emerging and problem analytes in the clinical...
TRANSCRIPT
1
Clinical Pathology Update: Emerging and Problem Analytes
in the Clinical Laboratory
Jay L. Bock, MD, PhD, FCAPSheldon M. Campbell, MD, PhD, FCAP
Peter L. Perrotta, MD, FCAP© College of American Pathologists 2004. Materials are used with the permission
of the faculty.

2
Disclosure
(no commercial relationships to disclose)

3
Agenda
11:50Summary and Closing10:50Microbiology Dr. Campbell
8:30Opening/ Introductions Dr. Bock
10:20Chemistry 2 – hCG Dr. Bock10:00Break9:30Chemistry 1 – CRP Dr. Bock8:35Hematology Dr. Perrotta
TimeTopic

4
“Emerging Analytes”
Hematology & Coagulation Laboratories
Peter L. Perrotta, MDAssistant Professor, Pathology
Stony Brook University

5
Coagulation Sessions
Wed @ 1:30
Tue @ 10:30
Sun @ 1:30
Sun @ 10:30
Date
Hemostasis, Lupus anticoagulantsThe Tipping Point to Thrombosis
vWD, TTP, Anticoagulants, INR
Recent Advances in Hemostasis/Thrombosis
$$$Use & Abuse of FVIIa concentrates
POC CoagCoagulation for Surgical Procedures
TopicsTitle

6
Session Objectives
• Describe newer methods that effectively screen patients for acquired & congenital platelet function defects
• Recognize clinical & laboratory features of heparin-induced thrombocytopenia
• Design & implement a Thrombophilia (hypercoagulable) test “panel”

7
Qualitative Platelet Defects
• Drug effects:ASA, NSAID, clopidogrel
• Congenital defects:GT, BS, SPD
• vWD:vWF essential for platelet adhesion
• Acquired platelet function defect:Uremia, FSP, ET, cardiac surgery

8
Lab Detection of Qualitative Platelet Defects
• Bleeding time• Platelet-rich plasma optical aggregation• Whole-blood impedance aggregation (Chronolog)• Platelet function analyzer (PFA-100®, Dade Behring)• Rapid Platelet Function Assay (Ultegra®, Accumetrics)• Thromboelastography (TEG, Haemoscope)• Multiple platelet function analyzer (Multiplate®)• Plateletworks®

9
Bleeding Time
• Described by Milian (1901)• Introduced by Duke (1910)• Platelet-vessel wall interaction• Influenced by platelet count
and hematocrit• Some sensitivity in acquired
and congenital platelet defects, no specificity
• No correlation between BT and surgical bleeding
Duke WW. JAMA 1910

10
Performing Bleeding Times
40 mmHg
Uremia, hepatic function, skin edema, hypothermia, vasculitis, DM, hyperlipidemia, Ehlers-Danlos
Medications (ASA, NSAID, platelet inhibitors, antibiotics, valproic acid, ethanol, garlic, ginkgo, ginger, ginseng
Platelet disorders, anemia, vWD, factor deficiencies (VIII, IX, V), hypofibrinogenemia, MPD, paraproteinemias
Blot q 15s
Normal < 7 min.

11
Impact of Discontinuing Bleeding Times
Clinicians report• No change in pre-procedure work-ups• No postponing of invasive procedures• No increase in bleeding complications
Objective measurements• No increase in blood product use• No increase in platelet aggregation studies• No increase in DDAVP administration• No increase in post-procedure bleeding
complications (major surgical risk cases and renal biopsies)
University of Utah, Clin Chem, 2001;47:1204

12
Platelet Function Analyzer (PFA-100)
• In vitro test of platelet function using anticoagulated whole blood
• Based on principle of Thrombostat 4000 (Germany)
• Prototype field-tested in 1995 (Sem ThrombHem 1995:21:113)
• Uses 0.45um nitrocellulose filtration membrane coated with 2 ug collagen (CEPI) and either 10ug epinephrine or 50ug ADP (CADP)
• Subjected to shear rate of 5000-6000s-1

13
How the PFA-100 WorksCol-Epi
Col-ADP
Closure time (sec)
147um

14
Preferable Lab Tests
24/7LimitedAvailability
LowHighTechnical difficulty
YesNoAutomated/Rapid
SoonNo (no sample)Proficiency
Electronic/?LiquidNoControls
Yes (CV<10%)Resident: No
Lab: ? CV 20-25%Reproducible
PFA-100Bleeding Time

15
Reference Range Determination and Validation of PFA
Method• Confirmed manufacturer’s suggested reference
range using 20 individuals• Confirmed response following 325 mg ASA• NO back-to-back testing with bleeding time• Limited back-to-back with PRP aggregation
Collagen/EPI [82-150 sec]Collagen/ADP [62-100 sec]

16
Historical back-to-back comparisons with bleeding time
0
0.2
0.4
0.6
0.8
1
0 0.2 0.4 0.6 0.8 1
BTPFA
Receiver/operator characteristic (ROC) curves which reflect combined sensitivity and specificity:
-99 “Normals” by consensus
-70 Abnormals (24 ASA, others)
Sem Thromb Hem 1995:21(2)
AUC BT = 0.698
AUC PFA = 0.89
1-Specificity
Sens
itivi
ty

17
Historical back-to-back comparisons with PRP aggregation
88
100 (A.A)
80%
NA
Sensitivity PRP Agg
NT95-98%127ASA
NT94176All Abnormals
5
44
206
n
100%
96%
NA
Sensitivity CEPI PFA
100%
59%
NA
Sensitivity BT
Glanzmann
vWD
Normal
Condition
Sem Thromb Hem 1998;24:2
18
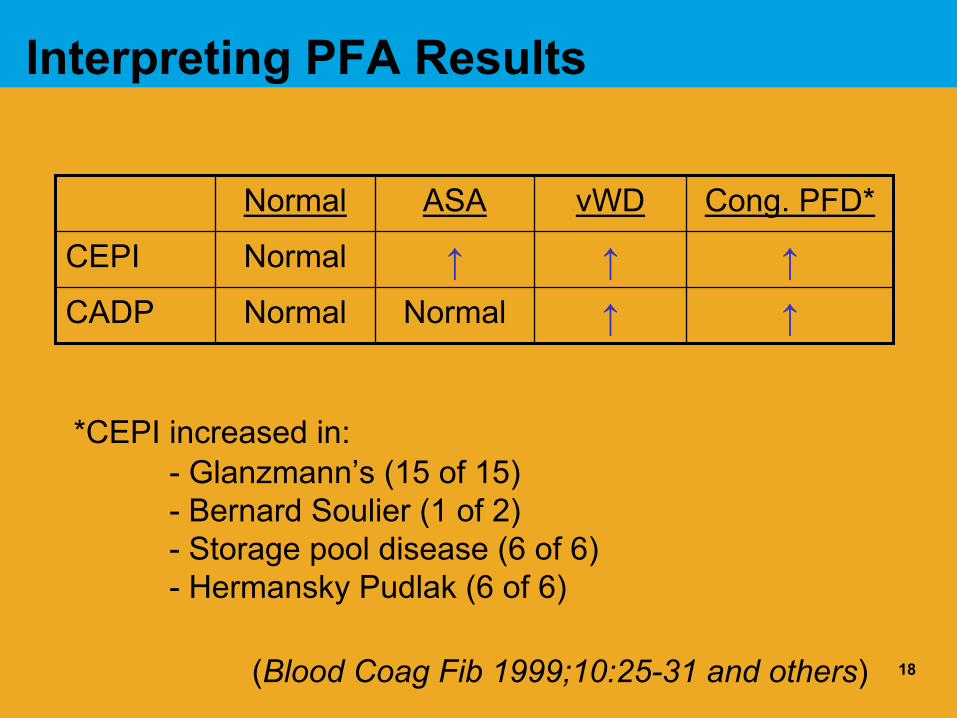
Interpreting PFA Results
↑↑NormalNormalCADP↑↑↑NormalCEPI
Cong. PFD*vWDASANormal
*CEPI increased in:- Glanzmann’s (15 of 15) - Bernard Soulier (1 of 2)- Storage pool disease (6 of 6)- Hermansky Pudlak (6 of 6)
(Blood Coag Fib 1999;10:25-31 and others)

