ersi voskaridou 1, md, phd, evangelos terpos 2, md, phd 1 thalassaemia reference center, laikon...
TRANSCRIPT

Ersi Voskaridou1, MD, PhD, Evangelos Terpos2, MD, PhD
1Thalassaemia Reference Center, Laikon General Hospital2Department of Clinical Therapeutics, University of Athens School of Medicine
Athens, Greece
Bone Disease in haemoglobin disorders

Bone Disease in Patients With Haemoglobinopathies
• Abnormalities in children with undermanaged thalassemia include– Enlarged cranial and facial bones– Spinal deformities– Nerve compression– Spontaneous fractures
• All thalassemia and SCD patients: effects of bone marrow expansion and other imbalances– Localized changes in bone (loss and formation)– Generalized decrease in bone mineral density
(BMD), osteppenia/osteoporosis– Mikroinfarction of vertebral bone marrow (fish
mouth)
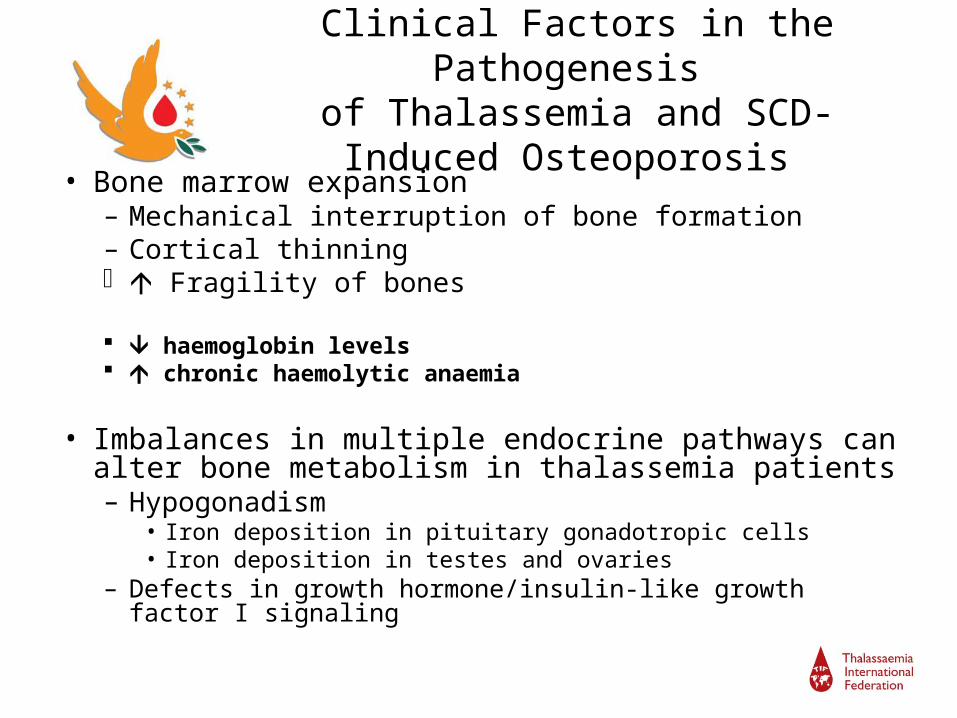
• Bone marrow expansion– Mechanical interruption of bone formation– Cortical thinning Fragility of bones
haemoglobin levels chronic haemolytic anaemia
• Imbalances in multiple endocrine pathways can alter bone metabolism in thalassemia patients– Hypogonadism
• Iron deposition in pituitary gonadotropic cells• Iron deposition in testes and ovaries
– Defects in growth hormone/insulin-like growth factor I signaling
Clinical Factors in the Pathogenesis of Thalassemia and SCD-Induced
Osteoporosis

Acquired Factors in the Pathogenesis of Thalassemia and SCD-Induced
Osteoporosis• Iron overload and chelation therapies
– Iron deposition in bone• Impaired maturation of bone cells (osteoids) Local mineralisation
– High-dose iron chelation therapy with desferoxamine Differentiation and proliferation of bone-forming cells (osteoblasts) Collagen (bone matrix) formation Osteoblast programmed cell death (apoptosis)
• Deficiencies in vitamins and minerals– Vitamin D deficiency
• Impaired regulation of bone metabolism
– Zinc deficiency• Prevalent in hemoglobinopathies and associated with low bone mineral
density• Role of zinc is not well defined, but might involve activation of bone-specific
alkaline phosphatase (bALP) and inhibition of osteoclast activity1,2
1. King JC. Am J Clin Nutr. 1996;64(3):375-376; 2. Reviewed in Voskaridou E, et al. Br J Haematol. 2004;127(2):2004; 127-139.

Genetic predisposition to reduced BMD
• Polymorphisms in genes that play key roles in bone maintenance and remodeling:
- Collagen type I
- Vitamin D receptor
- Transforming growth factor β 1
- Calcitonin receptor
- Oestrogen receptor
- Interleukin 6
• To date, although some genetic traits correlate with thalassaemia-induced osteoporosis, their roles in its development are unclear
Reviewed in Voskaridou E, et al. Br J Haematol. 2004;127(2):127-139.

