emergency room management of hypertensive urgencies and emergencies
TRANSCRIPT
JOURNAL OF CLINICAL HYPERTENSION VOL. III NO. III MAY/JUNE 2001158
Hypertensive crisis affects upward of 500,000Americans each year. Although the incidence ofhypertensive crisis is low, affecting fewer than 1% of hypertensive adults, more than 50 millionadult Americans suffer from hypertension. Presen-tation of a patient with severe hypertension to theemergency room demands immediate evaluation,prompt recognition of a hypertensive emergencyor urgency, and the prompt institution of appro-priate therapeutic measures to prevent progressionof target-organ damage and to avoid a catastroph-ic event. Hypertensive emergencies are severe ele-vations in blood pressure that are complicated byevidence of progressive target-organ dysfunctionsuch as coronary ischemia, disordered cerebralfunction, a cerebrovascular event, pulmonaryedema, or renal failure. Although therapy withparenteral antihypertensive agents may be initiat-ed in the emergency department, these patientswarrant prompt admission to an intensive careunit where continuous monitoring of blood pressure can be assured during therapy. (J Clin Hypertens. 2001;3:158–164). ©2001 by Le Jacq Communications, Inc.
Hypertensive urgencies are severe elevations inblood pressure without evidence of progres-
sive target organ dysfunction and can usually bemanaged by orally administered medications initi-ated in the emergency department with appropri-
ate follow-up within 24 hours, to several days depending upon individual characteristics of the patient. Elevated blood pressure alone rarelyrequires emergency therapy.1
Most hypertensive urgencies or emergencies arepreventable and are the result of inadequate treat-ment of mild to moderate hypertension or nonadher-ence to antihypertensive therapy.2,3 In a few cases, a previously unrecognized form of secondary hyper-tension, such as renal vascular hypertension orpheochromocytoma, and rarely, primary hyperaldos-teronism, may be responsible and will obviously require early recognition if specific therapy is to beinitiated. Prompt emergency room evaluation is un-dertaken to identify the clinical status of the patient,to provide clues to an underlying etiology of the hy-pertension, to assess the degree of target organ in-volvement, and to select the most appropriatepharmacologic agent and method of administration.
ASSESSMENTSInitialEarly triage is critical in an effort to assure the mosttimely and appropriate therapy for each patient.4 Abrief but thorough history should address the durationas well as the severity of hypertension, all current med-ications, including prescription and nonprescriptiondrugs, and the use of recreational drugs. A history ofother co morbid conditions and prior cardiovascularor renal disease is critical to the initial evaluation.
Direct questioning regarding the level of com-pliance with current antihypertensive medicationsmay establish inadequacy of therapy. Frequent orcontinuous monitoring of blood pressure shouldbe established. Look for historical information regarding neurologic, cardiovascular, and/or renalsymptoms and look for specific manifestations,such as headache, seizures, chest pain, dyspnea,and edema.
Emergency Room Management of Hypertensive Urgencies and Emergencies
Donald G. Vidt, MD
From the Cleveland Clinic Foundation, Cleveland,and Ohio State University, Columbus, OH Address for correspondence/reprint requests: Donald G. Vidt, MD, Cleveland Clinic Foundation,9500 Euclid Avenue, Cleveland, OH 44195Manuscript received October 19, 2000; accepted November 27, 2000

PhysicalPhysical assessment should start with an assess-ment of blood pressure, with an appropriate sizecuff, in both upper extremities. Brachial, femoral,and carotid pulses should be measured. A carefulcardiovascular examination as well as a thoroughneurologic examination, including mental status,should be conducted. This assessment should es-tablish the degree of involvement of affected tar-get organs and should provide clues to thepossible existence of a secondary form of hyper-tension, such as renal vascular hypertension. If asecondary cause of hypertension is suspected, ap-propriate blood and urine samples should be ob-tained before aggressive therapy is initiated. Acareful funduscopic examimation should be per-formed to detect hemorrhages, exudates, and/orpapilledema.
