endocrine – thyroid and parathyroid glands dr. geoffrey pollack october 10, 2007
TRANSCRIPT
Endocrine – Thyroid Endocrine – Thyroid and Parathyroid and Parathyroid GlandsGlands
Dr. Geoffrey PollackDr. Geoffrey Pollack
October 10, 2007October 10, 2007
Endocrine - ThyroidEndocrine - Thyroid
EmbryologyEmbryology Median thyroid anlage forms at base of tongue in Median thyroid anlage forms at base of tongue in
region of foramen cecum during 3region of foramen cecum during 3rdrd week of week of gestationgestation
Endodermal pocketEndodermal pocket Originates from primitive alimentary tract protruding Originates from primitive alimentary tract protruding
between first pair of pharyngeal pouchesbetween first pair of pharyngeal pouches Subsequently descends in the midline to reach its Subsequently descends in the midline to reach its
normal anatomic location developing into a bi-lobed normal anatomic location developing into a bi-lobed organorgan
Endocrine - ThyroidEndocrine - Thyroid
EmbryologyEmbryology Iodine trapping occurs as thyroid hormones are first seen Iodine trapping occurs as thyroid hormones are first seen
in the 3in the 3rdrd month of gestation month of gestation The principle cells of the thyroid form thyroid follicles and The principle cells of the thyroid form thyroid follicles and
produce thyroglobulinproduce thyroglobulin Lateral anlagen develop from the 4Lateral anlagen develop from the 4 thth pharyngeal pouch pharyngeal pouch
and fuse with the median anlagen at about the 7and fuse with the median anlagen at about the 7 thth week week of gestationof gestation
Ultimobranchial bodies which may orignate from the 4Ultimobranchial bodies which may orignate from the 4 thth pharyngeal pouch may give rise to parafollicular or C pharyngeal pouch may give rise to parafollicular or C cellscells
C cells secrete calcitoninC cells secrete calcitonin C cells originate from neural crest and are of ectodermal C cells originate from neural crest and are of ectodermal
originorigin
Endocrine - ThyroidEndocrine - Thyroid
Embryology – Thyroglossal Duct Cyst (TGDC)Embryology – Thyroglossal Duct Cyst (TGDC) TGDC are the most common non-odontogenic TGDC are the most common non-odontogenic
cysts occurring in the neckcysts occurring in the neck TGDC are second only to benign TGDC are second only to benign
lymphadenopathy of all cervical masses in lymphadenopathy of all cervical masses in children (70% of all congenital neck cysts) children (70% of all congenital neck cysts)
TGD represents the original attachment of the TGD represents the original attachment of the thyroid mass to the oropharynxthyroid mass to the oropharynx
TGD is normally resorbed by the 6TGD is normally resorbed by the 6thth week of week of gestationgestation
Distal end of duct may be retained as the Distal end of duct may be retained as the pyramidal lobe of thyroidpyramidal lobe of thyroid
Endocrine - ThyroidEndocrine - Thyroid
Embryology – Thyroglossal Duct Cyst (TGDC)Embryology – Thyroglossal Duct Cyst (TGDC) TGDC are located at or near midline between base of TGDC are located at or near midline between base of
tongue and suprasternal notchtongue and suprasternal notch 75% of TGDC are located just inferior to the hyoid bone75% of TGDC are located just inferior to the hyoid bone The importance of TGDC is related to The importance of TGDC is related to
High incidence of infectionHigh incidence of infection Recurrence after inadequate surgeryRecurrence after inadequate surgery Possible neoplastic changePossible neoplastic change
One-third are detected in first year of life; 50% are One-third are detected in first year of life; 50% are detected by age 10detected by age 10
They present as painless midline lesions that grow They present as painless midline lesions that grow slowlyslowly
They can increase in size after a URIThey can increase in size after a URI
Endocrine - ThyroidEndocrine - Thyroid
Embryology – Thyroglossal Duct Cyst (TGDC)Embryology – Thyroglossal Duct Cyst (TGDC) TGDC contains thyroid tissue (and perhaps only TGDC contains thyroid tissue (and perhaps only
functioning thyroid tissue in body – obtain sonogram functioning thyroid tissue in body – obtain sonogram in an adult prior to OR)in an adult prior to OR)
Rarely a source of thyroid carcinoma (usually Rarely a source of thyroid carcinoma (usually papillary)papillary)
Treatment: surgery via Treatment: surgery via SistrunkSistrunk procedure procedure This includes This includes midportion of hyoid bonemidportion of hyoid bone Must excise entire cyst/tract/fistula up to base of tongueMust excise entire cyst/tract/fistula up to base of tongue Recurrence rate with Sistrunk procedure is low (less than Recurrence rate with Sistrunk procedure is low (less than
4% compared with 50% when not done using this 4% compared with 50% when not done using this procedure)procedure)
Endocrine - ThyroidEndocrine - Thyroid
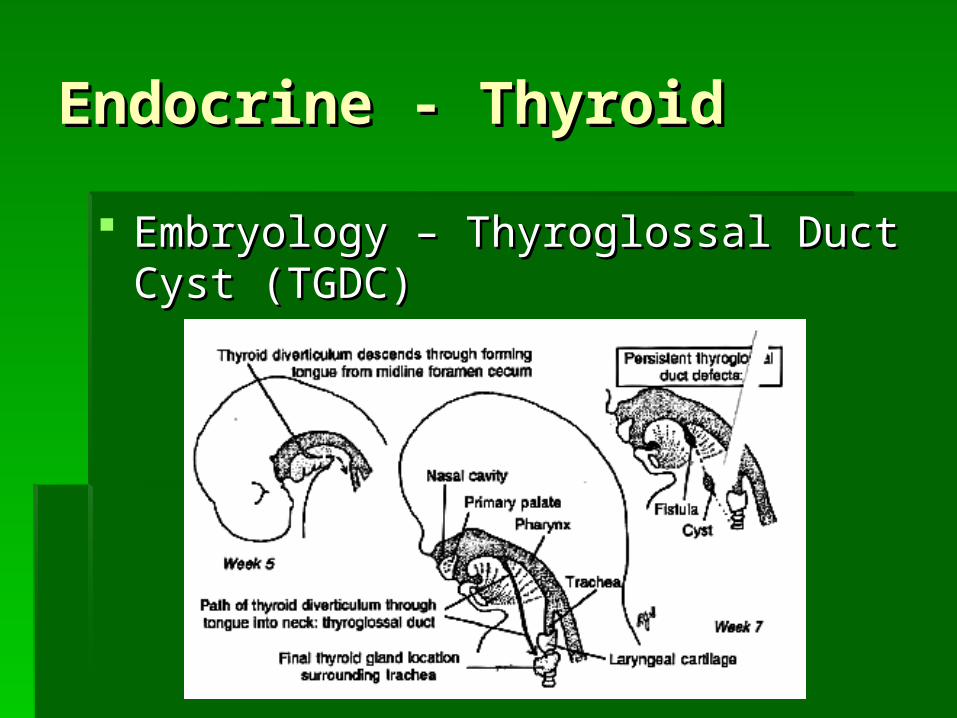
Embryology – Thyroglossal Duct Cyst Embryology – Thyroglossal Duct Cyst (TGDC)(TGDC)
Endocrine - ThyroidEndocrine - Thyroid
Embryology – Thyroglossal Duct Cyst Embryology – Thyroglossal Duct Cyst (TGDC)(TGDC)
Endocrine - ThyroidEndocrine - Thyroid
Embryology – Lingual TonsilEmbryology – Lingual Tonsil Failure of thyroid anlage to migrate can Failure of thyroid anlage to migrate can
result in persistence of a functional lingual result in persistence of a functional lingual thyroid glandthyroid gland May represent May represent onlyonly functional thyroid tissue functional thyroid tissue Excision may be necessary for airway Excision may be necessary for airway
obstruction, swallowing difficulty, or hemorrhageobstruction, swallowing difficulty, or hemorrhage
Endocrine - ThyroidEndocrine - Thyroid
AnatomyAnatomy Normal gland weights between 20-30 gramsNormal gland weights between 20-30 grams Thyroid lobes lie subadjacent to thyroid cartilage, anterior to Thyroid lobes lie subadjacent to thyroid cartilage, anterior to
larynx and trachealarynx and trachea 2 lobes connected by the isthmus 2 lobes connected by the isthmus Midline pyramidal process, distal remnant of TGD is present in Midline pyramidal process, distal remnant of TGD is present in
40-50% of adults40-50% of adults Anterior aspect covered by strap musclesAnterior aspect covered by strap muscles Posterolaterally lie common carotid arteries, internal jugular Posterolaterally lie common carotid arteries, internal jugular
veins and Vagus nervesveins and Vagus nerves Gland is covered by connective tissue layer derived from pre-Gland is covered by connective tissue layer derived from pre-
tracheal fasciatracheal fascia Fascia connects thyroid to upper tracheal rings and cricoid Fascia connects thyroid to upper tracheal rings and cricoid
posteromedially (Berry’s ligament)posteromedially (Berry’s ligament)
Endocrine - ThyroidEndocrine - Thyroid
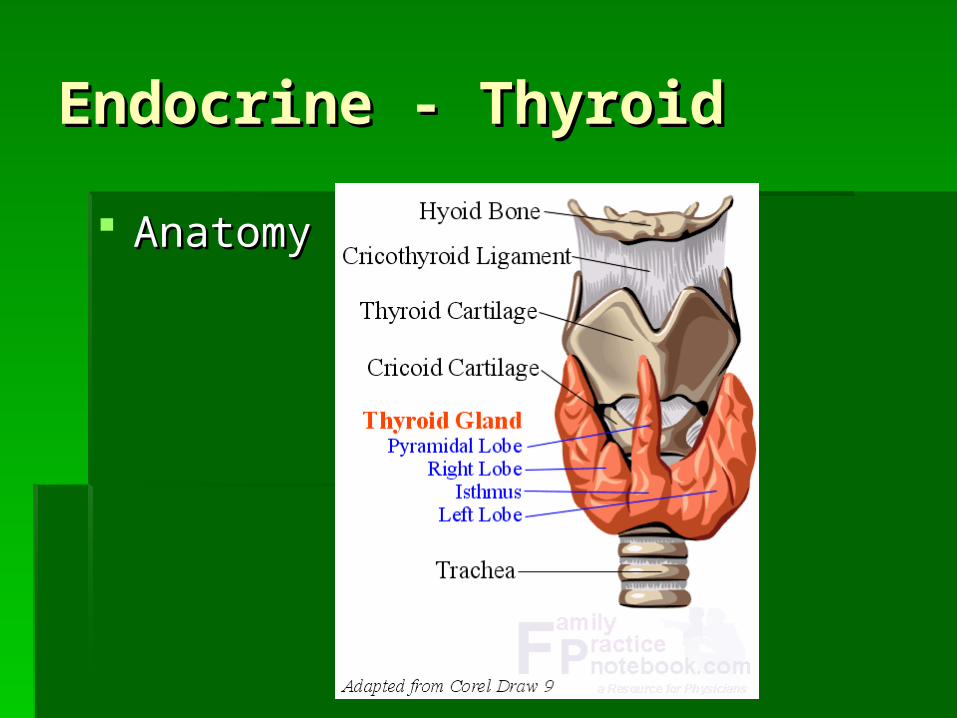
AnatomyAnatomy

