esophagus - rawalpindi medical college media club/4th year/patholgy 4tthyr/git... · histology...
TRANSCRIPT

ESOPHAGUS

ESOPHAGUS
Normal Anatomy Muscular tube, 25 cm in length in adults.
Extending from the upper esophageal sphincter at 15-18 c m from the incisors to lower esophageal sphincter at 40 c m (variable).
Histology Lined by stratified squamous non-keratinized epithelium.
Basal layer 4 cell thick; not more than 15% of total epithelial thickness. Melanocytes & neuroendocrine cells maybe found
Lamina propria: mucous glands in distal portion (cardiac glands)
Muscularis Mucosae: Thicker than other parts of GIT
Submucosa: Submucosal glands

ESOPHAGUS
Muscularis propria: Admixture of striated & smooth muscle in the upper quarter, only smooth muscle in the rest of the organ.
No serosal layer, except for the most distal portion.
Autonomic nervous system: Meissner’s plexus in submucosa Auerbach (Myenteric) plexus in muscularis propria
Lymphatics: Upper third drains into cervical nodes, middle third into paraesophageal & paratracheal nodes, & lower third into nodes around aorta & celiac axis.
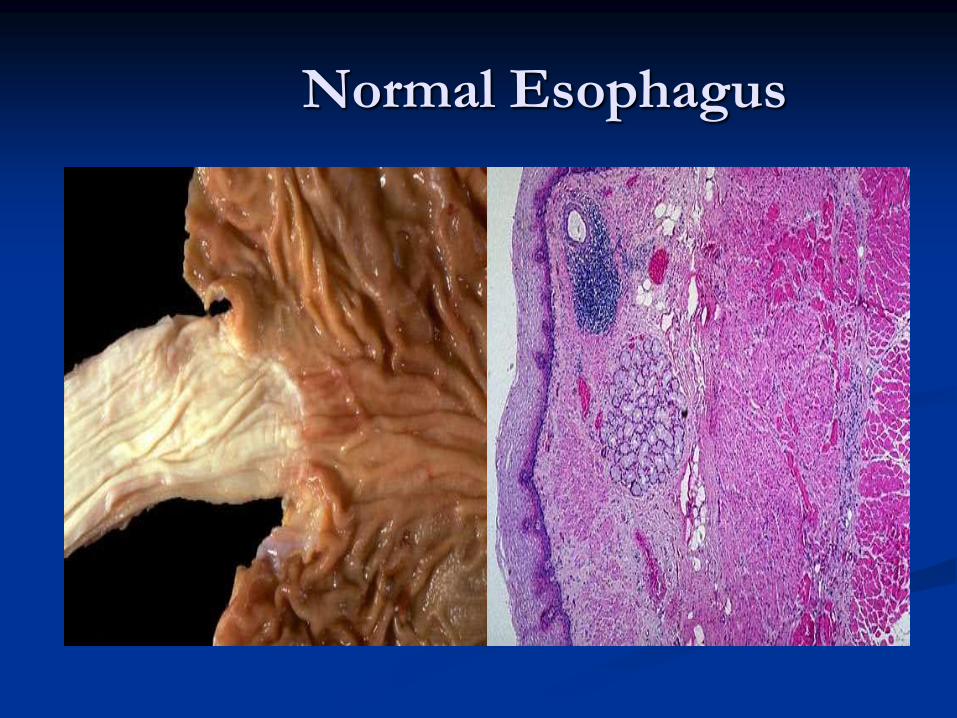
Normal Esophagus

ESOPHAGITIS
CHEMICAL AND INFECTIOUS
REFLUX
EOSINOPHILIC

CHEMICAL AND INFECTIOUS
ESOPHAGITIS
Alcohol, acids, alkalis, excessively hot fluids
Heavy smoking
Pill induced
Chemotherapy, radiotherapy
Graft versus host disease
HSV, CMV, FUNGAL
Desquamative skin diseases

Morphology
Ulceration
Necrosis
Granulation tissue
Fibrosis

Herpetic ulcer

HERPES SIMPLEX
ESOPHAGITIS

CMV

ESOPHAGEAL CANDIDIASIS

CANDIDIASIS

Candidiasis PAS & GMS Stain

Reflux Esophagitis
GERD: gastroesophageal reflux disease
Pathogenesis
Reflux of gastric juice
Reflux of bile may occur
Decreased lower esophageal tone
Increased abdominal pressure

SYMPTOMS
Dysphagia
Heartburn
Regurgitation
Severe chest pain

Morphology
Hyperemia
Eosinophils, Neutrophils
Basal zone hyperplasia

Reflux Esophagitis

Barrett esophagus
Complication of chronic GERD
INTESTINAL METAPLASIA within
squamous mucosa
Increased risk of esophageal carcinoma

