endoscopic and histologic diagnosis of barrett esophagus
TRANSCRIPT

Mayo Clin Proc, February 2001, Vol 76 Endoscopic and Histologic Diagnosis of Barrett Esophagus 217
Mayo Clin Proc. 2001;76:217-225 217 © 2001 Mayo Foundation for Medical Education and Research
From the Division of Gastroenterology and Hepatology and InternalMedicine (E.R., C.J.G.) and Department of Laboratory Medicine andPathology (L.J.B.), Mayo Clinic, Rochester, Minn.
Individual reprints of this article are not available. The entire Alan J.Cameron Symposium on Barrett Esophagus and GastroesophagealReflux Disease will be available for purchase as a bound bookletfrom the Proceedings Editorial Office at a later date.
Cameron Symposium on Barrett Esophagus and GERD
Endoscopic and Histologic Diagnosis of Barrett Esophagus
ELIZABETH RAJAN, MD; LAWRENCE J. BURGART, MD; AND CHRISTOPHER J. GOSTOUT, MD
Endoscopy plays an important role in the identification,diagnosis, and treatment of Barrett esophagus. Short-seg-ment (<2-3 cm) and traditional long-segment (>2-3 cm)Barrett esophagus are distinguished solely on the length ofmetaplastic tissue above the esophagogastric junction. Thehistologic hallmark of intestinal metaplasia is required toconfirm diagnosis. Biopsy specimens obtained from tissueof presumed Barrett esophagus or an irregular Z lineconfirm metaplastic glandular mucosa and permit evalua-tion of dysplastic or neoplastic changes. In the appropriateclinical setting, the use of adjunctive diagnostic techniquesmay facilitate the diagnosis of Barrett esophagus and se-quelae such as dysplasia. Chromoendoscopy with high-
resolution or magnified endoscopy is simple, safe, anddesirable for surveillance but requires additional proce-dural time. The use of light-induced fluorescence endos-copy and light-scattering spectroscopy (ie, optical biopsy)is appealing for the diagnosis and characterization of sus-picious lesions. Adjunctive endoscopic techniques and ad-herence to a protocol for performing biopsies facilitate theearly detection and subsequent surveillance of Barrettesophagus.
Mayo Clin Proc. 2001;76:217-225
EGJ = esophagogastric muscular junction; SCJ = squamoco-lumnar junction
In Barrett esophagus, the stratified squamous epitheliallining of the esophagus is replaced by metaplastic spe-
cialized columnar epithelium. Suggestive endoscopic find-ings and subsequent histologic confirmation of intestinalmetaplasia anywhere within the tubular esophagus is con-sidered diagnostic of Barrett esophagus. Endoscopy playsan important role in the identification, diagnosis, and treat-ment of Barrett esophagus. The endoscopist must be able todiscriminate Barrett mucosa from an irregular squamoco-lumnar junction (SCJ), from esophagitis, and from a smalldiaphragmatic hernia.
ENDOSCOPIC LANDMARKSNormal Anatomy
The location of the SCJ usually varies with the patient’sheight; it is generally situated at or just distal to the dia-phragmatic hiatus between 35 and 45 cm from the incisors. Itis recognized grossly as an abrupt color change from the paleesophageal squamous epithelium to the salmon-colored co-lumnar epithelium of the cardia. This typically appears as aslightly undulating circumferential border called the Z (zig-zag) line. In addition to gross color, the distal esophagealsquamous epithelium can be identified by the presence ofsuperficial, thin, capillary-type vessels that disappear at the
esophagogastric junction (Figure 1, left). The line of demar-cation between the 2 types of mucosa is readily identifiablein the absence of pathologic changes. The esophagogastricmuscular junction (EGJ), with only partial insufflation of thelumen, is located at the point where the mucosal vascularpattern disappears cephalad to the most proximal extent ofthe gastric rugal folds. This more subtle characterization ofthe EGJ is useful when distinguishing between a small hiatalhernia and a Barrett segment.
The distal mucosal columns or folds converge directlyinto the EGJ. These columns, when visible with only par-tial insufflation of the esophageal lumen, denote the rela-tive location of the lower esophageal sphincter. Once theendoscope is passed into the proximal stomach and retro-flexed to examine the proximal stomach, the insertion tubeof the endoscope can be seen coming through a tightlyfitting junction. In some patients, a to-and-fro movement ofthe instrument can reveal the Z line. A horseshoe-shapedring of tissue can be seen surrounding the endoscope, withthe open ends of the horseshoe marking the left and rightlateral boundary of the lesser curvature. This prominent ringof tissue is referred to as the angle of His (Figure 1, right).
Diaphragmatic HerniaThe importance of endoscopy lies less in demonstrating
the presence of a hernia than in establishing the existenceof associated reflux disease and distinguishing a Barrettesophagus. A small (2-3 cm) diaphragmatic hernia appearstubular, with the typical gastric epithelium and rugal foldsinferior to the Z line and above the diaphragmatic hiatus(Figure 2, left). The distal end of the diaphragmatic hernia
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Endoscopic and Histologic Diagnosis of Barrett Esophagus Mayo Clin Proc, February 2001, Vol 76218
is identified by the “rosette” of rugal folds. It is confirmedwhen the patient is asked to take a quick breath in, and thecontracture of the diaphragm is seen at the level of therosette. Other endoscopic landmarks include the proximaldisplacement of the Z line and the radiographic ring struc-tures described by Wolf.1 The retroverted endoscope can bepulled back to the level of the diaphragmatic hiatus or evena short distance into the hernia pouch, distinctively permit-ting recognition of the SCJ from below (Figure 2, right).