Endocrine - ThyroidEndocrine - Thyroid
Endocrine - ThyroidEndocrine - Thyroid
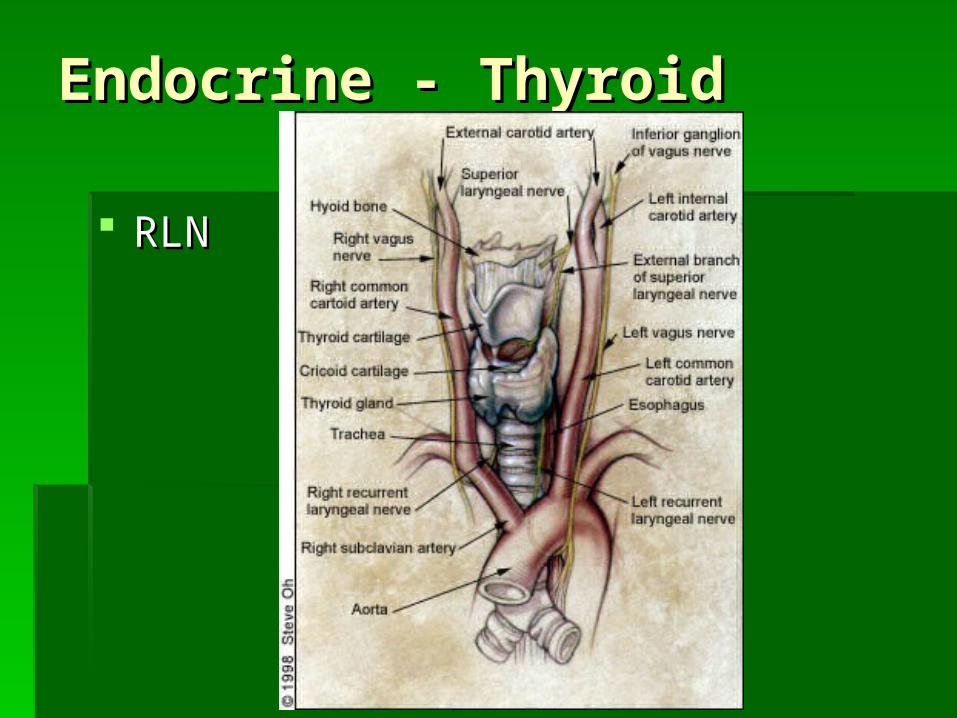
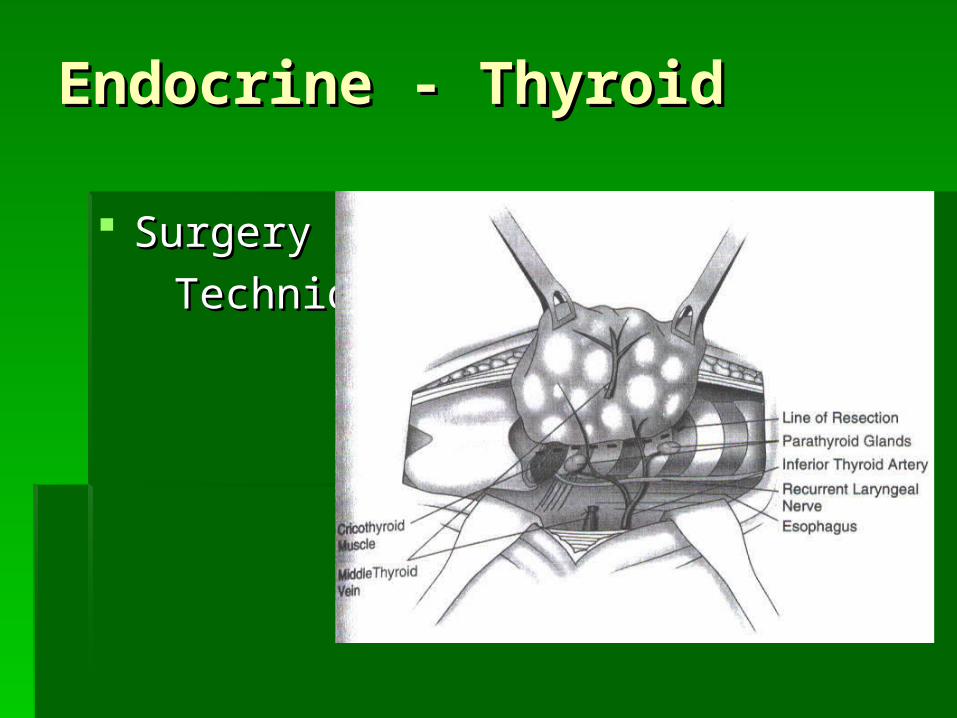
Anatomy - Recurrent laryngeal nerve (RLN)Anatomy - Recurrent laryngeal nerve (RLN) Arises in the chest as a branch of the Vagus nerveArises in the chest as a branch of the Vagus nerve The right nerve loops under the right subclavian The right nerve loops under the right subclavian
arteryartery The left nerve loops under the aortic archThe left nerve loops under the aortic arch The right can be non-recurrent in a small number of The right can be non-recurrent in a small number of
casescases As it ascends in the neck from the chest, the As it ascends in the neck from the chest, the
recurrent nerve usually runs just under Berry’s recurrent nerve usually runs just under Berry’s ligament before entering the larynx (posterior to the ligament before entering the larynx (posterior to the thyroid at the level of the cricothyroid junction)thyroid at the level of the cricothyroid junction)
Endocrine - ThyroidEndocrine - Thyroid
Anatomy - RLNAnatomy - RLN Motor nerve to intrinsic muscles of larynx except Motor nerve to intrinsic muscles of larynx except
cricothyroidcricothyroid Sensory to mucosa below vocal cords Sensory to mucosa below vocal cords Unilateral injury to the nerve can result in a Unilateral injury to the nerve can result in a
weakened voice and can lead to shortness of breathweakened voice and can lead to shortness of breath Bilateral injury is a devastating complication causing Bilateral injury is a devastating complication causing
airway obstructionairway obstruction RLN must be identified by a surgeon during any RLN must be identified by a surgeon during any
procedure performed on the thyroid glandprocedure performed on the thyroid gland
Endocrine - ThyroidEndocrine - Thyroid
RLNRLN
Endocrine - ThyroidEndocrine - Thyroid
Anatomy – Superior laryngeal nerve (SLN)Anatomy – Superior laryngeal nerve (SLN) Arises from the Vagus nerve at the skull base and Arises from the Vagus nerve at the skull base and
descends along the carotid artery in the neckdescends along the carotid artery in the neck 2 branches2 branches
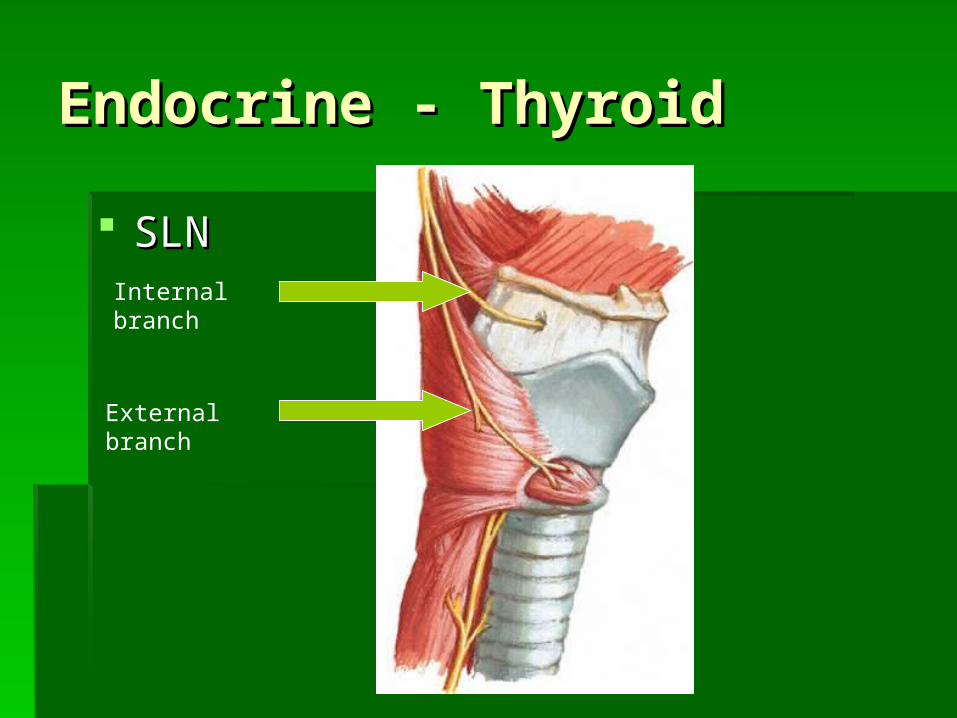
Internal branch is sensory to the larynx above the vocal Internal branch is sensory to the larynx above the vocal cords. It enters the larynx at the level of the thyrohyoid cords. It enters the larynx at the level of the thyrohyoid membranemembrane
External branch is motor to the cricothyroid muscle (tenses External branch is motor to the cricothyroid muscle (tenses the vocal cord) and inferior constrictor muscle. It enters the vocal cord) and inferior constrictor muscle. It enters the larynx behind the cricothyroid muscle. Injury to this the larynx behind the cricothyroid muscle. Injury to this nerve will produce hoarseness. Injury can be devastating nerve will produce hoarseness. Injury can be devastating to professional singersto professional singers
Endocrine - ThyroidEndocrine - Thyroid
SLNSLNInternal branch
External branch
Endocrine - ThyroidEndocrine - Thyroid
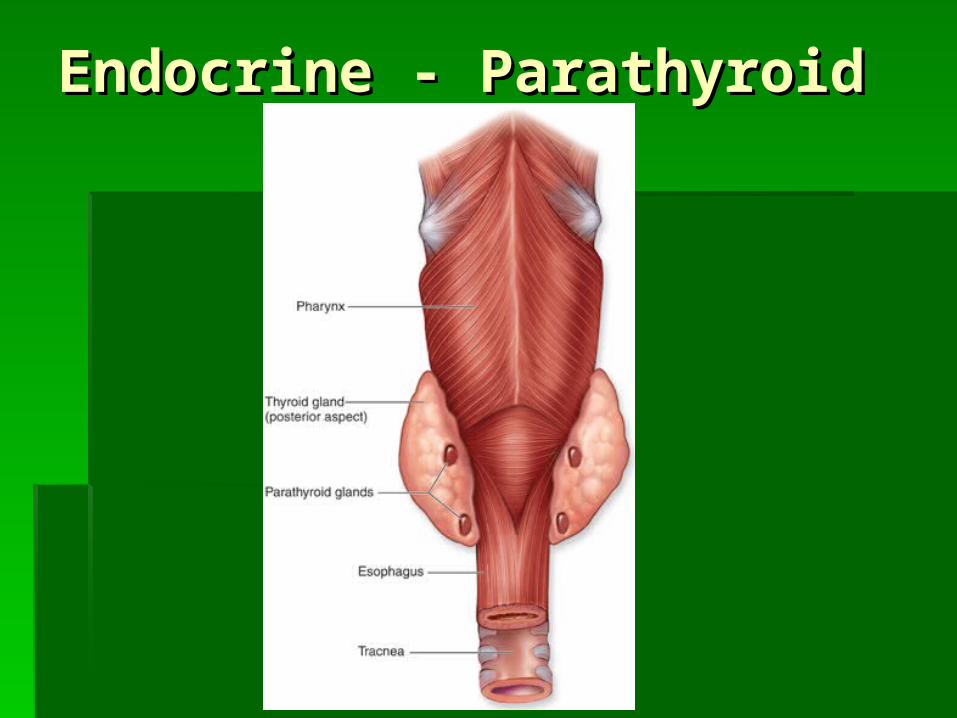
AnatomyAnatomy 4 parathyroid glands are associated with the 4 parathyroid glands are associated with the
thyroid glandthyroid gland 2 superior2 superior 2 inferior2 inferior
The parathyroid glands must be identified The parathyroid glands must be identified by the surgeon during any procedure by the surgeon during any procedure performed on the thyroid glandperformed on the thyroid gland
Endocrine - ThyroidEndocrine - Thyroid
AnatomyAnatomy Thyroid gland supplied by 4 main arteriesThyroid gland supplied by 4 main arteries
2 superior thyroid arteries (branches of external carotid)2 superior thyroid arteries (branches of external carotid) 2 inferior thyroid arteries (branches of thyrocervical trunk)2 inferior thyroid arteries (branches of thyrocervical trunk)
Superior, middle and inferior thyroid veins drain Superior, middle and inferior thyroid veins drain blood into internal jugular vein and brachiocephalic blood into internal jugular vein and brachiocephalic veinsveins
Lymphatic drainageLymphatic drainage Intraglandular – travels through isthmus (accounts for Intraglandular – travels through isthmus (accounts for
relative frequency of multifocal tumors)relative frequency of multifocal tumors) Central compartment (from hyoid to innominate artery)Central compartment (from hyoid to innominate artery) Jugular chain (especially levels II, III, IV, V)Jugular chain (especially levels II, III, IV, V)
Endocrine - ThyroidEndocrine - Thyroid
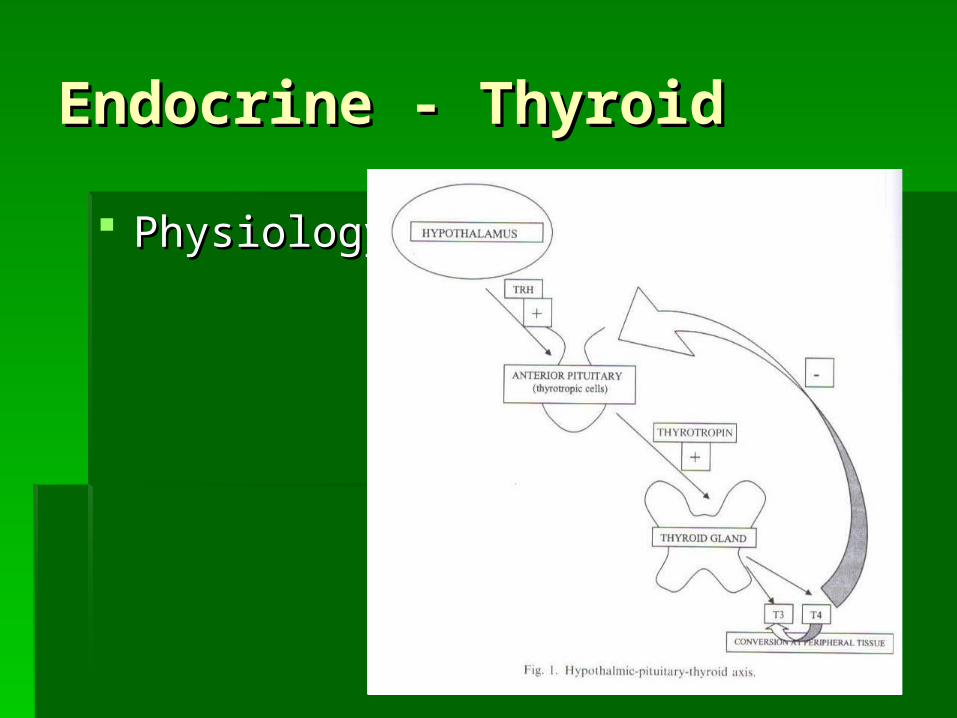
PhysiologyPhysiology Thyroid gland converts inorganic iodine into thyroid hormone (TH)Thyroid gland converts inorganic iodine into thyroid hormone (TH) Iodine enters thyroid and is trapped by follicular cellsIodine enters thyroid and is trapped by follicular cells TH synthesis takes place at interface of cell and thyroglobulin (THG)TH synthesis takes place at interface of cell and thyroglobulin (THG) THG is a glycoprotein (colloid)THG is a glycoprotein (colloid) Iodine oxidized by thyroid peroxidases to an activated form of iodine Iodine oxidized by thyroid peroxidases to an activated form of iodine
that binds the amino acid tyrosine forming T3 and T4 (TH)that binds the amino acid tyrosine forming T3 and T4 (TH) The newly formed TH is stored in THGThe newly formed TH is stored in THG Thyroid gland releases T3 and T4 into the circulationThyroid gland releases T3 and T4 into the circulation
20% of all T3 and the majority of T420% of all T3 and the majority of T4 99% of TH is protein-bound (thyroxin binding globulin, prealbumin, 99% of TH is protein-bound (thyroxin binding globulin, prealbumin,
albumin)albumin) 80% of T3 is formed from T4 in peripheral tissue80% of T3 is formed from T4 in peripheral tissue
Thyroid hormone release is regulated by TSH (thyrotropin stimulating Thyroid hormone release is regulated by TSH (thyrotropin stimulating hormone) from the pituitaryhormone) from the pituitary
Endocrine - ThyroidEndocrine - Thyroid
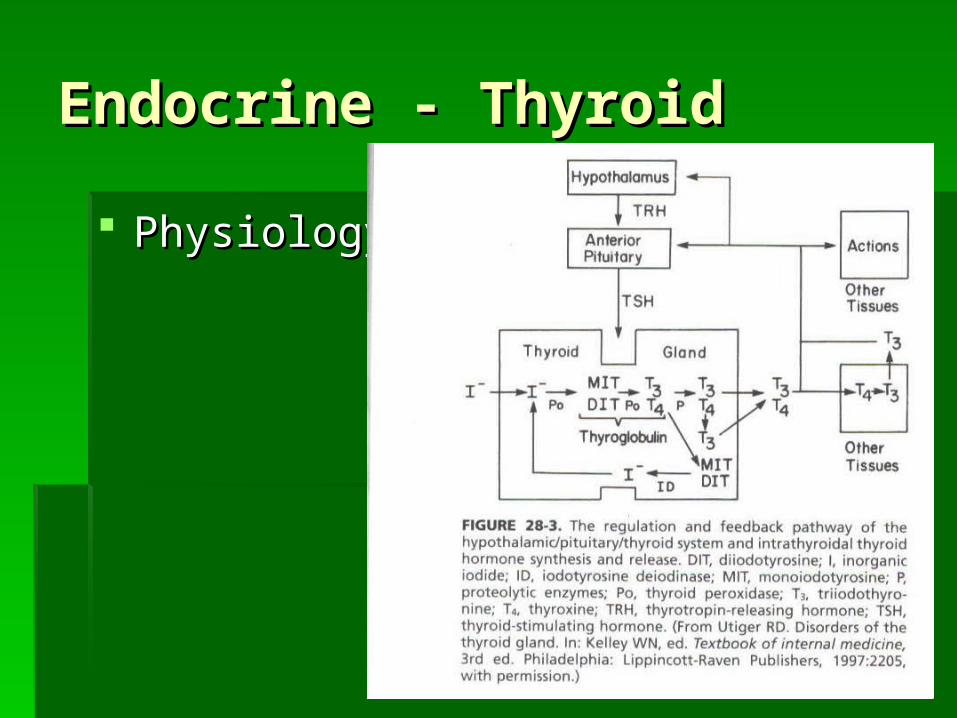
PhysiologyPhysiology
Endocrine - ThyroidEndocrine - Thyroid
PhysiologyPhysiology
Endocrine - ThyroidEndocrine - Thyroid
PhysiologyPhysiology Thyroid function testsThyroid function tests
Direct testsDirect tests Radioactive iodine uptake (RAIU)Radioactive iodine uptake (RAIU)
Tests of hormone concentration and bindingTests of hormone concentration and binding T4T4 T3T3 T3 resin uptakeT3 resin uptake T4 index (Totally T4 + T3 resin uptake)T4 index (Totally T4 + T3 resin uptake) T7T7
Tests of hypothalamic – pituitary – thyroid axisTests of hypothalamic – pituitary – thyroid axis TSHTSH
Other testsOther tests Anti-thyroid peroxidaseAnti-thyroid peroxidase Anti-thyroglobulinAnti-thyroglobulin
Endocrine - ThyroidEndocrine - Thyroid
Endocrine - ThyroidEndocrine - Thyroid
1. Operations on the thyroid account for the 1. Operations on the thyroid account for the largest number of procedures performed for largest number of procedures performed for tumors of the head and necktumors of the head and neck
2. Thyroid carcinoma is unique because of the 2. Thyroid carcinoma is unique because of the low-grade nature of the majority of lesionslow-grade nature of the majority of lesions
3. The major problem for surgeons 3. The major problem for surgeons Correct diagnosis of the small number of malignant Correct diagnosis of the small number of malignant
tumors from the large number of benign growthstumors from the large number of benign growths Selecting the optimal surgical treatment using a safe Selecting the optimal surgical treatment using a safe
effective techniqueeffective technique
Endocrine - ThyroidEndocrine - Thyroid
Benign conditionsBenign conditions Benign diseases are common and affect Benign diseases are common and affect
women 5 times more than menwomen 5 times more than men About 1% of women develop hypo or About 1% of women develop hypo or
hyperthyroidismhyperthyroidism Benign conditions can be categorized as Benign conditions can be categorized as
Toxic [toxic multinodular goiter, toxic solitary Toxic [toxic multinodular goiter, toxic solitary nodule, diffuse toxic goiter (Graves’ disease)]nodule, diffuse toxic goiter (Graves’ disease)]
Non-toxic [diffuse and nodular (solitary or Non-toxic [diffuse and nodular (solitary or multiple goiter)]multiple goiter)]
Inflammatory diseases consisting of thyroiditisInflammatory diseases consisting of thyroiditis
Endocrine - ThyroidEndocrine - Thyroid
Benign conditionsBenign conditions With the exception of hyperthyroidism, benign With the exception of hyperthyroidism, benign
thyroid diseases are of significance to the surgeon thyroid diseases are of significance to the surgeon either because of mechanical constraint on the either because of mechanical constraint on the upper aerodigestive tract or because it is not upper aerodigestive tract or because it is not possible to rule out carcinoma within a nodular or possible to rule out carcinoma within a nodular or diffuse lesiondiffuse lesion Nodular increase may be indistinguishable from goiter or Nodular increase may be indistinguishable from goiter or
cancercancer Autoimmune disease may cause firm nodular enlargement Autoimmune disease may cause firm nodular enlargement
difficult to distinguish from carcinomadifficult to distinguish from carcinoma Follicular adenoma is a true neoplasm that may be Follicular adenoma is a true neoplasm that may be
indistinguishable from follicular carcinoma except by indistinguishable from follicular carcinoma except by permanent histologic exam after surgery (vascular or permanent histologic exam after surgery (vascular or capsule invasion)capsule invasion)
Endocrine - ThyroidEndocrine - Thyroid
Benign conditions – HyperthyroidismBenign conditions – Hyperthyroidism Hyperthyroidism – an excess of production and Hyperthyroidism – an excess of production and
secretion of thyroid hormone with a characteristic secretion of thyroid hormone with a characteristic hypermetabolism resulthypermetabolism result
Thyrotoxicosis – hypermetabolic state that can be Thyrotoxicosis – hypermetabolic state that can be caused by hyperthyroidism (or can occur without caused by hyperthyroidism (or can occur without hyperthyroidism)hyperthyroidism)
Lab testsLab tests Elevated T4 or T3Elevated T4 or T3 Suppressed TSHSuppressed TSH Normal RAIUNormal RAIU
Endocrine – Endocrine – ThyroidThyroid
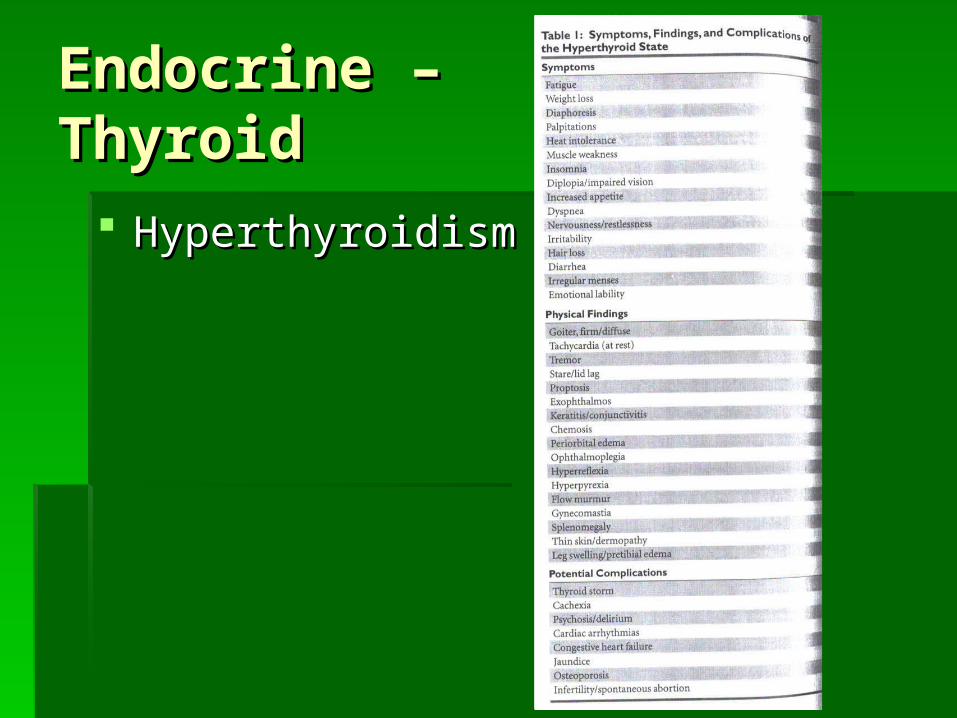
HyperthyroidismHyperthyroidism
Endocrine - ThyroidEndocrine - Thyroid
Benign conditions – HyperthyroidismBenign conditions – Hyperthyroidism TreatmentTreatment
Usually medical but surgery may be required if Usually medical but surgery may be required if medical treatment has failed or is contraindicated medical treatment has failed or is contraindicated in 3 conditionsin 3 conditions
Graves’ diseaseGraves’ disease Toxic multinodular goiter (TMNG)Toxic multinodular goiter (TMNG) Toxic solitary nodule (TSN)Toxic solitary nodule (TSN)