Haemoglobinopathies-Induced osteoporosis
• Most of these factors act through the imbalance in bone remodelling; they inhibit osteoblast activation and/or increase osteoclast function leading to bone loss and osteoporosis.
• The necessity of understanding the underlying mechanisms for bone destruction in these patients seems to be compulsory
Determination of optimal therapy
•
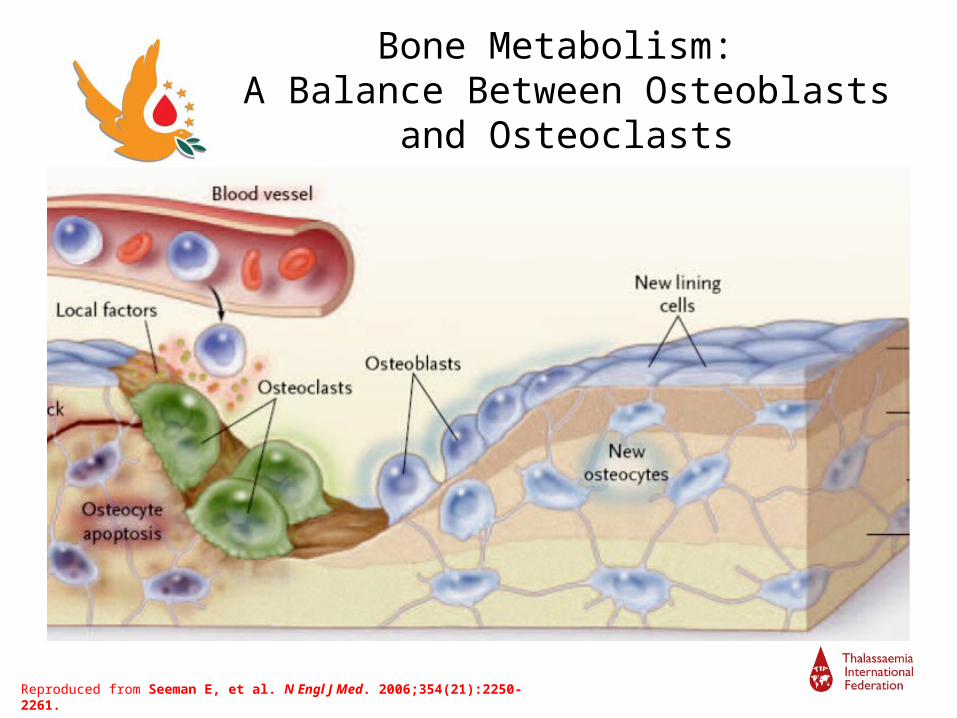
Bone Metabolism: A Balance Between Osteoblasts and
Osteoclasts
Reproduced from Seeman E, et al. N Engl J Med. 2006;354(21):2250-2261.

Results From an Imbalancein Bone Remodeling
• Decreased bone mineral density (BMD)
• Micro-architectural deterioration
• Decreased bone strength
• Increased fracture risk
Eastell R. N Engl J Med. 1998;736-46.Boyle JB, et al. Nature. 2003;423:337-42.Photos reproduced from Dempster DW, et al. J Bone Miner Res. 1986;1:15-21 with permission ofthe American Society for Bone and Mineral Research.
Osteoporotic Bone
Normal Bone

Osteoporosis
• Osteoporosis is a disease characterized by low bone mass and microarchitectural deterioration of bone issue, leading to enhanced bone fragility and a consequential increase in fracture risk
• Osteoporosis is the silent disease that makes
bones prone to fracture and is a major public health

Osteoporosis
Osteoporosis is defined as BMD T-score < – 2.5 leading to higher risk of fracture
Osteopenia: T-score –1.0 to –2.5
Normal BMD: T-score > –1.0
BMD = Bone mineral density.
•Consensus Development Conference. Am J Med. 1993;94(6):646-650.•National Osteoporosis Foundation. 2008.
Definition• T-score
– Number of standard deviations (SD) that a patient’s bone mass is above or below the mean peak bone mass for a 30-year-old healthy woman
• T-score –1 to +1 = normal BMD
– 1 SD decrease in T-score = 10% to 15% decrease in BMD
• Z-score– Number of SDs that a
patient’s bone mass is above or below the mean bone mass for age- and sex-matched controls
BMD = BMD = Bone mineral density.
•Consensus Development Conference. Am J Med. 1993;94(6):646-650.•National Osteoporosis Foundation. 2008.

Dual-Energy X-ray Absorptiometry (DEXA)
for Determination of BMD
BMD = Bone mineral density.
Typical DEXA equipment1
Sample DEXA scans of lumbar spine (top) and hip (bottom)2

