emi online tools - nm · • sociologists say 80% of communication is nonverbal. • the meaning of...
TRANSCRIPT

bcbsnm.com October 2013
Cultural Competency
Services are funded in part under a contract with the State of New Mexico.
Blue Cross and Blue Shield of New Mexico refers to HCSC Insurance Services Company (HISC), which is a wholly owned subsidiary of Health Care Service Corporation (HCSC), a Mutual Legal Reserve Company. Both HISC and HCSC are Independent Licensees of the Blue Cross and Blue Shield Association.
Note: Materials are subject to change based on ongoing feedback, newly communicated information and internal revisions.
This training is intended to include all cultures and not be limited to any particular population group(s). It is designed to address the needs of racial, ethnic, and linguistic populations that experience unequal access to health services.

The following course includes the following: • Introduction to cultural competency • Benefits of providing culturally competent health care • Regulatory requirements for cultural competency • Working with diverse patients • Cultural diversity in New Mexico • Tools and additional materials
Cultural competency training is required for providers and other health care personnel as part of the Medicaid contractual requirements for New Mexico.

Introduction to Cultural Competency Culture is a many layered process and it takes many steps on our part to be open and communicate with other cultures. Cultural competency requires that services are effectively provided to people of all cultures, races, ethnic backgrounds, and religions in a manner that respects the worth of the individual and preserves his or her dignity. Cultural Competence is a set of behaviors, attitudes, and policies that come together that enables effective work in cross-cultural situations. Many floors and steps, Just as our culture is comprised of many
layers ; Photo by Sonja Dewing

Cultural Humility refers to the fact that we can never completely know and understand another culture. However, we can approach culture with humility by following certain tenants: 1. Lifelong learning & critical self-reflection; 2. Recognize & challenge power imbalances, and 3. institutional accountability (modeling the principles). A helpful, 30 minute video “Cultural Humility: People, Principles, and Practices”, created by Vivian Chavez, is available on YouTube. Cultural humility is widely accepted as the goal in physical and behavioral practice, and requires us to take responsibility for our interactions with others beyond acknowledging or being sensitive to our differences.
Introduction to Cultural Competency
African medicine; photo by RW Felkin
Benefits of Providing Culturally Competent Health Care • Builds a relationship of trust • Makes more effective use of time with
patients • Improves communication with patients • Increases patient acceptance of treatment
protocols • Positively affects clinical outcomes • Decreases stress and increases satisfaction
for both the provider and the patient • Meets increasingly stringent government
regulations and medical accreditation requirements
Indigenous person of Peru; Photo by Sonja Dewing

A plant used to make medicines for the indigenous population of the Amazon; Photo by Sonja Dewing
Why is Cultural Competency in Health Care Important?
A patient’s health beliefs and communication style play critical roles in medical care. The issues of cross-cultural communication and variations in health beliefs impact patient satisfaction and clinical outcomes.
Demographics are changing rapidly throughout the nation and New Mexico. We strive to be at the cutting edge of developments in culturally competent medicine.
Regulatory Requirements for Cultural Competency
Health Care Organizations should: • Ensure that all staff provide patients with effective,
understandable, and respectful care in a manner compatible with their cultural health beliefs and practices and preferred language.
• Implement strategies to recruit, retain, and promote a diverse staff and leadership that are representative of the demographic characteristics of the service area.
• Ensure that all staff receive ongoing education and training in culturally and linguistically appropriate service delivery.
“Health Care Organization” refers to any organization in the health care industry.

• Assure the competence of language assistance provided to limited English proficient patients by interpreters and bilingual staff. Family and friends should not be used to provide interpretation services (unless requested by the patient).
• Make available easily understood patient-related materials and post signage in the languages of the commonly encountered or represented groups in the service area. (However, keep in mind most Navajo don’t read the Navajo language – it is primarily a spoken language.)
Regulatory Requirements for Cultural Competency Health Care Organizations must:
• Offer and provide language assistance services, including bilingual staff and interpreter services, at no cost to each patient with limited English proficiency at all points of contact, in a timely manner, during all hours of operation.
• Provide to patients in their preferred language verbal offers and written notices informing them of their right to receive language assistance services.
As per the Sapir-Whorf hypothesis, language is apart of our cultural understanding and cardinal to creating communication.

