enhancement of tendon graft osteointegration using...
TRANSCRIPT
TTw
s
N
FHS
Enhancement of Tendon Graft Osteointegration UsingMesenchymal Stem Cells in a Rabbit Model of Anterior
Cruciate Ligament Reconstruction
Jit-Kheng Lim, F.R.C.S., James Hui, F.R.C.S., Li Li, M.D., Ashvin Thambyah, M.Sc.,James Goh, Ph.D., and Eng-Hin Lee, F.R.C.S.C.
Purpose: To study the effect of coating tendon grafts with mesenchymal stem cells (MSCs) on therate and quality of graft osteointegration in anterior cruciate ligament (ACL) reconstruction. Type ofStudy: Animal model. Methods: Bilateral ACL reconstructions using hamstring tendon autograftswere performed on 48 adult rabbits. Grafts were coated with MSCs in a fibrin glue carrier in one limb,and fibrin glue only in the other. Assessment was done at 2, 4, and 8 weeks. Histologic analysis wascarried out using standard and immunohistochemical stains. Biomechanical testing of force andstiffness during loading to ultimate failure was performed. Results: Control reconstructions showedmature scar tissue with some Sharpey’s-like fibers spanning the tendon-bone interface at 8 weeks.The MSC-enhanced reconstructions had large areas of cartilage cells at the tendon-bone junction at2 weeks. By 8 weeks, a mature zone of cartilage was seen gradually blending from bone into thetendon grafts. This zone stained strongly for type II collagen and showed histologic characteristicssimilar to normal rabbit ACL insertions. Biomechanically, there was no statistical difference betweenlimbs at 2 and 4 weeks. At 8 weeks, the MSC-enhanced grafts had significantly higher failure loadand stiffness. Conclusions: Coating of tendon grafts with MSCs results in healing by an interveningzone of cartilage resembling the chondral enthesis of normal ACL insertions rather than collagenfibers and scar tissue. MSC-enhanced ACL reconstructions perform significantly better than controlson biomechanical testing. Clinical Relevance: Enhancement of tendon graft osteointegration withMSCs is a novel method offering the potential for more physiologic and biomechanically strongerligament reconstructions. Key Words: Graft healing—Stem cell—Mesenchymal—ACL reconstruc-tion—Bone tunnel—Tendon graft.
(ttfircs
atptaa
endon grafts anchored within bony tunnels areused in a wide variety of orthopaedic procedures.
endon pullout from bony tunnels occurs up to 12eeks after hamstring graft anterior cruciate ligament
From the Department of Orthopaedic Surgery, National Univer-ity Hospital, Singapore, Republic of Singapore.
Supported in part by Grant No. EF2001/33/ROC-009 from theational University Hospital, Singapore.Address correspondence and reprint requests to Jit-Kheng Lim,
.R.C.S., Department of Orthopaedic Surgery, National Universityospital, Lower Kent Ridge Road, Singapore 119074, Republic ofingapore. E-mail: [email protected]© 2004 by the Arthroscopy Association of North America
m0749-8063/04/2009-3814$30.00/0doi:10.1016/j.arthro.2004.06.035
Arthroscopy: The Journal of Arthroscopic and Related Sur
ACL) reconstruction in animal models,1-4 suggestinghat mechanical strength of reconstructions before thatime are dependent to a large extent on the method ofxation. For this reason, a large emphasis of recentesearch has been on the relative benefits and biome-hanical profiles of various fixation methods for ham-tring tendon autografts.5-7
There is increasing interest in the use of biologicalgents to enhance tendon-bone osteointegration withinhe bony tunnel. Recent studies have shown that ap-lication of bone morphogenic protein-21 and a mix-ure of bone growth proteins8 to the surface of tendonutografts resulted in enhanced tendon-bone healingnd improved biomechanical properties. Mesenchy-
al stem cells (MSCs) are pluripotential cells that are899gery, Vol 20, No 9 (November), 2004: pp 899-910

bstsWtmob
E
d4wrfAwctgsclawrrae
M
rrpmcPlSb(mrtwE
s�mDnacTicWwHacac
S
ne(1UBdmatntbsfgwfinbcwfiivtscft
900 J-K. LIM ET AL.
eing investigated extensively in a wide variety ofettings, including enhancement of tissue healing andissue bioengineering.9-16 We are unaware of anytudy using MSCs to enhance tendon graft healing.
e hypothesized that the application of MSCs at theendon-bone junction during ACL reconstructionight result in both acceleration and enhancement of
steointegration of the tendon graft to the surroundingone tunnel.
METHODS
xperimental Design
Bilateral ACL reconstructions with hamstring ten-on autografts were performed by a single surgeon in8 skeletally mature New Zealand White rabbitseighing 2.0 to 2.5 kg each. Autologous bone mar-
ow–derived MSCs were harvested 3 to 4 weeks be-ore ligament reconstruction surgery. During bilateralCL reconstruction, the treatment limb was coatedith MSCs mixed in a fibrin glue carrier and the
ontrol limb was coated with fibrin glue only. Thereatment side was determined randomly, and the sur-eon was blinded to the treatment limb at the time ofurgery. There were 36 animals assigned for biome-hanical testing and the remainder underwent histo-ogic analysis. The animals were euthanized at 2, 4,nd 8 weeks postoperatively. Biomechanical analysisas carried out by blinded observers. A further 2
abbits were used for histologic analysis of the normalabbit ACL. The experimental protocol, animal care,nd use procedures were approved by the institutionalthics review committee.
SC Preparation
MSCs were harvested from bone marrow of theabbits 3 to 4 weeks before ACL reconstruction. Theabbits were anesthetized, the posterior iliac crestsrepared in a sterile manner, and 5 to 10 mL of bonearrow was aspirated. The cells were separated and
ultured using a protocol similar to that described byhinney.17 The anti-coagulated bone marrow was di-
uted with 2 times of the volume of Hank’s Balancedalt Solution. The nucleated cell layer was obtainedy Ficoll-Paque density gradient centrifugationSigma Chemical, St. Louis, MO) at 450g for 20inutes. The nucleated cells were harvested and
insed with Hank’s Balanced Salt Solution using cen-rifugation at 250g for 10 minutes twice. The pelletsere resuspended in complete Dulbecco’s Modified
agle Medium (DMEM) containing 10% fetal bovine terum (FBS), penicillin 100 U/mL, streptomycin 100g/mL (pH 7.35), and centrifuged at 250g for 10inutes. The pellets were resuspended with completeMEM containing 10% FBS. The number of theucleated cells was determined with a hemocytometernd the volume of the suspension was adjusted. Theells were plated out at a density of 1.8 � 105/cm2 in-75 flasks and grown at 37°C, 5% CO2 in a humid-
fied tissue-culture incubator. The medium washanged after 3 days, and every 3 to 4 days thereafter.hen the cells became 75% to 80% confluent, theyere trypsinized and transferred into 2 T-75 flasks.aving completed 1 passage, the cells were enumer-
ted under a hemocytometer. When necessary, theells were passaged a second time by repeating theforementioned procedure to obtain 3 to 4 millionells for use with each graft.