Relationship Between BMD and Fracture Risk
BMD = Bone mineral density.
Adapted from Faulkner KG. J Bone Miner Res. 2000;15(2):183-187.
Osteoporosis
Osteopenia
Normal
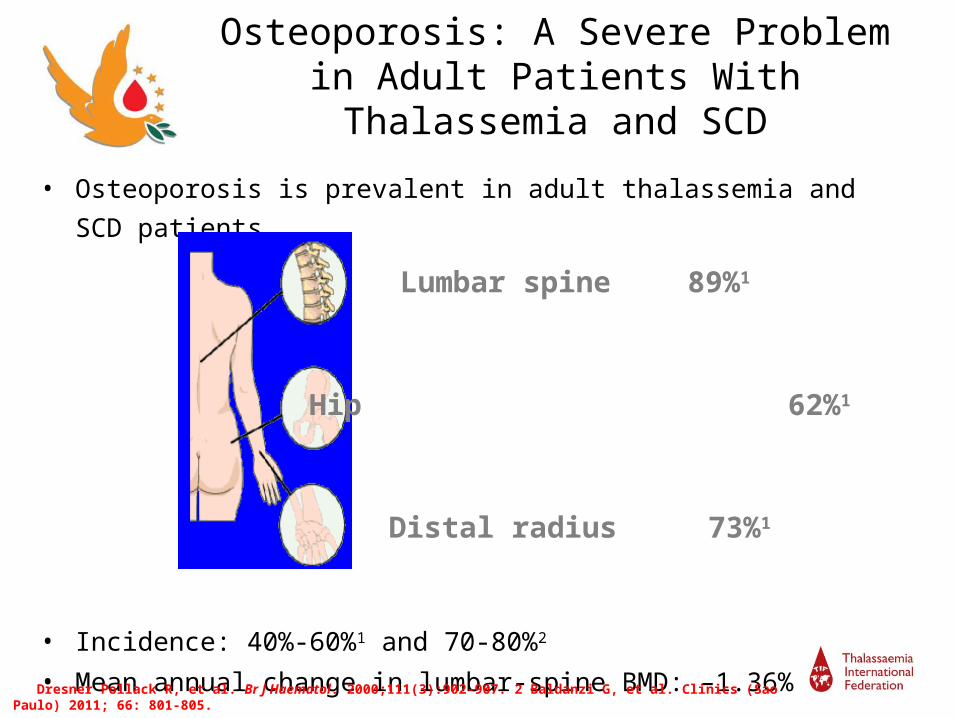
Osteoporosis: A Severe Problemin Adult Patients With Thalassemia and
SCD
• Osteoporosis is prevalent in adult thalassemia and SCD patients
• Incidence: 40%-60%1 and 70-80%2
• Mean annual change in lumbar-spine BMD: –1.36%1
1. Dresner Pollack R, et al. Br J Haematol. 2000;111(3):902-907. 2 Baldanzi G, et al. Clinics (Sao Paulo) 2011; 66: 801-805.
Lumbar spine 89%1
Hip 62%1
Distal radius 73%1

Biochemical Markers of Bone Metabolism
• Enzymes, protein fragments, or other molecules released into blood as a result of bone turnover
• In order to be clinically useful, markers should be– Highly specific to bone– Detectable in body fluids (blood or urine) using
standard assay methods (chemical, enzymatic or immunologic)
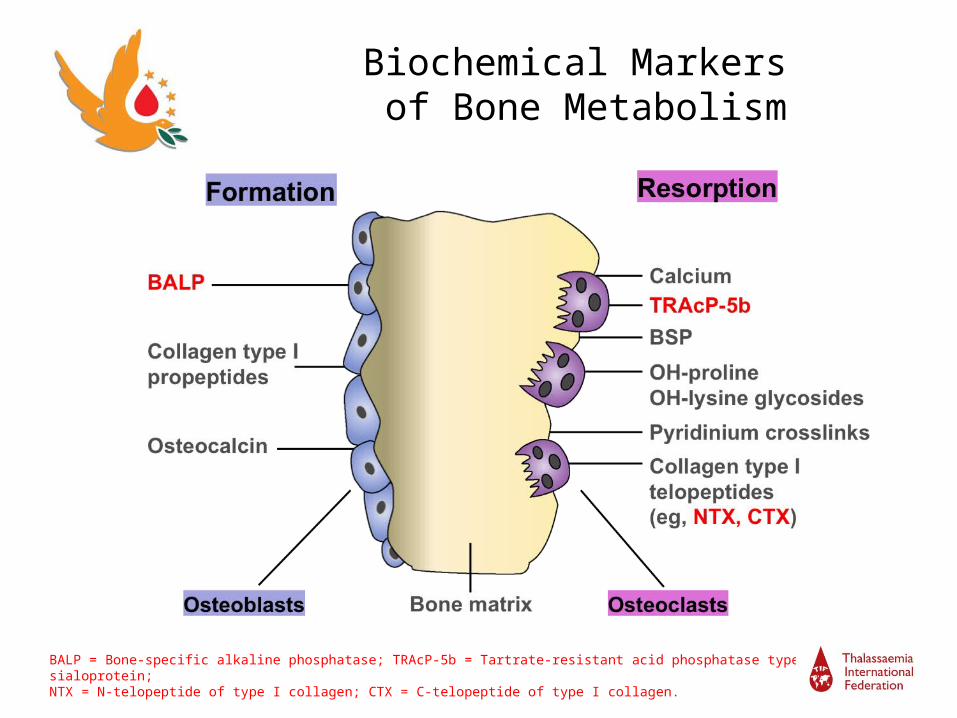
Biochemical Markers of Bone Metabolism
BALP = Bone-specific alkaline phosphatase; TRAcP-5b = Tartrate-resistant acid phosphatase type 5b; BSP = Bone sialoprotein; NTX = N-telopeptide of type I collagen; CTX = C-telopeptide of type I collagen. Adapted by permission from Fohr B, et al. J Clin Endocrinol Metab. 2003;88(11):5059-5075.

