encephalitis s. sears, md. herpes simplex virus type 1 most common cause of fatal sporadic...
TRANSCRIPT

Encephalitis
S. Sears, MD
Herpes simplex virus type 1
Most common cause of fatal sporadic encephalitis
HSV infection of the CNS• Immediate CNS invasion
– From the trigeminal nerve or olfactory tract– Follows an episode of primary HSV-1 of the oropharynx
• CNS invasion after recurrent HSV-1 infection– Represents viral reactivation with subsequent spread
• CNS infection without primary or recurrent HSV-1 infection– Represents reactivation of latent HSV in situ within the CNS

Pathogenesis
Necrosis occurs in the temporal lobe
• Direct viral-mediated inflammation– Extent of viral load may be directly related to severity of
disease
• Indirect immune-mediated CNS damage– Not more common in immunocompromised patients

Clinical features
Focal neurologic findings are acute (< 1 week)• Altered mentation - level of consciousness• Focal cranial nerve deficits• Hemiparesis• Dysphasia• Aphasia• Ataxia• Focal seizuresFeverLater in the clinical course• Diminished comprehension• Paraphasic (word substitution) spontaneous speech• Impaired memory• Loss of emotional control
Behavioral syndromes
Hypomania• Inflammation of the temporal - limbic system• Elevated mood• Excessive animation• Decreased need for sleep• Inflated self-esteem• Hypersexuality
Kluver-Bucy syndrome• Psychic blindness• Loss of normal anger and fear responses• Inappropriately oral and sexual
States of amnesia

Recurrent brainstem encephalitis
Upward gaze
Facial numbness
Signs of involvement• Corticospinal tract• Spinothalamic tract• Cerebrellar pathways

Investigations
Laboratory• CSF
– Lymphocytic pleocytosis– Increased RBC– Elevated protein– Normal glucose– PCR-diagnostic confirmation
Electroencephalogram (EEG)• Nonspecific• Continuous periodic lateralizing epileptiform discharges

Investigations
Imaging• CT
– Predominantly unilateral temporal lobe lesions– May be associated with mass effect
• MRI– More specific than CT– Brain perfusion studies demonstrate hyperperfusion early in
disease

HSV encephalitis

Differential diagnosis
Arthropod virusesOther herpesviruses (CMV,EBV,VZV)Viral MeningitisBrain abscessPost-infectious Reye syndromeAcute disseminated encephalomyelitisVasculitisNeurosyphilisPrimary or secondary malignancyToxic encephalopathy

Diagnosis
Gold standard• PCR• Detects HSV DNA in the CSF• Positive early in the course of the disease• Detectable 2-4 weeks after the onset of illness
If PCR negative • Patient clinically deteriorates on therapy• Brain biopsy• Still the only accurate way for certain diagnosis
CSF antigen and antibody determinations not helpful
Viral culture rarely positive

Treatment
Acyclovir 10mg/kg IV q8hrs for 21 days• Infuse slowly and with fluid to prevent crystalluria and renal failureShorter courses have been associated with relapseTreat early• Before loss of consciousness• Within 24 hours onset symptoms• Glasgow Coma Scale 9-15Discontinue therapy• Low probability of encephalitis• Normal imaging, CSF, mental status• Negative CSF PCRContinue therapy • High risk patient• Abnormal imaging, CSF, mental status,seizures, abnormal EEG• Look for alternative why PCR negative
– Early testing, antiviral therapy, PCR inhibitors (bloody CSF)

Prognosis
Fatality• 70 percentSurvivors• Serious neurologic deficits• Significant neuropsychiatric difficulties• Significant neurobehavioral issues

Rabies
Neurotropic RNA viruses• Belong to the family RhabdoviridaeHuman infections• From rabid animals through a bite• In developing countries
– Dogs account for 90 percent of reported cases
• In the United States– Four major animal reservoirs
• Bats• Raccoons• Skunks• Foxes
• Unusual transmission– Organ donor died of encephalitis-unknown cause– All recipients were diagnosed with rabies

Pathogenesis
Viruses deposit in peripheral wounds• Exposed skin vs bite through clothing• Face and head vs peripheral site (distance
from CNS)• Amount of virus in the saliva• Degree of innervation at the site of bite• Host immunity

