enteral nutrition in adults - mims.com malaysia
TRANSCRIPT

20 JUNE ISSUE
PHARMACY PRACTICE
Enteral nutrition in adults
Malaysians love food. We often greet our friends by asking have you eaten to-
day? Our beauty pageant contestant wore a nasi lemak inspired dress during the Miss Universe 2017 competition in Las Vegas, and because of our love for food and overnutrition, Malaysia is now known as the most obese country in Asia . However, our love for food does not extend to some of the disadvan-taged social groups particularly those having serious illnesses. Malnutrition has been found to affect 14 to 61.9% of adult cancer, surgical, geriatrics and paediatric patients in major Malaysian hospitals.1,2,3,4
Enteral nutrition support Enteral nutrition (EN) is also known as tube feeding. It is the nutrition provided through the gastrointestinal (GI) tract via a tube, catheter, or stoma that delivers nutrients distal to the oral cavity.5,6
EN is part of the nutrition support and an adjunctive management for pa-tients with certain diseases. The pro-vision of nutrition support must be a team effort. Healthcare providers in this
team include doctors, dietitians, nurses and pharmacists. Community pharma-cists should also see themselves as an important team member.
Although individualized nutri-tion care plan is often designed and planned in a hospital, many patients still require EN after discharge, especially those who cannot achieve sufficient oral intake to meet their basic nutrient requirements and those who have a partially functioning GI tract.
Pharmacists who work in a com-munity pharmacy setting can help in carrying out a discharge plan more ef-fectively and ensure the safe transition of these patients from hospital to home to reduce rehospitalization. They can assist family members in their purchase of the correct specialized formula and equipment used for EN administration.
Besides, pharmacists are trained in providing information to family mem-bers on interpreting EN content and health claims, identifying drug-nutrient interactions and unusual nutrient de-ficiencies, as well as ensuring that the
Hoo Yee YinClinical Pharmacist
Surgical and Cardiology Department
Hospital Serdang
Earn 1 CPD pointevery month!
Filler_ads_4C_206x276mm.pdf 1 22/5/17 5:37 pm

22 JUNE ISSUE
PHARMACY PRACTICE
formulations are properly prepared and administered.
Enteral nutrition formulations and clinical applicationEnteral formulas are available in ready-to-drink liquid and powder formulas and may be classified as standard, el-emental or specialized. There are many products under each category and the number of products continues to grow.
The usual components of an EN for-mula include carbohydrates, proteins, fats, vitamins, minerals and fluids while the ingredients include water, cow’s milk, milk-based whey and casein, milk protein concentrates, soybean, wheat, sugar, corn syrup, salt, vegetable oil, vitamin mineral mix, artificial flavour and many other ingredients, depending on the manufacturer. The common differ-ences between each category include osmolarity, caloric density, protein con-tent, fibre content, electrolytes, vitamins and mineral content.7,8,9,10
a) Standard formulaThe standard formula is also known as polymeric formula or complete formula. It is the most common enteral product in the market and suitable for most pa-tients. They are easily available and can usually be purchased at a lower cost compared to elemental and specialized formulas. Examples include Ensure®, Nutren Optimum®, Enercal Plus®, Cal-co®, Promaxe®, etc.8,9,10
These formulas are deemed com-plete because they contain proteins, fats, carbohydrates; all essential vi-tamins, minerals, and trace elements which provide 100% of dietary refer-ence intakes at a specific volume (usu-ally at 1.5 to 2 L)7 or when approximate-ly 1000 or more kilocalories (kcal) are delivered to a patient per day.11 A stan-dard formula can be used as an individ-ual’s sole source of nutrition if taken in an appropriate amount.
The standard formula is used in patients who are unable to take nutri-
ents through the oral route but have a functional GI tract with sufficient length and absorptive capacity.6 As the formu-la contains whole proteins, the patient’s digestive system must be able to break the whole proteins into smaller mole-cules for absorption into the body. Ex-amples of these patients include those suffering from dysphagia due to stroke, cancer, paralysis, severe rheumatoid arthritis, muscular dystrophy, neuro-logic disease, multiple sclerosis, end-stage Parkinson’s disease, oesopha-geal diseases, head or facial trauma, coma and other diseases which cause patients to have difficulty in chewing, swallowing or transporting normal food to the stomach.7,8,9,10
Most standard formulas provide 1.0 to 1.2 kcal/mL and protein content of 40 to 50 g/L. Ready-made concentrat-ed formulas at 1.5 to 2.0 kcal/mL are also available for patients who require fluid restriction or higher energy (Osmo-lite 1.5®, Jevity 1.5®, Supportan®).
