epothilones in breast cancer sandra m. swain, md december 7, 2005
TRANSCRIPT

Epothilones in Breast Cancer
Sandra M. Swain, MD
December 7, 2005

Sandra Swain, MD
No financial relationships with any commercial interest

• Microtubule-stabilizing agents• Epothilones• Ixabepilone (BMS-247550) trial at NCI
– Clinical outcome– Evaluation of neurotoxicity– Translational study
• Other ixabepilone trials in breast cancer
Recent Advances in the Development of Microtubule-Stabilizing Agents

Sorangium cellulosum
• Myxobacteria– Secondary metabolites
(epothilones/fungicides)
Zambezi river

Epothilones Bind Specifically and Uniquely to Beta-Tubulin
• Thiazole side-chain occupies the region of binding site not occupied by taxanes
• Only 1 polar contact point (C7-OH) is shared with taxanes
EpoA and paclitaxel bound to beta-tubulin
Paclitaxel Epothilone A
Nettles. Science. 2004;305:866-869.

Epothilones Are Strong Promoters of Tubulin Polymerization
• Epothilone B has tubulin polymerizing activity 2-10 times stronger than paclitaxel
Kowalski. J Biol Chem. 1997;272:2534.
1, Paclitaxel; 2, EpoA; 3, EpoB

Epothilones Are Less Susceptible to MDR Than
Paclitaxel• Poor substrates
for MDR proteins
• MDR expression not altered in epothilone- resistant cell lines
Modified from Data on file, Bristol- Myers Squibb Company.
PAT-7MDR/MRP
(Ovarian Ca)
Lo
g c
ell
kill
at
MT
D
1.3
4.5
HCT/VM46MDR
(Colon Ca)
0.4
3.1
0
1
2
3
4
5
6 Paclitaxel
Ixabepilone (epothilone B analog)

Potential Advantages of Epothilones
• Bind specifically and uniquely to beta-tubulin • Epothilone B has 2- to 10-fold greater
polymerizing activity than paclitaxel• No steroid premedication needed• Less susceptible to multidrug resistance
(MDR)– Poor substrates for MDR proteins– MDR expression not altered in epothilone-
resistant cell lines

Epothilones
IISchering AGEpothilone BZK-EPO
IBristol-Myers
SquibbEpothilone BBMS-310705
IIINovartisEpothilone BPatupilone
IIKosan/RocheEpothilone DKOS-862
IIIBristol-Myers
SquibbEpothilone BIxabepilone
PHASEDEVELOPERDerivativeNAME

Ixabepilone (BMS-247550)
• Epothilone B is a natural macrolide produced by the myxobacterium Sorangium cellulosum
• Ixabepilone is a semisynthetic analog of epothilone B (aza-epothilone B)
Epothilone B Ixabepilone

Antitumor Activity in Taxane-Resistant PAT-21 Breast Cancer
Xenografts
PAT-21 breast cancer xenografts are derived from a patient with MBC who received 10 cycles of CMF, then 4 cycles of paclitaxel. MTD=maximum tolerated dose.
Me
dia
n t
um
or
wt.
(m
g)
10
100
1000
40 70 100 130 160Days posttumor implantation
ControlIxabepilone (10 mg/kg, MTD)Paclitaxel (36 mg/kg, MTD)
ControlIxabepilone (13 mg/kg, MTD)Docetaxel (20 mg/kg, MTD)Vinorelbine (9 mg/kg, MTD)
Days posttumor implantation
10
100
1000
40 50 60 70 80 90
Me
dia
n t
um
or
wt.
(m
g)
Data on file, Bristol-Myers Squibb Company.

Ixabepilone Pharmacology
Daily x 5 q21d
Daily x 3 q21d
WeeklyOnce q21d
Infusion duration, hr
1 1 0.5-1 1
Dose (mg/m2), range
1.5-8 8-10 1-30 32-65
MTD (mg/m2)
6 8 25 50
DLT Neutropenia, neuropathy
Goodin. J Clin Oncol. 2004;22:2015-2025.
MTD=maximum tolerated dose; DLT=dose-limiting toxicity; q=every.

