endocrine exit revision - bma - home · feedback system / show how levels of certain ......
TRANSCRIPT

BMA EXIT RevisionEndocrine
Martin Hunter and Patrick Clements

Learning Objectives
Take you through the anatomy, physiology and pathology of the
following organs:
1. Hypothalamus-Pituitary Axis
2. Thyroid
3. Adrenals
----------------------------------------------------
1. Pancreas
2. Diabetes (majority of past paper questions)

So, what is expected of you by the end of 2nd year…
Past Paper Questions:
1. Wanted you to understand and be able to draw a negative feedback system / show how levels of certain hormones are controlled (e.g. 2011 – Cushing’s and Thyroid Hormones)
2. Describe the clinical symptoms of thyroid conditions
3. Most PPQs centre around Diabetes – this shall be the main focus of this lecture. Explain why patients experience increased thirst etc
4. Draw and label Pancreas including local structures

Hypothalamus and Pituitary
1. ANTERIOR [Adenohypophysis]- Growth: Rathke’s Pouch- Blood Supply: Hypophyseal portal vessels (link to
hypothalamus)
2. POSTERIOR [Neurohypophysis]- Growth: Downgrowth from brain and is a continuation of the
hypothalamus
- Oxytocin- Stimulated by mechanoreceptors in the breast during
suckling – stimulates milk ejection- Antidiuretic Hormone (ADH)
- Local osmoreceptors and baroreceptors in CVS- Rise in ADH promotes water reabsoprtion
Anatomical Location:Pituitary located in the Sella Turcica of the Sphenoid bone• Clinical implication in terms of visual problems if enlarged

Microadenoma <10mm vs Macroadenoma >10mm diameter
Hyperfunctioning Pituitary Adenomas↑↑GH Acromegaly
↑↑ ACTH Cushing’s Disease
Additional Information: Pituitary Adenomas and how they affect the Optic Chiasm – Bitemporal Hemianopia

Hypothalamic ‘Releasing’ Hormones
Anterior
CRH ACTH
TRH TSH
GnRH FSH / LH
PRH Prolactin
GNRH hGH
Hypothalamus Pituitary End Organs Feedback

Clinical: Abnormal Pituitary Function
Hormone Undersecretion Oversecretion
ACTH Cortisol Deficiency Cushing’s
TSH Secondary Hypothyroidism -
FSH/LH Sexual Dysfunction -
hGH Dwarfism Acromegaly
Prolactin - Hyperprolactinaemia
ADH Diabetes Insipidus SIADH
Acromegaly [increased Growth Hormone]:• 99% due to benign pituitary tumour• Effects of GH excess depend on epiphyseal plate fusion (gigantism vs
acromegaly)Signs and symptoms of excessive tissue growth: - Coarsening facial features - Macroglossia- Prominent mandible (prognathism) - Frontal bossing- Dilated cardiomyopathy - IGT or Diabetes

THYROID: Anatomical Position and Histological Structure

T3 / T4 – Production and Actions
MIT + DIT = T3 (more biologically active)
DIT + DIT = T4 (T4 > T3 production)
Know the effects of these hormones:
• Basal Metabolic Rate increased
• Heart Rate rises as does Cardiac Output
• Respiratory Rate increased
• Bowel activity increased
• Protein / Carbs / Fats metabolism increased
• Enhances Sympathetic nervous system
• Knowing the systemic effects can help determine symptoms when the hormones are in excess or are deficient….
Thyroid Hormone Synthesis

Hyperthyroidism - ↑T4 - ↓TRH & TSH
Management (PODT Lectures)
1. Block (Carbimazole)2. Block and Replace (Carbimazole + Levothyroxine)3. Radioactive Iodine (131I)4. Surgical (Thyroidectomy - be aware of early + late
complications)
5. Also consider symptom management: Beta-Blockers
Causes:1. Graves2. Toxic Multinodular Goitre3. Toxic Adenoma
• Goitres can occur in both hyper/hypo – but more common in hyperthyroid
• Thyroid [Grave’s] eye disease (see picture)

Past Paper Example:

Hypothyroidism - ↓T4 - ↑TRH & TSH
Management (PODT Lectures)
1. Levothyroxine – low and slow approach
Causes:1. Thyroiditis e.g. Hashimoto’s2. Severe Iodide Deficiency3. Deficiency in synthesis enzymes4. Removal or Destruction of Thyroid

Examination of Thyroid
Brief discussion of the main points to remember during a thyroid exam:
1. LOOK: Expose Adequately2. WATER: Swallow a sip of water3. TONGUE: Stick out tongue
4. FEEL: Examine one lobe at a time – stabilize the other5. WATER: Swallow whilst palpating thyroid6. TONGUE: Stick out tongue whilst palpating
7. Describe what you feel:• SSS / CCC / TTT