Bone Metabolism Unit
Voskaridou & Terpos. BJH 2004;127:127-39

RANKL: An Essential Mediator of Osteoclasts
BoneOsteoblast
lineage
Matureosteoclast
CFU-M
Prefusion osteoclast
Multinucleatedosteoclast
Growth factors HormonesCytokines
RANKRANKL
RARANK = Receptor activator of nuclear factor kappa B; RANKL = RANK ligand; CFU-M = Colony-forming unit macrophage.
Adapted by permission of Macmillan Publishers Ltd [NATURE] Boyle WJ, et al. Nature. 2003;423(6937):337-342.
RANK
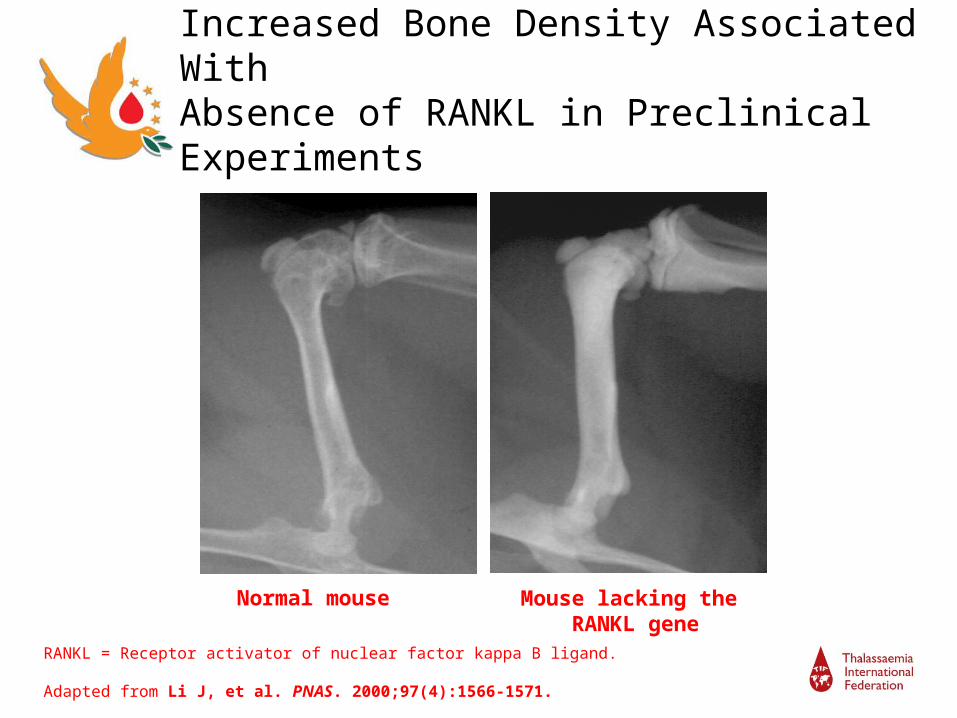
Increased Bone Density Associated With Absence of RANKL in Preclinical Experiments
Normal mouse
Normal mouse Mouse lacking the RANKL gene
RANKL = Receptor activator of nuclear factor kappa B ligand.
Adapted from Li J, et al. PNAS. 2000;97(4):1566-1571.

Osteoprotegerin (OPG): The Decoy Receptor of RANKL
Osteoclast formation, function, and survival inhibited by OPG
BoneOsteoblast
lineage
Inactiveosteoclast
CFU-M
Prefusion osteoclast
Multinucleatedosteoclast
Growth factors HormonesCytokines
RANKRANKL
OPG
OPG = Osteoprotegerin; RANK = Receptor activator of nuclear factor kappa B; RANKL = RANK ligand; CFU-M = Colony-forming unit macrophage.
Adapted by permission of Macmillan Publishers Ltd [NATURE] Boyle WJ, et al. Nature. 2003;423(6937):337-342.
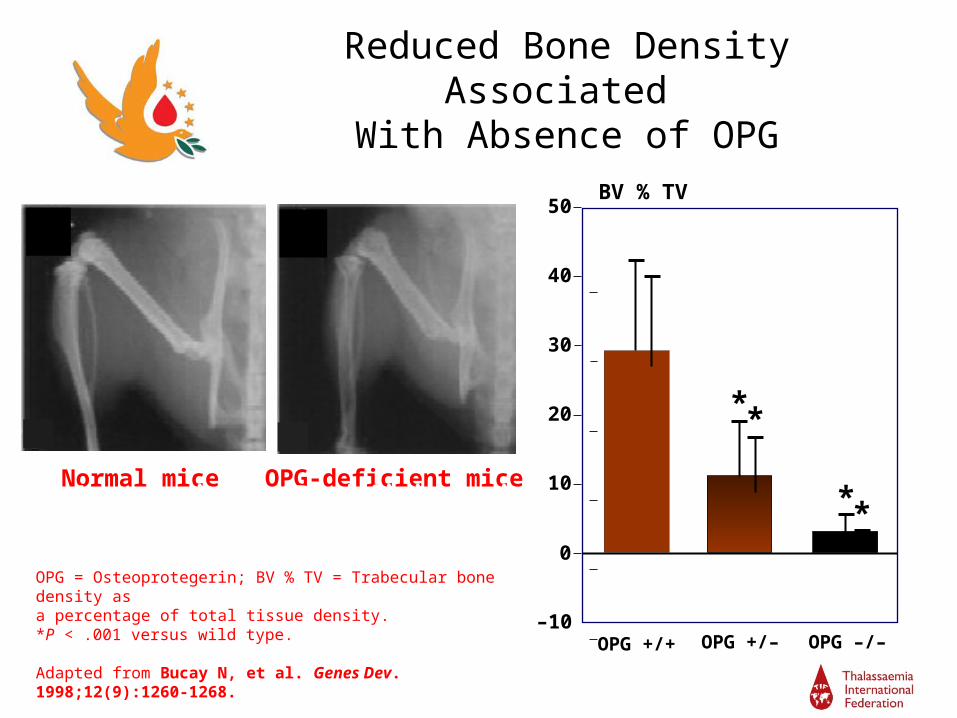
Reduced Bone Density Associated With Absence of OPG
*
OPG +/+ OPG +/– OPG –/–
40
Normal mice OPG-deficient mice
+/+ –/–
–10
0
10
20
30
50
*
*
BV % TV
Normal mice OPG-deficient mice*
OPG = Osteoprotegerin; BV % TV = Trabecular bone density as a percentage of total tissue density.*P < .001 versus wild type.
Adapted from Bucay N, et al. Genes Dev. 1998;12(9):1260-1268.