Pathogenesis
Retrograde passage of virus• Peripheral nerve• Dorsal root ganglia• To brainViral replication in CNS• Localizes
– Brainstem– Thalamus– Basal ganglia– Spinal cord
Spread from CNS• Heart • Skin• Salivary glands
Clinical manifestations
Classic forms• Encephalitic
– Hydrophobia– Aerophobia– Pharyngeal spasms– Hyperactivity
• Paralytic– Quadriparesis– Mimics Guillain-Barre– Cerebral involvement is late in the course

Clinical manifestation
Non-classic form• Bat-associated rabies• Neuropathic pain• Sensory/motor deficits• Choreiform movements of the bitten limb• Cranial nerve palsies• Myoclonus• Seizures
Clinical manifestation
Five general stages• Incubation period• Prodrome• Acute neurologic syndrome• Coma• Death

General stages of disease
Incubation period• One to three months• Can be days to one yearProdrome• Lasts days-not more than a week• Flu-like symptoms
– Malaise– Anorexia– Irritability– Low grade fever– Sore throat– Headache– Nausea– Vomiting
• Viral site of entry– Paresthesias– Pain– Pruritus– Percussion myoedema

General stages of the disease
Acute neurologic syndrome• Lasts two to seven days after prodrome• Encephalitic rabies• Paralytic rabies• Atypical rabiesComa• Generalized flaccid paralysis• Respiratory failure• Vascular collapseDeath• Two weeks after the onset of coma

Diagnosis
Clinical presentationInvestigations• Samples
– Saliva• Reverse transcriptase PCR• Viral culture
– Neck biopsy• Full thickness• At the hairline• Cutaneous nerve• Follicle• RT/PCR• Immunofluorescence staining for viral antigen
– Serum and CSF• Antibody titers
– Brain biopsy• RT/PCR• Immunofluorescence staining for viral antigen
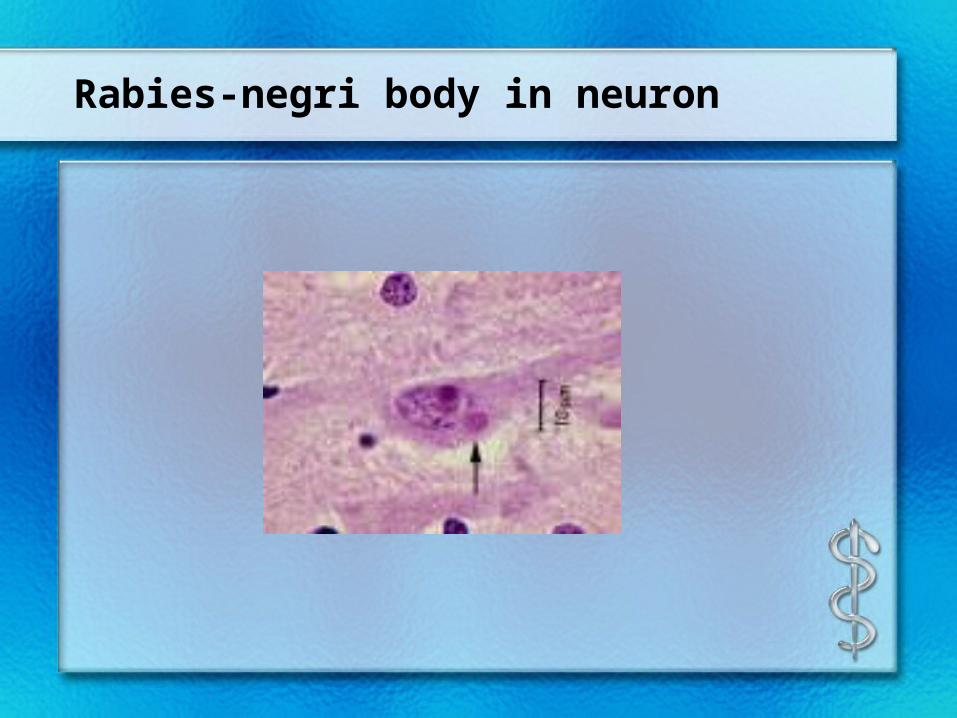
Rabies-negri body in neuron

