wks - Tumor incidence & multiplicity of treatment group is compared with DMBA control group
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

32
Mouse skin papillomas
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

33
MNU INDUCED RAT MAMMARY GLAND CA
• Induces hormone dependent tumors. • Single i.v of 50 mg/kg of methylnitrosourea - 50 days old SD
rats. • Adenocarcinoma will be produced within 180 days of post –
carcinogen – 75 to 95% • Reduction in tumor size is compared • Drawback – cannot detect inhibition of carcinogen activation.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

34
RAT MAMMARY GLAND CA
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

35
DMBA induced rat mammary gland ca
• Sprague dawley rats
• Intragastric injection of 12 mg / kg of DMBA at 50 days of age
• Cancer appears within 120 days – 80 to 100%
• Detect the drugs inhibiting carcinogen activation.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

36
MNU induced tracheal squamous cell ca
• Hamster
• 5% of MNU in normal saline is given once a week for 15 wks by catheter.
• Within 6 months – 40 to 50%
• Test drug efficacy is measured by comparing with carcinogen control group
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

37
DEN induced lung adenocarcinoma in Hamster
• 17.8mg DEN/kg body wt twice weekly by S.C inj for 20 weeks starting at age 7 to 8 weeks.
• Usually produces tracheal tumors in 90-100% and lung tumors in 40-50% of male syrian hamster.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

385/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat
Cancer site Cancer Type Species CarcinogenColon Adenocarcinomas Rat AOM (azoxymethane)
Prostate Adenocarcinomas Rat MNU (methylnitrosourea)
Esophagus Squamous cell carcinoma
Rat NMBA(N-nitroso-methylbenzylamine)
Breast Adenocarcinoma Mice NMU (N-Nitroso-N-methylurea)

39
Viral infection models• Mouse Mammary Tumor Virus (MMTV) was the first mouse
virus, isolated at Jackson labs as the “non-chromosomal factor” that caused mammary tumors in the C3H strain of mice.
• Some viruses cause cancer via random integration in certain cells
• Some viruses carry cellular oncogenes – Abelson murine leukemia virus – Abl– Moloneymurine sarcoma virus – Raf
• Engineered viruses now used routinely in the laboratory to induce cancer.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

40
Transplantation Models• Tumor cells or tissues (mouse or human) transplanted into a
host mouse.• Ectopic – Implanted into a different organ than the original
(typically subcutaneous or kidney capsule) • Orthotopic – Implanted into the analogous organ of the
original tumor.• Advantages :– Typically cheap, fast & easy to use.– Not covered by patents
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

41
Transplantation Models• Disadvantages:– Histopathology cannot be exactly correlated to human tumors
– Lack of step-wise progression through pre-neoplastic stages
– Evolution of tumor cells during passaging
– Requirement for angiogenesis to support the newly transplanted tumor
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

42
Transplantation Models : Human Tumor Xenografts• Athymic “nude”mice developed in 1960’s• Mutation in nu gene on chromosome 11• Phenotype: retarded growth, low fertility, no fur, immunocompromised
– Lack thymus gland, T-cell immunity
• First human tumor xenograft of colon adenocarcinoma by Rygaard & Poulson, 1969
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

43
Xenograft Sites
• Subcutaneous tumor (NCI method of choice) with IP drug administration
• Intraperitoneal• Intracranial• Intrasplenic• Renal subcapsule• Site-specific (orthotopic) organ inoculation
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

44
Xenograft Study Endpoints• Toxicity Endpoints:– Drug related death– Net animal weight loss
• Efficacy Endpoints:– Tumor weight change– Treated/control survival ratio– Tumor growth assay (corrected for tumor doubling time)
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

45
Xenograft Tumor Weight Change
• Tumor weight change ratio (used by the NCI in xenograft evaluation)
• Defined as: treated/control x 100%• Tumor weight in mg = (a x b2)/2– a = tumor length– b = tumor width
• T/C < 40-50% is considered significant
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

46
Human Tumor XenograftsAdvantages• Many different human tumor cell
lines transplantable• Wide representation of most
human solid tumors• Good correlation with drug
regimens active in human lung, colon, breast, and melanoma cancers
Disadvantages• Brain tumors difficult to model• Different biological behavior,
metastases rare– Survival not an ideal endpoint:
death from bulk of tumor, not invasion
• Shorter doubling times than original growth in human
• Difficult to maintain animals due to infection risks
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