19
PFA in vWD• Majority of patients with vWD will have abnormal CEPI and
CADP• If BT is long in vWD patient, CEPI will be long• CEPI could be normal in very mild type I or type 2N patients
with normal BT (Thromb Res 1999;96:487)• Probably useful in monitoring response of type I vWD to
DDAVP (Br J Haem 1999;106:777)
Blood 1998;91:1325

20
PFA in Cirrhosis & Uremia
• Study of 20 controls, 21 uremics, 20 cirrhotics
• Test subjects had lower Hcts(26%) and platelet counts (140K) and abnormal PRP aggregation
• CTs straddled upper limit of normal
• Fell into normal range when Hct was elevated by adding RBCs to sample
Haematologica 1999;84:1999
Interpret! Don’t just look at the flag

21
PFA in Neonates/Pediatrics
• No difference between 21- and 23-gauge needles or between vacutainer and syringe draws
• Children (age 2-17): Normal range similar to adults (? 5-10% lower CEPI CT)
• Newborns: Using cord blood results 25-35% shorter than adults, CEPI 61-108 sec CADP 48-65 sec (SemThromb Hem 1998;24:523)
Related to higher Hcts, WBCs, vWF, increased high weight multimers in neonates
• Not affected by factor VIII and IX levels
We run both CEPI and CADP cartridges in children
22
Monitoring for ASA “Resistance”
• Anti-platelet effects of ASA may vary in patients with ischemic stroke (Helgason et al. Stroke 1994)
• ASA resistance associated with increased risk of MI or CVI (Gum et al. J Am Coll Cad 2003)
• ASA resistance associated with increased risk myonecrosis after non-urgent PCI (Chen et al. J Am CollCard 2004)
• PFA can Identify “ASA resistant” patients (Am J Cardiol2001;88:230)
• Ultegra® Rapid Platelet Function Assay-ASA can detect ASA resistance (accumetrics.com)
• RPFA can be used to monitor abciximab therapy in PIC (POC setting)
Do you need to monitor ASA therapy ?Do you need to monitor ASA therapy ?

23
QA for PFA
• Each cartridge is self-contained
• Control donor in duplicate with each new cartridge lot or when performance is suspect
• If this donor is out of reference range, check another donor
• If 2nd also outside range, send instrument back
• Electronic instrument check before each run• Unexpected results reviewed by medical personnel• Check platelet count, platelet histogram, Hg if sample
integrity is suspect

24
PFA Tidbits
• PFA not influenced by heparin• PPACK O.K. as anticoagulant• Slightly or not prolonged in afibrinogenemia• Group O patients with lower vWF:Ag have
slightly longer (10-20%) CEPI closure times• Decreased when ESR is high (Sepsis)• Pregnant women: CT 20% shorter, shortest in
2nd trimester• Otherwise independent of gender, OC use,
smoking, or fibrinogen levels

25
PFA Tidbits, continued• Can detect δ-storage pool disease with CEPI CT
despite normal PRP aggregation (Thromb Res1999;96:213)
• Cannot detect GP Ia 807 C/C polymorphisms associated with low collagen receptor density butmild Type I vWD and polymorph have longer CT (Thromb Res 2001;103:123)
• 807 T/T with high collagen receptor density have shortest CT and respond poorly to ASA
• Check functionality of platelets from repeat platelet donors (Thromb Haem 2001;86:880)
• Decreased CEPI CT in trauma patients with activated platelets (J Trauma 2001;51:63)
• COX-2 inhibitors that inhibit TxB2 production < COX-1 inhibitors increase CT only 10%

26
Algorithm for Platelet Function Screening
Bleeding History*
Pre-surgery with Fam Hx PFD
Drug History
Vitamins
Health Foods
vWD Testing
PRP Aggregation
+/- Flow cytometry
PFA CEPI
PFA CADP
STOPNo
Normal
Normal
AdultSTOP
Abnormal
Abnormal

27
PFA Illustrative Case?
• 70 yoM post-MI and post-stenting• Meds: ASA & heparin• Labs: WBC = 14 K/uL Plt = 40 K/uL Hct = 31%,
PT= 13.3 sec, aPTT = 60 sec• Needs surgery: Order PFA to check platelet function:
PFA Collagen/EPI = >300 sec [82 – 150 sec]PFA Collagen/ADP = 151 sec [62 – 100 sec]
What is your interpretation?

28
Heparin Started
PFA Orders

29
Heparin Induced Thrombocytopenia (HIT)
• First described? Natelson et al, Ann Intern Med 1969• Common: 1% to 5% of patients exposed to heparin• Estimated 1/3 of patients with HIT develop thrombosis (HITTS),
of which 1/3 will have amputation or die
Clinically - Thrombocytopenia with or without:• DVT, PE, cerebral venous thrombosis• Coumarin-induced venous limb gangrene• Arterial thrombosis: Lower-limb, cerebral, MI, etc.• Skin lesions at heparin injection• Skin necrosis, erythrematous plaques• DIC• Acute systemic reaction post heparin bolus

30
Type I -vs- Type II HIT
Type I HIT• Mild thrombocytopenia (100-
150 x 109/L• Rapid onset (1-2 days)• Resolves despite
continuation of heparin• Asymptomatic• Non-immune mechanism ?
Via GPIIb/IIIa and ADP
Type II HIT• Severe thrombocytopenia
(<100 x 109/L)• Delayed onset (4-14 days)• Persists until heparin is
discontinued
• Thromboembolic complications
• Immune mechanism
Chong et al, 2003

31
Platelet Nadir in HIT (n=127, serologic confirmed)
Warkentin & Kelton, Am J Med 1996
59

32
Laboratory Testing for HITFUNCTIONAL TESTS• Serotonin release assay (SRA)• Heparin-induced platelet aggregation (HIPA)• ATP release by lumiaggregation• Microparticle release by flow cytometry• Annexin V binding & P-selectin expression by flow
cytometry
IMMUNOASSAYS• Solid-phase anti-PF4/heparin ELISA• PF4-polyvinylsulfonate antigen ELISA• Fluid-phase anti-PF4/heparin EIA• Particle gel immunoassay (Diamed)
Adapted from Chong, ISTH, 2003

33
Structure of Heparin“BIG & negatively charged”
• Molecular weight: 5,000 to 30,000 daltons• Structure: Long, unbranched polysaccharide
chains of repeating disacharide units, highly sulfated
• Source: Bovine lung more likely to cause HIT than porcine mucosa
• Low molecular weight heparin (LMWH): Prepared from unfractionated heparin, MW about 5,000 daltons

34
Heparin-PF4 Interaction with Platelets
Heparin-PF4-Antibody Complex
Thromboxane Synthesis
Platelet Granule Release
Microparticle Formation
Platelet aggregation
Activated Platelet
Adapted from Chong & Eisbacher, 1998
FcγRII
*Thrombin GenerationResting
Platelet

