electronic medical record benefits - health...
TRANSCRIPT

Department of Health
Electronic medical record benefits
A literature review


Electronic medical record benefits
A literature review

If you would like to receive this publication in an accessible format, please email: [email protected]
This document is available as a PDF on the internet at: www.health.vic.gov.au/divisions/fcs/cio.htm
© Copyright, State of Victoria, Department of Health, 2012 This publication is copyright, no part may be reproduced by any process except in accordance with the provisions of the Copyright Act 1968. Authorised and published by Victorian Government, 50 Lonsdale Street, Melbourne.
Except where otherwise indicated, the images in this publication show models and illustrative settings only, and do not necessarily depict actual services, facilities or recipients of services.
March 2012 (1203019)

Contents
Executive summary 1
Introduction 3 Document purpose and scope 3 Background 3 Intended audience 3
The healthcare opportunity 4 Benefits that ICT brings to quality care and demand management 4 The electronic medical record defined 4
Benefits analysis 5 How an EMR will realise the benefits 5 The benefits along a patient journey 6 Quantitative benefits 7 Qualitative benefits 9 Continuous optimisation 10 Tip of the iceberg 10
Conclusion 12
Appendices 13 Appendix 1: Benefit extrapolation methodology 13 Appendix 2: Cited references 15 Appendix 3: Other references 18


Page 1
Executive summary
An extensive literature review was undertaken to document and identify the benefits that may be attributed to using electronic medical record (EMR) information and communication technology (ICT) systems, and to quantify the economic benefits that could be realised through the introduction of these systems into Victorian public health services (VPHS).
The literature highlights benefits from both administrative and clinical perspectives that can be attributed to using an EMR system (Table 1, overleaf). Most of the literature identifies qualitative benefits, such as reducing duplication of administration data or providing the right information at the right time for the patient condition. It draws attention to the importance of establishing clinical pathways to reduce preventable in-hospital complications.
Four papers identified quantitative benefits that can be attributed to the implementation of ICT systems using an EMR as a tool to improve clinical pathways, providing evidence supporting the implementation of an EMR to reduce preventable in-hospital complications. Three of those studies demonstrated quantitative benefits that could be attributed to the implementation of clinical pathways and medication management using an EMR system to improve clinical outcomes and help drive efficiencies that result in decreased (18 to 30 per cent) patient length of stay (LOS) in hospitals. One study quantified the reduction of errors (76 per cent) in discharge summaries that could be attributable to an EMR.
The literature reinforces the argument that EMR systems will be pivotal in enabling the efficient collection of meaningful, accurate and complete data that supports active clinical decision support and the development, implementation and optimisation of clinical pathways.
The implementation of an EMR system will enable business process improvement activities such as the Redesigning Hospital Care Program to be set up as permanent continuous optimisation programs across the VPHS. This ensures that all clinical and business processes included in the EMR solution may be continuously monitored, optimised and deployed on a local and statewide basis, as required.
During the analysis an opportunity to estimate the economic benefits that may be realised through implementing an EMR system was identified. The estimation is based on extrapolation of two studies, one by Ehsani et al. (2006) using data from the Victorian Admitted Episodes Data Set (VAED), the other by Rotter et al. (2010) on the impact that introducing clinical pathways has on preventable in-hospital complications. Although no statistical analysis was undertaken to confirm a relationship between the clinical information in the medical record and the VAED data, our estimates suggest that if one accepts the assumption that an EMR system will make clinical pathways more easily developed and implemented across VPHS, there would be the opportunity for a reduction of up to 35,000 preventable in-hospital complications per year.
The quantified benefits identified in Table 1 (overleaf) pertain to reductions in preventable in-hospital complications and improvements to referral processes. We believe these represent only the tip of the iceberg and the full benefits to be gained from widespread use of continuously optimised clinical pathways will only be understood once an EMR solution is operating across the VPHS.