Abraham. J Clin Oncol. 2003;21:1866-1873; Mani. Clin Cancer Res. 2004;10:1289-1298; Zhuang. Cancer. 2005;103:1932-1938.
Phase I Trials of Ixabepilone
• Ixabepilone IV over 1 hr, 5 days every 21 days (N=27)– Objective responses in patients with cervical, breast, and
basal cell cancer
• Ixabepilone IV over 1 hr, 1 day every 21 days (N=25)– Objective PRs in paclitaxel-refractory ovarian cancer (N=2)
and breast cancer (1 taxane-naїve, 1 taxane-refractory)
• Ixabepilone IV over 1 hr, 3 days every 21 days (N=26)– DLT: neutropenia– Prolonged SD in patients with mesothelioma, ovarian cancer,
and renal cell carcinoma

Ixabepilone in Metastatic and Locally Advanced Breast Cancer Phase II Trial NCI-0229
6 mg/m2/day
Post-treatment biopsy
Baseline biopsy
Cycle 1 (3 weeks) Cycle 2 Cycle 3…
Daily x 5Daily x 5 Daily x 5
Taxane Naïve and Prior Taxane Treated Group

Clinical Response to Ixabepilone NCI-0229
Prior Taxane
Total 37
Complete Response 1 (3%)
Partial Response 7 (19%)
Stable Disease 13 (38%)
Progressive Disease
16 (43%)
Low. J Clin Oncol. 2005;23:2726-34.

Case StudyComplete Response
Baseline After 11 Cycles

Ixabepilone Phase II Trial NCI-0229: Grade 3/4 Toxicities
Toxicity, %Prior Taxanes(N=37)
Neutropenia, 16
Thrombocytopenia 8
Myalgia 3
Febrile neutropenia 14
Diarrhea 11
Fatigue 13
Low. J Clin Oncol. 2005;23:2726-34.

Incidence of Peripheral Neuropathy During Ixabepilone Treatment: NCI 0229
CTC Toxicity Grade
0 1 2 3 4
Prior Taxane (N=37)
46 % 29 % 22% 3% –
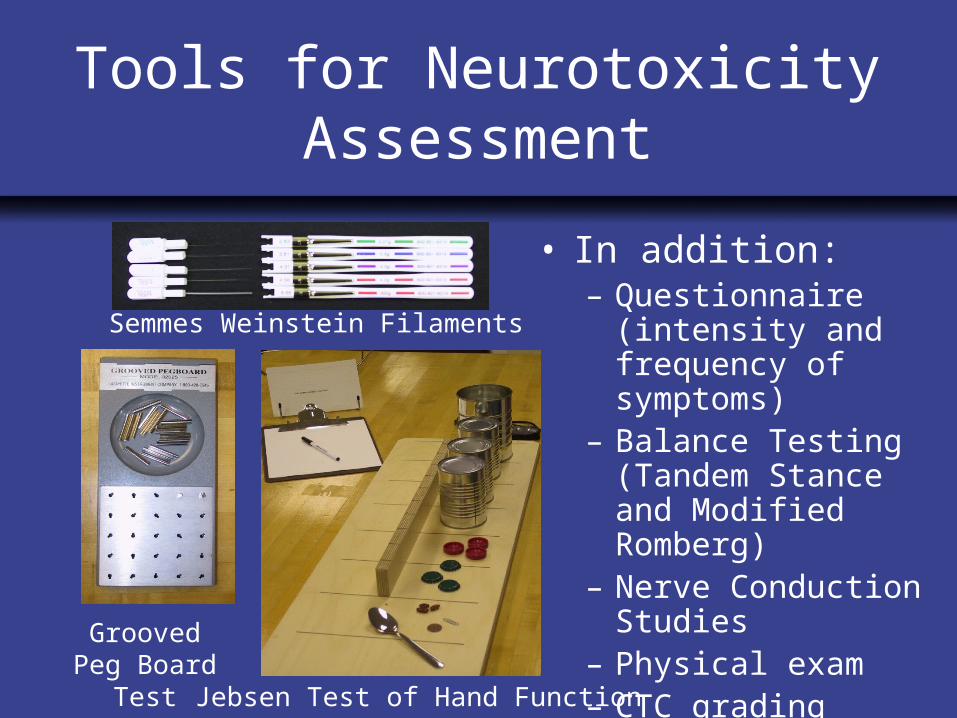
Tools for Neurotoxicity Assessment
Semmes Weinstein Filaments
Grooved Peg Board Test
Jebsen Test of Hand Function
• In addition:– Questionnaire
(intensity and frequency of symptoms)
– Balance Testing (Tandem Stance and Modified Romberg)
– Nerve Conduction Studies
– Physical exam – CTC grading