ENDOSCOPIC DIAGNOSISBarrett Esophagus
In Barrett esophagus, the SCJ is displaced upward andhas an asymmetric, irregular appearance with salmon-pink,
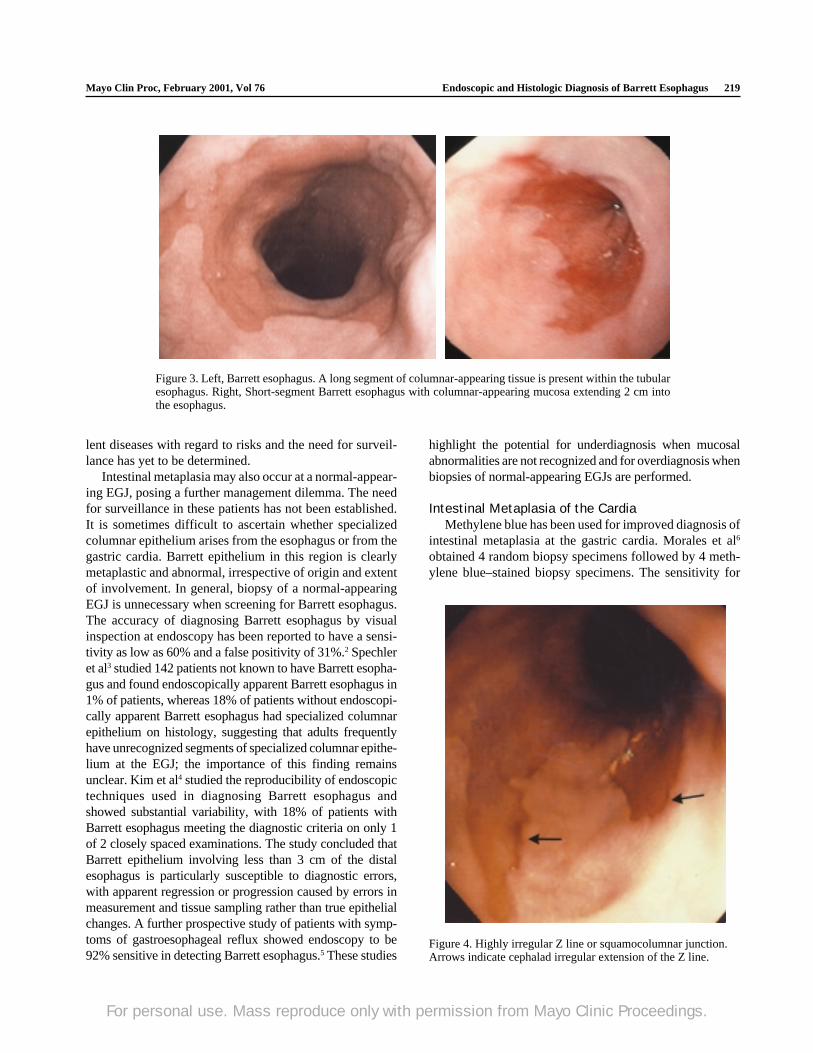
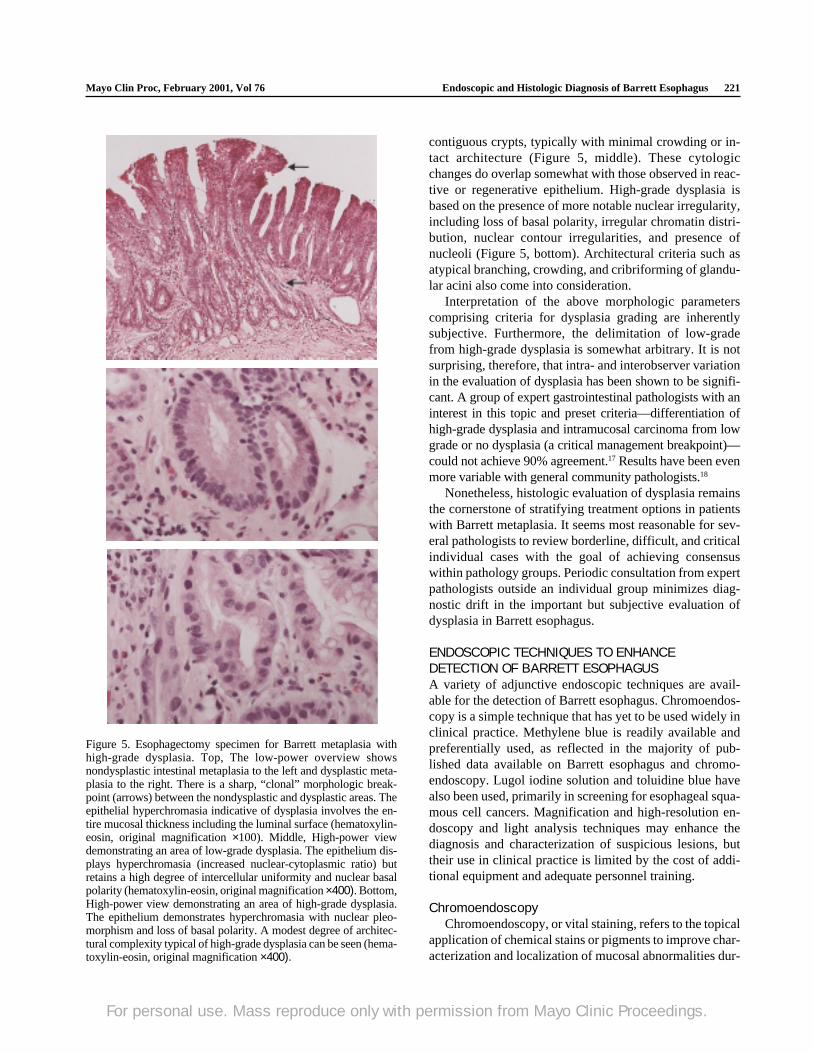
tonguelike mucosal projections extending up into the squa-mous epithelium. Barrett epithelium may take on severalconfigurations, including a circumferential segment or iso-lated islands of gastric-appearing mucosa contiguous orclose to the Z line. Short-segment (<2-3 cm) and traditionallong-segment (>2-3 cm) Barrett esophagus are arbitrarilydistinguished solely on the length of metaplastic tissueabove the EGJ (Figure 3). Furthermore, short-segmentBarrett esophagus may manifest as an irregular Z line andconsequently may be missed easily during endoscopy unlessthere is suspicion and biopsy specimens are taken (Figure 4).The histologic hallmark of intestinal metaplasia is needed toconfirm the diagnosis of Barrett esophagus. Whether short-segment and long-segment Barrett metaplasia are equiva-
Figure 1. Left, Squamocolumnar junction depicted by both a Z line (arrows) and the distinctive mucosalmicrovasculature of the distal esophageal mucosa interfacing with the proximal ends of the gastric rugalfolds. Right, Retroflexed view of the prominent ring of tissue referred to as the angle of His (arrows).
