espen congress copenhagen 2016 · espen congress copenhagen 2016 refeeding syndrome. zeno stanga,...
TRANSCRIPT

NUTRITION THERAPY IN THE PATIENT WITH REFEEDING SYNDROME: PRACTICAL GUIDANCE
Z. Stanga (CH)
ESPEN Congress Copenhagen 2016REFEEDING SYNDROME

Zeno Stanga, MD
Division of Nutritional Medicine
NUTRITION THERAPY IN THE PATIENT WITH
REFEEDING SYNDROME: practical guidance
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism
University Hospital of Bern, Switzerland
Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Learning objektives
• To rise awareness regarding RFS management
• To identify patients who are at risk of RFS
• To understand how safe nutrition therapy is started
in patients with different levels of risk of RFS
• To know how can RFS be prevented
• To know how to treat RFS

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016

Refeeding Syndrome - Nutrition Therapy
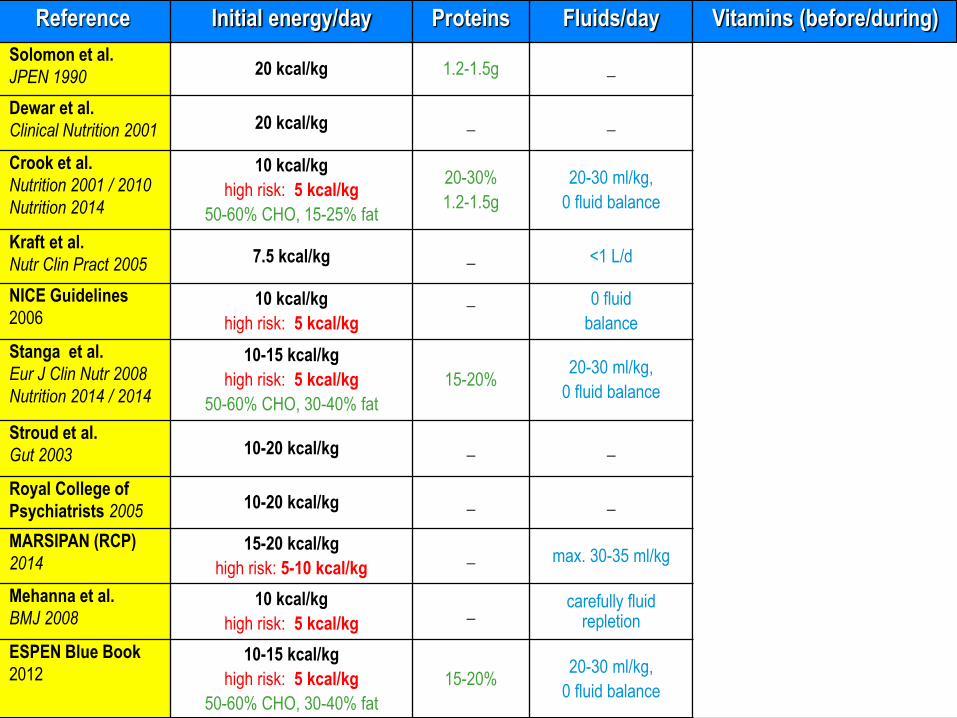
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016Reference Initial energy/day Proteins Fluids/day Vitamins (before/during)
Solomon et al.
JPEN 1990 20 kcal/kg 1.2-1.5g _ _
Dewar et al.
Clinical Nutrition 2001 20 kcal/kg _ _thiamine
IV or PO for 2 d
Crook et al.
Nutrition 2001 / 2010
Nutrition 2014
10 kcal/kg
high risk: 5 kcal/kg
50-60% CHO, 15-25% fat
20-30%
1.2-1.5g
20-30 ml/kg,
0 fluid balance
Thiamine 300 mg IV , than 100 mg daily during refeeding. In addition Vit B12, Vit B6 and folate
Kraft et al.
Nutr Clin Pract 2005 7.5 kcal/kg _ <1 L/dthiamine 50-100 mg IV or 100 mg PO for 5-7 d & multivitamin
NICE Guidelines
200610 kcal/kg
high risk: 5 kcal/kg
_ 0 fluid
balance
200-300 mg thiamine PO for 10 d & multivitamin for 10 days
Stanga et al.
Eur J Clin Nutr 2008
Nutrition 2014 / 2014
10-15 kcal/kg
high risk: 5 kcal/kg
50-60% CHO, 30-40% fat
15-20% 20-30 ml/kg,
0 fluid balance
200-300 mg thiamine IV or PO for 3 d & multivitamin for 10 days
Stroud et al.
Gut 2003 10-20 kcal/kg _ _thiamine and B vitamins IV for 3 days
Royal College of
Psychiatrists 200510-20 kcal/kg _ _ _
MARSIPAN (RCP)
201415-20 kcal/kg
high risk: 5-10 kcal/kg_ max. 30-35 ml/kg thiamine PO 4x/d for 7-10 days
Mehanna et al.
BMJ 200810 kcal/kg
high risk: 5 kcal/kg_
carefully fluid repletion
200-300 mg thiamine PO for 10 d & multivitamin for 10 days
ESPEN Blue Book
201210-15 kcal/kg
high risk: 5 kcal/kg
50-60% CHO, 30-40% fat
15-20%20-30 ml/kg,
0 fluid balance
200-300 mg thiamine IV or PO for 3 d & multivitamin for 10 days