Rabies-under electron microscope
Treatment
Rabies vaccine• Multiple site intradermal injections• To accelerate the immune responseHuman rabies immune globulin• Total dose 20 IU/kg• Intramuscular• Infiltrated around the wound• To promote clearance of the infectionRibavirin• Intravenous and intraventricularIFN-alfa• Intravenous and intraventricularKetamine• Intravenous infusion• Inhibits rabies virus replicationVaccine• For patients not previously vaccinated

Prevention
Rabies vaccine• Preexposure
– Rabies research lab workers– Rabies biologics manufacturing workers– Veterinarians– Animal control workers– Wildlife workers
• Postexposure– Any patient not previously vaccinated

West nile virus encephalitis
West nile virusMost widely distributed of all the arboviruses• From the group of flavivirusDistribution• Now North America• Was from• Africa• Middle East• Europe• Russia• South Asia• AustraliaCarried by wild birdsTransmitted • By the mosquito bite from the Culex species• Transfused blood• Transplanted organs

Culex pipiens pipiens-northern house mosquito

Clinical manifestation
Incubation ranges from 2-14 daysWest nile fever• Fever• Malaise• Back pain• Myalgias• Anorexia
Persists for 3-6 daysMost frequent symptom• Maculopapular rash• Involves
– Chest– Back– arms

West nile fever - rash

Neuroinvasive disease
Increased risk• Older age• Alcohol abuse• Diabetes• Immunocompromised
Encephalitis• Most common• Presents with
– Headache– Fever– Nausea – Vomiting
• Associated with muscle weakness and flaccid paralysis

Neurologic disease
TremorMyoclonusParkinsonian features• Rigidity• Postural instability• BradykinesiaCranial nerve palsies• Facial weakness• Vertigo• Dysarthria• DysphagiaAcute flaccid paralysis syndrome• Anterior horn cell process (like polio)SeizuresCerebellar ataxiaOptic neuritisWeakness• Brachial plexopathy• Radiculopathy• Demyelinating peripheral neuropathy

Other clinical features
Ocular manifestations• Chorioretinitis• Vitritis• UveitisRhabdomyolysisMyocarditisHepatitisPancreatitisCentral diabetes insipidusPalpable purpura
Diagnosis
Investigations• LP
– CSF• Increased lymphocytes• Increased protein• Normal glucose
• Imaging– CT
• Usually normal– MRI
• Hypertensity– Leptomeninges– Periventricular– Basal ganglia– Thalamus– Caudate nuclei– Brainstem– Spinal cord

Diagnosis
Serology• IgM antibody capture enzyme-linked
immunosorbent assay• Within first 8 days of illness• Convelescent-phase serum as well• Viral nucleic acidCSF• IgM antibody

West Nile fever
Treatment• SupportivePrognosis• Increased risk
– Older age– Immunosuppressed
Long-term sequelae

St. Louis encephalitis
Acute mosquito-borne illnessVirus is a single-stranded RNA flaviviridaeVector -Culex mosquitoSecond leading cause of encephalitis after West nile virusPrincipally occurring• Ohio-Mississippi valley• Eastern Texas• Florida• Southeastern Canada• Northern Mexico

St. Louis encephalitis
Human infection• Inoculation of the virus into human host• Spread via lymphatics and blood• Reaches the choroid plexus• Results in lymphocytic encephalitis
Most severely affected regions• Hypothalamus• Cerebellum• Cerebral cortex• Basal ganglia• Brainstem• Cervical spinal cordIncubation period• 4-21 days
Clinical features
Prodromal symptoms• Four to five days• Fever• Severe headache• Photophobia• Nausea• Vomiting• Malaise• Myalgias

Clinical features
Neurologic signs• Rapid onset• Alerted sensorium• Tremors
– Eyelids– Tongue– Lips– Extremities
• Cranial nerve dysfunction– Unilateral facial motor weakness– Oculomotor dysfunction– Dysarthria
• Myoclonus• Opsoclonus• Nystagmus• Ataxia

