essential drugs iron
TRANSCRIPT
Essential drugs
Iron
Form of iron - :
- Diet – farric form ( Fe+3) - Absorption – Ferous form (Fe+2) - Storage – Ferritin form
Requirment -:
- Adult – 1 mg/Kg - Pregnancy – 3 – 5 Mg/Kg
Oral Iron tablet -:
- It should not Be Give �̅� milk and ca+.
- S/E – N/V Matalic test
Parentral iron -:
- ‘Z’ techniques - Prevent back flow - Reduce pain - Liver store iron passed from the mother for 5-6 month to
baby. - Iron maximum absorption in – duodenum. - Maximum iron present in – Jaggery - Antidote – Desferoxamine - Appropriate site for iron inj – Dorsogluteal muscles - Give �̅� Vit because vit – C increase iron absorption - Instruct parent and child about side effect of iron
supplement – Black stool

Organophosphate poisoning (OP )
- m/c due to exposure to pesticide. - Op inhibit acetylcholine – Estrase lead to accumulation of
acetylcholine in body.
S/E -:
- Pin – point pupils - Increase saliva
Rx –
- D.O.C – Atropin ( Anticholinergic agent )

Vit B9 – (Folic acid ) :-
- Mostly indicated in pregnancy . - It prevent the neural tube defact . - Increase the formation of RBC. - Maximum absorption in jejunum.
Anti tubercular drug :-T.B
Mycobacterium tuberculosis (MTB)
- Gram + ve - Rod shape (Bacilli) - Cell wall thick - Acid fast bacilli

1st Line H – Isoniazide
R – Refampicin
Z – Pyrazinamide
E – Ethambutol
S – Streptomycin
Isoniazide :- - It is the most patent drug among ATT. - It is bacteriocidal drug
S/E:- INH –Hepato – toxicity
Injury to nerve ( Neuropathy )

Rifamficin -:
- It is also a bacteriocidal drug
Rifamficin crosses the all barriers of the body –
S/E :- Urine colour – orange red colour
Pyrazinamide :-
- Increase uric acid level .

Ethambutole :-
- It is bacterio – static drug
S/E :-
Demage optic nerve
Streptomycin :-
- It is on aminoglycoside - It is also bacteriocidal - It is Absultly contraindicated in pregnancy
It may demage VIII C.N
Cause(Cochtearport) Ototocity

2nd Line ATT :-
1. Kapriomycin
2. Ofloxacin
3. Clarithromycin
4. Cyclo serine
5. Ethionamid
6. Levofloxacin
- Use in resistance case of tuberculosis - In india the treatment is started as (DOTS) - (Direct observational treatment in short cause )
Malaria –
Protozoal parasit FOUR species of plasmodium - :
a. Plasmodium phalsipherum – most dangerous species of malaria
b. Plasmodium vivex – most common in india c. Plasmodium ovale d. Plasmodium malariae – maximum hemolysis
Most common organ affect by malaria – liver Plasmodium phalsipharum cause – cerebral malariae / black water fever D.O.C – Artesunate / Quinine
Antimalarial drug –
- Artesunate - Quinine - Chloroquine - Primaquine - Mefloquine - Dipivephrine

Respiratory system drugs :-
Cough -: it is the protective reflex.
1.Expectorant 1. Anti tussive drug
Ex- Ex - Codien
KI - Phalcodien
KBr - Dextrometharphan
Bromhexine
2. Mucolytics -:
Ex. Ambroxol
Guafenesin
Note-: KI is contraindicated in pregnancy – because couse hypothyroidism in baby
Asthma -:
1. Stabalized Ig – E antibody by – ex – Omalizumab 2. Mast cell inhibitor -:
Nadochrami
Ketotifen
Cormonlyn sodium = Undesirable S/E – Bronchospasm. 3. Lucotrian synthesis inhibitor -:
Ex. Zileuton

4. Lucotrian receptor blocker -:
Zafirlukast
Montilucost 5. Bronchodilator -:
Short acting- Salbutamol
Long acting – salmeterol 6. Anticholinergic drug -:
Ipratropium bromide
Tiotropium bromide