urgical Protocol
All rabbits were administered 15 mg/kg subcuta-eous cephalexin and 0.3 mL/kg diazepam preop-ratively. The animals were induced with Hypnorma mixture of fentanyl 0.315 mg/mL and fluanisone0 mg/mL) 0.3 mL/kg (Janssen-Cilag, Saunderton,K), followed by halothane inhalational anesthesia.ilateral ACL reconstructions were performed un-er the same anesthetic. A midline incision wasade, the semitendinosus tendon was harvested,
nd the length measured. A lateral parapatellar ar-hrotomy was used to expose the knee joint. Theative ACL was divided and tibial and femoralunnels were created with a 2-mm drill. The com-ined length of the tunnel from the anterior femoralurface, across the joint, to the anterior tibial sur-ace was recorded. Both the treatment and controlrafts (single-strand hamstring tendon) were coatedith Tisseel fibrin sealant (Baxter Healthcare, Deer-eld, IL) immediately before insertion into the tun-els. The fibrin sealant was supplied in 2 separateottles, which were to be mixed just before appli-ation. On the treatment limb, the autologous MSCsere added to one of the micropipettes containingbrin sealant solution. The grafts were advanced
nto the tunnels before the fibrin sealant becameiscous, allowing the fibrin sealant to harden withhe grafts in position in the tunnel. The grafts wereutured to the periosteum using 2-0 Ethibond (Ethi-on, Somerville, NJ) in a standard fashion on theemoral side. Then the tibial side was sutured withhe knee in 10° of flexion and slight tensioning of
he graft. The wound was closed in layers. The
aa
H
lffabsiawh
B
rspAcTtot1atcptmec
S
stpltpwlep
m�
G
4rsppoatrpiyoldb
aTtt
H
fi(tctcfitescbba
H
901MESENCHYMAL STEM CELL–ENHANCED ACL GRAFTS
nimals were allowed to move freely in their cagesfter the operation.
istologic Analysis
The femur and tibia were removed, the knee jointseft intact, and the specimens fixed in 10% bufferedormalin. Decalcification was performed using 30%ormic acid. The samples were embedded in paraffinnd cut into 5-�m thick sections longitudinal to theony tunnels in the femur and tibia. The slides weretained using hematoxylin and eosin, Safranin-O, andmmunohistochemical stains for collagens type I, II,nd III. Four knees from 2 rabbits with normal ACLsere harvested and prepared in a similar manner foristologic analysis.
iomechanical Analysis
At the time of death, the femora and tibiae wereemoved, and the knee joints were carefully dis-ected of surrounding soft tissue until the onlyhysical connection between the 2 bones was theCL tendon graft. The suture material used to se-
ure the grafts during surgery was left undisturbed.he fresh samples were mounted on a materials
esting machine (Instron, Canton, MA) with the linef distraction parallel to both the femoral and tibialunnels. The specimens were cyclically loaded with0% strain at a rate 4%/second for 20 cycles tochieve a steady state.18 The grafts were then testedo failure and the load at the point of failure re-orded. Stiffness was calculated from the linearortion of the load-displacement curve. The loca-ion of failure, either by pullout of the tunnel oridsubstance graft failure, was determined by gross
xamination and analysis of the load-displacementurves.
tatistical Analysis
Based on load-to-failure tests obtained from a pilottudy, the minimum number of animals was calculatedo be 10 animals in each time frame to achieve aower of 0.8 to detect a 50% difference at the 0.05evel. The mean failure load and stiffness betweenreatment and control groups were compared using aaired t test for equality of means. The differencesithin groups at the different time points were ana-
yzed with a 1-way analysis of variance. The differ-nces between treatment groups in the frequencies of
re-sacrifice graft failure and graft pullout during lechanical testing were cross-tabulated using the-square test for independence.
RESULTS
ross Observations
There were 96 ACL reconstructions performed on8 animals. There were 7 premature deaths, all occur-ing within 9 days of surgery. Of these, 4 animals hadevere bilateral joint infections and 3 failed to thriveostoperatively with no evidence of joint infection onostmortem examination of the knees. There were nother joint infections observed, and the remaining 41nimals were euthanized at the planned times. At theime of death, 6 of the 82 reconstructions (in 41emaining animals) were found to have undergonerior midsubstance graft failure, 2 in treatment and 4n control limbs. Cross-tabulation with �-square anal-sis identified no statistical difference in the incidencef early graft failure between treatment and controlimbs. One specimen (treatment limb at 2 weeks) wasamaged during dissection and was excluded fromiomechanical testing.The average length of the grafts was 6.0 cm and the
verage combined length of the tunnels was 4.0 cm.here were no statistically significant differences be-
ween treatment and control limbs for both graft andunnel lengths.
istologic Findings in the Control Limbs
At 2 weeks, specimens showed a distinct and widebrovascular interface between tendon and boneFig 1A). This interface consisted of irregular vascularissue and fibroblasts. No distinct areas of organizedollagen fibers or cartilage were observed. At 4 weeks,he zone between tendon and bone was seen to be-ome more mature, with occasional oblique collagenbers projecting from bone into the zone of fibrous
issue. By 8 weeks, the interface was still a distinctntity between tendon and bone (Fig 1B). It wasignificantly narrower, and occasional perpendicularollagen fibers resembling Sharpey’s fibers were seenridging the gap between tendon and bone. The fi-rous interface stained moderately on collagen type Ind III stains, but did not contain any type II collagen.