Endocrine - ThyroidEndocrine - Thyroid
Benign conditions – HyperthyroidismBenign conditions – Hyperthyroidism Graves’ diseaseGraves’ disease
Autoimmune toxic diffuse goiterAutoimmune toxic diffuse goiter Antibodies against TSH receptorAntibodies against TSH receptor 6-7 times more common in women6-7 times more common in women Genetic factors play a roleGenetic factors play a role TriadTriad
Diffuse toxic goiterDiffuse toxic goiter Infiltrative opthalmopathyInfiltrative opthalmopathy Infiltrative dermopathy (pre-tibial myxedema)Infiltrative dermopathy (pre-tibial myxedema)
Endocrine - ThyroidEndocrine - Thyroid
Benign conditions – HyperthyroidismBenign conditions – Hyperthyroidism Graves’ disease – TreatmentGraves’ disease – Treatment
Antithyroid drugs Antithyroid drugs Thionamides (PTU, Tapazole)Thionamides (PTU, Tapazole)
Inhibits organification of iodine and coupling of iodothyronineInhibits organification of iodine and coupling of iodothyronine Must be used for long duration; recurrence can occur if meds Must be used for long duration; recurrence can occur if meds
discontinueddiscontinued Success correlates inversely with gland sizeSuccess correlates inversely with gland size May cause agranulocytosisMay cause agranulocytosis
Beta-blockers – usually in adjuvant setting if patient is symptomatic Beta-blockers – usually in adjuvant setting if patient is symptomatic or pre-surgeryor pre-surgery
Radioactive IodineRadioactive Iodine Most commonly chosen therapyMost commonly chosen therapy Hypothyroidism expected complication Hypothyroidism expected complication
Endocrine - ThyroidEndocrine - Thyroid
Benign conditions – HyperthyroidismBenign conditions – Hyperthyroidism Graves’ disease – Treatment: SurgeryGraves’ disease – Treatment: Surgery
10% of patients require surgery10% of patients require surgery Pregnancy (131-I contraindicated)Pregnancy (131-I contraindicated) Failure of drug therapyFailure of drug therapy Concurrent nodular disease with positive FNAConcurrent nodular disease with positive FNA
Pre-op preparation to attain euthyroid state Pre-op preparation to attain euthyroid state increases safety (PTU, Tapazole, Beta-blockers, increases safety (PTU, Tapazole, Beta-blockers, Iodine)Iodine) Controls hypermetabolic stateControls hypermetabolic state Decreases risk of thyroid stormDecreases risk of thyroid storm May decrease vasularityMay decrease vasularity
Endocrine - ThyroidEndocrine - Thyroid
Benign conditions – HyperthyroidismBenign conditions – Hyperthyroidism Graves’ disease – Treatment: SurgeryGraves’ disease – Treatment: Surgery
Total vs. Subtotal thyroidectomyTotal vs. Subtotal thyroidectomy TotalTotal
Hypothyroidism expectedHypothyroidism expected Risks to nerves and parathyroidsRisks to nerves and parathyroids Recurrence of hyperthyroidism approaches 0%Recurrence of hyperthyroidism approaches 0%
Subtotal – purposefully leaving tissue behind at poles or Subtotal – purposefully leaving tissue behind at poles or laterallylaterally
Bilateral subtotalBilateral subtotal Unilateral total with contralateral subtotalUnilateral total with contralateral subtotal 50-60% recurrence rate50-60% recurrence rate Recurrence can occur 1-30 years after surgeryRecurrence can occur 1-30 years after surgery Re-op much more difficultRe-op much more difficult
Endocrine - ThyroidEndocrine - Thyroid
Benign conditions – HyperthyroidismBenign conditions – Hyperthyroidism Toxic multinodular goiter (TMG)Toxic multinodular goiter (TMG)
““Hot” nodules take up radioactive tracer at higher than Hot” nodules take up radioactive tracer at higher than normal levelsnormal levels
““Hot” nodules can beHot” nodules can be Autonomous (not responsive to TSH suppression)Autonomous (not responsive to TSH suppression) Not autonomous (responsive to TSH suppression)Not autonomous (responsive to TSH suppression)
Autonomous nodules can be Autonomous nodules can be Toxic (thyroid hormone in excess clinically hyperthyroid)Toxic (thyroid hormone in excess clinically hyperthyroid) Non-toxicNon-toxic
Rate of cancer in “hot” nodules is lowRate of cancer in “hot” nodules is low
Endocrine - ThyroidEndocrine - Thyroid
Benign conditions – HyperthyroidismBenign conditions – Hyperthyroidism Toxic multinodular goiter (TMG)Toxic multinodular goiter (TMG)
Over age 50 in setting of longstanding nontoxic Over age 50 in setting of longstanding nontoxic multinodular goitermultinodular goiter
Nodules become autonomous and toxic (clinically Nodules become autonomous and toxic (clinically hyperthyroid) - cannot be suppressedhyperthyroid) - cannot be suppressed
Treatment:Treatment: Same as Graves’ disease (thionamides, radioiodine, surgery)Same as Graves’ disease (thionamides, radioiodine, surgery) Radioiodine treatment of choiceRadioiodine treatment of choice Surgery performed for large goiters and compressive Surgery performed for large goiters and compressive
symptoms after patient made euthyroid. Remove all nodulessymptoms after patient made euthyroid. Remove all nodules

Endocrine - ThyroidEndocrine - Thyroid
Benign conditions – HyperthyroidismBenign conditions – Hyperthyroidism Toxic solitary nodule (TSN)Toxic solitary nodule (TSN)
Most are follicular adenomas that can have Most are follicular adenomas that can have spontaneous infarctionspontaneous infarction
Less than 1% are carcinomaLess than 1% are carcinoma Life cycle (“hot” nodule Life cycle (“hot” nodule autonomous “hot” autonomous “hot”
hodules hodules autonomous TSN) autonomous TSN) More worrisome in nodules greater than 2.5-3cmMore worrisome in nodules greater than 2.5-3cm Surgery for worrisome nodules otherwise 131-I Surgery for worrisome nodules otherwise 131-I
therapytherapy
Endocrine - ThyroidEndocrine - Thyroid
Benign conditions – HyperthyroidismBenign conditions – Hyperthyroidism
Endocrine - ThyroidEndocrine - Thyroid
Benign conditions – ThyroiditisBenign conditions – Thyroiditis Includes heterogeneous mixture of diseases Includes heterogeneous mixture of diseases
with variable etiologies, presentation and with variable etiologies, presentation and treatmenttreatment
Can result in diffusely enlarged, nodular and Can result in diffusely enlarged, nodular and even normal gland in appearanceeven normal gland in appearance
May be euthyroid, hypo or hyperMay be euthyroid, hypo or hyper Often preceding triggers (partuition, viruses, Often preceding triggers (partuition, viruses,
medication)medication)
Endocrine - ThyroidEndocrine - Thyroid
Benign conditions – ThyroiditisBenign conditions – Thyroiditis Classified byClassified by
Descriptive, subjective history (painful or not Descriptive, subjective history (painful or not painful)painful)
Temporal course (acute, subacute, chronic)Temporal course (acute, subacute, chronic) Histopathology (hyperplastic, lymphocytic, Histopathology (hyperplastic, lymphocytic,
granulomatous or fibrosis)granulomatous or fibrosis) Doctor’s name (Graves, Hashimoto, DeQuervain, Doctor’s name (Graves, Hashimoto, DeQuervain,
Reidel) Reidel)
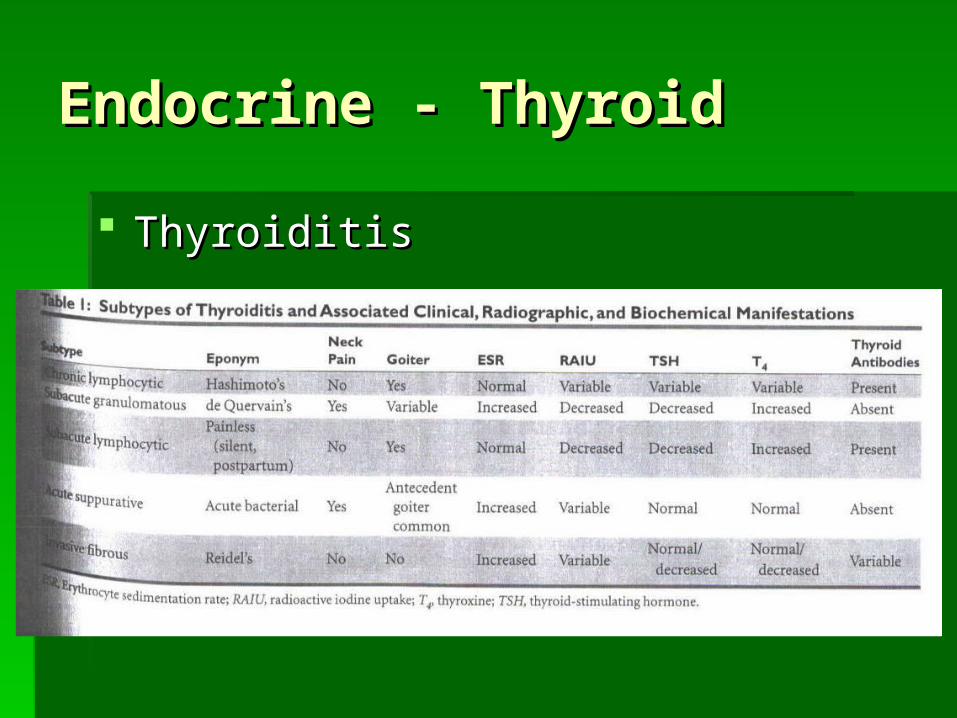
Endocrine - ThyroidEndocrine - Thyroid
ThyroiditisThyroiditis
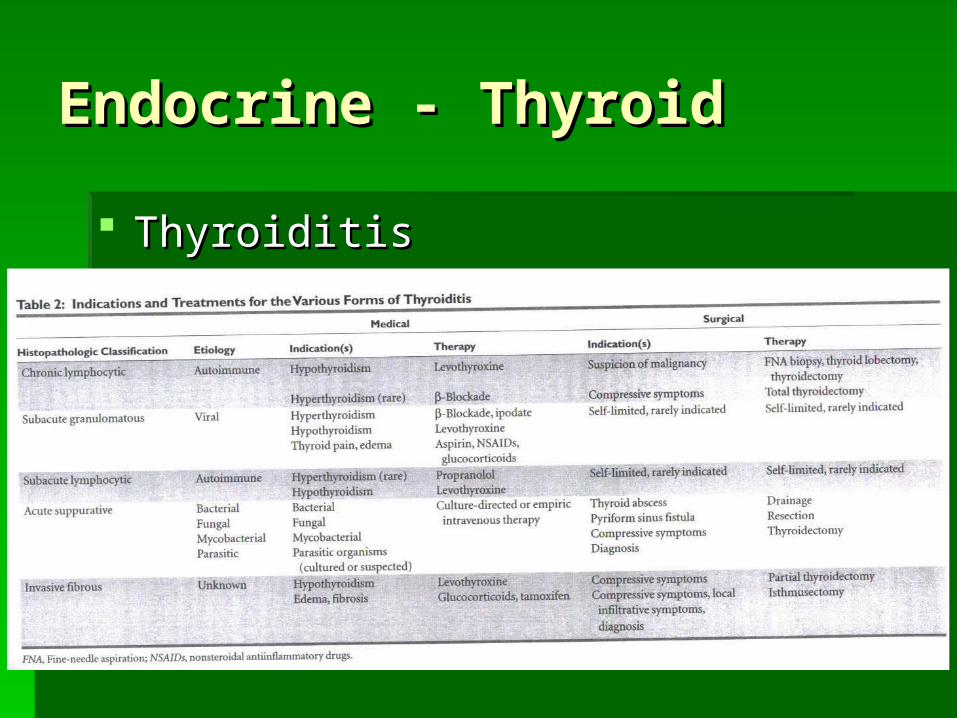
Endocrine - ThyroidEndocrine - Thyroid
ThyroiditisThyroiditis

Endocrine - ThyroidEndocrine - Thyroid
1. Operations on the thyroid account for the 1. Operations on the thyroid account for the largest number of procedures performed for largest number of procedures performed for tumors of the head and necktumors of the head and neck
2. Thyroid carcinoma is unique because of the 2. Thyroid carcinoma is unique because of the low-grade nature of the majority of lesionslow-grade nature of the majority of lesions
3. The major problem for surgeons 3. The major problem for surgeons Correct diagnosis of the small number of malignant Correct diagnosis of the small number of malignant
tumors from the large number of benign growthstumors from the large number of benign growths Selecting the optimal surgical treatment using a safe Selecting the optimal surgical treatment using a safe
effective techniqueeffective technique