Laxative Drugs -:
Cremaffin
Liquid paraffin
Lectulose
Contraindicated -:
These drug contraindicated for D.M.
These drug also contraindicated in intususception .
Contraindicated in intestinal obstructio
Antidiabetic Drugs :-
Drug of choice in type – 2 D.M 1. Sulfonylurias :-
It stimulate beta cell for insulin secreation.
Glipzide
Glemperide 2. Biguanides:-
Prevent liver output for glucose.
Metformine 3. Thiozolidiones:-
Increase insulin receptor for use of glucose .
Rosiglitazone
Pioglitazone
4. Alfa glucose inhibit:- These drugs decrease absorption of glucose from intestine.
Acarbose
Meglitol
NOTE:- Promlintide – one on only drug which can use in both type D.M.
NOTE:- sulphonylurias should not be take with alcohol because it can cause disulfluram like reaction.
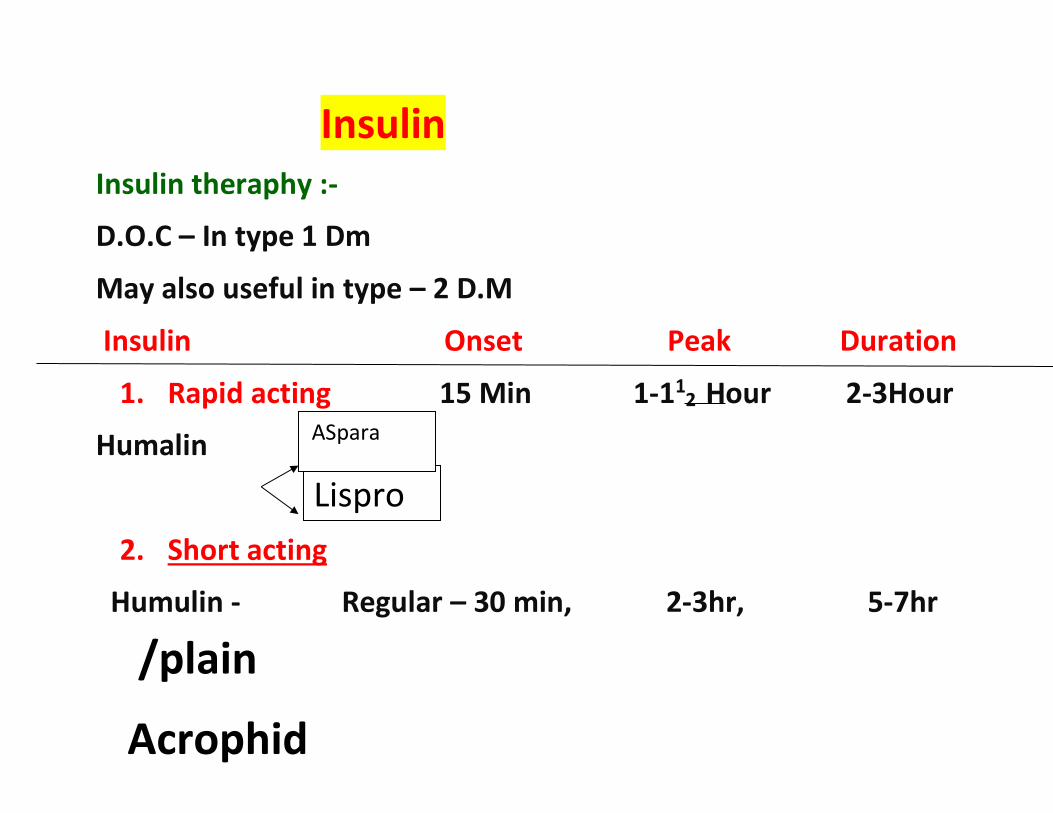
Insulin Insulin theraphy :-
D.O.C – In type 1 Dm
May also useful in type – 2 D.M
Insulin Onset Peak Duration
1. Rapid acting 15 Min 1-112 Hour 2-3Hour
Humalin
2. Short acting
Humulin - Regular – 30 min, 2-3hr, 5-7hr
Lispro
ASpara
/plain
Acrophid
3. Intermediate acting :-
Humulin – NPH – 112 hrs, 4 – 12 hrs, 16-24 hrs
Humulin – (30/70) – 30 min, 2-12 hrs, 16-24 hrs (Mixtard)
30% = rapid acting
70% = NPH
4. Long acting :-
Humulin = U – 212 Hrs, 12-16hrs, 24-36 hrs
Humulin = Glargine
NOTE :- Rapid acting & Short acting insulin can be given I.V.
Drugs for seizure:- Seizure:- It is sudden abnormal electrochemical discharge with in brain
Epilepsy:- It is a disease condition in which a tandancy is develop to having a recurrent episode of seizure.
Drugs:-
1. Phenytoin sodium:- Provide in all type of seizure accept patetmal seizure
2. Carbamazapine:- Provide in all type of seizure accept patetmal seizure.
3. Phenobarbiton:- Provide in all type of seizure accept patetmal seizure.
4. Sodium volproate / Volproic acid:- All type of seizure . 5. Ethosuximide:- Drug of choice for patetmal seizure.

