endoscopic treatment of gerd - education · treatment of gastroesophageal reflux disease: a ......
TRANSCRIPT

Endoscopic Treatment of GERD Gary “Taavi” Reiss. MD, MPH, MBA, FACG
Metropolitan Gastroenterology Associates
LSU Health Sciences Center, Gastroentology
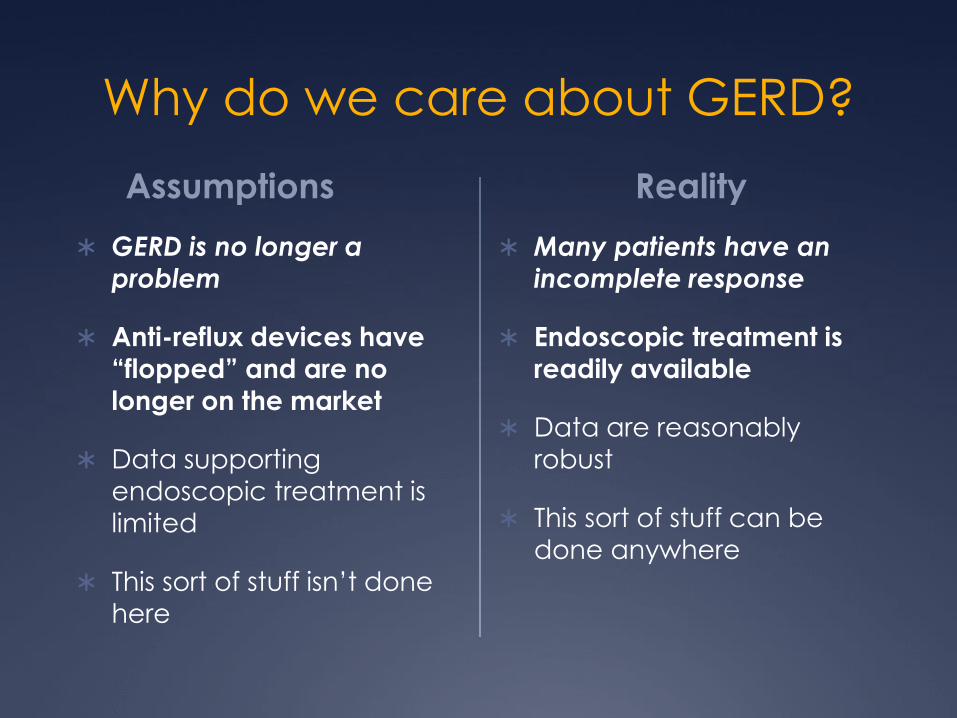
Why do we care about GERD?
Assumptions
GERD is no longer a
problem
Anti-reflux devices have
“flopped” and are no
longer on the market
Data supporting
endoscopic treatment is
limited
This sort of stuff isn’t done
here
Reality
Many patients have an
incomplete response to
medication
Endoscopic treatment is readily available
Data are reasonably
robust
This sort of stuff can be
done anywhere

GERD and PPI response
If you do well with a PPI, you will continue to do
well
Remission rates for PPI and Nissen fundoplication
equivalent five years out, with data trending
towards PPI trumping surgery
LOTUS trial, JAMA 2011;1969-1977.
30%-60% do not achieve complete remission; 28%
of these will not have reflux (normal acid and bile
exposure, normal EGD)
You will NEVER know if you don’t ask. Most of us
don’t ask.
Heartburn vs. Regurgitation
Heartburn has been the dominant
focus of symptom relief
Heartburn responds well to PPIs Therapeutic gain ~ 41%
31 RCTs; n = 9,457
Regurgitation as primary end-point 7 placebo controlled trials
Therapeutic gain = 17%
Kahrilas, Howden & Hughes, Am J Gastroenterol 2011; 106: 1419-1425.