Alternatively, carers for fluid-restrict-ed patients can also reduce the water volume upon mixing the formula pow-der to achieve higher calorie density, usually from 1.0 kcal/mL to 1.5 kcal/mL. However, carers need to be aware that reducing the water content may re-sult in a more viscous solution.11
Fibre content can also be used to subdivide standard formula. Examples of fibre-enriched formulas include Nu-tren Fibre®, Ensure®, and Calco® which have oligosaccharides, fructo-oligosac-charides (FOS), and inulin respectively in their products. These fibre or carbo-
hydrate compounds are not digested and can be used as prebiotics where they are fermented by the microorgan-isms in the GI tract.12
A meta-analysis conducted in a review showed that fibre supplementa-tion in EN reduces diarrhoea incidence by increasing the bulk, holding water and improving GI tract barrier function. However, the prebiotics effect is still controversial and cannot be concluded due to conflicting evidence.13
b) Elemental and semi-elemental formulaElemental and semi-elemental formula are oligomeric formulas with a caloric density of 1 to 1.5 kcal/mL. They are extensively or partially hydrolyzed for-mulas, providing the simplest form of nutrients for absorption, whereby the protein content present as short-chain peptides in semi-elemental formula, and free amino acids in elemental for-mula; carbohydrate as monosaccha-rides, and these formulas have higher amounts of medium-chain triglycerides (MCT) oil to facilitate absorption.
Examples of semi-elemental formu-las include Peptamen®, Peptamen Ju-nior® and Semital®, while examples of elemental formulas include Neocate®, and Comidagen®. These formulas are usually better tolerated when compared to the standard formulas because it by-passes hydrolysis of the intact protein, complex carbohydrates and fat emulsi-fication, thus they may be chosen to be used initially in tube feeding in certain patients and subsequently, transition-ing to standard formulas when they are more stable.9,11,15
The cost of pre-digested formulas is usually higher and they are less palat-able. They offer little additional benefits unless there is extensive impairment of the GI digestive and absorptive func-tions. The formulas may be beneficial in patients who cannot tolerate standard formulas, have persistent diarrhoea, delayed gastric emptying, malabsorp-
A standard formula can be used as an individual’s sole source of nutrition if taken in an appropriate amount.

23 JUNE ISSUE
PHARMACY PRACTICE
tion due to cystic fibrosis, pancreatic insufficiency (pancreatitis, pancreatic cancer, pancreatic injury and fistula)7,9,15 or short bowel syndrome (SBS) result-ing from surgical resection, congenital defect, disease-associated loss of ab-sorption when on a conventionally ac-ceptable, normal diet.14
c) Specialized formulaThe specialized formulas can be used in patients with specific disease states or organ dysfunction; however, these formulas are more expensive and lack improvement in clinical outcomes. Some of the examples of specialized formulas include EN for patients with diabetes, renal failure, hepatic failure, critical illness and cancer.
Glucose control for patients with diabetes and receiving EN is always a challenge because hyperglycaemia is associated with infection, poor wound healing, dehydration and poor pa-tient outcomes while hypoglycaemia increases mortality.16,17 Some of the marketed diabetes-specific formulas include Nutren Diabetic® and Glucer-na®. These products are usually slightly higher in fibre, fat (32–50% of energy), lower in carbohydrate (35–40% of ener-gy) or have carbohydrate that are more slowly digested and absorbed, with 15-20% protein content8,9,17, compared to standard formulas which are higher in carbohydrate (49 – 53%), low in fat (29 – 30%) and fibres.11,17
A meta-analysis showed that dia-betes-specific formulas result in signifi-cantly lower postprandial rise in blood glucose concentrations, lower peak blood glucose concentrations and re-duced insulin requirements. However, there was no significant difference in fasting blood glucose and the higher proportion of mono-unsaturated fatty acid (MUFA) does not significantly re-duce serum cholesterol concentration (total cholesterol, HDL, TG, LDL) when compared to standard formulas but the higher fat content had no detrimental effect on cardiovascular diseases.17,18
Next, protein-energy wasting (PEW) is common in chronic kidney disease (CKD) patients especially those under-going maintenance dialysis and it is the strongest predictors of mortality. Pa-tients are usually diagnosed with PEW if they are presented with low serum levels of albumin, pre-albumin, or cho-lesterol; reduced total body fat, weight loss, decrease in muscle mass and low protein or energy intakes.19 If left un-treated, PEW may cause cachexia and sarcopenia which may increase the risk of death from recurrent infections, car-diovascular or cerebrovascular disease, possibly due to vascular endothelial damage.20
Improving nutritional status is an important component of CKD patients. The recommended dietary energy in-take for patients undergoing haemodi-
alysis and peritoneal dialysis is 30–35 kcal/kg per day, mean dietary protein intake is 1.2 g/kg per day in patients on haemodialysis and 1.3 g/kg per day in patients on peritoneal dialysis.20 Specialized enteral formulas designed for kidney failure include Nepro®, Re-no-Pro®, Novasource Renal® which have lower sodium, potassium, magne-sium and phosphorus content as well as higher caloric concentrations (1.8 to 2.0 kcal/mL), that may help to improve patients’ health outcome and survival.