Figure 2. Left, Small diaphragmatic hernia with clearly seen squamocolumnar junction. Right,Distinctive retroflexed appearance of the squamocolumnar junction only seen in patients with adiaphragmatic (hiatal) hernia.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.
Mayo Clin Proc, February 2001, Vol 76 Endoscopic and Histologic Diagnosis of Barrett Esophagus 219
lent diseases with regard to risks and the need for surveil-lance has yet to be determined.
Intestinal metaplasia may also occur at a normal-appear-ing EGJ, posing a further management dilemma. The needfor surveillance in these patients has not been established.It is sometimes difficult to ascertain whether specializedcolumnar epithelium arises from the esophagus or from thegastric cardia. Barrett epithelium in this region is clearlymetaplastic and abnormal, irrespective of origin and extentof involvement. In general, biopsy of a normal-appearingEGJ is unnecessary when screening for Barrett esophagus.The accuracy of diagnosing Barrett esophagus by visualinspection at endoscopy has been reported to have a sensi-tivity as low as 60% and a false positivity of 31%.2 Spechleret al3 studied 142 patients not known to have Barrett esopha-gus and found endoscopically apparent Barrett esophagus in1% of patients, whereas 18% of patients without endoscopi-cally apparent Barrett esophagus had specialized columnarepithelium on histology, suggesting that adults frequentlyhave unrecognized segments of specialized columnar epithe-lium at the EGJ; the importance of this finding remainsunclear. Kim et al4 studied the reproducibility of endoscopictechniques used in diagnosing Barrett esophagus andshowed substantial variability, with 18% of patients withBarrett esophagus meeting the diagnostic criteria on only 1of 2 closely spaced examinations. The study concluded thatBarrett epithelium involving less than 3 cm of the distalesophagus is particularly susceptible to diagnostic errors,with apparent regression or progression caused by errors inmeasurement and tissue sampling rather than true epithelialchanges. A further prospective study of patients with symp-toms of gastroesophageal reflux showed endoscopy to be92% sensitive in detecting Barrett esophagus.5 These studies
highlight the potential for underdiagnosis when mucosalabnormalities are not recognized and for overdiagnosis whenbiopsies of normal-appearing EGJs are performed.
Intestinal Metaplasia of the CardiaMethylene blue has been used for improved diagnosis of
intestinal metaplasia at the gastric cardia. Morales et al6
obtained 4 random biopsy specimens followed by 4 meth-ylene blue–stained biopsy specimens. The sensitivity for
Figure 3. Left, Barrett esophagus. A long segment of columnar-appearing tissue is present within the tubularesophagus. Right, Short-segment Barrett esophagus with columnar-appearing mucosa extending 2 cm intothe esophagus.
Figure 4. Highly irregular Z line or squamocolumnar junction.Arrows indicate cephalad irregular extension of the Z line.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Endoscopic and Histologic Diagnosis of Barrett Esophagus Mayo Clin Proc, February 2001, Vol 76220
intestinal metaplasia at the cardia increased from 38% (forrandom biopsy alone) to 67% with a targeted methyleneblue–stained biopsy specimen. Positive staining was de-fined as blue-stained mucosa that persisted despite vigor-ous rinsing. Methylene blue staining was graded byFennerty et al7 as negative, subtle focal, subtle diffuse,prominent focal, prominent diffuse, and equivocal when itwas unclear if blue discoloration was secondary to the stainor an artifact. The most common pattern of mucosal stain-ing was subtle focal staining, which was associated withfocal glands of intestinal metaplasia, whereas generalizedintestinal metaplasia was associated with prominent stain-ing. Difficulties in interpretation during chromoendoscopyare equivocal results and false positives that may occurfrom inadequate mucolysis, staining or rinsing, or mucosaldamage from either instrumentation or erosive disease.
Biopsy ProtocolThe suggested protocol for surveillance for Barrett
esophagus recommends 4-quadrant biopsies taken at 2-cmintervals along the entire length of specialized columnarepithelial lining.8 With the exception of short-segmentBarrett esophagus, this format should be adhered to as wellduring an index endoscopy both to establish the diagnosisof a suspected Barrett eosophagus and to provide baselinesurveillance for the patient. In patients with short-segmentBarrett esophagus, especially those with 2 cm or less ofsuspected mucosa, a sufficient number of biopsies shouldbe taken to represent the mucosa in question. A jumbospiked biopsy forceps has been advocated to obtain a largerspecimen and improve histologic interpretation during sur-veillance. These biopsy devices require the use of largerendoscopes with sufficiently sized channels to accommo-date the larger forceps. They are infrequently used duringestablished surveillance and are impractical to use during anindex diagnostic or a screening endoscopy. Most important,biopsies of any mucosal abnormalities seen during surveil-lance or at an initial index examination, no matter howtrivial, should be assessed to exclude high-grade dysplasiaand early carcinoma. Active inflammation with erythema,erosions, ulceration, and exudate impair the ability to detectBarrett esophagus. If there is concern about the coexistenceof a Barrett segment under these circumstances, the patientshould undergo a course of proton pump inhibitor therapywith plans for follow-up endoscopy with assessment of bi-opsy specimens, as indicated, in 4 to 6 weeks.
In a prospective controlled trial, patients with biopsy-proven Barrett esophagus underwent both 4-quadrantjumbo random biopsy and methylene blue–directed jumbobiopsy in a randomized order.9 Methylene blue–directedbiopsy led to the identification of a much larger proportionof specialized columnar epithelium compared with random
biopsy (limited segment, 54% vs 94%; long-segmentBarrett esophagus, 72% vs 92%). Methylene blue–directedbiopsy diagnosed dysplasia or cancer in significantly morebiopsy samples (12% vs 6%) than did random biopsies.The use of vital staining and optical biopsy should improvethe diagnosis of and enhance the endoscopic surveillancefor Barrett esophagus.