GERD: So Simple, So Complex

Refractory Reflux: z/pH
57% 35%
8%
Refractory HB on BID
PPI
Functional Heartburn
Weakly Acidic Reflux
Acidic Reflux
Most patients are
functional
Functional HB dx
requires pH testing
(Rome IV)
Hypersensitive
esopahgus dx requires
pH testing (Rome IV)
Significant minority with
weakly acidic reflux
Mainie I et al. Gut, 2006; 55:1398-1402
Compliance / Patient
Perception Timing
50% of GERD patients are using PPI’s ‘on-demand’ after 4 weeks
70% of GERD patients are using PPI’s ‘on-demand’ after 3 months
15-20% of all medications refilled as indicated
~ 40% patients take > 1 hour before meals
~ 30% patients take AFTER meals
Concerns
Dementia
Cardiac disease
Infection
Osteopenia/osteoporosis
Kidney disease
Intolerance (diarrhea, headache)
www.nexiumlawsuit.com
Hershcovici T and Fass R Dis Esoph 2013;26:27-36
Gunaratnam et al. Aliment Pharmacol Ther 2006;23(10):1473-1477
Why do we care about GERD?
Assumptions
GERD is no longer a
problem
Anti-reflux devices have
“flopped” and are no
longer on the market
Data supporting
endoscopic treatment is
limited
This sort of stuff isn’t done
here
Reality
Many patients have an
incomplete response to
medication or do not take
medication (or will not)
Endoscopic treatment is
readily available
Data are reasonably robust
This sort of stuff can be
done anywhere
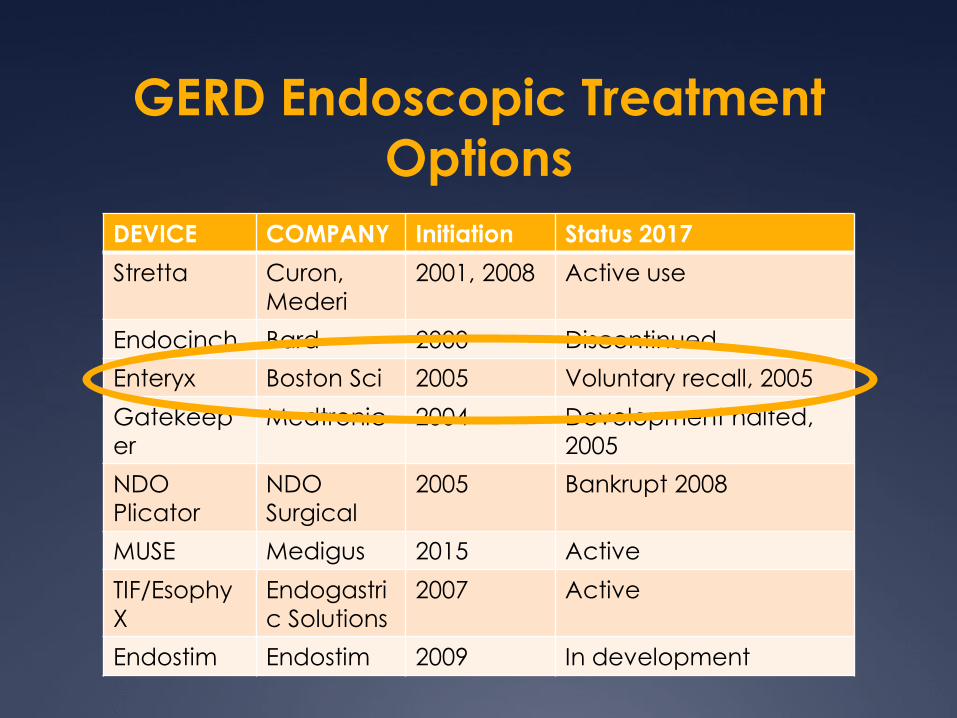
GERD Endoscopic Treatment
Options
DEVICE COMPANY Initiation Status 2017
Stretta Curon,
Mederi
2001, 2008 Active use
Endocinch Bard 2000 Discontinued
Enteryx Boston Sci 2005 Voluntary recall, 2005
Gatekeep
er
Medtronic 2004 Development halted,
2005
NDO
Plicator
NDO
Surgical
2005 Bankrupt 2008
MUSE Medigus 2015 Active
TIF/Esophy
X
Endogastri
c Solutions
2007 Active
Endostim Endostim 2009 In development

Available Options
Stretta
EsophyX / TIF 2.0
MUSE
Why do we care about GERD?
Assumptions
GERD is no longer a
problem
Anti-reflux devices have
“flopped” and are no
longer on the market
Data supporting
endoscopic treatment is
limited
This sort of stuff isn’t done
here
Reality
Many patients have an
incomplete response
Endoscopic treatment is
readily available
Data are reasonably
robust
This sort of stuff can be
done anywhere

Low power RF energy
delivered to tissue
“Stretta therapy remodels the musculature of the lower esophageal sphincter
(LES) and gastric cardia. Clinical studies demonstrate that the Stretta RF
treatment results in significant reductions in tissue compliance and
transient LES relaxations. These mechanisms act to restore the natural
barrier function of the LES as well as to significantly reduce spontaneous
regurgitation caused by transient inappropriate relaxations of the sphincter.”
Edward D. Auyang, Patrice Carter, Thomas Rauth, Robert D. Fanelli,
SAGES Guidelines Committee, Endoluminal Treatments for GERD, May 2013
Multi-level treatment remodels
LES and Gastric Cardia
Function improved, reduced
compliance, fewer TLESRs
Stretta - Procedure
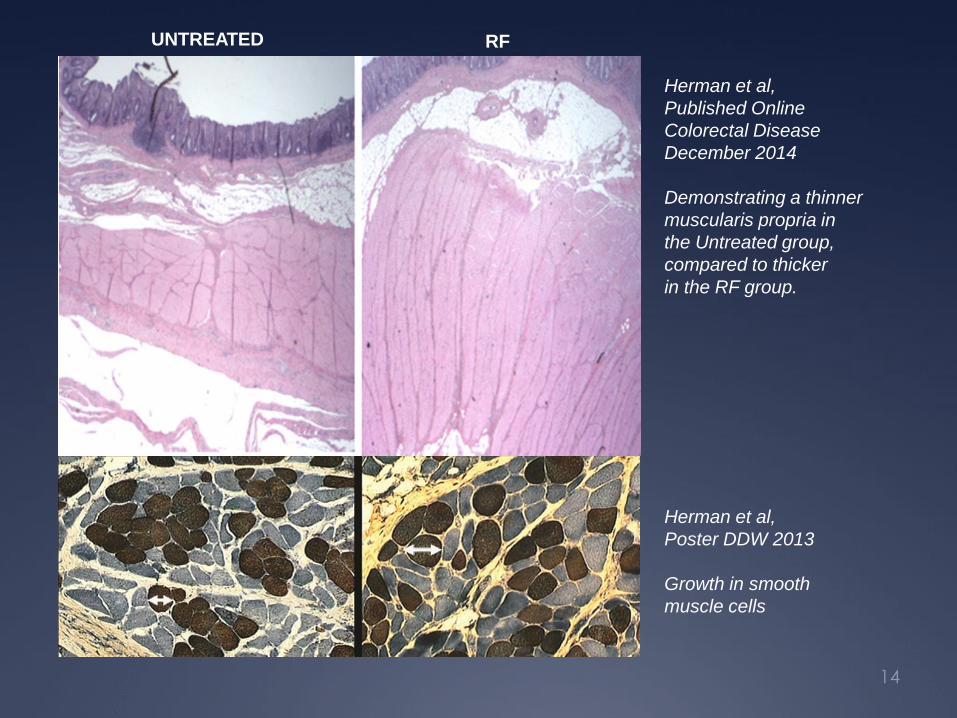
Herman et al,
Published Online
Colorectal Disease
December 2014
Demonstrating a thinner
muscularis propria in
the Untreated group,
compared to thicker
in the RF group.
UNTREATED RF
Herman et al,
Poster DDW 2013
Growth in smooth
muscle cells
14