Patients with cancer are at high risk for malnutrition due to the disease and its treatment. Malnutrition in these patients can cause adverse impacts on response to treatment, prognosis, and survival. Even though most cancer patients can be appropriately fed by a standard diet; when regular food intake
Feeding routesthrough the nose(or alternatively may be oral)1. Nasogastric2. Nasoduodenal3. Nasojejunal
Gastrostomy options*• Percutaneous endoscopic gastrostomy (PEG)• Percutaneous radiologic gastrostomy (PRG)• Percutaneous endoscopic jejunostomy (PEJ)• Percutaneous radiologic jejunostomy (PRJ)• Percutaneous endoscopic gastrojejunostomy (PEG/J)• Button• Surgically placed gastrostomy
Nasal cavity
Nasogastric(NG) tube
Esophagus
Stomach
Largeintestine
Smallintestine
Jejunostomy
* Gastrostomy and jejunostomy tubes may be placed endoscopically, radiologically or surgically.
3
2
1
Figure 1: Possible routes of enteral feeding.
(Adapted from: http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/
gastroenterology/principles-of-nutrition-support/)
24 JUNE ISSUE
PHARMACY PRACTICE
is reduced, oral nutritional supplements may be used.
There is a simple formula used for the calculation of the energy required when it is difficult to estimate the total energy expenditure. We can target 25 to 30 kcal/kg/day with 1.2 to 1.5 g pro-tein/kg/day to help maintain or restore lean body mass in these patients.21 Some enteral formulas which contain immune modulators such as fish oil, arginine, glutamine, selenium, and an-tioxidants have been shown in various studies to improve quality of life and physical function in cancer patients. Examples of EN with high calories and containing fish oil include Prosure® and Supportan®.8,21
d) Medical nutrition supplementsThere are some modular products avail-able in the market providing single nu-trient to enhance the protein, carbohy-
drate, fat, or fibre content of the enteral regimen. These supplements cannot be used as a sole source of nutrition, and they are given separately with en-teral formulas. Examples include Ener-sos MCT oil®, which provides a good source of calories via median chain tri-glycerides (8.3 calories per gram); Val-ens Myotein® which provides additional protein to help patients to achieve their protein requirements; Valens Thixer® which is a thickening agent to help to decrease swallowing difficulties in post-stroke patients.
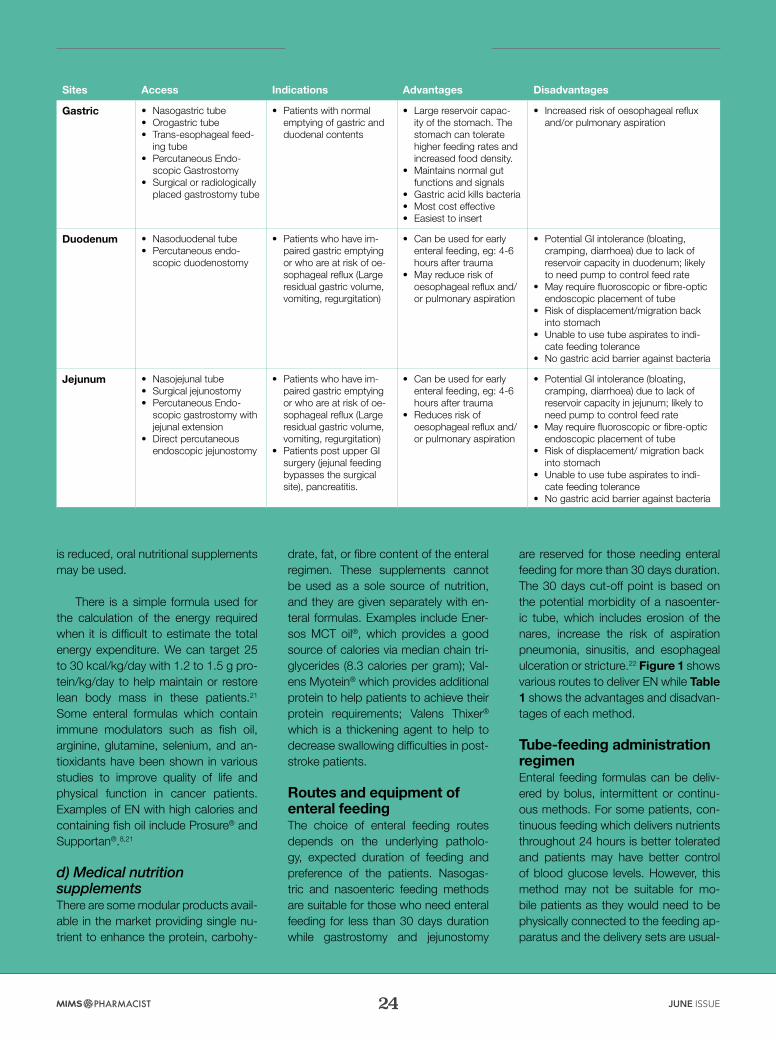
Routes and equipment of enteral feeding The choice of enteral feeding routes depends on the underlying patholo-gy, expected duration of feeding and preference of the patients. Nasogas-tric and nasoenteric feeding methods are suitable for those who need enteral feeding for less than 30 days duration while gastrostomy and jejunostomy
are reserved for those needing enteral feeding for more than 30 days duration. The 30 days cut-off point is based on the potential morbidity of a nasoenter-ic tube, which includes erosion of the nares, increase the risk of aspiration pneumonia, sinusitis, and esophageal ulceration or stricture.22 Figure 1 shows various routes to deliver EN while Table 1 shows the advantages and disadvan-tages of each method.