HISTOLOGIC CONFIRMATION OFBARRETT ESOPHAGUSBiopsy specimens obtained in presumed Barrett esophagusor irregular Z line serve 2 primary functions: confirmation ofmetaplastic glandular mucosa and evaluation of dysplastic orneoplastic changes. Both functions require only basic tissue-processing technology and light microscopy. Most centersfix biopsy specimens in formalin, a staple in histopathologylaboratories, which allows for standard handling, avoidanceof heavy metals, maximum flexibility for special stains, andpotential utility in polymerase chain reaction–based molecu-lar studies.10 Heavy metal–containing fixatives have beenadvocated by some subspecialists because they facilitatenuclear fixation, preserving some subtle nuclear morpho-logic features not uniformly present in formalin-fixed mate-rial. However, these cytologic variations are out of the main-stream of diagnostic pathology and may actually result inincreased diagnostic variability among medical centers.Routine hematoxylin and eosin–stained sections allow forconfirmation of glandular metaplasia, subclassification intometaplastic subtypes (eg, intestinal, cardiac, and fundic), andevaluation of dysplasia and neoplasia.
Some authors originally considered any variant of colum-nar metaplasia in the esophagus as equivalently diagnostic ofBarrett esophagus.11 Studies in the 1980s offered 2 keyobservations underscoring the primary importance of intesti-nal metaplasia as the critical subtype of columnar mucosa inBarrett esophagus12-15 (Figure 5, top). First, introduction ofstandard biopsy protocols resulting in improved samplingdemonstrated that 96% or more of true Barrett metaplasiacontained a considerable component of intestinal metaplasia,usually a vast majority. In other words, it is rare to haveBarrett esophagus without intestinal metaplasia, whereashiatal hernia or irregular Z line most often are not accompa-nied by intestinal metaplasia. Second, dysplasia and its in-herent risk of malignancy were intimately associated withintestinal metaplasia and not gastric metaplasia. Therefore,the rare patients with Barrett metaplasia without intestinalmetaplasia appear to have minimal risk of adverse outcome.
The histologic evaluation of dysplasia is based on cyto-logic and architectural criteria.16,17 Low-grade dysplasia isdependent on the presence of epithelial hyperchromasia (ie,an increased nucleus-cytoplasmic ratio), resulting in theappearance of clonal expansion of atypical cells involving
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.
Mayo Clin Proc, February 2001, Vol 76 Endoscopic and Histologic Diagnosis of Barrett Esophagus 221
contiguous crypts, typically with minimal crowding or in-tact architecture (Figure 5, middle). These cytologicchanges do overlap somewhat with those observed in reac-tive or regenerative epithelium. High-grade dysplasia isbased on the presence of more notable nuclear irregularity,including loss of basal polarity, irregular chromatin distri-bution, nuclear contour irregularities, and presence ofnucleoli (Figure 5, bottom). Architectural criteria such asatypical branching, crowding, and cribriforming of glandu-lar acini also come into consideration.
Interpretation of the above morphologic parameterscomprising criteria for dysplasia grading are inherentlysubjective. Furthermore, the delimitation of low-gradefrom high-grade dysplasia is somewhat arbitrary. It is notsurprising, therefore, that intra- and interobserver variationin the evaluation of dysplasia has been shown to be signifi-cant. A group of expert gastrointestinal pathologists with aninterest in this topic and preset criteria—differentiation ofhigh-grade dysplasia and intramucosal carcinoma from lowgrade or no dysplasia (a critical management breakpoint)—could not achieve 90% agreement.17 Results have been evenmore variable with general community pathologists.18
Nonetheless, histologic evaluation of dysplasia remainsthe cornerstone of stratifying treatment options in patientswith Barrett metaplasia. It seems most reasonable for sev-eral pathologists to review borderline, difficult, and criticalindividual cases with the goal of achieving consensuswithin pathology groups. Periodic consultation from expertpathologists outside an individual group minimizes diag-nostic drift in the important but subjective evaluation ofdysplasia in Barrett esophagus.
ENDOSCOPIC TECHNIQUES TO ENHANCEDETECTION OF BARRETT ESOPHAGUSA variety of adjunctive endoscopic techniques are avail-able for the detection of Barrett esophagus. Chromoendos-copy is a simple technique that has yet to be used widely inclinical practice. Methylene blue is readily available andpreferentially used, as reflected in the majority of pub-lished data available on Barrett esophagus and chromo-endoscopy. Lugol iodine solution and toluidine blue havealso been used, primarily in screening for esophageal squa-mous cell cancers. Magnification and high-resolution en-doscopy and light analysis techniques may enhance thediagnosis and characterization of suspicious lesions, buttheir use in clinical practice is limited by the cost of addi-tional equipment and adequate personnel training.
ChromoendoscopyChromoendoscopy, or vital staining, refers to the topical
application of chemical stains or pigments to improve char-acterization and localization of mucosal abnormalities dur-
Figure 5. Esophagectomy specimen for Barrett metaplasia withhigh-grade dysplasia. Top, The low-power overview showsnondysplastic intestinal metaplasia to the left and dysplastic meta-plasia to the right. There is a sharp, “clonal” morphologic break-point (arrows) between the nondysplastic and dysplastic areas. Theepithelial hyperchromasia indicative of dysplasia involves the en-tire mucosal thickness including the luminal surface (hematoxylin-eosin, original magnification ×100). Middle, High-power viewdemonstrating an area of low-grade dysplasia. The epithelium dis-plays hyperchromasia (increased nuclear-cytoplasmic ratio) butretains a high degree of intercellular uniformity and nuclear basalpolarity (hematoxylin-eosin, original magnification ×400). Bottom,High-power view demonstrating an area of high-grade dysplasia.The epithelium demonstrates hyperchromasia with nuclear pleo-morphism and loss of basal polarity. A modest degree of architec-tural complexity typical of high-grade dysplasia can be seen (hema-toxylin-eosin, original magnification ×400).
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.
Endoscopic and Histologic Diagnosis of Barrett Esophagus Mayo Clin Proc, February 2001, Vol 76222
ing endoscopy. Vital stains that have been used in Barrettesophagus include methylene blue, indigo carmine, Lugoliodine solution, and toluidine blue. Absorptive stains iden-tify specific epithelial cells or cellular constituents by pref-erential diffusion or absorption across the cell membrane.Contrast staining highlights tissue topography and accentu-ates irregularities in surface contour by outlining mucosalelevations, depressions, or crevices. The technique andyield of chromoendoscopy is improved when either magni-fication or high-resolution video endoscopes are used.