Adrenals
• Anatomical Position – superior pole of the kidneys
• Driven by ACTH – mainly by acting on the cortex
Layers of the Adrenal Gland:
• Cortex• Glomerulosa (Salt): Mineralocorticoid (Aldosterone)
• [reg RAAS, K+, ACTH – action is to retain sodium, water and release K+ and H+]
• Fasciculata (Sugar) : Glucocorticoids (Cortisol) • [stress hormone]
• Reticularis (Sex) : Androgens (Testosterone) • [small amount, mostly gonads]
• Medulla – Chromaffin cells / Catecholamines: • Adrenaline/Noradrenaline

PPQ: Can be asked to draw the separate layers and state which hormones are produced where

Clinical Perspective -Cushing’s Disease
Mnemonic:
C Central Obesity
Cervical Fat Pads
Comedones
U Urinary free glucose and cortisol increased
S Striae
Suppressed Immunity
H Hypertension
Hirsuitism
Hyperglycaemia / Hypercholesterolemia
I Iatrogenic (Corticosteroid Treatment)
N Neoplasms
G Glucose Intolerance
Growth Retardation
• Increased glucocorticoid activity – why?1. Increased ACTH2. Glucocorticoid-secreting tumour in
adrenal cortex3. Prolonged steroid treatment

Clinical Perspective -Addison’s Disease
Deficient Secretion:
• Primary: Failure of adrenal cortex, decreases negative feedback, increases ACTH
• Secondary: Reduced stimulation of the gland by ACTH following anterior pituitary damage.
So there is reduced mineralocorticoids and glucocorticoids.
Addison’s requires lifelong steroid replacement(Hydrocortisone and Fludrocortisone)


Diabetes Mellitus

Learning outcomes Know the relevant anatomy of the pancreas
Appreciate the actions of insulin and how this relates to the signs and symptoms of diabetes
Understand the distinction between type 1 and type 2 diabetes mellitus
Be aware of the presentation, diagnosis and management of diabetes
Understand the complications (both acute and chronic) and how these are managed

Pancreas

Endocrine pancreas Islets of LANGERHANS – endocrine portion
Islets possess 4 types of endocrine cell:

Insulin Insulin is a peptide hormone secreted by the beta cells of the Islets of
Langerhans
Insulin’s main role is to regulate cellular absorption and utilisation of glucose
It is therefore an important determinant of plasma glucose concentration
Under normal conditions glucose levels are maintained around 5 mmol/l under fasting conditions, but may rise up to 8mmol/l after a meal

Insulin A number of factors regulate insulin secretion but plasma glucose is the most
important
Elevation of the plasma glucose concentration directly stimulates a rapid rise in insulin secretion
Insulin levels are therefore low at fasting conditions but rise as glucose is absorbed after a meal
Secretion of insulin by beta cells decrease as glucose levels decline, so insulin falls back to a low concentration in the postabsorptive state 3-4 hours after a meal

Metabolic actions of insulin Insulin is an anabolic hormone, affecting carbohydrate, protein and lipid metabolism in a wide range of body tissues
Carbohydrate Metabolism Stimulates glucose uptake in most body tissues (except brain) Promotes glycogen storage Stimulates glucose use for energy by stimulating glycolysis
Protein Metabolism Promotes protein accumulation within cells by:
stimulating amino acid uptake particularly in muscle Stimulating protein synthesis and inhibiting protein breakdown Inhibiting conversion of amino acids to glucose (gluconeogenesis)
Lipid Metabolism Promotes triglyceride deposition in body lipid stores by:
inhibiting breakdown of stored lipids stimulating fatty acid synthesis from glucose Promoting triglyceride synthesis for storage Promoting carbohydrate metabolism so that fat is spared

Types of Diabetes Mellitus Inadequate insulin effect leads to the clinical syndrome of diabetes
mellitus. This may arise in 3 ways:
A primary deficiency of insulin is classified as type 1. This results from an autoimmune response to pancreatic beta cell components, triggered possibly by a viral infection. This typically occurs in younger people (from childhood to young adults)

Types of Diabetes Mellitus In type 2 diabetes insulin secretion is relatively unimpaired but insulin’s
metabolic effects on the body are inhibited. This condition of insulin resistance is usually seen in middle aged to elderly overweight individuals
Occasionally diabetes is not due to a defect in insulin action but is due to excess secretion of a diabetogenic hormone eg cortisol, growth hormone or glucagon (secondary diabetes)