Tube-feeding administration regimenEnteral feeding formulas can be deliv-ered by bolus, intermittent or continu-ous methods. For some patients, con-tinuous feeding which delivers nutrients throughout 24 hours is better tolerated and patients may have better control of blood glucose levels. However, this method may not be suitable for mo-bile patients as they would need to be physically connected to the feeding ap-paratus and the delivery sets are usual-
Sites Access Indications Advantages Disadvantages
Gastric • Nasogastric tube • Orogastric tube• Trans-esophageal feed-
ing tube• Percutaneous Endo-
scopic Gastrostomy • Surgical or radiologically
placed gastrostomy tube
• Patients with normal emptying of gastric and duodenal contents
• Large reservoir capac-ity of the stomach. The stomach can tolerate higher feeding rates and increased food density.
• Maintains normal gut functions and signals
• Gastric acid kills bacteria • Most cost effective • Easiest to insert
• Increased risk of oesophageal reflux and/or pulmonary aspiration
Duodenum • Nasoduodenal tube • Percutaneous endo-
scopic duodenostomy
• Patients who have im-paired gastric emptying or who are at risk of oe-sophageal reflux (Large residual gastric volume, vomiting, regurgitation)
• Can be used for early enteral feeding, eg: 4-6 hours after trauma
• May reduce risk of oesophageal reflux and/or pulmonary aspiration
• Potential GI intolerance (bloating, cramping, diarrhoea) due to lack of reservoir capacity in duodenum; likely to need pump to control feed rate
• May require fluoroscopic or fibre-optic endoscopic placement of tube
• Risk of displacement/migration back into stomach
• Unable to use tube aspirates to indi-cate feeding tolerance
• No gastric acid barrier against bacteria
Jejunum • Nasojejunal tube• Surgical jejunostomy • Percutaneous Endo-
scopic gastrostomy with jejunal extension
• Direct percutaneous endoscopic jejunostomy
• Patients who have im-paired gastric emptying or who are at risk of oe-sophageal reflux (Large residual gastric volume, vomiting, regurgitation)
• Patients post upper GI surgery (jejunal feeding bypasses the surgical site), pancreatitis.
• Can be used for early enteral feeding, eg: 4-6 hours after trauma
• Reduces risk of oesophageal reflux and/or pulmonary aspiration
• Potential GI intolerance (bloating, cramping, diarrhoea) due to lack of reservoir capacity in jejunum; likely to need pump to control feed rate
• May require fluoroscopic or fibre-optic endoscopic placement of tube
• Risk of displacement/ migration back into stomach
• Unable to use tube aspirates to indi-cate feeding tolerance
• No gastric acid barrier against bacteria
Table 1: Advantages and disadvantages of different sites of enteral feeding.23, 24

Filler_ads_4C_206x276mm_Non-MSE.pdf 2 22/5/17 5:47 pm

26 JUNE ISSUE
PHARMACY PRACTICE
ly more expensive.23,24
Going home with a tube and con-nected to the pump whole day long, and the need to adapt to a different sleeping pattern while attached to a continuous feeding pump may not be a good idea unless it is necessary.