INITIAL LABORATORY STUDIESA urinalysis with sediment examination, a statchemistry profile, and an electrocardiogram, together with a complete history and thoroughphysical examination, should enable a clinical assessment of the degree of target organ involve-ment and should facilitate the selection of an appropriate antihypertensive agent for initialtreatment. The urinalysis may show significantproteinuria, red blood cells, and/or cellular casts. Cellular casts are suggestive of renal parenchymaldisease. Electrolyte abnormalities, particularly hypokalemia or hypomagnesemia, increase therisk of cardiac arrhythmias, and the chemistryprofile will also provide evidence of renal dysfunc-tion. The electrocardiogram should identify evi-dence of coronary ischemia and left ventricularhypertrophy, and pulse deficits should raise thequestion of aortic dissection. A computed tomo-graphic (CT) scan of the head should be consid-ered when the clinical examination suggestscerebrovascular ischemia or hemorrhage, or in thecomatose patient. The decision to treat as a hyper-tensive emergency should prompt immediate admission to an intensive care unit where continu-ous monitoring of blood pressure can be estab-lished for subsequent parenteral treatment of thehypertensive emergency.
The clinical characteristics of the hypertensiveemergency are listed in Table I. The level of bloodpressure alone does not determine a hypertensiveemergency; rather, it is the degree of target organinvolvement that determines the rapidity withwhich blood pressure should be reduced to a saferlevel to prevent or limit target organ damage. Ini-tial therapy will often be based on a presumptive
diagnosis based on the information available dur-ing the initial triage evaluation (Table II). Bloodpressure reduction should not be delayed until theresults of all diagnostic studies are available for review, but rather should be initiated as soon asthe patient’s clinical status is established.
HYPERTENSIVE EMERGENCIESThe initial goal for blood pressure reduction is not toobtain a normal blood pressure, but rather to achievea progressive but controlled reduction in blood pres-sure to minimize the risk of hypoperfusion in cerebral,coronary, and renal vascular beds.5 It is recommendedthat the initial reduction in mean arterial pressure(MAP) not be more than 20%–25% below the pre-treatment blood pressure, or that MAP be reducedwithin the first 30–60 minutes to 110–115 mm Hg.6 Ifthis level of blood pressure is well tolerated and thepatient is clinically stable, further gradual reductionstoward a normal blood pressure can be effected overthe next 12–24 hours. Excessively rapid reduction inblood pressure has been associated with acute deterio-ration in renal function, ischemic, cardiac, or cerebralevents, and occasional retinal artery occlusion andacute blindness.
HYPERTENSIVE URGENCIESThe caveat with hypertensive urgencies is that “ele-vated blood pressure alone rarely requires emergencytherapy.” The initial triage should identify those patients who have an elevated blood pressure with-out any evidence of significant target organ damageand no evidence of other impending cardiovascularevents (Table II). An effort should be made to sepa-rate out those patients with severely elevated bloodpressure and clinical evidence of target organ dam-age who may benefit from a period of observation inthe emergency department following the administra-
VOL. III NO. III MAY/JUNE 2001 JOURNAL OF CLINICAL HYPERTENSION 159
TABLE I. CLINICAL CHARACTERISTICS OFTHE HYPERTENSIVE EMERGENCY
Blood pressureUsually >220/140 mm Hg
Funduscopic findingsHemorrhages, exudates, papilledema
Neurologic statusHeadache, confusion, somnolence, stupor, visual loss, seizures, focal neurologic deficits, coma
Cardiac findingsProminent apical pulsation, cardiac enlarge-ment, congestive heart failure
Renal symptomsAzotemia, proteinuria, oliguria
Gastrointestinal symptomsNausea, vomiting

JOURNAL OF CLINICAL HYPERTENSION VOL. III NO. III MAY/JUNE 2001160
tion of one or several oral medications to reduceblood pressure over a period of several hours. If clin-ically stable, these patients can safely be sent homewith oral medications, with arrangements made for afollow-up visit within 24 hours in an outpatient set-ting. Several oral agents can provide a rapid responsein blood pressure within 1–3 hours. Control effortscan then be continued under the supervision of a pri-mary physician. Most patients with hypertensive ur-gencies are previously diagnosed hypertensives whoare either noncompliant with therapy or are receiv-ing inadequate therapy to control blood pressure.Further evaluation, if needed, can then be performedin the outpatient setting.