47
Transplantation Models : Cell line based allografts
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

48
Transplantation Models : Cell line based allograftsAdvantages• Very easy to maintain cell lines
indefinitely; • Very fast to generate large
numbers of tumors • Relative homogeneity of tumors
makes it easy to detect differences
• Comparatively cheap • Intact immune system
Disadvantages• Mouse cells rather than human • Inaccurate histopathology
compared to human tumors • Evolution of tumor cells during
culture • As it involves murine CA, ability
to predict response to therapy in humans is controversial.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

495/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

50
In Vivo Hollow Fibre Assay
• In vivo screening tool implemented in 1995 by NCI• 12 human tumor cell lines (lung, breast, colon, melanoma,
ovary, and glioma• Cells suspended into hollow polyvinylidene fluoride fibers
implanted IP or SC in lab mice• After in vivo drug treatment, fibers are removed and analyzed
in vitro• Antitumor (growth inhibitory) activity assessed
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

51
In Vivo Hollow Fibre Assay
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

52
In Vivo Hollow Fibre Assay
Subcutaneous Hollow Fibre implants
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

Clinical Evaluation

54
Clinical Evaluation
• The most reliable method for demonstrating efficacy is to
show a statistically significant improvement in a clinically
meaningful endpoint in blinded randomized controlled trials
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

55
Regulatory considerations
1. Regular Approval– Longstanding route of drug approval based on the demonstration of
clinical benefit2. Accelerated Approval– Use of a surrogate endpoint that is reasonably likely to predict
benefit. – Serious or life-threatening diseases– Improvement over available therapy – No existing therapy
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

56
Endpoints
• 1970s - Objective Response Rate (ORR)• 1980s - improvement in survival, quality of life (QOL), physical
functioning, tumour related symptoms.• Three kinds of end points have been used:
1. Overall Survival2. Tumor assessment endpoints e.g. ORR,DFS, PFS,TTP, TTF; and3. Symptom assessment endpoints e.g. palliation of side effects, QOL
scores.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

575/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat
Endpoint Regulatory Evidence
Study Design Advantages Disadvantages
Overall Survival(OS)
Clinical benefit for regular approval
Randomized studies essential Blinding not essential
1)Universally accepted direct measure of benefit
2)Easily & Precisely measured
1)May involve larger studies 2)May be affected by crossover
therapy and sequential therapy 3)Includes non cancer deaths
Symptom Endpoints (patient reported Outcomes)
Clinical benefit for regular approval
Randomized blinded studies
1)Patient perspective of direct clinical benefit
1)Blinding is often difficult 2)Data are frequently missing or
incomplete 3)Clinical significance of small changes
is unknown 4)Multiple analyses 5)Lack of validated instruments
Objective Response Rate(ORR)
Surrogate for accelerated Approval or regular approval
Single-arm or randomized studies can be used Blinding preferred in comparative studies Blinded review recommended
1)Can be assessed in single-arm studies 2)Assessed earlier and in smaller studies compared with survival studies 3)Effect attributable to drug, not natural history 4) Anti tumour activity
1)Not a direct measure of benefit 2)Not a comprehensive measure of drug activity 3)Only a subset of patients who benefit4) Not useful in stable disease
Disease-Free Survival(DFS)
Surrogate for accelerated approval or regular approval
Randomized studies essential Blinding preferred Blinded review Recommended
1)Smaller sample size & shorter follow-up necessary compared with survival studies
1)Not statistically validated as surrogate for survival in all settings 2)Not precisely measured; 3)Subject to assessment bias, particularly in open-label studies 4)Definitions vary among studies
ProgressionFree Survival(PFS)
Surrogate for accelerated approval or regular approval
Randiomzed studies essential Blinding preferred Blinded review Recommended
1)Smaller sample size & shorter f/u reqd.2)Measurement of stable disease included 3)Not affected by crossover or subsequent therapies.4)Generally based on objective & quantitative Assessment.
1)Not statistically validated as surrogate for survival in all settings 2)Not precisely measured; 3)Subject to assessment bias particularly in open-label studies 4)Definitions vary among studies 5)Frequent radiological or other assessments 6) Involves balanced timing of assessments among treatment arms

Study Designs

59
Single-Arm Studies
• No available therapy • ORR (objective response rate) and response duration in single-arm
studies can be a substantial evidence supporting accelerated approval.
• Primary efficacy measure : Proportion of patients who achieve a complete or partial response to the treatment.
• Design eliminates truly ineffective therapy
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

60
Single-Arm Studies
• Challenges :1. Do not adequately characterize time-to-event endpoints (survival,
TTP, PFS)2. Because of variability in the natural history of cancer, a randomized
study is necessary to evaluate time-to-event endpoints.3. Inability to predict comparative performance vis-a`-vis the then-
available best possible, standard-of-care therapeutic option.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

61
Non-inferiority Studies• Rely on historical data to establish the active control’s treatment effect size
& constancy assumption• Estimated size of the active-control’s treatment effect should be based on a
comprehensive meta-analysis of historical studies
• Challenges :1. the estimation of active-control effect and the determination of amount of effect
(NI margin) to be retained. Usually large sample sizes.2. Subsequent therapies and crossover to the active-control arm can confound any
NI analysis3. NI trials with endpoints other than survival are problematic
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

62
Clinical Trial Phases
• What is the dose and schedule? Phase I
• Is it active?– spectrum of anticancer activity ? Phase II– is it better than standard therapy? Phase III
• Is it safe? Phase I to IV
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

63
Phase 0 : Microdosing• The FIH dose : significant safety risk for the patient volunteers.• Less than1/100th of the dose calculated to yield a pharmacological
effect of the test substance to a maximum dose of less than 100 µg.• Advantages:– Mitigate FIH dose risk,– Gather early pharmacokinetic data (bioavailability, clearance, elimination
rate), and – Increased efficiency of drug development.
• Highly sensitive analytical methods : PET, LCMS, accelerated mass spectroscopy(AMS)
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

64
Phase 1
• Usually conducted in patients, rather than healthy volunteers.
• This adds to the challenges : 1. Recruitment of tumor-specific patient volunteers2. The recruited volunteers may be in the advanced stages of the
disease - refractory to the currently available standard-of-care treatment options - cost escalation.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

65
Dose Escalation Studies
• Phase 1 entry dose is obtained from preclinical toxicity studies• Endpoints : – Along with MTD, info on clinical toxicity, pharmacokinetics, and preliminary antitumor activity is obtained. – Also for cytotoxic agents, dose-related toxicity is regarded as a
surrogate for efficacy.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat
Progressively escalating
doses
MTD

66
Dose Escalation Studies • Modified Fibonacci search :
1. Safe starting dose(d) = 1/10th of the LD10
2. Enroll patients in cohorts of three, and escalate the dose according to a modified Fibonacci sequence
3. Higher escalation steps have decreasing relative increments -100, 65, 52, 40, 29% & thereafter 33% increases over the previous dose.
4. Ethical issues : substantial numbers of patients are treated at nontherapeutic doses
5. Efficiency issues : Lengthy trials, time & cost incurred.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat
67
Dose escalation : Other Methods
• Pharmacologically guided dose escalation (PGDE)– Using the preclinical toxicology data to rapidly escalate doses to a
target area under the curve (AUC) value obtained from murine pharmacokinetic data.
• Non-pharmacokinetic statistical modeling approaches :– Statistical approaches model the dose–toxicity relationship as a
sigmoidal curve to predict the MTD. The toxicity is then evaluated & actual MTD found by rapid dose titration.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

68
Ethical Challenges In Phase I1. The paucity of benefits with substantial risks 2. Informed consent
• Majority of participants are treated at doses that cannot produce responses in human tumors.
• The objections based on informed consent are deficiencies of disclosure, understanding, and voluntariness
• Vulnerable group – Terminally ill patient
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

69
Phase II and III Clinical Trials• Phase II studies are carried out in a small group of patients with a
specific tumor type to – Determine anticancer efficacy &– To define the therapeutic window of the compound
• Any arm may be terminated early because of discouraging results, and the response rate of each arm is assessed separately against a historical control rate with definable α and β error probabilities
• Phase III trials are conducted in a much greater number of patient volunteers of the selected tumor type with prospective and randomized evaluation against standard of care.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

70
Phase II and III Clinical Trials
• Embedding a randomized phase II study within a phase III study– Patients who progress on one of the arms of Phase II would then be
randomly assigned to arms E or C of phase III & and – Their survival data would be combined in a stratified fashion with
data from patients directly assigned to arms C or E for the phase III assessment.
– This design allows untreated patients to be enrolled onto the phase II study, while assuring them a more established therapy if they progress
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

71
Phase II and III Clinical Trials
• Phase II studies act as a screen of antitumor efficacy to select the most promising agents to enter the pivotal phase III clinical trials.
• A Phase II study should efficiently eliminate truly ineffective therapy & reliably indicate whether subsequent phase III testing is warranted.
5/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat

725/4/2014 Evaluation of anticancer agents - Dr. Anup Thorat