istologic Findings in the MSC-Treated Limbs
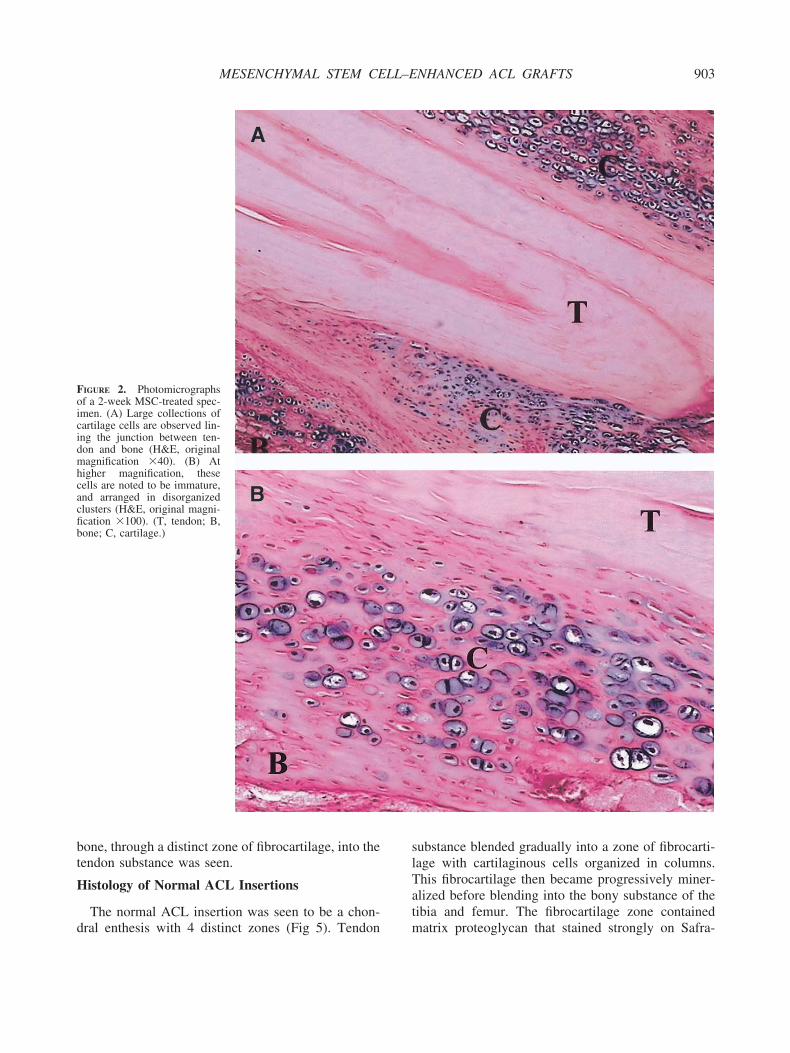
Specimens at 2 weeks showed large crops of carti-
age cells lining the junction between tendon and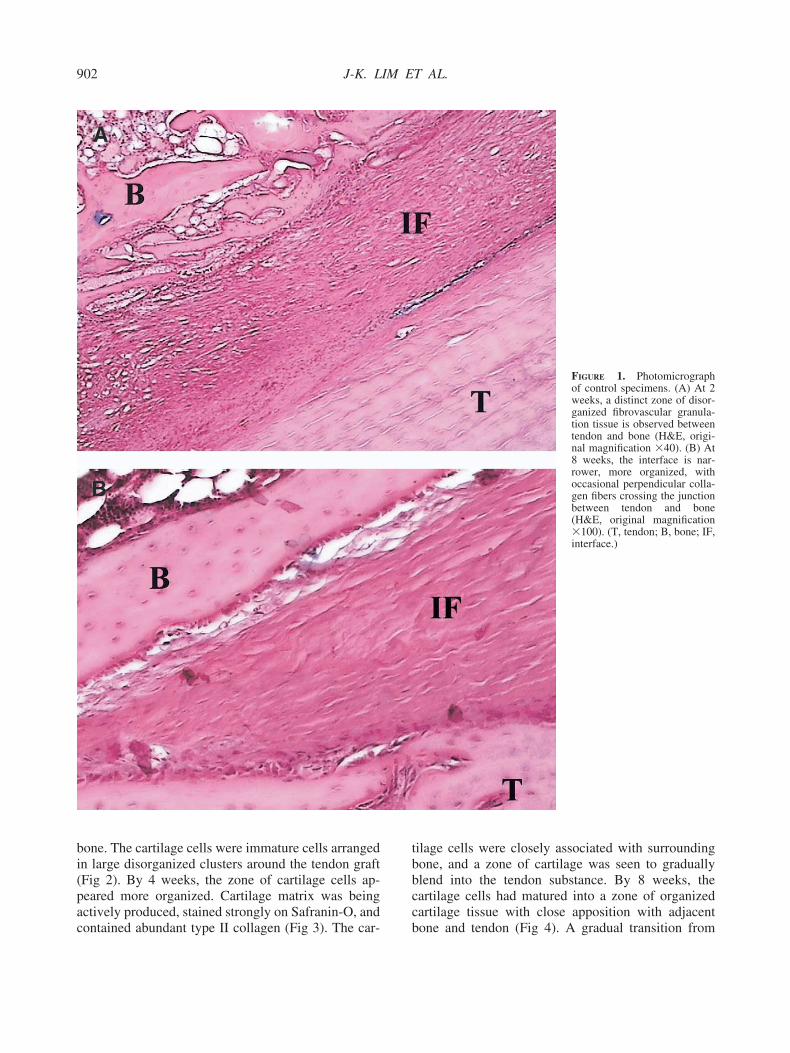
bi(pac
tbbcc
902 J-K. LIM ET AL.
one. The cartilage cells were immature cells arrangedn large disorganized clusters around the tendon graftFig 2). By 4 weeks, the zone of cartilage cells ap-eared more organized. Cartilage matrix was beingctively produced, stained strongly on Safranin-O, and
ontained abundant type II collagen (Fig 3). The car- bilage cells were closely associated with surroundingone, and a zone of cartilage was seen to graduallylend into the tendon substance. By 8 weeks, theartilage cells had matured into a zone of organizedartilage tissue with close apposition with adjacent
FIGURE 1. Photomicrographof control specimens. (A) At 2weeks, a distinct zone of disor-ganized fibrovascular granula-tion tissue is observed betweentendon and bone (H&E, origi-nal magnification �40). (B) At8 weeks, the interface is nar-rower, more organized, withoccasional perpendicular colla-gen fibers crossing the junctionbetween tendon and bone(H&E, original magnification�100). (T, tendon; B, bone; IF,interface.)
one and tendon (Fig 4). A gradual transition from
bt
H
d
slTat
Foicidmhcacfib
903MESENCHYMAL STEM CELL–ENHANCED ACL GRAFTS
one, through a distinct zone of fibrocartilage, into theendon substance was seen.
istology of Normal ACL Insertions
The normal ACL insertion was seen to be a chon-
IGURE 2. Photomicrographsf a 2-week MSC-treated spec-men. (A) Large collections ofartilage cells are observed lin-ng the junction between ten-on and bone (H&E, originalagnification �40). (B) At
igher magnification, theseells are noted to be immature,nd arranged in disorganizedlusters (H&E, original magni-cation �100). (T, tendon; B,one; C, cartilage.)