Electronic medical record benefits
Page 2
Table 1: Identified EMR benefits across the patient journey
No. Benefits Quantified benefit 1
Across the whole patient journey
1 Entering data once and using it many times (Garde 2006) -
2 Computerisation of data entry to achieve legible documentation (Schuler 2010); increasing the system’s ability to ensure completeness, consistency and legibility of medical records (Paneth-Pollak et al. 2010); providing the opportunity to evaluate medical record data in real time to inform clinical, program and policy decisions (Paneth-Pollak et al. 2010)
-
3 Coordination of processes across the patient journey at the clinical, administrative and management levels (Reid et al. 2005; Grossman 2008)
4 Reducing duplication of administration data by providing access to all the team (Australian Nursing Federation 2007)
-
Admission assessment
5 Average cost benefit of processing an electronic patient referral in a hospital (Cannaby et al. 2004)
�32 per cent processing referral
cost
Treatment / intervention
6 Improved clinical outcomes through sepsis clinical pathway (Hopper & Jacobs 2009)2 �18 per cent LOS
7 Improved clinical outcomes through pneumonia clinical pathway (Rotter et al. 2010) �20 per cent LOS
8 Reduced surgical adverse events through medication management (Murphy et al. 2009)
�30 per cent LOS
9 Standardisation of data elements and information models to ensure semantic interoperability enabling the implementation of decision support (Beale et al. 2007)
-
10 Development of precise clinical processes using evidence-based medicine (Christensen et al. 2009; Fickenscher 2009)
-
11 Adoption of clinical protocols based on key risk-prone processes (Rotter et al. 2010) that prevent adverse events by encouraging efforts to drive efficiencies in processes which are highly prone to errors (Department of Health 2010a; Australian Commission on Safety and Quality in Health Care 2010; Committee on Quality of Health Care in America, Institute of Medicine 2001; Agency for Healthcare Research and Quality 2010).
-
12 Identify the right information at the right time for the patient condition (de Graaf et al. 2007)
-
13 Provide accessibility to consolidated data, information and medical expertise at the point of care, anywhere, at any time through better use of inexpensive technologies such as mobile devices (Blaya et al. 2007; Fickenscher 2010)
-
Referral / discharge
14 Reduction of errors in discharge summaries (Lisby 2005) �76 per cent errors
15 Provide cost-effective use of referral documentation for legal, logistics and management of care during the patient journey (Lisby et al. 2005)
-
16 Reduce errors in communication between services by ensuring the intended destination receives key administration data (for example, email with certification) (Kohn et al. 2000)
-
1 Quantified benefits have been highlighted in orange and are illustrated on the patient journey in Figure 3. 2 Note that Hopper and Jacobs (2009) ‘Halting the sepsis cascade’ paper was published in a vendor-specific publication, The
Cerner Quarterly, vol. 5, no. 1, pp. 15–23.

Page 3
Introduction
Document purpose and scope This report documents and identifies the benefits that may be attributed to the implementation of an EMR system and provides an estimate of the economic benefits that could be realised if introduced into the VPHS.
The document supports the aim of the Victorian Health Priorities Framework 2012–2022 to deliver the best possible healthcare to Victorians by using e-health and communications technology and enabling continuous improvements and innovations (Department of Health 2011).
Section 141(3)(e) of the Health Services Act 1988 makes provision for an ‘electronic records system established for the purpose of enabling the sharing of information in or between public hospitals and denominational hospitals for the treatment of patients at any time’ (AustLII 2010). The legislation therefore sets the scope for a VPHS EMR implementation such that efficient electronic sharing of information between health services can occur without requiring explicit consent.
Background Victoria is implementing a number of programs to modernise and replace ICT systems throughout the Victorian public healthcare sector and build the foundations of an EMR system.
The Board of Health Information Systems (BHIS) within the Department of Health is committed to using e-health tools to improve healthcare delivery and has endorsed the following high-level principles regarding the completion of an EMR for Victorian public hospitals:
• elimination of paper medical records in Victoria’s public hospitals
• one patient, one Victorian public hospital medical record
• clinical transformation through active decision support.
The aim is to enable timely access to critical patient information and the clinical evidence base, such as best practice clinical guidelines and clinical pathways to support a reduction in medical errors, support better clinical decision making, improve patient health outcomes, reduce risks and optimise healthcare delivery processes (Department of Health 2011).
To realise the full benefits of electronic information sharing, the solution needs to adopt national and international standards to ensure scalability, interoperability and ability to accommodate future integration with other clinical systems that exist across the care continuum.
Intended audience This document is intended for broad distribution across the Victorian public health sector, including:
• Department of Health management and staff
• public health services management and clinical staff
• public health services related professional bodies and educational institutions.