Endocrine - ThyroidEndocrine - Thyroid
Benign conditionsBenign conditions Benign diseases are common and affect Benign diseases are common and affect
women 5 times more than menwomen 5 times more than men About 1% of women develop hypo or About 1% of women develop hypo or
hyperthyroidismhyperthyroidism Benign conditions can be categorized as Benign conditions can be categorized as
Toxic [toxic multinodular goiter, toxic solitary Toxic [toxic multinodular goiter, toxic solitary nodule, diffuse toxic goiter (Graves’ disease)]nodule, diffuse toxic goiter (Graves’ disease)]
Non-toxic [diffuse and nodular (solitary or Non-toxic [diffuse and nodular (solitary or multiple goiter)]multiple goiter)]
Inflammatory diseases consisting of thyroiditisInflammatory diseases consisting of thyroiditis
Endocrine - ThyroidEndocrine - Thyroid
Benign conditionsBenign conditions With the exception of hyperthyroidism, benign With the exception of hyperthyroidism, benign
thyroid diseases are of significance to the surgeon thyroid diseases are of significance to the surgeon either because of mechanical constraint on the either because of mechanical constraint on the upper aerodigestive tract or because it is not upper aerodigestive tract or because it is not possible to rule out carcinoma within a nodular or possible to rule out carcinoma within a nodular or diffuse lesiondiffuse lesion Nodular increase may be indistinguishable from goiter or Nodular increase may be indistinguishable from goiter or
cancercancer Autoimmune disease may cause firm nodular enlargement Autoimmune disease may cause firm nodular enlargement
difficult to distinguish from carcinomadifficult to distinguish from carcinoma Follicular adenoma is a true neoplasm that may be Follicular adenoma is a true neoplasm that may be
indistinguishable from follicular carcinoma except by indistinguishable from follicular carcinoma except by permanent histologic exam after surgery (vascular or permanent histologic exam after surgery (vascular or capsule invasion)capsule invasion)
Endocrine - ThyroidEndocrine - Thyroid
Thyroid NoduleThyroid Nodule Range of disease for thyroid noduleRange of disease for thyroid nodule
Benign cystBenign cyst Lethal malignancyLethal malignancy
Need strategy to identify malignant vs. Need strategy to identify malignant vs. benignbenign

Endocrine - ThyroidEndocrine - Thyroid
Thyroid NoduleThyroid Nodule PrevalencePrevalence
5% of adults by palpation (greater than 1.5cm)5% of adults by palpation (greater than 1.5cm) 30% of adults by sonography30% of adults by sonography Increased riskIncreased risk
FemaleFemale AgeAge History of XRTHistory of XRT Endemic iodine deficiency Endemic iodine deficiency
Endocrine - ThyroidEndocrine - Thyroid
Thyroid NoduleThyroid Nodule Risk of cancerRisk of cancer
New thyroid nodules 275,000 per yearNew thyroid nodules 275,000 per year 1:20 new nodules are malignant (This represents 1:20 new nodules are malignant (This represents
5%; however in some studies it can approach 5%; however in some studies it can approach 15%)15%)
Death from thyroid carcinoma 1,100 per yearDeath from thyroid carcinoma 1,100 per year 1:200 new nodules are lethal cancer1:200 new nodules are lethal cancer
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – Differential DiagnosisThyroid Nodule – Differential Diagnosis Colloid nodule – multinodular goiterColloid nodule – multinodular goiter AdenomaAdenoma CystCyst Focal thyroiditisFocal thyroiditis CarcinomaCarcinoma
95%
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – Differential DiagnosisThyroid Nodule – Differential Diagnosis Metastasis to thyroidMetastasis to thyroid Lobar hypertrophy status post hemithyroidectomyLobar hypertrophy status post hemithyroidectomy Non-thyroidNon-thyroid
Lymph nodeLymph node Laryngeal, esophageal tumorLaryngeal, esophageal tumor TGDCTGDC Cystic hygroma, dermoid, teratomaCystic hygroma, dermoid, teratoma LaryngoceleLaryngocele Nerve sheath tumorNerve sheath tumor
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – HistoryThyroid Nodule – History Age <20 or >60Age <20 or >60 Male (nodular disease is more common in women, but risk of cancer Male (nodular disease is more common in women, but risk of cancer
is 2 times greater in men)is 2 times greater in men) History of XRTHistory of XRT Family history (MTC)Family history (MTC) Size >4cmSize >4cm Rapid growthRapid growth Invasion/compressionInvasion/compression
Trachea/larynx: airway, vocal cord paralysis, coughTrachea/larynx: airway, vocal cord paralysis, cough Esophagus: dysphasiaEsophagus: dysphasia
Pain (subacute thyroiditis or hemorrhage)Pain (subacute thyroiditis or hemorrhage) Thyroid functional statusThyroid functional status
Hashimoto’sHashimoto’s MTNGMTNG STNSTN Remember most cancers are euthyroid that is, no functional deficiencyRemember most cancers are euthyroid that is, no functional deficiency
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – HistoryThyroid Nodule – History Low dose ionizing radiationLow dose ionizing radiation
Tonsils/thymus, acne, tinea (ended approx. Tonsils/thymus, acne, tinea (ended approx. 1955), Hodgkin’s, scatter from breast1955), Hodgkin’s, scatter from breast
20-30% develop nodules20-30% develop nodules Patients presenting with such a history have a 30-50% Patients presenting with such a history have a 30-50%
chance of developing cancerchance of developing cancer
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – Physical ExamThyroid Nodule – Physical Exam Solitary, dominantSolitary, dominant Consistency, fixedConsistency, fixed Trachea, larynx shiftTrachea, larynx shift Lymph nodesLymph nodes Vocal cord motionVocal cord motion Retrosternal/Pemburton’s signRetrosternal/Pemburton’s sign
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – Degree of clinical Thyroid Nodule – Degree of clinical concern for carcinoma based on history concern for carcinoma based on history and physical examand physical exam Less concernLess concern
Stable examStable exam Evidence of functional disorderEvidence of functional disorder Multinodular gland without dominant noduleMultinodular gland without dominant nodule
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – Degree of clinical concern for Thyroid Nodule – Degree of clinical concern for carcinoma based on history and physical examcarcinoma based on history and physical exam More concernMore concern
Age <20 >60Age <20 >60 MalesMales Rapid growth, painRapid growth, pain History of radiation therapyHistory of radiation therapy Family history of thyroid carcinomaFamily history of thyroid carcinoma Hard fixed lesionHard fixed lesion LymphadenopathyLymphadenopathy Vocal cord paralysisVocal cord paralysis Size >4cmSize >4cm Aerodigestive tract compromise (e.g., stridor, dysphagia)Aerodigestive tract compromise (e.g., stridor, dysphagia) Cyst recurrence after aspirationCyst recurrence after aspiration
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – Lab Work upThyroid Nodule – Lab Work up Thyroid function testsThyroid function tests
TSH, T4, Total T3, resin uptake, T4 index, T7TSH, T4, Total T3, resin uptake, T4 index, T7 Hashimoto’s: TPOHashimoto’s: TPO Malignancy: No effective markersMalignancy: No effective markers
ThyroglobulinThyroglobulin Extensive overlap benign vs. malignantExtensive overlap benign vs. malignant Hampered by anti-thyroglobulin autoantibodiesHampered by anti-thyroglobulin autoantibodies Useful in long-term follow-up in patients with Useful in long-term follow-up in patients with
thyroid carcinomathyroid carcinoma
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – Hashimoto’s ThyroiditisThyroid Nodule – Hashimoto’s Thyroiditis Can present with small, firm thyroid lobes which can Can present with small, firm thyroid lobes which can
be mistaken for thyroid nodules on exambe mistaken for thyroid nodules on exam Common cause of hypothyroidism in femalesCommon cause of hypothyroidism in females Development of progressively enlarging mass within Development of progressively enlarging mass within
Hashimoto’s should trigger concern for lymphomaHashimoto’s should trigger concern for lymphoma FNA can give false positive findings (microfollicles, FNA can give false positive findings (microfollicles,
Hurthle cells, lymphocytes) Hurthle cells, lymphocytes)

Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – Toxic NoduleThyroid Nodule – Toxic Nodule Decreased TSH (rationale for checking TSH Decreased TSH (rationale for checking TSH
prior to FNA)prior to FNA) Very low incidence of malignancyVery low incidence of malignancy High risk of microfollicle false positive FNAHigh risk of microfollicle false positive FNA
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – Multinodular GoiterThyroid Nodule – Multinodular Goiter Dominant nodule is considered as a solitary Dominant nodule is considered as a solitary
nodule in terms of malignancy risknodule in terms of malignancy risk

Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – Radiographic Work upThyroid Nodule – Radiographic Work up CXR – tracheal deviation, substernal extension, CXR – tracheal deviation, substernal extension,
metastasismetastasis CT – impact on adjacent cervical viscera, CT – impact on adjacent cervical viscera,
retrosternal extension, adenopathy (cervical or retrosternal extension, adenopathy (cervical or mediastinal), tracheal invasion; caution with use of mediastinal), tracheal invasion; caution with use of iodine in multinodular goiter where patient may be iodine in multinodular goiter where patient may be subclinically hyperthyroidsubclinically hyperthyroid
MR – Retrosternal mediastinal vascular relationshipMR – Retrosternal mediastinal vascular relationship
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – IThyroid Nodule – I123123 Scan Scan 95% cold: cold solid nodule, cyst, focal thyroiditis; 95% cold: cold solid nodule, cyst, focal thyroiditis;
only 10-15% malignantonly 10-15% malignant 5% hot: <4% hot nodules are malignant5% hot: <4% hot nodules are malignant
When to scan:When to scan: Identification of a functional solitary thyroid nodule when Identification of a functional solitary thyroid nodule when
TSH is decreasedTSH is decreased If an FNA is reported as a follicular neoplasm or If an FNA is reported as a follicular neoplasm or
suspicious, the finding of a “hot” nodule may decrease the suspicious, the finding of a “hot” nodule may decrease the suspicion of a cancersuspicion of a cancer
Detecting neck metastasisDetecting neck metastasis
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – SonographyThyroid Nodule – Sonography Does not distinguish between benign vs. malignantDoes not distinguish between benign vs. malignant Provides a sensitive and objective measure of nodule size Provides a sensitive and objective measure of nodule size
prior to FNA, surgery, suppressionprior to FNA, surgery, suppression Provides clear-cut baselineProvides clear-cut baseline Finds contralateral nodules, lymph nodes which can be helpful Finds contralateral nodules, lymph nodes which can be helpful
at surgeryat surgery Nonpalpable or difficult to palpate nodules for US-guided FNANonpalpable or difficult to palpate nodules for US-guided FNA Follow-up imaging for solitary nodules that are managed Follow-up imaging for solitary nodules that are managed
medically or by observationmedically or by observation Nondiagnostic fine needle aspirate (as an adjunct to repeat Nondiagnostic fine needle aspirate (as an adjunct to repeat
FNA)FNA)
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – SonographyThyroid Nodule – Sonography Studies show Studies show
70% of nodules are solid 70% of nodules are solid 20% are malignant 20% are malignant 19% are cystic 19% are cystic 7% are malignant 7% are malignant 11% are mixed 11% are mixed 12% are malignant 12% are malignant
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – SonographyThyroid Nodule – Sonography US features suggesting malignancyUS features suggesting malignancy
Absent “halo” signAbsent “halo” sign Solid or hypoechogenicitySolid or hypoechogenicity Heterogeneous echo structureHeterogeneous echo structure Irregular marginIrregular margin Fine calcificationsFine calcifications Extraglandular extensionExtraglandular extension
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule – Fine Needle Aspiration (FNA)Thyroid Nodule – Fine Needle Aspiration (FNA) All palpable lesions of the thyroid require FNAAll palpable lesions of the thyroid require FNA
Decreased the percent of patients brought to Decreased the percent of patients brought to surgery by 20-50%surgery by 20-50%
Increased the percent of carcinoma found in surgical Increased the percent of carcinoma found in surgical specimens by 10-15%specimens by 10-15%
Overall decreases cost of care by 25%Overall decreases cost of care by 25%

Endocrine - ThyroidEndocrine - Thyroid
FNAFNA
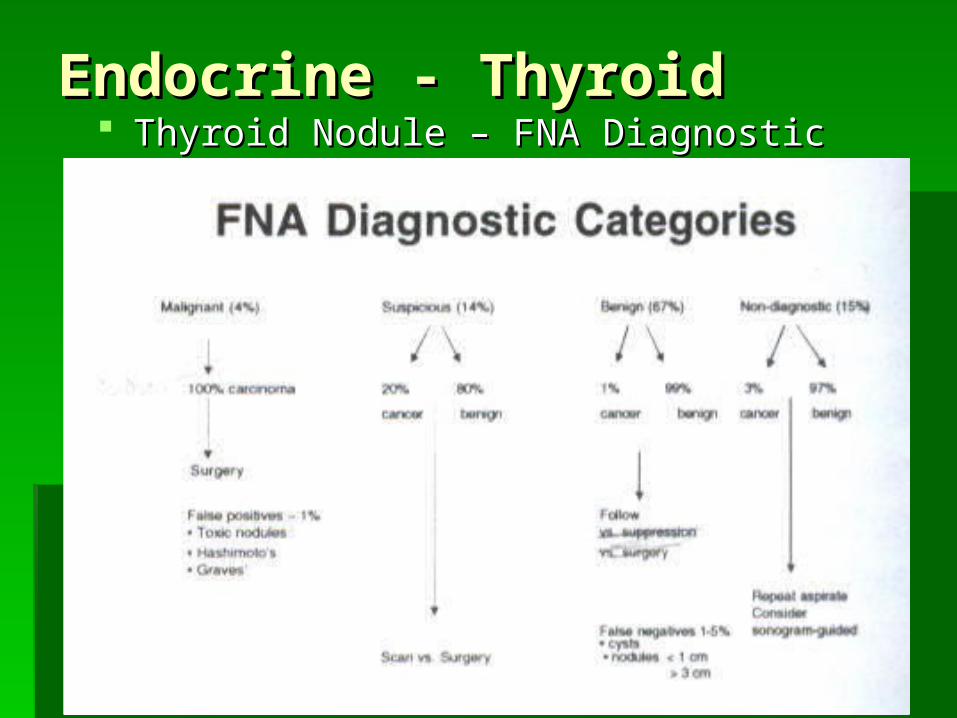
Endocrine - ThyroidEndocrine - Thyroid Thyroid Nodule – FNA Diagnostic CategoriesThyroid Nodule – FNA Diagnostic Categories
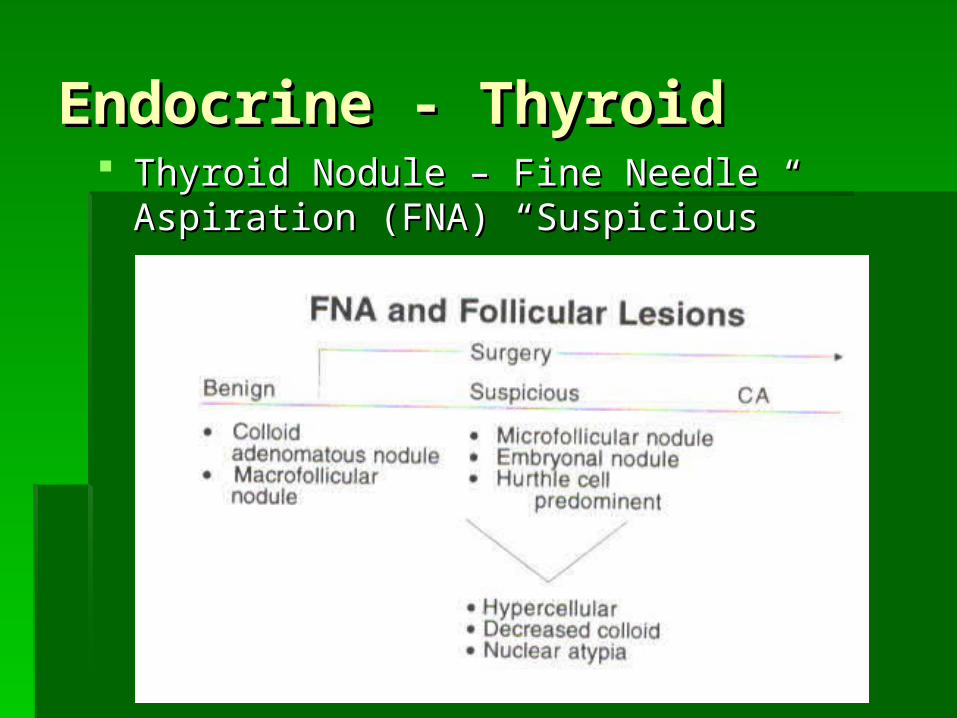
Endocrine - ThyroidEndocrine - Thyroid Thyroid Nodule – Fine Needle Aspiration (FNA) Thyroid Nodule – Fine Needle Aspiration (FNA)
“Suspicious”“Suspicious”
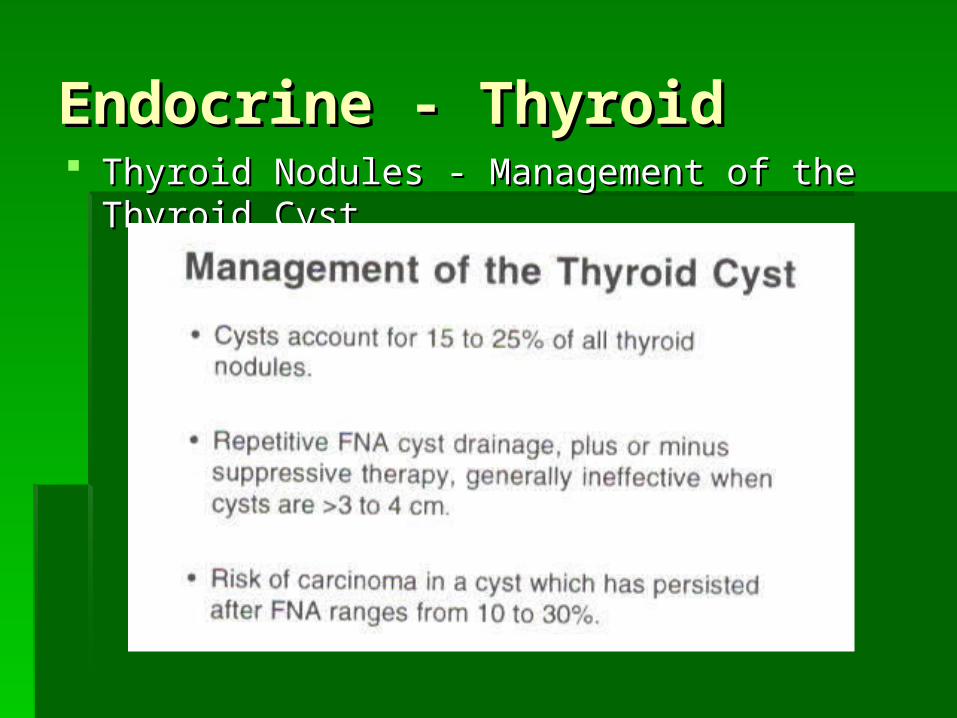
Endocrine - ThyroidEndocrine - Thyroid Thyroid Nodules - Management of the Thyroid CystThyroid Nodules - Management of the Thyroid Cyst