Increase in thickness of the GE
junction – muscularis propria
Baseline control-
untreated
7 months
post-treatment
Kim M, GI Endoscopy 2003
Increased Thickness CANINES
De Angelis C, Repici A, Dughera L. UEGW 2004
Before Stretta
After Stretta 3 Months
HUMANS

INFLUENCE ON TLESR’S
A six month follow up on 20 patients
Corley et al. Gastroenterology 2003

Mechanism
Data Sample
Reduction in esophageal acid exposure
• Perry et al. 2012 – Surg Lap, Endo & Perc Tech
• Aziz et al 2010 – Curr Opin Gastroenterol - RCT
• Arts et al 2007 – Digestive Disease Science
• Mattar et al. 2006 – Surg Endosc
• Lufti et al. 2005 – Surg Endosc
• Cipoletta et al. 2005 – Surg Endosc
• Torquati et al. 2004 – Surg Endosc
• Triadafilopoulos et al. 2004 – Surg Endosc
• Houston et al. 2003 – Surg Endosc
• Richards et al. 2003 – Annals of Surgery
• Triadafilopoulos et al. 2002 – Gastrointest Endosc
• Corley et al. 2003 – Gastroenterology - RCT
Reduction in transient LES relaxations
• Arts et al. 2012 – Am Journal of Gastroenterol - RCT
• Tam et al. 2003 – Gut
• Kim et al. 2003 – Gastrointestinal Endosc
Decreased tissue compliance without fibrosis
• Arts et al. 2012 – Am Journal of Gastroenterol – RCT
Increase in LES wall thickness
• DiBaise et al. 2002 – Am Journal of Gastroenterol
• Chang et al. 2001 – Gastrointestinal Endosc
• Kim et al. 2003 – Gastrointestinal Endosc
Increased LES pressure
• Aziz et al. 2010 – Curr Opin Gastroenterol
• Meier et al. 2007 – Scandinavian Journal of Gastro
• Tam et al. 2003 – Gut
• Utley et al. 2000 – Gastrointest Endosc
“A comparison of patients before vs. after
treatment indicated that acid exposure
decreased significantly (median decrease,
2.4%; P =0.01) between baseline and 12
months for all treated patients (both initial
active treatment and crossed-over
patients).”
- Corley et al. 2003
“Stretta improved GERD symptoms and
decreased GEJ compliance. Decreased
GEJ compliance, which reflects altered
LES neuromuscular function, may
contribute to symptomatic benefit by
decreasing refluxate volume.”
- Arts et al. 2012
“At 12 months, the mean HRQL scores of
those off medications, the LES basal
pressure, the 24-hr pH scores, and the
proton pump inhibitor (PPI) daily dose
consumption were significantly improved
from baseline...”
- Aziz et al. 2009
Stretta - Criticism
Small studies
Too much potential for bias (only 4 RCT)
Physiologic data not robust
Too many single study sites
Concern that neuromodulatory effect may play a role
Discordance between timeframe of pH improvement and symptom improvement