Electronic medical record benefits
Page 4
The healthcare opportunity
Benefits that ICT brings to quality care and demand management To address the increasing demand for quality healthcare, Victoria seeks to increase the effectiveness (efficiency and quality) of service provision through reducing the incidence of preventable and avoidable illness by reviewing practice variations and promoting a consistent and rapid adoption of best practice. This approach aligns well with clinical transformation which is defined as ‘a comprehensive, ongoing approach to care delivery excellence that measurably improves quality, enhances service, and reduces costs through the effective alignment of people , process , and technology ’ (Fickenscher 2010).
Health ICT systems can be considered the key ‘technology’ component (Figure 1) that will enable clinical transformation.
Figure 1: The Clinical Transformation Triad (Ficken scher 2010) ENABLE
CHANGE
The electronic medical record defined An EMR electronically documents all information that is administratively and clinically relevant to a patient’s hospital stay. An EMR system typically includes business modules that are used for registering a patient/client and a suite of clinical modules that support the services provided by the hospital. To realise the full benefits of an EMR, the ICT system’s functionalities cannot be implemented in isolation as patient treatment generally has touch points across a variety of functions and requires integrated and interoperable implementations.
An EMR system is recognised as a toolkit that enables clinical transformation becomes the source of truth for a patient's journey within hospitals and provides a framework for patient-centred healthcare delivery (Committee on Quality of Health Care in America, Institute of Medicine 2001; Bates & Gawande 2003; Hillestad 2005; Fickenscher 2010). Using an EMR enables continuous improvement in healthcare delivery by capturing structured information, supporting interoperability across systems and by enabling active decision support through the ability to access and interrogate atomic data elements.3 Despite this, the EMR adoption rate is low (Ashish et al. 2008) and there is currently no Australian hospital reaching Stage 7 on HiMSS EMR Adoption Model.4
3 Atomic data elements refer to data types that can no longer be broken down into smaller units and which have precise meaning or
semantics. A data element is the smallest named unit of information in the model that can be assigned a value, for example ‘DateTime of Observation’ and ‘Observation Note’ (National E-Health Transition Authority 2010b).
4 See: http://www.himssanalytics.org/docs/emram.pdf

Page 5
Benefits analysis
The literature identifies examples where an EMR system will be pivotal in enabling the efficient collection of meaningful, accurate and complete data that aid active clinical decision support and the development, implementation and optimisation of clinical pathways.
Rotter et al. (2010) describe clinical pathways as ‘structured multidisciplinary care plans used by health services to detail essential steps in the care of patients with a specific clinical problem. They aim to link evidence to practice and optimise clinical outcomes whilst maximising clinical efficiency.’
How an EMR will realise the benefits The key attributes of an EMR system that are important to deliver the benefits include:
• interoperability and messaging standards – adoption of interoperable technologies that adhere to technical standards to facilitate messaging (Standards Australia Limited 2010; Health Level 7 2010) and data exchange between hospitals (Department of Health 2010b)
• atomic data that can be interrogated – an EMR facilitates the computerisation of data entry to achieve legible documentation (Schuler 2010), the ability to query fine-grained data elements (Chen 2009) and provides the opportunity to evaluate medical record data in real time to inform clinical program and policy decisions (Paneth-Pollak et al. 2010)
• active decision support – standardisation of data elements and information models to ensure semantic interoperability enabling the implementation of active decision support (Beale et al. 2007).
The literature identifies a range of benefits that have been attributed to the implementation of standards, decision support and evidence-based processes and workflows. These benefits include:
• evidence-based clinical processes – development of precise clinical processes using evidence-based medicine (Christensen et al. 2009; Fickenscher 2009) driven by the need to provide expertise at the point of care (Christensen et al. 2009)
• clinically focussed business drivers – adoption of business models based on clinical processes and measured by clinical quality indicators (Australian Commission on Safety and Quality in Health Care 2010; Committee on Quality of Health Care in America, Institute of Medicine 2001) by supporting business workflows to automate and streamline processes
• clinically relevant information at the point of car e – access to consolidated data, information and medical expertise that allow clinical decisions to be made independent of location, time and context (Department of Health 2010c), where the EMR replaces the traditional paper medical record
• improved patient safety – preserves healthcare professionals’ implicit knowledge of patient safety and offers tools that provide decision support such as alerts for infectious diseases or allergies (Department of Health 2010a; Australian Commission on Safety and Quality in Health Care 2010; Committee on Quality of Health Care in America, Institute of Medicine 2001; Agency for Healthcare Research and Quality 2010). An EMR enables:
o reduction of human errors in prescribing treatment
o reduction of errors by providing active decision support to clinicians
o reduction of errors in primary source data, as it is entered immediately at the point of care by the health professional, or automatically by clinical monitoring tools
o reduction of poor quality data from hospital services due to reporting through provision of primary source data, eliminating need for potentially adapted aggregated data
• processes focusing on error prevention – adoption of clinical protocols based on key risk-prone processes (Rotter et al. 2010) that prevent adverse events by encouraging efforts to drive efficiencies in processes that are highly prone to errors (Department of Health 2010a; Australian Commission on Safety and Quality in Health Care 2010; Committee on Quality of Health Care in America, Institute of Medicine 2001; Agency for Healthcare Research and Quality 2010)