Intermittent feeding is commonly used in a hospital setting. This method allows greater patient mobility as feed-ing is stopped for 4 to 16 hours either during daytime or night time. This is often used during the transition period from tube feeding to oral intake or from continuous feeding to bolus feeding. In order to deliver the same amount of EN in a shorter period of time, patients may sometimes experience reflux, aspi-ration, abdominal distension, diarrhoea and nausea using this feeding meth-od.24
In conscious, mobile patients, bolus feeding is usually used. Patients and carers can organize their daily activi-ties as feeding time is reduced and this method is similar to a typical eating pat-tern. Bolus feeding is administered to the stomach as it has a larger reservoir. 100 to 400 mL of EN is usually given over 15 to 60 minutes at a regular inter-val. Although the cost of the equipment
involved may be lower compared to the two methods mentioned above, bolus feeding has the highest risk of intoler-ance.23,24
Potential complications of enteral feedingAfter the placement of the feeding tube, patients should be regularly monitored to prevent complications. Complica-tions can be divided into mechanical, GI and metabolic. Mechanical complica-tions are procedure related. For exam-ple, during nasogastric and nasojejunal tube insertion, patients may experience nasal, pharyngeal, esophageal irritation or erosion, epistaxis (bleeding from the nose), sinusitis, feeding tube malposi-tion or dislodgement. The experience of the personnel who insert the tubes and the quality of feeding tubes may affect the outcomes. Polyvinylchloride (PVC) tubes are the cheapest but they are more rigid while silicone, latex or polyurethane tubes are costlier but they are more flexible and thus causing less trauma on the mucosal surface.25
On the other hand, after gastros-tomy or jejunostomy tube insertion, increased leakage, enlarging stoma around the percutaneous tube site, skin infection, fistula, gastric ulcer and bur-ied bumper syndrome (partial or com-
plete overgrowth of the gastric muco-sa, covering the internal fixation device which can lead to tube dysfunction, gastric perforation, bleeding, peritonitis or death) can happen at a later stage.
Carers should monitor the access site, clean the area daily with mild soap and water as well as maintain the cor-rect positioning of the external fixation device. If there is increase drainage or infection causing severe skin injury, referral to a doctor is necessary as a course of broad-spectrum antibiotics orally or through the tube in addition to high dose of acid suppression may be needed. Occasionally, the tube may need to be removed.22,25
GI complications such as aspiration and diarrhoea are frequently associat-ed with enteral feeding. Aspiration can cause hypoxia and pneumonitis if the aspirated volume is large. It can be re-duced by keeping patients in an upright position with backrest elevation of 30 to 45 degrees during feeding, reducing feeding rate, giving more concentrated EN and administering gastric motility agents to promote gastric emptying. Moreover, good oral hygiene and using chlorhexidine mouthwash may reduce the risk of aspiration pneumonia if aspi-ration does occur.11,23
In the past, withdrawal of gastric content through the feeding tube using a syringe to check the gastric residual volume (GRV) in the stomach, is used in the hospital to check for feeding tol-erance to prevent aspiration. Greater than 500 mL GRV may warrant a tem-porary withhold in feeding.23 However, recent guidelines showed that the use of GRV as a monitor increases the likeli-hood of tube clogging and the sensitivi-ty to detect aspiration is poor. Thus, the experts advocate that GRV should not be routinely used at home.22
Diarrhoea is also a common com-plication. In most cases, the precise mechanism is usually not known and diarrhoea is often self-limited. If diar-

27 JUNE ISSUE
PHARMACY PRACTICE
rhoea occurs, EN does not need to be withheld and should be continued while investigating the cause factors. Some of the contributing factors include med-ications, infections, enteral feeding equipment contamination, predispos-ing illnesses, altered GI anatomy and nature of enteral feeding.22
There are many medications which can cause diarrhoea as shown in Ta-ble 2 beside. Identifying the causative agents can be challenging in real prac-tice especially in patients taking multi-ple medications. However, reviewing the onset of symptoms relative to when the medications were started can be helpful. Drug-induced diarrhoea can be managed by withdrawing or reducing the dose.26,27,31