Stretta is Safe & Efficacious
Results of Meta-Analysis
Outcome Variable Studies
(n)
Patients
(n)
Mean Follow-
up (mo)
Pre-
Stretta
Post-
Stretta
P-value
Subjective Measurements
GERD-HRQL 9 433 19.8 26.11 9.25 0.0001
QOLRAD 4 250 25.2 3.30 9.25 0.0010
SF-36 Physical 6 299 9.5 36.45 46.12 0.0001
SF-36 Mental 5 264 10.0 46.79 55.16 0.0015
Heartburn Score 9 525 24.1 3.55 1.19 0.0001
Satisfaction Score 5 366 21.9 1..43 4.07 0.0006
Objective Measurements
Esophageal Acid
Exposure (%pH<4)
11 364 11.9 10.29 6.51 0.0003
DeMeester score 7 267 13.1 44.37 28.53 0.0074
LES pressure 7 263 8.7 16.54 20.24 0.0302
•Perry et al. 2012 – Surg Lap, Endo & Perc Tech
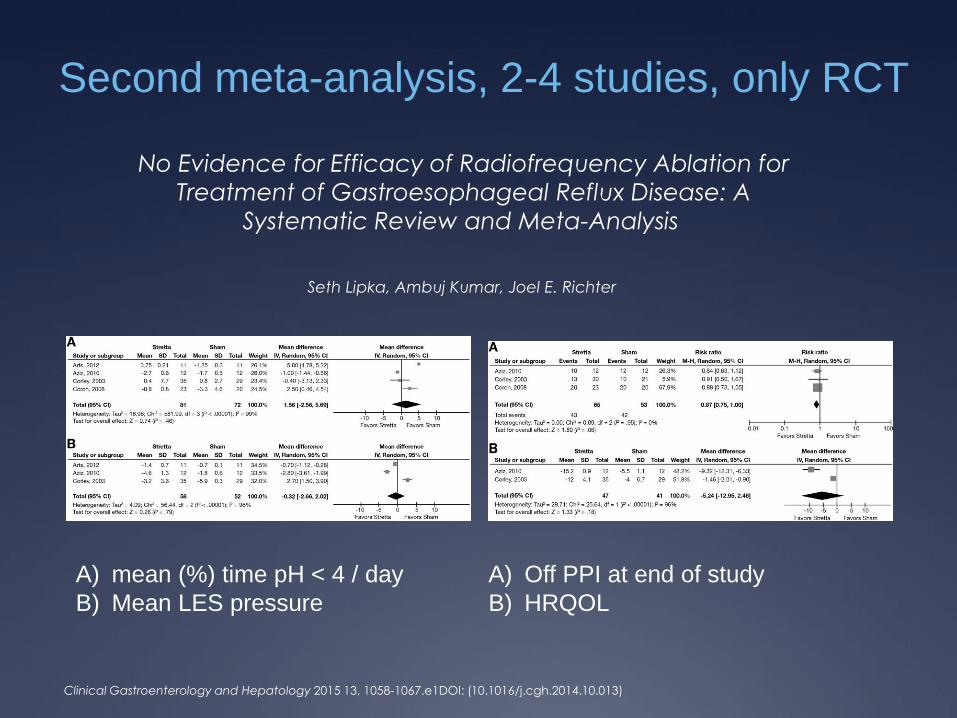
Second meta-analysis, 2-4 studies, only RCT
Clinical Gastroenterology and Hepatology 2015 13, 1058-1067.e1DOI: (10.1016/j.cgh.2014.10.013)
A) mean (%) time pH < 4 / day
B) Mean LES pressure
A) Off PPI at end of study
B) HRQOL
No Evidence for Efficacy of Radiofrequency Ablation for
Treatment of Gastroesophageal Reflux Disease: A
Systematic Review and Meta-Analysis
Seth Lipka, Ambuj Kumar, Joel E. Richter

New (Final?) Stretta Meta-Analysis 2017
Systematic Review and Meta-Analysis of Controlled
and Prospective Cohort Efficacy Studies of Endoscopic
Radiofrequency for Treatment of GERD
Ronnie Fass, Frederick Cahn, et al – Surgical Endoscopy Online 02/17
HIGH QUALITY – COMPREHENSIVE STUDY:
• Large size ranks in top 1% of Systematic Review/Meta-Analysis
• 28 Studies, 2468 Patients, up to 10-yrs follow-up (avg 25 months)
SUMMARY OF RESULTS: • Significant improvement in health related quality of life scores
• Significant reduction in heartburn symptom scores • The majority of patients off proton pump inhibitors (PPIs)
• Significant healing of erosive esophagitis
• Significant reduction in esophageal acid exposure • Low adverse event rate of <1%
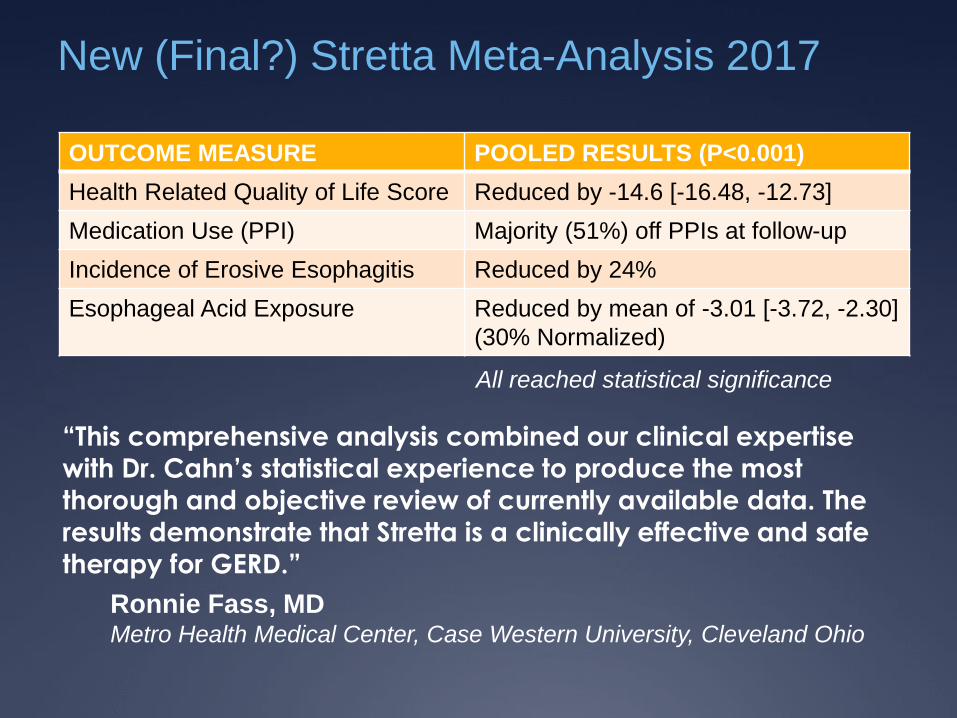
New (Final?) Stretta Meta-Analysis 2017
OUTCOME MEASURE POOLED RESULTS (P<0.001)
Health Related Quality of Life Score Reduced by -14.6 [-16.48, -12.73]
Medication Use (PPI) Majority (51%) off PPIs at follow-up
Incidence of Erosive Esophagitis Reduced by 24%
Esophageal Acid Exposure Reduced by mean of -3.01 [-3.72, -2.30]
(30% Normalized)
All reached statistical significance
“This comprehensive analysis combined our clinical expertise with Dr. Cahn’s statistical experience to produce the most
thorough and objective review of currently available data. The
results demonstrate that Stretta is a clinically effective and safe
therapy for GERD.”
Ronnie Fass, MD Metro Health Medical Center, Case Western University, Cleveland Ohio

