epidemiology of non communicable diseases in morocco · epidemiology of non communicable diseases...
TRANSCRIPT

Epidemiology of non communicable diseases in Morocco
Khalid Moumad, PhD student
Institut Pasteur, Morocco
EUNAM meeting, Tunis

Brief history of ALSC
a
Kingdom of Morocco
Morocco Population
• 2010 total population: 31 951 412
• Urbanisation rate: 55 %
• Population growth rate: 1.4 %
Social inequalities and health inequity in Morocco
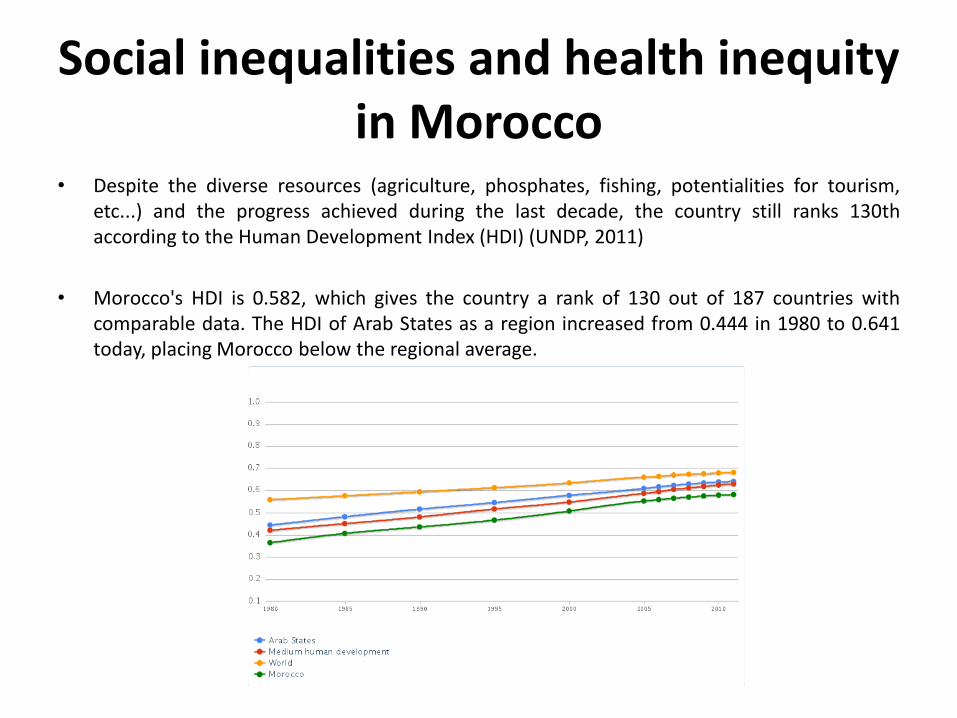
• Despite the diverse resources (agriculture, phosphates, fishing, potentialities for tourism, etc...) and the progress achieved during the last decade, the country still ranks 130th according to the Human Development Index (HDI) (UNDP, 2011)
• Morocco's HDI is 0.582, which gives the country a rank of 130 out of 187 countries with comparable data. The HDI of Arab States as a region increased from 0.444 in 1980 to 0.641 today, placing Morocco below the regional average.

0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
HDI Helth Education Income
HDI
Helth
Education
Income
Social inequalities and health inequity in Morocco
• This unpleasant position is mainly explained by low income, high adult illiteracy, lack of generalized education, and health indicators.
Social inequalities and health inequity in Morocco
• The "National Initiative for Human Development" (NIHD), launched in May 2005 by the King of Morocco, has at last, admitted that many districts and shanty towns, urban or periurban, and a multitude of rural communes live in uncomfortable situations characterized by difficult access to basic social services such as education and health.
• The Moroccan system of health care production is organized into three sectors: – The public health care sector
– The private health care sector
– The non-profit health sector

Health inequity
• In Morocco, until recently, health was considered as a non-productive sector. Indeed, during the last four decades, the budget affected to health represented, on average, 1% of GDP each year and bad governance conducted to an ill-health system.
• By the dawn of the third millennium, only 40% of births are attended by skilled health personnel, many women continue to die during childbirth and infant mortality rate remains relatively high
With these inequities and such an ill-health system, Morocco is facing the double
burden of communicable and non-communicable diseases

NON COMMUNICABLE DISEASES

Cardiovascular Chronic Respiratory Disease
Type 2 Diabetes Cancer
Chronic Diseases result in percent of deaths
4 59
Adult Population

NCD mortality
2008 estimates Males Females
Total NCD deaths (000s) 66.2 59
NCD deaths under age 60 (percent of all NCD deaths) 28.8 23
Age-standardized death rate per 100 000
All NCDs 665.2 523.6
Cancers 90.5 74.5
Chronic respiratory diseases 45.8 29.8
Cardiovascular diseases and diabetes 391.8 319
Behavioural risk factors 2008 estimated prevalence (%) Males Females Total
Current daily tobacco smoking 28.7 0.2 14.0
Physical inactivity … … …
Metabolic risk factors
2008 estimated prevalence (%) Males Females Total
Raised blood pressure 40.7 41.7 41.2
Raised blood glucose 9.8 10.0 9.9
Overweight 41.4 51.7 46.8
Obesity 10.5 21.9 16.4 10.5 21.9 16,4
Raised cholesterol 34.4 37.0 35.7 34.4 37 35/7
Met
abo
lic r
isk
fact
or
tre
nd
s
NCD Morocco Porfiles

