ethics of resource allocation and human rights
TRANSCRIPT

Ethics of Resource Allocation and Human Rights Professionalism and Patient Safety 2017 Please look through the slides prior to the session and come prepared to ask questions or clarifications

Ethics
Is the right course of action always obvious? Action or decision should withstand criticism; i.e., the reasoning process Aristotle – Character and Reasoning
10-Feb-17 © The University of Sheffield
2

Decisions that withstand criticism
• Valid arguments – premises lead logically to the conclusion so if the premises are true, then the conclusion must be true.
• Avoiding logical fallacy – a mistake in the logical relation between an argument’s conclusion and its premises; e.g., bifurcation – claiming that only two alternatives exist (Richard Cooper’s phase 1 Lecture on Philosophical bases….) 10-Feb-17 © The University of Sheffield
3

• Is Principlism alone adequate? • Consequentialism • Casuistry? – extracting theoretical rules
from specific instances, interpretation of ethical principles or cases….
• Deontology • Virtue • Care Ethics
10-Feb-17 © The University of Sheffield
4
10-Feb-17 © The University of Sheffield
5 Breast cancer mum back in High Court
for Herceptin battle Free IVF care 'denied to many' Secret NHS plan to ration patient care Cancer victim denied life-prolonging
drugs on NHS is given hope with £10,000 anonymous donation

10-Feb-17 © The University of Sheffield
6 Learning outcomes • An understanding of
• the key ethical theories of resource allocation
• the challenges of ‘individual responsibility’ in distributive justice; and relevance of human rights to resource allocation
• the factors that may form a part in the decision making models in distributive justice
• And develop awareness of topical issues around resource allocation
10-Feb-17 © The University of Sheffield
7
Rationing needs have increased because..
• Shift from acute illness to chronic long-term
• Normal physiological events medicalised • Increase in choice and increase in
expensive drugs (This is not an exhaustive list)
• 2011/12 -2014/15, NHS spending will increase by only 0.4 per cent in real terms (House of Commons Health Committee, 2010).
• On average, 1950 -2000 : 3.48 % per cent per year, rising to 6.56 % 1999/2000 -2010/11 (Appleby et al., 2009).
http://www.kingsfund.org.uk/audio-video/john-appleby-nhs-productivity-challenge
10-Feb-17 © The University of Sheffield
8
10-Feb-17 © The University of Sheffield
9
What is Just(ice) healthcare?

10-Feb-17 © The University of Sheffield
10
Allocation theories based on • Egalitarian principles • Maximising principles • Libertarian principles
10-Feb-17 © The University of Sheffield
11
• NHS was founded on a requirement to provide all care that is necessary and appropriate to everyone (equal access)-Aristotelian equality/justice
• Challenge: How to resolve the tensions between egalitarian aspirations and finite resources? (Rawlins and Dillon)
Egalitarian principles

10-Feb-17 © The University of Sheffield
12
• Criteria that maximize public utility
• Who is best to decide this? Should doctors be involved in rationing decisions?
Maximizing principle

10-Feb-17 © The University of Sheffield
13
Libertarian approach
• – each is responsible for their own health, well being and fulfilment of life plan.
An Example èèèèè

The German Health incentive Schemes? (BMJ, v339,p725,2009)
• Contributions are a percentage of income earned; so well off shoulder more burden
• Incentives to change individual health behaviour. E.g., bonuses (cash, sports or kitchen eqpt, or reduction for insurance contributions) for participation in routine screening, health promotion and check-up programmes.
• The pay out must come from the savings made by better health behaviour. 10-Feb-17 © The University of Sheffield
14