Investigations
Laboratory• Increased ALT and CPK• HyponatremiaCSF• Increased lymphocytes• Increased protein• Normal glucose• Negative gram stainImaging• No specific abnormalitiesEEG• Diffuse slowing

St. Louis encephalitis
Diagnosis• Serum• CSF• IgM antibodies• Acute and convalescenceTreatment• No specific antiviral therapy• Supportive• Interferon alfa-2B
– Reduced likelihood after first week in hospital– Quadriplegia– Quadriparesis– Respiratory insufficiency

Outcome
Death in the first two weeks• 20 percent• From direct brain injuryPoor prognosis• Sustained high fever• Convulsions• Advanced age• Severely depressed state of consciousnessConvalescence• Weeks to months• Residual• Headaches• Irritability• Memory deficits• Persistent tremor

Prevention
No available vaccine
Mosquito control
Dengue virus infection
Dengue virus• Member of the family flaviviridae• Distribution in every continent• Except Europe and AntarcticaTransmitted by• Mosquito-Aedes aegypti• Breed in or close to houses

Aedes aegypti mosquito

Clinical presentation
• Asymptomatic infection
• After incubation period 3-14 days– Self-limited dengue fever– Dengue hemorrhagic fever with shock

Asymptomatic infection
• Seen in children under the age of 15 in endemic areas

Dengue fever-classic
Acute febrile illness• Headache• Retroorbital pain• Marked muscle and joint pain• Fever-lasts 5-7 days• Biphasic
– Second febrile phase for 1-2 days
Rash- in 2-5 days after feverHemorrhagic manifestations• Spontaneous bleeding• Melena• Purpura

Classic dengue
Physical exam• Conjunctival injection• Pharyngeal erythema• Lymphadenopathy• Hepatomegaly• Maculopapular rash
Laboratory• Leukopenia• Thrombocytopenia• Serum aspartate transaminase elevated• Virus often found in high concentration in the liver

Dengue hemorrhagic fever
Defined by the World Health OrganizationFour cardinal features• Fever lasting 2-7 days• Marked thrombocytopenia (dec platelets)• Increased vascular permeability
– Plasma leak syndrome– Preceded by abdominal pain– hypothermia– Hemoconcentration– Pleural effusion– Ascites
• Hemorrhagic tendency– Positive tourniquet test (greater than 20 petechiae)– Hematemsis– Melena– epistaxis

Positive tourniquet test

Uncommon syndromes
Liver failureEncephalopathyEncephalitisSeizuresMotor weakness• Mononeuropathies• Polyneuropathies• Guillain-Barre syndrome• Transverse myelitisMyocarditisCholecystitisRetinal vasculitis

Diagnosis
Provisional diagnosis can be made on clinical basisLaboratory testing• Acute phase serum plasma for IgM immunoassay• If negative repeat in 6 days• At least 10-14 days later convalescent serum• Both specimens analyzed together• By hemagglutination inhibitionViral detection• Direct cultureDetection of plasma leakage• Ultrasound

Direct Dengue viral culture

Treatment
No specific therapy-mortality dependent on severity of disease and is variable
Directed atFever• AcetaminophenBleeding• Transfusion
– Red blood cells– Platelets
Reversal of hypovolemic shock• IV fluids• Prevention of end organ damage

Arthropod-borne encephalitides
Similarities• All viruses• Family
– Togaviridae– Flaviviridae– Bunyaviridae– Reoviridae
• Transmitted to humans via a vector– Mosquito-Culex– Tick
• Incubation time after inoculation– From 3 days to two weeks

Arthropod-borne encephalitides
Similarities• Prodrome
– Flu-like illness• Results in encephalitis• Diagnosis
– CSF• Lymphocytosis• Increased protein• Normal glucose• Gram stain negative
– IgM antibody by capture immunoassay in CSF– Demonstrate viral antigen or genome in tissue
• Treatment– Supportive
• Prevention– Arthropod
• Control• Avoidance

Family-Togaviridae
• Eastern equine encephalitis virus• Western equine encephalitis virus• Venezuelan equine encephalitis virus