RANKL/OPG Balance Drives Osteoclast Activity
Alterations of the RANKL / OPG ratio are critical in the pathogenesis of bone diseases that result in increased bone resorption1-3
RANKL
OPG
PreventsOC activaion
PromotesOC activation
OC Activity
RANKL = Receptor activator of nuclear factor kappa B ligand; OPG = Osteoprotegerin; OC = Osteoclast.1. Hofbauer LC, et al. JAMA. 2004;292(4):490-495; 2. Lacey DL, et al. Cell. 1998;93(2):165-176; 3. Boyle WJ, et al. Nature. 2003;423(6937):337-342.

OPG/sRANKL ratio in thalassaemiaOPG/sRANKL ratio in thalassaemia
2630N =
Thalassaemia patientsControls
Log
sRA
NK
L/O
PG
Log
sRA
NK
L/O
PG
2.0
1.5
1.0
.5
0.0
-.5
-1.0
-1.5
p<0.01p<0.01
Voskaridou et al. Br J Haematol 2003;123:730-7Morabito et al. J Bone Miner Res 2004;19:722-7
Parameter Patients(N=26)(m±SD)
Controls(N=30)
(μέση±SD)
p-value
OPG (pmol/L)
sRANKL (pmol/L)
OPG/sRANKL
2,6±1,6
5,6±3,8
0,4±0,4
4,0±0,4
4,6±1,4
0,8±0,2
0,002
0,09
0,006
Parameter Patients(N=54)(m±SD)
Controls(M±SD)
p-value
OPG (pmol/L)
sRANKL (pmol/L)
OPG/sRANKL
3,0±1,3
8,1±2,8
0,4±0,2
3,6±1,4
4,5±1,2
0,8±0,2
NS
<0,0001
<0,0001
L1-L4 and femoral neck BMD strongly correlated with OPG/sRANKL

Markers of Bone Remodeling in SCD patients
Nouraie M, et al. Haematologica. 2011; 96(8):1092-8

HbS/b-thalassemia induced osteoporosis
Ersi Voskaridou et al. Haematologica 2006; 91:813-816

Hu et al. Development 2005;132:49
A model that intergrates Hh and Wint signaling in osteoblast development

Marie PJ. Arch Biochem Biophys. 2008;473(2):98-105.
Regulation of Osteoblast FunctionProliferation and Differentiation
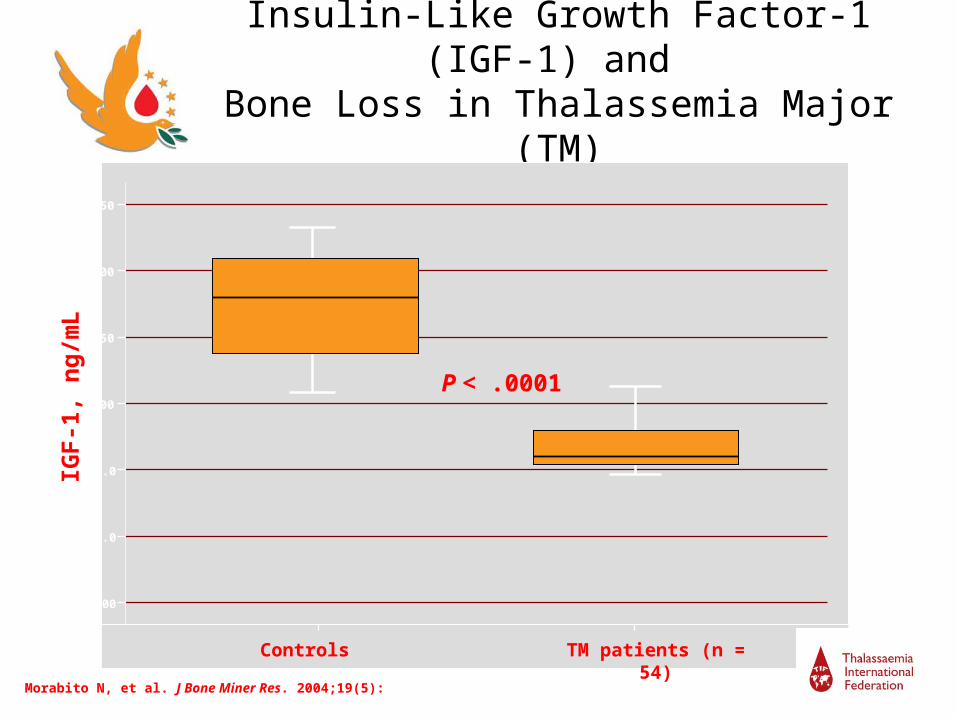
Insulin-Like Growth Factor-1 (IGF-1) and Bone Loss in Thalassemia Major (TM)
Controls TM patients (n = 54)
IGF
-1,
ng
/mL
250
200
150
100
50.0
25.0
0.00
P < .0001
Morabito N, et al. J Bone Miner Res. 2004;19(5):722-727.