Electronic medical record benefits
Page 6
• coordinated processes – coordination of processes across the patient journey at the clinical, administrative and management levels (Reid et al. 2005; Grossman 2008)
• cost-effective access to data at the point of care – accessibility to consolidated data, information and medical expertise at the point of care through better use of inexpensive technologies such as mobile devices (Department of Health 2010d; Fickenscher 2010). This reduces healthcare cost by preventing duplication of data, and encourages local accountability through down-up performance measurement
• efficiency tool – provides a tool for managers, executives, and auditors to measure hospital performance based on primary source data by giving access to atomic structured information in real time (as opposed to, for example, scanned documents). This dramatically reduces the time between the collection of data and the analysis of key performance indicators and offers unparalleled richness and visibility of operational activities from the point of care
• e-health tool – the EMR places the patient at the centre of care delivery and underpins a Personally Controlled Electronic Health Record (PCEHR). The resulting outcomes from an EMR as a key e-health tool include:
o providing a central repository for clinically relevant information
o supporting data collection used for secondary uses (for example, research)
o supporting effective implementation of public health strategies
o improved ability to respond to major incident/disaster needs in the community.
The section below describes where in the patient journey the identified benefits occur.
The benefits along a patient journey A patient journey can be described as all sequential steps involving the movement of the patient and all relevant information (for example, from emergency department to ward or X-ray department), and is performed within an accreditation or standards framework (Australian Council on Healthcare Standards 2009).
The patient journey is typically divided into three distinct stages: admission, treatment and discharge (Figure 2). The introduction of an EMR system will enable administrative as well as clinical benefits to be gained across all three stages of the patient journey.
Figure 2: Patient journey
Each patient journey stage follows a similar process in which patients are admitted, treated and moved to the next stage of the patient journey. The treatment stage consists of one or more ‘episodes of care’, where an ‘episode of care’ reflects the changing diagnosis or treatment of the patient.