Eastern equine encephalitis virus
• Virus distributed North,Central,South America and Caribbean
• Virus transmitted by mosquito found in swamp areas• Peak incidence in August and September• Outbreaks along the Atlantic and Gulf coasts• Neurologic deterioration is rapid once symptoms begin• Common
– Seizures– Focal neurologic signs
• Sequelae– Convulsions– Paralysis– Mental retardation
• Mortality is 30%

Western equine encephalitis virus
• Found in North and South America• Flooding
– Increases breeding of Culex mosquito• Summer outbreaks• Large outbreaks
– Horses and humans– Western United States
• Decreasing incidence– Declining horse population– Equine vaccine– Improved vector control
• Neurologic sequelae– Common in infants
• Mortality is 3-7%
Venezuelan equine encephalitis virus
• Distributed from Florida to South America• Six subtypes• Epizootic subtype
– IAB and IC– Produces outbreaks of illness in animals– Cause equine and severe human illness– Transmitted by several mosquitoes
• Enzootic subtype– ID-F, II, III, IV, V, VI– Infects animals sporadic illness– Causes illness in humans– Transmitted by Culex mosquito
• Long-term sequelae and fatalities uncommon

Family-Flaviviridae
• Japanese encephalitis virus• Murray Valley encephalitis virus• Powassan virus• Tick-borne encephalitis virus

Japanese encephalitis virus
• Widespread throughout Asia– Occurs in late summer in temperate regions– Transmitted by Culex mosquito in rice fields
• Seizures are common• Extrapyramidal features
– Expressionless facies– Hypertonia– Cogwheel rigidity
• MRI abnormalities– Thalamus– Basal ganglia– Midbrain– Pons– Medulla
• Diagnosis– Viral antigen or DNA in tissue
• Mortality is 30%• Severe neurologic sequelae
– Motor weakness– Cerebellar signs– Extrapyramidal signs

Murray Valley Encephalitis virus
• Occurs Australia, New Guinea, eastern part of Indonesia• Transmitted by Culex mosquito• Seizures are common in children• Severe cases
– Hyperactive reflexes– Spastic paresis– Coma– Death
• CT– Mild hydrocephalus– Cerebral edema– Decrease in thalamus to brainstem
• Mortality is 30% • Neurologic sequelae is 50%

Powassan virus
• Found in eastern Canada and northeastern United States• Occurs from June to September• Transmitted by ticks
– Species • Ixodes• Dermacentor
• Incubation period 8-34 days• Presents with
– GI complaints– Seizures– Confusion
• Mortality 5-10%• Neurologic sequelae
– Hemiplegia– Headaches– Memory impairment– Ophthalmoplegia
Tick-borne encephalitis virus
• Subtypes– Far eastern– Western Europe– Siberian
• Transmitted by– Ticks
• Species• Ixodes
– Ingestion of raw milk (cows,sheep,goats)• Occurs in spring and summer• Gastrointestinal complaints common• Forms
– Meningeal– Poliomyelitic– Polyradiculoneuritic– Chronic
• Over months to years• Parkinson-like,progressive muscle atrophy, mental deterioration
• Mortality is 1-8%• Vaccines are available in Europe and Canada

Family-Bunyaviridae
La Crosse (California) encephalitis virus• Found in central and eastern United States• Occurs July to September• Transmitted by Aedes mosquito• Common in school-aged children• Common features
– Seizures– Focal neurologic signs
• CT– Generalized cerebral edema
• Mortality is low• Neurologic sequelae 10%
– Focal neurologic– Cognitive deficit– Behavioral deficit

Family-Reoviridae
Colorado tick fever virus• Found in western United States and Canada• Transmitted by the wood tick• Occurs from March to September• Peaks April to June• Clinical features
– Petechial rash– Increasing fatigue
• Virus infects bone marrow– Leukopenia common
• Prognosis is favorable

Chandipura virus
• Found in India• Transmitted by the sandfly• Occurs mostly in children• Identified
– Electron microscopy– Complement fixation– Neutralizing tests
• Rapid onset– Vomiting– Altered mental status– Seizures
• Progressive encephalitis• Mortality rate 50%