6. Sedetive :-
Diazepam
Midazolam
Status Epilepticus :- It is life threatening situation in which recurrent episode of seizure without achiving his consaiousness
for about 30 minutes.

Leprosy :-
It is also known as hansen’s disease
International leprosy day 30 Jan
Leprosy is a chronic infectious disease caused by Mycobacterium leprae
Usually affects skin and peripheral nerves

INTERNATIONAL HEALTH AGENCIES
1. WHO ( World health organization )
WHO established in the 7 April 1948.
Situated Geneva Switzerland.
VISION :- the attainment of the highest level of health by All
people.
Improve quality of the all people of the world.
Organizational structure :-

World health assembly :- supreme fevering body of organization.
MAIN FUNCTION :-
It determine international health policy and programme.
It review work of past year.
It approve budget.
Function of WHO :-
Prevention and control of specific disease.
Development comprehensive health services.
Family health
Health statistics
Environmental health
Health statistics
WHO contribute in india :-
Control communicational disease.
Strengthening public health administration
Improving the environmental sanitation.
Provide MCH services
Provision of education and training of all types of
professional and auxiliary health workers.
Assist family planning method.
UNICEF
UNICEF ( United nations international children emergency fund )
: -
Establishment dec. 11, 1946
Head quarters – newyork.
Rehabilitated to was affected children.
Activity of UNICEF :-
Child nutrition low cost protein rich food.
With FAO aided applied nutrition programme.
Immunization :- production of vaccine and distribution.
Prevent spread of HIV., anti retoviral medicine for children
and mother with HIV.
Social welfare services for children.
Emergency relief and rehablitational.
UNICEF in india :- in 1949 UNICEF programme
Work with india.
1 RCH 2. Child environment 3. Child Protection and education
4. Child nutrition
FOOD AND AGRICULTURE ORGANIZATION (FAO)-
1945 , Head quater – ROME
Aims :-
To improve nutrition of the people of all countries.
To increase efficiency of farming forestly and fisheries.
UNITED NATIONS DEVELOPMENT PROGRAMME (UNDP)
UNDP :- Basic development of poor country.
1965 1 jan, 1966 applied.
Head quarter :- Newyork
Function :-
Assistance of poor country in world.
Need in poor country and fund arise.
Financial assistance in developing country.
Achieving minimum goal eradication, poorty, hunger.
Environmental preservation sanitation, proper disprsol of
waste.

UNITED NATION FUND FOR POPULATION ACTIVITY(UNFPA)-
UNFPA :- Focus population and MCH SERVICE
1969 Newyork
In india establish 1974,
MCH and family planning.
WORLD BANK :-
Specialized agency of the united nation.
Established july, 1944.
Helping less developing country

INTERNATIONAL RED CROSS :- BY Henry dunant
1863 Zaneva switzarland
In INDIA march 1920
Swiss business director henry dunant
70 million people services provided who victims of war.
FUNCTION :-
Huminitarian services to victims of wars.
Natural disaster
First aid care
Family planning
Health education
UNITED NATIONS EDUCATIONAL SCIENTIFIC AND CULTURAL
ORGANIZATION (UNESCO):-
4 Nov, 1946
Head quater – paris
193 countries member
Aim :-
Maintain peace
Eradication of poverty
Science and educational development
Information education technology development.
INTERNATIONAL LABOR ORGANIZATION (ILO):-
-Establish in 1919
NATIONAL AGENCY
1 INDIAN RED CROSS :- 17 March 1920
Headquater – new delhi
Activities :-
Natural climities
Make the arrangement of the food, cloth drinking water.
Medical services
Home for old age people.
Supply milk powder, drug
Blood band services
MCH services
Emergency health care provide.