In cases where diarrhoea persists and the underlying cause cannot be identified, the EN formula is to be re-viewed. A fibre-enriched feeding for-mula can be considered if the current formula does not contain fibre or try a fibre-free formula if the diarrhoea is oc-curring with a fibre-enriched formula, or change to an elemental formula tempo-rarily.23
Metabolic complications of EN in-clude hyperglycaemia, electrolyte and fluid imbalance. Discharged patients who have not reached their EN feed-ing target goal should have their blood glucose and electrolytes checked two to three times during the first week, then gradually decrease to weekly for 2 to 3 weeks after their EN has reached the target goal. Fluid input and output should be monitored daily especially in patients who are unable to recognize thirst or voluntarily adjust their fluid in-take. Dehydration can be assessed by skin turgor, dry mucosa, reduced urine output and very yellow or dark urine.7,23
In patients with diabetes, nutritional provision should not be compromised to control blood glucose levels. Pa-tients on EN may require insulin sliding scale during hospitalization and return
to prehospitalization treatment regimen (oral agents) after discharge. Thus, their glucose levels may still need adjust-ment following the change in EN needs. Diabetes management goal needs to be individualized considering the risk of hypoglycaemia and life expectan-cy. In general, blood glucose target is the same with the general population, except for terminal patients whereby there is no benefit of glycaemic control except to avoid symptomatic hypergly-caemia.28,29
Nutrition monitoring is also import-ant. For stable patients receiving long term EN, serum albumin, total protein, and prealbumin can be monitored once or twice yearly.7 Patients’ body weight, lean tissue, and adipose tissue stores should also be monitored at baseline and then at the frequency ranging from once a week to every 2 months in lon-ger term care. Patients with good nutri-tional status should not have the tem-
poral region (sides of the forehead) sink and indent inward; and their bony area: clavicle, shoulder, scapula, should not protrude prominently.23
Medications and enteral nu-trition by tubeThe external diameter of the feeding tube or catheter is often measured using French unit. It is abbreviated as Fr, Fg, FR or F. A value of 1 ‘French’ is approximately 0.33 mm. The small-er number is indicative of a smaller diameter and vice versa. Nasogastric or nasojejunum tube is usually smaller, ranging from 8 to 12 Fr whereas larger tubes which can be used for multiple functions (eg, feeding, aspiration and gastric suction), usually range from 12 to 16 Fr. The length of tubing is also different depending on the exit sites. A nasogastric tube is usually 90 to 100 cm long while nasojejunum tube may be 150 cm in length. In contrary, gas-
Types of diarrhoea Mechanism Possible medications /inactive ingredients
Osmotic diarrhoea Diarrhoea develops when an osmotically active substance is ingested, drawing water and ions into the intestinal lumen.
Enteral nutrition, acarbose, ampicillin, clindamycin, magne-sium-containing antacids, potassi-um and phosphorus supplements, methyldopa, quinidine, propanolol, ACE inhibitors, sorbitol, polyeth-ylene glycol
Secretory diarrhoea Diarrhoea could result either by inhibiting electrolyte and nutrient absorption or by increasing the secretion of electrolytes into the intestinal lumen.
Digoxin, amoxicillin-clavulanate, carbamazepine, colchicine, laxatives, metformin, NSAIDs, ticlopidine
Motility diarrhoea Diarrhoea could result either by hypermotility and shortened transit time or hypomotility and stasis, which can result in small bowel bacterial overgrowth.
Cisapride/metoclopramide/tegaserod, irinotecan, macro-lides (erythromycin), ticlopidine, thyroid hormones (levothyroxine), colchicine.
Inflammatory diar-rhoea
Drug-induced inflammatory diar-rhoea by causing direct mucosal damage, disruption of epithelial integrity and vascular compro-mise. In such cases, absorption of water occurs ineffectively and diarrhoea results.
Antibiotics (clindamycin, amoxi-cillin, ampicillin, cephalosporins), carbamazepine, chemotherapeu-tic agents (5-fluorouracil, metho-trexate, irinotecan, cisplatin, doxo-rubicin), lovastatin, pravastatin, simvastatin, isotretinoin, NSAIDs, olmesartan, proton-pump inhibi-tors (pantoprazole, lansoprazole, omeprazole and esomeprazole), rituximab, selective serotonin receptor inhibitors (paroxetine, sertraline), ticlopidine, laxatives.