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016Reference Initial energy/day Proteins Fluids/day Vitamins (before/during)
Solomon et al.
JPEN 1990 20 kcal/kg 1.2-1.5g _ _
Dewar et al.
Clinical Nutrition 2001 20 kcal/kg _ _thiamine
IV or PO for 2 d
Crook et al.
Nutrition 2001 / 2010
Nutrition 2014
10 kcal/kg
high risk: 5 kcal/kg
50-60% CHO, 15-25% fat
20-30%
1.2-1.5g
20-30 ml/kg,
0 fluid balance
Thiamine 300 mg IV , than 100 mg daily during refeeding. In addition Vit B12, Vit B6 and folate
Kraft et al.
Nutr Clin Pract 2005 7.5 kcal/kg _ <1 L/dthiamine 50-100 mg IV or 100 mg PO for 5-7 d & multivitamin
NICE Guidelines
200610 kcal/kg
high risk: 5 kcal/kg
_ 0 fluid
balance
200-300 mg thiamine PO for 10 d & multivitamin for 10 days
Stanga et al.
Eur J Clin Nutr 2008
Nutrition 2014 / 2014
10-15 kcal/kg
high risk: 5 kcal/kg
50-60% CHO, 30-40% fat
15-20% 20-30 ml/kg,
0 fluid balance
200-300 mg thiamine IV or PO for 3 d & multivitamin for 10 days
Stroud et al.
Gut 2003 10-20 kcal/kg _ _thiamine and B vitamins IV for 3 days
Royal College of
Psychiatrists 200510-20 kcal/kg _ _ _
MARSIPAN (RCP)
201415-20 kcal/kg
high risk: 5-10 kcal/kg_ max. 30-35 ml/kg thiamine PO 4x/d for 7-10 days
Mehanna et al.
BMJ 200810 kcal/kg
high risk: 5 kcal/kg_
carefully fluid repletion
200-300 mg thiamine PO for 10 d & multivitamin for 10 days
ESPEN Blue Book
201210-15 kcal/kg
high risk: 5 kcal/kg
50-60% CHO, 30-40% fat
15-20%20-30 ml/kg,
0 fluid balance
200-300 mg thiamine IV or PO for 3 d & multivitamin for 10 days
Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016Reference Initial energy/day Proteins Fluids/day Vitamins (before/during)
Solomon et al.
JPEN 1990 20 kcal/kg 1.2-1.5g _ _
Dewar et al.
Clinical Nutrition 2001 20 kcal/kg _ _thiamine
IV or PO for 2 d
Crook et al.
Nutrition 2001 / 2010
Nutrition 2014
10 kcal/kg
high risk: 5 kcal/kg
50-60% CHO, 15-25% fat
20-30%
1.2-1.5g
20-30 ml/kg,
0 fluid balance
Thiamine 300 mg IV , than 100 mg daily during refeeding. In addition Vit B12, Vit B6 and folate
Kraft et al.
Nutr Clin Pract 2005 7.5 kcal/kg _ <1 L/dthiamine 50-100 mg IV or 100 mg PO for 5-7 d & multivitamin
NICE Guidelines
200610 kcal/kg
high risk: 5 kcal/kg
_ 0 fluid
balance
200-300 mg thiamine PO for 10 d & multivitamin for 10 days
Stanga et al.
Eur J Clin Nutr 2008
Nutrition 2014 / 2014
10-15 kcal/kg
high risk: 5 kcal/kg
50-60% CHO, 30-40% fat
15-20% 20-30 ml/kg,
0 fluid balance
200-300 mg thiamine IV or PO for 3 d & multivitamin for 10 days
Stroud et al.
Gut 2003 10-20 kcal/kg _ _thiamine and B vitamins IV for 3 days
Royal College of
Psychiatrists 200510-20 kcal/kg _ _ _
MARSIPAN (RCP)
201415-20 kcal/kg
high risk: 5-10 kcal/kg_ max. 30-35 ml/kg thiamine PO 4x/d for 7-10 days
Mehanna et al.
BMJ 200810 kcal/kg
high risk: 5 kcal/kg_
carefully fluid repletion
200-300 mg thiamine PO for 10 d & multivitamin for 10 days
ESPEN Blue Book
201210-15 kcal/kg
high risk: 5 kcal/kg
50-60% CHO, 30-40% fat
15-20%20-30 ml/kg,
0 fluid balance
200-300 mg thiamine IV or PO for 3 d & multivitamin for 10 days

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016Reference Initial energy/day Proteins Fluids/day Vitamins (before/during)
Solomon et al.
JPEN 1990 20 kcal/kg 1.2-1.5g _ _
Dewar et al.
Clinical Nutrition 2001 20 kcal/kg _ _thiamine
IV or PO for 2 d
Crook et al.
Nutrition 2001 / 2010
Nutrition 2014
10 kcal/kg
high risk: 5 kcal/kg
50-60% CHO, 15-25% fat
20-30%
1.2-1.5g
20-30 ml/kg,
0 fluid balance
thiamine 300 mg IV , than 100 mg daily during refeeding. In addition Vit B12, Vit B6 and folate
Kraft et al.
Nutr Clin Pract 2005 7.5 kcal/kg _ <1 L/dthiamine 50-100 mg IV or 100 mg PO for 5-7 d & multivitamin
NICE Guidelines
200610 kcal/kg
high risk: 5 kcal/kg
_ 0 fluid
balance
200-300 mg thiamine PO for 10 d & multivitamin for 10 days
Stanga et al.
Eur J Clin Nutr 2008
Nutrition 2014 / 2014
10-15 kcal/kg
high risk: 5 kcal/kg
50-60% CHO, 30-40% fat
15-20% 20-30 ml/kg,
0 fluid balance
200-300 mg thiamine IV or PO for 3 d & multivitamin for 10 days
Stroud et al.
Gut 2003 10-20 kcal/kg _ _thiamine and B vitamins IV for 3 days
Royal College of
Psychiatrists 200510-20 kcal/kg _ _ _
MARSIPAN (RCP)
201415-20 kcal/kg
high risk: 5-10 kcal/kg_ max. 30-35 ml/kg thiamine PO 4x/d for 7-10 days
Mehanna et al.
BMJ 200810 kcal/kg
high risk: 5 kcal/kg_
carefully fluid repletion
200-300 mg thiamine PO for 10 d & multivitamin for 10 days
ESPEN Blue Book
201210-15 kcal/kg
high risk: 5 kcal/kg
50-60% CHO, 30-40% fat
15-20%20-30 ml/kg,
0 fluid balance
200-300 mg thiamine IV or PO for 3 d & multivitamin for 10 days

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016Reference Initial energy/day Proteins Fluids/day Vitamins (before/during)
Solomon et al.
JPEN 1990 20 kcal/kg 1.2-1.5g _ _
Dewar et al.
Clinical Nutrition 2001 20 kcal/kg _ _thiamine
IV or PO for 2 d
Crook et al.
Nutrition 2001 / 2010
Nutrition 2014
10 kcal/kg
high risk: 5 kcal/kg
50-60% CHO, 15-25% fat
20-30%
1.2-1.5g
20-30 ml/kg,
0 fluid balance
Thiamine 300 mg IV , than 100 mg daily during refeeding. In addition Vit B12, Vit B6 and folate
Kraft et al.
Nutr Clin Pract 2005 7.5 kcal/kg _ <1 L/dthiamine 50-100 mg IV or 100 mg PO for 5-7 d & multivitamin
NICE Guidelines
200610 kcal/kg
high risk: 5 kcal/kg
_ 0 fluid
balance
200-300 mg thiamine PO for 10 d & multivitamin for 10 days
Stanga et al.
Eur J Clin Nutr 2008
Nutrition 2014 / 2014
10-15 kcal/kg
high risk: 5 kcal/kg
50-60% CHO, 30-40% fat
15-20% 20-30 ml/kg,
0 fluid balance
200-300 mg thiamine IV or PO for 3 d & multivitamin for 10 days
Stroud et al.
Gut 2003 10-20 kcal/kg _ _thiamine and B vitamins IV for 3 days
Royal College of
Psychiatrists 200510-20 kcal/kg _ _ _
MARSIPAN (RCP)
201415-20 kcal/kg
high risk: 5-10 kcal/kg_ max. 30-35 ml/kg thiamine PO 4x/d for 7-10 days
Mehanna et al.
BMJ 200810 kcal/kg
high risk: 5 kcal/kg_
carefully fluid repletion
200-300 mg thiamine PO for 10 d & multivitamin for 10 days
ESPEN Blue Book
201210-15 kcal/kg
high risk: 5 kcal/kg
50-60% CHO, 30-40% fat
15-20%20-30 ml/kg,
0 fluid balance
200-300 mg thiamine IV or PO for 3 d & multivitamin for 10 days