ral enthesis with 4 distinct zones (Fig 5). Tendon m
ubstance blended gradually into a zone of fibrocarti-age with cartilaginous cells organized in columns.his fibrocartilage then became progressively miner-lized before blending into the bony substance of theibia and femur. The fibrocartilage zone contained
atrix proteoglycan that stained strongly on Safra-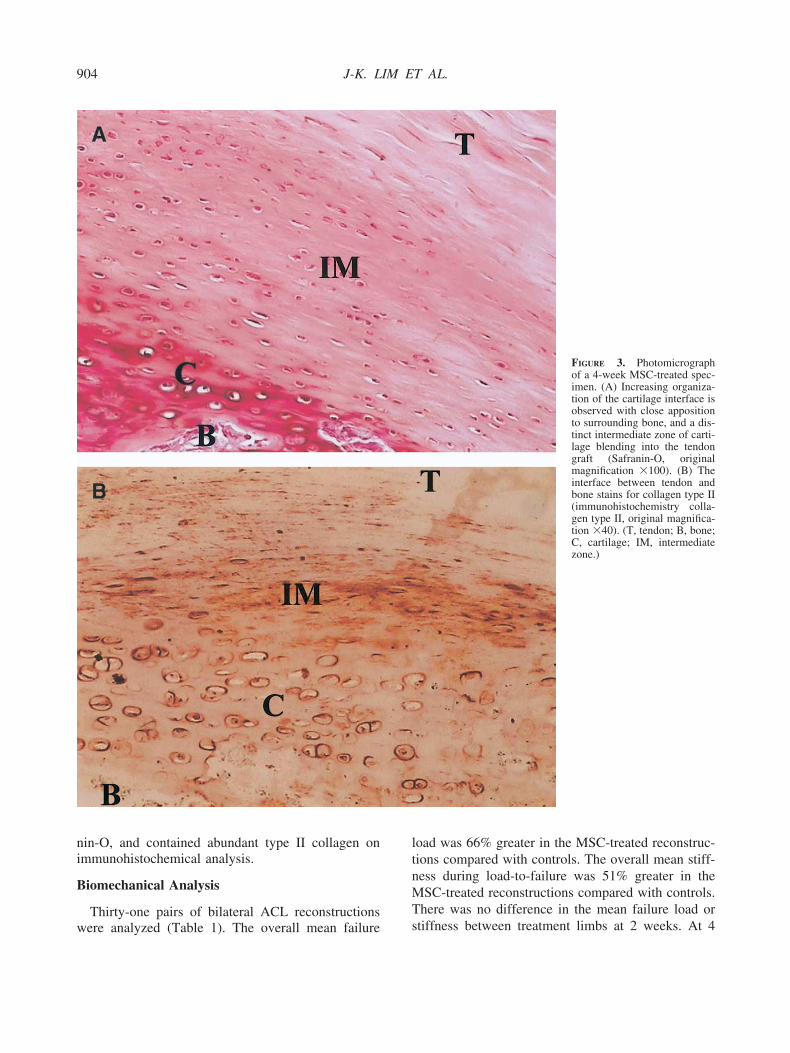
ni
B
w
ltnMT
904 J-K. LIM ET AL.
in-O, and contained abundant type II collagen onmmunohistochemical analysis.
iomechanical Analysis
Thirty-one pairs of bilateral ACL reconstructions
ere analyzed (Table 1). The overall mean failure soad was 66% greater in the MSC-treated reconstruc-ions compared with controls. The overall mean stiff-ess during load-to-failure was 51% greater in theSC-treated reconstructions compared with controls.
here was no difference in the mean failure load or
FIGURE 3. Photomicrographof a 4-week MSC-treated spec-imen. (A) Increasing organiza-tion of the cartilage interface isobserved with close appositionto surrounding bone, and a dis-tinct intermediate zone of carti-lage blending into the tendongraft (Safranin-O, originalmagnification �100). (B) Theinterface between tendon andbone stains for collagen type II(immunohistochemistry colla-gen type II, original magnifica-tion �40). (T, tendon; B, bone;C, cartilage; IM, intermediatezone.)
tiffness between treatment limbs at 2 weeks. At 4
wfths
nlcMi
Fosoab(�tsb(�c
905MESENCHYMAL STEM CELL–ENHANCED ACL GRAFTS
eeks, the treated limbs showed a trend toward higherailure loads and stiffness than controls. At 8 weeks,he MSC-treated reconstructions had significantlyigher failure loads and stiffness than control recon-tructions.
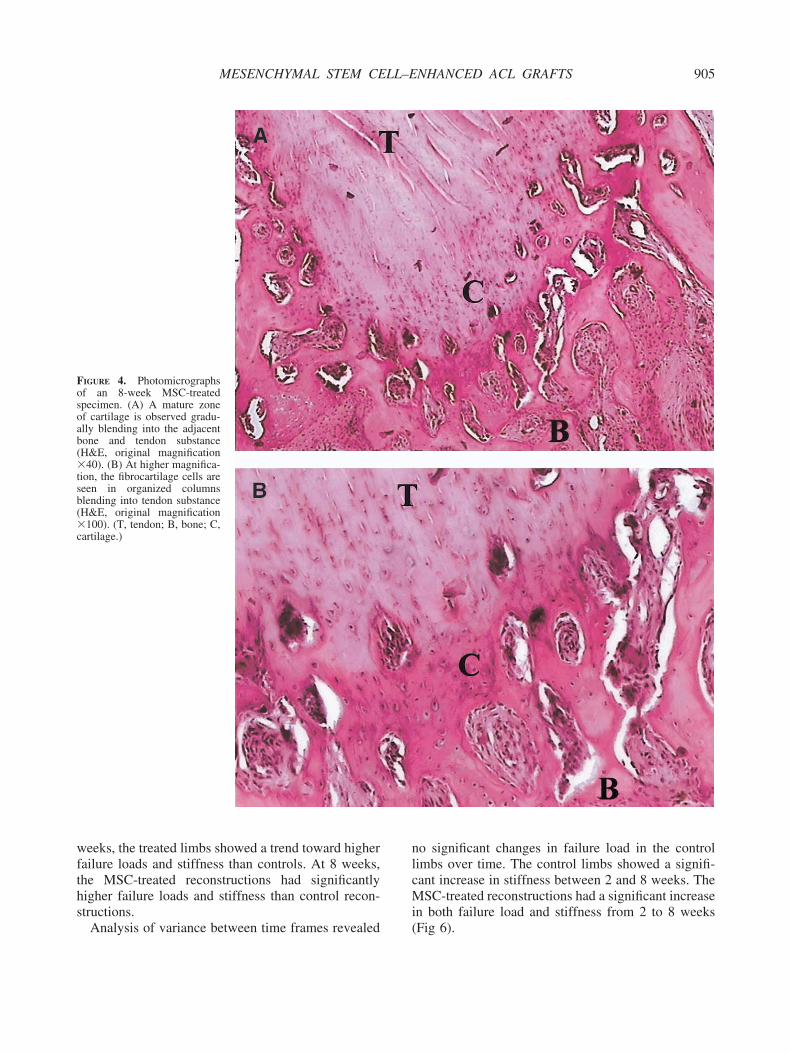
IGURE 4. Photomicrographsf an 8-week MSC-treatedpecimen. (A) A mature zonef cartilage is observed gradu-lly blending into the adjacentone and tendon substanceH&E, original magnification40). (B) At higher magnifica-
ion, the fibrocartilage cells areeen in organized columnslending into tendon substanceH&E, original magnification100). (T, tendon; B, bone; C,
artilage.)