35

36
Morphological and immunohistochemical characteristics of heparin-induced thrombi and thrombi of other origin
Adapted from Hermanns et al, Virch Arch 1998
White to grey to grey-redWhitishColor
(+)++ to +++IgG/IgM content
+++(+)Fibrin Content
Thrombocytes, RBCs, leukocytes, few lymphs
ThrombocytesCell Content
Fibrin webbingWide-meshed patternLayerlike structure
Structure
Other thrombiHIT ThrombiFeature

37
Pre-test Probability of HIT
Platelet count starts increasing 2 days after stopping heparin

38
SRA to detect HIT Antibodies“Gold Standard” in HIT antibody detection credited to
Sheridan et al, Blood 1986
• Based on immune-mediated 14C-serotonin release from platelet dense granules with activation
• Procedure1. Donor PRP is prepared, washed, and incubated with 14C-serotonin2. Incubate platelets with heat-treated patient serum and two concentrations heparin (0.1-0.4 U/mL and 100 U/mL)3. Spin to pellet platelets, measure radioactivity in supernatant4. Positive when >20% release with low dose heparin and <20% release with high dose heparin
• Disadvantages- Time-consuming- Biohazardous radioisotopes- Dependent on donor platelets like the HIPA

39
PF4-Heparin ELISA Is Easier
*GTI: PF4 from outdated platelets and polyvinyl sulphonate
*Asserachrom, Stago: recombinant PF4 and heparin
PF4 Heparin
HIT Antibody (IgG, IgA, IgM
Enzyme linked Goat anti-Human IgG,A,M

40
Sensitivities of Various HIT Assays
High>90%ELISA
High50-80%HIPA
High>90%SRA
SpecificitySensitivityAssay

41
Local validation of HIT ELISA Assay
• 4 positive by SRA & ELISA: Good Hx• 11 negative by SRA & ELISA: Poor Hx (includes ITP
and lupus anticoagulant)• 4 positive by ELISA but negative by SRA: All had
good Hx including (a) Pt dropped plt count on heparin re-exposure, (b) 2 had clinical HIT per hematologists, (c) one had a leg amputation
• 2 cases negative by ELISA but positive by SRA: One had good Hx and other not HIT
Can we institute this assay?

42
Reporting of HIT ELISA Results
Other test outcomes• Positive: Consistent with heparin-associated antibody in
appropriate clinical setting • Negative: No evidence of heparin-associated antibody by ELISA
technique. Reactivity in presence of excess heparin more consistent with anti-platelet factor 4 antibody
• Indeterminate result: Cannot demonstrate or exclude a heparin-associated antibody. Suggest repeat testing in 2-3 days or testing by another technique if clinically indicated.

43
Our Strategy for HIT Testing
• Clinically suspected HIT: HIT ELISA is performed as the first-line assay
• Expect to detect > 90% of HIT antibodies• If ELISA negative but clinical suspicion high, then
repeat ELISA in 24-72 hours• If repeat negative and suspicion high, then
perform serotonin release assay• Performed weekdays• Positives are “Critical Values”• Pharmacy informed of positives: “Allergy”
*Negative HIT test does not exclude HIT**Negative HIT test does not exclude HIT*

44
Treating HIT (stopping heparin may not be enough)
• LMW Heparin: Not recommended because of high cross-reactivity(80-90%) in vitro
• Danaparoid (Orgaran): Heparinoid compound related to LMW heparin. Approx. 10-20% HIT cross-reactive
• Anti-platelet agents: No proven role• High dose IVIG: 3 of 3 patients responded, consider in severe
cases• Plasma exchange: ??
• Direct thrombin inhibitors: Neutralize excess thrombin generated in HIT- Lepirudin (Refludan, recombinant hirudin): - Argatroban (small-molecule, direct thrombin inhibitor)

45
Direct Thrombin Inhibitors

46
HIT & Cardiac Surgery
(IIb/IIIa)
(prostacyclin)
Warkentin, Ann Thorac Surg 2003

47
Is this a HIT Case?
• 40 yoM post CVI• Meds: Received heparin & abciximab (Reopro)• 8 hours after CVI, platelet count was 2 K/uL and
patient bleeding at venous site
• Request for STAT HIT ELISA denied• Responded to platelet transfusions
48
Questions in Thrombophilic Testing?
• Why test?• Who should be “screened”?• When should tests be performed?• What are physicians doing at your
hospital?• What tests should comprise a
hypercoagulable “panel”?

49
Stages of Laboratory TestingPre-analytical• Patient selection (pre-test probability of disease)• Test selection (order, order entry, Clinicians want
help!)• Sample collection (anticoagulants, line draws, active
thrombosis)Analytical• Method (limitations)Post-analytical• Result reporting• Result interpretation• Action taken based on result (bias)

50
Why Test for Thrombophilia?
• Conditions have been identified that carry an increased risk for thrombosis
• Tests are more readily available (Bias toward ordering tests)
• Test results influence decisions on1) Therapy (anticoagulation choice, duration, intensity)2) Prevention (prophylaxis during surgery, pregnancy, etc.)3) Relative risk of thrombosis (counseling)

51
Conditions Associated with Venous Thromboembolism
Congenital• AT deficiency• PC deficiency• PS deficiency• FV Leiden• PT G20210A• Hyperhomocyteinemia• Dysfibrinogenemia
Acquired/Mixed• Anti-phospholipid
antibodies• Hyperhomocyteinemia 20
vitamin deficiency• APC resistance• Increased factor VIII (IX,
XI, fibrinogen, TAFI)
Rare, but strong associationCommon, but weak association

52
Hereditary Predisposing Conditions
20 – 505 (Caucasian)APC resistance
10 – 255 - 10Hyperhomocysteinemia
62PT G20210A mutation
2 – 80.7PS deficiency
3 - 90.14 - 0.50PC deficiency
1 - 50.17AT deficiency
Prevalence venous thrombosis (%)
Prevalence general population (%)
Disorder
Hematol Oncol Clin North Am, 1998

53
Who Should be “Screened”?
• Screening general population not justified (cost to avoid 1 thrombotic event too high)
• Unexplained thromboembolism at any age
• Age <50 with or without predisposing conditions (surgery, immobilization, trauma, malignancy, OCs, pregnancy, etc.
• First-degree relatives of patients with thrombosis & documented abnormality

54
When Should Thrombophila Testing be Performed?
• Test results typically don’t affect initial management• Acute thrombosis +/- anticoagulation therapy affect
several plasma-based assays- AT assays affected by heparin- PC and PS assays affected by Coumadin- AT, PC, PS affected by acute thrombosis
IdeallyWait 2 weeks once anticoagulants stopped to run these testsPerform tests 6 months after acute episode (inflammation and fibrinolysis subsides)

55
Tests Performed at SB
24Send out to ARUPLp(a)
178178
DNA (Molecular Diagnostics)DNA
FV LeidenPT gene mutation
30 (70)134
13, 83
RVVCT (Phospholipid dependence)ELISA (Immunology)Coag, dilute PT
LA screen (confirm)ACA (IgG + IgM)PT, TTI
110Clotting using FVIII def. plasmaFactor VIII
144Serum immunoassay (Chemistry)Homocysteine
1948282
APC cofactor activity of PC (PT based)ELISAELISA
PS activityPS total AgPS free Ag
22467
Amidolytic using venom activatorELISA
PC activityPC antigen
11073
Heparin cofactor Xa inactivationELISA
AT activityAT antigen
Cost ($)MethodTest

56
Review of Thrombophilia Evaluations at SB (n=30)
< 30 mg/dL16Lp(a)5-15 uM/L017Homocysteine
00
1754
FVLPT gene
Both
IgG<15, IgM<12.52
1/31320
LACSACA (IgG/IgM)
82-151% (F=64-138%)Free: 67-151% (F=51-131%)Total: 72-152% (F=60-136%)
33 free0 total
2013
9
PS activityPS free+total
Both
65-122%76-158%
34
22139
PC activityPC antigen
Both
85-130%191-369%
00
2075
AT activityAT antigen
Both
Reference rangeAbnormalPerformedTest

