epidermolysis bullosa: a case report - quintessence publishing!
TRANSCRIPT
Oral Medicine
Epidermolysis bullosa: A case reportMurat Sipahier"*
The term epidermolysis bullosa describes a group of rare genetic mechanicobullous disor-ders. The disease has .'several modes of inheritance with various degrees of severity and expres-sion. A patient with simplex epidermolysis hullosa had typical cutaneous lesions and dentalinvolvemeni. The teeth were severely affected by hypoplasia. Denial therapy consisted ofplacement of amalgam restorations and topical applications of fluoride. The need for. and ad-vantages of. early preventive and restorative dental care are illustrated by the case presented.(Quintessence Int }994;25:S39-S43.)
Introduction
Epidermolysis hullosa {EB) refers 10 an uncommongroup of skin disorders that are either acquired or ge-netically transmitted as either autosomal-dominantand autosomal-recessive traits. The prominent clinicalcharacteristic of the disease is the development of bul-lae or vesicles in response to minor mechanical trauma.These lesions generally appear on the skin, but mucosallesions are also common.'-
The disease is divided into the following types'"':
!. Epidermolysis hullosa simplex is transmitted as adominant trait. Lesions heal without scarring, andmucous membranes and nails are rarely affected.
2. Epidermolysis bullosa dystrophic exists in dominanthyperplastic and recessive polydysplastic forms. Thehyperplaslic form is characterized by mild scarringand few milia. and oral mucous membranes andnails are involved. The polydyspiastic type leavesextensive atrophie scars, milia are present, mucousmembranes are involved, and dystrophic changes
Assistant Professor, Department of Pédiatrie Dentistry, Univer-sity of Gazi. Faculty of Dentistry, Emek Mahallesi 8, Cadde 82,Sokak No. 4,0ñ510 Ankara, Turkey.
3. Epidermolysis bullosa letalis is a type of epidermol-ysis bullosa that is inherited as a recessive trait.Death usually occurs in 3 months. Bullae do notheal, leaving large eroded areas. Oral mucous mem-branes and nails are involved.
4. Epidermolysis bullosa (Weber-Cockayne type) istransmitted as a dominant trail. Adult unset of blis-ters is usually on the soles of the feet (iiouscarriug)but occasionally occurs on the palms,
5. Epidermolysis bullosa acquisita is a rare form ofEBin which there is no evidence of familial and heredi-tary transmission. The clinical features are blistersat the site of Iranma, milia, involved mucous mem-branes, and nail dystrophy.
Case report
On June 22,1992. a 9-year-old white boy with a knowndiagnosis of epidermolysis bullosa simplex was admit-ted to the Department of Pédiatrie Dentistry for dentalevaluation and care. The boy was unable to chew wellbecause of his malformed teeth.
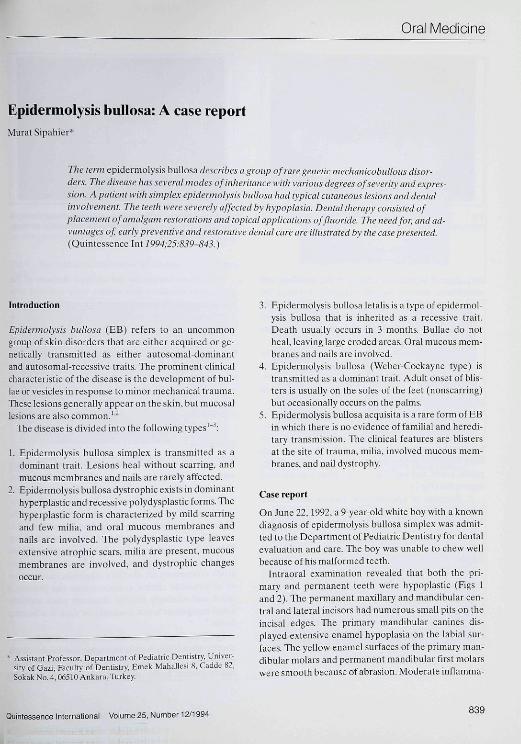
Intraoral examination revealed that both the pri-mary and permanent teeth were hypoplastic (Figs 1and 2). Tlie permanent maxillary and mandibtilar cen-tral and lateral incisors had numerous small pits on theincisai edges. The primary mandibular canines dis-played extensive enamel hypoplasia on the labial sur-faces. The yellow enamel surfaces of the primary man-dibular molars and permanent rnandibular first molarswere smooth because of abrasion. Moderate inflamma-
Quintessence International Volume 25, Number 12/Î 994839
Oral Medicine
Fig 1 The manaioular teeth of the 9-year-old patient arehypoplastic.
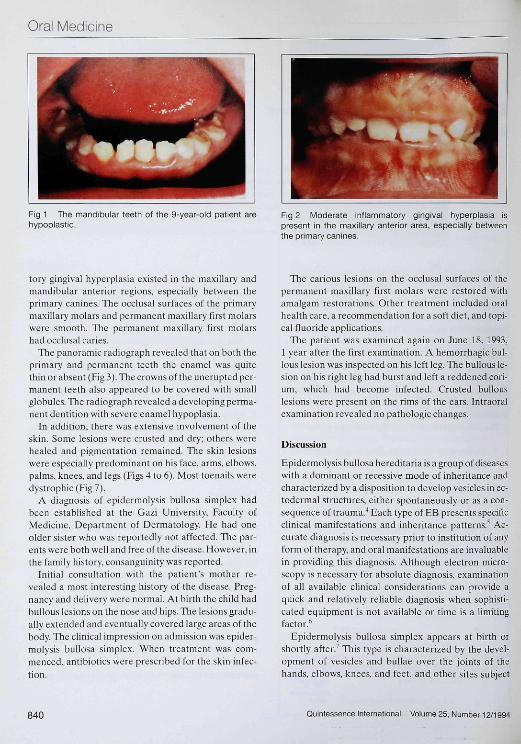
Fig 2 Moderate inflammatory gingival hyperplasia ispresent in the maxillary anterior area, especially betweenthe primary canines.
tory gingival hyperplasia existed in the maxillary andmandibular anterior regions, especially between theprimary canines. The occlusal surfaces of the primarymaxillary molars and permanent maxillary first molarswere smooth. The permanent maxillary first molarshad occlusal caries.
The panoramic radiograph revealed that on both theprimary and permanent teeth the enamel was quitethin or absent (Fig ,1). The crowns of the unerupted per-manent teeth also appeared to be covered with smallglobules. The radiograph revealed a developing perma-nent dentition with severe enamel hypoplasia.
In addition, there was extensive involvement of theskin. Some lesions were crusted and dry; others werehealed and pigmentation remained. The skin lesionswere especially predominant on his face, arms, elbows,palms, knees, and legs (Figs 4 to 6), Most toenails weredystrophic(Fig7).
A diagnosis of epidermolysis bullosa simplex hadbeen established at the Gazi University, Faculty ofMedicine, Department of Dermatology. He had oneolder sister who was reportedly not affected. The par-ents were both well and free of the disease. However, inthe family history, consanguinity was reported.
Initial consultation with the patient's mother re-vealed a most interesting history of the disease. Preg-nancy and dehvery were normal. At birth the child hadbullous lesions on the nose and hips. The lesions gradu-ally extended and eventually covered large areas of thebody. The clinical impression on admission was epider-molysis bullosa simplex. When treatment was com-menced, antibiotics were prescribed for the skin infec-tion.
The carious lesions on the occiusai surfaces of thepermanent maxillary first molars were restored withamalgam restorations. Other treatment included oralhealth care, a recommendation for a soft diet, and topi-cal fluoride applications.
The patient was examined again on June 18, 1993,1 year after the first examination. A hemorrhagic bul-lous lesion was inspected on his left leg. The bullous le-sion on his right leg had burst and left a reddened cori-um, which had become infected. Crusted bullouslesions were present on the rims of the ears. Intraoralexamination revealed no pathologic changes.
Discussion
Epidermolysis bullosa hereditaria is a group of diseaseswith a dominant or recessive mode of inheritance andcharacterized by a disposition to develop vesicles in ec-todermal structures, either spontaneously or as a con-sequence of trauma.''Each type of FB presents specificclinical manifestations and inheritance patterns.- Ac-curate diagnosis is necessary prior to institution of anyform of therapy, and oral manifestations are invaluablein providing this diagnosis. Although electron micro-scopy is necessary for absolute diagnosis, examinationof all available clinical considerations can provide aquick and relatively reliable diagnosis when sophisti-cated equipment is not available or time is a limitingfactor.*'
Epidermolysis bullosa simplex appears at birth orshortly after.' This type is characterized by the devel-opment of vesicles and bullae over the joints of thehands, elbows, knees, and feet, and other sites subject
840 Quintessence International Volume 25, Number 12/1994

Oral Medicine
Fig 3 The enamel ol the primary and permanent teetn isquite thin. The surface structure ot the enamel of the un-erupted permanent teeth is globular.
Fig 4 Numerous bulious lesions are visibieon the patient'sface.
Fig 5 Crusted bulious lesions ere present on the patient'spalms.
Fig 5 Crusted bulious lesions and postinflammatory pig-mentations are present on the patient's knees and legs.
Fig 7 Most of the patient's toenails are dystrophic.
Quintessence International Volume 25, Number 12/1994841

Orai Medicine
to repeated trauma.^ The frequency of development ofbuliae increases with heat, and the lesions heal withoutresidual scarring or pigmentation.' Usually the mucousmembranes and nails are not involved," Nails are af-fected in only a small percentage of patients. Oral mu-cosal and dental involvement occur rarelv.*" This formusually diminishes or disappears at puberty.'' Tliepatient's medical history and clinical findings can con-firm the diagnosis of epidermolysis bullosa simplex.
It appears that cause of EB is related to abnormalenzyme activity and collagen degradation; however,the exact pathogenesis remains unclear,^
Although there is no total agreement among investi-gators, there appears to be a consensus that patientswith the recessive dystrophic and junctional forms ofEB have dyspiastic teeth more often than do those withthe dominant dystrophic and simplex forms.'"
The enamel, dentin. and eementum of patients withEB have been studied with light microscopy, scanningelectron microscopy, and microradiography, and histo-pathologic changes during amelogenesis have beendescribed.''-^" ''' Vascular changes occur in the stellatereticulum. and the outer enamel epithelium of the ena-mel organ may degenerate. There appears to be con-sensus that the ameloblasts do not undergo any altera-tion. Random distribution of the hypopiastic defeets ofthe enamel indicates the possibility that some amelo-blasts have reduced activity at the time of matrix for-mation and perhaps even at the time of calcification.'''Clinically and radiographically diagnosed enamelhypoplasia in the present patient confirms previousreports that dental involvement may be observed inepidermolysis bullosa simplex.'''**
The marginal gingivitis in this patient may have beenpartly due to understimulation, Burket'^ stated thatunderstimulation of the gingival tissues is a frequentcause of gingivitis. Abnormal chewing habits are an-other cause. The normal chewing habits are modifiedby any painful lesion of the oral tissues.
In this patient another factor probably played an im-portant role in the development of the gingivitis. AsBeube"" stated, some teeth, because of their impropershape or atypical relationship with adjacent or oppositeteeth, may contribute to gingival irritation becausepoor contour may permit food and materia alba to be-come retained and impacted. This would occur in teethwith extensive dental caries, congenital defects, and hy-popiastic enamel,
Tliere is no specific treatment for epidermolysis bul-losa, only palliative therapy. Injections of cortisone andadrenocorticotropic hormone have provided only tem-
porary improvement. Prevention of undue trauma hasbeen the main goal in the care of persons affected byepidermolysis bullosa," Antibiotics may be used tocontrol the secondary infection that invariably followsthe riiptureof the vesicles.'"
Patients with epidermolysis bullosa simplex have nointraoral abnormalities related to their disorder, andtherefore are treated in the manner of a normal pa-tient,'' Individuals with milder forms of EB require fewalterations in their dental care and may be treatedmueh like any other patient. The practitioner should,however, carefully question any individual with EB asto the fragility of the mucosa because dental therapycan precipitate oral blistering even in some mildly af-fected patients.
Conversely, an altered approach to oral rehabilita-tion and anesthetic management may be required in in-dividuals with enamel hypoplasia. rampant caries, ex-treme fragility of the mucosa, or microstomia." Indi-viduals with severe soft tissue involvement requiringmultiple restorative and surgical procedures typicallyare best managed when they are under general anes-thesia.^"
References1. Lever WF, Sch a um burg-Lever GZ. Histopathology of the Skin.
Philadelphia: Lippiiicoll. 1983:68-70.2. Shaler WG, Hine MK, Levy BM. A Testbook of Orai Patholo-
gy, Philadelphia: Saunders, 1983:838-840.
3. Rocnigk HH, Ryan JG. Bergfeld WF. Epidermolysis bullosaac-quisita, Reporl of three cases and review of all published eases.Arch Dermatol Í971;103:l-10,
4. Arwili T, Bergenholtz A, Olsson O. Epidermolysis builosahereditaria. III. A histologie study of changes in teeth in thepoiydysplastic dystrophic and ¡ethal forms. Orai Surg Oral MedOrai Palhol 1965; 19:723-744.
5. Wright JT. Epidermolysis buliosa: Dental and anesthetic man-agement of two cases. Orai Surg Oral Med Oral Patho!1984;57:155-157.