• Incentives for early detection and treatment of chronic disease.
• Compliance in prevention and treatment reduces co-payment by patient.
• No claim benefits for reduction/responsible use of resources.
• Carrot or stick? E.g., max co-payment for some cancers was increased from 1 to 2% non compliance.
10-Feb-17 © The University of Sheffield
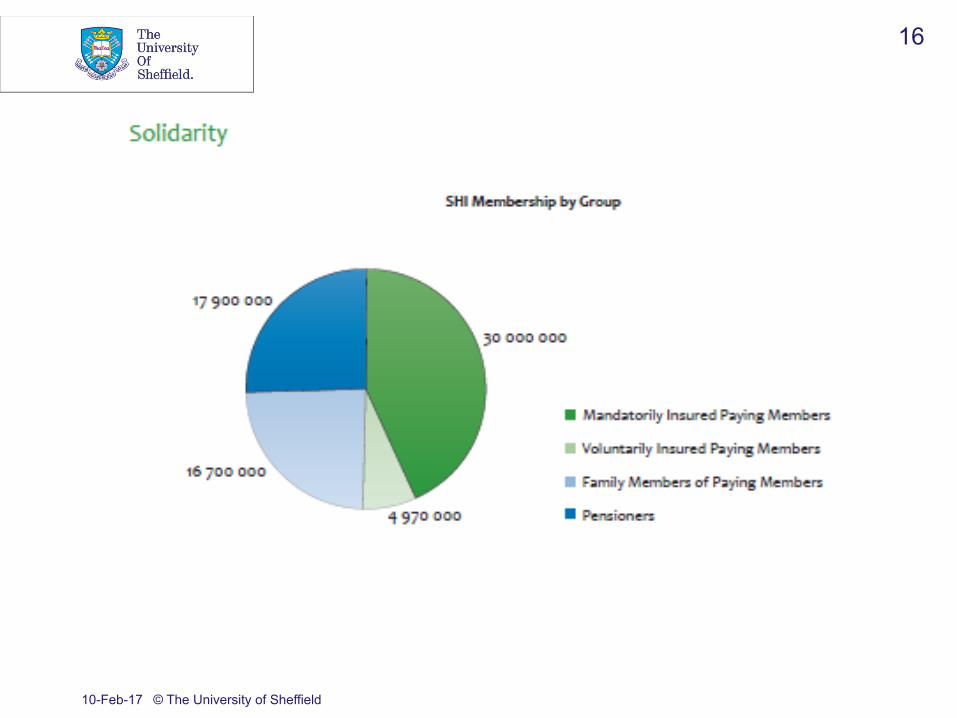
15
10-Feb-17 © The University of Sheffield
16

• The question of equity: Private programmes attract or retain higher income groups because they contribute more and cost less.
• To what extent bonuses result in Change of behaviour?
• Socio-Economic Status differences in incentive use?
• Should doctors police health behaviour?
10-Feb-17 © The University of Sheffield
17

10-Feb-17 © The University of Sheffield
18
10-Feb-17 © The University of Sheffield
19
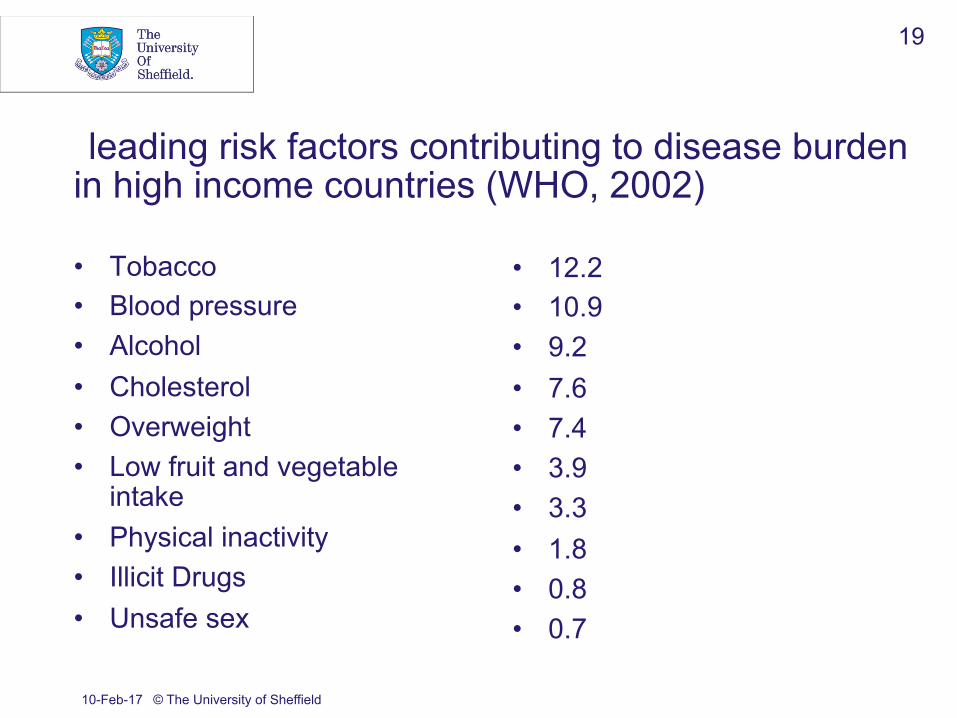
leading risk factors contributing to disease burden in high income countries (WHO, 2002) • Tobacco • Blood pressure • Alcohol • Cholesterol • Overweight • Low fruit and vegetable
intake • Physical inactivity • Illicit Drugs • Unsafe sex
• 12.2 • 10.9 • 9.2 • 7.6 • 7.4 • 3.9 • 3.3 • 1.8 • 0.8 • 0.7
WHO 2002

• 26% of both men and women aged 16 or over were classified as obese (BMI> 30kg/m2).
• 41% of respondents (aged 2+) said they made walks of >20 minutes at least 3 times a week
• 20% of respondents reported that they took walks of at least 20 minutes “less than once a year or never” in GB.
10-Feb-17 © The University of Sheffield
20
In the UK in 2010

• Significant upward trend in household expenditure on eggs, butter, beverages, sugar and preserves.
• Downward trend with fruit and vegetables
10-Feb-17 © The University of Sheffield
21
In the UK in 2010

10-Feb-17 © The University of Sheffield
22 What are the arguments for and against?
• Can individuals be held accountable (how and to what extent is debatable) for their current or future health?
10-Feb-17 © The University of Sheffield
23
• Obligation to help others in need
regardless of why they are there in the first place provided that helping would not impose unacceptable sacrifices on others.
A person who is unwell/poor health cannot exercise political and civil rights.
10-Feb-17 © The University of Sheffield
24
• Establishing causality between behaviour and the need for treatment is often uncertain/impossible.
• Justified inequalities (smokers) moralistic judgements (eating or exercise habits)
• A person’s productivity is influenced by many factors over which the person has little control
• Measuring the value of contribution
Motivation for unhealthy behaviour?
• The costs of most unhealthy activities impact in the future, but the benefits from them occur in the present
• The challenge of affluence to self control
• Social networks – obesity (Christakis and Fowler, 2007).
• Backward looking vs. forward looking 10-Feb-17 © The University of Sheffield
25
• The intrinsic value of every person’s life; and concern to this
AND • Personal responsibility for the governance
of our own life.
10-Feb-17 © The University of Sheffield
26
10-Feb-17 © The University of Sheffield
27
Sustainability in Resource Allocation The Hippocratic Canon offers the twin injunctions to do good and not to do harm. These ethics apply not only to individual patients, but to those systems that sustain human health, and not just to the current but to future generations. Sustainability also highlights prevailing tensions between freedom of action (autonomy) and the ethic of justice, as those most affected by harms to the global environment are those least responsible for causing them. The doctor will be able to recognise and articulate his or her own values and principles in relation to sustainability and, by upholding these values, to act with integrity.(13) …..From the Centre for Sustainable Healthcare
10-Feb-17 © The University of Sheffield
28
What is sustainable medical practice? Can you think of examples and challenges? The Brundtland Commission’s definition of a sustainable process is one that “meets the needs of the present without compromising the ability of future generations to meet their own needs.” Haines A, Dora C. How the low carbon economy can improve health. BMJ. 2012;344(mar19 1):e1018-e1018. doi:10.1136/bmj.e1018. Costello A, Abbas M, Allen A, et al. Managing the health effects of climate change. The Lancet. 2009;373(9676):1693-1733. doi:10.1016/S0140-6736(09)60935-1.

