encephaloceles: the kijabe experience€¦ · encephalocele repair is generally a clean procedure...
TRANSCRIPT

Authors:
Munyi N 1,2, Poenaru D 1, Bransford R 1, Albright L 1
Affiliation:
1.Bethany Kids at Kijabe Hospital, Kijabe, Kenya.2.School of Medicine, University of Nairobi
ENCEPHALOCELES: THE
KIJABE EXPERIENCE
INTRODUCTION
� Encephaloceles are congenital lesions consisting of a herniationof intracranial contents 1.
� The herniation may consist of :� Meninges only (meningocele),
� Brain matter (encephalocele)
� Meninges + brain matter (meningoencephalocele)
� Meninges + brain matter + ventricle (hydroencephalomeningocele) 1
1. JeffreyV. Rosenfeld and David A.K. Watters, Neurosurgery in the tropics: A practical
approach to common problems, Macmillan Education Ltd, 2000
Are they NTDs?� There has been controversy as to whether they are all truly NTDs.
� Studies have reported that only a minority are / are associated NTDs 2
� Rowland et al 2002 found that with folic acid fortification, prevalence decreased for spina bifida but not significantly for encephaloceles or anencephaly 3.
2. Humphreys R E. Encephaloceles and Dermal Sinuses in: Cheek W R et al, Pediatric
Neurosurgery: Surgery of the Developing Nervous system. 1994
3. Rowland et al Are encephaloceles neural tube defects? Pediatrics 2006; 118:916-923
Epidemiology� Are rare and the incidence varies with geographical location and race. 4
� Overall incidence is 0.8 to 3.0 per 10,000 live births. 5,6,
� Occipital type (85 % of encephaloceles) is most common in N. America and W. Europe with an incidence varying between 1 in 3000 to 1 in 10,000 LB 7,8
� 70% of occipital encephaloceles are in females 7
� 15-20% are associated with NTD
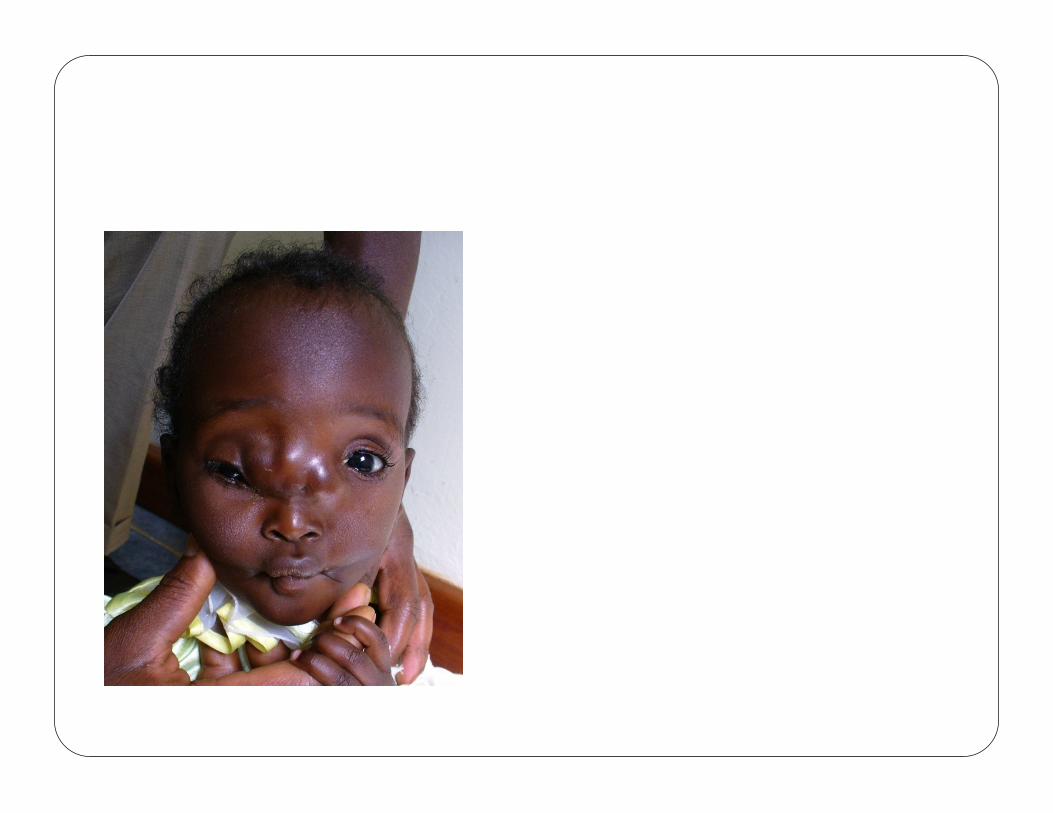
� Anterior encephaloceles are mostly found in SE Asia, Russia and Central Africa . The incidence ranges from 1 in 3500 to 1 in 5000 4,7
4. Suwanwela C and Suwanwela N, A morphological classification of Sincipital
Encephalomeningoceles. J Neurosurg 1972, 36 201-211
5Macfarlane R, Rutka JT, Armstrong D et al Encephaloceles of the anterior cranial fossa, Pediatric