Matched Pair Study
• Each patient who developed grade 2+ neuropathy was matched to a patient who did not
• Patients matched by age, cumulative dose of taxane therapy, length of time on study, number of prior regimens
Test Baseline Onset of Grade 2
Difference Between Baseline and Onset
Grooved peg board (dominant hand) 8* 25** 11
Jebsen Test of Hand Function (non-dominant hand)
1.7 6.1 7.9**
Median Difference Between Matched Subjects
*P < 0.05; **P < 0.01

Exploratory Univariate Analysis
• Hypothesis: Test scores above a certain cutpoint would indicate high likelihood of developing neuropathy
Example: Baseline score for Jebsen Test of Hand Function using non-dominant hand
For scores greater than 55, median time for neuropathy was 4 months from cycle 3

Functional Tests May Predict Development of Neuropathy
• Low incidence of neuropathy with ixabepilone on daily x 5 schedule– Grade 2: 24%– Grade 3: 5%– Grade 4-5: 0%
• Grooved Peg Board Test and Jebsen Test of Hand Function most often correlated and predicted ixabepilone-induced grade 2-3 neuropathy

Summary: NCI-0229
• Good clinical activity in heavily pretreated breast cancer patients (RR=22%) and taxane naïve patients (RR=43%)
• Grade 3/4 sensory peripheral neuropathy in 3% of patients
• Baseline neurologic functional tests may predict grade ≥ 2 peripheral neuropathy

NCI-0229*
(N=37)
CA-163010†
(N=61)
CA-163009‡
(N=49)CR 1 (3%) - -
PR 7 (19%) 27 (44%) 6 (12%)
SD 13 (35%) 21 (34%) 19 (39%)
PD 16 (43%) 12 (20%) 23 (47%)
Ixabepilone Phase II Clinical Trials in Metastatic Breast Cancer
*Taxane-pretreated.†Anthracycline-pretreated; Ixabepilone 40 mg/m2 q3wk; Roche et al. ASCO 2003;22:18. Abstract 69.
‡Taxane-refractory; Ixabepilone 40 mg/m2 q3wk; Thomas et al. ASCO. 2003;22:8. Abstract 30.

Incidence of Peripheral Neuropathy With Ixabepilone
Phase II Trial ScheduleCTC Toxicity Grade %
0 1 2 3 4
NCI-0229 (N=56)
6 mg/m2 over 1 hr qd (x5) q3wk
48 28 20 4 0
CA 163010 (N=65)
40 mg/m2 over 3 hr q3wk
N/A N/A N/A 22 0
CA 163009(N=49)
40 mg/m2 over 3 hr Q3wk
N/A N/A 33 12 0
Eng et al.(N=25)
40 mg/m2 over 3 hr q3wk
48 28 4 20 0

Incidence of Sensory Neuropathy With Microtubule-Stabilizing Agents
Agents ScheduleDose
(mg/m2)Incidence of Gr ≥ 3
Sensory PN (%)
Paclitaxel 1 wk 80-100 10-19
3 wk 135-250 0-33
Docetaxel 1 wk 35-40 0-3
3 wk 60-160 1-14
Ixabepilone 3 wk 6 (qd x5) 3
3 wk 40 7-22
ABI-007 1 wk 100 4
3 wk 175-300 0-10