Table 2: Drug-induced diarrhoea.26,27,31

28 JUNE ISSUE
PHARMACY PRACTICE
trostomy and jejunostomy tubes may range from 10 to 20 Fr depending on the preference of the person inserting them. Tubes with a smaller diameter is more acceptable by patients and more comfortable to use but they get clogged more often. Other than the diameter of tubes, inappropriately pre-pared medications, poor flushing tech-nique and bacterial colonization within the feeding tubes can also cause tube blockage.25,30
As patients receiving EN also re-ceive medications using the same tube, interactions among drugs, feed, and gastric acid; alteration of medication pharmacokinetics and pharmacody-namic profiles can occur. Pharmacists can help to review patients’ medica-
tions. Oral administration of medications is still the preferred route of admin-istration unless a strict nil by mouth status is required. As solid dos-age forms require more preparation steps, when-ever possible, an alter-native route of adminis-tration such as injection, patches, sublingual or depot injections is pre-ferred.
For medications only available in oral form, the pharmacist should en-sure that all prescribed medications are suitable for administration via a feeding tube and pref-erably in liquid forms, effervescent, dispers-ible tablets, where avail-able. For tablets, carers should also ensure they are crushed well and dis-solved completely, to be given together with plenty of boiled and cooled wa-ter or sterile water before and after administering medications. Generally,
15 to 30 mL water flush using a 50 mL syringe is recommended to prevent in-teractions between EN and the drugs. The routine uses of pancreatic enzyme and low pH drinks such as carbonat-ed drinks and cranberry juice have not been shown to be superior to warm water in preventing tube occlusion while low pH drinks may exacerbate tube occlusion by causing EN to coag-ulate or protein to denature.22,30
Other relevant practical skills in-clude choosing medications which only require once daily dosing and are not enteric-coated or modified release tablets. Do not crush enteric-coated or modified release tablets. The use of en-teric-coated tablets is not recommend-ed for the nasogastric route although it
is also not harmful; as the crushing of the coating may cause the drug to be degraded in the acidic environment, re-sulting in reduced absorption and low-ering of the efficacy of the drug.
Meanwhile, crushing modified re-lease or long acting tablets can result in the release of the entire daily dose immediately hence can cause some serious consequences in patients.30 Some of the medications which are often overlooked by clinicians include felodipine extended-release tablets, pantoprazole tablets, and potassi-um chloride extended-release tablets where they can be changed to am-lodipine immediate-release tablets, es-omeprazole tablets (Nexium®) and po-tassium chloride mixture respectively.
Pharmacists should also review non-essential medications and dis-cuss with the primary medical team to make adjustments. For example, medications causing a reduced level of consciousness, vomiting, or delayed gastric emptying (eg, antipsychotics, anticholinergics, opioids) should be re-viewed and stopped if it is not essen-tial.23 Carers should also be informed of the proper administration method for medications which is required to be given on empty stomachs such as phe-nytoin, levodopa, levothyroxine, warfa-rin, itraconazole, and fluoroquinolones. Feeding should be withheld 1 hour before and after drug administration. Phenytoin and theophylline levels need to be monitored closely and dosages adjusted accordingly when EN is start-ed or stopped. Besides, drugs such as methyldopa and levodopa which re-quire active transport systems used for nutrients, will have reduced absorption if given concurrently with a high protein diet.23,30
In conclusion, all healthcare profes-sionals should not underestimate the complexity of EN feeding and should be vigilant and work as a team in provid-ing appropriate EN to a diverse patient population across various settings.
29 JUNE ISSUE
PHARMACY PRACTICE
To answer the quiz for your CPD points, please go to www.mims-cpd.com.my