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
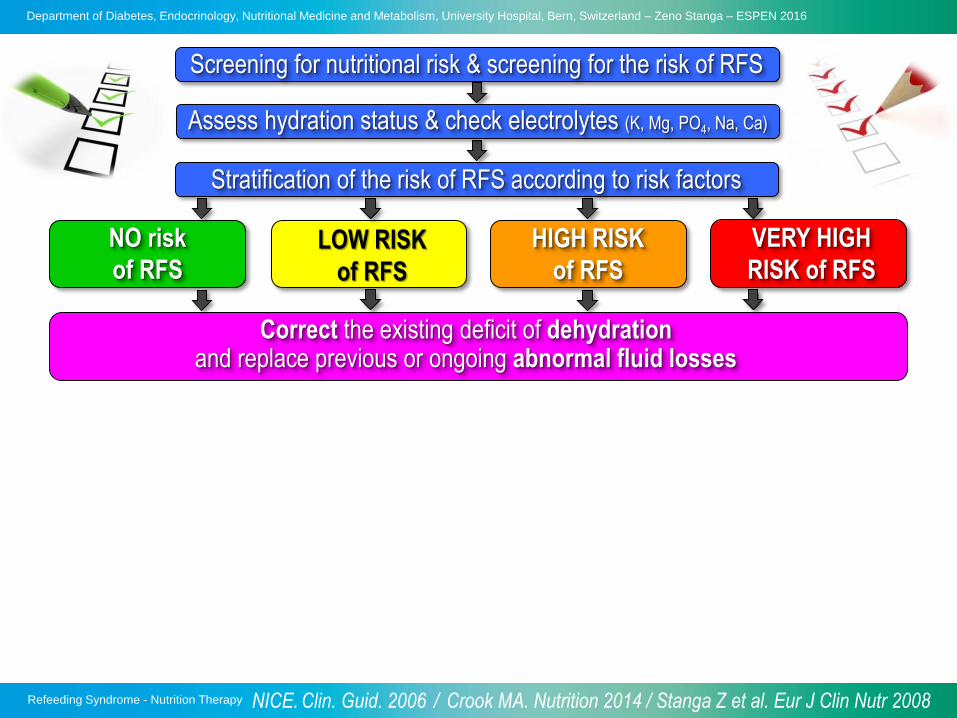
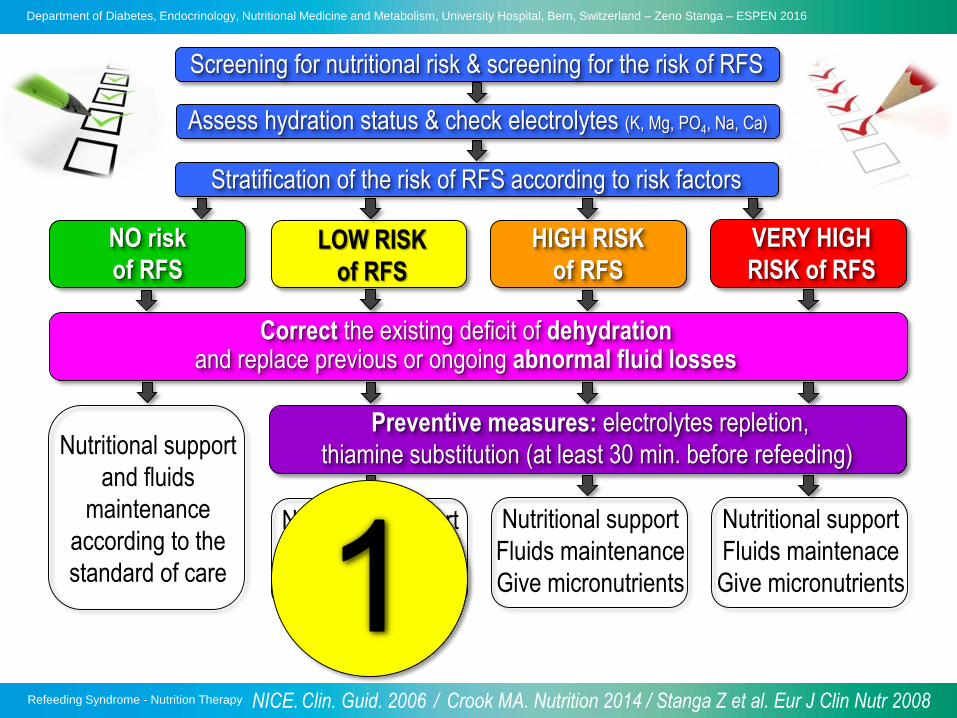
NO risk
of RFSLOW RISK
of RFS
HIGH RISK
of RFS
VERY HIGH
RISK of RFS
Screening for nutritional risk & screening for the risk of RFS
Stratification of the risk of RFS according to risk factors
Assess hydration status & check electrolytes (K, Mg, PO4, Na, Ca)

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
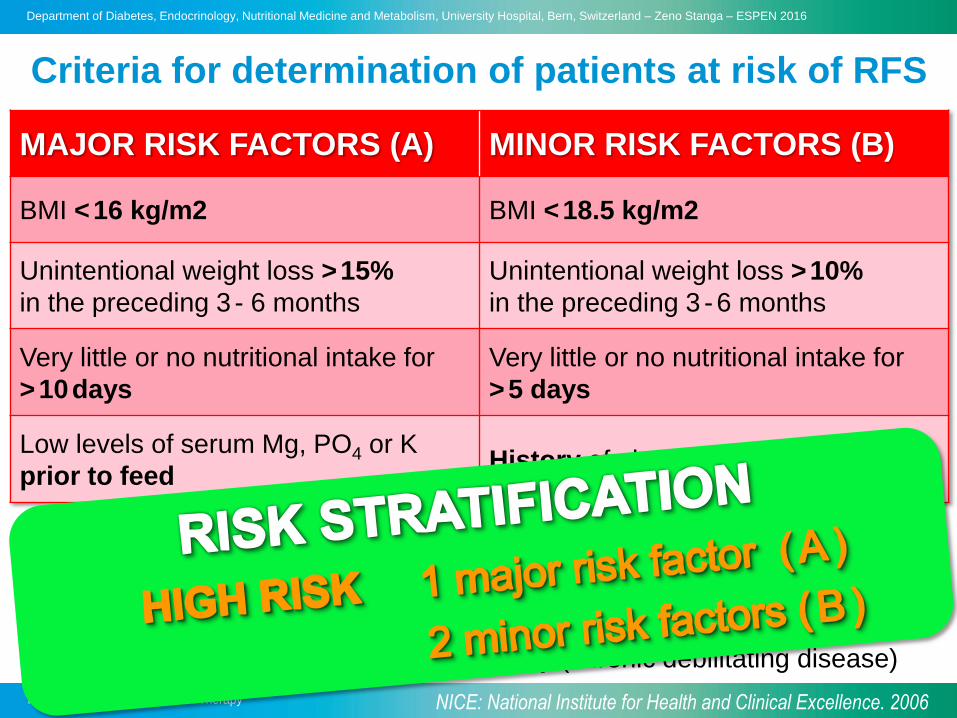
MAJOR RISK FACTORS (A) MINOR RISK FACTORS (B)
BMI <16 kg/m2 BMI <18.5 kg/m2
Unintentional weight loss >15%
in the preceding 3 - 6 months
Unintentional weight loss >10%
in the preceding 3 -6 months
Very little or no nutritional intake for
>10days
Very little or no nutritional intake for
>5 days
Low levels of serum Mg, PO4 or K
prior to feedHistory of alcool or drug abuse
Criteria for determination of patients at risk of RFS
NICE: National Institute for Health and Clinical Excellence. 2006

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
MAJOR RISK FACTORS (A) MINOR RISK FACTORS (B)
BMI <16 kg/m2 BMI <18.5 kg/m2
Unintentional weight loss >15%
in the preceding 3 - 6 months
Unintentional weight loss >10%
in the preceding 3 -6 months
Very little or no nutritional intake for
>10days
Very little or no nutritional intake for
>5 days
Low levels of serum Mg, PO4 or K
prior to feedHistory of alcool or drug abuse
Criteria for determination of patients at risk of RFS
RISK BY PATIENT’S CATEGORY
• Hunger strike, eating disorders, chronic severe dieting
• After bariatric surgery, short bowel syndrome
• Oncology patients and fraily elderly (chronic debilitating disease)
NICE: National Institute for Health and Clinical Excellence. 2006