Page 7
The benefits identified in the literature review (Table 1 on page 2) are depicted where they occur on the patient journey in Figure 3 below. The quantitative benefits and the qualitative benefits sections below provide more detailed information on each of the benefits identified.
Figure 3: Patient journey with identified EMR benef its
Quantitative benefits Of the 153 papers reviewed, 40 papers provided identifiable benefits, of which four papers presented quantitative benefits that can be attributed to the implementation of health ICT systems. Three studies quantified benefits attributable to the implementation of clinical pathways and medication management using an EMR system. The studies in Table 2 demonstrate that an EMR system may improve clinical outcomes and help drive efficiencies by decreasing (18–30 per cent) the patient’s LOS in hospitals. One study quantified the reduction of errors (76 per cent) in discharge summaries.
Table 2: Quantitative benefits identified
No. Benefits Quantified benefit
Admission assessment
5 Average cost benefit of processing an electronic patient referral in a hospital
�32 per cent processing referral cost (Cannaby et al. 2004)
Treatment / intervention
6 7
Improved clinical outcomes through clinical pathway
sepsis: �18 per cent LOS (Hopper & Jacobs 2009) pneumonia: �20 per cent LOS (Rotter et al. 2010)
8 Reduced surgical adverse events through medication management
�30 per cent LOS (Murphy et al. 2009)
Referral / discharge
14 Reduction of errors in discharge summaries �76 per cent errors (Lisby et al. 2005)
Hopper and Jacobs (2009) demonstrated that the implementation and use of an EMR as a tool to improve the outcomes for sepsis treatment had significant results. Their study at the Methodist North Hospital showed that LOS ‘for patients treated by sepsis complications fell to 13.6 days from 16.5 days’ (p. 22), an 18 per cent reduction in LOS. This reduction equated to ‘a positive financial impact of nearly [USD] $2 million based on efficiencies in care delivery and documentation of severe sepsis’ (p. 22).
The importance of addressing underlying causes of adverse events to reduce the LOS is illustrated in a study by Hauck and Zhao (2011). Their study was performed on VAED data for 2005–06 and shows that a hospital stay carries a 5.5 per cent risk of an adverse drug reaction, 17.6 per cent risk of infection and 3.1 per cent risk of ulcer for an average episode. Further to this, they found that each additional night in hospital increases the risk by 0.5 per cent for adverse drug reactions, 1.6 per cent for infections, and 0.5 per cent for ulcers.
Electronic medical record benefits
Page 8
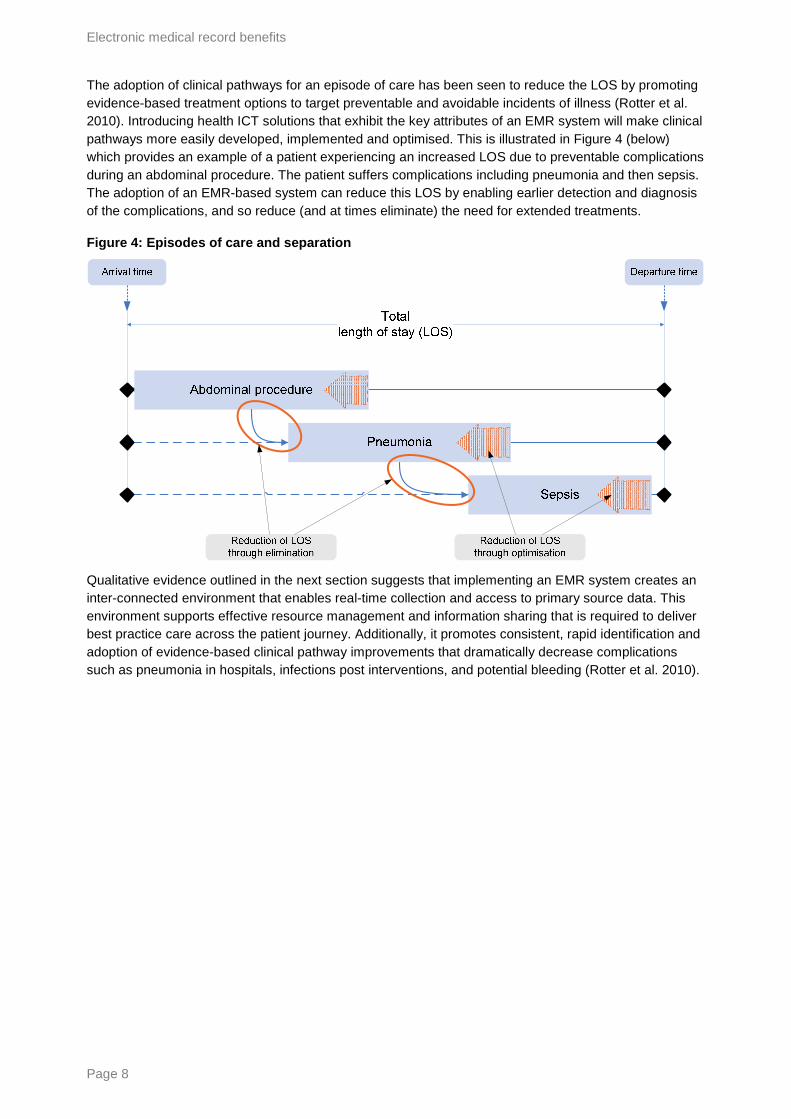
The adoption of clinical pathways for an episode of care has been seen to reduce the LOS by promoting evidence-based treatment options to target preventable and avoidable incidents of illness (Rotter et al. 2010). Introducing health ICT solutions that exhibit the key attributes of an EMR system will make clinical pathways more easily developed, implemented and optimised. This is illustrated in Figure 4 (below) which provides an example of a patient experiencing an increased LOS due to preventable complications during an abdominal procedure. The patient suffers complications including pneumonia and then sepsis. The adoption of an EMR-based system can reduce this LOS by enabling earlier detection and diagnosis of the complications, and so reduce (and at times eliminate) the need for extended treatments.
Figure 4: Episodes of care and separation
Qualitative evidence outlined in the next section suggests that implementing an EMR system creates an inter-connected environment that enables real-time collection and access to primary source data. This environment supports effective resource management and information sharing that is required to deliver best practice care across the patient journey. Additionally, it promotes consistent, rapid identification and adoption of evidence-based clinical pathway improvements that dramatically decrease complications such as pneumonia in hospitals, infections post interventions, and potential bleeding (Rotter et al. 2010).