2. TUBERCULOSIS ASSOSIATION IN INDIA :-
Established in 1939
The prevention, control treatment and relief of
tuberculosis.
Providing quality diagnostic and treatment services.
3. HIND KUSHT Nivaran Sangh :-
1950 , new delhi
Rehabilitation, conduct research and field investigation of
leprosy patient.
Mission :- leprosy free India
30th January- anti leprosy day activity

4. CENTRAL SOCIAL WELFARE BOARD :-
1953, control of ministry of education.
5. All India Women’s Conference :-
It is the only voluntary health agency otganized for the
welfare of the women in the country.
It was established 1927.
Activity :-
Litracy and education computer training centre
Increase women right and dissolve issue.
6. Blind Association In India :-
All india blind relief society was established in 1946.
It organize eye refief campus and takes step for the socio
economic relief of blind.
7. Indian Council for Child welfare (ICCW):-
Established in 1952.
NATIONAL ACUTE RESPIRATORY INFECTION
CONTROL PROGRAMME :-
Launched in 1990
Objective :-
To reduce morbidity and mortality among under 5 year
child.
To avoid delay getting treatment.
To reduce number of cases.
REVISED NATIONAL TUBERCULOSIS CONTROL PROGRAMME:-
National tuberculosis control programme 1962.
Relaunched 1992.
Revised programme because goal are not fulfilled.
National ante-malaria programme history:-
1953 april , National malaria control program (NMCP)
1958 – National malaria eradication program .
Urban malaria scheme 1971 modak committee modified
1977.
Method of malaria control:-
Vector control
Anti larva measure
Prevention of water
National filarial control programme (NFCP)-
Launch in 1955 to control lymphatic filariasis the endemic
state of country
Strategy :-
Improvement of sanitation
Antilarval operations
NATIONAL LEPROSY CONTROL PROGRAMME (NLCP ) :- 1954
Incubation – 3 to 5 year
Early case detection
Effective implementation
Control unit
National leprosy eradication programme (NLEP) :- 1983
OBJECTIVE :-
Intonation co-ordination
Leprosy centre
Multi drug therapy used
STD CONTROL PROGRAMME :-
1949 Project to control venereal disease.
Urethral discharge
Vaginal discharge
Genital ulcer
Recently HIV infection has been also added.
National AIDS control programme taking over the STD
control programme in 1992.
National AIDS control programme ( NACP ):-
India – 1986 1st case detect
Programme launch in 1987
GOAL :-
To prevent mortality and morbidity
Reduce case incidence
AIMS :-
Detection of casein early stage
Mortality and morbidity control
Prevention of further transmission
Preventive measure use

National programme of control blindness:-
Visual acuity of less than 3 / 60 (snellen) is called blind.)
( inability count finger in daylight at a distance of 3 meter )
1976 launch to all age group
GOAL :-
To prevent vision loss
Cataract centre programme zaunce

National iodine deficiency disorder control program (NIDDCP )
( National goiter control programme :- 1962)
Recomed NIDDCP in 1992
NIDDCP cover a wide spectrual of iodine deficiency dis-order
like mental and physical relardation , deafmutism and goiter.
AIM / GOAL :-
Reduce prevalence of IDD
Reduce incidence of IDD less than 10 % amnogadult 5 %
among children 10 -14 year, about 0 % among the
newborn.
Mainly goiter seen in Hilly area ( high altitudes )
Expanded programme of immunization:-
EPI :- 1974
Universal immunization programme 1985
Goal :- under 5 year child vaccine provided against 6 killers
disease DPT, TB, Polio , measles, TD, and diphtheria added.
Reproductive and child health programme. :-
Launch – 1997
Objective :-
To reduce infant mortality rate and maternal mortality
rate.

Component :- main component
Family planning child survival and safe motherhood
programme.
Package of services under RCH programme
For the mother :- essential case
Register by 12 – 16 week
Antenatal check up at least 3 time during pregnancy 20, 32,
36
Tetanus immunization should be given
IMCI ( Integrated MGT of childhood illness )
RCH Phase II – 1 april 2005
1. Essential obstratic case
institutional delivery.
Skilled attendance at delivery.
2. Emergency obstratic case
24 hr. delivery services normal and assisted delivery
C – section provide
New born care
Emergency care of sick children
Janani surksha yojana
1. Antenatal, natal and post natal case
JSY is for safe motherhood
ASHA would work as a link worker.
Free delivery free diagnosis free treatment
2. Vandematram scheme :- 9 feb 2004
To promote public private relationship
To improve safe mother hood services
Reduce MMR and neonatal death.
ICDS ( Integrated child development services)
2 oct. 1975
ICDS programme was initiates for the welfare of children
and development of human resources.
Objectives :-
improve to nutrition and health status of children in the age
group of 0 -6 year.
To reduce the mortality, morbidity malnutrition and school
drop out