Phase III Clinical Trials ofIxabepilone Plus Capecitabine
Ixabepilone 40 mg/m2 q3wk plus Capecitabine 1000 mg/m2 bid x 14 days
Capecitabine 1250 mg/m2 bid x 14 days
Trial Inclusion Criteria End Points
CA163046 • Anthracycline-resistant or minimum cumulative dose
• Taxane-resistant
• Measurable tumor
TTP (primary)OSRR
CA163048 • Anthracycline- and taxane-pretreated
• Measurable/nonmeasurable tumor
OS (primary)TTPRR
Randomized
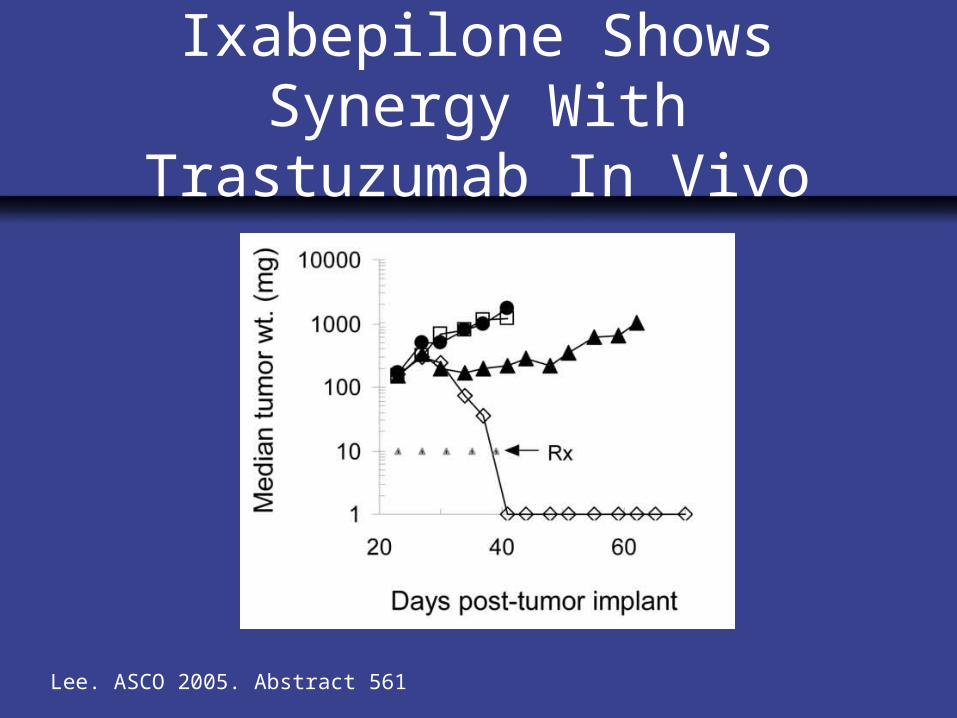
Ixabepilone Shows Synergy With Trastuzumab In Vivo
Lee. ASCO 2005. Abstract 561

Ixabepilone + Pegylated Liposomal Doxorubicin: Metastatic Breast
Cancer
http://www.clinicaltrials.gov/ct/show/NCT00182767
• Phase I/II study (PI: Ellen Chuang, MD, Weill Cornell)• Previously treated metastatic breast, ovarian epithelial,
primary peritoneal cavity, or fallopian tube cancer• Ixabepilone + pegylated doxorubicin (PLD) IV Day 1
every 21 days– Phase I (dose escalation): Ixabepilone over 3 hours + PLD
over 30-60 min– Phase II: Ixabepilone at MTD (determined in phase I) plus
fixed phase I PLD dose
• Endpoints: MTD, safety, efficacy