neurosurgery 1995: 23(3) 148-158
6. Simpson DA, David Dj, White J. Cephaloceles treatment, outcome, and antenatal diagnosis.
Neurosurgery. 1984;15:15-21
7. Chapman PH, Swearingen B, Caviness VS. Subtorcular occipital encephaloceles. J. Neurosurg.
1989;71:375-381
8. Mealey Jr J, Dzenitis AJ. The prognosis of encephaloceles. J Neurosurg. 1970; 32: 209-218
CLASSIFICATION
Convexity
� Occipital
� Parietal
� Saggital
� Occipitalcervical
Atretic
Sincipital
� Frontoethmoidal-nasofrontal-nasoethmoidal
-naso-orbital
� Interfrontal
� Craniofacial cleftBasal
� Intranasal
� Spheno-orbital
� Sphenomaxillary
� Spenopharyngeal
Are classified according to the anatomical location of the
skull defect 4
These include:
RATIONALE OF STUDY
� Though encephaloceles are rare congenital malformations, they are associated with severe morbidity and mortality if untreated.
� Most reported series of encephaloceles originate in the West, where resources for their treatment are radically different thanin Africa.
� This study seeks to find out the presentation, management and complications of encephaloceles in an African setting as well as
answer the question: Can encephaloceles be successfully managed in a resource-poor setting?
Design and Methodology� A retrospective study of patients seen and managed at Kijabe hospital between January 1998 and August 2006.
� Inclusion criteria: any patient with an encephalocele.
� Exclusion criteria: any patient who’s records were not available.� Data collected: Biodata, Type of encephalocele, Associated anomalies, US and CT features, Surgical approach used, Intra-OP and Post-OP complications and Follow up outcomes.
� Data Analysis: Calculation of Means, Drawing of frequency charts and distribution graphs done.
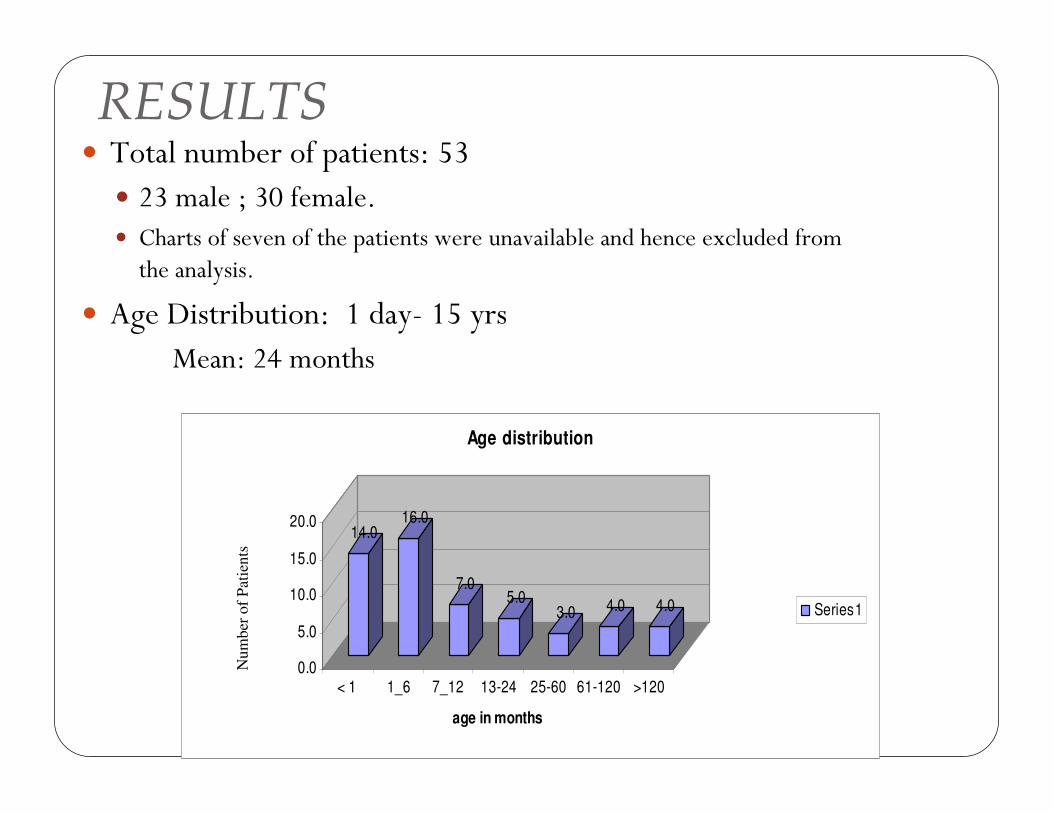
RESULTS� Total number of patients: 53
� 23 male ; 30 female.� Charts of seven of the patients were unavailable and hence excluded from the analysis.