National water supply and sanitation programme :-
Launched 1954
Main object of providing safe water supply and
adequate drainage facilities for the entire population of
the country.
1972 special programme known as accelerated rular
water supply programme
National diabetes control programme :-
Launch – 1987
Strategies :-
Identify of high risk subject
Early diagnosis
Prevent complication and mortality.
Training of the medical and paramedical personnel.
LEVEL OF HEALTH ORGANISATION:
1. Central level – It composed of three organs.
Union ministry of health &family welfare
Central council of health
Central family welfare council
2. AT STATE LEVEL – service It has two sectors 1. State ministry of health &family welfare.
2. State health directorate.
3. AT THE DISTRICT LEVEL
1. Subdivision:
Each district divided into two or more subdivision, each incharge of an assistant collector.
2. Tehsils:
Each division is again divided into tehsils or taluk,
incharge of a tehsildar. It has no. of village ranging from 200-
600.s
PANCHAYATI RAJ SYSTEM
Panchayati raj is a 3 tier structure of rural self government in India
1. Panchayat – at village level
2. Panchayat samiti –at the blocks level
3. Zila parisad –at the district level
AT THE VILLAGE LEVEL:- (i) The gram sabha
(ii) The gram panchayat
(iii)The nyaya panchayat
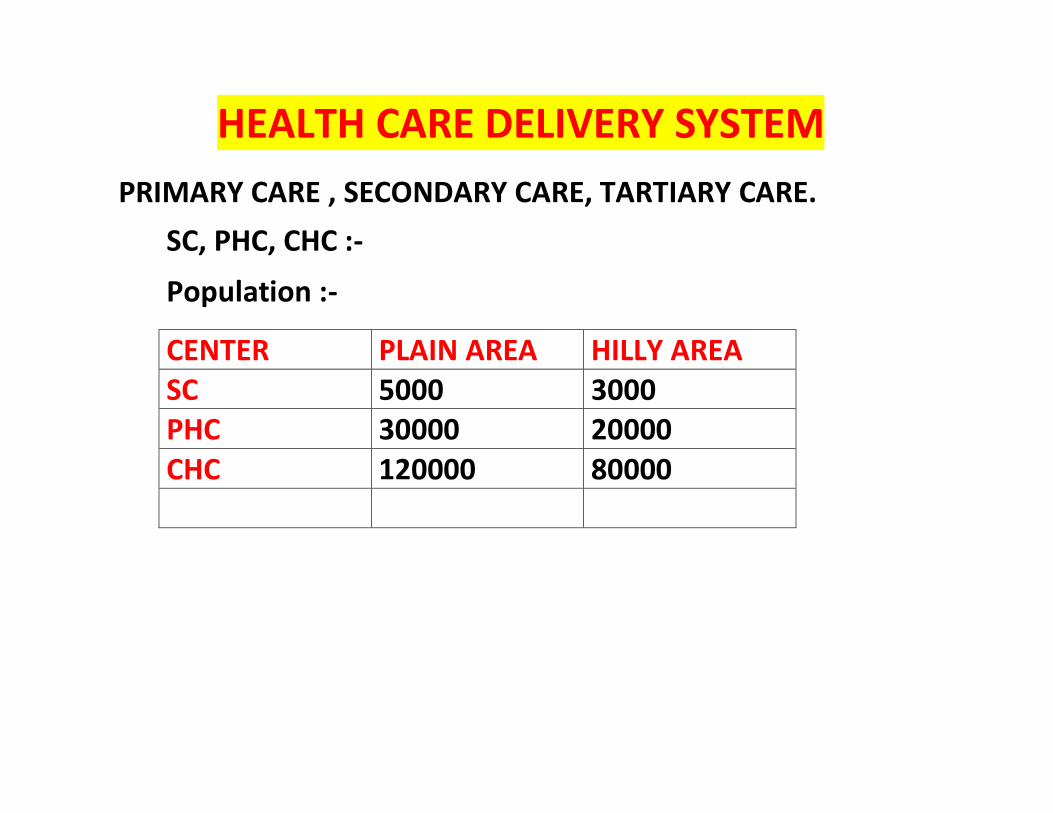
HEALTH CARE DELIVERY SYSTEM
PRIMARY CARE , SECONDARY CARE, TARTIARY CARE.
SC, PHC, CHC :-
Population :-
CENTER PLAIN AREA HILLY AREA SC 5000 3000 PHC 30000 20000
CHC 120000 80000

PRIMARY HEALTH CENTER – - Acc to alma atta declearation in 1978 give permission for
PHC.
- First concept given by bhore committee in 1946.
- PHC estabilished by state govt.
- First PHC in 1952 in india.
- Total PHC in india- 25743 (2018)
- One PHC control 6 sub center. - Bed capecity – 4-6 bed. Staff – 15-16