Methylene Blue.—The use of methylene blue may beof particular benefit in detecting short-segment Barrettesophagus, identifying potential foci of dysplasia within asegment of Barrett epithelium, or recognizing residual fociof metaplastic tissue after endoscopic treatment. Methy-lene blue (methylthionine chloride) is an absorptive stainthat is available as a 1% sterile solution. It is taken up byactively absorbing tissues such as small intestinal and co-lonic epithelial tissue, but importantly, it will not stainnonabsorptive squamous mucosa or gastric mucosa. Theexact mechanism of entry across the cell membrane into thecytoplasm remains unclear. Surface mucus impairs the up-take of an absorptive dye into epithelial cells. The segmentof esophagus to be studied is first washed and bathed forseveral minutes with a mucolytic agent such as 10%acetylcysteine. The mucolytic action is related to the sulf-hydryl group in the molecule that disrupts disulfide link-ages in mucus, thereby reducing or destroying mucus vis-cosity over a span of several minutes.19
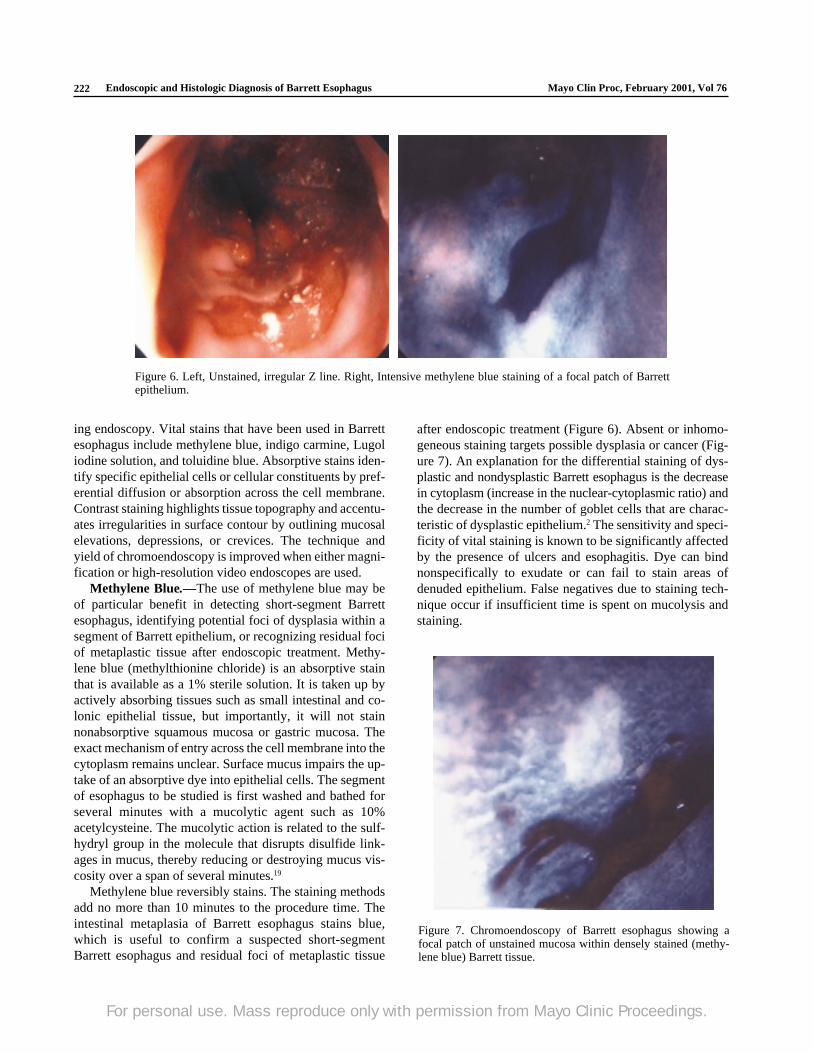
Methylene blue reversibly stains. The staining methodsadd no more than 10 minutes to the procedure time. Theintestinal metaplasia of Barrett esophagus stains blue,which is useful to confirm a suspected short-segmentBarrett esophagus and residual foci of metaplastic tissue
after endoscopic treatment (Figure 6). Absent or inhomo-geneous staining targets possible dysplasia or cancer (Fig-ure 7). An explanation for the differential staining of dys-plastic and nondysplastic Barrett esophagus is the decreasein cytoplasm (increase in the nuclear-cytoplasmic ratio) andthe decrease in the number of goblet cells that are charac-teristic of dysplastic epithelium.2 The sensitivity and speci-ficity of vital staining is known to be significantly affectedby the presence of ulcers and esophagitis. Dye can bindnonspecifically to exudate or can fail to stain areas ofdenuded epithelium. False negatives due to staining tech-nique occur if insufficient time is spent on mucolysis andstaining.
Figure 6. Left, Unstained, irregular Z line. Right, Intensive methylene blue staining of a focal patch of Barrettepithelium.
Figure 7. Chromoendoscopy of Barrett esophagus showing afocal patch of unstained mucosa within densely stained (methy-lene blue) Barrett tissue.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc, February 2001, Vol 76 Endoscopic and Histologic Diagnosis of Barrett Esophagus 223
Canto et al20 classified patterns of mucosal staining aseither diffuse (>75% of the pink columnar epithelium) ornondiffuse (<75% of pink columnar epithelium). The ma-jority (72%) of patients with positive staining had anondiffuse staining pattern. Furthermore, a reproduciblepattern of staining was demonstrated during repeat endos-copy within 2 to 4 weeks of a previously positive stain. Theaccuracy of methylene blue staining for detecting special-ized columnar epithelium was reported at 95%.20
Methylene blue staining characteristics for dysplasticand malignant Barrett esophagus were further studiedprospectively by Canto et al.21 The stain intensity wascharacterized as dark blue, moderate blue, light blue, andunstained, whereas stain heterogeneity (the degree of varia-tion in stain intensity) was classified as absent, mild, mod-erate, or marked. A total of 92% of biopsy specimens withhigh-grade dysplasia or cancer were unstained or stainedlight blue, compared with 82% with low-grade dysplasiaand 38% with no dysplasia. Furthermore, the presence ofmoderate to marked stain heterogeneity was present in allpatients with severe dysplasia or adenocarcinoma, com-pared with 21% of patients with low-grade dysplasia and3% without dysplasia. This study concluded that increasedheterogeneity and decreased stain intensity are strong inde-pendent predictors of high-grade dysplasia or cancer andmay help direct tissue biopsies. However, the reproducibil-ity of staining patterns needs to be further studied.