Dickkopf-1 and Bone Metabolism
Dkk-1 = Dickkopf-1 (protein).
Adapted from MacDonald B, et al, Bone 2007;41(3):331-339. © 2007, with permission from Elsevier.
Reduced Dkk-1 levels correlate with high bone mass:
d/– versus +/+ mice:75% in Dkk-1 expressionand18 to 25% in cortical thickness at the femur diaphysis; P < .01

Dkk-1: Dramatic Increase in Thalassemia Patients With Osteoporosis
Dkk-1: Dickkopf-1 (protein).
Voskaridou E, et al. Haematologica 2009;94(5):725-728.

Correlation Between Baseline Dkk-1 and Bone Turnover
Dkk-1: Dickkopf-1 (protein); TRAcP-5b = Tartrate-resistant acid phosphatase type-5b; BALP = Bone-specific alkaline phosphatase.
Voskaridou E, et al. Haematologica 2009;94(5):725-728.

Correlations Between Baseline Dkk-1 and BMD
L1-L4 BMD
Dkk
-1,
ng
/mL
1.11.00.90.80.70.60.5
60
40
20
0r = –0.290, P = .022
Wrist BMD
Dkk
-1,
ng
/mL
1.21.00.80.60.40.2
60
40
20
0
r = –0.415, P = .001
Dkk-1: Dickkopf-1 (protein); BMD = Bone mineral density.
Voskaridou E, et al. Haematologica 2009;94(5):725-728.

Treatment Options for Thalassemia-Induced Osteoporosis
• Prevention and general principles
• Hormonal replacement
• Calcitonin
• Bisphosphonates
• Denosumab (?)
Prevention and Treatment of Early Bone LossConsists the Best Policy
• Annual checking of BMD starting in adolescence is considered
indispensable
• Physical activity must always be encouraged
• Smoking should be discouraged
• Adequate calcium and zinc intake during skeleton development
can increase bone mass in adult life
• Low doses of vitamin D
• Early diagnosis and treatment of diabetes mellitus
• Adequate iron chelation may prevent iron toxicity in the bone
and sufficient blood transfusions may inhibit uncontrolled bone
marrow expansion

Hormonal replacement
Prevention of hypogonadism seems to be the most effective way for preventing osteoporosis and other bone deformities in TM patients
Therapeutic agent Dosage No of patient
s
Authors
Males: long-acting testosterone esterase
Females: equine oestrogen + metroxyprogesterone
for 16-32 months250mg, im, every
4weeks
0.625mg/d
5mg/d for 10 days monthly
67 Anapliotou et al, 1995
(Clin Endocrinol 42:279-87)

Hormonal replacement
Hormonal replacement do not seem to be the most effective treatment for preventing osteoporosis in TM patients and it is
not the only cause of bone disease
in β-TM
TM patients with hypogonadism and osteoporosis HRT POF patients HRT
Both groups had significant improvement but the POF group had normalization of spinal T scores following HRT in contrast to the β-TM patients
Chatterjee R, et al, Hemoglobin 2011;35(5-6):653-8.

Bisphosphonates Evaluated in Thalassemia-Induced Osteoporosis
The increased bone resorption observed in patients with thalassaemia-induced osteoporosis has led to the use of bisphosphonates (inhibitors of osteoclastic bone resorption) for the management of bone loss in these patients

Bisphosphonates Evaluated in Thalassemia-Induced Osteoporosis
• Alendronate (first generation)
• Clodronate (first generation)
• Pamidronate (second generation)
• Zoledronic acid (third generation)
• Neridronate (third generation)