Regulatory requirements state that Health Care Organizations must: • Develop, implement, and promote a written strategic plan that outlines clear
goals, policies, operational plans, and management accountability and oversight mechanisms to provide culturally and linguistically appropriate services.
• Conduct initial and ongoing organizational self-assessments of culturally and linguistically-related activities.
• Integrate cultural and linguistic competence-related measures into internal audits, performance improvement programs, patient satisfaction assessments, and outcomes-based evaluations.
• Ensure that data on patients’ race, ethnicity, and spoken and written language are collected in health records, integrated into the organization’s management information systems, and periodically updated.
• Maintain a current demographic, cultural, and epidemiological profile of the community as well as a needs assessment to accurately plan for and implement services that respond to the cultural and linguistic characteristics of the service area.
Regulatory Requirements for Cultural Competency

Health Care Organizations should: • Develop participatory, collaborative partnerships with
communities and use a variety of formal and informal mechanisms to facilitate community and patient involvement for designing and implementing culturally and linguistically related activities.
• Ensure that conflict and grievance resolution processes are culturally and linguistically sensitive and capable of identifying, preventing, and resolving cross-cultural conflicts or complaints by patients.
Regulatory Requirements for Cultural Competency

Working with Diverse Patients To enhance patient-provider communication and to avoid being unintentionally insulting or patronizing, be aware of the following: Styles of Speech • People vary greatly in the length of time between comment and response, the
speed of their speech, and their willingness to interrupt. • Tolerate gaps between questions and answers. Impatience can be seen as a
sign of disrespect. • Listen to the volume and speed of the patient’s speech as well as the content. • Modify your own speech to more closely match that of the patient to make
them more comfortable. • Rapid exchanges, and even interruptions, are a part of some conversational
styles. Don’t be offended if no offense is intended when a patient interrupts you.
• Be aware of your own pattern of interruptions, especially if the patient is older than you.

Working with Diverse Patients
Eye Contact • The way people interpret various types of eye contact is related to
cultural background and life experience. • Most Euro-Americans expect to look people directly in the eyes and
interpret failure to do so as a sign of dishonesty or disrespect. • For many other cultures direct gazing is considered rude or
disrespectful. • Never force a patient to make eye contact with you. • If a patient seems uncomfortable with direct gazes, try sitting next to
him or her instead of across from him or her.

Working with Diverse Patients
Body Language • The way that pain or fear is expressed is closely tied to a person’s
cultural and personal background. • Sociologists say 80% of communication is nonverbal. • The meaning of body language varies greatly by culture, class, gender,
and age. • Follow the patient’s lead on physical distance and touching. • If the patient moves closer to you or touches you, you may do the same.
However, be sensitive to those who do not feel comfortable, and ask permission to touch them.
• Gestures can mean very different things to different people. Be very conservative in your own use of gestures and body language. Ask patients about unknown gestures or reactions. Do not interpret a patient’s feelings or level of pain just from facial expressions.

Working with Diverse Patients
Gently Guide Patient Conversation • English predisposes us to a direct communication style;
however, other languages and cultures differ. Initial greetings can set the tone for the visit.
• Many older people from traditional societies expect to be addressed more formally, no matter how long they have known their physicians.
• If the patient’s preference is not clear, ask how he or she would like to be addressed.

Working with Diverse Patients
Gently Guide Patient Conversation (continued) • Patients from other language or cultural backgrounds may be less likely
to ask questions and more likely to answer questions through narrative than with direct responses.
• Facilitate patient-centered communication by asking open-ended questions whenever possible. Avoid questions that can be answered with “yes” or “no.” Research indicates that when patients, regardless of cultural background, are asked, “Do you understand?” many will answer “yes” even when they really do not understand. This tends to be more common in teens and older patients.
• Steer the patient back to the topic by asking a question that clearly demonstrates that you are listening. Some patients can tell you more about their health through storytelling than by answering direct questions.

Working with Diverse Patients
Nonverbal Communication and Patient Care • Nonverbal communication is a subtle form of
communication that takes place in the initial three seconds after meeting someone for the first time and can continue through the entire interaction. It can impact the success of communication more acutely than the spoken word.
• Based on our cultural background, we unconsciously evaluate gestures, appearance, body language, the face, and how space is used.
• We are rarely aware of how persons from other cultures perceive our nonverbal communication or the subtle cues we have used to assess another person.

Working with Diverse Patients
Nonverbal Communication and Patient Care (continued) • Broad cultural generalizations are used for illustrative purposes. They
should not be mistaken for stereotypes. • A stereotype is an ending point; no attempt is made to learn whether the
individual in question fits the statement. • A generalization is a beginning point; it indicates common trends, but
further information is needed to ascertain whether the statement is appropriate to a particular individual. Generalizations can serve as a guide to be accompanied by individualized, in-person assessments.
• As a rule, ask the patient, rather than assume you know the patient’s needs and wants. If asked, patients will usually share their personal beliefs, practices, and preferences related to prevention, diagnosis, and treatment.