� Age Distribution: 1 day- 15 yrs Mean: 24 months
14.016.0
7.05.0
3.0 4.0 4.0
0.0
5.0
10.0
15.0
20.0
< 1 1_6 7_12 13-24 25-60 61-120 >120
age in months
Age distribution
Series1
Num
ber
of
Pat
ien
ts

Types of encephaloceles
distribution0%
2%
4%
33%
61%
basal
complex
missing
sincipital
convexity
Convexity encephaloceles
88%
6%
0%6%
occipital
parietal
sagggital
occipitocervical
detailed distribution
53%
0%
4%
4%
24%
9%2% 0%
4%
occipital
parietal
sagggital
occipitocervical
frontoethmoidal
interfrontal
basal
complex
missing
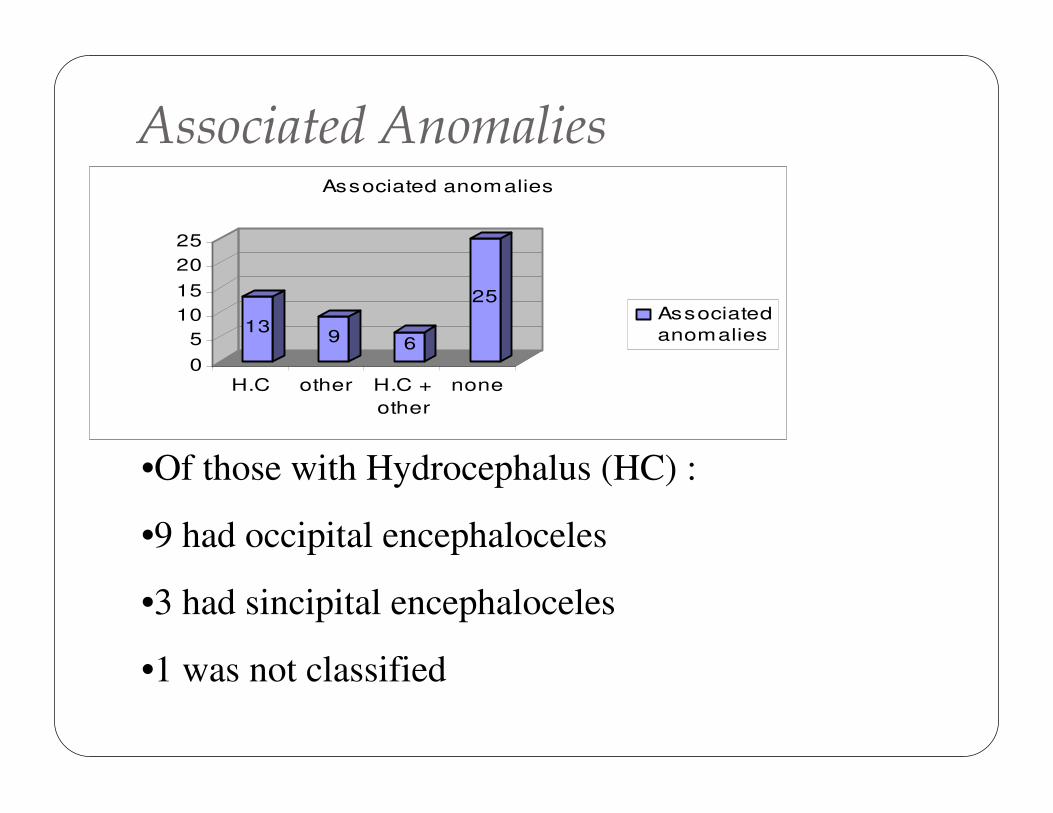
Associated Anomalies
•Of those with Hydrocephalus (HC) :
•9 had occipital encephaloceles
•3 had sincipital encephaloceles
•1 was not classified
139 6
25
0
5
10
15
20
25
H.C other H.C +
other
none
Associated anomalies
Associated
anomalies
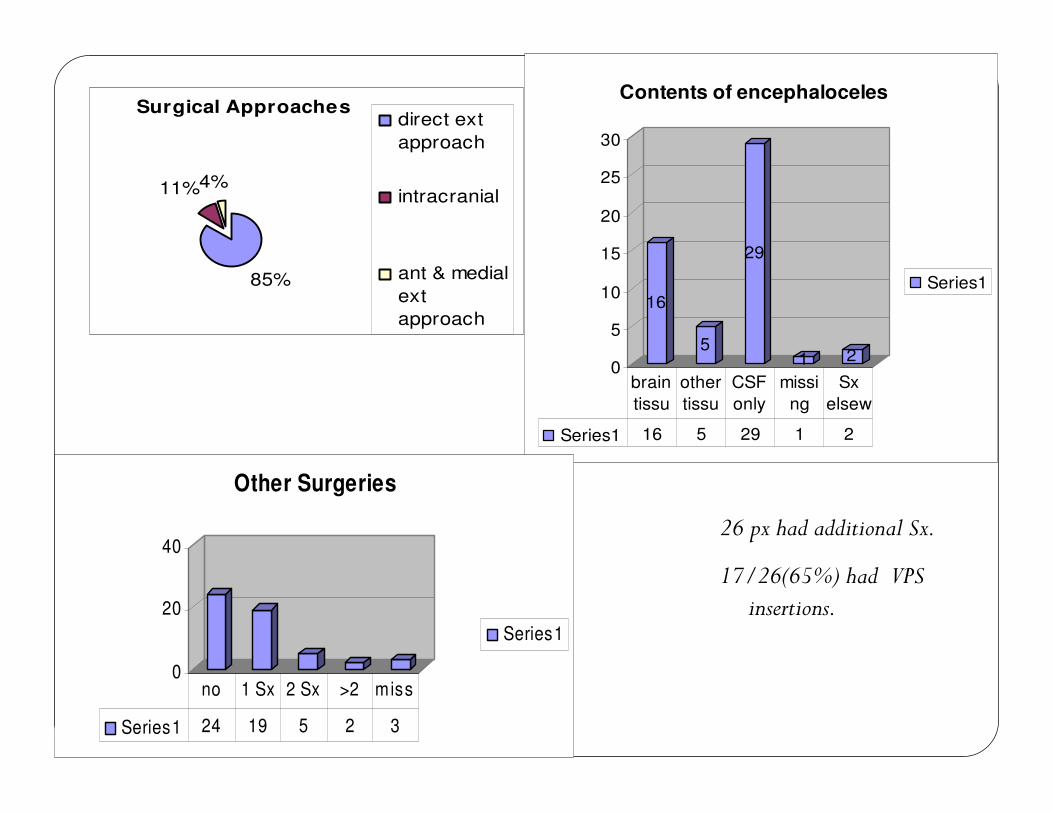
26 px had additional Sx.
17/26(65%) had VPS insertions.