SAGES CSR Guideline Gives Stretta
Strongest Grade Recommendation

ASGE Guidelines: June 2015
ENDOSCOPIC MANAGEMENT OF GERD
• Statements on Stretta: “Adverse events were infrequent and
typically minor. The technique appears to durably relieve GERD
symptoms for up to 10 years in the majority of patients…This
technique uses RF energy delivery to the distal esophagus and
appears to reduce GERD by decreasing tissue compliance and
reducing transient lower esophageal relaxations.”
Summary: Endoscopic antireflux therapy may be
considered for select GERD patients.
Gastrointest Endosc 2015;81:1305–1310 / DOI:
http://dx.doi.org/10.1016/j.gie.2015.02.021

Available Options
Stretta
EsophyX / TIF 2.0
MUSE
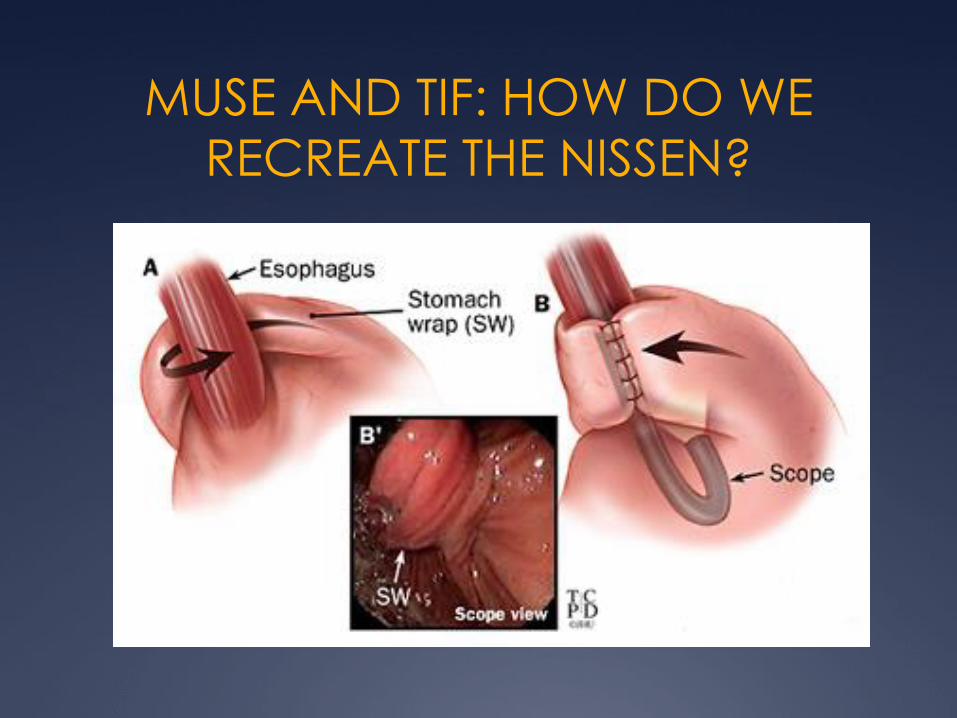
MUSE AND TIF: HOW DO WE
RECREATE THE NISSEN?
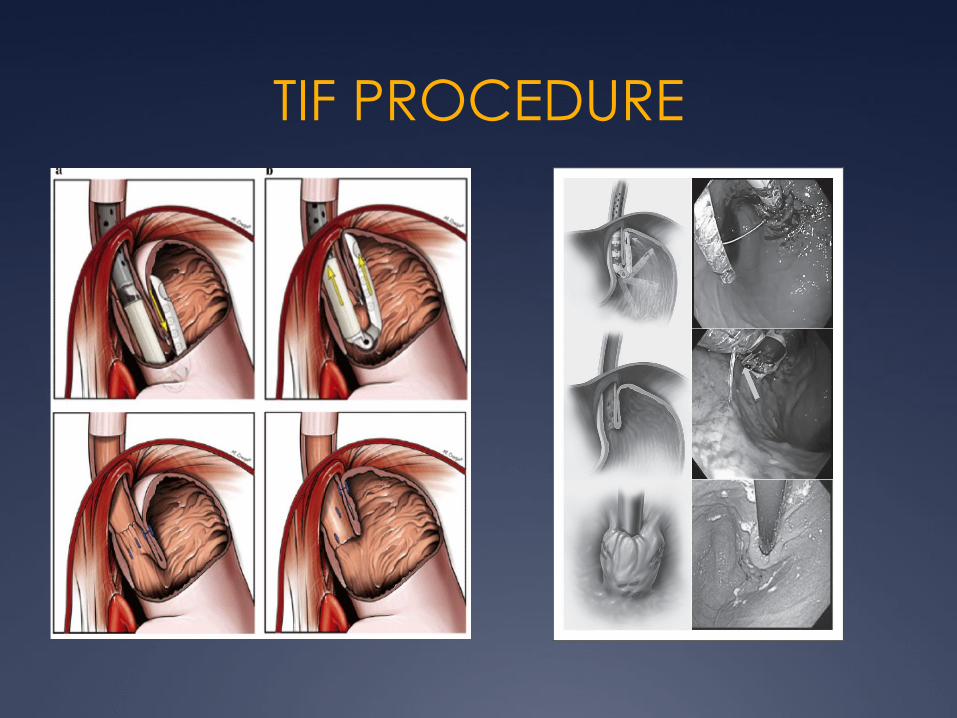
TIF PROCEDURE
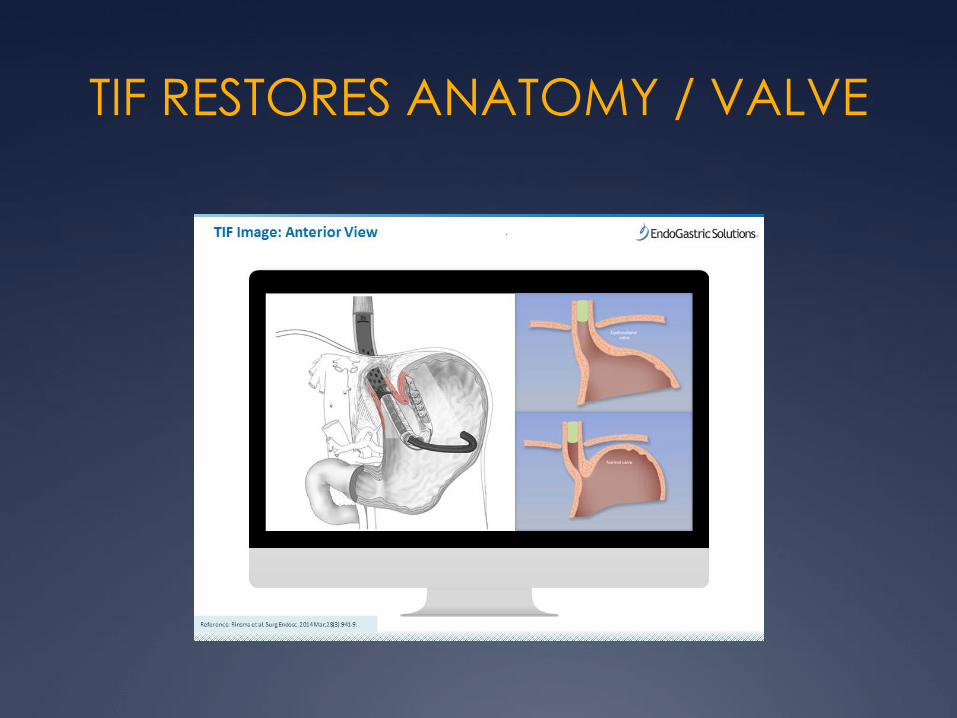
TIF RESTORES ANATOMY / VALVE

Initial Results Disapointing
SAGES Review of TIF
Quality of evidence
(++) low
Recommendation: weak
“Significant untoward events…”
“Results appear mixed…”
“Majority of literature is underpowered…”
ASGE
“Results variable…”
“Lack of routine reporting of pH data…”
“Most studies small, short term follow up…”
“Poorer results with earlier of the device / technique”
Gastrointest Endosc 2015;81:1305–1310 / DOI: http://dx.doi.org/10.1016/j.gie.2015.02.021

Why Such a Poor Initial Showing?
Intent: Mimic Surgery Practice: Learning Curve
Name TLA Fastner Plication Wrap
Endoluminal
fundoplicatio
n
ELF Below z line Gastro -
gastric
No
Transoral
incisionless
fundoplicatio
n
TIF 1 Above z line
1 cm
Esophago-
gastric
No
Transoral
incisionless
fundoplicatio
n
TIF 2 1-3 cm
above z
line; more
length
along
greater
curve
Esophago-
gastric
Yes

RCT: RESPECT TRIAL
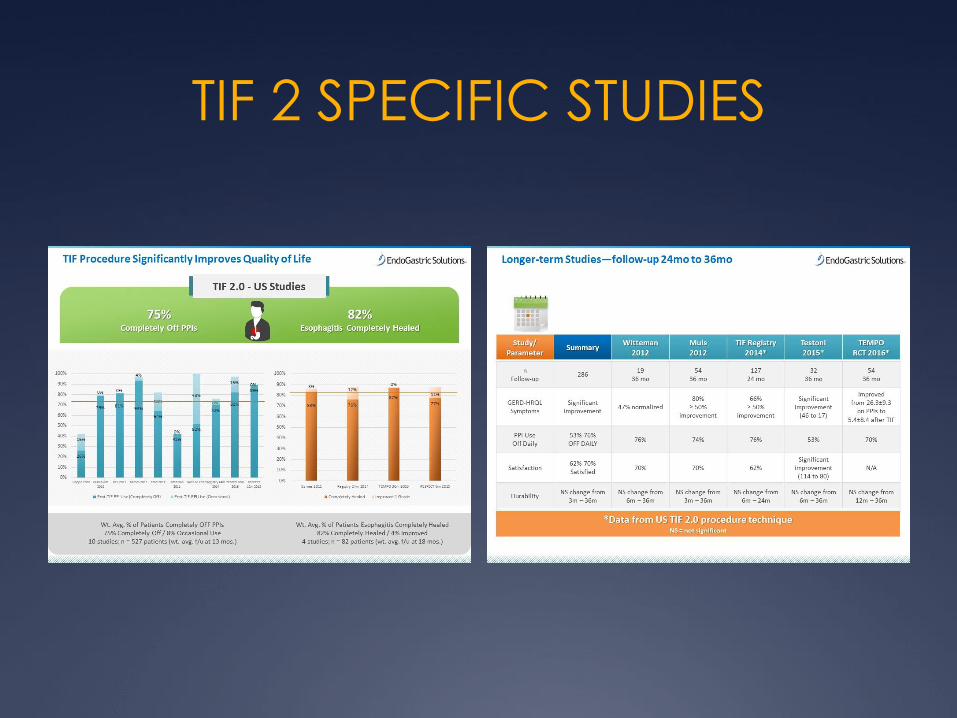
TIF 2 SPECIFIC STUDIES
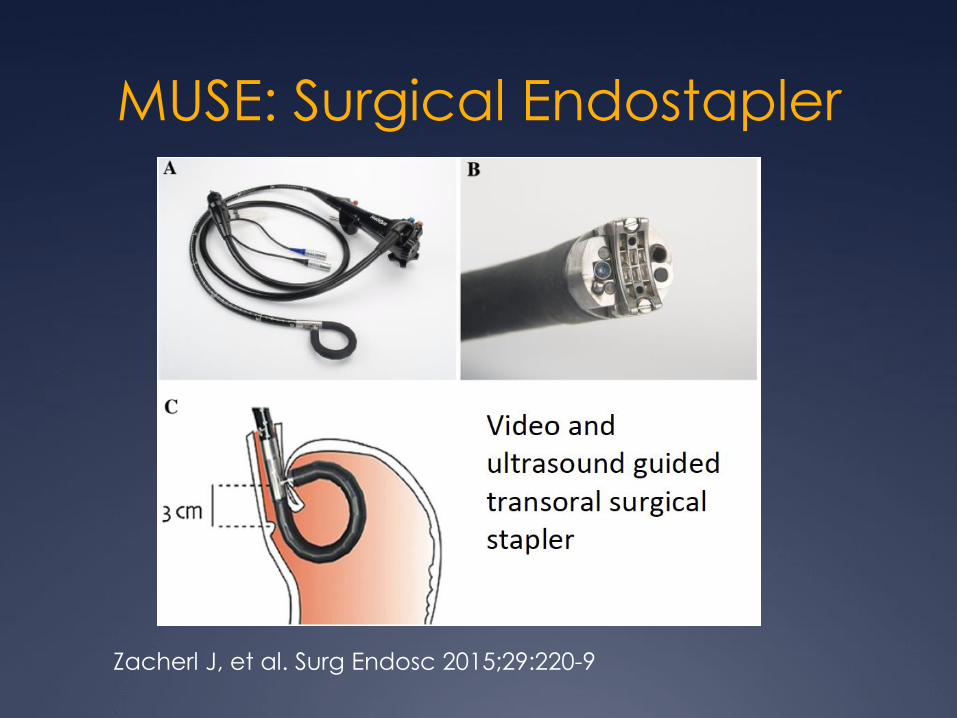
MUSE: Surgical Endostapler
Zacherl J, et al. Surg Endosc 2015;29:220-9

MUSE: Endoscopic Anterior
Fundoplication
Roy-Shapira A et al. Surg Endosc 2015;29:3717-
21
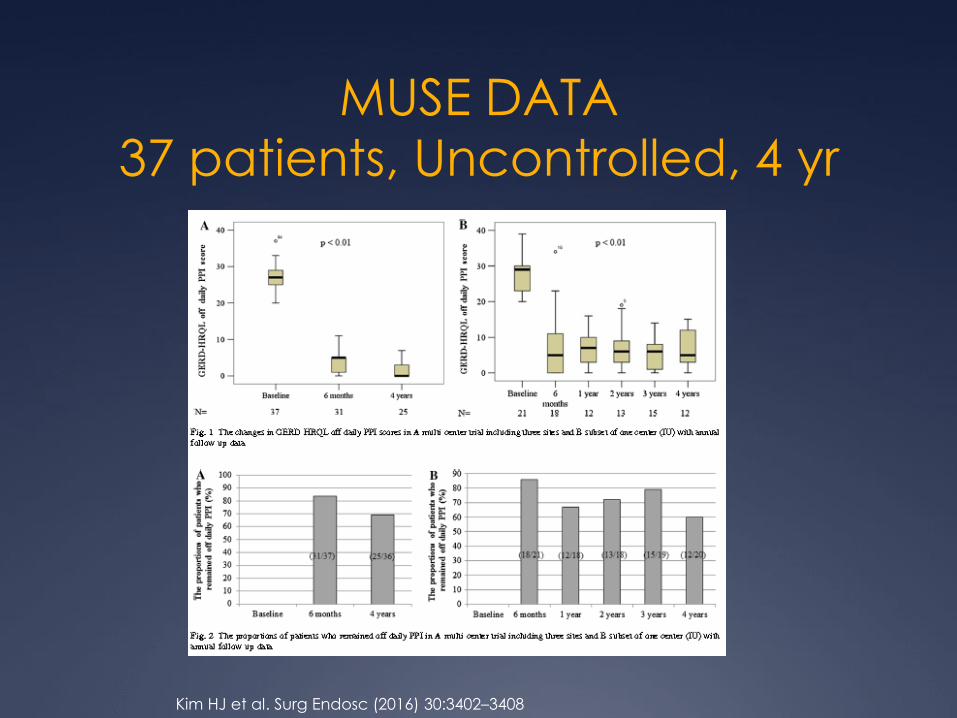
MUSE DATA
37 patients, Uncontrolled, 4 yr
Kim HJ et al. Surg Endosc (2016) 30:3402–3408
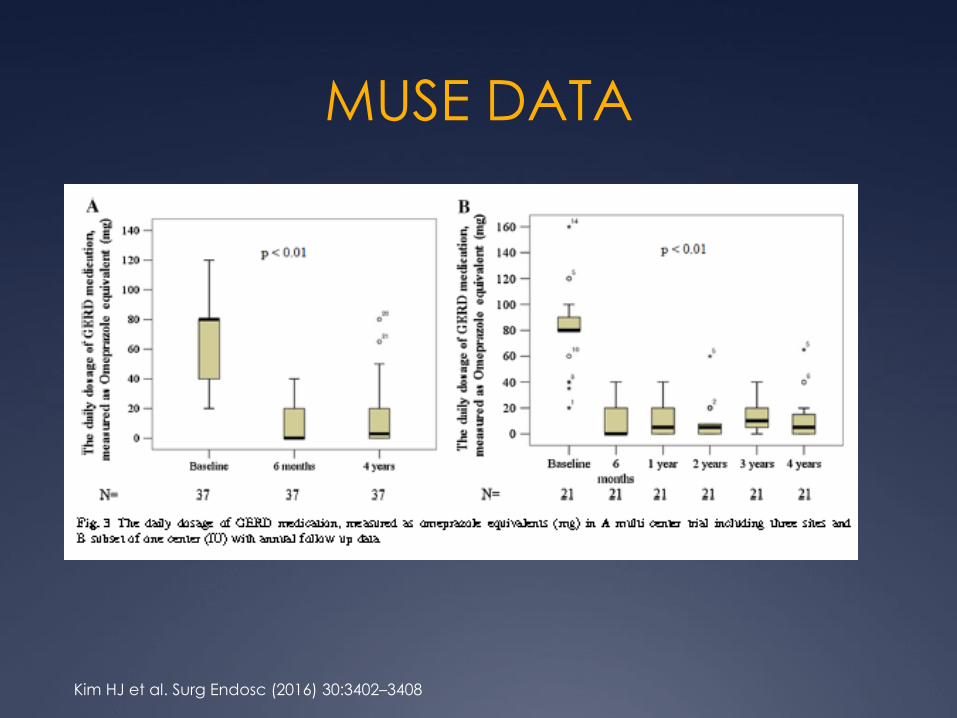
MUSE DATA
Kim HJ et al. Surg Endosc (2016) 30:3402–3408
Why do we care about GERD?
Assumptions
GERD is no longer a
problem
Anti-reflux devices have
“flopped” and are no
longer on the market
Data supporting
endoscopic treatment is
limited
This sort of stuff isn’t done
here
Reality
Many patients have an
incomplete response
Endoscopic treatment is
readily available
Data are reasonably
robust
This sort of stuff can be
done anywhere