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
MAJOR RISK FACTORS (A) MINOR RISK FACTORS (B)
BMI <16 kg/m2 BMI <18.5 kg/m2
Unintentional weight loss >15%
in the preceding 3 - 6 months
Unintentional weight loss >10%
in the preceding 3 -6 months
Very little or no nutritional intake for
>10days
Very little or no nutritional intake for
>5 days
Low levels of serum Mg, PO4 or K
prior to feedHistory of alcool or drug abuse
Criteria for determination of patients at risk of RFS
RISK BY PATIENT’S CATEGORY
• Hunger strike, eating disorders, chronic severe dieting
• After bariatric surgery, short bowel syndrome
• Oncology patients and fraily elderly (chronic debilitating disease)
NICE: National Institute for Health and Clinical Excellence. 2006
Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
MAJOR RISK FACTORS (A) MINOR RISK FACTORS (B)
BMI <16 kg/m2 BMI <18.5 kg/m2
Unintentional weight loss >15%
in the preceding 3 - 6 months
Unintentional weight loss >10%
in the preceding 3 -6 months
Very little or no nutritional intake for
>10days
Very little or no nutritional intake for
>5 days
Low levels of serum Mg, PO4 or K
prior to feedHistory of alcool or drug abuse
Criteria for determination of patients at risk of RFS
RISK BY PATIENT’S CATEGORY
• Hunger strike, eating disorders, chronic severe dieting
• After bariatric surgery, short bowel syndrome
• Oncology patients and fraily elderly (chronic debilitating disease)
NICE: National Institute for Health and Clinical Excellence. 2006

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
MAJOR RISK FACTORS (A) MINOR RISK FACTORS (B)
BMI <16 kg/m2 BMI <18.5 kg/m2
Unintentional weight loss >15%
in the preceding 3 - 6 months
Unintentional weight loss >10%
in the preceding 3 -6 months
Very little or no nutritional intake for
>10days
Very little or no nutritional intake for
>5 days
Low levels of serum Mg, PO4 or K
prior to feedHistory of alcool or drug abuse
Criteria for determination of patients at risk of RFS
RISK BY PATIENT’S CATEGORY
• Hunger strike, eating disorders, chronic severe dieting
• After bariatric surgery, short bowel syndrome
• Oncology patients and fraily elderly (chronic debilitating disease)
NICE: National Institute for Health and Clinical Excellence. 2006
Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
NO risk
of RFSLOW RISK
of RFS
HIGH RISK
of RFS
VERY HIGH
RISK of RFS
Screening for nutritional risk & screening for the risk of RFS
Stratification of the risk of RFS according to risk factors
Assess hydration status & check electrolytes (K, Mg, PO4, Na, Ca)
Correct the existing deficit of dehydrationand replace previous or ongoing abnormal fluid losses
NICE. Clin. Guid. 2006 / Crook MA. Nutrition 2014 / Stanga Z et al. Eur J Clin Nutr 2008
Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Fluid replacement
1• Correct the existing deficit of dehydration
2
• Replace losses: the most appropriate fluid to use
is that which most closely matches any previous
or ongoing losses
3
• Maintenance prescriptions should aim to provide
sufficient water and electrolytes to maintain
normal status of body fluid compartments
CONSIDER 3 ASPECTS OF REPLACEMENT

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
FEATURE
MILD
DEHYDRATION
<5%
MODERATE
DEHYDRATION
5-10%
SEVERE
DEHYDRATION
>10%
Pulse
ratenormal
slight
increasedrapid, weak
>90 bpm
Respiratory
ratenormal
slightly
increasedrapid
>20 breaths/min
Systolic
bpnormal
normal/
orthostatichypotension<100 mmHg
Mucosa
membraneslightly dry very dry parched
Urine
outputdecreased
oliguria<500 ml/d
anuria<50 ml/d
Clinical signs of dehydration
NICE Guidelines. May 2013

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
FEATURE
MILD
DEHYDRATION
<5%
MODERATE
DEHYDRATION
5-10%
SEVERE
DEHYDRATION
>10%
Pulse
ratenormal
slight
increasedrapid, weak
>90 bpm
Respiratory
ratenormal
slightly
increasedrapid
>20 breaths/min
Systolic
bpnormal
normal/
orthostatichypotension<100 mmHg
Mucosa
membraneslightly dry very dry parched
Urine
outputdecreased
oliguria<500 ml/d
anuria<50 ml/d
Clinical signs of dehydration
NICE Guidelines. May 2013

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Fluid replacement
1• Correct the existing deficit of dehydration
2
• Replace losses: the most appropriate fluid to use
is that which most closely matches any previous
or ongoing losses
3
• Maintenance prescriptions should aim to provide
sufficient water and electrolytes to maintain
normal status of body fluid compartments
CONSIDER 3 ASPECTS OF REPLACEMENT

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Cristalloid solutions for fluid replacement
INFUSION
(1000 ml)
Na
(mmol)
Cl
(mmol)
K
(mmol)
Glucose
(g)
Lactate
(mmol)
Glucose 5% - - - 50 -
Glucosaline 1:1 77 7 - 25 -
Glucosaline 2:1 55 55 - 33 -
Glucosaline 4:1 31 31 - 40 -
Saline 0.9% 154 154 - - -
Ringer’s lactate 130 109 4 - 28
Hartmann’s 131 111 5 - 29
LOBO DN et al. 2013, ISBN 978-3-89556-058-3

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Fluid replacement
1• Correct the existing deficit of dehydration
2
• Replace losses: the most appropriate fluid to use
is that which most closely matches any previous
or ongoing losses
3
• Maintenance prescriptions should aim to provide
sufficient water and electrolytes to maintain
normal status of body fluid compartments
CONSIDER 3 ASPECTS OF REPLACEMENT

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
NO risk
of RFSLOW RISK
of RFS
HIGH RISK
of RFS
VERY HIGH
RISK of RFS
Screening for nutritional risk & screening for the risk of RFS
Stratification of the risk of RFS according to risk factors
Assess hydration status & check electrolytes (K, Mg, PO4, Na, Ca)
Correct the existing deficit of dehydrationand replace previous or ongoing abnormal fluid losses
Nutritional support
and fluids
maintenance
according to the
standard of care
NICE. Clin. Guid. 2006 / Crook MA. Nutrition 2014 / Stanga Z et al. Eur J Clin Nutr 2008