Surgical Approaches
85%
11%4%
direct ext
approach
intracranial
ant & medial
ext
approach16
5
29
1 20
5
10
15
20
25
30
Contents of encephaloceles
Series1
Series1 16 5 29 1 2
brain
tissu
other
tissu
CSF
only
missi
ng
Sx
elsew
0
20
40
Other Surgeries
Series1
Series1 24 19 5 2 3
no 1 Sx 2 Sx >2 miss
Complications(Intra-op, post-op & late)
� 6/49 had intra-operative complications
� 20/49 had post operative complications.� 2 deaths, CSF leak was most common complication 6/20(30%), Others:seizures, wound infection, shunt malfomations, HC
� 10/47 had late post-operative complications� 2 deaths, 3 recurrences, 1CP, 2 HC, 1 infection, 1 frontal swelling
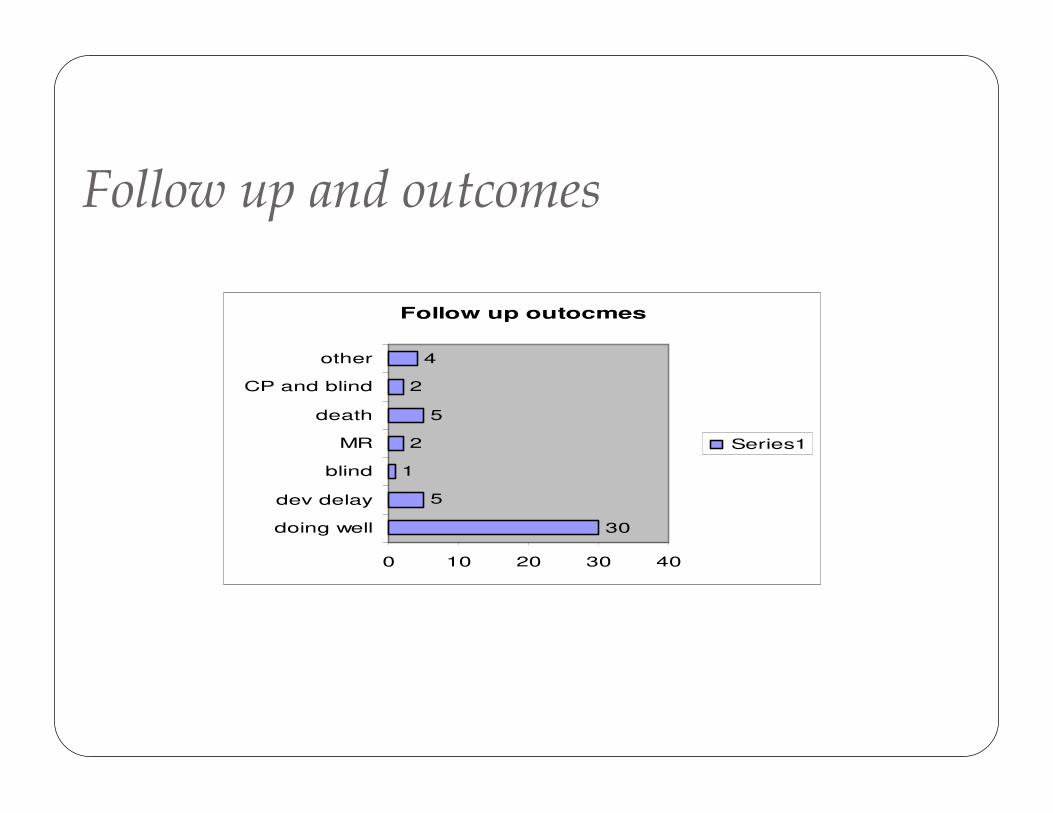
Follow up and outcomes
Follow up outocmes
30
5
1
2
5
2
4
0 10 20 30 40
doing well
dev delay
blind
MR
death
CP and blind
other
Series1
Discussion� Our sample size on of the largest case series in literature (over 8 yr period)
� Missing population based data therefore no conclusion on incidence can be made
� Female preponderance: our study 61% vs other studies:70%
� Contrary to other studies: occipital type is most common in our set up.
� Most of our patients had mainly CSF with little brain tissue: good prognosis

Discussion II
� Age at presentation: earlier presentation than in Thailand study (70% present under 6 months in our study, in Thailand most present between 6-12months)
� Imaging: inaccessible due to low socioeconomic status
� Various surgical approaches have different indications.
� Complications: most common CSF leak- similar to other studies.
Conclusions� Diagnosis can be done on clinical basis.� Encephalocele repair is generally a clean procedure hence no need for routine pre-operative medication.
� External approach is used for occipital but intracranial gives better outcome for frontal
� Most common associated anomaly is HC� Encephaloceles generally have good outcome even in an African setting.
ERROR: stackunderflow
OFFENDING COMMAND: ~
STACK: