enhanced care policy - bolton nhs ft
TRANSCRIPT

Version 1 Document Enhanced Care Policy Page 1 of 35 Date March 2017 Next Review Date March 2018
Enhanced Care Policy
Document type: Policy
Version: 1
Author (name): Paul Devlin
Kate McKenna
Antony Makepeace
Christopher Davidson
Author (designation): Divisional Nurse Director
Business Manager
Matron
Dementia Nurse Specialist
Validated by Clinical Governance & Quality Committee
Date validated
Ratified by: Executive Directors
Date ratified:
Name of responsible committee/individual:
Name of Executive Lead (for policies only)
Master Document Controller:
Date uploaded to intranet:
Key words
Review date:
Version control
Version Type of Change Date Revisions from previous issues
1 New Policy New Policy
Equality Impact
Version 1 Document Enhanced Care Policy Page 2 of 35 Date March 2017 Next Review Date March 2018
Bolton NHS Foundation Trust strives to ensure equality of opportunity for all service users, local people and the workforce. As an employer
and a provider of healthcare Bolton NHS FT aims to ensure that none are placed at a disadvantage as a result of its policies and
procedures. This document has therefore been equality impact assessed to ensure fairness and consistency for all those covered by it
regardless of their individuality. The results are shown in the Equality Impact Assessment (EIA).
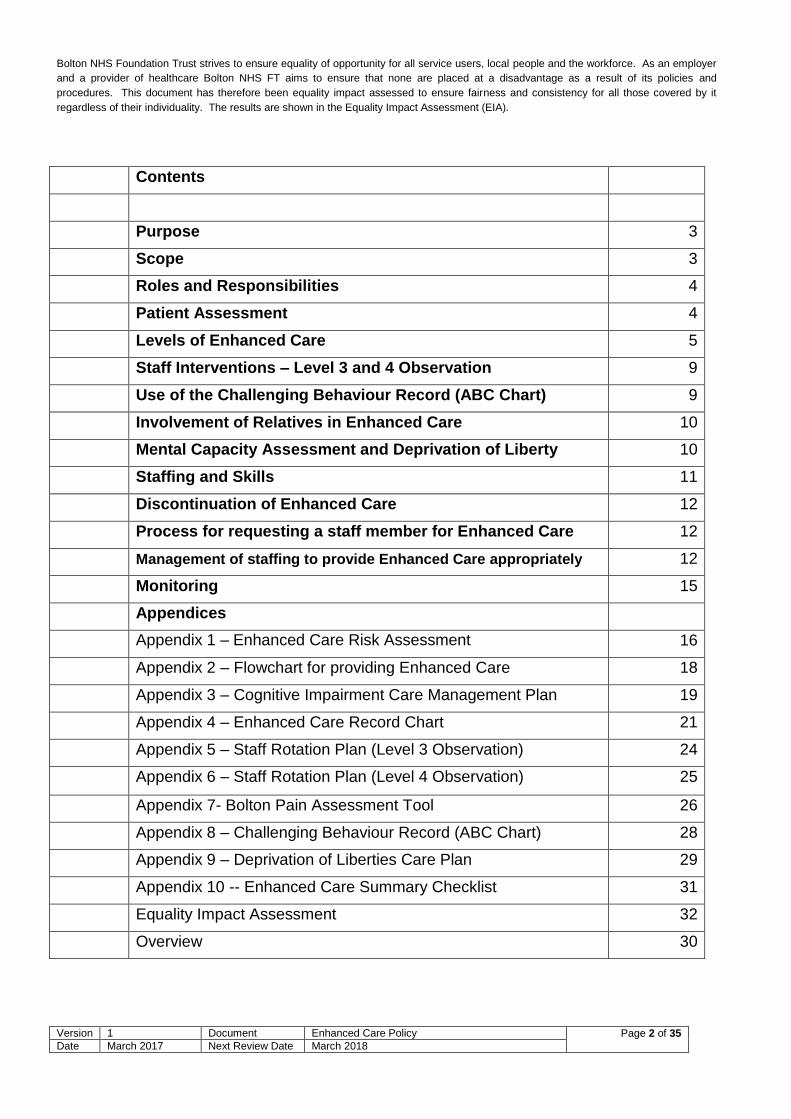
Contents
Purpose 3
Scope 3
Roles and Responsibilities 4
Patient Assessment 4
Levels of Enhanced Care 5
Staff Interventions – Level 3 and 4 Observation 9
Use of the Challenging Behaviour Record (ABC Chart) 9
Involvement of Relatives in Enhanced Care 10
Mental Capacity Assessment and Deprivation of Liberty 10
Staffing and Skills 11
Discontinuation of Enhanced Care 12
Process for requesting a staff member for Enhanced Care 12
Management of staffing to provide Enhanced Care appropriately 12
Monitoring 15
Appendices
Appendix 1 – Enhanced Care Risk Assessment 16
Appendix 2 – Flowchart for providing Enhanced Care 18
Appendix 3 – Cognitive Impairment Care Management Plan 19
Appendix 4 – Enhanced Care Record Chart 21
Appendix 5 – Staff Rotation Plan (Level 3 Observation) 24
Appendix 6 – Staff Rotation Plan (Level 4 Observation) 25
Appendix 7- Bolton Pain Assessment Tool 26
Appendix 8 – Challenging Behaviour Record (ABC Chart) 28
Appendix 9 – Deprivation of Liberties Care Plan 29
Appendix 10 -- Enhanced Care Summary Checklist 31
Equality Impact Assessment 32
Overview 30
Version 1 Document Enhanced Care Policy Page 3 of 35 Date March 2017 Next Review Date March 2018
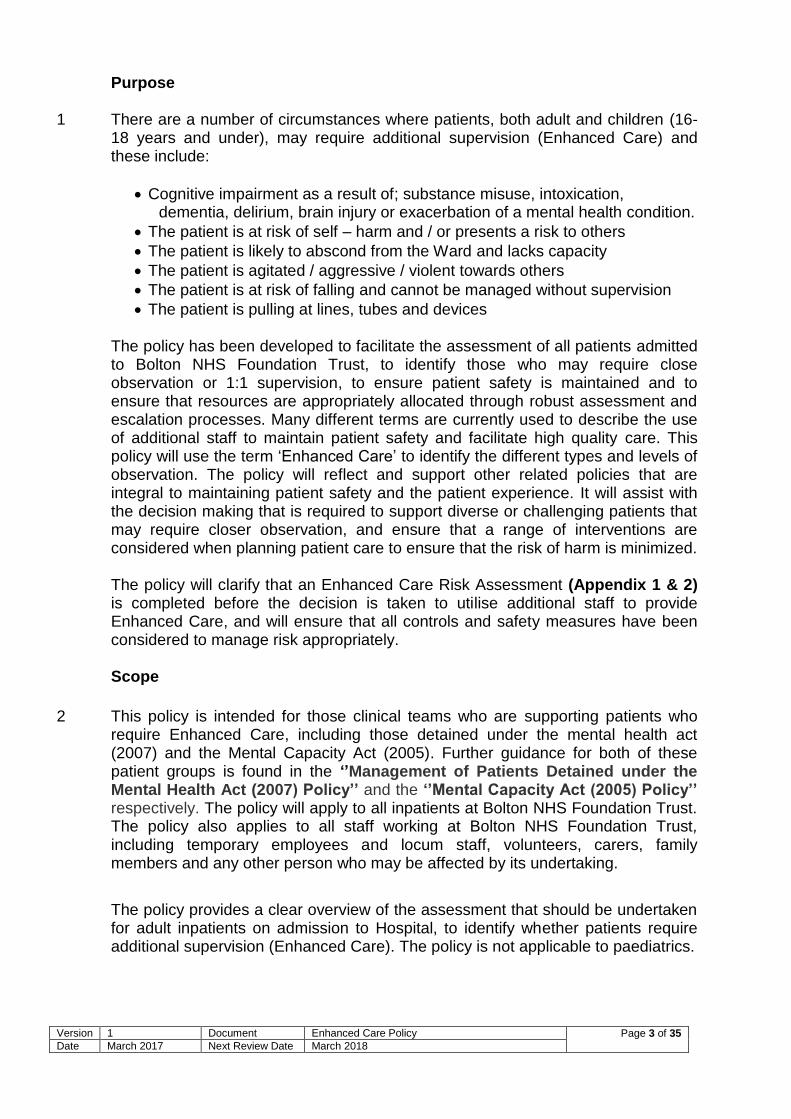
Purpose
1 There are a number of circumstances where patients, both adult and children (16-
18 years and under), may require additional supervision (Enhanced Care) and these include:
Cognitive impairment as a result of; substance misuse, intoxication, dementia, delirium, brain injury or exacerbation of a mental health condition.
The patient is at risk of self – harm and / or presents a risk to others
The patient is likely to abscond from the Ward and lacks capacity
The patient is agitated / aggressive / violent towards others
The patient is at risk of falling and cannot be managed without supervision
The patient is pulling at lines, tubes and devices The policy has been developed to facilitate the assessment of all patients admitted to Bolton NHS Foundation Trust, to identify those who may require close observation or 1:1 supervision, to ensure patient safety is maintained and to ensure that resources are appropriately allocated through robust assessment and escalation processes. Many different terms are currently used to describe the use of additional staff to maintain patient safety and facilitate high quality care. This policy will use the term ‘Enhanced Care’ to identify the different types and levels of observation. The policy will reflect and support other related policies that are integral to maintaining patient safety and the patient experience. It will assist with the decision making that is required to support diverse or challenging patients that may require closer observation, and ensure that a range of interventions are considered when planning patient care to ensure that the risk of harm is minimized. The policy will clarify that an Enhanced Care Risk Assessment (Appendix 1 & 2) is completed before the decision is taken to utilise additional staff to provide Enhanced Care, and will ensure that all controls and safety measures have been considered to manage risk appropriately.
Scope
2
This policy is intended for those clinical teams who are supporting patients who require Enhanced Care, including those detained under the mental health act (2007) and the Mental Capacity Act (2005). Further guidance for both of these patient groups is found in the ‘’Management of Patients Detained under the Mental Health Act (2007) Policy’’ and the ‘’Mental Capacity Act (2005) Policy’’ respectively. The policy will apply to all inpatients at Bolton NHS Foundation Trust. The policy also applies to all staff working at Bolton NHS Foundation Trust, including temporary employees and locum staff, volunteers, carers, family members and any other person who may be affected by its undertaking.
The policy provides a clear overview of the assessment that should be undertaken for adult inpatients on admission to Hospital, to identify whether patients require additional supervision (Enhanced Care). The policy is not applicable to paediatrics.
Version 1 Document Enhanced Care Policy Page 4 of 35 Date March 2017 Next Review Date March 2018
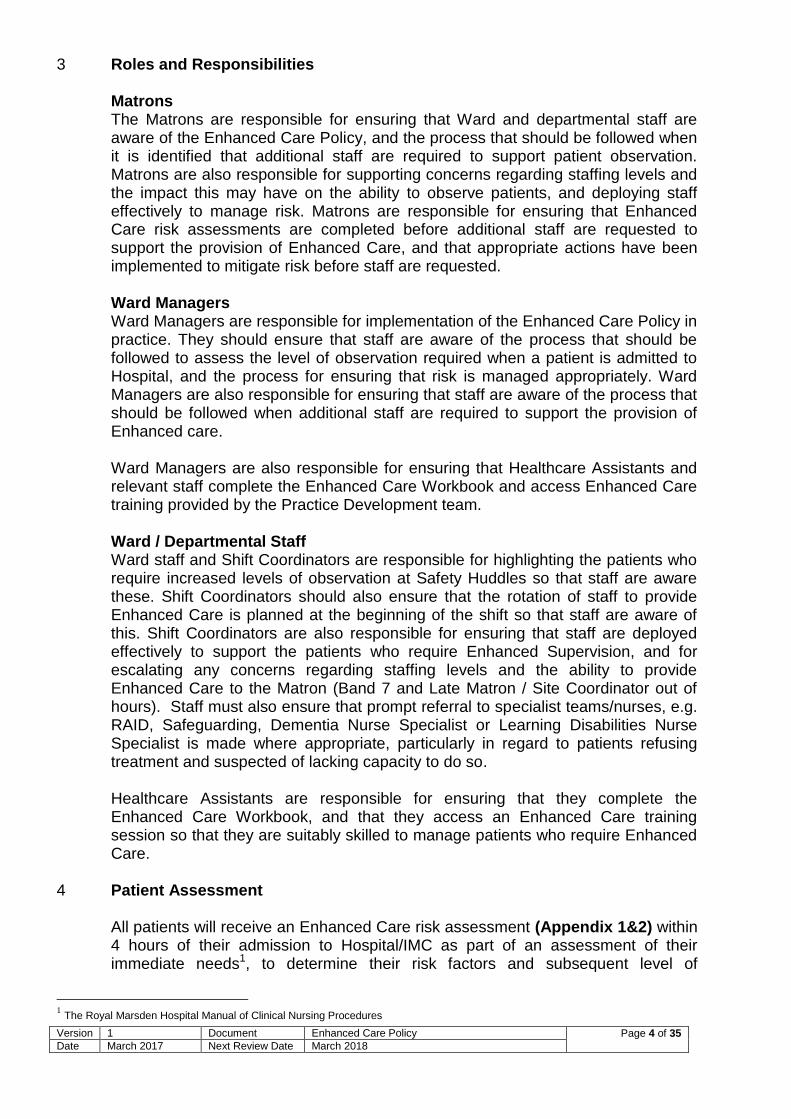
3 Roles and Responsibilities Matrons The Matrons are responsible for ensuring that Ward and departmental staff are aware of the Enhanced Care Policy, and the process that should be followed when it is identified that additional staff are required to support patient observation. Matrons are also responsible for supporting concerns regarding staffing levels and the impact this may have on the ability to observe patients, and deploying staff effectively to manage risk. Matrons are responsible for ensuring that Enhanced Care risk assessments are completed before additional staff are requested to support the provision of Enhanced Care, and that appropriate actions have been implemented to mitigate risk before staff are requested. Ward Managers Ward Managers are responsible for implementation of the Enhanced Care Policy in practice. They should ensure that staff are aware of the process that should be followed to assess the level of observation required when a patient is admitted to Hospital, and the process for ensuring that risk is managed appropriately. Ward Managers are also responsible for ensuring that staff are aware of the process that should be followed when additional staff are required to support the provision of Enhanced care. Ward Managers are also responsible for ensuring that Healthcare Assistants and relevant staff complete the Enhanced Care Workbook and access Enhanced Care training provided by the Practice Development team. Ward / Departmental Staff Ward staff and Shift Coordinators are responsible for highlighting the patients who require increased levels of observation at Safety Huddles so that staff are aware these. Shift Coordinators should also ensure that the rotation of staff to provide Enhanced Care is planned at the beginning of the shift so that staff are aware of this. Shift Coordinators are also responsible for ensuring that staff are deployed effectively to support the patients who require Enhanced Supervision, and for escalating any concerns regarding staffing levels and the ability to provide Enhanced Care to the Matron (Band 7 and Late Matron / Site Coordinator out of hours). Staff must also ensure that prompt referral to specialist teams/nurses, e.g. RAID, Safeguarding, Dementia Nurse Specialist or Learning Disabilities Nurse Specialist is made where appropriate, particularly in regard to patients refusing treatment and suspected of lacking capacity to do so. Healthcare Assistants are responsible for ensuring that they complete the Enhanced Care Workbook, and that they access an Enhanced Care training session so that they are suitably skilled to manage patients who require Enhanced Care.
4 Patient Assessment All patients will receive an Enhanced Care risk assessment (Appendix 1&2) within 4 hours of their admission to Hospital/IMC as part of an assessment of their immediate needs1, to determine their risk factors and subsequent level of
1 The Royal Marsden Hospital Manual of Clinical Nursing Procedures

Version 1 Document Enhanced Care Policy Page 5 of 35 Date March 2017 Next Review Date March 2018
observation they require. If it is determined that the patient requires level 1 observation, reassessment will only be required if the patient’s condition or cognitive state changes. The level of observation required will be determined by the score from the Enhanced Care risk assessment. If a patient requires greater than Level 1 care then an assessment should be completed daily using the Enhanced Care risk assessment tool. The assessment should be completed by the Registered Nurse who is responsible for the patient. The shift coordinator should be informed about the outcome of enhanced care risk assessments to ensure that actions required as a result of the assessment have been completed, and so that appropriate levels of supervision can be provided to patients that require this.
Level 1 Observation = Score 0 to 3 Level 2 Observation = Score 4 to 7 Level 3 Observation = Score 8 to 9
Level 4 Observation = Score 10 to 11
Levels of Enhanced Care
5 Level 1 Observation Level 1 is the minimum acceptable level of observation for all inpatients. The location of patients should be known to staff at all times, but not all patients on Level 1 need to be kept within sight of health care staff. Patient wellbeing and welfare will be monitored through intentional rounding and routine observations which should be recorded on Intentional Rounding documentation and in Nursing evaluations on every shift.
6 Level 2 Observation Examples of patients who need this level of observation are patients who are at risk of removing medical devices, patients who are at moderate risk of falling and also patients who are liable to wander. If the Enhanced Care risk assessment indicates that the patient needs this level of observation then the following interventions should be implemented:
Moving or locating the patient(s) closer to the nurse’s station for observation or consider a side room to reduce stimulation if this is considered to be safe for the patient. Patients who require level 2 observations can be given privacy when using the bathroom, and do not require observation whilst washing, dressing and toileting, if the individual completing the risk assessment does not feel that the patient could be left alone, this may be indicative of a higher score and that person should be re-assessed.
Cohorting patients of the same sex if appropriate, and if they have no known infection risk
Using equipment / assistive technology to lower the risk to the patient. e.g. low rise beds, falls alarms, bed safety rails, nasal bridles/safety mittens to prevent dislodgement of feeding tubes or cannula/catheters.
Reviewing the skill mix on the shift and within the specialty to support the requirement for closer observation and increase the frequency of intentional rounding.

Version 1 Document Enhanced Care Policy Page 6 of 35 Date March 2017 Next Review Date March 2018
Ensure that the area surrounding the bed is free from hazards and clutter.
Refer to the Delirium ‘’Policy for the Diagnosis, Management and
Prevention of Delirium (Acute Confusion) (2016)’’ to ensure the appropriate
strategies in caring for this group of patients are adopted.
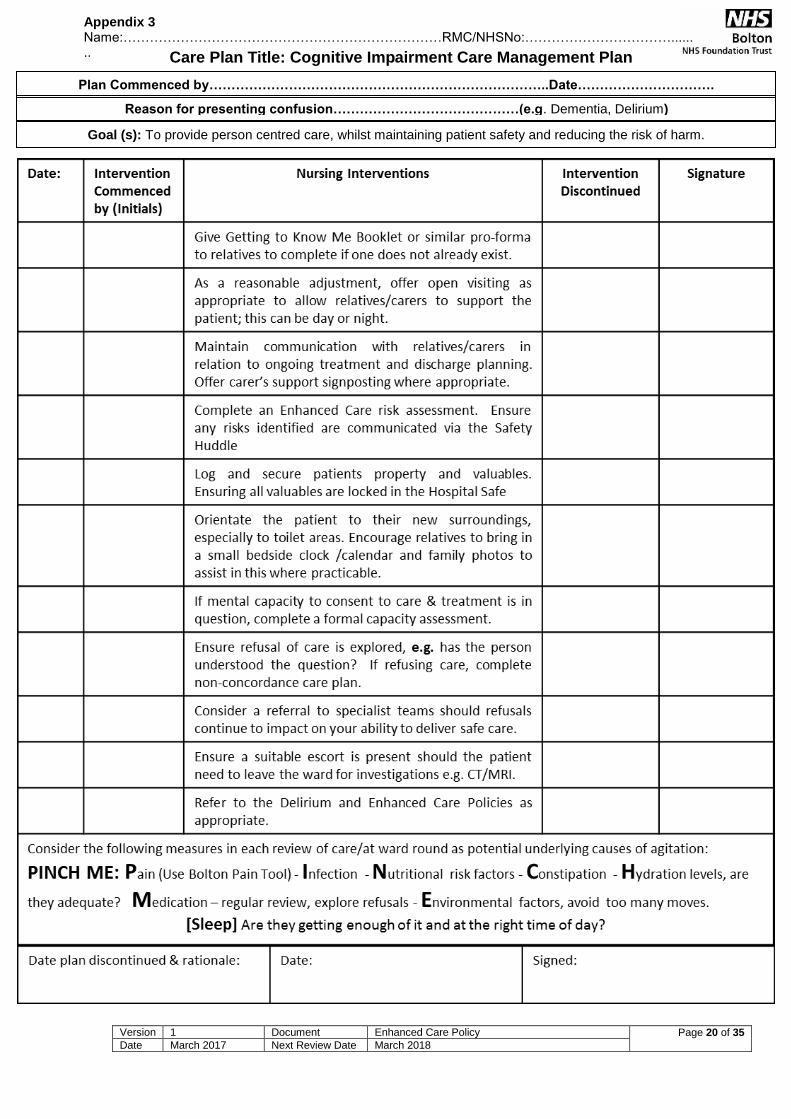
Complete and implement the Cognitive Impairment Care Management Plan
(Appendix 3) where appropriate.
In all cases where Enhanced Care is required, an Enhanced Supervision Record (Appendix 4) should be completed and updated every hour to detail the patient’s activity, and any intervention that was provided by Nursing staff.
7 Level 3 Observation Examples of patients who need this level of observation are patients who are at risk of removing medical devices with serious implications, patients who are at risk of falling and also patients who are liable to wander. If the Enhanced Care risk assessment indicates that the patient needs this level of observation, then the following interventions should be implemented:
‘Bay Tagging’ - Staff member present at all times in the bay / room, and patients always visible to the member of staff
Moving or locating the patient(s) closer to the nurse’s station for observation or consider a side room to reduce over-stimulation
Cohorting patients of the same sex if appropriate and if they have no known infection risk
Using equipment/assistive technology to lower the risk to the patient. e.g. falls mats, low rise beds, nasal bridles/safety mittens to prevent dislodgement of feeding tubes or cannula/catheters. Assistive technology includes the use of ‘My Life’ software and activity boxes to support reminiscence with patients.
Ensure that where bed rails are indicated, that the appropriate risk assessment has been carried out as set out in the ‘’Using Bed Rails Safely Policy’’.
Reviewing the skill mix on the shift and within the specialty to support the requirement for closer observation and increase intentional rounding
Consider offering open visiting to family members if the patient is settled in their presence, and make reasonable adjustments to support this.
Refer to the ‘’Policy for the Diagnosis, Management and Prevention of Delirium (Acute Confusion)’’ and implement the Cognitive Impairment Care Management Plan (Appendix 3) to ensure the appropriate strategies in caring for this group of patients are adopted.
If indicated, referral to RAID, Dementia and Learning Disabilities Specialist Nurses for specialist advice regarding patient management
Staff should ensure that the patient is informed of the reason for close observation, and that staff introduce themselves to the patient and inform them of the reason for
Version 1 Document Enhanced Care Policy Page 7 of 35 Date March 2017 Next Review Date March 2018
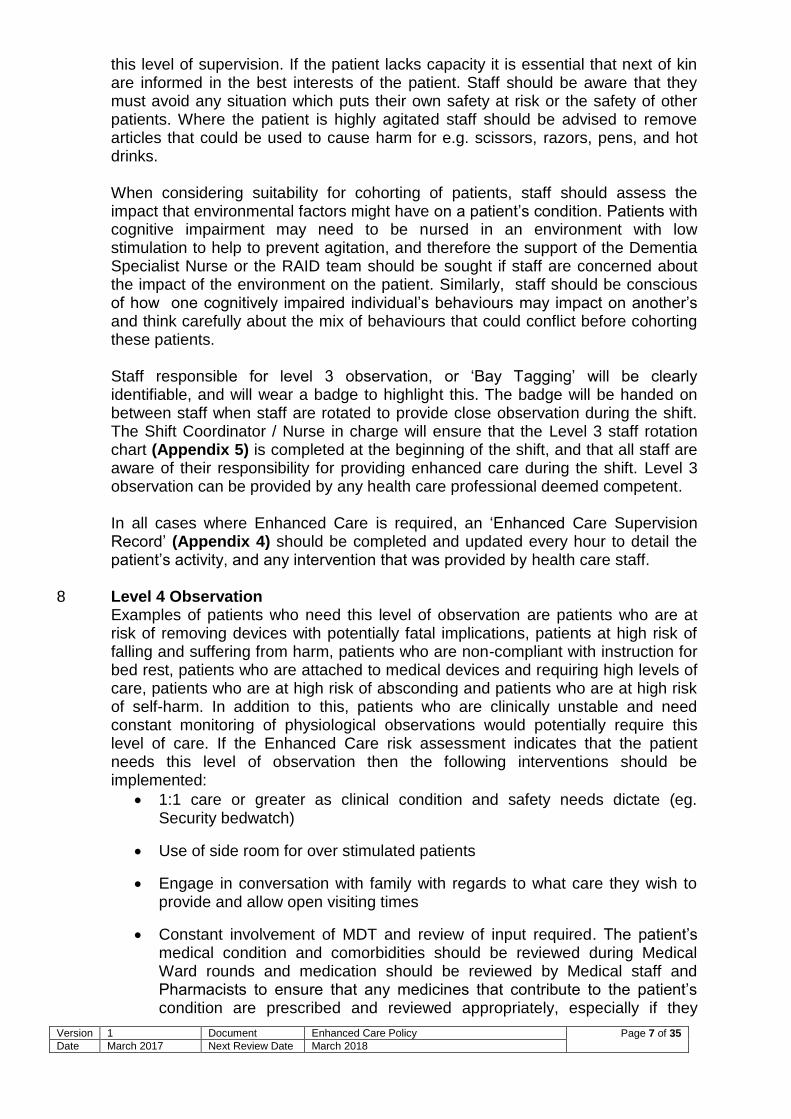
this level of supervision. If the patient lacks capacity it is essential that next of kin are informed in the best interests of the patient. Staff should be aware that they must avoid any situation which puts their own safety at risk or the safety of other patients. Where the patient is highly agitated staff should be advised to remove articles that could be used to cause harm for e.g. scissors, razors, pens, and hot drinks. When considering suitability for cohorting of patients, staff should assess the impact that environmental factors might have on a patient’s condition. Patients with cognitive impairment may need to be nursed in an environment with low stimulation to help to prevent agitation, and therefore the support of the Dementia Specialist Nurse or the RAID team should be sought if staff are concerned about the impact of the environment on the patient. Similarly, staff should be conscious of how one cognitively impaired individual’s behaviours may impact on another’s and think carefully about the mix of behaviours that could conflict before cohorting these patients. Staff responsible for level 3 observation, or ‘Bay Tagging’ will be clearly identifiable, and will wear a badge to highlight this. The badge will be handed on between staff when staff are rotated to provide close observation during the shift. The Shift Coordinator / Nurse in charge will ensure that the Level 3 staff rotation chart (Appendix 5) is completed at the beginning of the shift, and that all staff are aware of their responsibility for providing enhanced care during the shift. Level 3 observation can be provided by any health care professional deemed competent. In all cases where Enhanced Care is required, an ‘Enhanced Care Supervision Record’ (Appendix 4) should be completed and updated every hour to detail the patient’s activity, and any intervention that was provided by health care staff.
8 Level 4 Observation Examples of patients who need this level of observation are patients who are at risk of removing devices with potentially fatal implications, patients at high risk of falling and suffering from harm, patients who are non-compliant with instruction for bed rest, patients who are attached to medical devices and requiring high levels of care, patients who are at high risk of absconding and patients who are at high risk of self-harm. In addition to this, patients who are clinically unstable and need constant monitoring of physiological observations would potentially require this level of care. If the Enhanced Care risk assessment indicates that the patient needs this level of observation then the following interventions should be implemented:
1:1 care or greater as clinical condition and safety needs dictate (eg. Security bedwatch)
Use of side room for over stimulated patients
Engage in conversation with family with regards to what care they wish to provide and allow open visiting times
Constant involvement of MDT and review of input required. The patient’s medical condition and comorbidities should be reviewed during Medical Ward rounds and medication should be reviewed by Medical staff and Pharmacists to ensure that any medicines that contribute to the patient’s condition are prescribed and reviewed appropriately, especially if they

Version 1 Document Enhanced Care Policy Page 8 of 35 Date March 2017 Next Review Date March 2018
appear to be having adverse side-effects which may increase the patient’s risk of falls or acute confusion.
Using equipment/assistive technology to lower the risk to the patient. e.g. low rise beds, bed safety rails, nasal bridles/safety mittens to prevent dislodgement of feeding tubes or cannula/catheters. As with level 3 observation, assistive technology includes the use of ‘My Life’ software and activity boxes to support reminiscence with patients
Consider use of Registered Mental Health Nurse to provide specialist nursing intervention as deemed appropriate, and in all cases a referral to the RAID service for advice regarding management of condition and behavioural interventions that will help to support the provision of care especially if patient detained under the Mental Health Act
Refer to the Delirium Policy and implement the Cognitive Impairment Care Management Plan to ensure the appropriate strategies in caring for this group of patients are adopted, and if indicated, referral to Dementia Specialist Nurse for specialist advice regarding patient management
Development of an individualised care / management plan that is clearly documented, and is available at the patient’s bedside for staff to refer to
The use of physical restraints will only be used within the ICU/HDU as per their local policy ‘Physical restraint in critical care’ (July 2015) Level 4 Observation can be provided by Healthcare Assistants, unless the patient is deemed to be at risk of acute deterioration in which case a Registered Nurse would be required to provide 1:1 care. In these cases, the patient should have been reviewed by the Medical team with a view to escalation of care to a higher dependency area. Ensure that staff introduce themselves to the patient and inform them of the reason for level 4 observation. If the patient lacks capacity, to consent to their care and treatment, it is essential that a formal mental capacity assessment is completed. Further guidance on the management of patients lacking capacity can be found on page 10, section 12. Staff should be aware that they must avoid any situation which puts their own safety at risk or the safety of other patients. Where the patient is highly agitated staff should be advised to remove articles that could be used to cause harm for e.g. scissors, pens, and hot drinks. Staff responsible for level 4 observation will be clearly identifiable, and will wear a badge to highlight this. The badge will be handed on between staff when staff are rotated to provide level 4 observation during the shift. The Shift Coordinator / Nurse in charge will ensure that the staff rotation chart (Appendix 6) is completed at the beginning of the shift, and that all staff are aware of their responsibility for providing enhanced care during the shift. This should be retained on the ward as a record of the staff involved in the care of a patient on enhanced care. In all cases where Enhanced Care is required, a Sleep / Activity chart should be completed and updated every hour to detail the patient’s activity, and any intervention that was provided by Health Care staff.
Version 1 Document Enhanced Care Policy Page 9 of 35 Date March 2017 Next Review Date March 2018
9 10
Staff Interventions – Level 3 and 4 Observation As far as is reasonably practicable, staff must ensure that the level of care given is least restrictive, with patients offered the opportunity to make their own choices where possible, within the context of their situation. Distraction is a very useful way to settle patients with anxiety or fear, agitation or restlessness and wandering. If the patient finds interest in a game or activity let them play or use it how they see fit. Discuss the patient’s interests with relatives and carers and incorporate these into the patient’s management plan to ensure that it is holistic and patient centred. Exercise such as walking may help if the patient is bored or if there is too much going on around them. If the patient is not at high risk of falling and is safe to mobilise, support the patient to do so. Use large signs to help to orientate the patient. Encourage relatives to bring in a small clock or calendar to help with orientation to time and place, pack away any belongings such as hat/coat/umbrella which may prompt the person to leave. Keep plenty of space between you and the patient. Aggressive or angry patients need more space because they may feel scared when people come close to them, and may want to protect themselves. If it is safer to discreetly observe then this should be considered. This is a judgement that must be made carefully at the time based on the level of aggression a patient may be exhibiting. Where patients refuse care and intervention, please refer to the Management of the Non-Concordant Patient Policy (2017) and where medications are being refused specifically, refer to the Administration of Covert Medications Policy (2016). Use of the Challenging Behaviour Record (ABC Chart) and Bolton Pain Tool (BPAT) At times a patient receiving Enhanced Care may demonstrate behaviours that are particularly challenging for them and the multi-disciplinary team caring for them. Examples of this might include verbal or physical aggression to staff, relatives or other patients, persistent attempts to leave ward in a short space of time despite attempts to dissuade them, a period of sexually inappropriate behaviour or lack of inhibition, or an acute period of delirium. At such times it is essential to try and identify what the trigger factors are in order to try and prevent future ones. To assist this process, it is expected that the nurse providing the enhanced care will complete the Bolton Pain Tool (Appendix 7) to determine whether the patient’s actions stem from unresolved or undiagnosed pain which they are unable to communicate verbally or express in a manner that is clearly implied. It is also essential that the “Challenging Behaviour Record” (ABC Chart) (Appendix 8) be used, to document the behaviours observed around a particular event. This should be retained in the medical records to support assessment of the patient’s behaviour and assist team efforts to prevent future similar episodes. It is beneficial to include as much information as possible on this form.
Version 1 Document Enhanced Care Policy Page 10 of 35 Date March 2017 Next Review Date March 2018
11 12
As well as the challenging behaviour record, if a patient displays behaviours that are of risk to themselves or others (such as physical or verbal aggression, attempting to abscond) then this should be reported as an adverse incident on Safeguard. Involvement of Relatives in Enhanced Care
It is recognized that in many circumstances, patients who are confused or have cognitive impairment often respond well to support provided by their relatives. Information gathering around how the patient functions in their home environment and what methods family and carers employ in making patients feel safe is essential to reducing refusals and providing person centred care. For persons with dementia, complete a Getting to Know Me Booklet with the relative if present or in the case of patients with a learning disability a ‘’Keep Me Safe in Hospital document must be used. Consider also asking the next of kin if they wish to support the provision of Enhanced Care if this is appropriate and in the best interests of the patient. This should not be an expectation and should be discussed with the family / next of kin and details of any discussion should be documented in the patient’s Medical records. It is important that when considering the use of relatives to provide Enhanced Care, staff consider whether this would place either the patient or relative at risk of harm. If this is a possibility, relatives should not be asked to support Enhanced Care. When it is deemed that a patient required Enhanced Care, consideration should also be made for the impact that increased observation or supervision may have on the patient’s relatives or carer. The close proximity of Nursing staff when providing Level 4 care should be explained clearly to relatives and carers because this could be considered to be intrusive. Altered behaviours are likely to be distressing for patients, relatives and carers and therefore they will need to be fully involved in the assessment and planning of care, and provided with reassurance accordingly. The patient’s next of kin / Carer should also be provided with an Enhanced Care leaflet which explains the process in more detail, these are available on BOB>A-Z of Services>D>Dementia & Delirium>Information Leaflets or in printed form through Integra. Mental Capacity Assessment and Deprivation of Liberty (DoLS) A mental capacity assessment should be completed and a Deprivation Liberties Safeguard considered if the patient meets the following criteria (the ‘’Acid Test’’ MCA 2005)
The person is lacking the capacity to consent to their current care and treatment
Is under constant supervision directly or indirectly
Are not free to leave If all three criteria are met, impose a Deprivation of Liberty Safeguard, following the DoLS Policy (2005) and Implement the DoLS Care Plan (Appendix 9). THE RESTRICTION OF PATIENT ACTIVITY AND PROVISION OF 1:1 SUPERVISION IS EFFECTIVELY A DEPRIVATION OF LIBERTY AND IN ALL CASES WHERE PATIENTS NEED ADDITIONAL SUPERVISION / 1:1 SUPERVISION, A DEPRIVATION

Version 1 Document Enhanced Care Policy Page 11 of 35 Date March 2017 Next Review Date March 2018
13
OF LIBERTY SAFEGUARD APPLICATION SHOULD BE CONSIDERED.
Staffing and Skills Registered Nurses and Healthcare Assistants who are employed substantively at Bolton NHS Foundation Trust will receive Conflict Resolution Training and Dementia training/e-learning as part of their mandatory / statutory training. Healthcare Assistants should also complete the Enhanced Care workbook. Newly recruited Healthcare Assistants will be provided with Enhanced Care training through the Care Certificate Programme that is provided within the initial 6 months of employment. A record of the staff who have completed this training should be maintained on the Ward. Staff should also be familiar with the use of ‘My Life’ software as a diversionary tool. Other training related to communication such as ‘Sage and Thyme’ may be useful and can be accessed by contacting the End of Life Care Education Team. There may be circumstances where staff are asked to provide enhanced care before they have completed the Enhanced Care training or the Enhanced Care workbook. On such occasions the Nurse in Charge should consider the ability of the member of staff in the context of managing the patient’s condition to determine whether it would be appropriate for them to provide the patient with supervision. The Nurse in Charge should also confirm with the staff member that they feel confident to provide enhanced care. If it is agreed that temporary staffing is required to support the provision of Enhanced Care, consider what competencies or skills are required to care for the patient safely. In most cases, Ward staff will be more familiar with the individual and have the skills necessary to support Enhanced Care and diffuse challenging situations. In light of this, locum staff should not be allocated responsibility for the provision of Enhanced Care as a first option, and not at all If they are not compliant with mandatory training requirements. Where temporary staffing may be required to support Ward staffing to enable the provision of Enhanced Care, please refer to the temporary staffing policy for booking additional staff. Ensure that the members of staff providing Enhanced Care receive a full report on the patient’s condition, the rationale for this level of care and a summary of concerns and risk factors. This should also be repeated at every safety huddle, ward handover and at rotation of the staff member providing Enhanced Care. All staff should receive a handover of all other patients on the ward. All staff should have access to patient management plans which should be explained in detail to ensure staff understanding of these plans. All staff allocated responsibility for the provision of Enhanced Care will be rotated after a maximum of 2 hours or after any incident that they have found very challenging. The allocation of the staff member providing enhanced care is part of the essential responsibilities of the shift coordinator. The rotation sheet should be completed at the start of the shift, and communicated to all staff. It is recognized that this may be changed during the course of the shift

Version 1 Document Enhanced Care Policy Page 12 of 35 Date March 2017 Next Review Date March 2018
14
Ensure that support and assistance from other members of the team are available as required and that those providing Enhanced Care are informed as to how to get help in an emergency. All concerns or incidents involving patients who need close observation or additional supervision should be reported to the Nurse in charge, and reported though the Safeguard system. The Security Manager should be informed of patients with particularly challenging behavior in the event of security calls. The shift coordinator should ensure that those patients lacking in capacity should have this documented in the patient’s medical records. Discontinuation of Enhanced Care Nursing staff should ensure that patients who require Level 2 observation and above receive daily risk assessment to determine their ongoing level of observation. The outcome of the risk assessment should be communicated to team members so that they are aware and can support patients as necessary. If it is identified that the level of observation required is decreased and that the patient no longer requires ongoing supervision, this should be clearly documented in the patient’s Medical and Nursing records. This should also be communicated to the Nursing team, and to the patient and relatives / carer. A short summary of the guidance and actions given in this policy can be found in Appendix 10 which can be printed and given to staff as a daily work list.
15 Process for requesting a Staff Member for Enhanced Care
If a patient requires Level 4 care and this cannot be provided within the Ward establishment, or patients require Level 3 care and bay supervision cannot be provided then the shift coordinator should escalate this to the Matron for the area (outside of working hours, staff should contact the Band 7 on – call or the Late Matron / Site Coordinator) who will review staffing levels across the Division to identify whether support can be provided from another area within the Division or the Trust. The Senior Nurse should attend the Ward to review the risk assessment. If additional staff are required, the shift coordinator should complete a request for additional staffing following the guidance in section 16 below and escalate this to the Matron (Late Band 7 or Late Matron / Site Coordinator outside of working hours) for authorisation. Following authorisation, a request for additional staffing will be submitted electronically to the Workforce Department who will submit the shift requests to be fulfilled. Any assessment should consider the level of support the patient requires at different times of the day whilst this could vary according to the time of day / night.
16 Management of Staffing to provide enhanced care appropriately
-Step 1 Ward Manager or Nurse in Charge of shift should:

Version 1 Document Enhanced Care Policy Page 13 of 35 Date March 2017 Next Review Date March 2018
Review the staffing numbers, skill mix and specific competencies of Ward Nurses on duty. They should also ensure that the actual staffing numbers are accurately displayed on the Ward staffing board.
Ensure Enhanced Care risk assessments are up to date and complete
Make a professional judgement about the ability of the team to manage the workload and any known changes in patients and / or dependency or reduced numbers of staff.
Allocate staff to patient workload in the most efficient manner
Assess the need for additional staff and if required, review rota in relation to staff rostered on days off, study leave and other leave to assess if these are essential and may be changed.
Ensure that Matron is informed of staffing concerns.
If unable to escalate, proceed to Step 2
-Step 2 Ward Manager or Nurse in Charge of shift should:
In Hours:
Escalate to Matron when all actions in step 1 have been completed
Matron / Ward Manager to liaise with Division to consider redeployment of staff between Wards and Departments
If unable to redeploy staff then consider redeploying staff from other Divisions.
If not resolved then escalate to Divisional Nurse Director.
Out of Hours:
Escalate to Site Coordinator or Late Matron (Up until 9pm)
Site Coordinator/ Matron to liaise with other wards to consider redeployment of staff between wards and departments.
If unable to redeploy staff the Senior Manager on call (Tier 1) should be informed and should agree any actions arising from recommendations made to them.
The Senior Manager on call should inform the Executive on call should these issues remain unresolved.
Action Taken:
Contact Matron/Divisional Nurse Director to ascertain a broader perspective of available staff.
Review the rota in relation to staff rostered on days off, study leave and other leave to assess if these are essential and may be changed.
Matron/Divisional Nurse Director will review the unit provision of staffing and reallocate staff across the unit as necessary.
Ward Sister/Charge Nurse or Nurse in Charge will contact Bank to submit a request to provide additional bank staff. If this exceeds the available budget then permission from Matron must be sought first. The bank will liaise with ward first if bank staff are unavailable and agency staff are required. Authorisation for agency will only be agreed by the Matron.
Version 1 Document Enhanced Care Policy Page 14 of 35 Date March 2017 Next Review Date March 2018
Document all action and complete an incident form on the Safeguard System.
If the problem remains and safe skill mix/numbers as agreed are not achieved as a result of these actions, the following stage should be followed:
-Step 3 Staffing levels inadequate to manage current needs.
Matron/Divisional Nurse Director/Ward Manager (Monday- Friday 08:00 – 17:00)
hours should:
If bank or agency staff are unavailable then Matron to contact Divisional Nurse
Director to review Trust wide allocation of staff and liaise with peers to action staff
movement between wards and departments.
Consider distribution of nurses including Nurse Specialists and non-ward based
nurses etc.
Consider movement of patients/case mix/ dependency within the unit to safely
manage the patients within the available skill mix. Liaise with Divisional Nurse
Director.
Inform Divisional Nurse Director (who will decide if at this stage the Divisional
Director of Operations, Director of Nursing and Chief Operating Officer need to be
informed) with a view to moving patients across the trust +/- temporary closure of a
bed for less than 2 hours.
DDO to contact Director of Nursing and Chief Operating Officer to review the need
to reduce planned patient activity and the possibility of closing beds.
Document all actions and complete an incident report.
Site Co-ordinator/On Call Senior Manager (Out of Hours) should:
Review and ensure actions from earlier escalation are in place
Ensure Matron/Divisional Nurse Director have reviewed Trust wide staffing levels
and acuity together.
Contact “On Call” Senior Manager to review the need to redirect admissions and
the possibility of closing beds.
At no time will beds be closed without prior consultation with the Chief Operating Officer or the Director of Nursing “in hours” and the on-call Executive “out of hours

Version 1 Document Enhanced Care Policy Page 15 of 35 Date March 2017 Next Review Date March 2018
17 Monitoring Area to be Monitored
Methodology Who Reported To Frequency
Compliance with enhanced care risk assessments
Audit of enhanced care risk assessments
Matrons Divisional Governance Committee
Audit of Wards once per month for confirmation that risk assessments being completed daily, and for assurance regarding quality.
Audit of Safecare data entry to ensure that this reflects the need for and provision of enhanced care to patients
Audit of Safecare data
Matrons Workforce team / Divisional
Governance Committee
Weekly audits of Safecare data

Version 1 Document Enhanced Care Policy Page 16 of 35 Date March 2017 Next Review Date March 2018
Appendix 1 (Part A) Enhanced Care Risk Assessment Date of Assessment: Risk Assessment Score: This should be Completed Daily Cognition The patient is not confused The patient is confused, but is not agitated. The
patient is not at risk of harming self. The patient is confused and agitated. The patient requires frequent reassurance and reorientation to the environment. The patient is at risk of removing indwelling devices that are required to support patient care. The patient is at risk of harming self.
The patient is confused and agitated, with episodes of violence and aggression directed towards staff and / or other people. The patient has the potential to, or has displayed sexually disinhibited behaviour. The patient is at risk of removing indwelling devices, with life – threatening consequences.
0 1 2 3
Risk of Falls The patient is at low risk of falling. The patient is at risk of falling, but is able to
summon assistance to mobilise / has no history of falling.
The patient is at risk of falling, and is unable to understand the need to summon assistance to mobilise / has a history of falling.
The patient is at risk of falling, and is unable to understand the need to summon assistance to mobilise. The patient has a history of falling and is at high risk of harm as a result of falling.
0 1 2 3
Risk of Absconding The patient is able to leave the Ward / is not attempting to leave the Ward.
The patient needs to remain on the Ward for their safety, but is not attempting to leave the Ward. The patient is attempting to leave the Ward, and needs to remain on the Ward for their safety.
0 1 2
Clinical Condition The patient remains clinically stable and is not at risk of deterioration
The patient remains clinically stable with a low risk of deterioration.
The patient is at risk of deterioration and requires clinical observations recording at a frequency of >1hrly
The patient is clinically unstable, and requires constant monitoring of physiological observations.
0 1 2 3
Total Risk Score =
Level 1 Observation Level 2 Observation Level 3 Observation Level 4 Observation
Score 0 - 3 Score 4 - 7 Score 8 - 9 Score 10 - 11
THE RESTRICTION OF PATIENT ACTIVITY AND PROVISION OF 1:1 SUPERVISION IS EFFECTIVELY A DEPRIVATION OF LIBERTY AND IN ALL CASES WHERE PATIENTS NEED ADDITIONAL SUPERVISION / 1:1 SUPERVISION, A DEPRIVATION OF LIBERTY SAFEGUARD APPLICATION SHOULD BE CONSIDERED.
Addressograph Label

Version 1 Document Enhanced Care Policy Page 17 of 35 Date March 2017 Next Review Date March 2018
Appendix 1 (Part B)
Enhanced Care Overview
Level Of Observation Observation Required
Level 1 Intentional Rounding and Support - Hourly
Level of Observation Observation Required
Level 2 Minimum hourly observation and needs to be in an observable area
Document observations of condition and behaviour on Enhanced Supervision Record
Level of Observation Observation Required
Level 3 The patient should be visible at all times and needs ongoing monitoring and observation
A member of staff should be present in the bay at all times, and with the patient if they mobilise out of the bay
The patient should be assisted in the bathroom, and this should be discussed and agreed with the patient / relatives
Document observations of condition and behaviour on Enhanced Supervision Record
Level of Observation Observation Required
Level 4 1:1 or 2:1 care or greater, provided by an appropriately skilled member of staff
A member of staff should remain with the patient or at arm’s length at all times
The patient should be assisted in the bathroom, and this should be discussed and agreed with the patient / relatives
Document observations of condition and behaviour on Enhanced Supervision Record.
Document challenging behaviour on ‘Challenging Behaviour Record’
Ensure that the ‘Staff Rotation’ plans for Level 3 and Level 4 Observation are completed at the beginning of the shift, and that staff who are providing Enhanced Care are rotated on a two hourly basis accordingly

Version 1 Document Enhanced Care Policy Page 18 of 35 Date March 2017 Next Review Date March 2018
Appendix 1 Daily Review of Enhanced Care Risk: To be reviewed daily if patient triggers a score on the above matrix.
Date/ Time Cognition Risk of Falls
Risk of Absconding
Clinical Condition
Total risk score
Signature Comments

Version 1 Document Enhanced Care Policy Page 19 of 35 Date March 2017 Next Review Date March 2018
Appendix 2
Flowchart for Providing Enhanced Care The nurse in charge or nominated Registered Nurse will undertake a risk assessment of the patient
Two members of the Multi – Disciplinary / Nursing team
1) Agree level of observation required through assessment using Enhanced Care risk (Daily Assessment)
2) Agree responsibilities for undertaking observations, and agree rotation of staff on a 2hrly basis to support Enhanced Care
Level 1 Observation Level 2 Observation Level 3 Observation Level 4 Observation
Intentional Rounding – Check every hour
Patient will be observable, but can safely be given privacy
when in the toiler or bathroom with the door unlocked.
A member of staff will be present in the bay at all times. The patient will be observable at all times. The patient needs to be supervised when in the toilet or bathroom, and needs
to be supervised when mobilising.
The patient needs to be supervised at arms length at all
times on a 1:1 basis.
Level 1 Observation Levels 2, 3 and 4 Observation
Staff responsible for observation to:
Record checks on Intentional Rounding / Comfort tool
Record location of patient
At a minimum of once per shift, Registered Nurse to review the patient to ensure a review of Mental Capacity, associated behaviours, level of risk and record as a clinical entry on Enhanced Care documentation and in Nursing evaluation
Maintain principles of supportive observation
Discuss level of care required at Safety Huddle, and discuss behaviours and presentation at handover
Staff responsible for observation to:
Explain level of observation to patients and relatives, and develop care plan to clarify the support that should be provided to patients by staff to manage behaviours and reduce risk
At a minimum of once per shift, Registered Nurse to review the patient to ensure a review of Mental Capacity, associated behaviours, level of risk and records as a clinical entry on Enhanced Care documentation and in Nursing evaluation
Discuss level of care required at Safety Huddle, and discuss behaviours and presentation at handover
Version 1 Document Enhanced Care Policy Page 20 of 35 Date March 2017 Next Review Date March 2018
Appendix 3 Name:………………………………………………………………RMC/NHSNo:……………………………........
Plan Commenced by…………………………………………………………………..Date………………………….
Reason for presenting confusion……………………………………(e.g. Dementia, Delirium)
Goal (s): To provide person centred care, whilst maintaining patient safety and reducing the risk of harm.
Care Plan Title: Cognitive Impairment Care Management Plan