57
Hypercoagulable Test Panel
Potential benefits• Standardize test ordering practices• Facilitate ordering in LIS• Maximize chance of identifying an abnormality• Detect combined abnormalities• Decrease need to redraw for additional tests• Algorithms not helpful as in bleeding patient
Drawbacks• Will increase overall costs• Questionable cost/benefit ratio• Label patients inappropriately as “clotters”• Regulatory aspects of “bundling” tests

58
What Panels do Popular Reference Labs Offer?
ARUP• Acquired: PT, PTT, mix, dRVVT, ACA, d-dimer• Inherited: PTT, FVIII, Homocyst, PVL, APCR, PT gene• Uncommon: PT, PTT, PC activity, AT activity, PS
(free+total)
MGH• Hypercoag: APCR, FVL, ACA, AT, CRP, Homocyst,
Lp(a), plasminogen, PAI-1, platelet hyperaggregation, PC, PS, PT gene, reptilase time, thrombin time
Tricore• Hypercoag: AT, PC activ, PS activ, lupus panel, ACA,
homocyst, FVL, PT gene

59
Reference Lab Offerings (continued)
University Vermont• On warfarin: PT, PTT, dRVVT, ACA, TT, AT, FVL, homocyst• No warfarin: dRVVT, ACA, TT, AT, APCR (FVL if abnormal),
homocyst, PC activity (Ag if low), PS activ (Ags if low)
University of Florida• If PC low, reflex to FVII to exclude liver disease, vit. K def.• If PS low, reflex to FVIII to exclude acute phase reactant• If homocyst high, reflex to MTHFR gene mutation
Blood Center Milwaukee• Thrombosis: AT activ., PC activ, PS activ, lupus panel, ACA, FVL,
PT gene• On warfarin: ACA, AT activity, FVL, LA, PC Ag + FX Ag, Free+total
PS Ag, PT gene

60
Our Thrombophilia Panel• Antithrombin activity (reflex to antigen if low)• Protein C activity (reflex to antigen if low)• Protein S activity (reflex to free/total antigen if low)
• Lupus anticoagulant screen (confirmatory step in positive)
• Anticardiolipin antibodies (IgG & IgM)
• Factor V Leiden R506Q mutation• Prothrombin nucleotide 20210A mutation
• Homocysteine (total after 12 hour fast) TOTAL
Should requests for hypercoag panels be screened?Should an interpretive report be provided?
Need better screening test for overall thrombotic potential?

61
Pearls of Pathology (Summary)
• There are in vitro laboratory tests and POC instruments that are effective alternatives to the bleeding time
• Laboratory assays are helpful in confirming a clinical diagnosis of HIT
• “Panels” provide a more comprehensive approach to thrombophilia testing

62
C-reactive protein in coronary risk assessment—a better test than cholesterol?
Jay L. Bock, MD, PhDDepartment of PathologyStony Brook University

63
Objectives
• Consider the characteristics that may make a test useful for the evaluation of cardiac risk
• Summarize the biology of CRP and the evidence relating it to coronary heart disease
• Evaluate high-sensitivity CRP as a test for cardiac risk

64
Study Says a Protein May Be Better Than Cholesterol in Predicting Heart Disease RiskBy DENISE GRADY
n inexpensive blood test for a protein linked to artery disease may be better than a cholesterol test at predicting a person's risk for a heart attack or stroke, researchers are reporting today.
New York Times, November 14, 2002

65
“Supportive but not conclusive research shows that eating 1.5 ounces per day of walnuts as part of a diet low in saturated
fat and cholesterol may reduce the risk of heart
disease.”New York Times, March 28, 2004

Physical InactivityPhysical Inactivity
AgeGender
Family History
Smoking
Hypertension
Diabetes MellitusObesity
CholesterolHDL
LDL
TriglycerideLp(a)
Homocyst(e)ineB12
B6
folate
Fibrinogen
PlateletsFactors II, V, ...
IronOxidants
Anti-oxidantsRed wine
Flavonoids
Alcohol
AggressivenessDepression
InsulinTWARCMV
CRP
Fiber
VegetablesSat. fat
Total fat
Unsat. fat
trans-FA
fish oil
apolipoproteins
vit. Cvit. E
carotenoids
Anxiety Cortisol
IL6aspirin

67
What is a risk factor?
• How do you define risk?• Is high risk a disease?• How do you know if a risk assessment
is accurate?• What do you do about it?

68
Risk factors may be ...
• Causes• Consequences• Associations

Clinical reasons for measuring risk factors
• Allow individuals to know their risk• Encourage lifestyle improvements• Undertake and monitor preventive measures
– before clinical disease (primary prevention)– after clinical disease (secondary prevention)
• Make decisions regarding acute treatment

70
Lines of evidence
• Involvement in the disease mechanism• Animal studies• Uniform occurrence of the disease
when the risk factor is very high• Epidemiology studies• Controlled intervention studies

71
The classic example
• Involvement in the disease mechanism
• Animal studies • Uniform occurrence of the disease when
the risk factor is very high • Epidemiology studies • Controlled intervention studies
Serum cholesterol (or LDL cholesterol)

72
A change in paradigm
• Old paradigm: coronary risk relates to the degree of obstruction– Gold standard test: coronary angiography– “Cure:” bypass, angioplasty, stent
• New paradigm: risk relates to plaque vulnerability– Acute coronary syndromes are due to erosion or
rupture of unstable plaques– How to test?– How to cure?
73
C-Reactive Protein (CRP)
• First described in 1930 - fraction of plasma protein from infected patients that reacted with the C-polysaccharide of pneumococcus
• Also found in patients with other acute illnesses (including acute coronary syndrome) - hence the term “acute phase reactant.”

74
Biochemistry• Pentameric protein: five protomers, each of
206 amino acids, arranged in cyclic symmetry (pentraxin family)
• Binds various proteins and phospholipids, particularly phosphocholine. Ca2+ ions ligate the phosphate group and a hydrophobic pocket accommodates the methyl groups of phosphocholine.
• Opsonizes particles and also activates complement via the classical pathway. Actual biological function unknown.

75
Pathophysiology
• Normal plasma levels: median ~1 mg/L, 99th percentile is ~10 mg/L
• Synthesized in hepatocytes. In acute illness, cytokines stimulate hepatic productions, levels rise rapidly to as high as 300 mg/L in 24 hr.
• Increased in many disorders, including bacterial (but usually not viral) infections

76
Epidemiology Studies
• Study of 22,000 healthy male physicians to examine effect of beta-carotene and aspirin. 543 who developed MI or stroke were compared to 543 controls.
• CRP higher in those who had MI (1.51 mg/L) or stroke (1.26) versus control (1.13)
• Three-fold higher risk of MI in highest quartile. Risk was stable over time and independent of other factors.
• Aspirin reduced risk of those in the highest quartile.
Ridker et al., NEJM 1997;336:973-9
PhysiciansHealth Study

77
0
1
2
3
4
5
Rel
ativ
e R
isk
of M
I
1 2 3 4Quartile of CRP
PlaceboAspirin
Ridker et al., NEJM 1997;336:973-9

78
[PM Ridker, Circulation 2003;107:363-9; NEJM 2002; 347:1557]

79
[PM Ridker, Circulation 2003;107:363-9; NEJM 2002; 347:1557]

80
[PM Ridker, Circulation 2003;107:363-9; NEJM 2002; 347:1557]

81
Risk of recurrent events
0
0.5
1
1.5
2
<1.2 1.2-2.0 2.1-3.7 3.8-6.6 >6.6CRP, mg/L
0
0.5
1
1.5
2
<1.7 1.7-2.3 2.4-3.4 3.5-5.9 >5.9SAA, mg/L
Ridker, Circulation 1998;98:839-844

82
HEALTH & FITNESS | April 6, 2004, Tuesday
Heart Study Challenges Protein's Predictive Power
By ANAHAD O'CONNOR (NYT) words Late Edition - Final , Section F , Page 8 , Column 5
83
[Danesh et al., C-Reactive Protein and Other Circulating Markers of Inflammation in the Prediction of Coronary Heart Disease, NEJM 2004; 350:1387-97].