Endocrine - ThyroidEndocrine - Thyroid
Thyroid Nodule SuppressionThyroid Nodule Suppression Exogenous T4 suppresses TSH and withdraws Exogenous T4 suppresses TSH and withdraws
stimulatory influence on the thyroid and nodules stimulatory influence on the thyroid and nodules within itwithin it
Goal and length of treatment are unclearGoal and length of treatment are unclear Controversy regarding whether suppressive therapy Controversy regarding whether suppressive therapy
is superior to placebois superior to placebo RisksRisks
Suppressive therapy promotes osteoporosis and in an Suppressive therapy promotes osteoporosis and in an elderly population increases atrial fibrillationelderly population increases atrial fibrillation
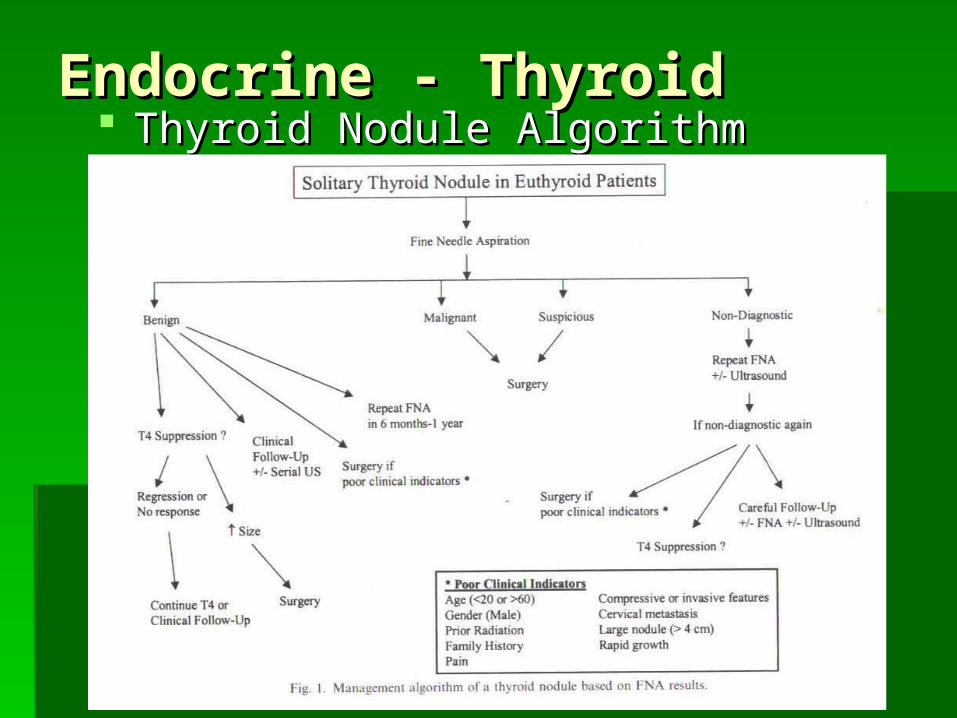
Endocrine - ThyroidEndocrine - Thyroid Thyroid Nodule AlgorithmThyroid Nodule Algorithm
Endocrine - ThyroidEndocrine - Thyroid
Nontoxic GoiterNontoxic Goiter Goiter is defined as any benign enlargement Goiter is defined as any benign enlargement
of the thyroid glandof the thyroid gland Iodine deficiency is most common cause Iodine deficiency is most common cause
(endemic goiter)(endemic goiter) In response to iodine deficiency In response to iodine deficiency increase TSH increase TSH Epithelial hyperplagia of thyroid gland followed by focal Epithelial hyperplagia of thyroid gland followed by focal
nodular hyperplagianodular hyperplagia Can grow extremely largeCan grow extremely large
In US, most goiters are nonendemicIn US, most goiters are nonendemic 3-4% of US population3-4% of US population Cause unknownCause unknown

Endocrine - ThyroidEndocrine - Thyroid
Nontoxic Goiter – Indications for SurgeryNontoxic Goiter – Indications for Surgery Symptoms of airway, esophageal, or superior vena Symptoms of airway, esophageal, or superior vena
caval obstructioncaval obstruction Thyroid enlargement despite nonoperative treatmentThyroid enlargement despite nonoperative treatment FNA biopsy positive or suspicious for malignancyFNA biopsy positive or suspicious for malignancy Radiologic finding of tracheal deviation or Radiologic finding of tracheal deviation or
compressioncompression Susternal goiterSusternal goiter Cosmetic deformity/patient preferenceCosmetic deformity/patient preference

Endocrine - ThyroidEndocrine - Thyroid
Nontoxic Goiter – Surgery: ControversyNontoxic Goiter – Surgery: Controversy Patients with unilateral thyroid enlargement Patients with unilateral thyroid enlargement
lobectomy and isthmusectomylobectomy and isthmusectomy Patients with diffuse or multinodule goiterPatients with diffuse or multinodule goiter
Total on one side and subtotal on the otherTotal on one side and subtotal on the other TotalTotal Bilateral subtotalBilateral subtotal
High recurrence rate (up to 25%)High recurrence rate (up to 25%) Need for reoperationNeed for reoperation
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – StatisticsThyroid Cancer – Statistics 1.5% of all cancers in the US 1.5% of all cancers in the US Most common endocrine malignancy (95% Most common endocrine malignancy (95%
of all endocrine cancers)of all endocrine cancers) Approx. 22,000 new cases each yearApprox. 22,000 new cases each year 74% occur in women74% occur in women
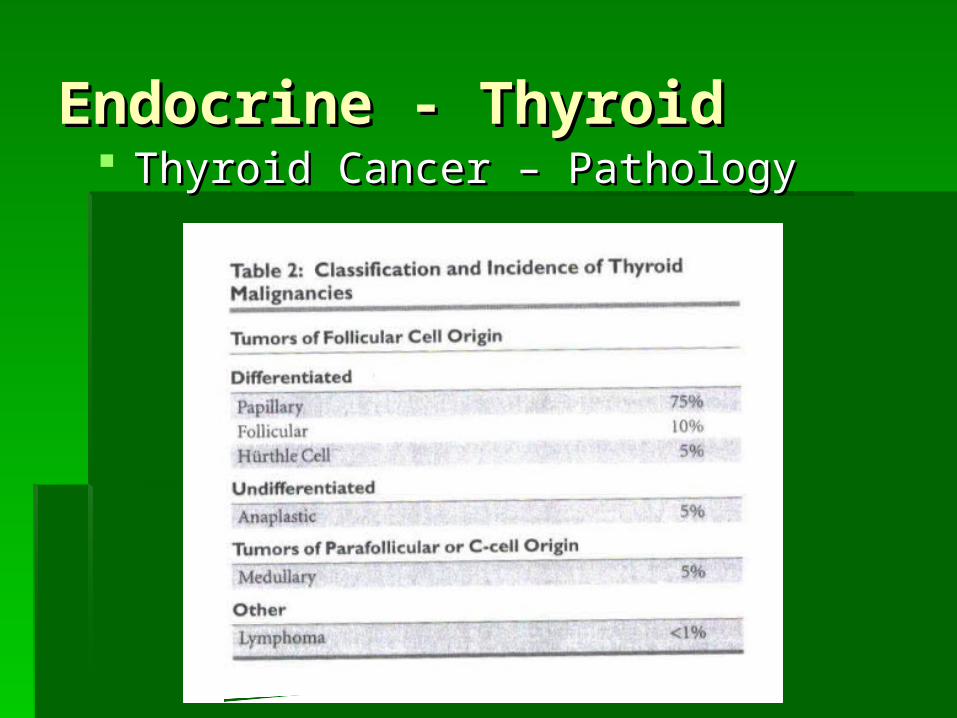
Endocrine - ThyroidEndocrine - Thyroid Thyroid Cancer – PathologyThyroid Cancer – Pathology
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – Papillary CarcinomaThyroid Cancer – Papillary Carcinoma 75-80% of all thyroid cancers75-80% of all thyroid cancers Consists of pure papillary, follicular, tall cell*, Consists of pure papillary, follicular, tall cell*,
columnar cell*, oxyphilic*, diffuse sclerosing, and columnar cell*, oxyphilic*, diffuse sclerosing, and encapsulated variantsencapsulated variants
Accounts for 90% of radiation-induced thyroid ca.Accounts for 90% of radiation-induced thyroid ca. Familial in 3% of patients (Cowden’s syndrome and Familial in 3% of patients (Cowden’s syndrome and
Gardner’s syndrome)Gardner’s syndrome)
* Aggressive forms of papillary carcinoma* Aggressive forms of papillary carcinoma
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – Papillary CarcinomaThyroid Cancer – Papillary Carcinoma Histological featuresHistological features
Psammoma bodiesPsammoma bodies Intranuclear groovesIntranuclear grooves Cytoplasmic inclusionsCytoplasmic inclusions
Multicentric in 30-50% of tumorsMulticentric in 30-50% of tumors Spreads via lymphaticsSpreads via lymphatics Cervical metastasis is not uncommon on initial Cervical metastasis is not uncommon on initial
presentation (in one study, microscopic mets presentation (in one study, microscopic mets present in 90% of elective neck dissection present in 90% of elective neck dissection specimens)specimens)
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – Papillary CarcinomaThyroid Cancer – Papillary Carcinoma TreatmentTreatment
Papillary carcinoma <1cm in size “microcarcinoma” Papillary carcinoma <1cm in size “microcarcinoma” lobectomy and isthmusectomylobectomy and isthmusectomy
Papillary carcinoma >1cm in low-risk group Papillary carcinoma >1cm in low-risk group lobectomy lobectomy and isthmusectomy (low-risk have recurrence rate of 5-and isthmusectomy (low-risk have recurrence rate of 5-11%; mortality rate .07-5%)11%; mortality rate .07-5%)
Papillary carcinoma >1cm in high-risk group Papillary carcinoma >1cm in high-risk group total total thyroidectomy (high-risk have recurrence rate of 48%; thyroidectomy (high-risk have recurrence rate of 48%; mortality rate 48%)mortality rate 48%)
Patients with history of head and neck irradiation Patients with history of head and neck irradiation total total thyroidectomy (high incidence of ca. at sites other than thyroidectomy (high incidence of ca. at sites other than nodule and increased lifetime risk of developing thyroid nodule and increased lifetime risk of developing thyroid carcinoma)carcinoma)
Endocrine - ThyroidEndocrine - Thyroid
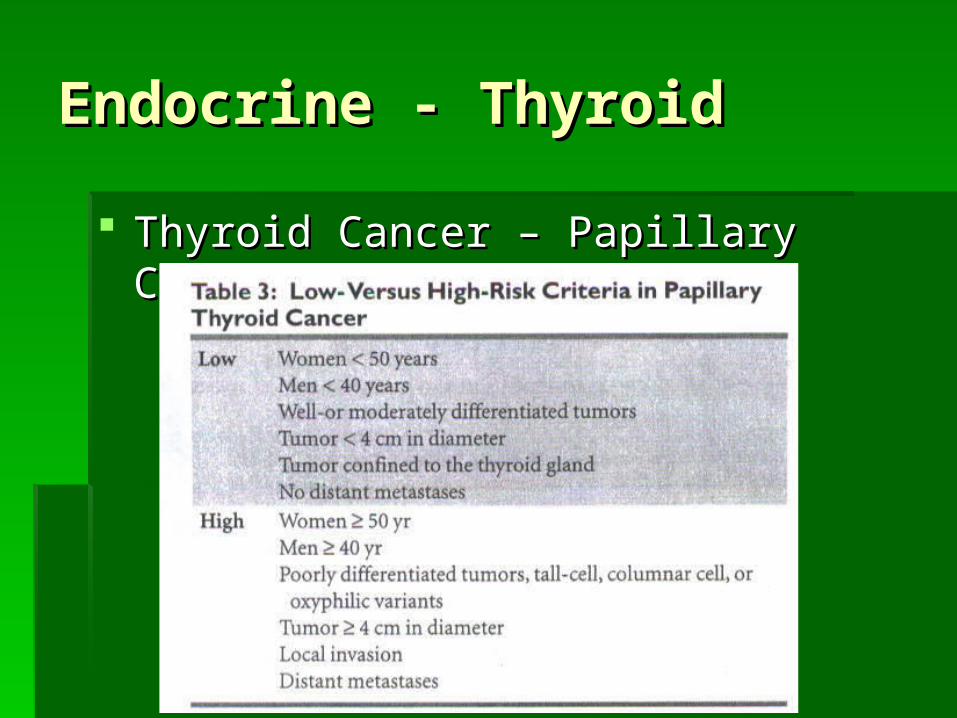
Thyroid Cancer – Papillary CarcinomaThyroid Cancer – Papillary Carcinoma
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – Papillary CarcinomaThyroid Cancer – Papillary Carcinoma TreatmentTreatment
Total thyroidectomy – AdvantagesTotal thyroidectomy – Advantages Associated with lowest incidence of local and regional Associated with lowest incidence of local and regional
occurrenceoccurrence When combined with post-op When combined with post-op 131131I ablation there is improved I ablation there is improved
survivalsurvival Allows use of serum thyroglobulin (Tg) and radioiodine for Allows use of serum thyroglobulin (Tg) and radioiodine for
early detection and treatment of metastatic diseaseearly detection and treatment of metastatic disease Avoids possible future re-op surgeryAvoids possible future re-op surgery
Total thyroidectomy – DisadvantagesTotal thyroidectomy – Disadvantages Injury to recurrent laryngeal nerves and parathyroid glandsInjury to recurrent laryngeal nerves and parathyroid glands
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – Papillary CarcinomaThyroid Cancer – Papillary Carcinoma TreatmentTreatment
Lymph nodesLymph nodes Prophylactic lymph node dissection not warrantedProphylactic lymph node dissection not warranted Enlarged lymph nodes in central and lateral neck Enlarged lymph nodes in central and lateral neck
should be removed and submitted for frozen sectionshould be removed and submitted for frozen section If FS+ in central neck If FS+ in central neck central neck dissection central neck dissection
performedperformed If FS+ in lateral neck If FS+ in lateral neck modified radical neck modified radical neck
dissection (functional neck) performeddissection (functional neck) performed
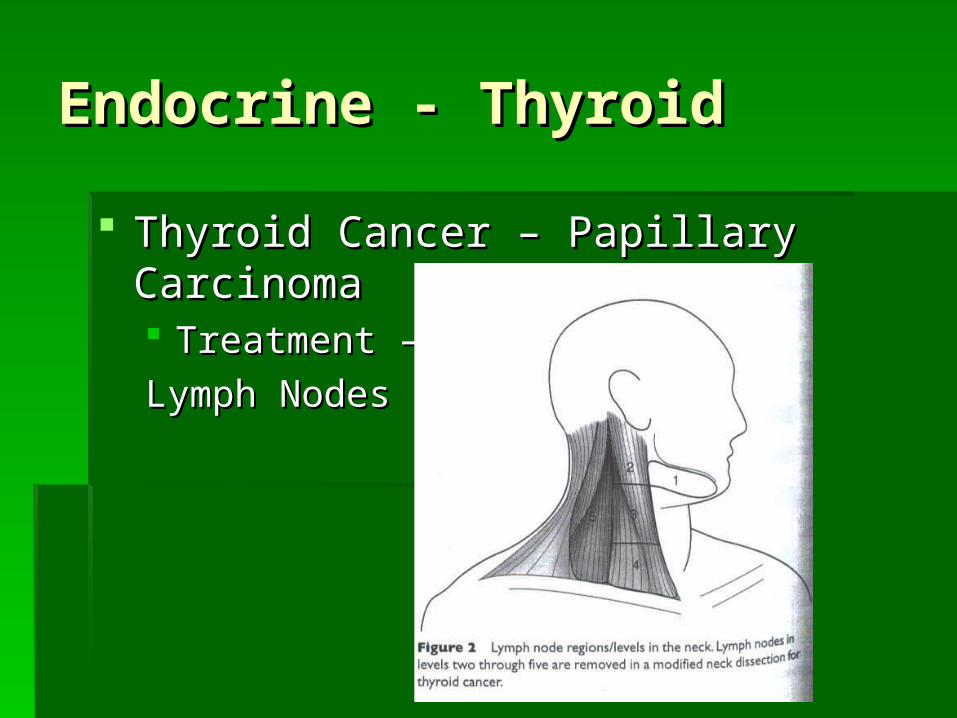
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – Papillary CarcinomaThyroid Cancer – Papillary Carcinoma Treatment – Treatment –
Lymph NodesLymph Nodes
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – Follicular CarcinomaThyroid Cancer – Follicular Carcinoma 10% of all thyroid cancers10% of all thyroid cancers Spreads hematogenously (lungs and bones)Spreads hematogenously (lungs and bones) Only 10% spread to cervical lymph nodesOnly 10% spread to cervical lymph nodes FNA cannot distinguish benign from malignant follicular FNA cannot distinguish benign from malignant follicular
neoplasm (capsule or vascular invasion are determining neoplasm (capsule or vascular invasion are determining factors)factors)
FNA report “consistent with follicular neoplasm” has 20% FNA report “consistent with follicular neoplasm” has 20% chance of malignancychance of malignancy These patients should undergo lobectomy and isthmusectomyThese patients should undergo lobectomy and isthmusectomy If permanent section is positive for carcinoma, then completion If permanent section is positive for carcinoma, then completion
thyroidectomy is donethyroidectomy is done
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – Hurthle Cell CarcinomaThyroid Cancer – Hurthle Cell Carcinoma 5% of thyroid cancers5% of thyroid cancers Similar to follicular carcinoma but more Similar to follicular carcinoma but more
aggressive tumoraggressive tumor 10-year survival 30%10-year survival 30%