Indigo Carmine.—Indigo carmine is a blue contraststain that can highlight the villiform appearance of intesti-nal metaplasia in Barrett esophagus and accentuate subtlemucosal abnormalities. Because it is a contrast agent, endos-copy with higher-resolution instruments is advantageous. Itis simple to use and does not require a mucolytic agent. A0.5% to 0.8% solution is sprayed onto the mucosa andprovides a dark layer that rapidly disperses because of theeffects of secretions and gut motility.
Lugol Iodine Solution.—Lugol iodine solution (namedafter the 19th-century French physician Jean GuillaumeLugol) is an iodine-based absorptive stain with an affinityfor glycogen in nonkeratinized squamous epithelium. Afterthe solution is sprayed onto the mucosa, the normal esoph-ageal mucosa turns a prominent green-brown color withinmoments of application, gradually fading over minutes tohours. Absence of staining indicates diminished or absentglycogen content, as seen in squamous cell cancers, dyspla-sia, Barrett epithelium, gastric metaplasia, and some de-grees of inflammatory esophagitis.22,23 It is used primarilyin screening for early esophageal squamous cell carcinoma,particularly in areas where it is endemic, such as Japan andChina.24 The sensitivity and specificity of Lugol iodine solu-tion–enhanced endoscopy for diagnosing Barrett esophagushave been reported at 89% and 93%, respectively.25
Toluidine Blue.—Toluidine blue is a basic absorptivedye that preferentially stains nuclei, thus staining tissuethat has increased mitotic activity. It is most commonlyused for identifying esophageal squamous cell carcinoma.Following a 1% mucolytic acetic acid rinse, a 1% or 2%aqueous solution of toluidine blue is applied, followed byanother 1% acetic acid wash. Positive staining identifiesintestinal and gastric metaplastic tissue equally. A study byChobanian et al26 reported a sensitivity of 98% and speci-ficity of 80% for diagnosing Barrett esophagus. In thisstudy, Barrett epithelium was histologically characterizedas specialized columnar epithelium, junctional type, or gas-tric fundic type.
Safety of Chromoendoscopy.—All the endoscopicstains are accepted as nontoxic, although maximal safedoses are not known. Both methylene blue and acetyl-cysteine are minimally absorbed. Lugol iodine solutionmust be avoided in patients with a history of iodine allergy.Concentrated Lugol iodine solution (50%) caused heart-burn in 3 patients and bronchospasm in 1 patient withiodine sensitivity.27 Methylene blue and indigo carminehave caused serious systemic reactions during parenteraladministration.28,29 Stains should be limited to the describedconcentrations, using the smallest volumes, generally 10 to20 mL. Pooled stain can be reused to minimize volumes.The patient must be instructed about possible discolorationof urine and feces. The dyes used for chromoendoscopystain anything they contact, especially clothing fabric, socare must be used to avoid any accidental leakage or spray-ing outside the patient. They pose no risks to clinical per-sonnel and do not damage the endoscopy equipment, butwith frequent use, they may discolor the outer markings onendoscope insertion tubes.
Magnification and High-Resolution EndoscopyEndoscopic detection of gastrointestinal pathology de-
pends on the recognition of visible mucosal lesions. Mag-nification and high-resolution endoscopy enable detectionof subtle changes of the gastrointestinal mucosa that maybe unrecognized or of indeterminate importance when con-ventional fiberoptic and video endoscopes are used. Mag-nification instruments were built in Japan in the 1960s andcan magnify the mucosa from ×3 to ×170, with most mag-nification performed within a more practical range of ×10to ×35.30 High-magnification endoscopy is best used withabsorptive staining because of time-consuming technicalaspects of magnification (focusing in and out of magnifica-tion) and the need for long-lasting staining.
Magnification instruments allow the examination of cel-lular mucosal patterns. There are limited data on the use ofmagnification endoscopy in Barrett esophagus. Stevens etal27 described the use of magnification endoscopy in con-
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Endoscopic and Histologic Diagnosis of Barrett Esophagus Mayo Clin Proc, February 2001, Vol 76224
junction with combined dye spraying. Lugol iodine solu-tion was initially sprayed to define the SCJ, and then areasof unstained mucosa, representing possible Barrett esopha-gus, were stained with indigo carmine, which was followedby magnification endoscopy to image the resultant finemucosal pattern. Barrett epithelium was visualized asraised with a villiform surface pattern, an appearance similarto that of small bowel mucosa obtained using the sameprocedure. This pattern correlated with histologic confirma-tion of Barrett esophagus. The villous surface appearanceseen on magnified examination corresponds to mucosalridges with depressions (openings of intestinal glands) asseen by electron microscopy and are not true villi.
High-resolution instruments are video based and pro-vide greater pixel density along with minor magnification.In our own experience, the perceived advantage of theseinstruments is their ease of use and the flexibility to useeither contrast or absorptive chromoendoscopy stains. Suffi-cient mucosal surface detail is continually provided withoutthe manipulations needed to focus to a desired magnificationand simultaneously readjust the instrument position to ac-commodate for movement and fluids altering the viewingfield. Most of the latest-model commercially available videoendoscopes offer higher resolution, which often exceeds60% of the resolution capabilities of previous video endo-scope models. Resolution beyond these instruments is avail-able only in prototype instruments undergoing evaluation.