6. Crawford EG. Burkes EJ. Briggaman RA. Hereditary epider-molysis builosa: Orai manifestations and dental therapy. OraiSurgOralMedOral Palhol 1976:42:490-501).
7. MoghadaniBK, Gier RE, Epidermolysis builosa: Oral manage-ment and case reports. ASDC J Dent Child 1992:59:66-69.
8. Domoniios AN. Andrews" Diseases of the Skin' Clinieal Der-matology, Phiiadelphia: Saunders. 1971:663-657.
9. Wright JT, Gantt DG. Epidermolysis buliosa. Associated withenamel hypoplasia and taurodoatism. J Oral Pathol 1983;12:73-83.
Kl, Nowak AJ. Oropharyngeal iesions and their management inepidermolysis buliosa. Arch Dermatol 1988; 124:742-745.
11. Brain EB, WigglesworthJS. Developing teeth in epidermolysisbullosa hereditaria letalis. A histologieal study Br Dent J1908:124:255-260.
12. Gardner DG. Hudson CD. The disturbances in odonlogenesis
842 Quintessence Intemational Volume 25, Number 12/1994

Oral Medicine
in epidermolysis bullosa hereditaria Ictalis, Oral Surg Oral MedOral Pathol 1975:40:4S3-iy3.
13. Hitchin AD. Tiie defects of cementum in epidermolysis btillosadystrophia. Br DentJ 1973il35:437-442.
14. Koshiba H, Kiniura O. Nakata M. A elinical and histologie ob-servation of enamel hypoplasia in a case of epidermolysis bullo-sa hereditaria. Oral Surg Oral Med Or.il Pathol 1977;43:585-5911.
15. Burke LW. Oral Medicine, Philadelphia: Lippincott, 1957:23-25.
16. Beube FE. Periodontology, New York: Macniillan, 1953:97-99,121-126,659.660.
17. Gormley JW, Schow CE. Epidermolysis bullosa and associatedproblems in oral surgical treatment. J Oral Surgl976;34:45-52.
18. Kiislick RS, Brustein HC. Epidermolysis bullosa. Review of theliterature and report of a case. Oral Surg Oral Med Oral PatholI%1;14:I315-I33O.
19. Wright JT. Comprehensive denial ciire and general anestheticmanagement of hereditary epidermolysis bullosa: A review offourteen cases. Oral Surg Oral Med Oral Pathol 1990;70:573-578.
20. Wrigth JT, Fine JD. Johnson L. Hereditary epidermolysis bullo-sa: Oral manifestations and dental management. Pediatr Dent1993;]5:242-248.
Moving Soon?Please notify us promptly of any change of addressto assure an uninterrupted subscriplion.
Complete the form below and send to:QI Subscription Department, QuinlessencePublishing Co., Inc., 551 North Kimberly Drive,Carol Stream, IL 60188
Name.
New address.
City, State, ZIP_
Moving from:_
(Old address).
¡City, State, ZIP). .
Note: To expedite delivery, send the change of address assoon as you know it. and allow 6 weeks for processing.
DISTRICT OF COLUMBIA DENTAL SOCIETY
63rd ANNUAL SPRING MEETINGRegistered Clinicians:
Dr. Mort Amsterdam Dr. David HoexterDr. Irwin Becker Dr. Ronald JacksonCNA Risk Management Dr. Joseph Konzelman
Setnitiar Ms, Sally McKenzieI>r, Hugh Doheny Dr. James SciubbaDr. Ralph Duffin Dr. Barbara StcinhergDr. Thotn Dumsha Dr. William StruppDr. Jacqueline Dzierzak Dr. Van ThompsonDr. Mark Friedman Ms. Kathedtie West
Also Featuring:Keynote Speaker: Dental Team Luncheoti
Ms. Helen ThomasOffice Design Lecture
and TourLunch and LearnSpecialists" BreakfastClinical Abstracts SessionTable Clinics
Over 275 Exhibit Booths!
Auxiliary ProgramsGala a( the Ketinedy CenterU.S. Holocaust Memorial
Museum TourNight Photo TourMt. Vemon TourArlitigton Cemetery Tour
I
T a preliminaiy program, cof'tpffte and teaiin l\
D/C. Dental SocietyS02 C SUfPt, N E
Washington. D,C. 2O(X)2-58tÜ(202|547-7613'FAX (202) 546-t432
. Z i p .
Maich 2-5 . 1995 • The Sheraton Washington Hotel • Washington. D.C.
Quintessence International Volume 25. Number 12/1994843