84
[Danesh et al., C-Reactive Protein and Other Circulating Markers of Inflammation in the Prediction of Coronary Heart Disease, NEJM 2004; 350:1387-97].

85
[Danesh et al., C-Reactive Protein and Other Circulating Markers of Inflammation in the Prediction of Coronary Heart Disease, NEJM 2004; 350:1387-97].

86
Other lines of evidence
• Is CRP involved in the atherosclerotic process?– Inflammation appears to play an important role in CHD– CRP has been identified in coronary plaque– But why is there the association between CRP and
CHD?• CHD may cause an inflammatory response which causes CRP
elevation• A chronic state of inflammation may cause or exacerbate CHD• CRP itself could cause or exacerbate the atherosclerotic
process

87
[Lagrand, Circulation 100:96, 1999]

88
Summary of CRP evidence
• Involvement in the disease mechanism • Animal studies ±• Uniform occurrence of the disease when the
risk factor is very high ±• Epidemiology studies • Controlled intervention studies

89
Clinical Guidelines
• Cholesterol/lipids– 1988 – ATP-I– 1993 – ATP-II– 2001 – ATP-III
• CRP– 2003 – AHA/CDC Scientific Statement
(Pearson et al., Circulation 2003;107:499-511)

90
2003 AHA/CDC Scientific Statement
• Current evidence supports the use of hs-CRP as the analyte of choice [if inflammatory markers are to be used].
• The hs-CRP assay should be performed in a metabolically stable person without obvious inflammatory or infectious conditions. Two assays, optimally 2 weeks apart, are recommended.
• Patients without known CHD and at intermediate risk (ie, 10-20% over 10 years) may benefit from measurement of hs-CRP.
• The entire adult population should not be screened.

91
Risk stratification
• Low: <1.0 mg/L• Average: 1.0 – 3.0 mg/L• High: >3.0 mg/L

92

93
Summary / Pearls of Pathology
• Epidemiology studies have consistently shown an association of CRP with coronary risk, independent of other established risk factors
• The magnitude of the risk association is moderate• The role of CRP in coronary disease is unclear• Treatment specifically directed to high CRP is not
available• Current guidelines suggest testing is most useful in
those at intermediate risk based on established factors

94
Summary / Pearls of Pathology
“‘It’s not clear exactly yet which patients need CRP screening,’ says Dr. Robert Bonow, president of the American Heart Association.”
Newsweek June 16, 2003, p. 50

95
False-positive, “discordant”, “phantom”, “low-level ‘real’ ”, and other confusing results of hCG assays
Jay L. Bock, MD, PhDDepartment of PathologyStony Brook University

96
Objectives
• Many instances are known where incorrect or misleading results of hCG assays have led to patient harm. – Understand the causes– Know the solutions

97
Case 1 - 1982
A 23-year-old woman presented with amenorrhea and had a positive, qualitative serum hCG test. The test was done by a competitive-binding, radiolabeled procedure (RIA) and was reproducible on subsequent specimens. She eventually had both uterine curettage and an exploratory laparotomy, with no fetal or placental tissue found. The positive hCG test persisted after these procedures. A different brand of hCG RIA test was performed, and it gave a negative result.

98
Case 1 - explanation
The RIA method that gave a positive result used a goat anti-hCG antibody, whereas the kit that gave a negative result used a rabbit antibody. It was shown that the patient’s serum contained antibodies that bound to goat IgG but not rabbit IgG.AO Vladutiu, JM Sulewski, KA Pudlak, CG Stull. Heterophilic antibodies interfering with radioimmunoassay: a false-postivie pregnancy test. JAMA 1982;248:2489-90

Polyclonal Ab
Protein analyte
Labeled protein

Heterophilic Ab

101
Case 2 - 1985A 28-year-old woman presented to the emergency room with abdominal pain. A quantitative serum hCG test, performed using the newly released Hybritech Tandem-E® double-monoclonal immunoenzymometric assay (IEMA) gave a positive result of 32 mIU/mL. Uterine curettage and laparoscopy were eventually performed, with no fetal or placental tissue found. The quantitative hCG result persisted in the range of 32-55 mIU/mL. When specimens were tested using an older β-subunit RIA, results were negative.

102
Case 2 - explanationThe positive result in the Tandem-E assay was diminished by adding goat anti-(human IgM) to the specimen, and was abolished by adding nonspecific mouse IgG to the specimen.It was therefore attributed to heterophilic antibodies (HAMA) in the patient’s serum.
JL Bock, J Furgiuele, B Wenz. False positive immunometric assays caused by anti-immunoglobulin antibodies: a case report. Clin ChimActa 1985;147:241-6.

solid phase
Capture Ab (monoclonal conjugated to solid phase)
Detector Ab (labeled monoclonal)
Protein analyte

solid phase
HAMA

105
Case 3 - 2001A 22-year-old went to her doctor because of irregular menses. A serum hCG test, done by an IEMA method on the Abbot Axsym® analyzer, was positive. There was no other evidence of pregnancy, but the hCG test was consistently positive. She was referred to an oncologist who instituted chemotherapy to cover the possibility of a trophoblastic tumor. The elevated hCG level persisted. She eventually had a hysterectomy and additional surgery before it was found that her hCG level, using other brands of test, was negative.
106
[see: http://abcnews.go.com/sections/primetime/2020/PRIMETIME_010726_abbott_feature.html]

107
Myth
• A “positive” hCG test means the patient is pregnant—if it’s not an intrauterine pregnancy, it’s likely an ectopic pregnancy, and if it’s not either of those—it’s likely cancer!

108
Reality
• hCG tests can be positive for a number of reasons. Some simple follow-up measures can often rule out pregnancy or cancer as the cause.

109
Basic facts
• Choriogonadotropin (CG, or hCG) is a member of the glycoprotein hormone (GPH) family (other members are the pituitary hormones LH, FSH, and TSH).
• The GPH’s are heterodimers, each sharing the same α-subunit and having a distinctive β-subunit.
• Plasma hCG rises exponentially in the early first trimester of pregnancy, peaks at 8-10 weeks, then gradually declines

110
hCG assays
• Modern hCG assays are all immunoassays• They have progressed from:
– competitive-binding assays using polyclonal Ab’sagainst the whole molecule
– to competitive assays using Ab’s specific for β-subunit
– to immunometric assays using monoclonals that can have varying molecular specificities.The term “β-subunit assay” is obsolete and should not be used.
• Results generally reported in mIU/mL, relative to the 3rd/4th IS, which is a relatively pure preparation of intact hCG

111
Causes of false-positive, “discordant”, “phantom”,
“low-level ‘real’ ”, and other confusing results of hCG
assays

112
Causes of hCG results that are misleading, discrepant, spurious, …
• 10. Laboratory error– Pre- or post-analytical (specimen mix-up,
etc.)– Analytical
• Reading difficulty with a qualitative test• Specimen carryover• Hook effect

113
Causes of hCG results that are misleading, discrepant, spurious, …
• 9. Cross-reactivity– Other GPH’s, especially LH, have similar
structure– But with modern assays this problem is
usually insignificant.