Presentation Patients with all types of diabetes may present with polyuria, polydipsia,
lethargy, or with frequent, recurrent or prolonged infections
Patients with type 1 diabetes may also present with weight loss, dehydration, ketonuria and hyperventilation. Presentation of type 1 diabetes tends to be acute with a short duration of symptoms
Presentation in patients with type 2 diabetes tends to be subacute with a longer duration of symptoms
Patients with diabetes may present with acute or chronic complications of diabetes

Symptoms explained Many of the symptoms and biochemical disturbances in insulin dependant
diabetes can be explained by thinking of the metabolic effects of insulin on the body: Hyperglycaemia - decreased glucose uptake and utilisation leads to high plasma glucose
Glycosuria - excess glucose is excreted via the kidneys (usually gets completely reabsorbed, but in diabetes mellitus renal transport mechanisms get saturated)
Polyuria - elevated glucose in renal tubules leads to osmotic retention of water, and so an increased rate of urine production (osmotic diuresis)
Polydipsia - thirst in response to dehydration from renal fluid loss
Weight loss - lipid mobilization from fat stores
Ketosis - low levels of glucose uptake and utilisation means that fat is oxidised for energy, forming ketone bodies and causing a metabolic acidosis
Increased ventilation - respiratory compensation for the acidosis, trying to ‘blow off’ CO2 with increased respiration

Diagnosing diabetes Fasting glucose > 7 mmol/l or
2 hour post oral glucose tolerance test (OGTT) > 11.1 mmol/l
Can now also be diagnosed from HbA1c (Type 2 only). An HbA1c of 6.5% is recommended as the cut off point for diagnosing diabetes.
However a value of less than 6.5% does not exclude diabetes diagnosed using glucose tests.
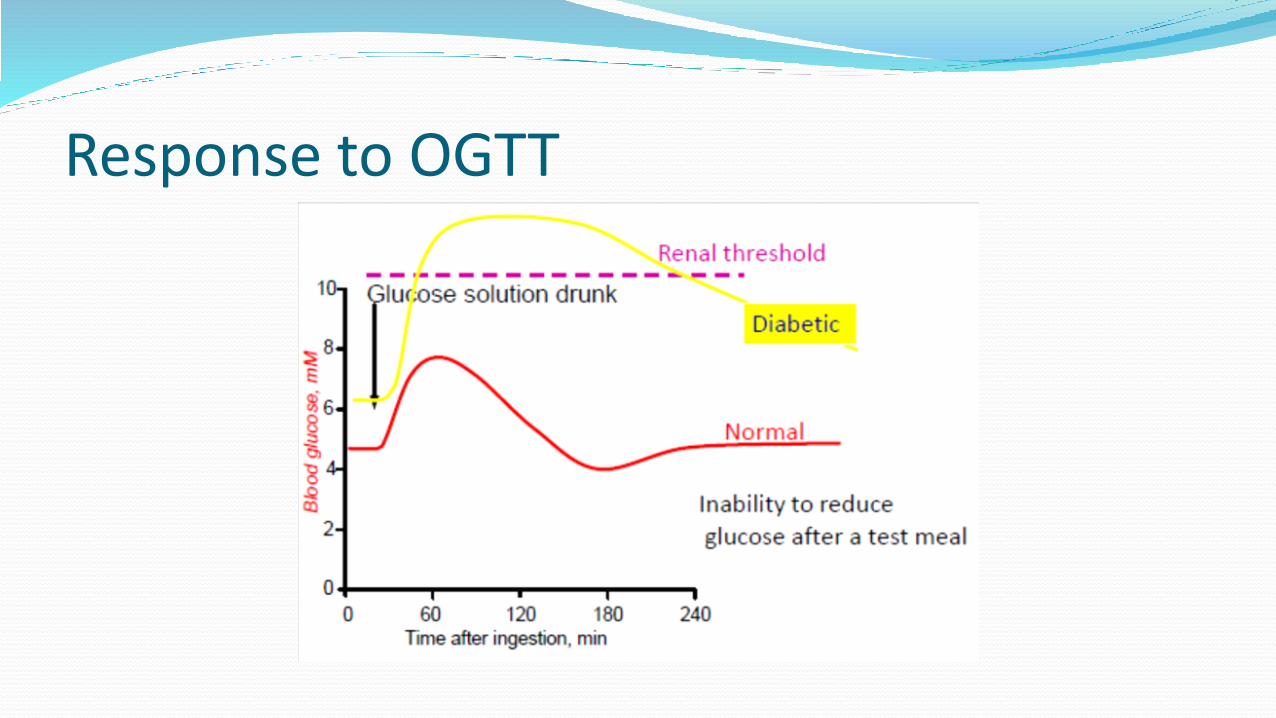
Response to OGTT