Endocrine - ThyroidEndocrine - Thyroid
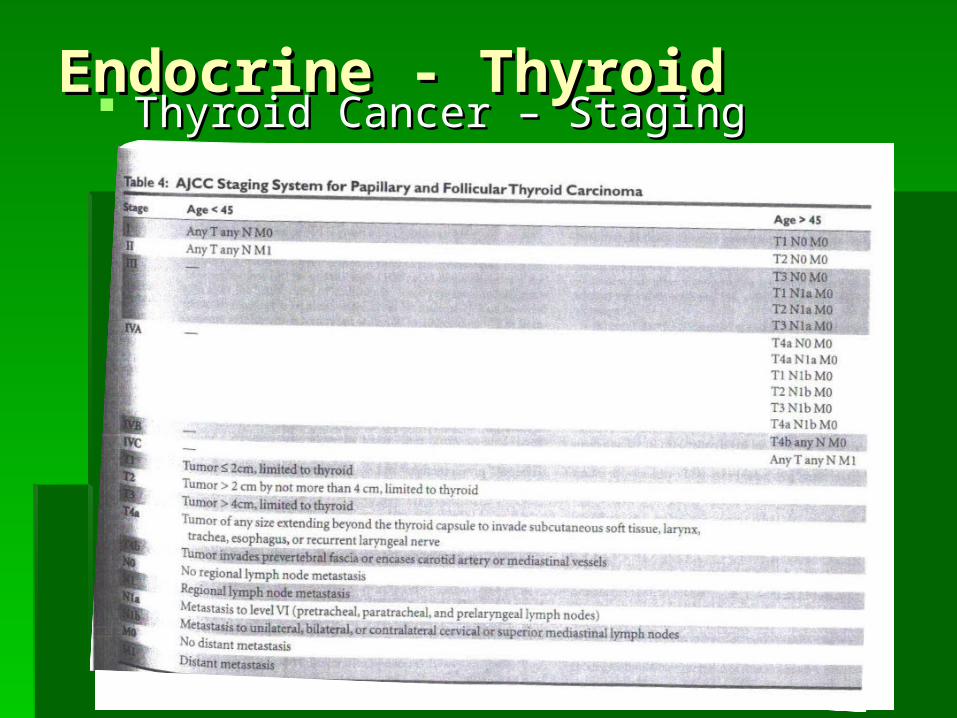
Thyroid Cancer – StagingThyroid Cancer – Staging Papillary and Follicular carcinoma are Papillary and Follicular carcinoma are
considered well-differentiated thyroid tumorsconsidered well-differentiated thyroid tumors Both Papillary and Follicular ca have good Both Papillary and Follicular ca have good
prognosesprognoses 20-year survival rates are 90% and 70% 20-year survival rates are 90% and 70%
respectivelyrespectively Most important prognostic factor is ageMost important prognostic factor is age
Endocrine - ThyroidEndocrine - Thyroid Thyroid Cancer – StagingThyroid Cancer – Staging

Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – Post-op Treatment of Well-Thyroid Cancer – Post-op Treatment of Well-Differentiated Thyroid CarcinomaDifferentiated Thyroid Carcinoma Thyroid remnant ablation destroys residual thyroid tissue after Thyroid remnant ablation destroys residual thyroid tissue after
surgery using surgery using 131131II Destroys microscopic diseaseDestroys microscopic disease Allows for detection of recurrent disease by radioiodine scanningAllows for detection of recurrent disease by radioiodine scanning Allows for improved sensitivity of serum thyroglobulin (Tg) Allows for improved sensitivity of serum thyroglobulin (Tg)
measurements during follow-upmeasurements during follow-up Used for:Used for:
Papillary ca. >1.5cmPapillary ca. >1.5cm Papillary ca. with metsPapillary ca. with mets Invasive follicular or Hurthle Cell ca.Invasive follicular or Hurthle Cell ca.
Patient should be off thyroid hormone for weeks (or T3 for 2 Patient should be off thyroid hormone for weeks (or T3 for 2 weeks) to allow for maximal TSH levelsweeks) to allow for maximal TSH levels
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – Post-op Treatment of Thyroid Cancer – Post-op Treatment of Well-Differentiated Thyroid CarcinomaWell-Differentiated Thyroid Carcinoma Thyroid hormone given post-ablation to Thyroid hormone given post-ablation to
suppress TSH (TSH stimulates tumor suppress TSH (TSH stimulates tumor growth, invasion, angiogenesis, Tg growth, invasion, angiogenesis, Tg secretion)secretion)
Long-term follow-up using serum Tg and Long-term follow-up using serum Tg and 131131I I whole-body scanswhole-body scans
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – Medullary Carcinoma (MTC)Thyroid Cancer – Medullary Carcinoma (MTC) Parafollicular cells of neuroectoderm originParafollicular cells of neuroectoderm origin 5% of all thyroid cancers (75% sporadic; 25% hereditary)5% of all thyroid cancers (75% sporadic; 25% hereditary) FNA can be characteristic along with special staining for FNA can be characteristic along with special staining for
calcitonincalcitonin HereditaryHereditary
Part of multiple endocrine neoplasia syndromes type IIA and IIB Part of multiple endocrine neoplasia syndromes type IIA and IIB (IIA – hyperparathyroidism and pheochromocytoma, lichen planus (IIA – hyperparathyroidism and pheochromocytoma, lichen planus amyloidosis, Hirschprung’s disease; IIB – pheochromocytoma, amyloidosis, Hirschprung’s disease; IIB – pheochromocytoma, marfanoid body habitus, mucosal neuromas, ganglioneuromatosis marfanoid body habitus, mucosal neuromas, ganglioneuromatosis of the GI tract)of the GI tract)
RET proto-oncogene is currently primary factor implicated RET proto-oncogene is currently primary factor implicated This allows for screening, early detection and treatmentThis allows for screening, early detection and treatment

Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – Medullary Carcinoma (MTC)Thyroid Cancer – Medullary Carcinoma (MTC) TreatmentTreatment
Surgery is main modality of treatmentSurgery is main modality of treatment Total thyroidectomy with central neck dissectionTotal thyroidectomy with central neck dissection Modified radical neck dissection is performed for cervical Modified radical neck dissection is performed for cervical
lymph node metastasislymph node metastasis These tumors are not amenable to radioiodine therapy or These tumors are not amenable to radioiodine therapy or
other adjuvant therapyother adjuvant therapy
Post-treatmentPost-treatment Monitor serum calcitonin levelsMonitor serum calcitonin levels
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – Anaplastic CancerThyroid Cancer – Anaplastic Cancer A most aggressive cancerA most aggressive cancer Overall 5-year survival; 3.6% with median survival of Overall 5-year survival; 3.6% with median survival of
4 months4 months No adequate therapy known; complete surgical No adequate therapy known; complete surgical
resection is difficult because of tumor size, extra resection is difficult because of tumor size, extra thyroid growth and invasion into surrounding thyroid growth and invasion into surrounding tissues. Besides attempted resection, surgery may tissues. Besides attempted resection, surgery may be indicated for airway management (e.g., be indicated for airway management (e.g., tracheotomy)tracheotomy)
Surgery, radiation therapy, chemotherapy combined Surgery, radiation therapy, chemotherapy combined may improve local controlmay improve local control
Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – LymphomaThyroid Cancer – Lymphoma Less than 1% of thyroid cancersLess than 1% of thyroid cancers Usually non-Hodgkin’s B-cell typeUsually non-Hodgkin’s B-cell type Associated with Hashimoto’s thyroiditisAssociated with Hashimoto’s thyroiditis Usually in older womenUsually in older women Presents as rapidly enlarging painless neck massPresents as rapidly enlarging painless neck mass FNA 80% accurate FNA 80% accurate Occasional biopsy is necessary for tissue diagnosisOccasional biopsy is necessary for tissue diagnosis 50-70% 5-year survival50-70% 5-year survival

Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – Surgery: ComplicationsThyroid Cancer – Surgery: Complications 2 primary potential complications that must be considered in 2 primary potential complications that must be considered in
performing thyroid surgery are RLN injury and performing thyroid surgery are RLN injury and hypoparathyroidismhypoparathyroidism
With total thyroidectomy, incidence of temporary With total thyroidectomy, incidence of temporary hypoparathyroidism ranges from 5-40%hypoparathyroidism ranges from 5-40%
With total thyroidectoy, the incidence of permanent With total thyroidectoy, the incidence of permanent hypoparathyroidism ranges from 1-5% in some studies to 8-hypoparathyroidism ranges from 1-5% in some studies to 8-32% in other studies32% in other studies
The rate of temporary RLN injury is 3-7%The rate of temporary RLN injury is 3-7% With total thyroidectomy the incidence of permanent RLN With total thyroidectomy the incidence of permanent RLN
injury is 0-3% per side in some studies, and up to 11% in other injury is 0-3% per side in some studies, and up to 11% in other studiesstudies
Lastly, injury to the superior laryngeal nerve can be a Lastly, injury to the superior laryngeal nerve can be a devastating complication to professional singersdevastating complication to professional singers

Endocrine - ThyroidEndocrine - Thyroid
Thyroid Cancer – Surgery: ComplicationsThyroid Cancer – Surgery: Complications Hypoparathyroidism (hypocalcemia)Hypoparathyroidism (hypocalcemia)
CircumoralparasthesiaCircumoralparasthesia Mental status changeMental status change Carpopedal spasmCarpopedal spasm SeizuresSeizures QT interval prolongationQT interval prolongation Cardiac arrestCardiac arrest Most common after total thyroidectomy but can occur in Most common after total thyroidectomy but can occur in
patients with hyperparathyroidism who undergo parathyroid patients with hyperparathyroidism who undergo parathyroid surgery, especially when the calcium is extremely elevated surgery, especially when the calcium is extremely elevated preoperatively, with significant bone disease (hungry bone preoperatively, with significant bone disease (hungry bone syndrome)syndrome)
Should be treated as a general rule when serum calcium Should be treated as a general rule when serum calcium falls below 7 and / or patient is symptomaticfalls below 7 and / or patient is symptomatic
Endocrine - ThyroidEndocrine - Thyroid
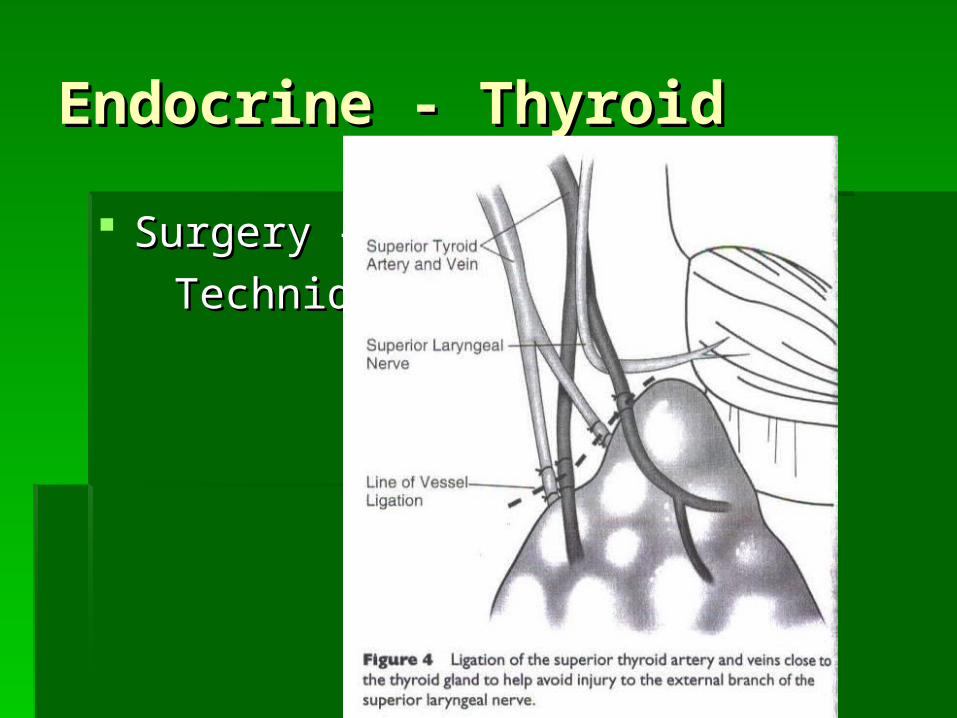
Surgery – Surgery –
Technique Technique
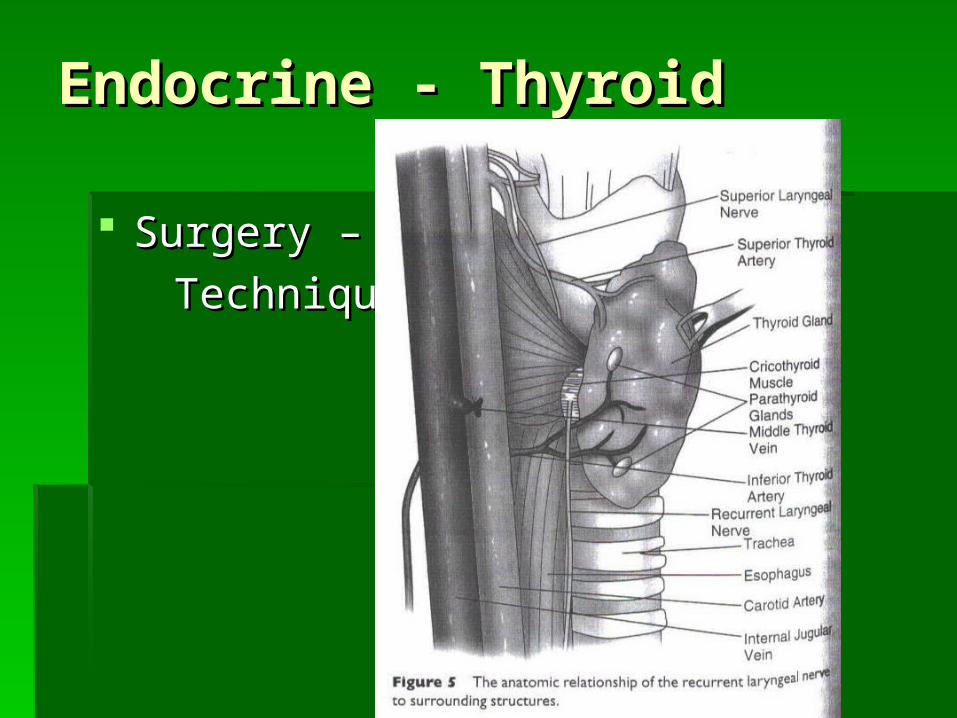
Endocrine - ThyroidEndocrine - Thyroid
Surgery – Surgery –
Technique Technique
Endocrine - ThyroidEndocrine - Thyroid
Surgery – Surgery –
Technique Technique