Trastuzumab + Ixabepilone in HER2+ Metastatic Breast Cancer
• Ongoing phase II (PI: Craig Bunnell, MD, Dana Farber)
• Women with stage IV/recurrent HER2+ metastatic breast cancer (3+ by IHC or FISH+)
• Prior therapy– Cohort 1: No prior treatment for metastatic breast
cancer except hormone therapy– Cohort 2: Prior chemotherapy + trastuzumab– Trastuzumab + ixabepilone IV Day 1 every 21 days
• Primary objective, response ratehttp://www.clinicaltrials.gov/ct/gui/show/NCT00079326

Trastuzumab, Ixabepilone and Carboplatin in HER2+ MBC
http://www.clinicaltrials.gov/ct/gui/show/NCT00077376
• Phase II trial (PI: Stacy L. Moulder, MD)
• Patients with HER2+ metastatic breast cancer
• No prior chemotherapy for metastatic disease
• Primary objective, response rate
• Treatment schedule– Trastuzumab IV on Days 1, 8, 15, and 22
– Ixabepilone + carboplatin IV on Days 1, 8, and 15
– Treatment every 28 days for ≤ 6 cycles in the absence of unacceptable toxicity
Can we predict which patients will respond and which are resistant?

Barlow. J Cell Sci. 2002;115:3469.
Status of Microtubule Assembly May Dictate Drug Sensitivity (Cabral Model)
Sensitive to Stabilizing Agents
Resistant to Stabilizing Agents
Increased Microtubule Assembly
Decreased Microtubule Assembly
Functional Microtubules

Post-translational Modifications of α-Tubulin
• These modifications occur in α-tubulins in MTs (not free form), and are correlated with stable microtubules.
H2NAc
40GEEY
Acetylation
Detyrosination
α-Tubulin H2N GEEY
H2N GEE

= Tumor
= Stromal Staining
Baseline Cycle 2
Patient 1(PR)
Patient 5(PD)
Ixabepilone May Enhance Microtubule Stability Preferentially in Tumor Cells
Acetylated Tubulin

0
2000
4000
6000
8000
10000
12000
14000
16000
18000
20000
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
0
5000
10000
15000
20000
25000
30000
35000
40000
45000
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Sensitive ResistantCell lines
Sen
siti
vity
mar
kers
Res
ista
nce
mar
kers
High
Low
Exp
ress
ion
le
vel
Genes Identified That Correlated With Ixabepilone Sensitivity
Lee. ASCO 2005.

Novel Agents

Kinase Inhibitors Involved With Mitosis
IOnconovaPolo-like Kinase
ON01910
IICytokinetics/
GSKKinesin Spindle Protein (KSP)
SB-715992
ICytokineticsKSPSB-743921
IVertexAurora KinaseVX-680
PHASEDEVELOPERTARGETNAME

Epidermal Growth Factor Receptor Family
INovartisEGFR, HER2, and VEGFR
AEE788
IIPfizer, NCIEGFR and
HER2CI-1033
IIIAbgenix/AmgenEGFRPantimimumab
IIGlaxoSmithKlineEGFR and
HER2Lapatinib
PHASEDEVELOPERTARGETNAME

CONTROL - No Therapy
C1
AZD2171 30 mg qd
DOCETAXEL 75mg/m2 DOXORUBICIN 50mg/m2
CYCLOPHOSPHAMIDE 600mg/m2
FILGRASTIM 300 mcg Days 2-11or PEGFILGRASTIM 6mg Day 2
C2 C3 C4 C5 C6 C7
Surgery, XRT and hormonal therapy as indicated
AZD2171 Neoadjuvant NCI Trial
Accrual Goal: 30 patients
Cycle 1: 7 days Cycles 2-7: Every three weeks
N=20
N=10
DYNAMIC MRI
TUMOR BIOPSIES, SERUM STUDIES

AZD2171 Neoadjuvant NCI Trial
Objectives• Pathologic CR in the breast
• Changes in parameters of angiogenesis:– Phospho-VEGFR-2 in tumor– VEGF in tumor – Soluble VEGFR-2, VEGF, and circulating
endothelial cells.– Vascular permeability using Dynamic Contrast
Enhanced MRI