Obesity
• The dietary and lifestyle changes in the last two decades, as a part of the nutrition transition, was associated with an increase in overweight, obesity and non-communicable diseases in adult Moroccan population markedly in urban women.
• Considering the high prevalence and the increasing trends, obesity is now considered as a public health problem in Morocco.
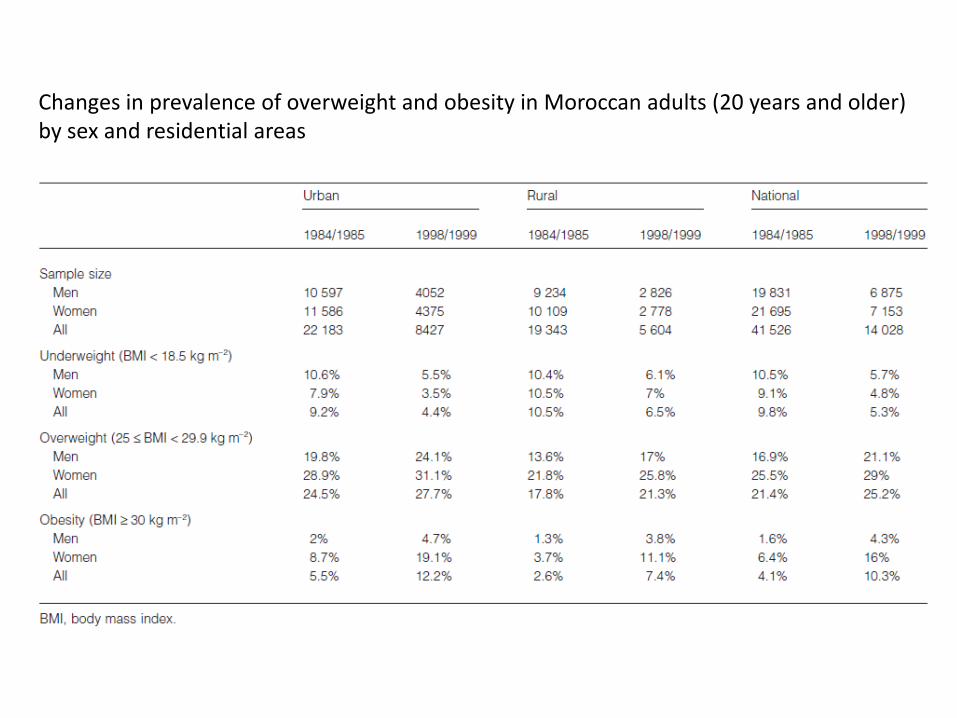
Changes in prevalence of overweight and obesity in Moroccan adults (20 years and older) by sex and residential areas

BMI adults % obese (>=30)
WHO

Obesity and age in Morocco
<25.0 25.0–29.9 >30.0 <25.0 25.0–29.9 >30.0
Men Women
<25
25–34
35–44
45–54
55–64
BMI (kg/m2)
The prevalence of obesity increased with age until 64 years in women, but in men the highest prevalence is between 45 and 54 years of age
K El Rhazi 2010

Obesity and origin area
<25.0 25.0–29.9 >30.0 <25.0 25.0–29.9 >30.0
Men Women
All
Rural
Urban
BMI (kg/m2)
This prevalence of obesity is significantly higher in urban areas than rural areas, but the difference is significant only in women.
K El Rhazi 2010
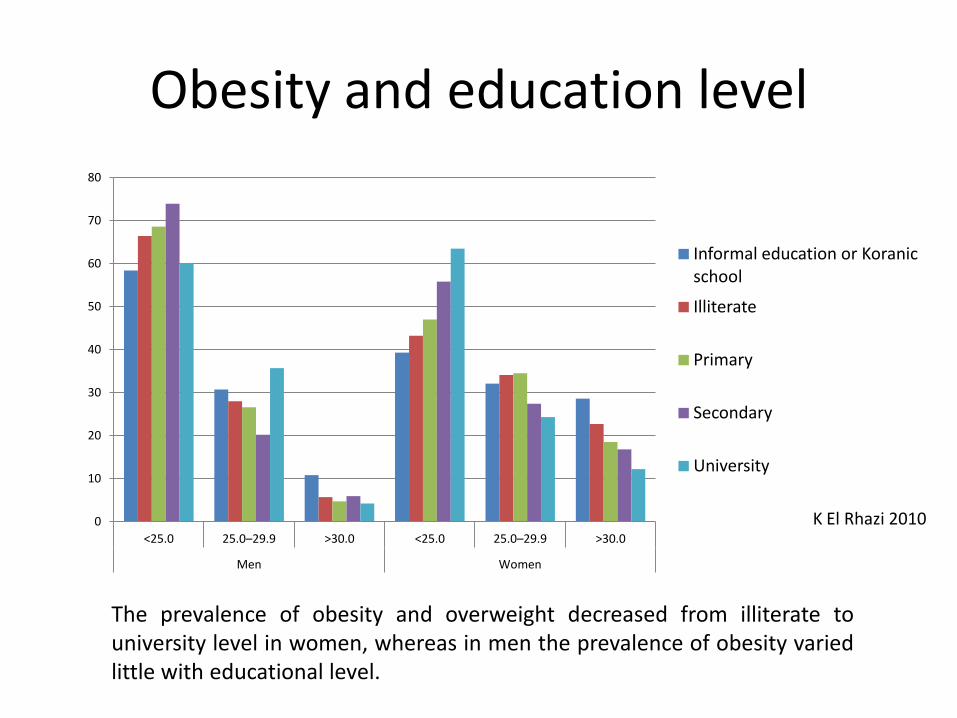
Obesity and education level
0
10
20
30
40
50
60
70
80
<25.0 25.0–29.9 >30.0 <25.0 25.0–29.9 >30.0
Men Women
Informal education or Koranic school
Illiterate
Primary
Secondary
University
The prevalence of obesity and overweight decreased from illiterate to university level in women, whereas in men the prevalence of obesity varied little with educational level.
K El Rhazi 2010