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
NO risk
of RFSLOW RISK
of RFS
HIGH RISK
of RFS
VERY HIGH
RISK of RFS
Screening for nutritional risk & screening for the risk of RFS
Stratification of the risk of RFS according to risk factors
Assess hydration status & check electrolytes (K, Mg, PO4, Na, Ca)
Correct the existing deficit of dehydrationand replace previous or ongoing abnormal fluid losses
Preventive measures: electrolytes repletion,
thiamine substitution (at least 30 min. before refeeding) Nutritional support
and fluids
maintenance
according to the
standard of care
Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
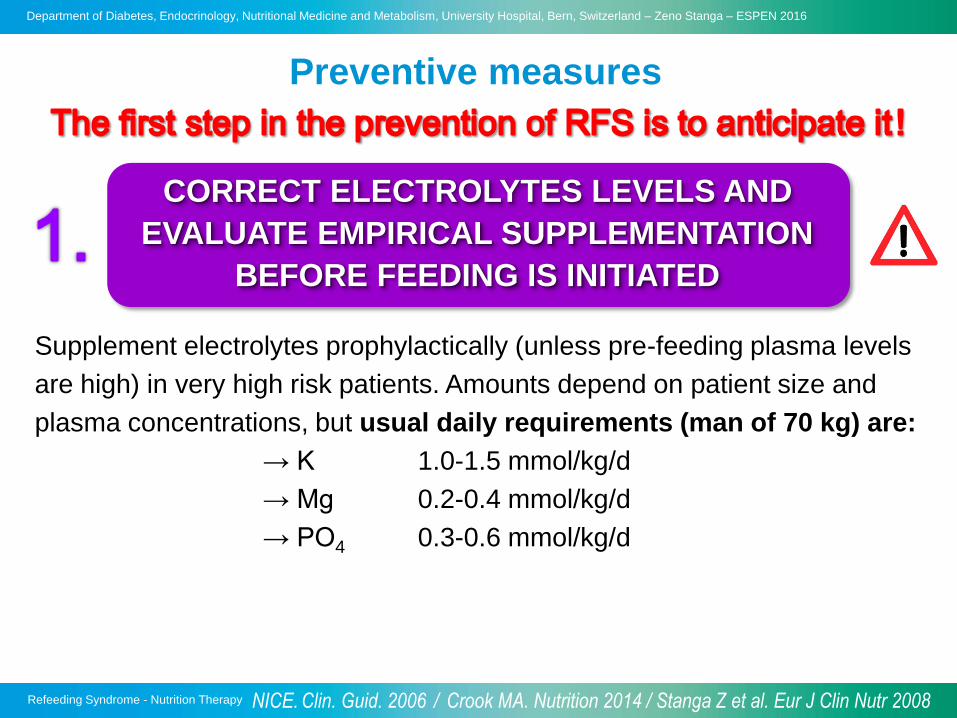
Preventive measures
Supplement electrolytes prophylactically (unless pre-feeding plasma levels
are high) in very high risk patients. Amounts depend on patient size and
plasma concentrations, but usual daily requirements (man of 70 kg) are:
→ K 1.0-1.5 mmol/kg/d
→ Mg 0.2-0.4 mmol/kg/d
→ PO4 0.3-0.6 mmol/kg/d
CORRECT ELECTROLYTES LEVELS AND
EVALUATE EMPIRICAL SUPPLEMENTATION
BEFORE FEEDING IS INITIATED
NICE. Clin. Guid. 2006 / Crook MA. Nutrition 2014 / Stanga Z et al. Eur J Clin Nutr 2008

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Predictors of RFS
Rio A et al. BMJ Open 2013
• Prospective cohort study
• 243 patients starting EE oder PE
• 133 at risk of RFS
• Predictors of RFS (sensitivity 67%, specificity 80%)
Poor intake for >10 days
Weight loss of >15%
Low plasma magnesium (<0.7 mmol/L; p=0.021)
• STARVATION is the most reliable predictor

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Preventive measures
Supplement electrolytes prophylactically (unless pre-feeding plasma levels
are high) in very high risk patients. Amounts depend on patient size and
plasma concentrations, but usual daily requirements (man of 70 kg) are:
→ K 1.0-1.5 mmol/kg/d
→ Mg 0.2-0.4 mmol/kg/d
→ PO4 0.3-0.6 mmol/kg/d
CORRECT ELECTROLYTES LEVELS AND
EVALUATE EMPIRICAL SUPPLEMENTATION
BEFORE FEEDING IS INITIATED
GIVE 200-300 mg THIAMINE I.V. OR
ORALLY BEFORE FEEDING
NICE. Clin. Guid. 2006 / Crook MA. Nutrition 2014 / Stanga Z et al. Eur J Clin Nutr 2008
Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
NO risk
of RFSLOW RISK
of RFS
HIGH RISK
of RFS
VERY HIGH
RISK of RFS
Screening for nutritional risk & screening for the risk of RFS
Stratification of the risk of RFS according to risk factors
Assess hydration status & check electrolytes (K, Mg, PO4, Na, Ca)
Correct the existing deficit of dehydrationand replace previous or ongoing abnormal fluid losses
Nutritional support
and fluids
maintenance
according to the
standard of care
Preventive measures: electrolytes repletion,
thiamine substitution (at least 30 min. before refeeding)
Nutritional support
Fluids maintenace
Give micronutrients
Nutritional support
Fluids maintenance
Give micronutrients
Nutritional support
Fluids maintenace
Give micronutrients
NICE. Clin. Guid. 2006 / Crook MA. Nutrition 2014 / Stanga Z et al. Eur J Clin Nutr 2008

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
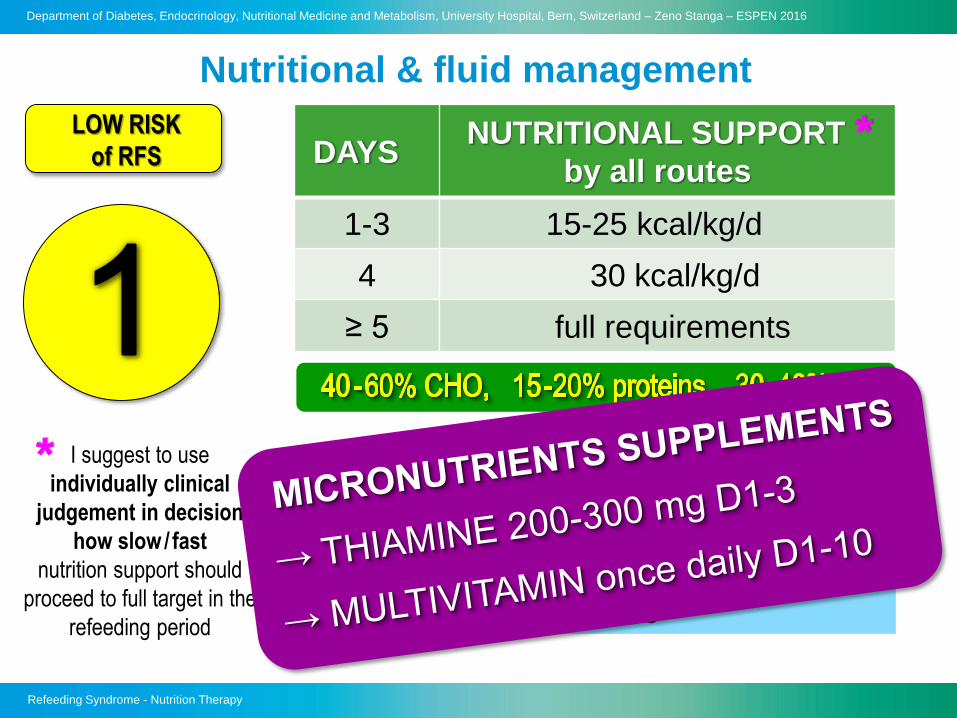
LOW RISK
of RFS DAYSNUTRITIONAL SUPPORT
by all routes
1-3 15-25 kcal/kg/d
4 30 kcal/kg/d
≥ 5 full requirements
I suggest to use
individually clinical
judgement in decision
how slow / fast
nutrition support should
proceed to full target in the
refeeding period
*
FLUID AND SODIUM BALANCE
Fluids to maintain zero balance,approx. 30-35 ml/kg/d
No restriction in salt intake
Nutritional & fluid management
*
Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
LOW RISK
of RFS DAYSNUTRITIONAL SUPPORT
by all routes
1-3 15-25 kcal/kg/d
4 30 kcal/kg/d
≥ 5 full requirements
I suggest to use
individually clinical
judgement in decision
how slow / fast
nutrition support should
proceed to full target in the
refeeding period
*
*FLUID AND SODIUM BALANCE
Fluids to maintain zero balance,approx. 30-35 ml/kg/d
No restriction in salt intake
Nutritional & fluid management