Endoscopy
Long segment ( 3 cm or more )
Short segmnt ( less than 3 cm )
Tongues of red velvety mucosa extending upward from GE junction
Morphology
Intestinal metaplasia, goblet cells
Dysplasia, precancerous

Barrett Esophagus

BARRETT ESOPHAGUS

LOW GRADE DYSPLASIA

HIGH GRADE DYSPLASIA
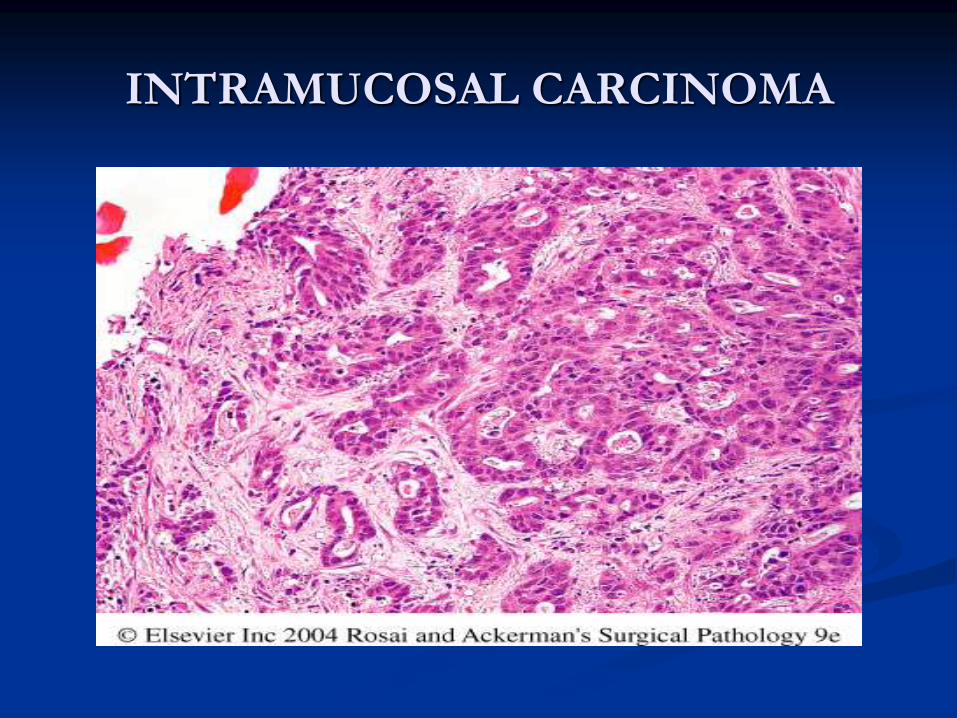
INTRAMUCOSAL CARCINOMA

Adenocarcinoma
Barrett esophagus
Longstanding GERD
Tobacco, obesity, radiation
Decreased fresh fruit and vegetables
Seven times more in males
Dysphagia, weight loss, hematemesis, chest pain,
vomiting



Distal third of esophagus
Flat, raised, 5 cm or more mass
Infiltrative, deep ulcer
Intestinal type carcinoma
Signet ring type

Squamous cell carcinoma
Epidemiology
Most frequent in men , over 45 yrs of age
Male to female ratio is 4:1
Blacks are at higher risk than whites
Relatively common in China, Iran, Southern Brazil and other oriental countries, most common tumor of alimentary tract in African Bantus
In western countries, there has been a recent epidemiologic switch from tobacco and alcohol-related SCC to Barrett’s-related adenocarcinoma.

Associated Factors in Development of SCC of
Esophagus
Betel chewing
Deficiency of vitamins
Deficiency of trace elements
Fungal contamination of foodstuffs
High content of nitrites/nitrosamines
Lifestyle
Burning-hot beverages or food
Alcohol consumption
Tobacco use
Rural environment

Esophageal Disorders
Caustic injury
Achalasia
Plummer-Vinson syndrome
Genetic Predisposition
P53 and p16INK4 mutations

Morphologic features and local spread: Occur in any part of esophagus, most common in middle
50% and lower thirds30%
Grossly
Intraepithelial neoplasia (EIN) or carcinoma-in-situ
Early lesion small grey white plaque like thickenings or elevation of mucosa
Late circumferential tumour mass, often ulcerated with sharply demarcated margins
Three morphologic pattern:
1. Exophytic or polypoid
2. Flat , Diffuse thickening of wall with narrowing of lumen
3. Ulcerated




Morphology
Well differentiated
Moderately differentiated
Poorly differentiated

SQUAMOUS CELL
CARCINOMA