Page 9
Qualitative benefits The literature documents qualitative benefits that can be derived by introducing health ICT systems, such as reducing the reliance on tools such as pen, paper and the human memory (National E-Health Transition Authority 2010a), reducing duplication of administration data or providing the right information at the right time for the patient condition. Table 3 summarises 11 qualitative benefits that were identified.
Table 3: Qualitative benefits identified
No. Benefits
Across the whole patient journey
1 Entering data once and using it many times (Garde 2006)
2 Computerisation of data entry enabling the achievement of legible documentation (Schuler 2010); increasing the system’s ability to ensure completeness, consistency and legibility of medical records (Paneth-Pollak et al. 2010); and providing the opportunity to evaluate medical record data in real time to inform clinical program and policy decisions (Paneth-Pollak et al. 2010)
3 Coordination of processes across the patient journey at the clinical, administrative and management levels (Reid et al. 2005; Grossman 2008)
4 Reducing duplication of administration data by providing access to all the team (Australian Nursing Federation 2007)
Admission assessment Administration and clinical assessment to determine the type of intervention required for the treatment stage
1-4 As above
Treatment / intervention
9 Standardisation of data elements and information models to ensure semantic interoperability enabling the implementation of decision support (Beale et al. 2007)
10 Development of precise clinical processes using evidence-based medicine (Christensen et al. 2009; Fickenscher 2009)
11 Adoption of clinical protocols based on key risk-prone processes (Rotter et al. 2010) that prevent adverse events by encouraging efforts to drive efficiencies in processes that are highly prone to errors (Department of Health 2010a; Australian Commission on Safety and Quality in Health Care 2010; Committee on Quality of Health Care in America, Institute of Medicine 2001; Agency for Healthcare Research and Quality 2010)
12 Identify the right information at the right time for the patient condition (de Graaf et al. 2007)
13 Provide accessibility to consolidated data, information and medical expertise at the point of care, anywhere, at any time through better use of inexpensive technologies such as mobile devices (Blaya et al. 2007; Fickenscher 2010)
Referral / discharge
15 Provide cost-effective use of referral documentation for legal, logistics and management of care during the patient journey (Lisby et al. 2005)
16 Reduce errors in communication between services by ensuring reception of key administration data to the intended destination (for example, email with certification) (Kohn et al. 2000)

Electronic medical record benefits
Page 10
Continuous optimisation Currently within the VPHS, it is extremely costly and time intensive to collect accurate and complete data to identify, develop and implement business (including clinical) process improvements. As a consequence, this important activity is not undertaken frequently and/or is limited to only specific processes and interventions.
Implementing an EMR system, where all data is captured and stored in a structured and semantically well-defined atomic form will enable Victorian public hospitals to readily identify and implement process improvements. This aligns well with the concept of using continuous business process optimisation (BPO) to drive process improvements, resulting in better health outcomes and a more efficient healthcare system.
Vergidis et al. (2008) describe BPO as the automated improvement of business processes using pre-specified quantitative measures of performance (objectives). The deliverables in this process are continuously refined and optimised in a basic lifecycle (Figure 5), where the ‘define’ step includes defining the organisation's strategic goals and purposes, as well as identifying the organisation's customers. The ‘measure’, ‘analyse’, and ‘improve’ steps of the lifecycle align the business processes to realise the organisation’s goals.
Figure 5: Business process optimisation lifecycle
Improve D
efine
Measure
Analyse
Applying this approach to the VPHS will help to ensure that all clinical and business processes that are supported by the EMR system may be continuously monitored, optimised and deployed on a local and/or statewide basis as required. Current activities such as the Redesigning Hospital Care Program5 will be able to be set up as permanent continuous optimisation programs across the VPHS.
Tip of the iceberg The quantified benefits identified in Table 2 pertain to reductions of preventable in-hospital complications and improvements to referral processes. It is anticipated that these benefits represent just the tip of the iceberg and the full benefits to be gained from widespread use of continuously optimised clinical pathways will only be understood once an EMR system is operating across the VPHS.
5 See: http://www.health.vic.gov.au/redesigningcare/index.htm