114
Causes of hCG results that are misleading, discrepant, spurious, …
• 8. Molecular heterogeneity
Less of a problem now that standard materials are highly purified. But different commercial kits will react differently with the different forms of CG, which include:
– Intact dimer– Free subunits– Cleaved forms (β-core fragment)– Nicked– Hypo- or hyperglycosylated


116
Causes of hCG results that are misleading, discrepant, spurious, …
7. Persistent levels from an earlier pregnancy
Half-time for disappearance is fairly long (~24 h), so measurable levels can persist for weeks in the absence of complications

117
Causes of hCG results that are misleading, discrepant, spurious, …
6. Early (“micro”) abortion

118
[see: Wilcox, NEJM 1988; 319:189-94]

119
Causes of hCG results that are misleading, discrepant, spurious, …
5. Administration of hCG as a drug
see Karoshi, Lancet January 4, 2004; 363:362. (“I recently learnt a lesson that I will never forget …”)

120
Causes of hCG results that are misleading, discrepant, spurious, …
4. An ectopic pregnancy may secrete little or no measurable hCG
see: Lonky NM, Sauer MV. Ectopic pregnancy with shock and undetectable β-human chorionic gonadotropin: a case report. J Reprod Med 1987; 32:559-560. Taylor RN, Padula C, Goldsmith PC. Pitfall in the diagnosis of ectopic pregnancy: immunocytochemical evaluation in a patient with false-negative serum β-hCG levels. Obstet Gynecol 1988; 71:1035-1038.
121
Causes of hCG results that are misleading, discrepant, spurious, …
3. A finite amount of hCG is normally present in male and female serum
Probably derives mainly from the pituitary

122
[see: Odell & Griffin, NEJM 1987; 317:1688-91.]

123
[see: Odell & Griffin, NEJM 1987; 317:1688-91.]

124
Causes of hCG results that are misleading, discrepant, spurious, …
2. Interfering antibodiesHeterophilic Ab’s may arise due to animal exposure, treatment with mAbdrugs, or for no apparent causeA problem for all immunoassays

125
[see: Cole, Gynecologic Oncology, 1998;71:325-329; Lancet 2000; 355:712-15, Clinical Biochemistry 2004; 37:344-349]

126
Causes of hCG results that are misleading, discrepant, spurious, …
• 1. “Low-level real” hCG

127
[see: Kohorn, Gynecologic Oncology 2002; 85:315-20; Cole, Am J Obstet Gynecol2003; 188:1254-9]

128
[see: Kohorn, Gynecologic Oncology 2002; 85:315-20; Cole, Am J Obstet Gynecol2003; 188:1254-9]

129
“Low-level real” hCG
• Persistent low-level results, usually <50 mIU/mL, that are verified to be real hCG
• No pregnancy, no GTD, no tumor• History of pregnancy or mole• hCG levels respond poorly to surgery or
chemotherapy• GTD, with surge in hCG, may occur later• Quiescent GTD ?

130
131
Further hCG testing
• Dilution study (best to use diluent containing animal Ig)
• Different brand of test• Urine test• Refer to hCG Reference Service (Laurence
Cole) at University of New Mexico (www.hcglab.com)
• Test at a later time

132
Block or detect heterophilic Ab’s
• Add nonspecific mouse Ig• Other species work, too—eg, bovine Ig
(commercial assays include blocking reagents, but they are not 100% effective)
• Remove Ig, eg, with protein A column• Heat-inactivate Ig• Assay for HAMA

133
Improve ligand-binding assays
• Use engineered Ab fragments or other binders
• But interfering Ab’s may be anti-idiotypic; there is probably no perfect solution
• Move to other type of assay?

134
Summary / Pearls of Pathology
• A steady, low-level hCG result should be treated judiciously!– It might be a dangerous ectopic pregnancy—but
consider history, symptoms, imaging findings– It is unlikely to be a cancer for which treatment,
before definitive diagnosis, is essential

135
Emerging Analytes in Microbiology
Sheldon Campbell M.D., Ph.D. Yale School of Medicine
VA Connecticut Healthcare System

136
Disclosure
• No conflicts of interest. • I could probably be bought, but
nobody’s tried that hard.

137
Course Objectives
• Emerging Antibiotic Resistance• Emerging Infections & Bioterrorism• Emerging Technologies

138
Emerging Antibiotic Resistance
• The dreaded Staph. aureus– MRSA detection– Staph with reduced glycopeptide
susceptibility – VISA/VRSA– Inducible clindamycin resistance

139
Staphylococcus aureus• Major nosocomial and community-acquired
pathogen– Responsible for >20% of bacteremia in US/Canada– Transmissible nosocomially and in the community.
• Antibiotic resistance -- lots– Methicillin (oxacillin) resistance
• Nosocomial• Community-acquired
– Vancomycin resistance• Relative resistance (VISA)• High-level resistance (VRSA)
– Macrolide resistance• The D-test

140
MRSA• First described in 1961; first penicillinase-
resistant semisynthetic menicillin introduced in 1960.
• Acquisition of the mecA gene. – Codes for altered PBP; PBP2a– Variable expression
• Steadily increasing in nosocomial populations– Multi-resistant
• Community-acquired strains– Tend to be non-multi-resistant– Outbreak and sporadic– Skin & soft tissue infections

141
010203040506070
1989 1991 1993 1995 1997 1999 2001 2003
Year
Perc
ent R
esis
tanc
eProportion of S. aureus Nosocomial
Infections Resistant to Oxacillin (MRSA) Among Intensive Care Unit Patients,
1989-2003*
*CDC Slide: Source: NNIS System, data for 2003 are incomplete
Rise of MRSA

142
Detection of MRSA
• NO completely satisfactory method• Hetero- and inducible- resistance
– Oxacillin screening agar– Cefoxitin disk test– PBP2a antigen

143
Oxicillin Screening Agar
• 6 µg/ml oxacillin• Mueller-Hinton agar supplemented with
4% NaCl• Incubate 24h before reading (-)• Requires a separate plate• 24h reporting delay if not done on all
isolates

144
Cefoxitin disk screen
• Normal (30 µg) cefoxitin disk• Report zone ≤19mm as oxacillinR
• Usable also for coagulase(-) staph, zones ≤24mm
• Relatively inexpensive• Requires a separate plate, but may be
combined with D-test and others• 24h reporting delay if not performed on
all isolates

145
PBP2a Antigen
• Rapid antigen test for PBP2a; gene product of mecA
• Rapid but expensive• May require overnight induction for best
sensitivity• Alternatively, confirm negatives by
alternate method or induction

146
VISA/VRSA
• Both rare resistance patterns• 3 VRSA (MIC >8) reported; probably
others missed, though• 11 VISAs (MIC=8) reported• ~3 dozen near-VISAs (MIC=4)• No spread to HCW, family, other
patients– Good infection control practices– Requires detection – the Micro Lab

147
VISA
• Vancomycin Intermediate S. aureus• Accumulated changes associated with
decreased fitness– Thickened cell wall by EM– Mixed large & small colony morphotypes
on plates

148
VRSA
• MIC >8• Acquisition of vanA cluster from
Enterococcus• Typically very high MICs, no loss of
fitness– Michigan strain: vanA cluster on a Staph
conjugal plasmid, MIC>1000– PA strain MIC=32 (?loss of cluster or ↓expression)
– NY strain MIC=64

149
VRSA (cont.)
• Neither Microscan nor Vitek detected all 3 VRSA strains
• Agar diffusion methods require careful examination –inhibition present in zone.
• Vancomycin Screening Agar is required for sensitive detection
Image from Image from TenoverTenover FC et al FC et al AntimicrobAntimicrob. . Agents & Chemo. 48:275Agents & Chemo. 48:275--80 (2004)80 (2004)

150
VRSA and Automated Methods
≤1, ≤1, ≤1≤0.5, 1, 1≤2, ≤2, ≤2, ATCC 29213
8, 8, 81, 16, 16≤2, ≤2, 4PA-VRSA (induced)
2, 2, 22, 1, 44, ≤2, ≤2, PA-VRSA (uninduced)
Vitek2VitekMicroScan
MICs (ug/ml) by methodS. aureusStrain
Pennsylvania strain; from Pennsylvania strain; from TenoverTenover et al et al AntimicrobAntimicrob. Agents. Chemo. 48:275. Agents. Chemo. 48:275--280 (2004) 280 (2004)

151
AcceptablePrimary Test Methods
Include: Disk diffusion2 plus VA screen plate(BHIA with 6 µg/ml of VA)
VA MIC <2 µg/mlAnd NO growth on
VA screen plate
VA MIC <2 µg/mlAND GROWTH onVA screen plate
(rare)
VA MIC >4 µg/mlAND GROWTH onVA screen plate
VA zone <14 mmAND GROWTH on VA screen plate
VA zone >14 mm AND GROWTH onVA screen plate
Report as VSSA3Report as VSSA3 Possible VISA/VRSA
CHECK purity
SAVE ISOLATE
NOTIFY infection control, physician, local health department and CDC5 of “possible VISA/VRSA”
MIC method1 plus VA screen plate(BHIA with 6 µg/ml of VA)
Possible VISA/VRSA
VA zone >14 mmand NO growth on
VA screen plate
CONFIRM isolate ID
RETEST using non-automated MIC method4
SEND to reference laboratory for confirmation
Important Footnotes1Laboratories using automated susceptibility test methods should add a commercial vancomycin agar screen plate. 2Disk diffusion alone is not sufficient to detect VISA.3If a laboratory is concerned about a result based on a patient’s history, MIC testing can be performed at CDC.4 Non-automated methods: reference broth microdilution, agar dilution, agar gradient diffusion (Etest; use a 0.5 McFarland inoculum and Mueller-Hinton agar).5Report to CDC by email: [email protected]
April 2004
More VISA/VRSA info: www.cdc.gov/ncidod/hip/vanco/vanco.htm
Algorithm for Testing S. aureus with Vancomycin (VA)

152
S. aureus -- Inducible Clindamycin Resistance
• Clindamycin resistance inducible via cross-resistance with macrolides– erm-mediated; methylation of 23S rRNA
• ‘D-test’ now recommended per Jan. 2002 NCCLS standards for erythromycin-resistant clindamycin-susceptible strains
• Alternatives:– Do D-test routinely– Do only on request; in that case, don’t
report clinda for erythro-R strains

153
A positive D-test
• 2 µg clindamycin disk
• 15 mm to 26 mm from edge of 15 µg erythromycin disk
• The erythromycininduces resistanceto the clindamycin
• QC strain TBA

154
15 15 -- 26 mm26 mm
Photos courtesy Photos courtesy FiebelkornFiebelkorn KR & Jorgensen JHKR & Jorgensen JH::FiebelkornFiebelkorn KR et al KR et al JClinJClin. Micro. 41(10):4740. Micro. 41(10):4740--4, 2003 Oct4, 2003 Oct ..
Another positive…

155
Negative D-test
• NO induction; round zone
• (msrA; efflux-mediated erythromycin resistance)

156
The ‘N Disks’ strategy
• A scheme for providing rapid susceptibility to common drugs– Cefoxitin– Erythromycin– Clindamycin– + others…
• The D-test spacing corresponds to the inner ring of a disk dispenser.
• Same inoculum can be used on Vancomycin Screening Agar
• Some laboratories are contemplating going back to K-B for S. aureus pending ability of automated systems to detect resistance

157
Discussion Question 1
• What other information would you want before reporting final susceptibilities on the following S. aureus isolate?
• Microscan results:– Vanco <2 (S)– Oxacillin <2 (S)– Erythro <.5 (S)– Clinda <.5 (S)

158
Answer 1
• You’d need to know the results of: – Vancomycin screening agar
• Automated methods are insensitive for vancomycin resistance
– Cefoxitin disk OR oxacillin screening agar OR PBP2a testing• Automated methods don’t pick up hetero-and
inducible MRSA

159
Discussion Question 2
• What other information would you want before reporting final susceptibilities on the following S. aureus isolate?
• Microscan results:– Vanco <2 (S)– Oxacillin >8 (R)– Erythro >8 (R)– Clinda <.5 (S)

160
Answer 2
• A D-test to look for inducible clindamycin resistance

161
Emerging Infections
• Laboratory role in emerging infections• Example
– West Nile• Biological Weapons and Sentinel
Laboratories– Responsibilities– Resources

162
The Laboratory in Emerging Infections
• Recognition• Laboratory safety• Diagnostic information resource• Transfusion medicine implications• Diagnostic testing

163
West Nile Virus
• The largest outbreak of arboviral meningoencephalitis in the Western Hemisphere.
• A flavivirus, related to Japanese encephalitis, St. Louis encephalitis, and HCV.
• Maintained via a bird-mosquito cycle, mammals probably incidental hosts

164
WNV: Epidemiology• Spread in
US from 1999-2004
• 2003 –spread of human infections in 45/48 lower US states
• 49 (!) vector mosquito species
200120012001
200220022002
200320032003

165
WNV: Clinical Illness
• Asymptomatic seroconversion (80%)• West Nile Fever (20%)• West Nile Meningitis or Encephalitis
(roughly 1/150)• Incubation: 3-14d• Sequelae common in CNS disease• Prolonged syptoms (~30d) in WNF, with
headache lasting >10d• Flaccid paralysis

166
WNV: Laboratory• WN CNS disease
– CSF pleiocytosis, <100 cells, usually lymphs– Elevated total WBC with lymphopenia– Serology most useful tool
• IgM (+) by symptom onset in 60% of cases, >95% by day 7
– Virus detection• Culture• RNA virus, RT-PCR• Viremia low in humans (1-130 pfu/ml), rare to isolate from
blood in patients with CNS disease• Viremia is short-lived: 2 Taqman(+) samples / 100 IgM(+)• Persistent virus in CSF

167
WNV Serology
• Commercial EIA kits becoming available• Cross-reaction with other flaviviruses;
SLE, dengue. • Confirmation with plaque neutralization
testing at a reference lab. • Patients may remain IgM(+) 6 months
or more after infection.