Working with Diverse Patients
Nonverbal Communication and Patient Care (continued) Eye Contact • It is rude to meet and hold eye contact with an elder or
someone in a position of authority such as health professionals in most Latino, Asian, American Indian, and many Arab cultures.
• It may also be considered a form of social aggression if a male insists on meeting and holding eye contact with a female.

Working with Diverse Patients
Nonverbal Communication and Patient Care (continued) Touch and Use of Space • Talk the patient through each exam so that the need for the physical
contact is understood prior to the initiation of the examination. • Ease into the patient’s personal space. If there are any concerns, ask
before entering the three-foot zone. This will help ease the patient’s level of discomfort and avoid any misinterpretation of physical contact.
• Physical contact between a male and female is strictly regulated in many cultures. An older female companion may be necessary during the visit.

Working with Diverse Patients
Nonverbal Communication and Patient Care (continued) Gestures • Gestures have dramatically different meanings across cultures. • Think of gestures as a local dialect familiar only to insiders of
the culture. • Be conservative with hand or body gestures to avoid
misunderstanding. Body Posture and Presentation • Many cultures prioritize and demonstrate family respect in their
manner of dress and presentation in public. • A person’s physical presentation is not an indicator of his or her
economic situation.

Working with Diverse Patients
Nonverbal Communication and Patient Care (continued) Use of Voice • The voice is perhaps one of the most difficult forms of nonverbal
communication to change. • Fast speech may be interpreted as not being interested in the patient. • Too-loud or too-soft speech may be interpreted as domineering or lacking
confidence. • Expectations for use of voice vary greatly among and within cultures,
gender, and age. • Search for nonverbal cues to determine how your voice is affecting your
patient.

Working with Diverse Patients
• Necessary things to keep in mind when planning a health educational activity with a Member:
• Differential abilities are sometimes called learning styles and refer to the various ways people process information.
• These different ways of learning are: • Kinesthetic - movement • Visual - sight • Auditory – hearing / listening

Working with Diverse Patients
• Centennial Care requires that we incorporate this info into health education and health literacy sessions and materials so that we reach a wider audience.
• What does your clinic or office do to accommodate members who are blind?
• Deaf? Speech impaired? Have ADHD? • How will Wheelchair access impact locations for
referrals, lab work, therapy?

Working with Diverse Populations
• Every effort needs to be made to supply resources that address the wide range of knowledge, ability levels, interests, and learning styles members bring with them and that address different instructional strategies.
• Your target audience impacts the health educational activity. So if you only talk about preventing diabetes to a group of diabetics in the final stages will this be effective?

Working with Diverse Patients
Connecting Literacy Rates and Health Care Assess/Use
• National Research illustrates that 75% of individuals with chronic illnesses have low literacy.
• Patients with low literacy rates use the Emergency Room more frequently, have higher admission rates, more costly and prolonged stays
• Populations with the highest prevalence of low literacy rates include: • People over age 75 • People with less than a high school diploma • Certain ethnic groups have lower English proficiency and thus low
literacy rates

Working with Diverse Populations
Connecting Literacy Rates and Health Care Assess/Use
• Target health literacy efforts to the patients below the poverty line: Medicaid, Duals who are Medicaid and Medicare, as well as some Medicare individuals
• We provide AskMe3 for your offices, this is a great tool to help individuals understand the three basic questions they should ask while visiting your offices. Contact Network Services for more brochures.
• You can find more resources and tools at http://www.ahrq.ogv/questionsaretheanswer