To discharge the patient from an emergency roomwithout a confirmed follow-up appointment is amissed opportunity to get that patient back intotreatment, and optimal control of blood pressureshould be a management goal. For the patient withelevated blood pressure and no evidence of targetorgan damage or other acute cardiovascular prob-lems, reassurance and a period of observation in theemergency department may be appropriate, particu-larly if an anxiety-related event is suspected. Forthose patients inadequately treated or noncompliantwith therapy, medication may be resumed or modi-fied and arrangements made for outpatient follow-up within several days. For the occasional patient
with previously undiagnosed hypertension, effortsshould be made to confirm access to a primaryphysician for follow-up blood pressure screening andevaluation, if indicated. For most patients who arenoncompliant with therapy or undertreated by theirprimary physician, the recommendations outlined inthe Joint National Committee VI Guidelines are ap-propriate.1
ORAL AGENTS FOR HYPERTENSIVE URGENCIESThe following oral agents can be used for hypertensiveurgencies (see Table III).7 Captopril, an angiotensin-converting enzyme inhibitor, is well tolerated and haseffectively reduced blood pressure in hypertensive urgencies. Given by mouth, captopril is usually effec-tive within 15–30 minutes and may be repeated in 1–2hours depending upon the response.8 The drug hasbeen administered sublingually, in which case theonset of action may occur within 10–20 minutes, withthe maximal effect reached within 1 hour. Administra-tion may lead to acute renal failure in patients with bilateral renal artery stenosis, and reflex tachycardiamay be observed. Responsiveness to this agent can beenhanced by the administration of a loop diuretic,such as furosemide.
Clonidine is a centrally acting α-adrenergic agonist with onset of action 30–60 minutes following
TABLE II. ALGORITHM: TRIAGE EVALUATION
GROUP I – HIGH BP GROUP II – URGENCY GROUP III – EMERGENCY
BP >180/110 >180/110 USUALLY >220/140
Symptoms Headache Severe headache Shortness of breathAnxiety Shortness of breath Chest painOften asymptomatic Edema Nocturia
DysarthriaWeaknessAltered consciousness
Exam No target organ damage Target-organ damage EncephalopathyNo clinical cardiovascular disease Clinical cardiovascular disease Pulmonary edema
present /stable Renal insufficiencyCerebrovascular accidentCardiac ischemia
Therapy Observe 1–3 hr Observe 3–6 hr Baseline labsInitiate/resume medication Lower BP with short-acting Intravenous lineIncrease dosage of inadequate oral agent Monitor BPagent Adjust current therapy May initiate parenteral
therapy in emergency room
Plan Arrange follow-up <72 hr Arrange follow-up Immediate admission to ICUIf no prior evaluation, evaluation <24 hr Treat to initial goal BPschedule appointment Additional diagnostic studies
BP=blood pressure; ICU=intensive care unit

oral administration and maximal effects seen within2–4 hours. Although it is most commonly adminis-tered in a loading regimen of 0.1–0.2 mg followed by0.1 mg hourly for several hours, evidence suggests thatcomparable responses may be seen with a single 0.2mg dose.3 The most common adverse effect seen inthe acute setting is drowsiness, affecting up to 45% of patients. Clonidine may be a poor choice when moni-toring of mental status is important. Dry mouth is alsoa common complaint and lightheadedness is occasion-ally observed.
Labetalol is a combined α- and β-adrenergicblocking agent. It can be effective given orally in adose of 200–400 mg, which may be repeated after2–3 hours. The onset of effect is observed within 1–2hours.9,10 Like any β blocking agent, it has the po-tential to induce heart block and to worsen symp-toms of bronchospasm. Therefore, it should beavoided in patients with uncontrolled asthma orthose with more than first-degree heart block, symp-tomatic bradycardia, or congestive heart failure.
Prazosin is an α-adrenergic blocking agent thatcan have limited benefit in the early management ofpheochromocytoma. Side effects include first-dosesyncope, palpitations, tachycardia, and orthostatichypertension.
AGENTS FOR HYPERTENSIVE EMERGENCIES Parenteral AgentsThe following parenteral agents are effective in treat-ing hypertensive emergencies (see Table IV).7 La-betalol has proved particularly effective when used inbolus intravenous injections in the initial treatmentof hypertensive emergencies, and can provide a con-trolled reduction in blood pressure to a predeter-mined goal.11 Once a goal pressure is achieved, injections are stopped, and the long duration of action facilitates conversion to effective oral therapy.
The infusion of labetalol at a rate of 2 mg per minuteoffers an alternative method of administration and isassociated with a gradual yet controlled reduction inblood pressure.12 Because β blocking effects predom-inate with this agent, bradycardia or heart block mayoccur in patients with intrinsic heart disease.