COMMUNITY HEALTH CENTER- The idea of CHC was involved under the National health policy (2002).the CHC are estabilished by the state govt
POPULATION :- 80000 – hilly / tribal 120000 – plain. Bed - 30
It is First Referral Units – FRU
CHC control 4 PHC or 24 SC
VILLAGE LEVEL STAFF –
ASHA – ACCREDITED SOCIAL HEALTH ACTIVIST
Under NRHM.
Dress - Blue Saree / Pink blue apron
ANGANWADI – Control by MAHILA BAL VIKAS MANTRALAYA
Female & child development ministry. Opened as a ICDS . Population ( 1000 – rural / urban) (700 – tribal) Total staff – 3

MATERNAL AND CHILD HEALTH Antenatal or prenatal visits:- Register every pregnancy within 12th weeks . First 7 months (28 weeks) – once a month. Next two month (36 weeks) – twice a month. Thereafter – once a week till delivery.
Minimum:-
Minimum 4 visit (according to WHO)
1st visit around 12-16 weeks 2nd visit between 24-28 weeks 3rd visit at 32 weeks. 4th visit at 36 weeks.
Antenatal / prenatal advice:- Calcium requirement per day 500 to 1000 mg in pregnancy and
1000 to 1500 gm in lactation. Folic acid requirement 200 to 500 ug/day. Iron requirement (needed from 16 week) – average 22 mg/
day in pregnancy and 12 mg/day in lactation. o In more than 10 gm% Hb give 1 tab 60mg elementary
iron / day. o In less than 10gm% Hb give 3 tab 180 mg elementary
iron/ day. Total pregnancy require additional supplementary need of
60000 kcal (350 kcal/day additional) energy and 400 gm protein (15gm/day).
Lactation requires additional supplementary need of 550 kcal/day energy and 25 gm/day protein for first 6 months.

Normal healthy women weight gains about 12 kg during whole pregnancy.
8 hours sleep and at least 2 hours rest after mid day meals (total 10 hour rest).
Avoid certain drugs because it cause teratogenic effect in new born (if taken between 4 to 8 weeks of pregnancy or during period of organogenesis)
e.g. Thalidomide cause deformed hands and feet of the babies born
o LSD cause chromosomal damage. o Streptomycin cause 8th nerve damage so deafness in
the fetus. o Tetracycline causes teeth malformation.

Immunization by tetanus toxoid- o 1st dose (0.5 ml/IM) at 16-24 weeks or as soon as
pregnancy recognize. o 2nd dose after one month. o Minimum interval between two doses should be 1
month. o Second dose should be given 1 month before EDD. o Give only one booster if second pregnancy occurs
within 5 year and primary immunization was completed.
Avoid live viral vaccines like measles, OPV, rubella etc

Intra – natal care – • Rooming in :- keeping baby’s crib at close to mother’s bed
immediately after delivery called rooming – in. o To maintain asepsis throughout delivery process. o Delivery with minimum injury to the infant and mother. o Readiness to deal with complications such
as prolonged labour, ante- partum hemorrhage, convulsion, mal- presentation, prolapsed of cords etc.
Postnatal care Complication of post – partum period:-
o Puerperal sepsis:- infection of genital tract within 3 weeks after delivery.
o Secondary PPH:- vaginal bleeding between 24 hours of delivery to end of puerperium (6 weeks) called secondary hemorrhage. It mainly occurs due to retained placenta or membrane.
o Thrombo – phlebitis:- infection of the veins of the leg. o Others are UTI & mastitis.
Post natal examination- o First 3 day – twice a day. o Till umbilical cord off – once a day.
Post natal visit – o Female health worker to give at least 3-6 post natal

visit. o First 6 month once a month. o Thereafter once in 2 or 3 month till end of one year.
INDICATORS OF MCH CARE o Mortality in infancy and child hood.
Still birth rate - peri- natal mortality rate Neonatal mortality rate - post neonatal mortality rate Infant mortality rate - 1-4 years mortality rate Under – 5 mortality rate - child survival rate
1. Maternal mortality rate (MMR)-
o WHO define maternal death as “ death of mother during pregnancy and puerpeirium (6 weeks of delivery) related to complication of pregnancy and its management”
MMR = total number of female death due to complications
Preg. Child birth or within 42 days of delivery x100000
Total number of live births in the given area & year
o MMR based on per 100000 live birth o Late maternal death – maternal death after 42 days but
before 1 year after termination of pregnancy due to direct or indirect obstetric cause.
Foetal deaths weighing over 1000 gm at birth during the year Still birth rate = x 1000 Total live + still births weighing over 1000 gm at birth during the year
IMR = number of deaths of children less than 1 year of age in a
year x 1000 Number of live births in the same year Child mortality rate -
= No. of deaths of children less than 5 year Of age in a given year
Total no. live births in the same year x 1000
UNICEF consider under 5 mortality rate as best single indicator of social development and well being.
DEMOGRAPHY Scientific study of population is known as demography.
Demography cycle:-
It contains 5 stages
i. 1st stages (high stationary)
Birth rate is – high Death rate is – high No increment in population
ii. 2nd stage (early expanding)
Birth rate – stable Death rate – decreased Population – increases