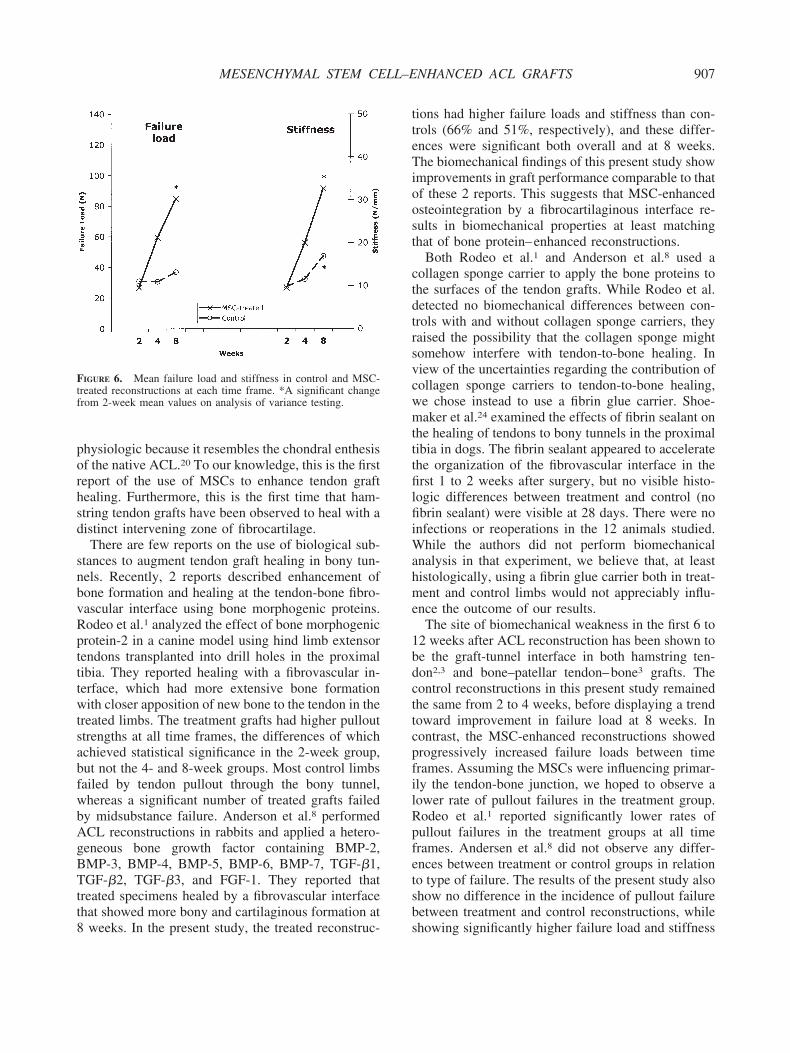
Analysis of variance between time frames revealed (
o significant changes in failure load in the controlimbs over time. The control limbs showed a signifi-ant increase in stiffness between 2 and 8 weeks. TheSC-treated reconstructions had a significant increase
n both failure load and stiffness from 2 to 8 weeks
Fig 6).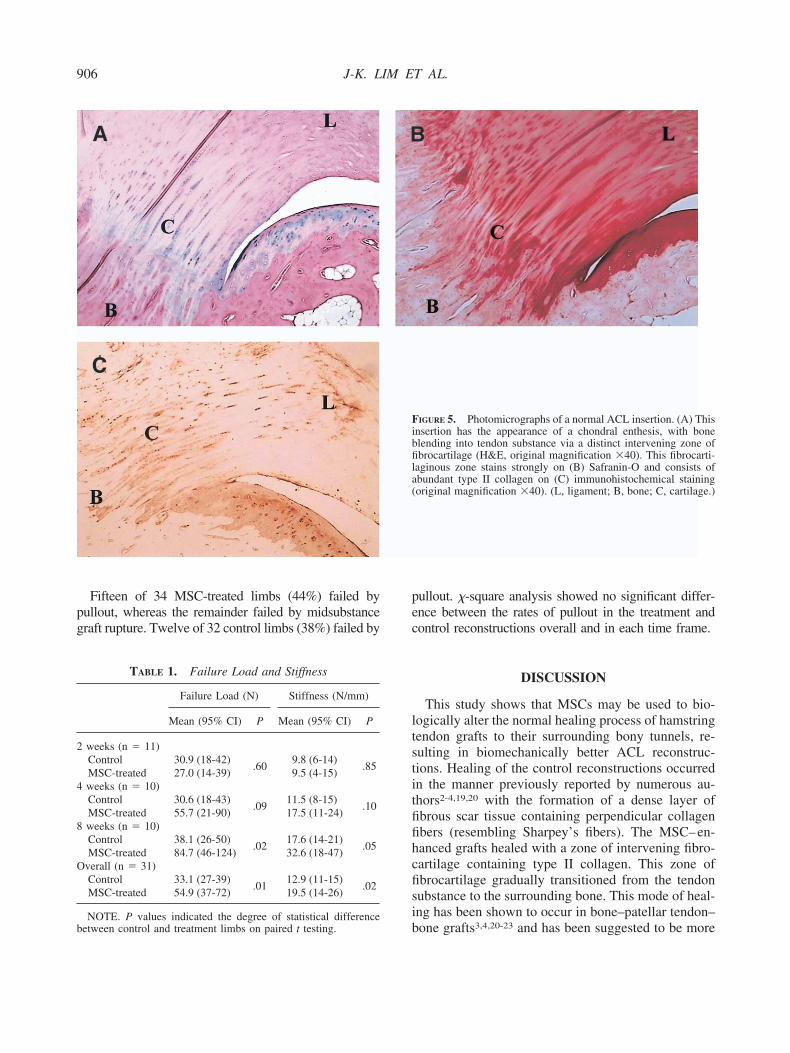
pg
pec
ltstitfifihcfisi
2
4
8
O
b
906 J-K. LIM ET AL.
Fifteen of 34 MSC-treated limbs (44%) failed byullout, whereas the remainder failed by midsubstanceraft rupture. Twelve of 32 control limbs (38%) failed by
TABLE 1. Failure Load and Stiffness
Failure Load (N) Stiffness (N/mm)
Mean (95% CI) P Mean (95% CI) P
weeks (n � 11)Control 30.9 (18-42)
.609.8 (6-14)
.85MSC-treated 27.0 (14-39) 9.5 (4-15)weeks (n � 10)Control 30.6 (18-43)
.0911.5 (8-15)
.10MSC-treated 55.7 (21-90) 17.5 (11-24)weeks (n � 10)Control 38.1 (26-50)
.0217.6 (14-21)
.05MSC-treated 84.7 (46-124) 32.6 (18-47)
verall (n � 31)Control 33.1 (27-39)
.0112.9 (11-15)
.02MSC-treated 54.9 (37-72) 19.5 (14-26)
bNOTE. P values indicated the degree of statistical difference
etween control and treatment limbs on paired t testing.
ullout. �-square analysis showed no significant differ-nce between the rates of pullout in the treatment andontrol reconstructions overall and in each time frame.
DISCUSSION
This study shows that MSCs may be used to bio-ogically alter the normal healing process of hamstringendon grafts to their surrounding bony tunnels, re-ulting in biomechanically better ACL reconstruc-ions. Healing of the control reconstructions occurredn the manner previously reported by numerous au-hors2-4,19,20 with the formation of a dense layer ofbrous scar tissue containing perpendicular collagenbers (resembling Sharpey’s fibers). The MSC–en-anced grafts healed with a zone of intervening fibro-artilage containing type II collagen. This zone ofbrocartilage gradually transitioned from the tendonubstance to the surrounding bone. This mode of heal-ng has been shown to occur in bone–patellar tendon–
IGURE 5. Photomicrographs of a normal ACL insertion. (A) Thisnsertion has the appearance of a chondral enthesis, with bonelending into tendon substance via a distinct intervening zone ofbrocartilage (H&E, original magnification �40). This fibrocarti-
aginous zone stains strongly on (B) Safranin-O and consists ofbundant type II collagen on (C) immunohistochemical stainingoriginal magnification �40). (L, ligament; B, bone; C, cartilage.)
Fibfila(
one grafts3,4,20-23 and has been suggested to be more
porhsd
snbvRptttwtsabfwbAgBTtt8
tteTioost
ctdtrsvcwmtttfilfiiWahme
1bdcttcpfilRpfetsb
Ftf
907MESENCHYMAL STEM CELL–ENHANCED ACL GRAFTS
hysiologic because it resembles the chondral enthesisf the native ACL.20 To our knowledge, this is the firsteport of the use of MSCs to enhance tendon graftealing. Furthermore, this is the first time that ham-tring tendon grafts have been observed to heal with aistinct intervening zone of fibrocartilage.There are few reports on the use of biological sub-
tances to augment tendon graft healing in bony tun-els. Recently, 2 reports described enhancement ofone formation and healing at the tendon-bone fibro-ascular interface using bone morphogenic proteins.odeo et al.1 analyzed the effect of bone morphogenicrotein-2 in a canine model using hind limb extensorendons transplanted into drill holes in the proximalibia. They reported healing with a fibrovascular in-erface, which had more extensive bone formationith closer apposition of new bone to the tendon in the
reated limbs. The treatment grafts had higher pullouttrengths at all time frames, the differences of whichchieved statistical significance in the 2-week group,ut not the 4- and 8-week groups. Most control limbsailed by tendon pullout through the bony tunnel,hereas a significant number of treated grafts failedy midsubstance failure. Anderson et al.8 performedCL reconstructions in rabbits and applied a hetero-eneous bone growth factor containing BMP-2,MP-3, BMP-4, BMP-5, BMP-6, BMP-7, TGF-�1,GF-�2, TGF-�3, and FGF-1. They reported that
reated specimens healed by a fibrovascular interfacehat showed more bony and cartilaginous formation at
IGURE 6. Mean failure load and stiffness in control and MSC-reated reconstructions at each time frame. *A significant changerom 2-week mean values on analysis of variance testing.
weeks. In the present study, the treated reconstruc- s
ions had higher failure loads and stiffness than con-rols (66% and 51%, respectively), and these differ-nces were significant both overall and at 8 weeks.he biomechanical findings of this present study show
mprovements in graft performance comparable to thatf these 2 reports. This suggests that MSC-enhancedsteointegration by a fibrocartilaginous interface re-ults in biomechanical properties at least matchinghat of bone protein–enhanced reconstructions.
Both Rodeo et al.1 and Anderson et al.8 used aollagen sponge carrier to apply the bone proteins tohe surfaces of the tendon grafts. While Rodeo et al.etected no biomechanical differences between con-rols with and without collagen sponge carriers, theyaised the possibility that the collagen sponge mightomehow interfere with tendon-to-bone healing. Iniew of the uncertainties regarding the contribution ofollagen sponge carriers to tendon-to-bone healing,e chose instead to use a fibrin glue carrier. Shoe-aker et al.24 examined the effects of fibrin sealant on
he healing of tendons to bony tunnels in the proximalibia in dogs. The fibrin sealant appeared to acceleratehe organization of the fibrovascular interface in therst 1 to 2 weeks after surgery, but no visible histo-
ogic differences between treatment and control (nobrin sealant) were visible at 28 days. There were no
nfections or reoperations in the 12 animals studied.hile the authors did not perform biomechanical
nalysis in that experiment, we believe that, at leastistologically, using a fibrin glue carrier both in treat-ent and control limbs would not appreciably influ-
nce the outcome of our results.The site of biomechanical weakness in the first 6 to
2 weeks after ACL reconstruction has been shown toe the graft-tunnel interface in both hamstring ten-on2,3 and bone–patellar tendon–bone3 grafts. Theontrol reconstructions in this present study remainedhe same from 2 to 4 weeks, before displaying a trendoward improvement in failure load at 8 weeks. Inontrast, the MSC-enhanced reconstructions showedrogressively increased failure loads between timerames. Assuming the MSCs were influencing primar-ly the tendon-bone junction, we hoped to observe aower rate of pullout failures in the treatment group.odeo et al.1 reported significantly lower rates ofullout failures in the treatment groups at all timerames. Andersen et al.8 did not observe any differ-nces between treatment or control groups in relationo type of failure. The results of the present study alsohow no difference in the incidence of pullout failureetween treatment and control reconstructions, while
howing significantly higher failure load and stiffness
itoft
tlbasohbpcpacib
iorcfiftwdwiihthdb
to(t9(S(ltrt
wutnlsatwsaawdsooc
FMfiMfMs
bewgMldttfwbo
sirschttlo
908 J-K. LIM ET AL.
n the MSC-treated limbs. These findings may suggesthat, aside from the obvious histologic enhancementf the tendon-bone junction healing, the MSCs may inact be influencing the biomechanical properties of theendon substance itself.
Goradia et al.25 reported that hamstring tendon au-ografts progress through a period of relative hypocel-ularity at 4 weeks before gradually being repopulatedy fibroblast-like cells from 8 to 12 weeks. This isccompanied by collagen fiber disorganization thatlowly begins to show a crimp pattern from 12 weeksnward. MSCs have been successfully used to en-ance tendon defect healing.26 Acceleration of fibro-last/tenocyte repopulation of the tendon graft in theresent study may explain the enhanced early biome-hanical properties of reconstructions. The MSCs ap-lied to the surface of tendon grafts may have serveds a source of additional recruitable fibroblast-likeells for tendon repopulation, or they may have beennvolved in activation and recruitment of local fibro-last precursors.Hamstring grafts have been associated with a higher
ncidence of bony tunnel widening27-29 and the devel-pment of graft laxity in the medium-term in someeports.30,31 Tunnel widening in hamstring ACL re-onstruction has been postulated to result from graftxation points being further away from the joint sur-ace.27 However, recent reports suggest that femoralunnel widening still occurs in hamstring tendon graftsith anatomic fixation,32 whereas bone–patellar ten-on–bone grafts have less tunnel widening, evenhen femoral suspensory fixation is used.31 The find-
ngs of these reports suggest that tunnel widening mayn fact be related to the differences in healing ofamstring and bone–patellar tendon–bone grafts toheir surrounding bony tunnels. By modifying theealing process and creating a more physiologic ten-on-bone interface, MSC-enhanced ACL grafts maye less likely to develop tunnel widening.We chose to use a rabbit model of ACL reconstruc-
ion. This is a model that has been validated in previ-us reports in the literature.8,22,33-39 The mortality14%) and infection rates (8%) were comparable tohose reported in previous studies (0 to 17% and 0 to%, respectively).8,33,35,36,38 Six of 82 reconstructions7%) were found to have failed at the time of death.akai et al.38 reported that 2 of 27 reconstructions7%) had unrecordable force measurements. Simi-arly, Anderson et al.8 reported that 2 of 84 reconstruc-ions (2%) were grossly atrophic and resulted in un-ecordable force measurements on biomechanical
esting. We did not perform control reconstructions lithout fibrin glue, and cannot comment whether these of fibrin as a carrier might have contributed tohese findings. Although there were statistically sig-ificant differences between treatment and controlimbs in biomechanical testing, the range of test re-ults was wide, with standard errors of between 8%nd 27% of the mean failure load and stiffness in eachime frame. We believe this is an inherent problemith the use of small animal models of ACL recon-
truction and previous studies4,8,38 have also reportedwide range in their biomechanical results. More
ccurate and reliable testing may have been achievedith the use of a larger animal model, such as sheep orog. Nonetheless, the range of values for force andtiffness in our study are similar to those obtained byther investigators performing ACL reconstructionsn rabbits4,8,33,35,38 and, thus, useful comparisons andonclusions may still be drawn.
There are several other limitations of this study.irst, we did not perform the experiment with labeledSCs. We are thus unable to comment on whether the
brocartilage interface formed originated from theSCs themselves, or whether this cartilage originated
rom cells recruited locally. Analysis of the fate of theSCs with green fluorescent protein labeling is the
ubject of a subsequent experiment by our group.Second, we chose to analyze our results at and
efore 8 weeks because the original intention of thexperiment was to detect acceleration of early healinghen tendon grafts are known to fail at the tendon-raft junction. However, with the discovery that theSC-enhanced reconstructions healed by fibrocarti-
age rather than granulation tissue, it would have beenesirable to observe the histologic appearances ofhese fibrocartilaginous tendon-bone junctions at in-ervals even up to a year after surgery. Longer timerames would have also allowed us to documenthether the histologic and biomechanical differencesetween treatment and control limbs remain the samer diminish over time.Last, the mean failure loads of the control recon-
tructions in this present study did not increase signif-cantly over the 8 weeks of the experiment. Some haveeported an increase in failure loads in control recon-tructions from 2 to 8 weeks.1,3,4 The fact that theontrol reconstructions did not change in strength mayave accentuated the differences in results betweenreatment and control limbs at 4 and 8 weeks. None-heless, the biomechanical behavior of the controlimbs in this present study is similar to that of severalther reports2,8,33 that also found no increase in failure
oads in the initial 8 to 12 weeks.
ficemearttst
aDp
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
909MESENCHYMAL STEM CELL–ENHANCED ACL GRAFTS
CONCLUSIONS
Applying MSCs to tendon grafts results in a zone ofbrocartilage at the graft-tendon junction that morelosely resembles that of the normal ACL chondralnthesis. These enhanced grafts have improved bio-echanical properties compared with controls and
xhibit a rapid and significant increase in failure loadnd stiffness in the first 8 weeks following ACLeconstruction. Further research is required to evaluatehis novel method of enhancing tendon-graft os-eointegration, which offers more physiologic healing,tronger reconstructions, and an earlier return to ac-ivity.
Acknowledgment: The authors acknowledge the invalu-ble contributions of Ms. Sue-Wee Chong, Ms. Julee Chan,r. H. W. Ouyong, and the Tissue Engineering Group, De-artment of Orthopaedics, National University of Singapore.
REFERENCES
1. Rodeo SA, Suzuki K, Deng XH, Wozney J, Warren RF. Use ofrecombinant human bone morphogenetic protein-2 to enhancetendon healing in a bone tunnel. Am J Sports Med 1999;27:476-488.
2. Goradia VK, Rochat MC, Grana WA, Rohrer MD, Prasad HS.Tendon-to-bone healing of a semitendinosus tendon autograftused for ACL reconstruction in a sheep model. Am J KneeSurg 2000;13:143-151.
3. Tomita F, Yasuda K, Mikami S, Sakai T, Yamazaki S,Tohyama H. Comparisons of intraosseous graft healing be-tween the doubled flexor tendon graft and the bone–patellartendon–bone graft in anterior cruciate ligament reconstruction.Arthroscopy 2001;17:461-476.
4. Park MJ, Lee MC, Seong SC. A comparative study of thehealing of tendon autograft and tendon-bone autograft usingpatellar tendon in rabbits. Int Orthop 2001;25:35-39.
5. Harner CD, Rihn JA, Vogrin TM. What’s new in sportsmedicine. J Bone Joint Surg Am 2003;85:1173-1181.
6. Kousa P, Jarvinen TL, Vihavainen M, Kannus P, Jarvinen M.The fixation strength of six hamstring tendon graft fixationdevices in anterior cruciate ligament reconstruction. Part II:Tibial site. Am J Sports Med 2003;31:182-188.
7. Kousa P, Jarvinen TL, Vihavainen M, Kannus P, Jarvinen M.The fixation strength of six hamstring tendon graft fixationdevices in anterior cruciate ligament reconstruction. Part I:Femoral site. Am J Sports Med 2003;31:174-181.
8. Anderson K, Seneviratne AM, Izawa K, Atkinson BL, PotterHG, Rodeo SA. Augmentation of tendon healing in an intra-articular bone tunnel with use of a bone growth factor. Am JSports Med 2001;29:689-698.
9. Arnoczky SP. Building a meniscus. Biologic considerations.Clin Orthop 1999;367:S244-S253 (suppl).
0. Woo SL, Hildebrand K, Watanabe N, Fenwick JA, Papageor-giou CD, Wang JH. Tissue engineering of ligament and tendonhealing. Clin Orthop 1999;367:S312-S323 (suppl).
1. Ohgushi H, Caplan AI. Stem cell technology and bioceramics:From cell to gene engineering. J Biomed Mater Res 1999;48:913-927.
2. Fibbe WE. Mesenchymal stem cells. A potential source forskeletal repair. Ann Rheum Dis 2002;61:ii29-ii31 (suppl 2).
3. Cancedda R, Dozin B, Giannoni P, Quarto R. Tissue engineer-ing and cell therapy of cartilage and bone. Matrix Biol 2003;22:81-91.
4. Tuan RS, Boland G, Tuli R. Adult mesenchymal stem cellsand cell-based tissue engineering. Arthritis Res Ther 2003;5:32-45.
5. Jorgensen C, Djouad F, Apparailly F, Noel D. Engineeringmesenchymal stem cells for immunotherapy. Gene Ther 2003;10:928-931.
6. Tocci A, Forte L. Mesenchymal stem cell: Use and perspec-tives. Hematol J 2003;4:92-96.
7. Phinney DG. Building a consensus regarding the nature andorigin of mesenchymal stem cells. J Cell Biochem Suppl2002;38:7-12.
8. Woo SL, Debski RE, Withrow JD, Janaushek MA. Biome-chanics of knee ligaments. Am J Sports Med 1999;27:533-543.
9. Pinczewski LA, Clingeleffer AJ, Otto DD, Bonar SF, Corry IS.Integration of hamstring tendon graft with bone in reconstruc-tion of the anterior cruciate ligament. Arthroscopy 1997;13:641-643.
0. Petersen W, Laprell H. Insertion of autologous tendon grafts tothe bone: A histological and immunohistochemical study ofhamstring and patellar tendon grafts. Knee Surg Sports Trau-matol Arthrosc 2000;8:26-31.
1. Rodeo SA, Arnoczky SP, Torzilli PA, Hidaka C, Warren RF.Tendon-healing in a bone tunnel. A biomechanical and histo-logical study in the dog. J Bone Joint Surg Am 1993;75:1795-1803.
2. Panni AS, Milano G, Lucania L, Fabbriciani C. Graft healingafter anterior cruciate ligament reconstruction in rabbits. ClinOrthop 1997;343:203-212.
3. Yoshiya S, Nagano M, Kurosaka M, Muratsu H, Mizuno K.Graft healing in the bone tunnel in anterior cruciate ligamentreconstruction. Clin Orthop 2000;376:278-286.
4. Shoemaker SC, Rechl H, Campbell P, Kram HB, Sanchez M.Effects of fibrin sealant on incorporation of autograft andxenograft tendons within bone tunnels. A preliminary study.Am J Sports Med 1989;17:318-324.
5. Goradia VK, Rochat MC, Kida M, Grana WA. Natural historyof a hamstring tendon autograft used for anterior cruciateligament reconstruction in a sheep model. Am J Sports Med2000;28:40-46.
6. Young RG, Butler DL, Weber W, Caplan AI, Gordon SL, FinkDJ. Use of mesenchymal stem cells in a collagen matrix forAchilles tendon repair. J Orthop Res 1998;16:406-413.
7. L’Insalata JC, Klatt B, Fu FH, Harner CD. Tunnel expansionfollowing anterior cruciate ligament reconstruction: A com-parison of hamstring and patellar tendon autografts. Knee SurgSports Traumatol Arthrosc 1997;5:234-238.
8. Clatworthy MG, Annear P, Bulow JU, Bartlett RJ. Tunnelwidening in anterior cruciate ligament reconstruction: A pro-spective evaluation of hamstring and patella tendon grafts.Knee Surg Sports Traumatol Arthrosc 1999;7:138-145.
9. Webster KE, Feller JA, Hameister KA. Bone tunnel enlarge-ment following anterior cruciate ligament reconstruction: Arandomized comparison of hamstring and patellar tendongrafts with 2-year follow-up. Knee Surg Sports TraumatolArthrosc 2001;9:86-91.
0. Yunes M, Richmond JC, Engels EA, Pinczewski LA. Patellarversus hamstring tendons in anterior cruciate ligament recon-struction: A meta-analysis. Arthroscopy 2001;17:248-257.
1. Barrett GR, Noojin FK, Hartzog CW, Nash CR. Reconstruc-tion of the anterior cruciate ligament in females: A comparisonof hamstring versus patellar tendon autograft. Arthroscopy
2002;18:46-54.
3
3
3
3
3
3
3
3
910 J-K. LIM ET AL.
2. Buelow JU, Siebold R, Ellermann A. A prospective evaluationof tunnel enlargement in anterior cruciate ligament reconstruc-tion with hamstrings: Extracortical versus anatomical fixation.Knee Surg Sports Traumatol Arthrosc 2002;10:80-85.
3. Grana WA, Egle DM, Mahnken R, Goodhart CW. An analysisof autograft fixation after anterior cruciate ligament recon-struction in a rabbit model. Am J Sports Med 1994;22:344-351.
4. Guzzanti V, Falciglia F, Gigante A, Fabbriciani C. The effectof intra-articular ACL reconstruction on the growth plates ofrabbits. J Bone Joint Surg Br 1994;76:960-963.
5. Blickenstaff KR, Grana WA, Egle D. Analysis of a semiten-dinosus autograft in a rabbit model. Am J Sports Med 1997;25:554-559.
6. Papachristou G, Tilentzoglou A, Efstathopoulos N, Khaldi L.Reconstruction of anterior cruciate ligament using the doubled
tendon graft technique: An experimental study in rabbits. KneeSurg Sports Traumatol Arthrosc 1998;6:246-252.
7. Ono T, Wada Y, Takahashi K, Tsuchida T, Minamide M,Moriya H. Tibial deformities and failures of anterior cruciateligament reconstruction in immature rabbits. J Orthop Sci1998;3:150-155.
8. Sakai H, Fukui N, Kawakami A, Kurosawa H. Biologicalfixation of the graft within bone after anterior cruciateligament reconstruction in rabbits: Effects of the durationof postoperative immobilization. J Orthop Sci 2000;5:43-51.
9. Labs K, Perka C, Schneider F. The biological and biomechani-cal effect of different graft tensioning in anterior cruciate
ligament reconstruction: An experimental study. Arch OrthopTrauma Surg 2002;122:193-199.