Sodium nitroprusside is a potent vasodilator andan exceptionally predictable agent when adminis-tered in a hypertensive crisis of any etiology.5,13
The drug has an extremely rapid onset of action,within seconds of initiating an infusion, and a veryrapid offset of effect within 1–2 minutes, which ne-cessitates constant supervision of blood pressure.Its popularity relates in part to its effectiveness in reducing both preload and afterload and the abilityto achieve a controlled titration of blood pressure. Nitroprusside does not cause sedation or somno-lence but is rapidly degraded by light, requiring pe-riodic exchange of solution.
One of the major concerns in using sodium nitro-prusside is its metabolism to cyanogen and to thio-cyanate. In patients with significant impairment inrenal function, accumulation of thiocyanate mayoccur over several days, with toxic effects. In patientswith impaired hepatic function and poor cardiac per-fusion, cyanide poisoning has been reported.14
Nicardipine, an intravenous form of the dihy-dropyridine calcium antagonist, has proved effectivein a high percentage of hypertensive emergencies,particularly at higher infusion rates.15 The growingpopularity of this agent can be attributed to its easeof administration as a continuous infusion startingat 5 mg per hour. The infusion rate can be increasedby 2.5 mg per hour at intervals of 15–20 minutesuntil a maximum recommended infusion rate of 15mg per hour is obtained or until the desired reduc-tion in blood pressure is achieved. An excellent cor-relation has been demonstrated between plasmaconcentration and dose response of diastolic blood
VOL. III NO. III MAY/JUNE 2001 JOURNAL OF CLINICAL HYPERTENSION 161
TABLE III. MANAGEMENT OF HYPERTENSIVE URGENCIES: ORAL AGENTS
AGENT DOSE ONSET/DURATION OF ACTION PRECAUTIONS
(AFTER DISCONTINUATION)
Captopril 25 mg p.o., repeat as needed SL, 25 mg 15–30 min/6–8 hr SL Hypotension, renal failure in15–30 min/2–6 hr bilateral renal artery stenosis
Clonidine 0.1–0.2 mg p.o., repeat hourly as 30–60 min/8–16 hr Hypotension, drowsiness,required to total dose of 0.6 mg dry mouth
Labetalol 200–400 mg p.o., repeat every 2–3 hr 30 min–2 hr/2–12 hr Bronchoconstriction, heartblock, orthostatic hypotension
Prazosin 1–2 mg p.o., repeat hourly as needed 1–2 hr/8–12 hr Syncope (first dose), palpitations, tachycardia, orthostatic hypotension
JOURNAL OF CLINICAL HYPERTENSION VOL. III NO. III MAY/JUNE 2001162
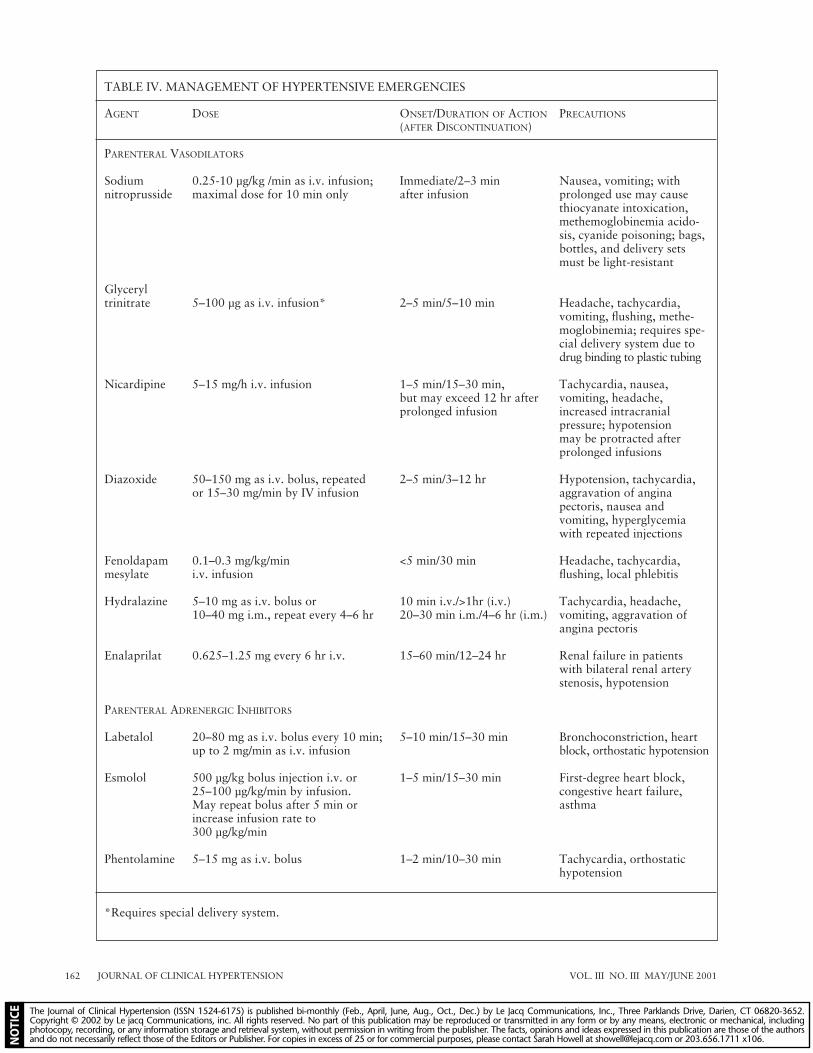
TABLE IV. MANAGEMENT OF HYPERTENSIVE EMERGENCIES
AGENT DOSE ONSET/DURATION OF ACTION PRECAUTIONS
(AFTER DISCONTINUATION)
PARENTERAL VASODILATORS