Obesity and Marital status
0
10
20
30
40
50
60
70
80
90
<25.0 25.0–29.9 >30.0 <25.0 25.0–29.9 >30.0
Men Women
Single
Married
Divorced or widowed
• Married women and men had the highest prevalence of obesity. • In both genders, single persons had the lowest prevalence of both
overweight and obesity.
K El Rhazi 2010

Obesity and Occupational activity
0
10
20
30
40
50
60
70
80
90
100
<25.0 25.0–29.9 >30.0 <25.0 25.0–29.9 >30.0
Men Women
Active
Retired
Unemployed
Housewife
Student
Within the five occupational groups and according to sex, retired subjects were more often obese or overweight than those with other occupational activities
K El Rhazi 2010

Obesity and Housing
0
10
20
30
40
50
60
70
80
<25.0 25.0–29.9 >30.0 <25.0 25.0–29.9 >30.0
Men Women
Luxurious or modern
New medina
Old medina
Poor housing or slums
Rural housing
According to housing, the prevalence of obesity and overweight increased with the quality of housing. A higher prevalence was observed among individuals who lived in new or old medina or in luxurious or modern houses than in those who lived in poor housing or in slums.
K El Rhazi 2010

Obesity and Physical activity
0
10
20
30
40
50
60
70
80
<25.0 25.0–29.9 >30.0 <25.0 25.0–29.9 >30.0
Men Women
Yes
No
The prevalence of obesity appeared to be lower among subjects who practised physical activity than in the others
K El Rhazi 2010
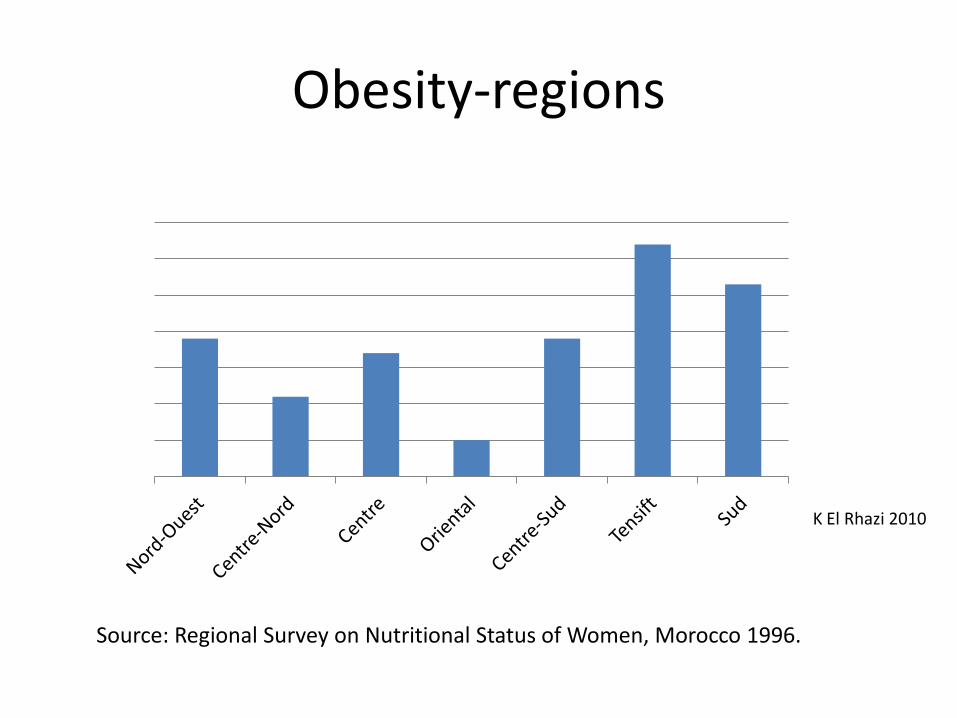
Obesity-regions
Source: Regional Survey on Nutritional Status of Women, Morocco 1996.
K El Rhazi 2010
Obesity: children
• The only available data on overweight are obtained from two previous surveys . The first one is the 1987 national survey conducted on a representative sample of 5982 women and 5559 children based on 5982 households selected randomly by area of residency. The survey data report that among 3292 children under 36 months of age the prevalence of overweight was 3.1% (2.6% for boy and 3.6% for girls), slightly higher in urban (4.3%) than in rural areas (2.5%).
• The other available national survey was conducted in 1992 on a representative sample of 38 770 people including 4502 children based on 6577 households selected randomly by area of residency. Data from this survey show that while undernourishment persists (24% stunting) among children under 5 years, the prevalence of overweight is quite high (9.2%). The prevalence was slightly higher among boys (9.5%) than among girls (8.8%) and higher among urban (10.1%) than among rural children (8.6%).
Possible causes of obesity in Morocco
• Many hypotheses have been proposed to explain the increase of the prevalence of obesity, ranging from the effects of excess of dietary intakes and low physical activity level.
• However, the combination of urban living and an abundant food supply does not provide the entire explanation of obesity in women. It is very likely that the cultural preference for female plumpness coupled with physical and cultural barriers to physical activity makes the difference.
Asthma
• In many regions of the world, notably Africa, there is a paucity of recent information on the epidemiology of asthma.
• Three centres in Morocco (Rabat, Casablanca and Marrakech) participated in the ISAAC survey in 1994-1995. In this survey, twelve-month prevalence rates for wheeze in the 13 14 year old age group were 7.5% in Morocco.
• The ISAAC III study also found that prevalence rates in Africa were around twice as high in urban areas compared to rural areas. A number of older studies conducted in the 1980s in individual centres or regions of all three Maghreb countries identified lower prevalence rates of paediatric asthma, ranging from 2% to 5% 22, although more recent studies revealed rates, ranging from 8% to 10% 22, consistent with the ISAAC study.