PARP Inhibition
• Inhibition leads to sensitization to DNA damaging agents – Radiation– Platinums, cyclophosphamide,
irinotecan, temozolomide, anthracyclines
– May be more potent in tumors with defective DNA repair mechanisms
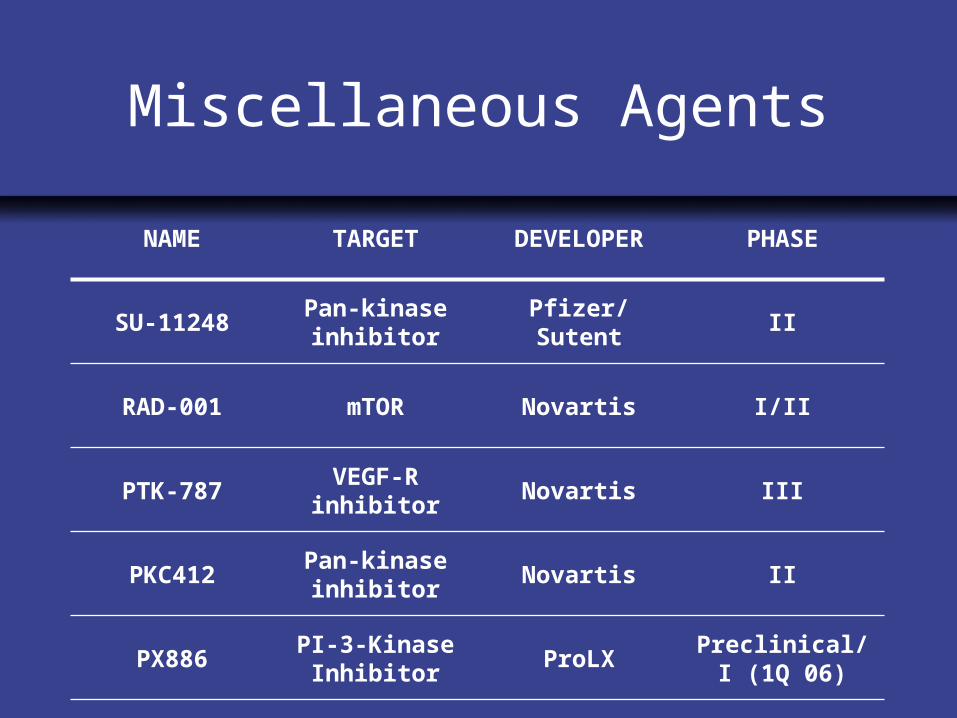
Miscellaneous Agents
Preclinical/I (1Q 06)
ProLXPI-3-Kinase
InhibitorPX886
IINovartisPan-kinase
inhibitorPKC412
I/IINovartismTORRAD-001
IIINovartisVEGF-R inhibitor
PTK-787
IIPfizer/SutentPan-kinase
inhibitorSU-11248
PHASEDEVELOPERTARGETNAME

Conclusion
• Ixabepilone very active in breast cancer
• Advantages – No steroid premedication– Minimal hypersensitivity reactions and
nausea/ vomiting– 3%-5% Grade 3 peripheral neuropathy
• Combinations in progress
• Many new agents on the horizon

Acknowledgments
Cancer Therapeutics Branch
James Lee, MD, PhD
Tito Fojo, MD, PhD
Xiaowei Yang, MD, PhD
Marianne Poruchynsky, PhD
Neelima Denduluri, MD
Janice Walshe, MD
Suparna Bonthala, MD
Arlene Berman, RN
Michael Cox, PharmD
Nitin Mannan
Ujala Vatas
CTEP
Jennifer A. Low, MD, PhD
Dimitrios Colevas, MD
Radiology
Catherine Chow, MD
Rehabilitation Medicine
Earllaine Croarkin
Rebecca Parks
Statistics
Seth Steinberg, PhD
Bristol-Myers Squibb Co
Ron Peck, MD