Sodium 0.25-10 µg/kg /min as i.v. infusion; Immediate/2–3 min Nausea, vomiting; withnitroprusside maximal dose for 10 min only after infusion prolonged use may cause
thiocyanate intoxication,methemoglobinemia acido-sis, cyanide poisoning; bags,bottles, and delivery setsmust be light-resistant
Glyceryl trinitrate 5–100 µg as i.v. infusion* 2–5 min/5–10 min Headache, tachycardia,
vomiting, flushing, methe-moglobinemia; requires spe-cial delivery system due todrug binding to plastic tubing
Nicardipine 5–15 mg/h i.v. infusion 1–5 min/15–30 min, Tachycardia, nausea, but may exceed 12 hr after vomiting, headache, prolonged infusion increased intracranial
pressure; hypotension may be protracted after prolonged infusions
Diazoxide 50–150 mg as i.v. bolus, repeated 2–5 min/3–12 hr Hypotension, tachycardia,or 15–30 mg/min by IV infusion aggravation of angina
pectoris, nausea and vomiting, hyperglycemiawith repeated injections
Fenoldapam 0.1–0.3 mg/kg/min <5 min/30 min Headache, tachycardia,mesylate i.v. infusion flushing, local phlebitis
Hydralazine 5–10 mg as i.v. bolus or 10 min i.v./>1hr (i.v.) Tachycardia, headache,10–40 mg i.m., repeat every 4–6 hr 20–30 min i.m./4–6 hr (i.m.) vomiting, aggravation of
angina pectoris
Enalaprilat 0.625–1.25 mg every 6 hr i.v. 15–60 min/12–24 hr Renal failure in patients with bilateral renal arterystenosis, hypotension
PARENTERAL ADRENERGIC INHIBITORS
Labetalol 20–80 mg as i.v. bolus every 10 min; 5–10 min/15–30 min Bronchoconstriction, heartup to 2 mg/min as i.v. infusion block, orthostatic hypotension
Esmolol 500 µg/kg bolus injection i.v. or 1–5 min/15–30 min First-degree heart block,25–100 µg/kg/min by infusion. congestive heart failure,May repeat bolus after 5 min or asthmaincrease infusion rate to 300 µg/kg/min
Phentolamine 5–15 mg as i.v. bolus 1–2 min/10–30 min Tachycardia, orthostatic hypotension
*Requires special delivery system.

pressure. The dosing of nicardipine is not dependentupon the patient’s body weight. Nicardipine hasbeen shown to reduce both cerebral and coronaryischemia, and headache, nausea, and vomiting mayoccur. Modest tachycardia may be observed.
Nitroglycerine may be of particular efficacy inhypertensive emergencies with coexistent coronaryischemia.16 Nitroglycerine dilates collateral coro-nary vessels, and like nitroprusside, has a rapidonset and offset of effect, requiring close nursingsupervision. When infused at low doses (5–10 µgper minute), nitroglycerine dilates capacitance ves-sels, whereas much higher infusion rates are re-quired to affect arteriolar vasodilatation. Theinfusion rate may be increased at 3–5-minute in-tervals until the desired effect is achieved.