The rule of rescue (Jonsen)
• Can we fund expensive treatment to prolong life short term?
• How does this marry with equal concern and self determination; does this maximise good with fairness?
10-Feb-17 © The University of Sheffield
29

10-Feb-17 © The University of Sheffield
30
Do nothing /monitor
Inform and educate
Enable choice: to change behaviours
Guide choice through changing the default: make ‘healthier’ choices the default
Guide choice through incentives: use financial and other incentives to guide people to pursue certain activities
Guide through disincentives: use disincentives to influence people to not pursue certain activities
Restrict choice: regulate to restrict the options available to people
Eliminate choice

What are the current key resource allocation challenge in our healthcare system?
10-Feb-17 © The University of Sheffield
31
Organ transplantation, expensive treatments to few leaving others without, lifestyle inflicted conditions….What else?
• R (Tracey) v Cambridge University Hospitals NHS Foundation Trust & Ors [2014] • Montgomery v Lanarkshire Health Board (2015)
10-Feb-17 © The University of Sheffield
32 Cases you should know about and implications to practice

Human Rights in Medical Ethics
10-Feb-17 © The University of Sheffield
33

• Are Rights only about legality?
• How about the value of moral rights?
• Can a rights discourse help secure the best interests of dementia patients?
10-Feb-17 © The University of Sheffield
34

10-Feb-17 © The University of Sheffield
35 Rights that are frequently engaged in healthcare
• Art 2 – the right to life (limited)
• Art 3 – the right to be free from inhuman and degrading treatment (absolute)
• Art 8 – the right to respect for privacy and family life. (qualified)
• Article 12 – right to marry and found a family
R v Havering London Borough Council: R v Coventry City Council, 2008
• Medical evidence indicates that mortality rates
amongst care home residents who were moved were higher than in those who were left in place.
• Therefore is the council in breach of the resident’s article 2 rights in deciding to close the home?
10-Feb-17 © The University of Sheffield
36
• Risk to the resident was found to be no more than speculative and could be minimised by careful management.
• Also individual needs assessment for each resident.
10-Feb-17 © The University of Sheffield
37

Mencap inquiry finds institutional discrimination against people with learning disabilities
• Ignoring family concerns • Failing to diagnose serious illnesses • Denying basic nursing care or pain relief • Staff attitude that some LD patients quality
of life is too poor to be worth saving • The Guardian, 2 January 2012
10-Feb-17 © The University of Sheffield
38

ARTICLE 14 The enjoyment of the rights and freedoms set forth in this Convention shall be secured without discrimination on any ground such as sex, race, colour, language, religion, political or other opinion, national or social origin, association with a national minority, property, birth or other status.
10-Feb-17 © The University of Sheffield
39

10-Feb-17 © The University of Sheffield
40
Rights Underlying assumptions
• The irreducible moral status of individuals demands that people are treated in ways that are compatible with that moral status
• These claims can be made against a duty bearer such as the state and are universal
10-Feb-17 © The University of Sheffield
41 Human Rights Act
• Forms part of the decision making processes when making decisions about people’s rights
• Is part of all policy making

The NHS Constitution
10-Feb-17 © The University of Sheffield
42

10-Feb-17 © The University of Sheffield
43 Problems with human rights
• Are they universal? Female genital mutilation, judicial executions
• Which interests are significant enough to justify ennobling a human right?
• All basic rights are claim rights
• Can absolute claims conflict? All rights are interdependent and inter-related

Human Rights Act 1998 (in force since 2000)
Gives further effect to the rights in
• European Convention on Human Rights (1950, 1953)
10-Feb-17 © The University of Sheffield
44

Health is the state of complete physical, mental and social wellbeing and not merely the absence of disease or informity...the highest attainable level of health is the fundamental right of every human being. (Preface to the WHO constitution) The Lancet, 2007)
10-Feb-17 © The University of Sheffield
45