First-Generation Bisphosphonates for Treatment of Thalassemia-Induced Osteoporosis
• N = 25 patients with thalassemia major and osteoporosis
• Bisphosphonate treatment for 2 years1
– Alendronate (10 mg PO qd) – Clodronate (100 mg IM qd for 10d/month)
• At 2 years– BMD at all measured sites in placebo arm– BMD constant in clodronate arm– BMD in alendronate arm
• Lack of efficacy of clodronate confirmed in a second study2
PO = Oral; IM = Intramuscular; BMD = Bone mineral density.
1. Morabito N, et al. Osteoporosis Int. 2002;13(8):644-649; 2. Pennisi P, et al. J Bone Miner Metab. 2003;21(6):402-408.
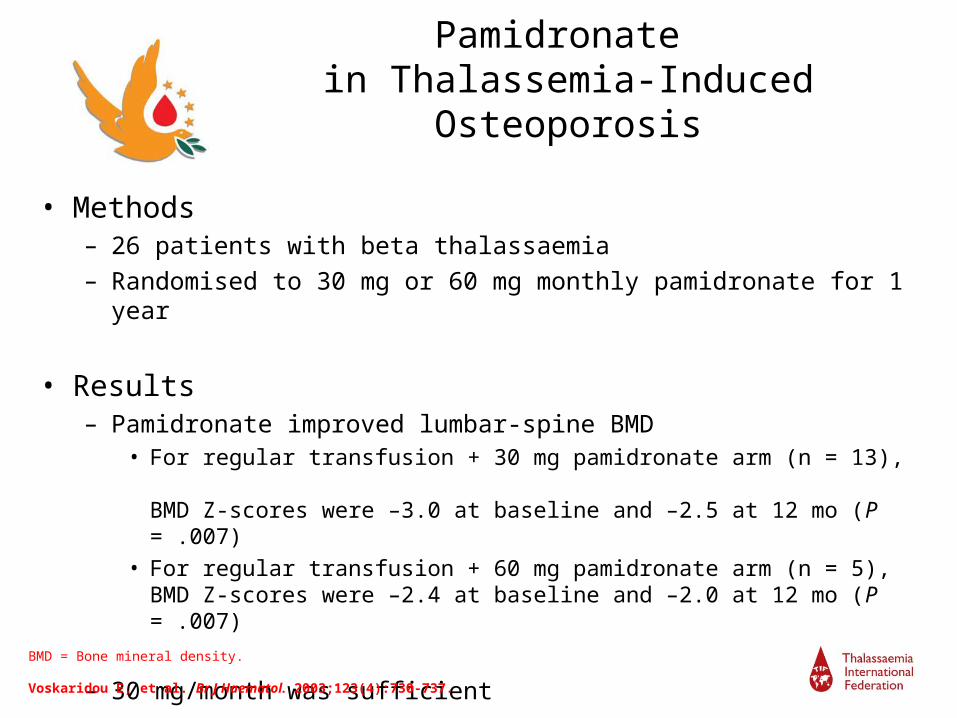
Pamidronate in Thalassemia-Induced Osteoporosis
• Methods– 26 patients with beta thalassaemia – Randomised to 30 mg or 60 mg monthly pamidronate for 1 year
• Results– Pamidronate improved lumbar-spine BMD
• For regular transfusion + 30 mg pamidronate arm (n = 13), BMD Z-scores were –3.0 at baseline and –2.5 at 12 mo (P = .007)
• For regular transfusion + 60 mg pamidronate arm (n = 5), BMD Z-scores were –2.4 at baseline and –2.0 at 12 mo (P = .007)
– 30 mg/month was sufficientBMD = Bone mineral density.
Voskaridou E, et al. Br J Haematol. 2003;123(4):730-737.

Pamidronate in Thalassemia-Induced Osteoporosis
• Pamidronate every month IV (1 mg/kg body weight) for 3 years.• Non randomised: 1. N=12 adult TM and 5 TI received Pamidronate +HRT
2. N=17 pts received only HRT
• Methods - DEXA
- Markers of bone turnover (PICP and ICTP)
- Histomorphometric measurements (trabecular bone volume, osteoid
volume, osteoid surface (formation indices) and resorption surface
(bone resorption)
• Results– Pamidronate improved BMD of lumbar spine and total hip plasma PICP and plasma ICTP levels – bone formation and resorption in TM bone formation and resorption in TI BMD = Bone mineral density.Ratna Chatterjee et al. BJH 2012

Pamidronate in Thalassemia-Induced Osteoporosis
Ratna Chatterjee et al. BJH 2012

Pamidronate in Thalassemia-Induced Osteoporosis
Histomorphometry
Ratna Chatterjee et al. BJH 2012

Long-term Follow-up of ZOL-Treated Patients
ZOL = Zoledronic acid.
Voskaridou E, et al. Haematologica. 2008;93(10):1588-1590.
Baseline
36 months
Patients(N = 66)
Group A (n = 23)ZOL q 6 mo for 12 mo
Group B (n = 21)ZOL q 3 mo for 12 mo
Group C (n = 22)Placebo for 12 mo
Follow-up Follow-upZOL 4 mg q 3 mo
Treat 12 mo
Follow-up 12 moFollow-up 24 mo Follow-up 24 mo
2
0
–2
–4
–6
L1-L4 1
2 mo
L1-L4 3
6 mo
Femoral
neck B
aseli
ne
Femoral
neck 1
2 mo
Femoral
neck 3
6 mo
C
P < .01
P = .01

ZOL Decreases Bone Turnover Marker Levels in Patients With Thalassaemia
ControlZOL 4 mg q3m
ZOL = Zoledronic acid; CTX = C-telopeptide of type I collagen; TRAcP-5b = Tartrate-resistant acid phosphatase type 5b; BALP = Bone-specific alkaline phosphatase.
Voskaridou E, et al. Haematologica. 2006;91(9):1193-1202.
0
0.2
0.4
0.6
0.8
1
0 6 12
Time, months
Med
ian
CT
X, n
g/m
L
0
0.5
1
1.5
2
2.5
3
0 6 12
Time, months
TR
AcP
-5b
, U/L
Bone resorption
Pain Score
Voskaridou E, et al. Haematologica. 2006;91(9):1193-1202.

Safety of ZOL in Patients With Thalassemia-Induced Osteoporosis
• ZOL (4 mg q 3 or 6 mo) was generally well tolerated• No alteration in serum hemoglobin or ferritin levels• Adverse events
– Diffuse bone pain (in 9% of patients)– Fever (in 20% of patients)
• Noted after first dose of ZOL• Duration < 24 hours• Symptoms relieved by antipyretics (paracetamol/acetaminophen)
– No bone pain or fever after subsequent infusions of ZOL• No cases of
– Renal abnormalities– Hypocalcemia– Osteonecrosis of the jaw (ONJ)
ZOL = zoledronic acid.
Voskaridou E, et al. Haematologica. 2006;91(9):1193-1202.