168
WNV: Laboratory Safety
• Virus is present in blood, serum, and CSF of affected patients
• Lab-associated infections documented, primarily research labs
• BSL-2 for primary specimens• BSL-3 for cultures and research in
animals/vectors

169
WNV: Novel Routes of Transmission
• Transplacental– Of 8 women with proven infections during gestation,
one affected infant with severe CNS damage• Breast milk
– Well-documented for other flaviviruses and HCV– One case in 2002, child had asymptomatic
seroconversion• Solid organ transplantation• Blood transfusion
– WNV is the only flavivirus other than HCV and HGV with documented transfusion-transmission

170
WNV: Transfusion
• Transfusion-related cases in the 2002 North American outbreak – prior to NAT– 61 investigations– 23 confirmed cases (1 pt. got 2 infected units)– 16 donors– 19 inconclusive (some probably real)– 19 no evidence for TT WNV
• Estimated risk 5-20/10,000 donations

171
WNV: Donors
• Donors in 2002 TT Cases– 18-72 y/o– 14/16 lived in counties with active WNV
transmission– At least 5 asymptomatic– All IgM (-) at donation– Viral titers <80 pfu/ml, higher in
symptomatic donors

172
WNV: FDA Guidelines for 2003• Reporting
– Patients with diagnosed WNV who received blood or organs within 4 weeks of onset
– Donors with diagnosed WNV with onset within 2 weeks of donation• Donor screening
– Defer for 28d from onset or 14d from end of symptoms• Diagnosis of WNV• Postdonation febrile illness with suggestive symptoms
– Defer for 28d• Potential donors who respond positively to “In the past week, have you
had fever with headache?”• Donors whose product is associated with a transfusion-related WNV
transmission– NO deferral
• (+) IgM asymptomatic within last 2 weeks
• NAT Testing of minipools
173
WNV: 2003 Testing Guidelines
• Minipool NAT testing from pools of 6 or 16 donors began June 2003. – Reactives retested by individual donor
testing– Selected blood banks in high-transmission
areas implemented individual donor testing during epidemic season
– Follow-up of positives with IgM serology as well as NAT; 28d deferral after last positive NAT and (+) antibody

174
WNV: 2003 NAT Positives• NAT positive
donors detected from Jun-Dec.
• At least 818 viremic donations removed from supply.

175
WNV: Transfusion-Transmitted Cases in 2003• 23 suspected cases
– 15 from public health system– 8 in follow-up of single-donor retrospective testing
• Investigation– Six cases probable or confirmed– 11 non-cases– 3 inconclusive
• Probable & confirmed– All were minipool NAT-negative
• Viral titers .06-.5 pfu/ml– 13-82 y/o recipients– 4 w/ WNV encephalitis, 1 w/ WN fever, 1 critically ill
pt. with no attributable symptoms

176
Lessons from West Nile
• Emerging infections can appear anywhere, any time. – Everything bad comes from New York?
• PCR isn’t all-powerful. • Emerging pathogens can enter the
blood supply.

177
Bioterrorism and the Clinical Lab
• Low probability – high impact• Priorities
– Protect the lab– Rule-out– Refer

178
Class A Biological Agents
• Variola major (Smallpox)• Bacillus anthracis (Anthrax)• Yersinia pestis (Plague)• Francisella tularensis (Tularemia)• Botulinum toxin (Botulism)• Filoviruses and Arenaviruses (Viral
hemorrhagic fevers)• ALL suspected or confirmed cases
should be reported to health authorities immediately

179
Disaster Management
•Disaster Occurs
•First Responders•Identify Problem, Limit Spread, Rescue Victims
•Disaster Management•Rescue / Transport victims, Evidence Gathering, Site Assessment
•Recovery Operations

180
First Responders
• Natural disasters, conventional terrorism– Fire Services– Police Services
• Bioterrorism– ER & Primary Care
Physicians– Clinical Laboratories
& Radiologists– Hazmat Teams– Fire & Police
(sometimes)

181
Disaster Management
• Conventional– Fire Services– Police Services– Federal Disaster
Mgmt. Teams– FBI & Investigatory
Agencies– Etc.
• Bioterrorism– Public Health
Authorities• Federal• State• Local
– FBI & Investigatory Agencies
– Physicians– Clinical Laboratories

182
The Laboratory Response Network
USUS

183
The Role of the Laboratory
• Recognition– ‘Rule-out’ BT pathogens
• Notification– Clinical care team– Public Health authorities; local, state– Hospital authorities
• Referral– Transporting specimens– Continuing workup of suspected cases

184
Laboratory Preparedness
• Plan in place• Sentinel lab protocols
– Rule-out or refer– Protect laboratory staff
• Transporting specimens– Chain of custody– Shipping regulations
• Train and Maintain– Protocols up to date

185
Emerging Pathogens and BT Resources
• Emerging Pathogens– CDC notification listserve
• http://www2a.cdc.gov/ncidod/hip/rns/hip_rns_subscribe.html
– ProMed mail• www.promedmail.org
• CDC BT Protocols & resources– http://www.bt.cdc.gov/labissues/index.asp– Also from ASM; Google ‘Sentinel Lab
Protocols’ (it’s a strange URL)

186
Emerging Technologies
• Molecular microbiology– MRSA by RT-PCR; – The face of the future?

187
MRSA by RT-PCR
• There’s no completely satisfactory screening method for MRSA carriage.
• Multiple mecA types and competition with coag-negative staph makes this a challenging problem.
• Newly FDA-approved method using Real Time PCR on the Cepheid SmartCycler.

188
Design of the MRSA Assay
• A multiplex PCR scheme which requires 5 left-side primers (for various mecA cassette types) and one right-side primer.
• Detection by three molecular beacon probes (for various orfX variants)• Internal amplification control, detected by a fourth probe.
• Huletsky et al J. Clin. Microbiol. 42:1875-1884 (2004)

189
MRSA detection
• Method identified 1,636/1,657 (98.7%) of known MRSA strains.
• Mis-detected 26/569 (4.6%) MSSA strains. • Detected 0/62 non-staph, 0/286 CoNS (212
of them methicillin-resistant). • Detected ~25 organisms into MRSa-negative
nasal specimens. • Detected 97% of MRSA detected by culture in
epidemiologic surveillance program.

190
MRSA Product
• Roughly 2h TAT• Manual sample prep• More sensitive than a single culture plate, but
with some false positives

191
The Face of the Future?

192
One More Scary(?) Thought
• The major patents on PCR expire in Spring of 2005.
• Will there be an explosion of new tests?

193
Discussion Question #3• Dr. Welby-Price from the ER calls you about a patient.
– A 57 year old man. – Jaundiced, thrombocytopenic, in DIC. – Dripping green slime from fingernails and conjunctivae.
• You’ve been reading in Promed about an outbreak.– It resembles Crimean-Congo hemorrhagic fever, except the
victims drip green slime. – Began in Turkmenistan after a strange meteorite impact.
• Dr. W-P asks you what specimens to send. What do you tell him? <hint: at least part of the answer is ‘let me look a few things up and get back to you?>

194
Answers #3• Things I’d address:
– Who’s the patient? Lab needs to quarantine the specimens and not perform any further testing until biosafety issues are clarified.
– Does the patient have risk factors (e.g. travel to the endemic area)?
– Does the patient have clinical signs/symptoms or risk factors for more common, similar syndromes (sepsis, rickettsial or Ehrlichial disease, acute leukemia…)

195
Question #4• After some research, you get more
information on Crimean-Congo hemorrhagic fever. – It’s a Level A BT agent; hemorrhagic fever virus. – There’s usually detectable viremia during the
acute phase. – There’s a serologic response 5-14d after onset.
• Who do you contact? • What specimens do you suggest to Dr.
Welby-Price• What other actions might you take?

196
Answers #4
• What, you think I’ve got all the answers?
• Discussion…

197
Summary• Microbes are smart. Individually, their IQ is ~10-9, but
there are lots of them. • Emerging antibiotic resistance patterns will require
labs to keep up with continuing changes in methodology and interpretation.
• Emerging pathogens will challenge laboratories to provide diagnostic support and consultation, to protect lab workers, provide safe blod products, and to develop new procedures.
• Emerging technology will challenge labs to answer new clinical questions and to answer old questions more rapidly and accurately.
• Pathologists need to play an active role in keeping their laboratories up to date and assisting the front-line clinicians in managing emerging infectious problems.

198
Pearls of Pathology• Emerging Antimicrobial Resistance
– Keep up with NCCLS susceptibility guidelines; even if you can’t implement them immediately
– Be aware of emerging mechanisms• Emerging pathogens
– Use listserves to stay aware of emerging threats and information resources
– Be aware of emerging infections– Protect the lab– Be a resource for patient care
• Prepare for the impact of emerging technologies