Light Analysis TechniquesSpectroscopy, the analysis of wavelength and intensity
of light, can also be used to analyze the mucosa. The abilityto characterize tissue using light by rapid, contact-onlyspectroscopic techniques is referred to as optical biopsyand has far-reaching potential. When tissue is illuminatedwith light (monochromatic laser or nonlaser), photons pen-etrate into the tissue at varying depths, with some photonsabsorbed and others reemitted in another wavelength oflight (this property is called fluorescence—eg, light-in-duced fluorescence endoscopy), or the photons can be scat-tered within the tissue (eg, light-scattering spectroscopy).31
Light-induced fluorescence endoscopy is based on the use ofendogenous (naturally occurring) or exogenous (adminis-tered) fluorescent agents. Autofluorescence arises from en-dogenous molecules called fluorophores within tissues suchas aromatic amino acids, connective tissue, lipopigments,and by-products of heme synthesis.32 Mucosa, submucosa,and muscularis propria have distinct fluorophore composi-tions, so that the fluorescence measured at the luminal sur-face comprises contributions from the various layers. Tissueautofluorescence is sensitive to alterations in tissue morphol-ogy and biochemistry and theoretically may be used to detectearly malignant transformation. An alternative to optical
biopsy by autofluorescence is the use of exogenous fluores-cence-inducing drugs such as hematoporphyrin derivative,phthalocyanines, and 5-aminolevulinic acid. Drug-inducedfluorescence is dependent on the degree of selective localiza-tion of the light-sensitizing drug within tissue and drugpharmacokinetics. Both methods are performed with a con-tact optical fiber probe, typically 0.5 to 1 mm in diameter,passed through the endoscope biopsy channel and placed incontact with the targeted surface of suspicious mucosa. Al-though this procedure is technically simple, the sampling ofonly a small volume of tissue (1-3 mm) immediately beneaththe probe tip is a disadvantage.
Endoscopic systems capable of producing real-timehigh-resolution fluorescence images and evaluating largeareas of mucosal surface in parallel with conventionalwhite light endoscopic examination have recently becomeavailable.33 The use of light-induced fluorescence endos-copy to target biopsies may offer more effective screeningand surveillance for high-risk patients, such as those withBarrett esophagus. The role of exogenous fluorescence-inducing agents in identifying Barrett mucosa is uncertain.There are 2 contradictory experiences that reported using5-aminolevulinic acid–induced fluorescence to distinguishbetween normal squamous and Barrett mucosa.34,35
In light-scattering spectroscopy, the determinants oflight scattering within tissue are the size and number of thescatterers (eg, mitochondria or nuclei) and the wavelengthof light used to illuminate the tissue.31,36 This property oflight has been used during endoscopic procedures to deter-mine the number and size of nuclei and the degree of nucleicrowding in patients with Barrett esophagus. A prospectivestudy that assessed the potential of light-scattering spec-troscopy to measure epithelial nuclear enlargement andcrowding in patients with Barrett esophagus showed thatboth the sensitivity and specificity of this technique fordetecting dysplasia (either high-grade or low-grade dyspla-sia) were 90%.37 Dysplasia was diagnosed if 30% or moreof the nuclei exceeded 10 µm in diameter. This suggeststhat light-scattering spectroscopy may readily detect areasof dysplasia during endoscopy.
CONCLUSIONEndoscopy plays an integral part in the diagnosis and man-agement of Barrett esophagus and its associated complica-tions. In the appropriate clinical setting, the use of adjunc-tive diagnostic techniques may facilitate the diagnosis ofBarrett esophagus. Chromoendoscopy is simple and safe,but this technique requires additional procedural time aswell as late-model video endoscopes with improved resolu-tion. To our knowledge, the relative performance, accu-racy, ease of use, and cost of the various vital stains fordiagnosing Barrett esophagus and the yield in detecting
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.

Mayo Clin Proc, February 2001, Vol 76 Endoscopic and Histologic Diagnosis of Barrett Esophagus 225
dysplasia or cancer have not been formally compared.There are insufficient data to recommend the use of high-magnification endoscopes for screening or surveillanceprocedures. The use of light-induced fluorescence endos-copy and light-scattering spectroscopy (ie, optical biopsy)is appealing for the diagnosis and characterization of suspi-cious lesions to target biopsies. Chromoendoscopy andoptical biopsy methods are advocated for both the diagno-sis and surveillance of Barrett esophagus but require fur-ther study. A high level of suspicion and adherence to aprotocol for performing biopsies are mandatory.
REFERENCES1. Wolf BS. Sliding hiatal hernia: the need for redefinition. AJR Am J
Roentgenol Radium Ther Nucl Med. 1973;117:231-247.2. Canto MI. Vital staining and Barrett’s esophagus. Gastrointest
Endosc. 1999;49(3, pt 2):S12-S16.3. Spechler SJ, Zeroogian JM, Antonioli DA, Wang HH, Goyal RK.
Prevalence of metaplasia at the gastro-oesophageal junction. Lan-cet. 1994;344:1533-1536.
4. Kim SL, Waring JP, Spechler SJ, et al, Department of VeteransAffairs Gastroesophageal Reflux Study Group. Diagnostic incon-sistencies in Barrett’s esophagus. Gastroenterology. 1994;107:945-949.
5. Winters C Jr, Spurling TJ, Chobanian SJ, et al. Barrett’s esophagus:a prevalent, occult complication of gastroesophageal reflux dis-ease. Gastroenterology. 1987;92:118-124.
6. Morales TG, Bhattacharyya A, Camargo E, Johnson C, Sampliner RE.Methylene blue staining for intestinal metaplasia of the gastric cardiawith follow-up for dysplasia. Gastrointest Endosc. 1998;48:26-31.
7. Fennerty MB, Sampliner RE, McGee DL, Hixson LJ, Garewal HS.Intestinal metaplasia of the stomach: identification by a selectivemucosal staining technique. Gastrointest Endosc. 1992;38:696-698.
8. Falk GW. Barrett’s esophagus. Gastrointest Endosc Clin N Am.1994;4:773-789.
9. Canto MI, Setrakian S, Willis J, Chak A, Sivak MV Jr. Methyleneblue directed biopsy for improved detection of intestinal metaplasiaand dysplasia in Barrett’s esophagus: a controlled sequential trial[abstract]. Gastrointest Endosc. 1996:43. Abstract 165.
10. Tbakhi A, Totos G, Pettay JD, Myles J, Tubbs RR. The effect offixation on detection of B-cell clonality by polymerase chain reac-tion. Mod Pathol. 1999;12:272-278.
11. Paull A, Trier JS, Dalton MD, Camp RC, Loeb P, Goyal RK. Thehistologic spectrum of Barrett’s esophagus. N Engl J Med. 1976;295:476-480.
12. Zwas F, Shields HM, Doos WG, et al. Scanning electron micros-copy of Barrett’s epithelium and its correlation with light micros-copy and mucin stains. Gastroenterology. 1986;90:1932-1941.
13. Spechler SJ, Robbins AH, Rubins HB, et al. Adenocarcinoma andBarrett’s esophagus: an overrated risk? Gastroenterology. 1984;87:927-933.
14. Hamilton SR, Smith RR. The relationship between columnar epi-thelial dysplasia and invasive adenocarcinoma arising in Barrett’sesophagus. Am J Clin Pathol. 1987;87:301-312.
15. Schmidt HG, Riddell RH, Walther B, Skinner DB, Riemann JF.Dysplasia in Barrett’s esophagus. J Cancer Res Clin Oncol. 1985;110:145-152.
16. Riddell RH, Goldman H, Ransohoff DE, et al. Dysplasia in inflam-matory bowel disease: standardized classification with provisionalclinical applications. Hum Pathol. 1983;14:931-968.
17. Reid BJ, Haggitt RC, Rubin CE, et al. Observer variation in thediagnosis of dysplasia in Barrett’s esophagus. Hum Pathol. 1988;19:166-178.
18. Alikhan M, Rex D, Khan A, Rahmani E, Cummings O, UlbrightTM. Variable pathologic interpretation of columnar lined esopha-gus by general pathologists in community practice. GastrointestEndosc. 1999;50:23-26.
19. Acosta MM, Boyce HW Jr. Chromoendoscopy—where is it useful?J Clin Gastroenterol. 1998;27:13-20.
20. Canto MI, Setrakian S, Petras RE, Blades E, Chak A, Sivak MV Jr.Methylene blue selectively stains intestinal metaplasia in Barrett’sesophagus. Gastrointest Endosc. 1996;44:1-7.
21. Canto MI, Setrakian S, Willis J, Chak A, Sivak MV Jr. Methyleneblue staining of dysplastic and non-dysplastic Barrett’s esophagus:an in vivo and ex vivo study [abstract]. Gastrointest Endosc.1996:43. Abstract 164.
22. Mori M, Adachi Y, Matsushima T, Matsuda H, Kuwano H,Sugimachi K. Lugol staining pattern and histology of esophageallesions. Am J Gastroenterol. 1993;88:701-705.
23. Sugimachi K, Kitamura K, Baba K, Ikebe M, Kuwano H. Endo-scopic diagnosis of early carcinoma of the esophagus using Lugol’ssolution. Gastrointest Endosc. 1992;38:657-661.
24. Okumura T, Aruga H, Inohara H, et al. Endoscopic examination ofthe upper gastrointestinal tract for the presence of second primarycancers in head and neck cancer patients. Acta Otolaryngol Suppl.1993;501:103-106.
25. Woolf GM, Riddell RH, Irvine EJ, Hunt RH. A study to examineagreement between endoscopy and histology for the diagnosis ofcolumnar lined (Barrett’s) esophagus. Gastrointest Endosc. 1989;35:541-544.
26. Chobanian SJ, Cattau EL Jr, Winters C Jr, et al. In vivo stainingwith toluidine blue as an adjunct to the endoscopic detection ofBarrett’s esophagus. Gastrointest Endosc. 1987;33:99-101.
27. Stevens PD, Lightdale CJ, Green PH, Siegel LM, Garcia-Carrasquillo RJ, Rotterdam H. Combined magnification endoscopywith chromoendoscopy for the evaluation of Barrett’s esophagus.Gastrointest Endosc. 1994;40:747-749.
28. Naitoh J, Fox BM. Severe hypotension, bronchospasm, and urti-caria from intravenous indigo carmine. Urology. 1994;44:271-272.
29. Sills MR, Zinkham WH. Methylene blue-induced Heinz bodyhemolytic anemia. Arch Pediatr Adolesc Med. 1994;148:306-310.
30. Sorbi D, Gostout CJ. Polyp identification and marking: chromo-endoscopy, high-resolution and high-magnification endoscopy, tat-tooing and clipping. Tech Gastrointest Endosc. 2000;2:2-8.
31. Wallace MB, Van Dam J. Enhanced gastrointestinal diagnosis.Gastrointest Endosc Clin N Am. 2000;10:71-80.
32. DaCosta RS, Wilson BC, Marcon NE. Light-induced fluorescenceendoscopy of the gastrointestinal tract. Gastrointest Endosc Clin NAm. 2000;10:37-69.
33. Namihisa A, Watanabe H, Tanaka H, Miwa H, Ogihara T, Sato N.Detection of gastric lesions by endoscopic autofluorescence realtime imaging system (light induced fluorescence endoscopy) [ab-stract]. Gastrointest Endosc. 1997;45:AB35. Abstract 43.
34. Messmann H, Kullmann F, Wild T, et al. Detection of dysplasticlesions by fluorescence in a model of colitis in rats after previousphotosensitization with 5-aminolaevulinic acid. Endoscopy. 1998;30:333-338.
35. van den Boogert J, Houtsmuller AB, de Rooij FWM, de BruinRWF, Siersema PD, van Hillegersberg R. Kinetics, localization,and mechanism of 5-aminolevulinic acid-induced porphyrin accu-mulation in normal and Barrett’s-like rat esophagus. Lasers SurgMed. 1999;24:3-13.
36. Perelman LT, Backman V, Wallace M, et al. Observation of peri-odic fine structure in reflectance from biological tissue: a newtechnique for measuring nuclear size distribution. Phys Rev Lett.1998;80:627-630.
37. Wallace MB, Shields SJ, Perelmen LT, et al. Fiber-optic detectionof low-grade dysplasia in patients with Barrett’s esophagus usingreflectance spectroscopy [abstract]. Gastroenterology. 1998;114(4,pt 2):A327. Abstract G1337.
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.