New Mexico Diversity Information
New Mexico has a unique history and a topography that includes sweeping landscapes and isolated towns and individuals.
The desert views that are unique to New Mexico, Photos by Sonja Dewing
New Mexico Diversity Information
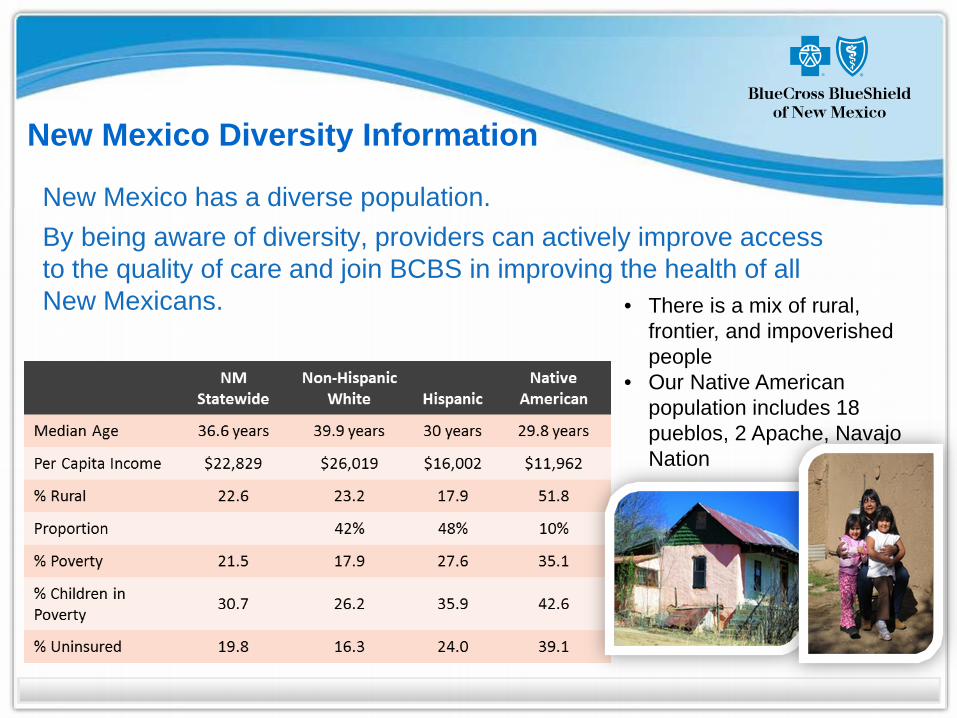
• There is a mix of rural, frontier, and impoverished people
• Our Native American population includes 18 pueblos, 2 Apache, Navajo Nation
New Mexico has a diverse population. By being aware of diversity, providers can actively improve access to the quality of care and join BCBS in improving the health of all New Mexicans.

New Mexico Diversity Information
Different Ways of Thinking
• Patients may be unwilling to share health beliefs or health problems until a safe environment has been created and a trusting relationship has been established. • Consider starting a personal dialogue and making patients and any family
they bring with them to feel welcome and included. • A patient may not be willing to make a decision until they have spoken
with family in a home setting and/or seen an alternative cultural healer.
Note: Although most materials should be made available in predominant languages, Navajo is truly verbal language. Most Navajo don’t read the language, so creating something in writing most likely will not be helpful unless there is someone to read it.

New Mexico Diversity Information
Straight from an experienced provider: LuAnn, Nurse and Medical Director of the Ortiz Mountain Health Center and recently recognized at the University of New Mexico for establishing the health center and her contributions to the many cultures established in the area says: “Don’t make assumptions based on a person’s apparent culture, simply apply a person-centered approach. Treat every person as a unique individual.”

Cultural Diversity in Action
- Do not assume that you know anything about the patient. - Preface your interview with a statement of cultural sensitivity. - Express the importance of respect.
A health care provider interviews a woman who is in need of long term care:
Care Provider: Hello, Ms. Begay, how are you today?
Patient: I feel a bit better today.
Care Provider: “That’s great. Today I will need to ask you some questions regarding your health, diet, and living standards. Before I do these interviews I always like to let the patient know, that I deeply respect all cultures and am going to be as sensitive as possible. These questions are designed to assist me in helping you.” About the photo above: Assumption would lead us to believe that the person in the photo might be from the Asian culture. In fact this woman is 100% Native American from the Inuit Tribe.

Tools
You may wish to mark special areas in your office to help any Limited English Proficient (LEP) patients. English – Welcome Español – Spanish Bienvenido/a Tieáng Vieät – Vietnamese Haân haïnh tieáp ñoùn quyù vò 中 文 – Chinese 歡 迎 English – Registration Español – Spanish Oficina de Registro Tieáng Vieät – Vietnamese QuaÀy tieáp khaách 中 文 – Chinese 登 記 處
English – Enter Español – Spanish Entrada Tieáng Vieät – Vietnamese
Loái vaøo 中 文 – Chinese 入 口 English – Restroom Español – Spanish Baños Tieáng Vieät – Vietnamese
Phoøng veä sinh 中 文 – Chinese 洗 手 間