Endocrine – Parathyroid Endocrine – Parathyroid
-84% of adults have 4 parathyroids
-Autopsy results reveal 13% have greater than 4 and 3% have less than 4
-84% of adults have 4 parathyroids
-Autopsy results reveal 13% have greater than 4 and 3% have less than 4
Endocrine - ParathyroidEndocrine - Parathyroid
Endocrine - ParathyroidEndocrine - Parathyroid
Anatomy and EmbryologyAnatomy and Embryology Inferior glands are derived from the 3Inferior glands are derived from the 3 rdrd
branchial pouch and migrate caudally with branchial pouch and migrate caudally with the thymus. They then separate at the level the thymus. They then separate at the level of the inferior thyroid poleof the inferior thyroid pole
Superior glands are derived from the 4Superior glands are derived from the 4 thth branchial pouch and follow the migration of branchial pouch and follow the migration of the ultimobranchial bodies at the lateral part the ultimobranchial bodies at the lateral part of the thyroid anlageof the thyroid anlage
Endocrine - ParathyroidEndocrine - Parathyroid
Anatomy and EmbryologyAnatomy and Embryology The inferior glands vary more in their The inferior glands vary more in their
location than the superior glandslocation than the superior glands The superior glands are generally located The superior glands are generally located
superior to the inferior thyroid artery and superior to the inferior thyroid artery and posterior to the recurrent laryngeal nerve posterior to the recurrent laryngeal nerve (classically described as lying 1cm above (classically described as lying 1cm above the intersection of the RLN and inferior the intersection of the RLN and inferior thyroid arterythyroid artery
Endocrine - ParathyroidEndocrine - Parathyroid
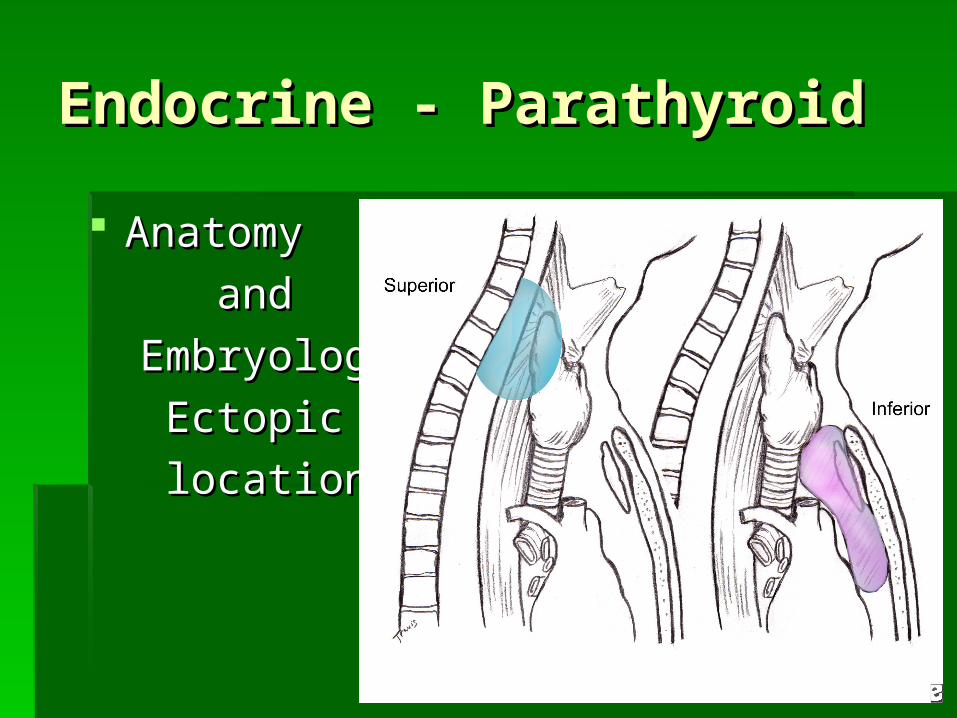
Anatomy and EmbryologyAnatomy and Embryology Common ectopic location for the superior gland Common ectopic location for the superior gland
includes paraesophageal or retroesophageal areas includes paraesophageal or retroesophageal areas (superior posterior mediastinum) and intrathyroid(superior posterior mediastinum) and intrathyroid
The inferior glands usually lie near the inferior pole The inferior glands usually lie near the inferior pole of the thyroid and are inferior to the inferior thyroid of the thyroid and are inferior to the inferior thyroid artery and anterior to the RLNartery and anterior to the RLN
The inferior glands are more variable in location. The inferior glands are more variable in location. Ectopic locations include in or around the thymus Ectopic locations include in or around the thymus (anterior mediastinum)(anterior mediastinum)
Endocrine - ParathyroidEndocrine - Parathyroid
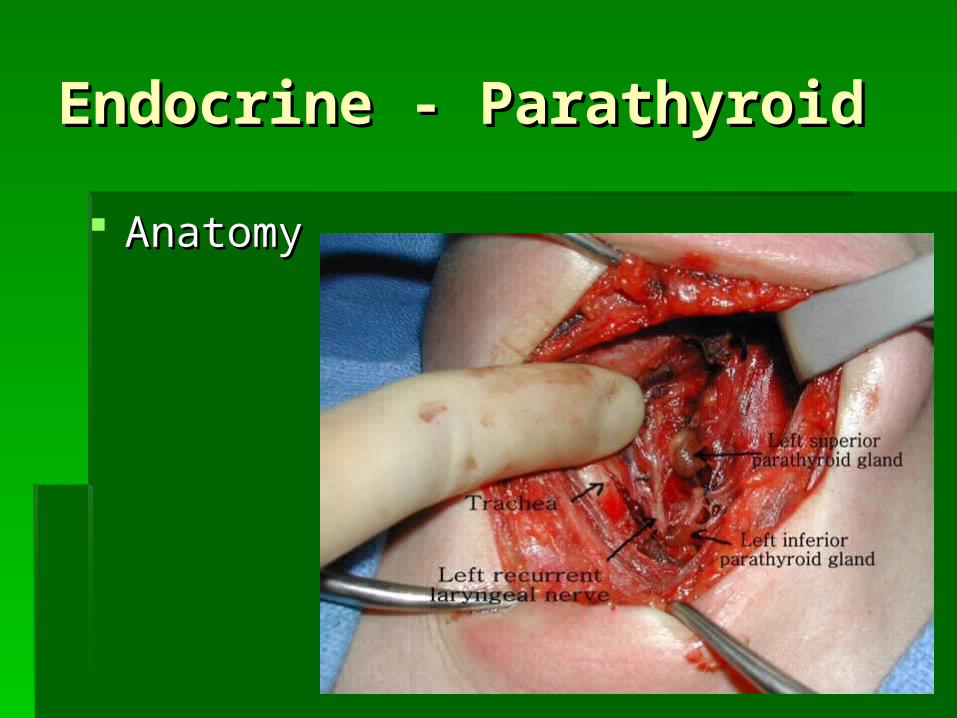
Anatomy Anatomy
and and
Embryology:Embryology:
EctopicEctopic
locationslocations
Endocrine - ParathyroidEndocrine - Parathyroid
Anatomy Anatomy Glands are usually oval, bean-shaped or oblongGlands are usually oval, bean-shaped or oblong Weigh 30-65mgWeigh 30-65mg Average 5x3x2mmAverage 5x3x2mm Light yellow to caramel colorLight yellow to caramel color Blood supply to the superior and inferior glands is Blood supply to the superior and inferior glands is
from the inferior thyroid artery in 86% of patients. In from the inferior thyroid artery in 86% of patients. In the remainder, both glands are supplied by the the remainder, both glands are supplied by the superior thyroid artery or by anastomotic arch from superior thyroid artery or by anastomotic arch from both vesselsboth vessels
Endocrine - ParathyroidEndocrine - Parathyroid
Anatomy Anatomy
Endocrine - ParathyroidEndocrine - Parathyroid
PhysiologyPhysiology Parathyroid hormone (PTH) is an 84-amino acid Parathyroid hormone (PTH) is an 84-amino acid
peptide with the biologic activity residing at its amino peptide with the biologic activity residing at its amino terminalterminal
PTH regulates serum calcium concentration and PTH regulates serum calcium concentration and bone metabolism (affects bone, kidney and intestine bone metabolism (affects bone, kidney and intestine particularly)particularly)
Serum calcium concentration in turn regulates PTH Serum calcium concentration in turn regulates PTH secretionsecretion
high calcium high calcium PTH secretion PTH secretion low calcium low calcium PTH secretion PTH secretion
Endocrine - ParathyroidEndocrine - Parathyroid
PhysiologyPhysiology PTHPTH
Increase in renal calcium absorptionIncrease in renal calcium absorption Increase in enzyme activity converting Vitamin D Increase in enzyme activity converting Vitamin D
to its active form and thereby increasing intestinal to its active form and thereby increasing intestinal absorption of calciumabsorption of calcium
Increases osteoclast activity which increases Increases osteoclast activity which increases bone resorption and bone remodelingbone resorption and bone remodeling
Decreased phosphorous excretion, mild Decreased phosphorous excretion, mild metabolic acidosis and decrease in GFR also metabolic acidosis and decrease in GFR also occuroccur
Endocrine - ParathyroidEndocrine - Parathyroid
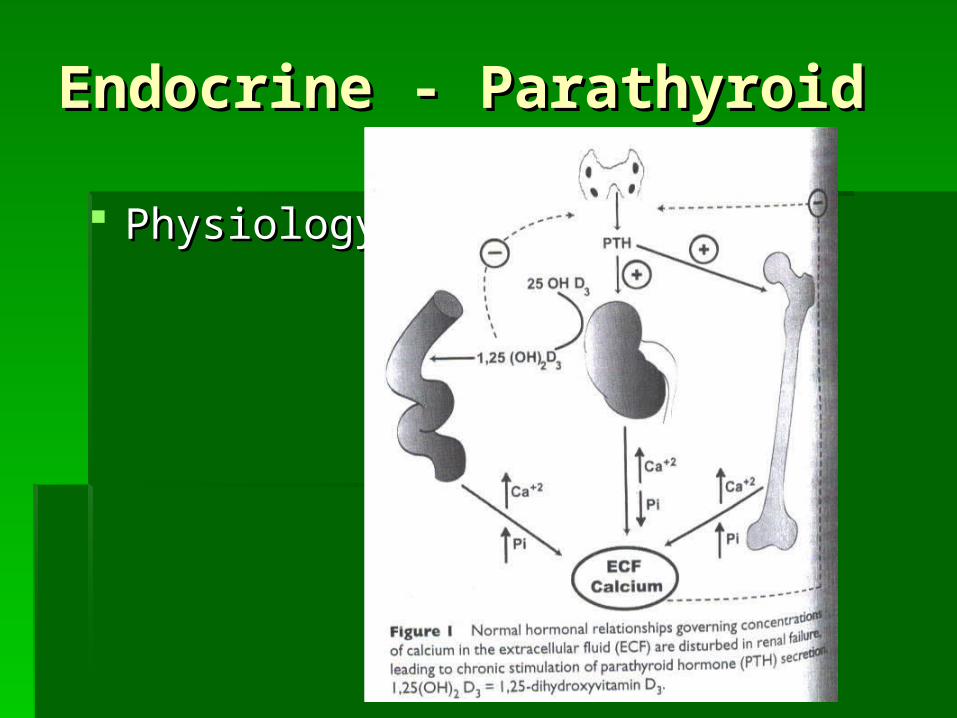
PhysiologyPhysiology
Endocrine - ParathyroidEndocrine - Parathyroid
Primary hyperparathyroidism (PHPT)Primary hyperparathyroidism (PHPT) Syndrome of inappropriate secretion of PTH by one Syndrome of inappropriate secretion of PTH by one
or more abnormal glandsor more abnormal glands Most cases are sporadic with female to male 4:1Most cases are sporadic with female to male 4:1 Familial syndrome are relatively rare and include: Familial syndrome are relatively rare and include:
MEN Types I and IIMEN Types I and II Familial isolated HPTFamilial isolated HPT Hereditary HPT jaw tumor syndromeHereditary HPT jaw tumor syndrome 85-90% are caused by a single adenoma85-90% are caused by a single adenoma Multiple gland disease either as multiple adenomas Multiple gland disease either as multiple adenomas
or hyperplasia of all 4 glands 10-15%or hyperplasia of all 4 glands 10-15% <1% parathyroid carcinoma<1% parathyroid carcinoma

Endocrine - ParathyroidEndocrine - Parathyroid
Parathyroid Adenoma – Right inferiorParathyroid Adenoma – Right inferior
Endocrine - ParathyroidEndocrine - Parathyroid
Primary hyperparathyroidism (PHPT)Primary hyperparathyroidism (PHPT) Classic presentation: “renal stones, painful bones, Classic presentation: “renal stones, painful bones,
abdominal groans, psychic moans and fatigue abdominal groans, psychic moans and fatigue overtones”overtones”
Severe symptoms which are uncommon include: Severe symptoms which are uncommon include: osteitis fibrosis cystica, osteoclastomas (Brown osteitis fibrosis cystica, osteoclastomas (Brown tumors) and nephrocalcinosistumors) and nephrocalcinosis
Most patients today are “asymptomatic” with Most patients today are “asymptomatic” with increased calcium found in routine blood testsincreased calcium found in routine blood tests
““Asymptomatic” patients may have subtle symptoms Asymptomatic” patients may have subtle symptoms such as neuropsych disorders, dyspepsia, such as neuropsych disorders, dyspepsia, constipation and high blood pressureconstipation and high blood pressure
Endocrine - ParathyroidEndocrine - Parathyroid
Primary hyperparathyroidism (PHPT)Primary hyperparathyroidism (PHPT) Diagnosis made by blood test of increased Diagnosis made by blood test of increased
calcium and increased circulating intact PTHcalcium and increased circulating intact PTH Other causes of hypercalcemia should be Other causes of hypercalcemia should be
ruled outruled out Familial hypocalciuric hypercalcemia (FHH) Familial hypocalciuric hypercalcemia (FHH)
Autosomal dominantAutosomal dominant <1% of patients with hypercalcemia<1% of patients with hypercalcemia PTH usually normal or slightly elevatedPTH usually normal or slightly elevated Urinary calcium secretion NOT usually elevated (in Urinary calcium secretion NOT usually elevated (in
contrast to PHPT) so the fasting urinary calcium to contrast to PHPT) so the fasting urinary calcium to creatnine ratio is less than 0.01creatnine ratio is less than 0.01

Endocrine - ParathyroidEndocrine - Parathyroid Differential diagnosis of hypercalcemiaDifferential diagnosis of hypercalcemia