* Registre des cancers du Grand Casablanca Année 2004, ALSC 2007
Cancers
• First population registry in Morocco
– Taking place in Casablanca region
– Data of the year 2004
– 30 500 new cases of disease are recorded each year*

LEADING CANCER SITES
• The overall standardized cancer rate is 101.71 new cases per 100,000 inhabitants per year. Cancer affects women more frequently (crude incidence = 100.1) than men (crude incidence = 84.3). This could be explained by the high incidence of breast cancer that accounts for 36% of all cancers in women in Morocco.
• Breast cancer is by far the most common cancer in women, while prostate cancer is the second most commonafter lung cancer in men.
Site Male Female
Morocco 2004 Cases Age Standardized Rate
/ 100000 Cases Age Standardized
Rate / 100000
All sites 1503 100,3 1833 104,2
Breast 662 35,0
Lung 357 25,5 32 2,1
Prostate 124 9,6
Colorectal 105 6,7 94 5,8
NHL 92 6,1 73 4,6
Bladder 84 5,8 10 0,7
Stomach 62 4,1 46 3,0
Uterine cervix 235 13,5

ALL CANCER SITES
• Cancer incidence was substantially on the rise over the age of 40 in both men and women. Between the age of 35 and 54 years the rates in women far exceeded those in men. By contrast in the 60+ age group rates in men were higher than in women.
0.0
50.0
100.0
150.0
200.0
250.0
300.0
0-4 5-9 10-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75+
Male
Female
Age Specific Rate / 100,000 ; All sites combined, 2004
BREAST CANCER (FEMALE)
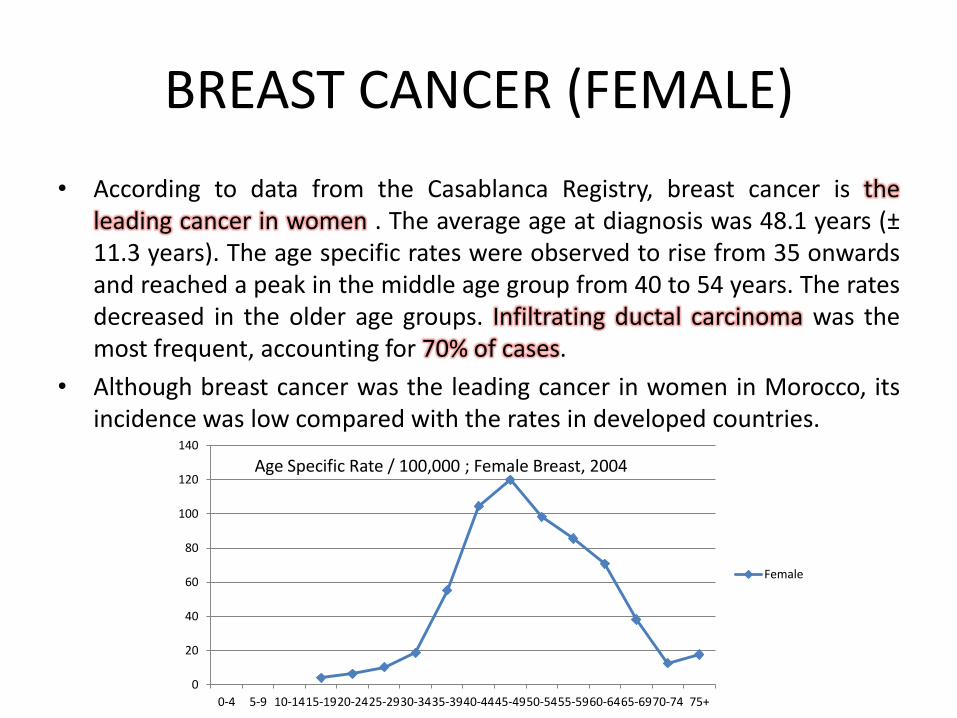