Neridronate a third generation bisphosphonate
Forni GL et al. Br J Haematol. 2012;158(2):274-82
Randomized: a. 54 pts with neridronate (100mg X 3m), calcium, and vitanin D x 3 ys b. 64 pts with calcium and vitamin D x 3 ys

Reduction of Dkk-1 in ZOL Groups
ZOL = Zoledronic acid; Dkk-1 = Dickkopf-1 (protein)
Voskaridou E, et al. Haematologica 2009;94(5):725-728.
Group C (Placebo)Groups A + B (ZOL)
Dkk
-1, n
g/m
L
80
60
40
20
0
P = .004 P = .08B
asel
ine
12-m
o Z
OL
Bas
elin
e
12-m
o p
lace
bo

p<0.001 p<0.001
Sclerostin is a Wnt signaling inhibitorSclerostin in TM vs. Controls
Voskaridou E et al. Sclerostin in Thalassemia Osteoporosis Horm Metab Res 2012; 44: 1–5
Sclerostin (pg/ml)
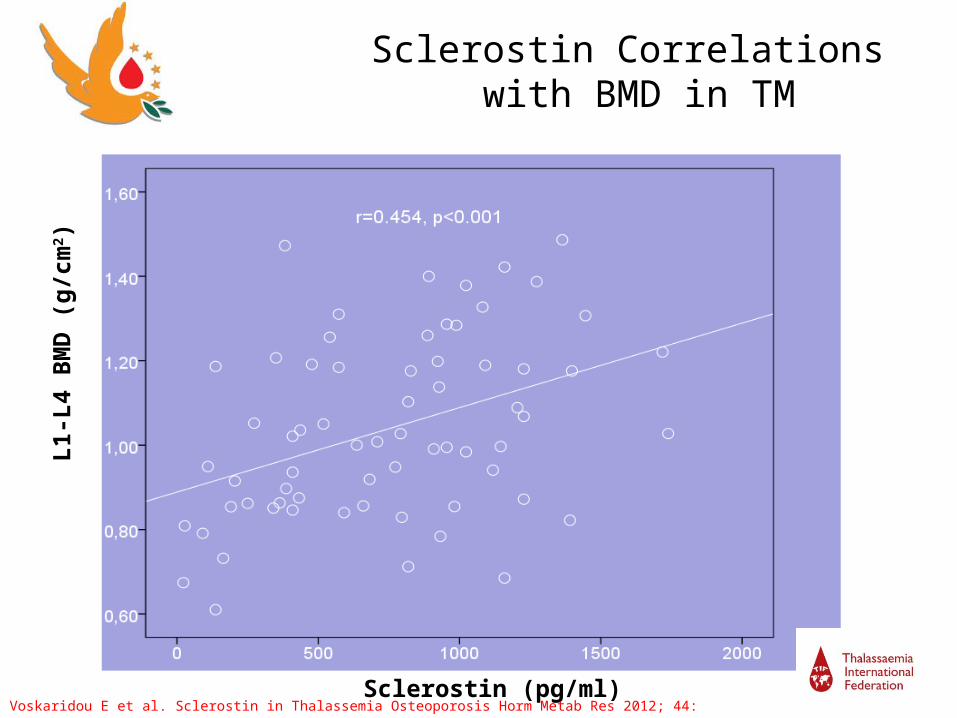
Sclerostin Correlations with BMD in TM
L1-
L4
BM
D (
g/c
m2 )
Voskaridou E et al. Sclerostin in Thalassemia Osteoporosis Horm Metab Res 2012; 44: 1–5

Novel drugs?
• These findings give the rationale for the use of novel drugs targeting sclerostin and Dkk-1 in patients with thalassemia-induced osteoporosis

Conclusions and Future Perspectives I
• Thalassemia-induced osteoporosis is multifactorial and, therefore, very difficult to manage
• Monitoring BMD with DXA is especially important in adolescents and adults patients with hemoglobinopathies
• Preventive measures are essential
• Bisphosphonates effectively restores BMD and reduces pain in hemoglobinopathies patients with osteoporosis– Generally well tolerated– Benefits continue for ≥ 2 years after cessation of ZOL or NER
• Outstanding questions regarding the use of bisphosphonates in this setting include– Most suitable agent– Optimal dose, frequency, and duration of therapy– Combination therapies using bisphosphonates and other agents

Conclusions and Future Perspectives II
• New data suggest that the reduced osteoblastic activity, which is believed to be the basic mechanism of bone loss in thalassemia, is accompanied by a comparable or even greater increase in bone resorption through the RANK/RANKL/OPG pathway
• Wingless-type (Wnt) signaling is an important pathway for osteoblast differentiation
• The high circulating sclerostin & Dkk-1 levels and their association with BMD support the notion of a disrupted Wnt signaling in patients with thalassemia and osteoporosis which leads to osteoblast deregulation
Use of novel antiresorptive agents (denosumab/anti-RANKL) or novel drugs targeting sclerostin and Dkk-1, may
be effective in patients with hemoglobinopathies

Thanksall of you