Tools (continued)
Assessment Sample Questions
D
Demographics – Explore regional background, level of acculturation, age and sex as they influence health care behaviors.
Where were you born? Where was “home” before coming to the U.S.? How long have you lived in the U.S.? What is the patient’s age and sex?
I
Ideas – Ask the patient to explain his/her ideas or concepts of health and illness.
What do you think keeps you healthy/ sick? What do you think is the cause of your illness? Why do you think the problem started?
V
Views of health care treatments – Ask about treatment preference, use of home remedies, and treatment avoidance practices.
Are there any health care procedures that might not be acceptable? Do you use any traditional or home health remedies to improve your health? What have you used before? Have you used alternative healers? Which? What kind of treatment do you think will work?
E Expectations – Ask about what your patient expects from his/her doctor?
What do you hope to achieve from today’s visit? What do you hope to achieve from treatment? Do you find it easier to talk with a male/female? Someone younger/older?
R
Religion – Ask about your patient’s religious and spiritual traditions.
Will religious or spiritual observances affect your ability to follow treatment? How? Do you avoid any particular foods? During the year, do you change your diet in celebration of religious and other holidays?
S
Speech – Identify your patient’s language needs including health literacy levels. Avoid using a family member as an interpreter.
What language do you prefer to speak? Do you need an interpreter? What language do you prefer to read? Are you satisfied with how well you read? Would you prefer printed or spoken instructions?
E
Environment – Identify patient’s home environment and the cultural/diversity aspects that are part of the environment. Home environment includes the patient’s daily schedule, support system, and level of independence.
Do you live alone? How many other people live in your house? Do you have transportation? Who gives you emotional support? Who helps you when you are ill or need help? Can you shop/cook for yourself? When do you usually eat? What is your largest meal of the day?

35 April 2010
General • Diversity RX: Improving health care for a diverse world – http://diversityrx.org • Office of Minority Health – http://minorityhealth.hhs.gov
Includes an online, nine-hour, nine-credit Continuing Medical Educational cultural competence course for providers and office staff
• The Cross Cultural Health Care Program – http://xculture.org • Provider’s Guide to Quality and Culture – http://erc.msh.org • DHHS Office of Civil Rights – http://www.hhs.gov/ocr • Kaiser Family Foundation Minority Health –
http://www.kff.org/minorityhealth/index.cfm • Providing care to diverse populations –
http://archive.ahrq.gov/news/ulp/ulpcultr.htm • AMSA Diversity in Medicine –
http://www.amsa.org/AMSA/Homepage/About/Priorities/Diversity/ CulturalCompetency.aspx
• Video “Cultural Humility: People, Principles and Practices” http://www.youtube.com/watch?v=SaSHLbS1V4w
Tools (continued)

36 April 2010
Aging • Administration on Aging – http://www.aoa.gov • Center on an Aging Society –
http://ihcrp.georgetown.edu/agingsociety African American • National Black Church Initiative – http://www.naltblackchurch.com • NAACP Health Division –
http://www.naacp.org/advocacy/health/index.htm • National Association of Black Cardiologists – http://www.abcardio.org • National Black Nurses Association – http://www.nbna.org • National Caucus and Center on Black Aged, Inc. –
http://www.ncba-aged.org • National Medical Association – http://www.nmanet.org
Tools (continued)

37 April 2010
American Indian/Alaskan Native • Association of American Indian Physicians – http://www.aaip.org • Native American Cancer Research – http://www.natamcancer.org • National Indian Council on Aging – http://www.nicoa.org • National Indian Health Board – http://www.nihb.org
Asian American/ Pacific Islander American • Asian & Pacific Islander American Health Forum – http://www.apiahf.org • Chinese American Medical Society – http://www.camsociety.org • National Asian Pacific Center on Aging – http://www.napca.org • National Asian Women’s Health Organization – http://www.nawho.org • National Resource Center on Native American Aging (Native Hawaiian) –
http://ruralhealth.und.edu/projects/nrcnaa
Tools (continued)
38 April 2010
Hispanic/Latino American • Hispanic Center of Excellence in Medicine –
http://hcoe.medicine.uic.edu • Inter-American College of Physicians and Surgeons –
http://www.icps.org • National Alliance for Hispanic Health – http://www.hispanichealth.org • National Association of Hispanic Nurses –
http://www.thehispanicnurses.org • National Council of La Raza – http://www.nclr.org • National Hispanic Council on Aging – http://www.nhcoa.org • National Hispanic Medical Association – http://www.nhmamd.org
Tools (continued)