epidemiology of the metabolic syndrome in the usa incidence ? prevalence distribution control ?...
TRANSCRIPT

Epidemiology of the Metabolic Syndrome in the USA
• Incidence ?
• Prevalence
• Distribution
• Control ?
• Incidence ?
• Prevalence
• Distribution
• Control ?
Epidemiology Evaluates a Disease

Epidemiology of the Metabolic Syndrome
What is It ?
Why are its Limitations ?
Why is It Important ?
What is its Prevalence ?
What are its Clinical Outcomes ?
- Cardiac
- Diabetes
- Nonalcoholic Fatty Liver Disease

The Metabolic Syndrome
Obesity Diabetes
HyperlipidemiaHypertension
Insulin Resistance

Epidemiology of the Metabolic Syndrome
What is It ?
Why are its Limitations ?
Why is It Important ?
What is its Prevalence ?
What are its Clinical Outcomes ?
- Cardiac
- Diabetes
- Nonalcoholic Fatty Liver Disease
Metabolic Syndrome
• World Health Organization (WHO)
• International Diabetes Association (IDF)
• Adult Treatment Panel (ATP III)
-National Cholesterol Education Program Expert Panel
• World Health Organization (WHO)
• International Diabetes Association (IDF)
• Adult Treatment Panel (ATP III)
-National Cholesterol Education Program Expert Panel
There are 3 Definitions

Three Different Definitions
Obesity
BP
Fasting Glucose
Triglycerides
HDL Cholesterol
Micro Albumin
BMI
Similar
IPG/HOMA
Same
Not Used
Used
BMI
Similar
IPG/HOMA
Same
Not Used
Used
Central
Same
>6.1mol/L
Same
Similar
Not Used
Central
Same
>6.1mol/L
Same
Similar
Not Used
IDF WHOATP
Central
Same
>5.6mol/L
Same
Similar
Not Used
Central
Same
>5.6mol/L
Same
Similar
Not Used

Concerns About the Metabolic Syndrome
• Criteria are Ambiguous
• Rationale for Thresholds ill defined
• Inclusion of Diabetes Questionable
• Importance of Insulin Resistance Unclear
• Questions about CVD Risk Factors Remain
• Treating MS no different than treating its parts
• Medical Value of Diagnosing MS is Unclear
• Criteria are Ambiguous
• Rationale for Thresholds ill defined
• Inclusion of Diabetes Questionable
• Importance of Insulin Resistance Unclear
• Questions about CVD Risk Factors Remain
• Treating MS no different than treating its parts
• Medical Value of Diagnosing MS is Unclear
(ADA and EASD)(ADA and EASD)

Epidemiology of the Metabolic Syndrome
What is It ?
Why are its Limitations ?
Why is It Important ?
What is its Prevalence ?
What are its Clinical Outcomes ?
- Cardiac
- Diabetes
- Nonalcoholic Fatty Liver Disease

Prevalence (%) of Metabolic Syndrome
Country ATP IDF WHO
South Asia 26 18 23
Australia 19 16 21
France 9 13 18
Italy 18 34

Prevalence (%) of Metabolic Syndrome
United States and China
County ATP IDF WHO
USA
National 24 40
Texas 25 25
China
Hong Kong 17 21
InterAsia 14

Epidemiology of the Metabolic Syndrome
What is It ?
Why are its Limitations ?
Why is It Important ?
What is its Prevalence ?
What are its Clinical Outcomes ?
- Cardiac
- Diabetes
- Nonalcoholic Fatty Liver Disease

Metabolic Syndrome Predicts All Cause Mortality (13 year Follow up)
Metabolic Syndrome
No Yes
ATP III (%) 10 21 p<0.01
WHO (%) 10 18 p<0.05

Metabolic Syndrome and Cardiac Death
0.8
0.85
0.9
0.95
1
0 2 4 6 8 10 12 14 16
No
Yes
Years Of Follow-Up
NCEP-MetS

Metabolic Syndrome Predicts Diabetes (8 year Follow up)
Diabetes
No Yes
ATP III (%) 14.4 28.7 p<0.0001
WHO (%) 12.5 41.3 p<0.0001

Epidemiology of the Metabolic Syndrome
What is It ?
Why are its Limitations ?
Why is It Important ?
What is its Prevalence ?
What are its Clinical Outcomes ?
- Cardiac
- Diabetes
- Nonalcoholic Fatty Liver Disease

Non-Alcoholic Fatty Liver Disease
• What is it?
• Why is it Important?
• How do you treat it?
• What is it?
• Why is it Important?
• How do you treat it?

Proposed Classification for NAFLD*
• Conditions associated with an insulin resistance syndrome - Diabetes mellitus (type II) - Obesity - Hyperlipidemia
• Conditions associated with an insulin resistance syndrome - Diabetes mellitus (type II) - Obesity - Hyperlipidemia
PrimaryPrimarySecondarySecondary
• DRUGS
- Corticosteroids - Synthetic Estrogens - Amiodarone - Perhexiline - Nifedipine
• DRUGS
- Corticosteroids - Synthetic Estrogens - Amiodarone - Perhexiline - Nifedipine
• SURGICAL PROCEDURES - Gastroplexy - Jejunoileal bypass - Extensive small bowel resection - Bilio-pancreatic Diversion
• SURGICAL PROCEDURES - Gastroplexy - Jejunoileal bypass - Extensive small bowel resection - Bilio-pancreatic Diversion
• MISCELLANEOUS
- Abeta/ hypobeta - Weber-Christian Disease - TPN with glucose - Environmental toxins - S. Bowel Diverticulosis
• MISCELLANEOUS
- Abeta/ hypobeta - Weber-Christian Disease - TPN with glucose - Environmental toxins - S. Bowel Diverticulosis

Non-Alcoholic Fatty Liver DiseaseNon-Alcoholic Fatty Liver Disease
NASHNASH
INFLAMMATIONINFLAMMATION
STEATOSISSTEATOSIS

Non-Alcoholic Fatty Liver(NAFL)
Non-Alcoholic Fatty Liver(NAFL)
Type 1Type 2Type 3Type 4
Type 1Type 2Type 3Type 4
- Fat alone- Fat + Inflammation- Fat + Hepatocyte Injury- Fat + Fibrosis and/ or Mallory Bodies
- Fat alone- Fat + Inflammation- Fat + Hepatocyte Injury- Fat + Fibrosis and/ or Mallory Bodies

NAFLD Activity Score (NASH CRN)
GradeGrade
SteatosisInflammationBallooning Injury
Maximum Score
SteatosisInflammationBallooning Injury
Maximum Score
0 - 30 - 30 - 2
8
0 - 30 - 30 - 2
8
Histologic FindingHistologic Finding
NASH Requires a Score of 4 with at least 1 Point from Ballooning InjuryNASH Requires a Score of 4 with at least 1 Point from Ballooning Injury

WHAT IS NON-ALCOHOLIC?WHAT IS NON-ALCOHOLIC?



Benefits of BeerBenefits of Beer
• Religion
• Patriot
• Government
• Religion
• Patriot
• Government
9 Patron Saints
Ben Franklin
NIAAA
9 Patron Saints
Ben Franklin
NIAAA

Beer Is Proof That God Loves UsAnd Wants Us To Be Happy
Beer Is Proof That God Loves UsAnd Wants Us To Be Happy
- Ben Franklin- Ben Franklin

Relative Mortality (All Causes)
Wine DrinkersWine Drinkers
0 1-7 8-21 22-35 350 1-7 8-21 22-35 35
1.6
1.4
1.2
1.0
0.8
0.6
0.4
1.6
1.4
1.2
1.0
0.8
0.6
0.4
Non WineDrinkersNon WineDrinkers


Risk Factors for Fibrosis in NAFLD
OR 95%CI P
Age, years 1.07 1.04 – 1.08 <0.0001
Diabetes, yes vs. no 2.54 1.75 – 3.69 <0.0001
Alcohol usage, not abstinentvs abstinent 0.53 0.37 – 0.75 0.0004

Benefits of Alcohol in NonAlcolic Fatty Liver Disease
• Improves Insulin Resistance
• Decreases ALT
• Less NASH in Bariatric Surgery Pts
• Less Fibrosis in Nash CRN
• Improves Insulin Resistance
• Decreases ALT
• Less NASH in Bariatric Surgery Pts
• Less Fibrosis in Nash CRN
Practical ConclusionsPractical Conclusions
• Histologic Definition Fat + Ballooning Degeneration Fat + Fibrosis
• Exclusion Limit for Daily Alcohol Use 7 units per wk for women 14 units per wk for men
• Histologic Definition Fat + Ballooning Degeneration Fat + Fibrosis
• Exclusion Limit for Daily Alcohol Use 7 units per wk for women 14 units per wk for men

Non-Alcoholic Fatty Liver Disease
• What is it?
• Why is it Important?
• How do you treat it?
• What is it?
• Why is it Important?
• How do you treat it?

The Importance of Any Disease
The Importance of Any Disease
• Natural History• Prevalence
• Natural History• Prevalence
Determined by:Determined by:

Progressive FibrosisSteatosis Alone
Teli(1995)
1/40
Teli(1995)
1/40
(10 Year Follow-Up)(10 Year Follow-Up)
Matteoni(1999)
2/49
Matteoni(1999)
2/49
Dam-Larsen(2003)
1/109
Dam-Larsen(2003)
1/109
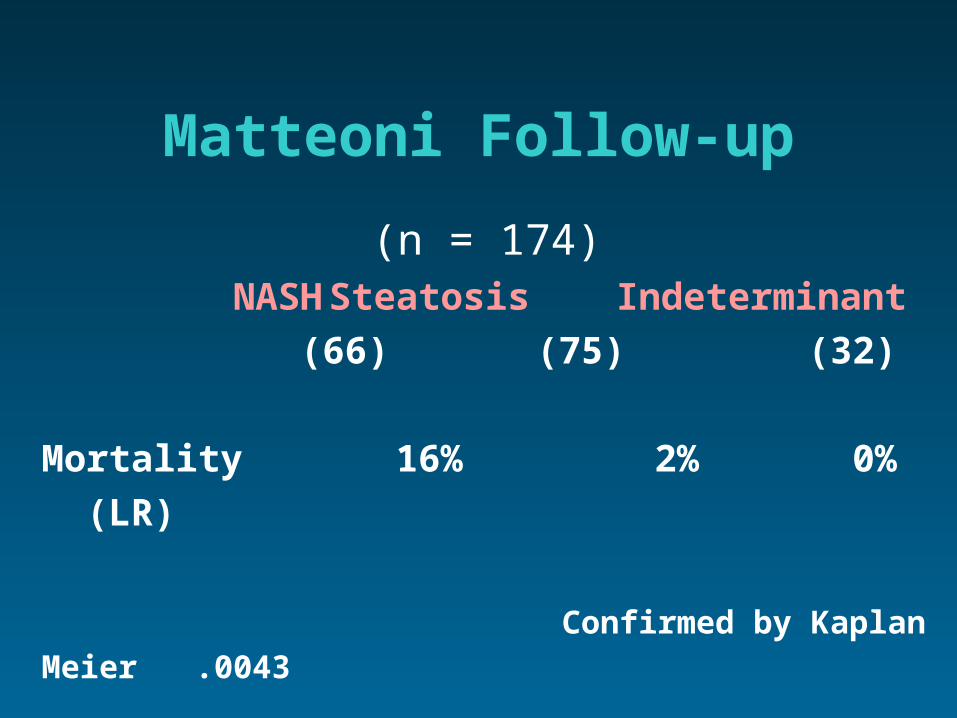
Matteoni Follow-up
(n = 174)NASH Steatosis Indeterminant
(66) (75) (32)
Mortality 16% 2% 0%
(LR)
Confirmed by Kaplan Meier .0043

Natural History of NASH
Sub-AcuteFailure
Sub-AcuteFailure
CIRRHOSISCIRRHOSIS
HCCHCC Post-OLTXRecurrencePost-OLTXRecurrence
Liver RelatedDeath
Liver RelatedDeath
NASHNASH
20%20% 30 - 40%30 - 40%
(2%)(2%)(8%)(8%) ??

Su r
viva
l (%
)S
u rvi
val (
%)
1.0
0.8
0.6 0.4
0.2
0
1.0
0.8
0.6 0.4
0.2
0
0 2 4 6 8 10 12 14 160 2 4 6 8 10 12 14 16
Time (years) Time (years)
Expected Expected
Observed Observed
p = 0.005 p = 0.005
Adams, 2005
Survival in NAFLD

Time (years)Time (years)
1.0
0.8
0.6
0.4
0.2
0
1.0
0.8
0.6
0.4
0.2
0
0 5 10 15 200 5 10 15 20
NAFLD patients
Referencepopulation
NAFLD patients
Referencepopulation
Ekstedt, 2006
Survival in NAFLD
n=129

Time (years)Time (years)
1.0
0.8
0.6
0.4
0.2
0
1.0
0.8
0.6
0.4
0.2
0
0 5 10 15 200 5 10 15 20
Steatosis
Referencepopulation
Steatosis
Referencepopulation
Ekstedt,2006
Survival in Steatosis

Time (years)Time (years)
1.0
0.8
0.6
0.4
0.2
0
1.0
0.8
0.6
0.4
0.2
0
0 5 10 15 200 5 10 15 20
NASH
Referencepopulation
NASH
Referencepopulation
Ekstedt, 2006
Survival in NASH
p<0.01

Subjects with NAFLD have a greater than expected mortality compared to matched
controls
• Risk factors for mortality:– Diabetes (p< 0.005)– Age (p < 0.001)– Cirrhosis (p< 0.02)
• Increased mortality:*– cardiovascular disease– liver diseaseAdams et al, Gastroenterology, 2005, 129:113-121
* Ekstedt et al, Hepatology, 2006, 44:865-873* Sanyal et al, Hepatology, 2006, 43:682-689

SUMMARYSUMMARY
• NASH is Not a Benign Disease
• Cirrhosis Develops in 20-25% of Cases -Liver Related Deaths in 10%
• The Prevalence is High and Increasing World Wide
• NASH is Not a Benign Disease
• Cirrhosis Develops in 20-25% of Cases -Liver Related Deaths in 10%
• The Prevalence is High and Increasing World Wide

The Importance of Any Disease
The Importance of Any Disease
• Prevalence• Natural History
• Prevalence• Natural History
Determined by:Determined by:

Metabolic Syndrome(NHANES III, 1988-1994)
OVERALL PREVALENCE24%
Diagnosis Based on Elevated Serum Enzymes

Dallas Heart Study
Hepatic TriglycerideContent (%) *
Hepatic TriglycerideContent (%) *
HepaticSteatosis (%)
HepaticSteatosis (%)
All
Black
White
Hispanic
All
Black
White
Hispanic
3.6 (2.1 – 6.6)
3.2 (2.0 – 5.3)
3.6 (2.1 – 7.3)
4.6 (2.6 – 10.3)
3.6 (2.1 – 6.6)
3.2 (2.0 – 5.3)
3.6 (2.1 – 7.3)
4.6 (2.6 – 10.3)
31
24
33
45
31
24
33
45
Browning, 2005Browning, 2005
* Based on NMR and presented as Median (interquartiles)* Based on NMR and presented as Median (interquartiles)
SubjectsSubjects

Prevalence of NAFLD(Updated)
Prevalence of NAFLD(Updated)
Steatosis
30%
Steatosis
30%
NASH
6-8%
NASH
6-8%

Epidemiology of NAFLD
USA
Italy
Japan
Taiwan
India
USA
Italy
Japan
Taiwan
India
Cases(in millions)
Cases(in millions)
Country Country
90
17
78
8
240
90
17
78
8
240
30
30
30
37
24.5
30
30
30
37
24.5
Prevalence(%)
Prevalence(%)

SUMMARYSUMMARY
• NASH is Not a Benign Disease
• Cirrhosis Develops in 20-25% of Cases -Liver Related Deaths in 10%
• The Prevalence is High in the United States and Increasing World Wide

The Metabolic Syndrome
NAFLD Diabetes
CancerCardiovascular
Metabolic Syndrome
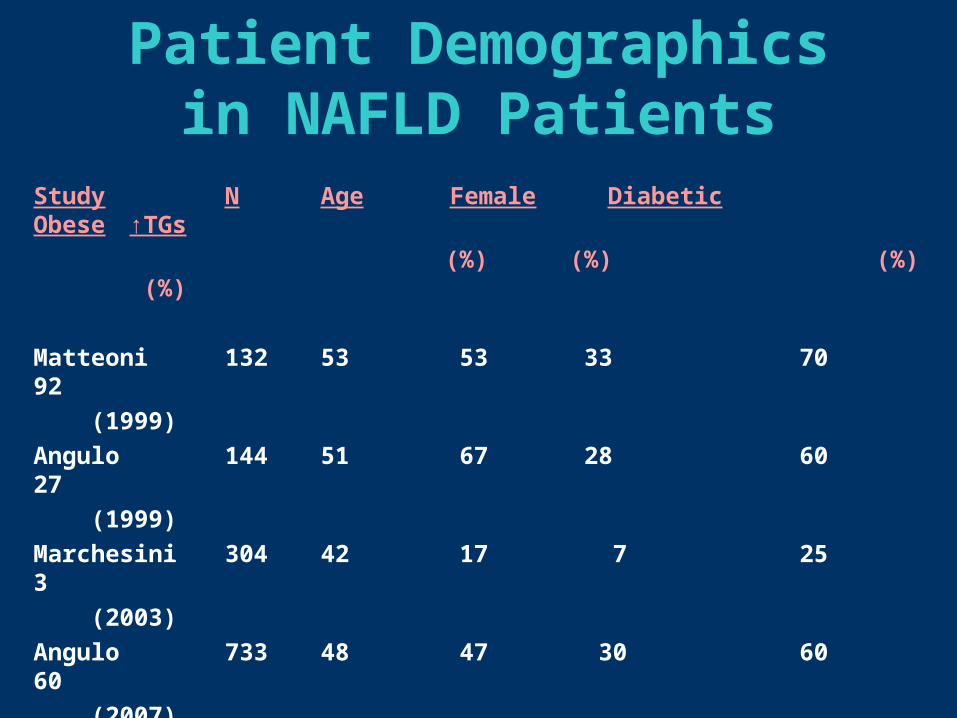
Patient Demographicsin NAFLD Patients
Study N Age Female Diabetic Obese ↑TGs
(%) (%) (%) (%)
Matteoni 132 53 53 33 70 92
(1999)
Angulo 144 51 67 28 60 27
(1999)
Marchesini 304 42 17 7 25 3
(2003)
Angulo 733 48 47 30 60 60
(2007)
NASH CRN 1,266 50 64 31 62 55
(2010)

Metabolic Syndrome
BMI
Waist(cm)
% Hypertension
% Low HDL
% Hyperglycemia
HOMA-R %
Metabolic Syndrome(%)
Fatty Liver (n=63)
NASH(n=110)
28
96
53
57
60
3.2
67
29
100
72
76
91
4.2
88
Marchesini, 2003

The Metabolic Syndrome
NAFLD Diabetes
CancerCardiovascular
Metabolic Syndrome

NAFLDNAFLD
Age at DiagnosisFemalesBMITriglyceridesDevelopment of CirrhosisLiver Related Deaths
Age at DiagnosisFemalesBMITriglyceridesDevelopment of CirrhosisLiver Related Deaths
Diabetes(n=42)
Diabetes(n=42)
37 ± 1167%
31 ± 5489 ± 312
23.9%19%
37 ± 1167%
31 ± 5489 ± 312
23.9%19%
54 ± 1447%
29 ± 6226 ± 115
10.6%2%
54 ± 1447%
29 ± 6226 ± 115
10.6%2%
NS.04.02.04
.05
.02
NS.04.02.04
.05
.02
No Diabetes(n=42)
No Diabetes(n=42) P ValueP Value

The Metabolic Syndrome
NAFLD Diabetes
CancerCardiovascular
Metabolic Syndrome

RISK OF CARDIOVASCULAR DISEASE
Type 2 Diabetes
Odds ratio
NAFLD present 1.84 (2.4-2.1) p <.04 1.96(1.4-2.7) p <.001
Adjusted for 1.54 (1.2-1.7) p = .02Metabolic 1.87 (1.2-2.6) p>.001Syndrome
Targher, 2005,2007

Non-Alcoholic Fatty Liver Disease
• What is it?
• Why is it Important?
• How do you treat it?
• What is it?
• Why is it Important?
• How do you treat it?

Emerging TherapiesEmerging Therapies
RevisitCommon Sense
RevisitCommon Sense
CurrentStrategiesCurrent
Strategies New IdeasNew Ideas
• Diet• Supplements• Co-Morbidities
• Diet• Supplements• Co-Morbidities
• Insulin Resistance• Anti-cytokines• Anti-oxidants
• Insulin Resistance• Anti-cytokines• Anti-oxidants
• Inflammation• Apoptosis• Nuclear Receptor Ligands
• Inflammation• Apoptosis• Nuclear Receptor Ligands

Weight Loss and NASH
Weight Improved
Loss(%) Histology
Life Style Change 9.3 Yes
Control 0.25 No
Hepatology 2010;51:121-129

Primary Outcome –Vitamin E alone met
the pre-specified primary endpoint
Vit E placebo Pio0
10
20
30
40
50
treatment groups
Pro
po
rtio
n o
f su
bje
cts
(%)
P< 0.001 (P< 0.04)
36/84NNT=4.4
26/80NNT= 6.6
16/83

Vitamin E for NASH• Vitamin E (800 IU/day), but not pioglitazone (30
mg/day), was superior to placebo for histological improvement as defined as the primary outcome
• Both vitamin E and pioglitazone significantly improved:– Steatohepatitis– Steatosis grade– Inflammation grade– NAFLD activity score
• Neither drug improved fibrosis scores

Prevention of Insulin Mediated Disease
Environment / Genes
Normal IROS
Obesity DiabetesHypertensionDyslipidemiaVascular diseaseLiver diseaseCancer National Screening
Early Counseling
X