Endocrine - ParathyroidEndocrine - Parathyroid
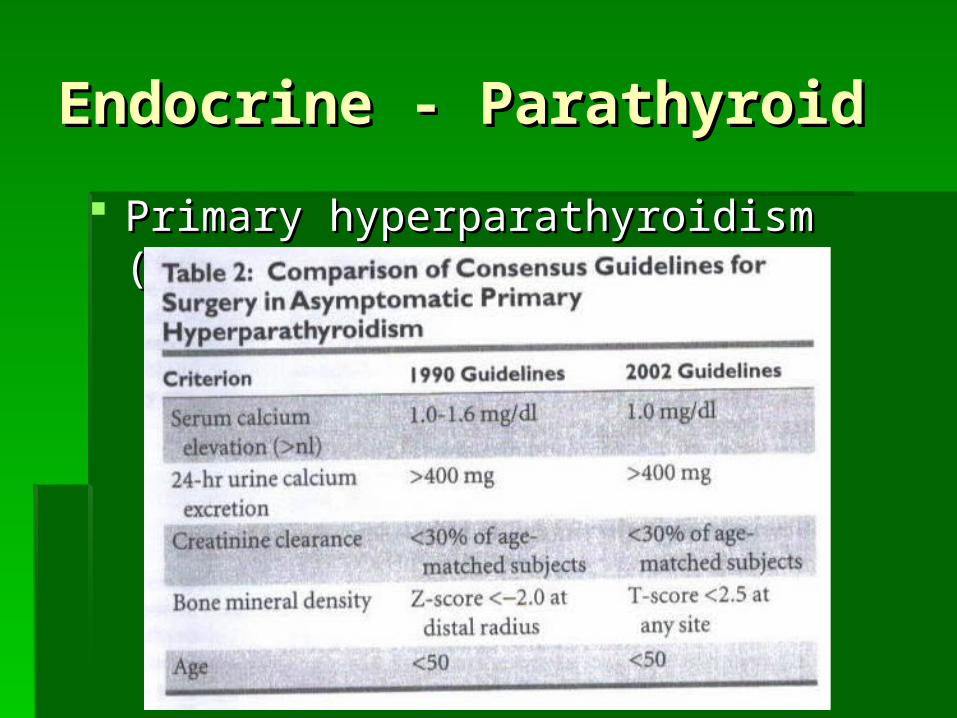
Primary hyperparathyroidism (PHPT)Primary hyperparathyroidism (PHPT) Indications for surgeryIndications for surgery
Virtually all patients with symptomatic PHPT and selected Virtually all patients with symptomatic PHPT and selected patients with asymptomatic PHPT should undergo surgerypatients with asymptomatic PHPT should undergo surgery
Guidelines have been liberalized over the years; that is, Guidelines have been liberalized over the years; that is, more people who are asymptomatic now come to surgery more people who are asymptomatic now come to surgery (in one study, 25% of asymptomatic patients develop some (in one study, 25% of asymptomatic patients develop some form of metabolic complication within 5 years of diagnosisform of metabolic complication within 5 years of diagnosis
Asymptomatic patients not meeting criteria for surgery Asymptomatic patients not meeting criteria for surgery should have serum calcium checked twice a year and bone should have serum calcium checked twice a year and bone densitometry and serum creatnine checked yearlydensitometry and serum creatnine checked yearly
Endocrine - ParathyroidEndocrine - Parathyroid
Primary hyperparathyroidism (PHPT)Primary hyperparathyroidism (PHPT)
Endocrine - ParathyroidEndocrine - Parathyroid
Primary hyperparathyroidism (PHPT)Primary hyperparathyroidism (PHPT) Conventional parathyroidectomyConventional parathyroidectomy
Bilateral neck exploration with identification of all Bilateral neck exploration with identification of all 4 glands4 glands
Removal of enlarged gland(s) (+ / - biopsy of Removal of enlarged gland(s) (+ / - biopsy of normal glands)normal glands)
95% success rate95% success rate This operation is indicated when localization This operation is indicated when localization
studies fail; when diagnosis of hyperplasia is studies fail; when diagnosis of hyperplasia is suspected; and for cases of secondary and suspected; and for cases of secondary and tertiary hyperparathyroidismtertiary hyperparathyroidism
Endocrine - ParathyroidEndocrine - Parathyroid
Primary hyperparathyroidism (PHPT)Primary hyperparathyroidism (PHPT) New approaches to surgeryNew approaches to surgery
Localization studiesLocalization studies Technetium-99 –labeled sestamibi Technetium-99 –labeled sestamibi
Absorbed and retained by parathyroid disease but Absorbed and retained by parathyroid disease but rapidly washed out from thyroidrapidly washed out from thyroid
Accuracy enhanced by combining it with single Accuracy enhanced by combining it with single photon emission CT (SPECT) photon emission CT (SPECT)
Picks up 85% of adenomasPicks up 85% of adenomas Sensitivity decreases with multiple gland diseaseSensitivity decreases with multiple gland disease
Endocrine - ParathyroidEndocrine - Parathyroid
Primary hyperparathyroidism (PHPT)Primary hyperparathyroidism (PHPT) New approaches to surgeryNew approaches to surgery
Localization studiesLocalization studies Cervical USG – 60-70% of abnormal glandsCervical USG – 60-70% of abnormal glands MRI / CT 75% sensitivity but usually reserved for MRI / CT 75% sensitivity but usually reserved for
reoperationreoperation
Endocrine - ParathyroidEndocrine - Parathyroid
Primary hyperparathyroidism (PHPT)Primary hyperparathyroidism (PHPT) New approaches to surgeryNew approaches to surgery
Directed parathyroidectomyDirected parathyroidectomy Makes use of localization studies to allow for unilateral Makes use of localization studies to allow for unilateral
neck dissection on the side of the positive localizationneck dissection on the side of the positive localization Methylene blue, when used preoperatively, can Methylene blue, when used preoperatively, can
enhance success of localization intraoperatively. enhance success of localization intraoperatively. Abnormal tissue turns dark blue in colorAbnormal tissue turns dark blue in color
Endocrine - ParathyroidEndocrine - Parathyroid
Primary hyperparathyroidism (PHPT)Primary hyperparathyroidism (PHPT) New approaches to surgeryNew approaches to surgery
Directed parathyroidectomyDirected parathyroidectomy Intraoperative PTH monitoring Intraoperative PTH monitoring
iPTH has short half-lifeiPTH has short half-life Serial measurement of serum iPTH before, during Serial measurement of serum iPTH before, during
and at 5 and 10 minutes after removal of enlarged and at 5 and 10 minutes after removal of enlarged gland will show fall in iPTHgland will show fall in iPTH
Reduction in iPTH greater than of equal to 50% of Reduction in iPTH greater than of equal to 50% of pre-surgery level indicates successpre-surgery level indicates success
Absolute level of iPTH should fall to normalAbsolute level of iPTH should fall to normal Success exceeds 90%Success exceeds 90%
Endocrine - ParathyroidEndocrine - Parathyroid
Primary hyperparathyroidism (PHPT)Primary hyperparathyroidism (PHPT) New approaches to surgeryNew approaches to surgery
Directed parathyroidectomyDirected parathyroidectomy Radioguided parathyroidectomyRadioguided parathyroidectomy
Employs injection of 99-Tc sestamibi immediately Employs injection of 99-Tc sestamibi immediately before ORbefore OR
Using gamma probe to detect area of greatest Using gamma probe to detect area of greatest radioactivityradioactivity
Can combine techniquesCan combine techniques Minimally invasive parathyroidectomy – requires Minimally invasive parathyroidectomy – requires
proper localization studiesproper localization studies Open minimal access parathyroidectomyOpen minimal access parathyroidectomy Endoscopic parathyroidectomyEndoscopic parathyroidectomy

Endocrine - ParathyroidEndocrine - Parathyroid
Primary hyperparathyroidism (PHPT)Primary hyperparathyroidism (PHPT) ResultsResults
Parathyroidectomy is curative in 95% of cases of Parathyroidectomy is curative in 95% of cases of PHPTPHPT
Persistent PHPT usually results from a missed Persistent PHPT usually results from a missed adenomaadenoma
Recurrent PHPT (occurs 6 months or more post-Recurrent PHPT (occurs 6 months or more post-op) may develop 5-10% of time, probably due to op) may develop 5-10% of time, probably due to a second adenoma or hyperplasia of remaining a second adenoma or hyperplasia of remaining glandsglands
Endocrine - ParathyroidEndocrine - Parathyroid
Primary hyperparathyroidism (PHPT)Primary hyperparathyroidism (PHPT) ComplicationsComplications
Temporary hypocalcemia (20-30%)Temporary hypocalcemia (20-30%) Cervical hematoma (less than 1%)Cervical hematoma (less than 1%) Recurrent nerve palsy (1-2%)Recurrent nerve palsy (1-2%) Recurrent nerve injury (less than 1%)Recurrent nerve injury (less than 1%)
Endocrine - ParathyroidEndocrine - Parathyroid
Primary hyperparathyroidism (PHPT)Primary hyperparathyroidism (PHPT) Parathyroid hyperplasiaParathyroid hyperplasia
Consider this diagnosis when localization studies are not Consider this diagnosis when localization studies are not helpfulhelpful
15% of all PHPT 15% of all PHPT Diagnosis in 37% of patients undergoing re-opDiagnosis in 37% of patients undergoing re-op Pathology found in secondary and tertiary Pathology found in secondary and tertiary
hyperparathyroidism and MEN syndromeshyperparathyroidism and MEN syndromes Requires bilateral neck explorationRequires bilateral neck exploration In PHPT – perform either 3 ½ gland resection making sure In PHPT – perform either 3 ½ gland resection making sure
remnant left is viable and marking remnant with vascular remnant left is viable and marking remnant with vascular clip in case of need for re-exploration or total clip in case of need for re-exploration or total parathyroidectomy with autotransplantationparathyroidectomy with autotransplantation
Endocrine - ParathyroidEndocrine - Parathyroid
Secondary and Tertiary HyperparathyroidismSecondary and Tertiary Hyperparathyroidism Secondary hyperparathyroidismSecondary hyperparathyroidism
Result of chronic overstimulation leading to hyper Result of chronic overstimulation leading to hyper secretion and hyperplasia of normal parathyroid secretion and hyperplasia of normal parathyroid glands, i.e., chronic hypocalcemic stimulationglands, i.e., chronic hypocalcemic stimulation
Seen most commonly in chronic renal failureSeen most commonly in chronic renal failure Surgery is associated with end-stage renal failure, Surgery is associated with end-stage renal failure,
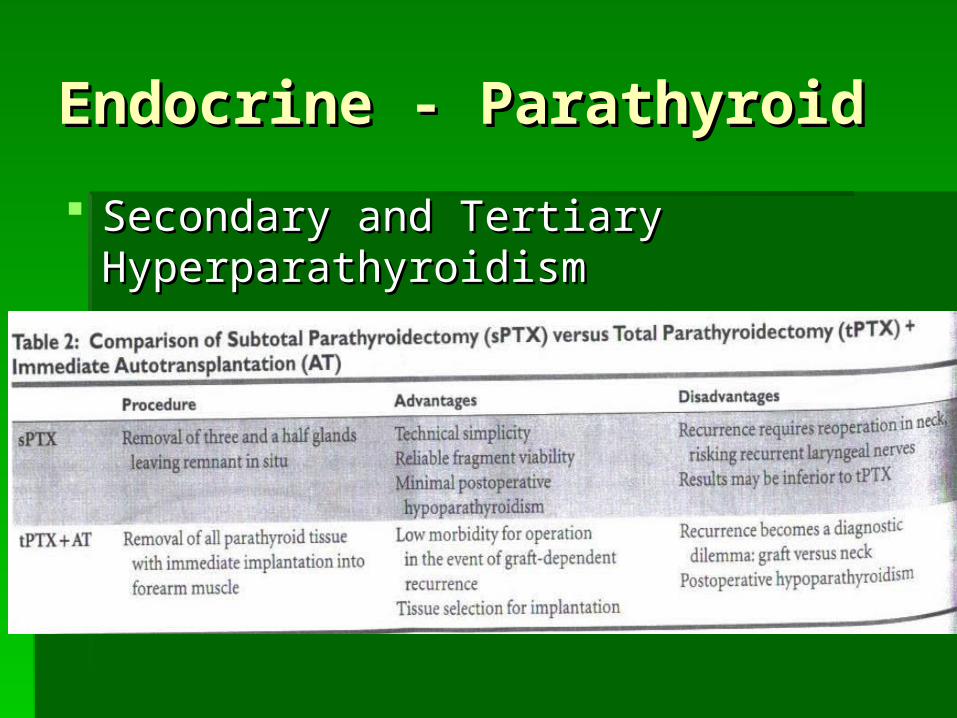
only 1% usually require surgeryonly 1% usually require surgery Bilateral exploration either performing subtotal Bilateral exploration either performing subtotal
parathyroidectomy or total parathyroidectomy with parathyroidectomy or total parathyroidectomy with immediate autotransplantationimmediate autotransplantation
Endocrine - ParathyroidEndocrine - Parathyroid
Secondary and Tertiary HyperparathyroidismSecondary and Tertiary Hyperparathyroidism Tertiary hyperparathyroidismTertiary hyperparathyroidism
Occurs in setting of longstanding 2HPTOccurs in setting of longstanding 2HPT Longstanding parathyroid hyperplasia leads to Longstanding parathyroid hyperplasia leads to
autonomous functionautonomous function Bilateral exploration either performing subtotal Bilateral exploration either performing subtotal
parathyroidectomy or total parathyroidectomy with parathyroidectomy or total parathyroidectomy with immediate autotransplantation immediate autotransplantation
Endocrine - ParathyroidEndocrine - Parathyroid
Secondary and Tertiary HyperparathyroidismSecondary and Tertiary Hyperparathyroidism Indications for surgeryIndications for surgery
Bone and joint painBone and joint pain Intractable pruritisIntractable pruritis Muscle weaknessMuscle weakness MalaiseMalaise X-ray signs of renal osteodystrophyX-ray signs of renal osteodystrophy Uncontrolled hypercalcemiaUncontrolled hypercalcemia Uncontrolled hyperphosphatemiaUncontrolled hyperphosphatemia Extraskeletal nonvascular calcificationsExtraskeletal nonvascular calcifications calciphylaxiscalciphylaxis
Endocrine - ParathyroidEndocrine - Parathyroid
Secondary and Tertiary HyperparathyroidismSecondary and Tertiary Hyperparathyroidism
Endocrine - ParathyroidEndocrine - Parathyroid
Persistent or Recurrent HyperparathyroidismPersistent or Recurrent Hyperparathyroidism Re-operation surgery includes surgery for Re-operation surgery includes surgery for
persistent HPT when the previous operation has persistent HPT when the previous operation has failed, and recurrent HPT following initially failed, and recurrent HPT following initially successful surgerysuccessful surgery
Main causes of recurrent or persistent PHT is Main causes of recurrent or persistent PHT is missing an adenoma on initial surgery (e.g., missing an adenoma on initial surgery (e.g., failure to locate an ectopic gland), multiglandular failure to locate an ectopic gland), multiglandular disease, multiple adenomas or hyperplasia of disease, multiple adenomas or hyperplasia of the remaining glands, or transplanted the remaining glands, or transplanted parathyroid tissueparathyroid tissue
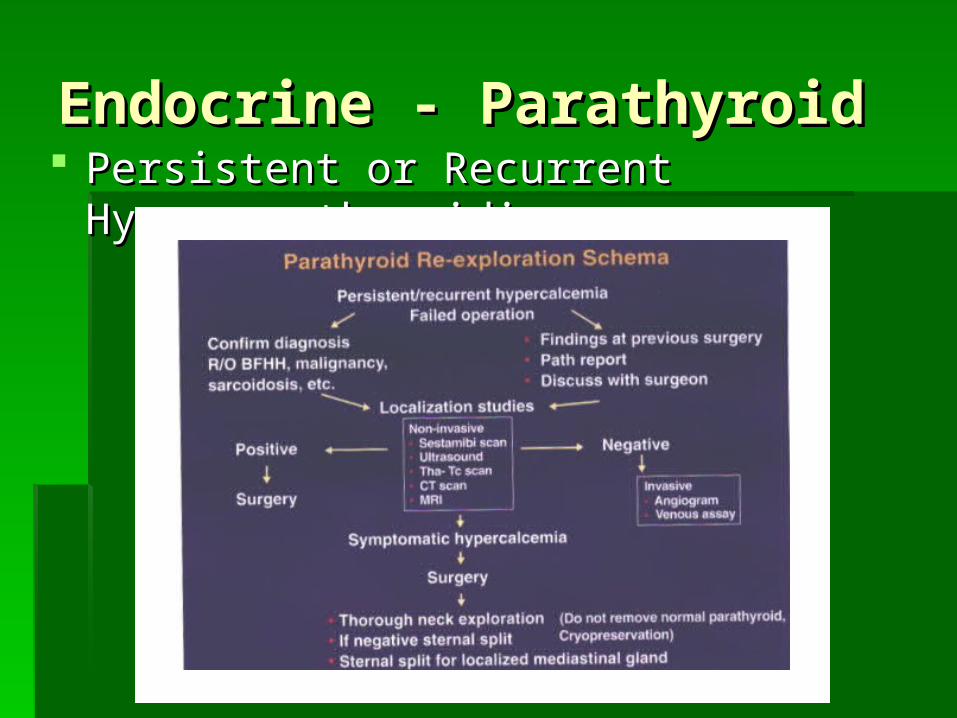
Endocrine - ParathyroidEndocrine - Parathyroid Persistent or Recurrent HyperparathyroidismPersistent or Recurrent Hyperparathyroidism

BibliographyBibliography
BibliographyBibliography
BibliographyBibliography
Kreisel, D. et al. Kreisel, D. et al. The Surgical Review: An integrated basic and clinical science The Surgical Review: An integrated basic and clinical science study guide.study guide. Lippincott, 2001. Lippincott, 2001.
Randolph, G. Randolph, G. Management of the Thyroid NoduleManagement of the Thyroid Nodule. American Academy of . American Academy of Otolaryngology – Head and Neck Surgery Foundation, Inc., 1999.Otolaryngology – Head and Neck Surgery Foundation, Inc., 1999.
Silver, C. and Rubin, J. Silver, C. and Rubin, J. Atlas of Head and Neck SurgeryAtlas of Head and Neck Surgery. Churchill Livingston, . Churchill Livingston, 1999.1999.
Cummings, C. et al. Cummings, C. et al. Otolaryngology Head and Neck SurgeryOtolaryngology Head and Neck Surgery. Mosby, 1993.. Mosby, 1993. Bailey. Head and Neck Surgery – Otolaryngology. Lippincott Greenfield. Surgery – Scientific Principles and Practice. Lippincott Harvey, H. The Otolaryngologic Clinics of North America: Disorders of the thyroid
and parathyroid. Vol I. April 1990. Harvey, H. The Otolaryngologic Clinics of North America: Disorders of the thyroid
and parathyroid. Vol II. June 1990. Shindo, M., and Singer, P. The Otolaryngologic Clinics of North America: Current
concepts in the management of thyroid and parathyroid disorders. August 1996. Miller, F., and Otto, R. The Otolaryngologic Clinics of North America: Disorders of
the thyroid. February 2003. Stack, B. The Otolaryngologic Clinics of North America: Parathyroids. August 2004