Treatment Type 1
– Insulin [twice-daily regimen, basal-bolus regimen, continuous subcutaneous insulin infusion (insulin pump therapy)]
Type 2 Lifestyle modifications (may be enough on their own)
Diet, exercise and weight reduction
Oral hypoglycaemic agents Metformin 1st line for those with BMI > 25 Sulphonylureas (gliclazide) 1st line if BMI < 25 Others eg thiazolidinediones [pioglitazone (warning: heart failure)] and DDP4 inhibitors
(sitagliptin) may be used as 2nd line treatment
If not effectively controlled on oral treatment insulin will be commenced (most patients should be started on a long or intermediate acting insulin once a day eg insulatard. This may be stepped up to a basal-bolus regime if required)
In type 2, insulin is added to current oral therapy and doesn’t replace it

Treatment Metformin
Mechanism of action - decreases hepatic glucose output and increases utilisation of glucose in peripheral tissues
Side effects – Nausea, vomiting, anorexia, diarrhoea, metallic taste, rarely lactic acidosis
Treatment algorithm - 1st line if BMI>25 Monitoring - Renal function
Sulphonylureas (Gliclazide) Mechanism of action - ↑ insulin release via sulphonylurea receptor on beta islet cells Side effects – GI disturbance, weight gain, hypoglycaemia, hyponatraemia,
occasionally liver function derangement Treatment algorithm - 1st line if BMI<25 Monitoring - Liver and Renal function

Student formulary

Complications Acute and chronic Acute:
Hypoglycaemia Diabetic Ketoacidosis
Chronic: Microvascular
Retinopathy and other eye problems (cataract and glaucoma) Nephropathy Neuropathy (including diabetic foot)
Macrovascular Cerebrovascular disease Coronary heart disease Peripheral vascular disease in lower limbs
Frequent, recurrent and persistent infections

Hypoglycaemia Causes
Too much insulin, missed meal, exercise, weight loss, alcohol
Symptoms Sympathetic response occurs first. Sweating, anxiety, palpitations, hunger and
tremor occur when plasma glucose less than 3.3 mmol/l However in poorly controlled diabetics this threshold may be higher
Neuroglycopenia occurs later when plasma glucose less than 3.1 mmol/l. (Again thresholds may differ) Lethargy, drowsiness, seizures, coma, death
Management If alert give sugar either 4 dextrose tablets or half a glass of lemonade, followed by
slow release carbohydrate e.g. biscuits or bread
If oral intake not possible glucagon injection should be given

Diabetic Ketoacidosis (DKA) Cause
Insulin deficiency due to omission of insulin.
Insulin requirements increased due to illness e.g. infection or MI
Symptoms
May be vague – abdominal pain, thirst, nausea/vomiting, fatigue, breathlessness
Management
DKA protocol [lots of fluid (0.9% sodium chloride), insulin 0.1 units/kg/hour]

Sick day rules Never stop taking your insulin or omit doses. Your blood sugar levels may continue to rise even if you do not eat
If your blood sugar levels are higher than 10 mmol/l consider taking a larger or additional dose of insulin
Test your blood glucose more often. If your levels are unstable increase the frequency to every 2-4 hours or more
If blood glucose readings are higher than 13 mmol/l, and you are unwell or vomiting, check your urine/blood for ketones
Drink lots of fluids. It is easy to become dehydrated when you are ill especially if you have a temperature, vomiting or diarrhoea. You also lose fluids through sweating and breathing
Aim to drink at least 3 litres of fluid a day. If you take this in small amounts such as a glass every hour you should manage to cope with the extra volume. If this is difficult persist with regular sips
When people are admitted to hospital with ketoacidosis they are severely dehydrated and require as much as 6-9 litres of fluids to restore lost volumes
Stick to your normal diet as far as possible. If unable to eat solids take liquids
If you are unable to keep fluids down attend your doctor/A+E

Reducing risk of chronic complications Education to maximise glucose control (while minimizing adverse effects
such as hypoglycaemia)
Diet and exercise
Smoking cessation and weight loss (if appropriate)
Reduction of other risk factors for complications of diabetes, including the early detection and management of hypertension, drug treatment to modify lipid levels and consideration of antiplatelet therapy with aspirin
Monitoring and early intervention for complications of diabetes, including cardiovascular disease, foot problems, eye problems, kidney problems and neuropathy

Learning outcomes Know the relevant anatomy of the pancreas
Appreciate the actions of insulin and how this relates to the signs and symptoms of diabetes
Understand the distinction between type 1 and type 2 diabetes mellitus
Be aware of the presentation, diagnosis and management of diabetes
Understand the complications (both acute and chronic) and how these are managed

Good Luck

Questions?