• According to data from the Casablanca Registry, breast cancer is the leading cancer in women . The average age at diagnosis was 48.1 years (± 11.3 years). The age specific rates were observed to rise from 35 onwards and reached a peak in the middle age group from 40 to 54 years. The rates decreased in the older age groups. Infiltrating ductal carcinoma was the most frequent, accounting for 70% of cases.
• Although breast cancer was the leading cancer in women in Morocco, its incidence was low compared with the rates in developed countries.
0
20
40
60
80
100
120
140
0-4 5-9 10-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75+
Female
Age Specific Rate / 100,000 ; Female Breast, 2004
PROSTATE CANCER
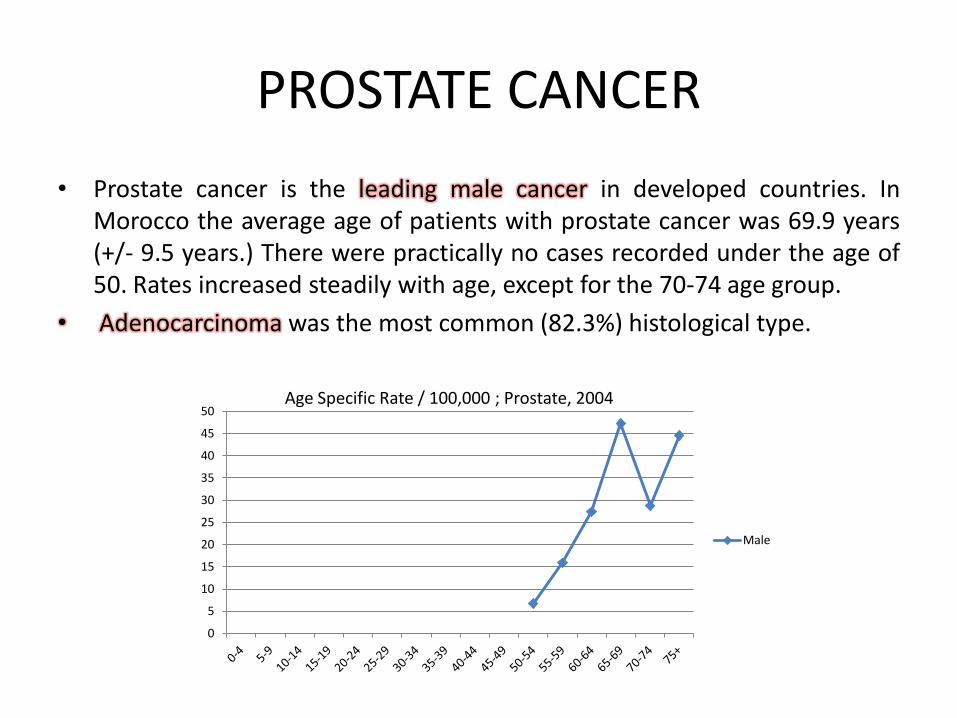
• Prostate cancer is the leading male cancer in developed countries. In Morocco the average age of patients with prostate cancer was 69.9 years (+/- 9.5 years.) There were practically no cases recorded under the age of 50. Rates increased steadily with age, except for the 70-74 age group.
• Adenocarcinoma was the most common (82.3%) histological type.
0
5
10
15
20
25
30
35
40
45
50
Male
Age Specific Rate / 100,000 ; Prostate, 2004
LUNG CANCER
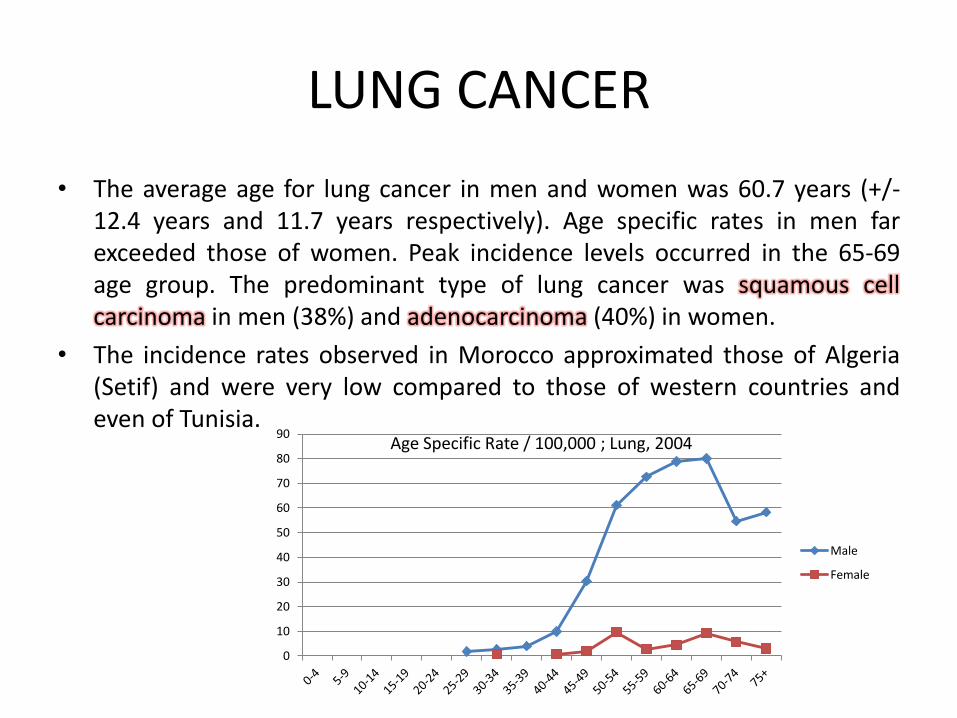
• The average age for lung cancer in men and women was 60.7 years (+/- 12.4 years and 11.7 years respectively). Age specific rates in men far exceeded those of women. Peak incidence levels occurred in the 65-69 age group. The predominant type of lung cancer was squamous cell carcinoma in men (38%) and adenocarcinoma (40%) in women.
• The incidence rates observed in Morocco approximated those of Algeria (Setif) and were very low compared to those of western countries and even of Tunisia.
0
10
20
30
40
50
60
70
80
90
Male
Female
Age Specific Rate / 100,000 ; Lung, 2004