iii. 3rd stage ( late expanding)
Birth rate – decreased Death rate – decreased Comparatively birth rate is more than death rate and
population increased.
iv. Fourth stage (low stationary)
Birth rate – decreases Death rate – decreases Population does not increases
v. Fifth stage (decline)
Birth rate decrease Death rate – increases Population increases

Registration of births and deaths (Birth and Death Registration Act, 1969) and marriages is compulsory at their place of occurrence with local registrar in India
– Births must be registered within: 21 days – Deaths must be registered within: 21 days – Marriages must be registered within: Variable limits within India

Family planning - (WHO 1971) India launched family planning programme (firstly in world)
in 1952. In 1970 slogan – “DO YA TEEN BAS” three child norms. In 1980- 2 child norms. Themes - : son or daughter two will do same. “ Second child after 3 year.” National population policy – 1 aprail 1976 It increase legal age of marriage. Female - 15→18 & male - 18→21. Note- National population policy- 2000
Best contraceptive for 20 year nulliparous is pills. Ideal contraception in recent married couple is oral
contraceptive pills. Contraception of choice for a working women with
irregular& profuse bleeding is oral pills. OCP helps in prevention of carcinoma cervix. OCP decrease risk of ovarian cancer & colorectal cancer,
increase risk of cervical & breasrt cancer.
Best Contraceptive for lactation mother is mini pill. Copper T acts by causing aseptic endometritis. Best method for spacing child birth in women is IUCD.
BARRIER METHODS -
1. Condom (male) – In india trade name is – NIRODH
2. Diaphragm – It is cervical barrier type method.
3. Vaginal Sponge : 100 mg nonoxynol 4. IUD - IUD’s prevent’s the implantation of fertilized ovum
Non – medicated: - Does not release any metal ion or hormone.
Medicated:- Release either a metal ion like copper Ag (silver) and hormone (progesterone).
1. First generation:-
Non – medicated Different size & shape loop, spirals, coils & rings. e.g. – lippes
loop. Double “S” shaped device made up of polyethylene Contain BaSO4 (barium sulphate) to allow x-ray observation.
2. Second generation:-
Copper containing Add in 1970 “T” shaped device. Copper has strong anti – fertility effect by spermicidal action.
E.g.- Earlier device:-
Copper T-7 -1 year Copper T-200B – 4 year
Newer device:- CU –T 220 4 year
CU –T 380A 10 year (maximum) Nova-T 5 year Multi Load
device-
MICU – T 250 - 3 YEAR
MICU – T 375 - 5 YEAR
3. Third generation:- (hormonal)
Progesterone hormones

e.g. – progestasert – ‘T’ shaped device filled with 38mg of progesterone. Release - 65 mcg/daily Duration – 1 year LNG 20 (mirena)
‘T’ shaped device filled with 52 mg of LNG Release 20 mcg/day
Contraindication:- Suspected pregnancy PID Vaginal bleeding
Cancer of Cx and uterus Previous ectopic
Time of insertion:- During M.C.:- within 10 days of M.C.
Best 7 days of menstrual period diameter of Cx is greater Immediate post partum:- 1st week of delivery Post puerperal:- after 6-8 week of delivery.
Side effect – 1st Bleeding & 2nd Pain
HORMONAL METHOD : Combined mixed pills:-
Estrogen + progesterone
Pill give orally for 21 days consecutive from beginning on the 5th day of the M.C.
7 day iron supplementation Pill should be taken every day at a fixed time preferably
before going to bed at night. used only after 16 year of old She forgets take one dose of pill then she should take it
as soon as possible when she remember that and then Second dose taken at usual time .
She forgets two dose of pill continuously then consent with obstetrician or may take double dose.