Page 11
During the analysis, we identified an opportunity to estimate the economic benefits that may be realised through implementing an EMR system. The estimation is based on the extrapolation of two studies:
• Rotter et al. (2010) demonstrated that the introduction of clinical pathways reduced preventable in-hospital complications by up to 42 per cent and found a clear correlation with ‘a decrease in hospital costs/charges’ due to improvements in treating infections [sepsis], pneumonia and bleeding (p. 2).
• Ehsani et al. (2006) quantified the financial impact that preventable in-hospital complications impose on Victorian hospitals. Ehsani’s key finding was that the average expenditure for preventable in-hospital complications is $6,826 per admitted episode, resulting in a total cost of $460 million for the 67,435 incidents in 45 major hospitals in 2003–04 (see Appendix 1 Benefits extrapolation methodology).
Ehsani et al. (2006) used data from the VAED, and although no statistical analysis was undertaken to confirm a relationship between the clinical information in the medical record and the VAED data, our analysis suggests that if one accepts the assumption that an EMR system will make clinical pathways more easily developed and implemented across VPHS, there could be significant reductions of preventable in-hospital complications. This assumption is based on well-substantiated evidence (see pages 5 and 6) that EMR systems will be pivotal in enabling the efficient collection of meaningful, accurate and complete data that supports active clinical decision support and facilitates the development and implementation of clinical pathways.
By extrapolating the potential reductions of preventable in-hospital complications and their related costs based on the above studies, there is an opportunity to reduce complications by 30 per cent (see Appendix 1: Benefits extrapolation methodology) and achieve a released value of up to $296 million (Table 4). The released value should not be considered a financial saving, but rather a released capacity to treat more patients with the same fixed resources.
Table 4: Health economic benefits through reduction of preventable complications
Year Total hospital separations
Preventable complications
Potential reduction in preventable complications 6
Potential released value ($m) 7
2003–048 979,834 67,435 20,230 $138.09
2003–049 1,141,545 79,637 23,891 $198.39
2009–1010 1,375,320 118,970 35,691 $296.38
6 Assuming a 30 per cent reduction of preventable in-hospital complications. 7 Assuming average expenditure for preventable in-hospital complications is $6,826 in 2003–04 and $8,304 in 2009–10. 8 2003–2004 numbers based on the study of 45 major Victorian hospitals by Ehsani et al. (2006). 9 2003–2004 numbers based on Department of Health VAED data for all reporting Victorian Public Hospitals, excluding ICD-10-AM
diagnosis codes in the O-range (obstetrics). 10 2009–2010 numbers based on Department of Health VAED data for all reporting Victorian Public Hospitals, excluding ICD-10-
AM diagnosis codes in the O-range (obstetrics).

Electronic medical record benefits
Page 12
Conclusion
Although further evidence is required to confirm a direct link between implementing an EMR system and the reduction of preventable in-hospital complications, there is growing recognition of the critical role an EMR system will play in clinical transformation.
The literature provides evidence that an EMR system will be pivotal in enabling the efficient collection of meaningful, accurate and complete data that supports active clinical decision support and the development and implementation of clinical pathways.
The literature highlights 16 benefits (Table 1) from both administrative and clinical perspectives that can be attributed to implementing a health ICT system.
It is anticipated that, once implemented, an EMR solution will improve the ability of VPHS to achieve sustainable service delivery by providing the facility to measure the effectiveness of processes and to target improvements to deliver the services more efficiently. The EMR system will enable staff to drive continuous evidence-based improvements and error reduction programs in the healthcare sector through clinical transformation to establish a standardised approach for the provision of care with active decision support.
The result will be an opportunity to continuously optimise our healthcare, significantly reduce preventable in-hospital complications and thereby achieve reduction in LOS, improve patient outcomes and release value to treat more patients with the same fixed resources.