References: 1. Norshariza J, Siti F, Aini Z, et al. Prevalence of malnutrition among hospitalised adult cancer patients at the National Cancer Institute, Putrajaya, Malaysia. Malaysian Journal of Nutrition. 2017;23(2):161-74. 2. Nur Fazimah S, Sakinah H, Rosminah M. Hospitalized Geriatric Malnutrition: A Perspective of Prevalence, Identification and Implications to Patient and Healthcare Cost. Health and the Environment Journal 2013;4(1):55-67. 3. Shahar S, Wong SF, Chik WC. A prospective study on malnutrition and duration of hospitalisation among hospitalised geriatric patients admitted to surgical and medical wards of Hospital Universiti Kebangsaan Malaysia. Malaysian Journal of Nutrition. 2002;8(1):55-62. 4. Lee WS, Ahmad Z. The Prevalence of Undernutrition upon Hospitalization in Children in a Developing Country: A Single Hospital Study from Malaysia. Pediatr Neonatol. 2017;58(5):415-20. 5. American Society for Parenteral and Enteral Nutrition Board of Directors and Standards Committee: Teitelbaum D, Guenter P, Howell WH, Kochevar ME, Roth J, Seidner DL. Definition of terms, style, and conventions used in A.S.P.E.N. guidelines and standards. Nutr Clin Pract. 2005;20:281-285. 6. Bankhead R, Boullata J, Brantley S, et al. ASPEN enteral nutrition practice recommendations. JPEN J Parenter Enteral Nutr. 2009;33(2):122-67. 7. Alldredge BK, Corelli RL, Ernst ME, et al., eds. Koda-Kimble and Young’s Applied Therapeutics: The Clinical Use of Drugs. 10th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2013. 8. Abbott nutrition products. https://abbottnutrition.com.my/products [ assessed on 3/2/18] 9. Nestle nutrition products. https://www.nestlehealthscience.us/brands [assessed on 3/2/18] 10. Pharm-D nutrition products. http://valensnutrition.com/# [ assessed on 3/2/18] 11. Seres D. Nutrition support in critically ill patients: Enteral nutrition. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. [Accessed on February 03, 2018.] 12. Slavin J. Fiber and prebiotics: mechanisms and health benefits. Nutrients. 2013;5(4):1417-35. 13. Zaman MK, Chin KF, Rai V, et al. Fiber and prebiotic supplementation in enteral nutrition: a systematic review and meta-analysis. World J Gastroenterol. 2015;21(17):5372-81. 14. O'Keefe SJ, Buchman AL, Fishbein TM, et al. Short bowel syndrome and intestinal failure: consensus definitions and overview. Clin Gastroenterol Hepatol 2006;4:6-10. 15. Evia nutrition products. http://www.britishbiologicals.com/criticare/index.php [assessed on 7/2/18] 16. Qaseem A, Chou R, Humphrey LL, et al. Inpatient glycaemic control: Best practice advice from the clinical guidelines committee of the American College of Physicians. Am J Med Qual. 2014;29(2):95-8. 17. Elia M, Ceriello A, Laube H, et al. Enteral nutritional support and use of diabetes-specific formulas for patients with diabetes: a systematic review and meta-analysis. Diabetes Care. 2005;28(9):2267-79. 18. Ojo O, Brooke J. Evaluation of the role of enteral nutrition in managing patients with diabetes: a systematic review. Nutrients. 2014;6(11):5142-52. 19. Fouque D, Kalantar-Zadeh K, Kopple J, et al. A proposed nomenclature and diagnostic criteria for protein–energy wasting in acute and chronic kidney disease. Kidney Int. 2008;73(4):391-8. 20. Kalantar-Zadeh K, Cano NJ, Budde K, et al. Diets and enteral supplements for improving outcomes in chronic kidney disease. Nat Rev Nephrol. 2011;7(7):369-84. 21. Arends J, Baracos V, Bertz H, et al. ESPEN expert group recommendations for action against cancer-related malnutrition. Clin Nutr. 2017;36(5):1187-96. 22. McClave SA, DiBaise JK, Mullin GE, et al. ACG clinical guideline: nutrition therapy in the adult hospitalized patient. Am J Gastroenterol. 2016;111(3):315-34. 23. Dietitians Association. Enteral nutrition manual for adults in health care facilities. Nutrition Support Interest Group 2014 [updated 2015; cited 2014]. 24. M Pirlich, 2016 Techniques of enteral nutrition. Lifelong learning LLL program http://lllnutrition.com/mod_lll/TOPIC8/m83.pdf Accessed on 19 February]. 25. Toussaint E, Van Gossum A, Ballarin A, et al. Enteral access in adults. Clin Nutr. 2015;34(3):350-8. 26. Chang SJ, Huang HH. Diarrhea in enterally fed patients: blame the diet? Curr Opin Clin Nutr Metab Care. 2013;16(5):588-94. 27. Hamilton AC, Auron M. Diarrhea. Hospital Medicine Clinics. 2013;2(2):e227-46. 28. Handelsman Y, Bloomgarden ZT, Grunberger G, et al. American Association of Clinical Endocrinologists and American College of Endocrinology–clinical practice guidelines for developing a diabetes mellitus comprehensive care plan–2015. Endocr Pract. 2015;21 Suppl 1:1-87. 29. Munshi MN, Florez H, Huang ES, et al. Management of diabetes in long-term care and skilled nursing facilities: a position statement of the American Diabetes Association. Diabetes Care. 2016;39(2):308-18. 30. White R, Bradnam V. Handbook of drug administration via enteral feeding tubes. pharmaceutical press; 2015 Mar 11. 31. Philip NA, Ahmed N, Pitchumoni CS. Spectrum of Drug-induced Chronic Diarrhea. J Clin Gastroenterol. 2017;51(2):111-7.