COLORECTAL CANCERS
• The average age of occurrence of colorectal cancers in Morocco was 57 years in women (± 10.6 years) and 56 years in men (± 12.8 years).
• Rates increased after the age of 50 and reached a peak in the 55 to 64 age group in males and in the 60-64 age group in females.
• The incidence of colorectal cancers is comparable to the three Maghreb countries (Morocco, Tunisia and Algeria) and it is low compared to industrialized countries.
0
5
10
15
20
25
30
0-4 5-9 10-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75+
Male
Female
Age Specific Rate / 100,000 ; Colorectal cancers, 2004

URINARY BLADDER CANCER
• The average age of occurrence of bladder cancer was 62.9 years in women (+/- 12.2 years) and about 63.8 years (+/- 13.8 years) in men. Urothelial carcinoma was by far the most frequent histological type (70% in women and 82% in men) while squamous cell carcinoma accounted for 10% of cases in women and 4.8% in men.
0
5
10
15
20
25
Male
Female
Age Specific Rate / 100,000 ; Bladder cancer, 2004
NON HODGKIN’S LYMPHOMA
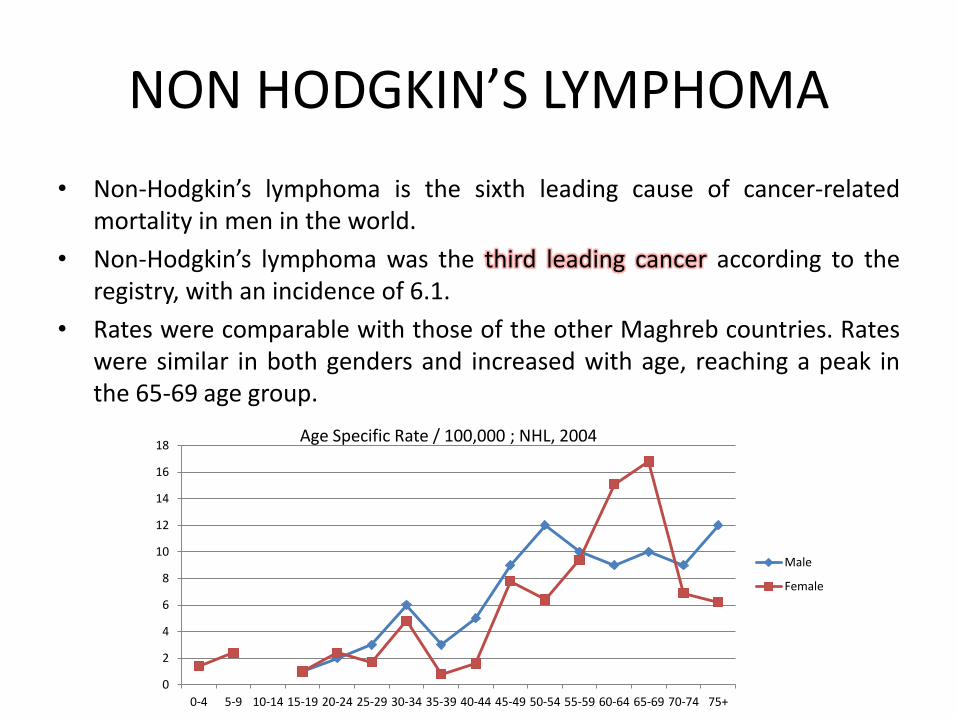
• Non-Hodgkin’s lymphoma is the sixth leading cause of cancer-related mortality in men in the world.
• Non-Hodgkin’s lymphoma was the third leading cancer according to the registry, with an incidence of 6.1.
• Rates were comparable with those of the other Maghreb countries. Rates were similar in both genders and increased with age, reaching a peak in the 65-69 age group.
0
2
4
6
8
10
12
14
16
18
0-4 5-9 10-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75+
Male
Female
Age Specific Rate / 100,000 ; NHL, 2004