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
NO risk
of RFSLOW RISK
of RFS
HIGH RISK
of RFS
VERY HIGH
RISK of RFS
Screening for nutritional risk & screening for the risk of RFS
Stratification of the risk of RFS according to risk factors
Assess hydration status & check electrolytes (K, Mg, PO4, Na, Ca)
Correct the existing deficit of dehydrationand replace previous or ongoing abnormal fluid losses
Nutritional support
and fluids
maintenance
according to the
standard of care
Preventive measures: electrolytes repletion,
thiamine substitution (at least 30 min. before refeeding)
Nutritional support
Fluids maintenace
Give micronutrients
Nutritional support
Fluids maintenance
Give micronutrients
Nutritional support
Fluids maintenace
Give micronutrients
NICE. Clin. Guid. 2006 / Crook MA. Nutrition 2014 / Stanga Z et al. Eur J Clin Nutr 2008
Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
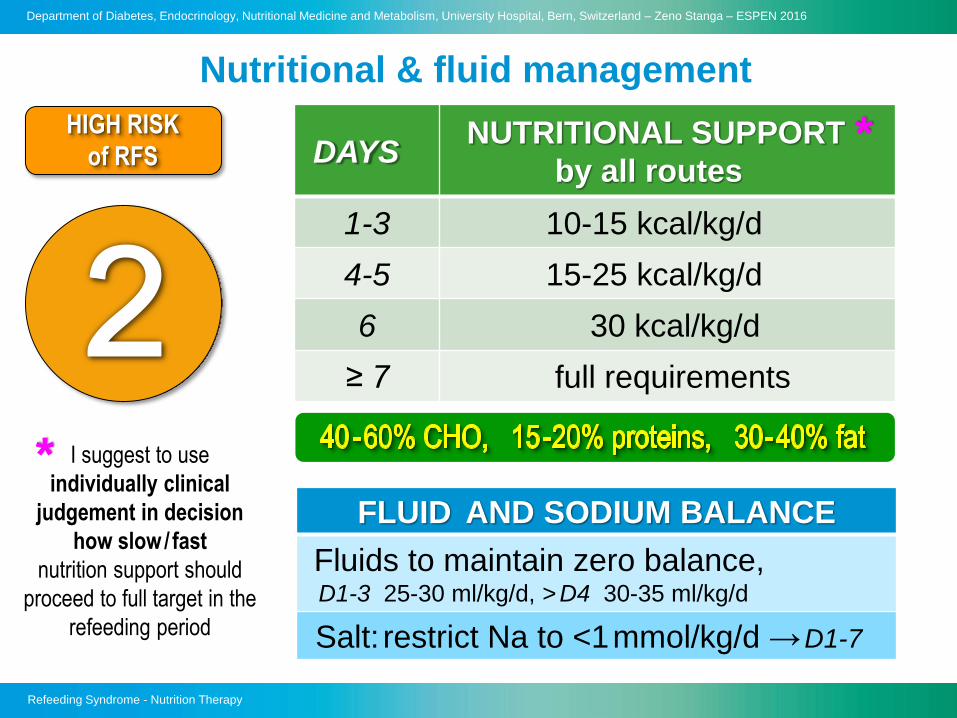
Nutritional & fluid management
HIGH RISK
of RFS DAYSNUTRITIONAL SUPPORT
by all routes
1-3 10-15 kcal/kg/d
4-5 15-25 kcal/kg/d
6 30 kcal/kg/d
≥ 7 full requirements
I suggest to use
individually clinical
judgement in decision
how slow / fast
nutrition support should
proceed to full target in the
refeeding period
*
FLUID AND SODIUM BALANCE
Fluids to maintain zero balance,D1-3 25-30 ml/kg/d, > D4 30-35 ml/kg/d
Salt: restrict Na to <1mmol/kg/d →D1-7
*

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Intracellular volume (ICV)
Distribution of infused solutions
40 % 15 % 5 %
Colloids
0.9% NaCl
Interstitial Intravascular
fluid fluid
5% Glucose
Extracellular volume (ECV)
LOBO DN et al. 2013, ISBN 978-3-89556-058-3

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Intracellular volume (ICV)
Distribution of infused solutions
40 % 15 % 5 %
Colloids
0.9% NaCl
Interstitial Intravascular
fluid fluid
5% Glucose
Extracellular volume (ECV)
LOBO DN et al. 2013, ISBN 978-3-89556-058-3

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Cristalloid solutions for fluid maintenance
INFUSION
(1000 ml)
Na
(mmol)
Cl
(mmol)
K
(mmol)
Glucose
(g)
Lactate
(mmol)
Glocose 5% - - - 50 -
Glucosaline 1:1 77 7 - 25 -
Glucosaline 2:1 55 55 - 33 -
Glucosaline 4:1 31 31 - 40 -
Saline 0.9% 154 154 - - -
Ringer’s lactate 130 109 4 - 28
Hartmann’s 131 111 5 - 29
9g NaCl
6g NaCl
6g NaCl
4.5g NaCl
3g NaCl
1.8g NaCl
0g NaCl
LOBO DN et al. 2013, ISBN 978-3-89556-058-3

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Nutritional & fluid management
HIGH RISK
of RFS DAYSNUTRITIONAL SUPPORT
by all routes
1-3 10-15 kcal/kg/d
4-5 15-25 kcal/kg/d
6 30 kcal/kg/d
≥ 7 full requirements
I suggest to use
individually clinical
judgement in decision
how slow / fast
nutrition support should
proceed to full target in the
refeeding period
*
FLUID AND SODIUM BALANCE
Fluids to maintain zero balance,D1-3 25-30 ml/kg/d, > D4 30-35 ml/kg/d
Salt: restrict Na to <1mmol/kg/d →D1-7
*

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
NO risk
of RFSLOW RISK
of RFS
HIGH RISK
of RFS
VERY HIGH
RISK of RFS
Screening for nutritional risk & screening for the risk of RFS
Stratification of the risk of RFS according to risk factors
Assess hydration status & Check electrolytes (K, Mg, PO4, Na, Ca)
Correct the existing deficit of dehydrationand replace previous or ongoing abnormal fluid losses
Nutritional support
and fluids
maintenance
according to the
standard of care
Preventive measures: electrolytes repletion,
thiamine substitution (at least 30 min. before refeeding)
Nutritional support
Fluids maintenace
Give micronutrients
Nutritional support
Fluids maintenance
Give micronutrients
Nutritional support
Fluids maintenace
Give micronutrients
NICE. Clin. Guid. 2006 / Crook MA. Nutrition 2014 / Stanga Z et al. Eur J Clin Nutr 2008