Nitroglycerine may be particularly useful in patients with severe coronary ischemia in whomblood pressures are only modestly elevated or inpatients with postcoronary artery bypass hyper-tension. Tolerance to intravenous nitroglycerinemay be observed within 24–48 hours of infusion,and unpredictable absorption in polyvinyl chlo-ride containers and tubing necessitates the use ofglass containers.
Fenoldapam is a unique, selective, peripheraldopamine-I receptor agonist that provides systemicvasodilation, particularly in the renal circulation,and also has effects on renal proximal and distaltubules.17 It does not bind to dopamine II receptorsor β adrenergic receptors, has no α-adrenergic ago-nist effects, but is an α-I antagonist and does notcross the blood-brain barrier. Compared to otherparenteral antihypertensive agents, fenoldipine’sunique effects on the kidney provide increasedurine flow rate, sodium and potassium excretion,and creatinine clearance, making this agent particu-larly attractive in hypertensive emergencies withrenal impairment.
Clinical studies have suggested that fenoldapamis as effective as sodium nitroprusside in improv-ing cardiac hemodynamics in patients with acute,severe congestive heart failure.18
The onset of clinical effect is usually seen within 5minutes and affects dissipate within 30 minutes fol-lowing discontinuation of the infusion. Side effectsinclude headache, flushing, tachycardia, and dizzi-ness. Bradycardia has occasionally been noted and adose-related increase in intraocular pressure has beenobserved in normotensive and hypertensive patients.Inactive metabolites are primarily eliminated in theurine and no dosage adjustments are required for pa-tients with renal or hepatic impairment.
Hydralazine should be restricted to pregnantwomen with pre-eclampsia. Five to 10 mg may be
administered intravenously as a bolus injection andmay be repeated.19 The major advantage is thisagent’s ability to improve uterine blood flow. Hydralazine is contraindicated in patients with coro-nary atherosclerosis, and administration is associatedwith reflex tachycardia, sodium and water retention,and intense flushing. Headache and increased in-tracranial pressure have also been observed.
Other AgentsEnalaprilat, the active form of enalapril, is admin-istered intravenously in a dose of 1.25 mg admin-istered at 6-hour intervals. The onset of action isseen within 30 minutes and the response toenalaprilat in hypertensive emergencies is unpre-dictable, in part because of variable degrees ofplasma volume expansion. This agent may be par-ticularly useful in hypertensive emergencies associ-ated with congestive heart failure or high plasmaangiotensin II concentrations.
Esmolol is an intravenous, ultra-short-acting β-adrenergic blocker. Onset of effect is seen within1–5 minutes, with a rapid offset of effect within15–30 minutes following discontinuation. Esmololis administered as a 500 µg/kg bolus injection,which may be repeated after 5 minutes. Alterna-tively, an infusion of 50–100 µg/kg/min may beinitiated and increased to 300 µg/kg/min as need-ed. Adverse effects include increased heart block,congestive heart failure, and bronchoconstriction.
Phentolamine, a nonselective α-adrenergic block-ing agent, is reserved today for use in suspected excess catecholamine states, such as pheochromocy-toma. It may be useful as a diagnostic agent admin-istered as a bolus injection of 5–10 mg in patientswith suspected pheochromocytoma. Acute bloodpressure lowering will be seen within several min-utes and may last 10–30 minutes. Tachycardia is acommon occurrence and may precipitate myocar-dial ischemia. Nitroprusside and labetalol are moreeasily titrated in the management of hypertensiveemergencies associated with high circulating levelsof catecholamines; therefore, phentolamine is rarelyutilized therapeutically today.
Diazoxide is rarely used today in the treatmentof hypertensive emergencies. Although a potentvasodilator, large doses of 300 mg were often as-sociated with severe hypotension. Smaller mini-boluses of 50 mg administered every 10–15minutes can provide a controlled reduction inblood pressure but can cause reflex tachycardia,hyperglycemia, hyperuricemia, and sodium andwater retention. Diazoxide offers no advantageover several other agents that have more accept-able adverse effect profiles.