UTERINE CERVIX
• Worldwide, cervical cancer is the second most common cancer in women with 500,000 new cases diagnosed each year, 80% of which occur in developing countries. Human Papillomavirus (HPV) infection is the main risk factor.
• The average age of women with cervical cancer in Morocco was 53.5 years (+/-11.8 years). Age specific rates increased after the age of 35 and reached peak incidence levels in the middle age groups.
0
10
20
30
40
50
60
0-4 5-9 10-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75+
Male
Age Specific Rate / 100,000 ; Uterine Cervix cancer, 2004
Incidence rates of selected cancers in North African Countries, compared with the pool of
European Registries Rabat (Morocco) 2005
Casablanca (Morocco) 2004
Sétif (Algeria) 1998–2002
Algier (Algeria) 2006
Northern Tunisia 1999–2003
Sousse (Tunisia) 1998–2002
Sfax (Tunisia) 2000–2002
Benghaz (Libya) 2004 i
Gharbiah (Egypt) 1999–2002
Pool Europe 1998–2002
Men
Average annual population coverage
305,856 1,782,255 684,636 1,478,947 2,382,720 250,500 417,300 832,346 1,857,618 114,072,386
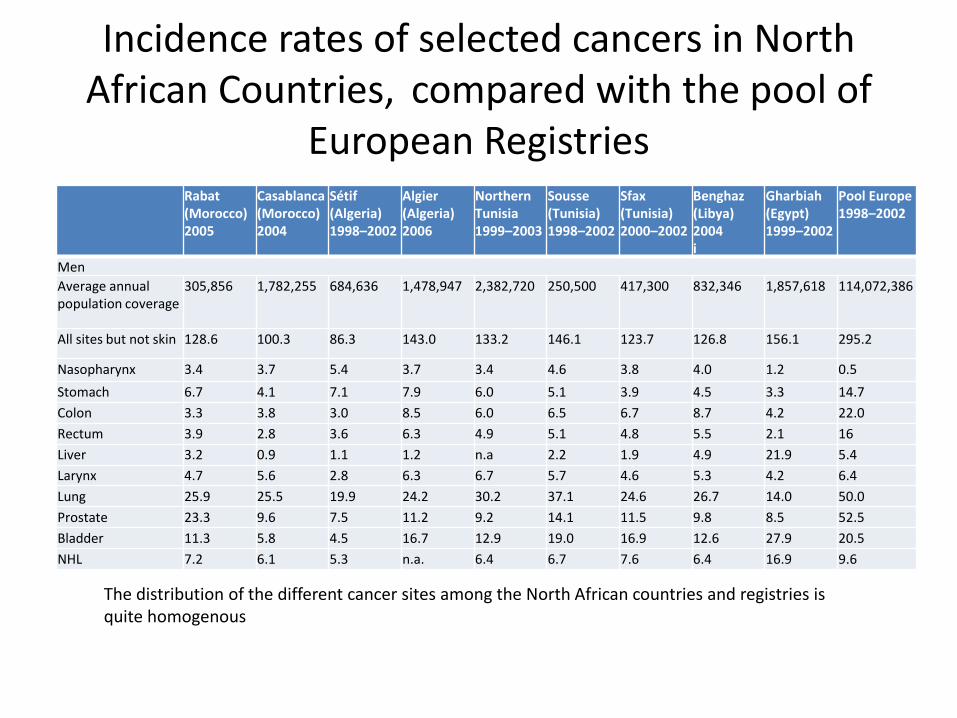
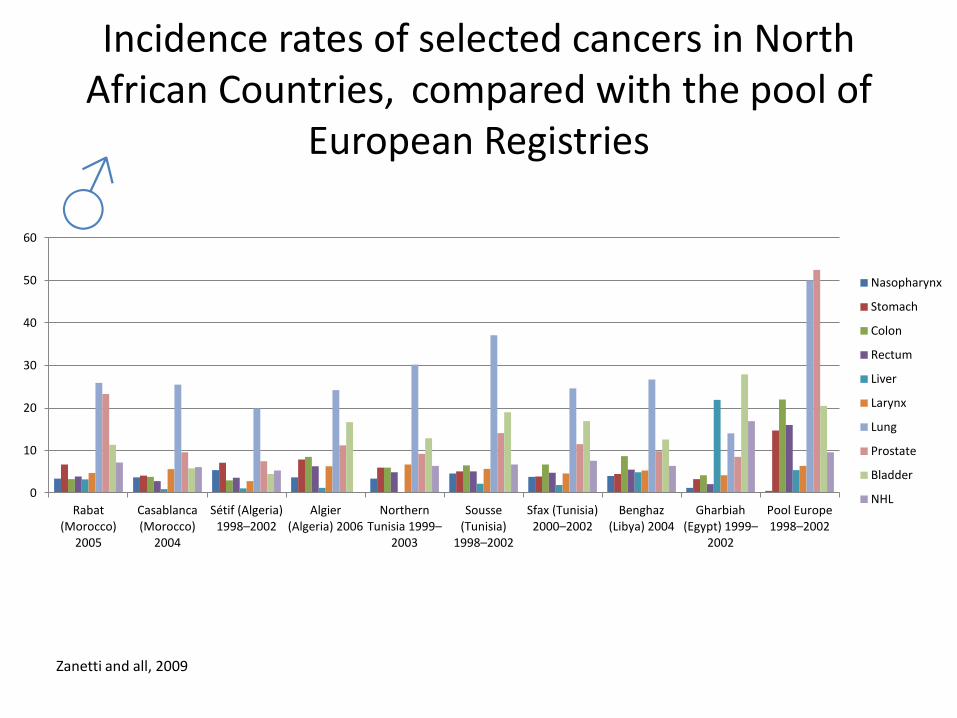
All sites but not skin 128.6 100.3 86.3 143.0 133.2 146.1 123.7 126.8 156.1 295.2
Nasopharynx 3.4 3.7 5.4 3.7 3.4 4.6 3.8 4.0 1.2 0.5
Stomach 6.7 4.1 7.1 7.9 6.0 5.1 3.9 4.5 3.3 14.7
Colon 3.3 3.8 3.0 8.5 6.0 6.5 6.7 8.7 4.2 22.0
Rectum 3.9 2.8 3.6 6.3 4.9 5.1 4.8 5.5 2.1 16
Liver 3.2 0.9 1.1 1.2 n.a 2.2 1.9 4.9 21.9 5.4
Larynx 4.7 5.6 2.8 6.3 6.7 5.7 4.6 5.3 4.2 6.4
Lung 25.9 25.5 19.9 24.2 30.2 37.1 24.6 26.7 14.0 50.0
Prostate 23.3 9.6 7.5 11.2 9.2 14.1 11.5 9.8 8.5 52.5
Bladder 11.3 5.8 4.5 16.7 12.9 19.0 16.9 12.6 27.9 20.5
NHL 7.2 6.1 5.3 n.a. 6.4 6.7 7.6 6.4 16.9 9.6
The distribution of the different cancer sites among the North African countries and registries is quite homogenous
0
10
20
30
40
50
60
Rabat (Morocco)
2005
Casablanca (Morocco)
2004
Sétif (Algeria) 1998–2002
Algier (Algeria) 2006
Northern Tunisia 1999–
2003
Sousse (Tunisia)
1998–2002
Sfax (Tunisia) 2000–2002
Benghaz (Libya) 2004
Gharbiah (Egypt) 1999–
2002
Pool Europe 1998–2002
Nasopharynx
Stomach
Colon
Rectum
Liver
Larynx
Lung
Prostate
Bladder
NHL
♂
Incidence rates of selected cancers in North African Countries, compared with the pool of
European Registries
Zanetti and all, 2009