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
VERY HIGH
RISK of RFS DAYSNUTRITIONAL SUPPORT
by all routes
1-3 5-10 kcal/kg/d
4-6 10-20 kcal/kg/d
7-9 20-30 kcal/kg/d
≥ 10 full requirements
I suggest to use
individually clinical
judgement in decision
how slow / fast
nutrition support should
proceed to full target in the
refeeding period
*
FLUID AND SODIUM BALANCE
Fluids to maintain zero balance,D1-3 20-25 ml/kg/d, D4-6 25-30 ml/kg/d, > D7 25-35 ml/kg/d
Salt: restrict Na to <1mmol/kg/d →D1-10
Nutritional & fluid management
*

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
VERY HIGH
RISK of RFS DAYSNUTRITIONAL SUPPORT
by all routes
1-3 5-10 kcal/kg/d
4-6 10-20 kcal/kg/d
7-9 20-30 kcal/kg/d
≥ 10 full requirements
I suggest to use
individually clinical
judgement in decision
how slow / fast
nutrition support should
proceed to full target in the
refeeding period
*
FLUID AND SODIUM BALANCE
Fluids to maintain zero balance,D1-3 20-25 ml/kg/d, D4-6 25-30 ml/kg/d, > D7 25-35 ml/kg/d
Salt: restrict Na to <1mmol/kg/d →D1-10
Nutritional & fluid management
*

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
NO risk
of RFSLOW RISK
of RFS
HIGH RISK
of RFS
VERY HIGH
RISK of RFS
Screening for nutritional risk & screening for the risk of RFS
Stratification of the risk of RFS according to risk factors
Assess hydration status & check electrolytes (K, Mg, PO4, Na, Ca)
Correct the existing deficit of dehydrationand replace previous or ongoing abnormal fluid losses
Nutritional support
and fluids
maintenance
according to the
standard of care
Preventive measures: electrolytes repletion,
thiamine substitution (at least 30 min. before refeeding)
Nutritional support
Fluids maintenace
Give micronutrients
Nutritional support
Fluids maintenance
Give micronutrients
Nutritional support
Fluids maintenace
Give micronutrients
Clinical and laboratory monitoring, management of complications
NICE. Clin. Guid. 2006 / Crook MA. Nutrition 2014 / Stanga Z et al. Eur J Clin Nutr 2008

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Monitoring
• Body weight (or fluid balance)
• Vital signs
→ blood pressure, pulse rate, respiratory rate, oxygen sat.
• Clinical examination
→ hydration state, oedema, cardiopulmonary state
• Lab serum-parameters
→ PO4, K, Mg, Na, Ca, glucose, urea, creatinine
DAY 1-3
monitor
daily
DAY 4-6
monitor
every 2nd day
DAY 7-10
monitor
1-2x wkly
Crook MA. Nutrition 2009 / Stanga Z et al. Eur J Clin Nutr 2008

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Monitoring
• Body weight (or fluid balance)
• Vital signs
→ blood pressure, pulse rate, respiratory rate, oxygen sat.
• Clinical examination
→ hydration state, oedema, cardiopulmonary state
• Lab serum-parameters
→ PO4, K, Mg, Na, Ca, glucose, urea, creatinine
DAY 1-3
monitor
daily
DAY 4-6
monitor
every 2nd day
DAY 7-10
monitor
1-2x wkly
Crook MA. Nutrition 2009 / Stanga Z et al. Eur J Clin Nutr 2008

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Monitoring
• Body weight (or fluid balance)
• Vital signs
→ blood pressure, pulse rate, respiratory rate, oxygen sat.
• Clinical examination
→ hydration state, oedema, cardiopulmonary state
• Lab serum-parameters
→ PO4, K, Mg, Na, Ca, glucose, urea, creatinine
DAY 1-3
monitor
daily
DAY 4-6
monitor
every 2nd day
DAY 7-10
monitor
1-2x wkly
Crook MA. Nutrition 2009 / Stanga Z et al. Eur J Clin Nutr 2008

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Monitoring
• Body weight (or fluid balance)
• Vital signs
→ blood pressure, pulse rate, respiratory rate, oxygen sat.
• Clinical examination
→ hydration state, oedema, cardiopulmonary state
• Lab serum-parameters
→ PO4, K, Mg, Na, Ca, glucose, urea, creatinine
DAY 1-3
monitor
daily
DAY 4-6
monitor
every 2nd day
DAY 7-10
monitor
1-2x weekly
Crook MA. Nutrition 2009 / Stanga Z et al. Eur J Clin Nutr 2008

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Monitoring
• Body weight (or fluid balance)
• Vital signs
→ blood pressure, pulse rate, respiratory rate, oxygen sat.
• Clinical examination
→ hydration state, oedema, cardiopulmonary state
• Lab serum-parameters
→ PO4, K, Mg, Na, Ca, glucose, urea, creatinine
DAY 1-3
monitor
daily
DAY 4-6
monitor
every 2nd day
DAY 7-10
monitor
1-2x weekly
Crook MA. Nutrition 2009 / Stanga Z et al. Eur J Clin Nutr 2008

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Electrolyte deficiency and replacement
POTASSIUM REPLETION
S-POTASSIUM RECOMMENDATION FOR REPLETION
Mild deficit
3.1- 3.5 mmol/l
oral replacement with 20 mmol (as KCl or other
formularies) OR i.v. replacement with 20
mmol KCl over 4-8 h → check K levels the next day
Moderate deficit
2.5 - 3.0 mmol/l
i.v. replacement with 20-40 mmol KCl over 4-8 h
→ check K levels after 8 hours
→ if not normal levels, give further 20 mmol KCL
Severe deficit
<2.5 mmol/l
i.v. replacement with 40 mmol KCl over 4-8 h
→ check K levels after 8 hours
→ if not normal levels, give further 40 mmol KCL
Marinella MA et al. Int J Clin Pract 2008 / Stanga Z et al. Eur J Clin Nutr 2008
Gennari FJ. NEJM 1998 / Boateng AA et al. Nutrition 2010 / ESPEN Blue Book 2011

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Electrolyte deficiency and replacement
POTASSIUM REPLETION
S-POTASSIUM RECOMMENDATION FOR REPLETION
Mild deficit
3.1- 3.5 mmol/l
oral replacement with 20 mmol (as KCl or other
formularies) OR i.v. replacement with 20
mmol KCl over 4-8 h → check K levels the next day
Moderate deficit
2.5 - 3.0 mmol/l
i.v. replacement with 20-40 mmol KCl over 4-8 h
→ check K levels after 8 hours
→ if not normal levels, give further 20 mmol KCL
Severe deficit
<2.5 mmol/l
i.v. replacement with 40 mmol KCl over 4-8 h
→ check K levels after 8 hours
→ if not normal levels, give further 40 mmol KCL
Marinella MA et al. Int J Clin Pract 2008 / Stanga Z et al. Eur J Clin Nutr 2008
Gennari FJ. NEJM 1998 / Boateng AA et al. Nutrition 2010 / ESPEN Blue Book 2011

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Electrolyte deficiency and replacement
POTASSIUM REPLETION
S-POTASSIUM RECOMMENDATION FOR REPLETION
Mild deficit
3.1- 3.5 mmol/l
oral replacement with 20 mmol (as KCl or other
formularies) OR i.v. replacement with 20
mmol KCl over 4-8 h → check K levels the next day
Moderate deficit
2.5 - 3.0 mmol/l
i.v. replacement with 20-40 mmol KCl over 4-8 h
→ check K levels after 8 hours
→ if not normal levels, give further 20 mmol KCL
Severe deficit
<2.5 mmol/l
i.v. replacement with 40 mmol KCl over 4-8 h
→ check K levels after 8 hours
→ if not normal levels, give further 40 mmol KCL
Marinella MA et al. Int J Clin Pract 2008 / Stanga Z et al. Eur J Clin Nutr 2008
Gennari FJ. NEJM 1998 / Boateng AA et al. Nutrition 2010 / ESPEN Blue Book 2011