10-Feb-17 © The University of Sheffield
46 Rights that are frequently engaged in healthcare and their relevance to clinical practice
• Art 2 – the right to life (limited)
• Art 3 – the right to be free from inhuman and degrading treatment (absolute)
• Art 8 – the right to respect for privacy and family life. (qualified)
• Article 12 – right to marry and found a family
10-Feb-17 © The University of Sheffield
47 Rights that are frequently engaged in healthcare
• Art 2 – the right to life (limited)
• Art 3 – the right to be free from inhuman and degrading treatment (absolute)
• Art 8 – the right to respect for privacy and family life. (qualified)
• Article 12 – right to marry and found a family

10-Feb-17 © The University of Sheffield
48
Absolute rights • right to protection
from torture, inhuman and degrading treatment and punishment (Article 3),
• the prohibition on slavery and enforced labour (Article 4)
• protection from retrospective criminal penalties (Article 7)

10-Feb-17 © The University of Sheffield
49
Limited/qualified rights
• These rights are limited under explicit and finite circumstances,
• e.g., right to liberty (Article 5)
• Article 8(2) - state can restrict the right to respect for private and family life;
• To protect health or morals, or the protection of the rights and freedoms of others; social needs
Viewing dementia as a disability with scope for a human rights discourse
What is Dementia? How might a rights discourse be applied in the best interests of people with dementia?
10-Feb-17 © The University of Sheffield
50

10-Feb-17 © The University of Sheffield
51

Individual Rights vs. Collective Good?
10-Feb-17 © The University of Sheffield
52
• Human rights but what value do you place on an individual’s autonomy? (Liberalism)
• Should vaccinations become compulsory? • What about blood/organ donations? • Minority group representation in policy? • Is screening a form of collectivism?
10-Feb-17 © The University of Sheffield
53

Is there a right to medical treatment? • Article 2 - There is a positive obligation upon the
State; to take appropriate steps to safeguard life
• But cannot impose an impossible or disproportionate burden on the authorities.
10-Feb-17 © The University of Sheffield
54

S3, NHS Act, 2006
10-Feb-17 © The University of Sheffield
55
No absolute duty No positive obligation on the Secretary of State to provide funds
Duty to provide services to such extent as he considers necessary to meet all reasonable requirements

Judicial Review
• Opportunity for an individual to challenge the exercise of power by a public body.
10-Feb-17 © The University of Sheffield
56

Exceptionality criteria
It is proper for an authority to adopt a general policy for the exercise of such an administrative discretion, to allow for exceptions from it in ‘exceptional circumstances’ and to leave those circumstances undefined’.
10-Feb-17 © The University of Sheffield
57

• Refusing treatment because of advanced age alone - Article 2 and Article 14 (prohibition on discrimination).
• Deny resources because of gender or sexuality - Article 14
10-Feb-17 © The University of Sheffield
58

10-Feb-17 © The University of Sheffield
59
Cost Effectiveness
Clinical Effectiveness
• The intrinsic value of every person’s life; and concern to this
• Personal responsibility for the governance of our own life.
10-Feb-17 © The University of Sheffield
60
Questions
• Why is some awareness of human rights in policy is relevant to you?
• Please give examples where human right arguments or acts can be applied to clinical practice?
10-Feb-17 © The University of Sheffield
61
10-Feb-17 © The University of Sheffield
62
In distributing finite resources – a decision model
• Judgement of disease burden (judges: physicians, patients and society) - High, moderate, low
• Effectiveness (utilitarianism) - High, moderate, small, unknown
• Cost effectiveness (egalitarian) - High, moderate, low, negative
• Other factors such as total costs at society level, or individual payment

Fair processes
• Involvement and oversight by a legitimate institution, meaningful public engagement
• transparent decision making, • reasoning according to information and
principles that all can accept as relevant, and • Procedures for appealing and revising
individual decisions. Daniel and Sabin
10-Feb-17 © The University of Sheffield
63

Worth a few minutes…. • http://www.theguardian.com/society/2016/jan/18/10-
truths-about-britains-health-service
• http://www.gmc-uk.org/guidance/20706.asp
• http://www.theguardian.com/commentisfree/2015/oct/24/growing-old-silicon-valley-prescription-for-misery?CMP=Share_iOSApp_Other
10-Feb-17 © The University of Sheffield
64