MALA –N (N= niisulk) MALA – D (D = –rs -3/packet) MALA – D = ( D – norgestrol) Levonorgestrel – 0.15mg Ethinnyl estradiol – 0.03 mg
1. MALA – N Norethisterone acetate 1 mg Ethinyl estradiol Hormonal 21 tab = white color Iron 7 tab = brown color
2. Mini pill / micro pill/ pop (progesterone only pill) Contain only progesterone
(Norethisterone)
3. Post coital pill / emergency pill :-
Used after unprotected coitus Unwanted 72 – 1.5 gm levonorgestrel Normal – 0.75 mg levonorgestrel
4. Weekly pill/ centchroman:-
Taken orally one a week e.g. saheli Action:- block the function of estrogen in uterus. First 13 week taken twice a weekly.
5. DEPOT FORMATION-
Injection:- DMPA (depot medroxy progesterone acetate)
150 mg of medroxy progesterone acetate Progesterone hormone Duratio 3 month
NET – EN:- Nor ethisterone enantate – 200 mg IM Every – 2month
6. Vaginal Rings / Intra Vaginal Rings- Release estrogen & progesterone Action:- Stopping ovulation & thickening the cervical mucus.
Time of insertion:- within 5 days of M.C.
7. Intradermal implant : Norplant implant:-
210 mg levonorgestril Sub dermal implant Six silastic (silicon rubber) capsule containing 35mg
levonorgestrol (LNG). Each capsule contain – 35 mg LNG
Breast feeding
Exclusive breast feeding leads lactational amenorrhoea for 6 month
Breast feeding act as contraception for 6 month in EBF. But require extra contraception after 3 month of delivery. If female not on EBF require contraception after one month
Permanent method
85% female sterilization 10-15% male sterilization
COMMITTEE OF HEALTH 1946 – Bhore committee ( health survey & development ) 1952 – Shetty committee 1962 – Mudliar committee ( health survey & planning
committee) 1963 – Chaddha committee 1965 – Mukherji committee 1966 – Mukherji committee 1967 – Jungalwala committee(committee on integration of
health services. 1973 – Kartar singh committee (committee on MPW under
health & family planning) 1975 – Shrivastav committee ( group of medical education &
support man power) 1983 – Mehta committee
1983 – National health policy 1984 – Working group on medical education & training &
manpower training. 1986–Bajaj committee(Committee of health manpower
planning production & management. 1989 – Sarojini verdhapan committee ( high power committee
on nsg education.
The Employees State Insurance Act, 1948
Act passed in 1948 for social security and health insurance.
Benefits to employee in ESI act 1948 –
o Medical benefits – “full medical care” including
hospitalization at free of cost. o Sickness benefits – payable for a maximum period of 91
days in any continuous period of 365 days, the daily rate being about 50% of the average daily wages.
o Maternity benefits – on delivery 12 weeks leave and on miscarriage 6 weeks leave.
o Dependent benefits – pension at the rate of 70% of wages payable.
Occupational Health Occupational hazards and occupational disease:-
Physical Hazards:-
o Heat – hyperpyrexia, heat syncope, heat cramps, burns. o Cold – trench foot, frost bite, chilblains o Light – eye strain, occupational cataract and miner’s
nystagmus o Noise – occupational deafness (chronic posure to more
than 85 dB sound intensity) o Vibration – 10 to 500 Hz vibration into fingers may cause
white fingers. o U.V. radiation – welding cause conjunctivitis and keratitis
(welder’s flash). o Ionizing radiation – cancer leukemia, aplastic anemia,

pancytopenia.
Chemical Hazards
o Gases:- CO2, CO, HCN, CS2, NH2, N2, SO2 etc. may cause gas poisoning.
o Dusts/ pneumoconiosis:- dust size 0.5 to 3 micron after a variable time may cause pneumoconiosis, dust may be –
i. Inorganic dusts:- it cause following hazards -
Silica – silicosis (X-ray show “snow storm” appearance). Coal dust – accumulation of carbon deposits in the
lungs due to inhalation of smoke or coal dust called anthracosis.
Iron:- inhalation of dust or fumes containing iron particles called siderosis (hemosiderosis means deposition of hemosiderin (an iron – containing pigment) mainly in the liver and spleen).
Asbestos:- protracted inhalation of asbestos particles called asbestosis (diagnosis – sputum show asbestos bodies and X – ray show ground glass appearance)
ii. Organic (vegetable) dust:- it cause following hazards- Tobacco causes tobacosis Cotton dust cause byssinosis Sugar cane dust cause bagassosis.
o Bagasse or sugar cane dust, first reported by ganguli and pal in 1955.
o Skiagram – show mottling in lungs or shadow Grain dust causes farmers lungs.