Version 1 Document Enhanced Care Policy Page 21 of 35 Date March 2017 Next Review Date March 2018
Care Plan Title: Cognitive Impairment Care Management Plan
Name: RMC/NHS No.:
Care Plan Number

Version 1 Document Enhanced Care Policy Page 22 of 35 Date March 2017 Next Review Date March 2018
LABEL
LABEL
LABEL
Care Plan Title: Cognitive Impairment Care Management
Plan
Name: RMC/NHS No.:
Care Plan Number

Version 1 Document Enhanced Care Policy Page 23 of 35 Date March 2017 Next Review Date March 2018
Appendix 4
Enhanced Supervision Record
Patient Name: Level of Observation:
RMC Number: Date:
Please document patient behaviour and activity within the chart below to enable the identification of trends in patient behaviour, or times of the day when patients may require additional support (Applicable to patients
receiving Levels 2 - 4 Observation)
Time Patient Behaviour / Interaction
Example Overview of Observation
What was the patient’s behaviour?
What support was needed?
Did anything trigger behaviour?
Did anything settle behaviour?
Concerns reported to?
Name and Signature of Observer
00:00hrs
02:00hrs
04:00hrs
06:00hrs
07:00hrs
08:00hrs
09:00hrs
10:00hrs
11:00hrs
12:00hrs
13:00hrs
14:00hrs
15:00hrs
Version 1 Document Enhanced Care Policy Page 24 of 35 Date March 2017 Next Review Date March 2018
16:00hrs
17:00hrs
18:00hrs
19:00hrs
20:00hrs
21:00hrs
22:00hrs
23:00hrs
Continuation

Version 1 Document Enhanced Care Policy Page 25 of 35 Date March 2017 Next Review Date March 2018
Appendix 5: Staff Rotation Plan – Level 3 Observation
Please indicate the name of the staff member who will remain in the bay to observe and supervise the patients deemed to need Level 3 observation in the table below, to ensure that staff are rotated
on a 2 hourly basis, and are aware of this.
Pt. Name: Ruby Tuesday
Bay Number: Bay Number: Bay Number: Bay Number:
Eg. 00:00hrs – 02:00hrs
Penny Lane
00:00 – 02:00hrs
Eleanor Rigby
02:00hrs – 04:00hrs
04:00hrs – 06:00hrs
06:00hrs – 08:00hrs
08:00hrs – 10:00hrs
10:00hrs – 12:00hrs
12:00hrs – 14:00hrs
14:00hrs – 16:00hrs
16:00hrs – 18:00hrs
18:00hrs – 20:00hrs
20:00hrs – 22:00hrs
22:00hrs – 00:00hrs

Version 1 Document Enhanced Care Policy Page 26 of 35 Date March 2017 Next Review Date March 2018
Appendix 6
Staff Rotation Chart – Level 4 Observation
Please indicate the name of the staff member who will provide 1:1 supervision for patients deemed to need Level 4 observation in the table below, to ensure that staff are rotated on a 2 hourly basis,
and are aware of this.
Pt. Name: John Doe
Pt. Name:
Example 00:00hrs – 02:00hrs
Penny Lane
00:00 – 02:00hrs
02:00hrs – 04:00hrs
04:00hrs – 06:00hrs
06:00hrs – 08:00hrs
08:00hrs – 10:00hrs
10:00hrs – 12:00hrs
12:00hrs – 14:00hrs
14:00hrs – 16:00hrs
16:00hrs – 18:00hrs
18:00hrs – 20:00hrs
20:00hrs – 22:00hrs
22:00hrs – 00:00hrs

Version 1 Document Enhanced Care Policy Page 27 of 35 Date March 2017 Next Review Date March 2018
Appendix 7
BOLTON PAIN ASSESSMENT SCALE
For patients with communication problems NAME OF PATIENT/PATIENT STICKER
……………………………………………………………. Date of Birth……………………WARD RMC/NHS Number………………………………………………………………..
SCORE NO PAIN
MILD MODERATE SEVERE
VOCALISATION
none
Occasional moan or groan
Intermittent shouting/moaning
Repeatedly crying out, loud moaning or crying
FACIAL EXPRESSION
Smiling or relaxed
Looking tense, Sad Frowning,
Grimacing and looks frightened
CHANGE IN BODY LANGUAGE
None Tense, fidgeting
Guarding. Withdrawn, rigid, fists clenched. Knees pulled up
BEHAVIOURAL CHANGE
None
Slight/intermittent confusion or agitation
Increased confusion or agitation
Severe agitation/aggression
PHYSIOLOGICAL CHANGE
Normal
Mild increase in heart or respiratory rate
Increased heart rate, respiratory rate and Bp
Continued changes in vital signs. Perspiring flushed or change in pallor.
PHYSICAL CHANGES
None Mild trauma, ie skin tears etc
Pressure ulcers, moisture lesions etc
Post surgery, trauma,
PAIN SCORE
Predominantly
WHITE = NO PAIN 0
Predominantly GREEN
= MILD PAIN 1
Predominantly AMBER
=MODERATE PAIN 2
Predominantly RED
= SEVERE PAIN 3
Date & Time
Pain Score
Family/Staff Comments Signature

Version 1 Document Enhanced Care Policy Page 28 of 35 Date March 2017 Next Review Date March 2018
Date & Time
Pain Score
Family/Staff Comments Signature

Version 1 Document Enhanced Care Policy Page 29 of 35 Date March 2017 Next Review Date March 2018
Appendix 8
Challenging Behaviour Record (ABC Chart)
Date / Time
What was the patient doing just before the incident? (A – Antecedent)
Where did the incident occur?
What did you observe? (B – Actual Behaviour)i.e – touching staff inappropriately, verbal or sexual references, touching self in
public
Which staff were involved?
What did they say at the time of the incident?
How did they appear at the time of the incident? (You can circle more than one)
Angry Content Frightened Irritable
Anxious Depressed Frustrated Physically Unwell
Bored Despairing Happy Restless
Sad Worried Disorientated
How did staff respond? How was the situation resolved? (C – Consequences)

Version 1 Document Enhanced Care Policy Page 30 of 35 Date March 2017 Next Review Date March 2018
Appendix 9
CARE PLAN NUMBER ……………………………………………. Bolton NHS Foundation Trust
CARE PLAN TITLE: Patient has a Deprivation of Liberty Authorisation and Lacks Capacity.
Care plan is only to be used on those patients with a deprivation of liberty safeguard authorisation.
PATIENT’S NAME ………………………………………………….NHS NUMBER…………………….... WARD ………
Plan Commenced by ………………………………………… Date…………………………………….
Problem: The patient has a deprivation of liberty safeguard authorisation and lacks capacity due to Dementia / Delirium / withdrawal from alcohol which may impact on safety and nursing care.
Goal (s): To promote independence within a safe environment. To maintain safety.
Date: Intervention Commenced by
Nursing Interventions: Intervention Discontinued
Signature
At all times give constant reassurances to ……………………. and try to orientate to date, time and place.
Encourage ………………………… to make own decisions but prompt where necessary regards diet choice, personal hygiene / clothes to wear.
All ward staff to be aware of …………………….. inability to maintain his / her own safety.
Provide (tick as appropriate)
1:1 nursing care Indirect observation / supervision . Direct observation / supervision
Keep ward doors closed at all times.
Do not allow patient to leave ward /clinical area unless accompanied by a responsible other e.g. member of staff, relative or carer and they are assessed as safe to be with patient.
If …………………….. leaves the ward unaccompanied, Hospital Security, Police, Matron and Site Co-ordinator must be informed – vulnerable adult.
Member of the multi-disciplinary team to review capacity assessment at least daily.
Review staffing and complete ‘one to one’ care and assessment form if additional staff are required.
Discuss the plan of care with the patient’s relatives/carer.
The person is not free to leave.
Version 1 Document Enhanced Care Policy Page 31 of 35 Date March 2017 Next Review Date March 2018
CARE PLAN CONTINUED: CARE PLAN NUMBER ……………………………………………. Bolton NHS Foundation Trust
CARE PLAN TITLE: Lack of Capacity due to Dementia / Delirium / Alcohol Withdrawal
PATIENT’S NAME ………………………………………………….NHS NUMBER…………………….... WARD ………
Date: Intervention
Commenced by
Nursing Interventions: Intervention Discontinued
Signature
Date plan discontinued & rationale:
Date: Signed:

Version 1 Document Enhanced Care Policy Page 32 of 35 Date March 2017 Next Review Date March 2018
Appendix 10
Enhanced Care Summary Checklist Name…………………….RMC Number…………………….Ward…………………….
SECTION 1: IMMEDIATE ACTIONS TO ASSESS AND REDUCE RISKS Please tick -Yes or No
Yes No Recent medical review (within 48 hrs & must include review of current medication?
If No – Request review
Is the patient displaying any of the following behaviors? Pulling at tubes or lines, wandering and confused, unsteady and risk of falling, attempting to abscond or agitated and / or aggressive
Document in notes
Have the appropriate referrals been made to the multi-disciplinary team?
Is there a clear multi-disciplinary management plan?
If No – Make referrals and use triggers to develop a management plan
Falls risk assessment been completed?
Does the patient have a history of falls during this episode?
If Yes record number of falls? Is patient on a Rambleguard fall mat?
Is there a current substance misuse problem? If Yes refer to RAID for support / alcohol team
Have environmental concerns been considered? i.e. over stimuli , side room available
If No – Reduce environmental stimuli Move to a side room or to a more observable position etc
Can patient be cohorted? If No - document reason
Does the patient require a mental capacity assessment ?
If Yes – complete one
Can the patient’s care be safely maintained within usual staffing levels?
If No - Proceed to Section 2
Discharge Date If yes state Date
SECTION 2: RISK REASON & STAFFING RECOMMENDATION Please tick appropriate risk. This should be completed and signed by Ward Manager / Shift Coordinator, and then
the Matron
Consent should be considered for all patients No Risk / Reason Tick Recommended Level of Enhanced Care
1 Acutely ill / complex care requiring constant observation and intervention by RN
1:1 RN
2 Reduce the risk of falls requiring 1:1 observation
1:1 HCA
3 Confused and wandering presenting a risk to self and others (patient & staff)
1:1 HCA
4 Pulling lines / tubes that may result in significant harm (tracheostomy, PEG, IV)
1:1 HCA
5 Extreme challenging behavior (violence & aggression)
1:1 HCA Consider the use of 2 staff per patient
6 Expressing intent or recently attempted to self harm / suicide ideation
Immediate review with MDT and consider 2 HCA
Print Name: ……………………../………………………… Designation:…….………../…………… Sign: ………………………….…./…………………………. Date…………………. Date for review…………………..
The Ward Manager or Deputy and Matron must sign this form on the day of assessment
Version 1 Document Enhanced Care Policy Page 33 of 35 Date March 2017 Next Review Date March 2018
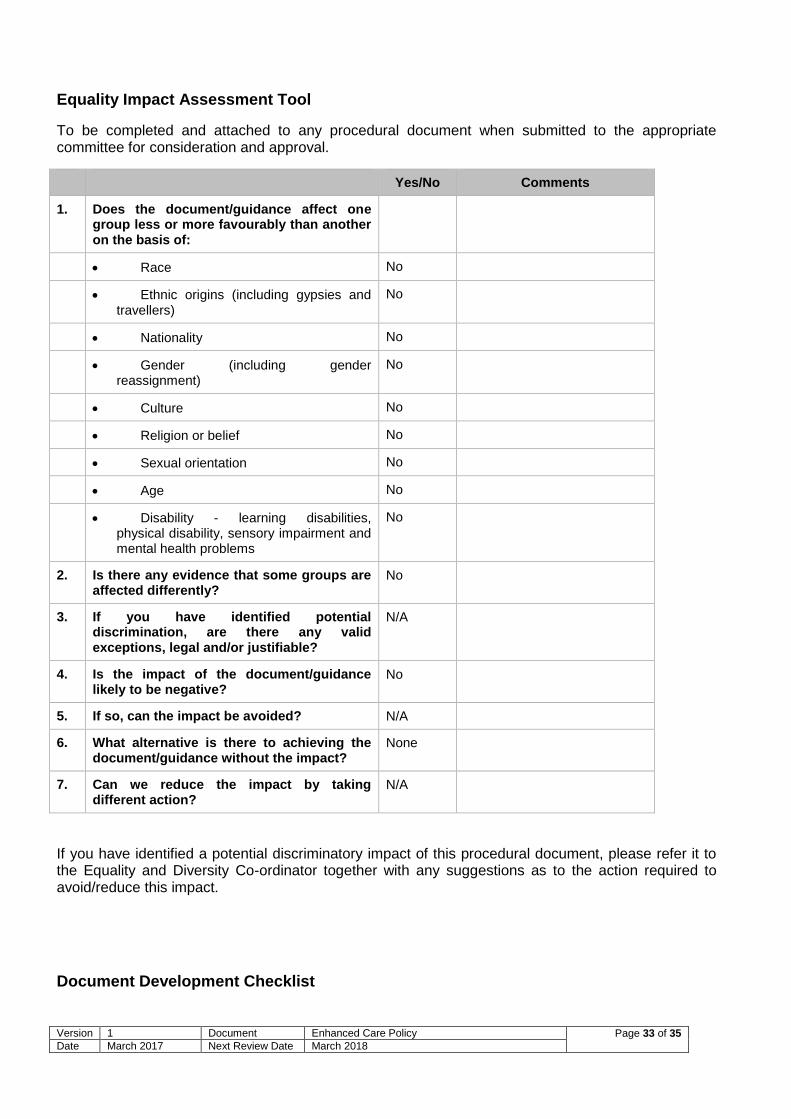
Equality Impact Assessment Tool
To be completed and attached to any procedural document when submitted to the appropriate committee for consideration and approval.
Yes/No Comments
1. Does the document/guidance affect one group less or more favourably than another on the basis of:
Race No
Ethnic origins (including gypsies and travellers)
No
Nationality No
Gender (including gender reassignment)
No
Culture No
Religion or belief No
Sexual orientation No
Age No
Disability - learning disabilities, physical disability, sensory impairment and mental health problems
No
2. Is there any evidence that some groups are affected differently?
No
3. If you have identified potential discrimination, are there any valid exceptions, legal and/or justifiable?
N/A
4. Is the impact of the document/guidance likely to be negative?
No
5. If so, can the impact be avoided? N/A
6. What alternative is there to achieving the document/guidance without the impact?
None
7. Can we reduce the impact by taking different action?
N/A
If you have identified a potential discriminatory impact of this procedural document, please refer it to the Equality and Diversity Co-ordinator together with any suggestions as to the action required to avoid/reduce this impact.
Document Development Checklist

Version 1 Document Enhanced Care Policy Page 34 of 35 Date March 2017 Next Review Date March 2018
Type of document Policy
Lead author: Paul Devlin
Is this new or does it replace an
existing document?
New document
What is the rationale/ Primary purpose
for the document
To provide guidance to staff regarding the
assessment process for identifying when patients
require additional supervision. The policy also aims
to provide teams with clear guidance regarding the
competency that staff should be provided with to
ensure the safe delivery of enhanced care.
What evidence/standard is the
document based on?
National Guidance for Patient Observation (NICE
2006)
Is this document being used anywhere
else, locally or nationally?
Other organisations have similar policies.
Who will use the document? Clinical teams responsible for the provision of
inpatient care.
Is a pilot run of the document required?
(optional)
Policy has previously been piloted prior to updates
and amendment, therefore no.
Has an evaluation taken place? What
are the results? (optional)
What is the implementation and
dissemination plan? (How will this be
shared?)
Detailed implementation plan to be confirmed. Policy
will be disseminated to staff through Ward /
Departmental meetings, and through the provision of
Enhanced Care training.
How will the document be reviewed?
(When, how and who will be
responsible?)
The document will be reviewed in 2018 following
formal evaluation of policy effectiveness.
Are there any service implications?
(How will any change to services be
met? Resource implications?)
The policy has potential resource implications in that
patients who may not have been provided with
Enhanced care previously may be identified as
requiring this.
Keywords (Include keywords for the
document controller to include to assist
searching for the policy on the Intranet)
Enhanced; Supervision; Specialling; Observation
Staff/stakeholders consulted Nursing staff within Acute Adult and Elective Care
Division
Safeguarding Lead Nurse
Dementia Nurse Specialist
Any document that gives an instruction to prescribe or administer a medicine should have that instruction reviewed by the senior divisional pharmacist
Signature of pharmacist:
Version 1 Document Enhanced Care Policy Page 35 of 35 Date March 2017 Next Review Date March 2018
before it goes for ratification.
EIA Attached at Appendix 7
Signed and dated
By validator
By ratifying officer
Paul Devlin
..................................................................................