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
S-MAGNESIUM RECOMMENDATION FOR REPLETION
Mild to moderate
deficit
0.5 - 0.6 mmol/l
oral replacement with 10-15 mmol Mg-chlorid or
Mg-citrat or Mg-L-aspartat
→ oral Mg should be given in divided doses to
minimise diarrhoea (absorption process is
saturated at about 5-10 mmol Mg)
Severe deficit
<0.5 mmol/l
i.v. replacement with 20-24 mmol MgSO4 (4-6 g)
over 4-8 h → reassess every 8-12 h
MAGNESIUM REPLETION
Weisinger JR et al. Lancet 1998 / Stanga Z et al. Eur J Clin Nutr 2008
Brannan GB et al. J Clin Invest 1976 / Boateng AA et al. Nutrition 2010 / ESPEN Blue Book 2011
Electrolyte deficiency and replacement

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
S-MAGNESIUM RECOMMENDATION FOR REPLETION
Mild to moderate
deficit
0.5 - 0.6 mmol/l
oral replacement with 10-15 mmol Mg-chlorid or
Mg-citrat or Mg-L-aspartat
→ oral Mg should be given in divided doses to
minimise diarrhoea (absorption process is
saturated at about 5-10 mmol Mg)
Severe deficit
<0.5 mmol/l
i.v. replacement with 20-24 mmol MgSO4 (4-6 g)
over 4-8 h → reassess every 8-12 h
MAGNESIUM REPLETION
Weisinger JR et al. Lancet 1998 / Stanga Z et al. Eur J Clin Nutr 2008
Brannan GB et al. J Clin Invest 1976 / Boateng AA et al. Nutrition 2010 / ESPEN Blue Book 2011
Electrolyte deficiency and replacement

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
S-MAGNESIUM RECOMMENDATION FOR REPLETION
Mild to moderate
deficit
0.5 - 0.6 mmol/l
oral replacement with 10-15 mmol Mg-chlorid or
Mg-citrat or Mg-L-aspartat
→ oral Mg should be given in divided doses to
minimise diarrhoea (absorption process is
saturated at about 5-10 mmol Mg)
Severe deficit
<0.5 mmol/l
i.v. replacement with 20-24 mmol MgSO4 (4-6 g)
over 4-8 h → reassess every 8-12 h
MAGNESIUM REPLETION
Weisinger JR et al. Lancet 1998 / Stanga Z et al. Eur J Clin Nutr 2008
Brannan GB et al. J Clin Invest 1976 / Boateng AA et al. Nutrition 2010 / ESPEN Blue Book 2011
Electrolyte deficiency and replacement

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
S-PHOSPHATE RECOMMENDATION FOR REPLETION
Mild deficit
0.61- 0.8 mmol/l
oral replacement with 0.3 mmol/kg/d PO4 (divided
doses to minimise diarrhoea) OR i.v. replacement
with 0.3 mmol/kg/d PO4 (as K3PO4 or Na3PO4) over
8-12 h → check PO4 levels next day
Moderate deficit
0.32 - 0.6 mmol/l
i.v. replacement with 0.6 mmol/kg/d PO4 (as K3PO4
or Na3PO4) over 8-12 h
→ check PO4 levels after 8-12h and repeat infusion
if necessary (max. of 50 mmol PO4 in 24 h).
Severe deficit
<0.32 mmol/l
same replacement therapy as above (moderate
deficit)
PHOSPHATE REPLETION
Electrolyte deficiency and replacement
Thatte L et al. Am J Med 1995 / Crook MA. Nutrition 2009 / Stanga Z et al. Eur J Clin Nutr 2008

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
S-PHOSPHATE RECOMMENDATION FOR REPLETION
Mild deficit
0.61- 0.8 mmol/l
oral replacement with 0.3 mmol/kg/d PO4 (divided
doses to minimise diarrhoea) OR i.v. replacement
with 0.3 mmol/kg/d PO4 (as K3PO4 or Na3PO4) over
8-12 h → check PO4 levels next day
Moderate deficit
0.32 - 0.6 mmol/l
i.v. replacement with 0.6 mmol/kg/d PO4 (as K3PO4
or Na3PO4) over 8-12 h
→ check PO4 levels after 8-12h and repeat infusion
if necessary (max. of 50 mmol PO4 in 24 h).
Severe deficit
<0.32 mmol/l
same replacement therapy as above (moderate
deficit)
PHOSPHATE REPLETION
Electrolyte deficiency and replacement
Thatte L et al. Am J Med 1995 / Crook MA. Nutrition 2009 / Stanga Z et al. Eur J Clin Nutr 2008

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
S-PHOSPHATE RECOMMENDATION FOR REPLETION
Mild deficit
0.61- 0.8 mmol/l
oral replacement with 0.3 mmol/kg/d PO4 (divided
doses to minimise diarrhoea) OR i.v. replacement
with 0.3 mmol/kg/d PO4 (as K3PO4 or Na3PO4) over
8-12 h → check PO4 levels next day
Moderate deficit
0.32 - 0.6 mmol/l
i.v. replacement with 0.6 mmol/kg/d PO4 (as K3PO4
or Na3PO4) over 8-12 h
→ check PO4 levels after 8-12h and repeat infusion
if necessary (max. of 50 mmol PO4 in 24 h).
Severe deficit
<0.32 mmol/l
same replacement therapy as above (moderate
deficit)
PHOSPHATE REPLETION
Electrolyte deficiency and replacement
Thatte L et al. Am J Med 1995 / Crook MA. Nutrition 2009 / Stanga Z et al. Eur J Clin Nutr 2008

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016E
ne
rgy (
kc
al)
S-P
O4
(m
mo
l/l)
Enrollment: 72h after start feeding (EE/PE) & PO4↓, 1:1 rand., stratification by PO4 > 0.32 vs ≤ 0.32 mmol/l
and BMI < 18 vs ≤ 18 kg/m2 n = 170 Standard care n = 169 Hypocaloric management
PO4-substitution i.v. (mmol )
Energy intake/d (mean) Lowest daily s-phosphates
Days Days
(15 ICUs)
Doig GS et al. Lancet Respir Med 2015

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Doig GS et al. Lancet Respir Med 2015
Su
rviv
al
(%
)
Overall survival time
Survival time (days )
p = 0.002
78%
91%

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Culkin A. Copenhagen 2013

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Pending questions
• To date only low quality evidence exists........
• Too cautious energy step up?
so far conflicting statements
possible start feeding higher energy/CHO in hospital?
• Build-up of full food intake within 3-4 days?
reduction of the catabolic phase
• Do we have to give electrolytes in a prophylactic way?
prevention is better than cure
• Reliable predictors?
• How important is the clinical examination?

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
The big challenge

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
Take home message

Refeeding Syndrome - Nutrition Therapy
Department of Diabetes, Endocrinology, Nutritional Medicine and Metabolism, University Hospital, Bern, Switzerland – Zeno Stanga – ESPEN 2016
UNIVERSITY HOSPITAL BERN