Incidence rates of selected cancers in North African Countries, compared with the pool of
European Registries Rabat (Morocco) 2005
Casablanca (Morocco) 2004
Sétif (Algeria) 1998–2002
Algier (Algeria) 2006
Northern Tunisia 1999–20037
Sousse (Tunisia) 1998–2002
Sfax (Tunisia) 2000–2002
Benghaz (Libya) 2004 i
Gharbiah (Egypt) 1999–2002
Pool Europe 1998–2002
Women
Average annual population coverage
327,145 1,833,648 680,852 1,455,244 2,318,400 244,300 403,300 799,705 1,807,906 120,739,480
All sites but not skin
109.3 104.2 80.3 164.0 101.4 95.5 89.1 102.4 119.3 227:01:00
Nasopharynx 1.9 0.9 1.7 1.8 1.6 1.9 0.9 1.4 0.4 0.2
Stomach 3.4 3.0 3.1 7.4 3.6 2.5 3.0 2.1 2.0 7.0
Colon 1.8 2.6 2.8 5.9 5.3 6.1 5.3 8.1 2.7 15.6
Rectum 2.8 3.1 3.8 5.1 4.0 2.9 3.8 4.1 1.7 8.4
Liver 1.2 0.5 0.8 0.1 n.a 0.7 0.6 2.5 4.5 2.0
Breast 35.8 35.0 18.8 60.5 29.6 29.8 28.0 23.3 42.5 71.5
Cervix uteri 15.4 13.5 11.6 9.5 5.4 7.1 2.3 3.5 2.1 9.4
Ovary 5.2 5.1 2.1 7.3 3.8 3.3 3.7 3.9 5.1 10.8
Thyroid 4.6 4.8 3.6 8.6 3.7 3.1 3.0 3.9 2.6 5.1
NHL 3.2 4.6 3.8 n.a. 4.0 3.7 4.1 4.5 9.9 6.7

0
10
20
30
40
50
60
70
80
Rabat (Morocco)
2005
Casablanca (Morocco)
2004
Sétif (Algeria) 1998–2002
Algier (Algeria) 2006
Northern Tunisia 1999–
2003
Sousse (Tunisia)
1998–2002
Sfax (Tunisia) 2000–2002
Benghaz (Libya) 2004
Gharbiah (Egypt) 1999–
2002
Pool Europe 1998–2002
Nasopharynx
Stomach
Colon
Rectum
Liver
Breast
Cervix uteri
Ovary
Thyroid
NHL
♀
Incidence rates of selected cancers in North African Countries, compared with the pool of
European Registries
Zanetti and all, 2009

COMMON CANCERS IN MALES
MOROCCO
(Casablanca*)
ALGERIA
(Algiers**)
TUNISIA
(Tunis***)
LYBIA
(Benghazi****)
Lung Lung Lung Lung
Prostate Colon/Rectum Bladder Colon/Rectum
Colon/Rectum Bladder Colon/Rectum Head Neck
NHL Stomach Prostate Bladder
Larynx Prostate Skin Prostate
* Registre des Cancers de la région du Grand Casablanca Edition 2004
** Registre des tumeurs d’Alger Edition 2003
*** Registre des Cancers de Nord Tunisie 1999-2003
**** Benghazi Cancer Registry 2004

COMMON CANCERS IN FEMALES
MOROCCO
(Casablanca*)
ALGERIA
(Algiers**)
TUNISIA
(Tunis***)
LYBIA
(Benghazi****)
Breast Breast Breast Breast
Cervix uteri Colon/Rectum Colon/Rectum Colon/Rectum
Thyroid Cervix uteri Skin Corpus uteri
Colon/Rectum Thyroid Cervix uteri NHL
Ovaries Ovaries
Thyroid Cervix uteri
* Registre des Cancers de la région du Grand Casablanca Edition 2004
** Registre des tumeurs d’Alger Edition 2003
*** Registre des Cancers de Nord Tunisie 1999-2003
**** Benghazi Cancer Registry 2004

• The four Maghreb countries and Egypt are quite comparable in their demographic, economic and socio-cultural aspects, and, therefore, the similarities in cancer patterns are not surprising.
• They are coherent with what is known about the potential risk and protection factors distribution in the region: low industrialisation, traditional control of infectious diseases, Mediterranean diet, compliance with religious prohibitions (notably for alcohol, and, at a lesser extent, for tobacco), sexual and reproductive behaviours.

Challenges
• Lack of enough national policies for NCD prevention and control
• Poor Fundings
• Re orientation of the health system from acute to chronic diseases.
• Dealing with NCDs is beyond the capacity of the health sector alone. Necessary interventions should come from other sectors, e.g. ministries of industry, commerce, agriculture, justice, etc.
• Dealing with NCDs is beyond the capacity of the health sector alone. Necessary interventions should come from other sectors, e.g. ministries of industry, commerce, agriculture, justice, etc.

Thank you