VOL. III NO. III MAY/JUNE 2001 JOURNAL OF CLINICAL HYPERTENSION 163

JOURNAL OF CLINICAL HYPERTENSION VOL. III NO. III MAY/JUNE 2001164
SUMMARYPatients presenting to emergency departmentswith severe hypertension deserve prompt triage toestablish the presence of a hypertensive emergencyor urgency. Those with hypertensive emergenciesmust be promptly admitted to an intensive careunit where continuous monitoring of blood pres-sure is available, as well as prompt therapy withparenteral antihypertensive drugs to prevent pro-gression of target organ damage. Most patientswith hypertensive urgencies can be managed on anambulatory basis with initiation or adjustment ofappropriate oral antihypertensive therapy. A keyto the management of hypertensive urgencies isthe assurance of appropriate follow-up care to as-sure continued optimal hypertension management.
REFERENCES1 Joint National Committee. The sixth report of the Com-
mittee on the Prevention, Detection, Evaluation and Treat-ment of High Blood Pressure (JNC-VI). Arch Intern Med.1997;157:2413–2446.
2 Ferguson RK, Vlasses PH. How urgent is “urgent” hyper-tension? [editorial]. Arch Intern Med. 1989;149:257–258.
3 Zeller KR, Kunert LV, Matthews C. Rapid reduction ofsevere asymptomatic hypertension; a prospective, con-trolled trial. Arch Intern Med. 1989;149:2186–2189.
4 Jackson RE. Hypertension in the emergency department.Emerg Med Clin North Am. 1988;6:173–196.78.
5 Bedoya LA, Vidt DG. Treatment of the hypertensive emer-gency. In: Jacobson HR, Striker GE, Klahr S, eds. ThePrinciples and Practice of Nephrology. Philadelphia, PA:Decker; 1991:547–557.
6 Calhoun DA. Hypertensive crisis. In: Oparil S, Weber MA, eds.Hypertension: A Companion to Brenner and Rector’s The Kid-ney. Philadelphia, PA: W.B. Saunders; 2000:715–718.
7 Vidt DG. Management of hypertensive urgencies andemergencies. In: Izzo JL, Jr, Black HR, eds. HypertensionPrimer: The Essentials of High Blood Pressure. Dallas,TX: American Heart Association; 1999;437–440.
8 Biollaz J, Waeber B, Brunner HR. Hypertensive crisistreated with orally administered captopril. Eur J ClinPharmacol. 1983;25:145–149.
9 Ghose RR. Acute management of severe hypertension withoral labetalol. Br J Clin Pharmacol. 1979;8:189S–193S.
10 Catapano MS, Marx JA. Management of urgent hyperten-sion: A comparison of oral treatment regimens in theemergency department. J Emerg Med. 1986;4:361–368.
11 Cressman MD, Vidt DG, Gifford RW, Jr, et al. Intravenouslabetalol in the management of severe hypertension and hy-pertensive emergencies. Am Heart J. 1984;107:980–985.
12 Lebel M, Langlois S, Belleau LJ, et al. Labetalol infusionin hypertensive emergencies. Clin Pharmacol Ther.1985;37:615–618.
13 Garcia JY Jr, Vidt DG. Current management of hyperten-sive emergencies. Drugs. 1987;34:263–278.
14 Nightingale SL. New labeling for sodium nitroprussideemphasizes risk of cyanide toxicity (from the Food andDrug Administration). JAMA. 1991;265:847.
15 IV Nicardipine Study Group. Efficacy and safety of intra-venous nicardipine in the control of postoperative hyper-tension. Chest. 1991;99:393–398.
16 Flaherty JT, Magee PA, Gardner TL, et al. Comparison ofintravenous nitroglycerin and sodium nitroprusside fortreatment of acute hypertension developing after coronaryartery bypass surgery. Circulation. 1982;65:1072–1077.
17 Munger MA, Rutherford WF, Anderson L, et al. Assess-ment of intravenous fenoldapam mesylate in the manage-ment of severe systemic hypertension. Crit Care Med.1990;18:502–504.
18 Panacek EA, Bednarczyk EM, Dunbar LM, et al. Random-ized, prospective trial of fenoldapam vs sodium nitroprussidein the treatment of acute severe hypertension. FenoldapamStudy Group. Acad Emerg Med. 1995;2:959–965.
19 Paterson-Brown S, Robson SC, Redfern N, et al. Hy-dralazine boluses for the treatment of severe hypertensionin pre-eclampsia. Br J Obstet Gynaecol. 1994; 101:409–413.