Page 13
Appendices
Appendix 1: Benefit extrapolation methodology Two studies were used to extrapolate the potential benefits that could be achieved by implementing standardised clinical pathways into the Victorian public hospitals using an EMR system. The studies (detailed below) are by Ehsani et al. (2006) using VAED data to estimate the cost of preventable in-hospital complications, and Rotter et al. (2010) on the impact that introducing clinical pathways has on such complications.
Ehsani study:
Ehsani et al. (2006) demonstrated that the total healthcare cost of unexpected adverse events, or preventable in-hospital complications, in Victoria reached $460 million in the 2003–04 financial year. Ehsani et al. (2006) found that:
• 6.88 per cent of admitted episodes had at least one adverse event
• 979,834 admitted episodes in 2003–04 resulted in 67,435 episodes with at least one adverse event
• admitted episodes without an adverse event had an average LOS of 2.49 days, at an average cost of $2,181
• admitted episodes with an adverse event had an average LOS of 12.61 days (or 10 days more than without adverse events), at an average cost of $14,027.
Once the average cost was adjusted for age and comorbidity, Ehsani et al. (2006) found that the additional cost for each admitted episode with an adverse event was $6,826.
Rotter study:
Rotter et al. (2010) demonstrated through a comparison of 27 studies from eight countries, spanning the years 1987 until 2006, that in-hospital complications were reduced by 42 per cent once clinical pathways were introduced.
Benefit extrapolation
To estimate the potential benefits that could be derived by using an EMR system to introduce standardised clinical pathways into Victorian public hospitals, the following steps were undertaken:
1. The cost burden of unexpected adverse events was estimated using ‘The incidence and cost of adverse events in Victorian hospitals 2003–2004’ by Ehsani et al. (2006). The cost identified in the study was adjusted for inflation using the Reserve Bank of Australia’s inflation calculator11 to reach an equivalent additional cost of $8,304 for each admitted episode with an adverse event in 2009–10.
2. Potential reduction of unexpected adverse events was estimated using ‘Clinical pathways: effects on professional practice, patient outcomes, length of stay and hospital costs’ by Rotter et al. (2010). While acknowledging that clinical pathways are already present across the VPHS, it has been assumed that a 30 per cent reduction of in-hospital complications may be achieved through improved ability to standardise, optimise and deploy new evidence-based processes across the VPHS. This will be particularly true for environments where the clinical pathways are currently paper-based or non-existent. A 30 per cent reduction of in-hospital complications is relatively conservative when compared to findings by Rotter et al. (2010).
3. Adjustments were made to accommodate changes to the Victorian prefixing of ICD-10-AM obstetric diagnosis codes since 2003–04. All obstetric cases have been excluded to ensure comparability of the data used for benefits extrapolation.
11 http://www.rba.gov.au/calculator/annualDecimal.html (accessed 31 January 2011)

Electronic medical record benefits
Page 14
It should be noted that, even after removing the obstetrics codes from the data, unexpected adverse events increased by 33 per cent while the number of separations increased by around 16 per cent. The reason for this increase has not been investigated at the time of writing this paper.
Benefits extrapolation results
The following tables (Table 5 and Table 6) illustrate the results of the benefits extrapolation using Department of Health VAED data.
Table 5: Total cost of adverse events in Victoria
Year Total hospital separations
Preventable complications
Average extra cost of preventable complications
Total cost of preventable complications ($m)
2003–200412 979,834 67,435 (6.88%) $6,826 $460.311
2003–200413 1,141,545 79,637 (6.98%) $6,826 $543.602
2009–201014 1,375,320 118,970 (8.65%) $8,304 $987.927
Table 6: Health economic benefits through reduction of preventable complications
Year Total hospital separations
Preventable complications
Potential reduction in preventable complications 15
Potential released value ($m) 16
2003–200417 1,141,545 79,637 23,891 $198.391
2009–201018 1,375,320 118,970 35,691 $296.378
12 2003–2004 numbers based on the study of 45 major Victorian hospitals by Ehsani et al. (2006). 13 2003–2004 numbers based on Department of Health VAED data for all reporting Victorian Public Hospitals,
excluding ICD-10-AM diagnosis codes in the O-range (obstetrics). 14 2009–2010 numbers based on Department of Health VAED data for all reporting Victorian Public Hospitals,
excluding ICD-10-AM diagnosis codes in the O-range (obstetrics). 15 Assuming a 30 per cent reduction of preventable in-hospital complications. 16 Assuming average expenditure for preventable in-hospital complications is $6,826 in 2003–04 and $8,304 in
2009–10. 17 2003–2004 numbers based Department of Health VAED data for all reporting Victorian Public Hospitals. 18 2009–2010 numbers based Department of Health VAED data for all reporting Victorian Public Hospitals.

Page 15
Appendix 2: Cited references Agency for Healthcare Research and Quality 2010, ‘AHRQ study shows using bar-code technology with eMAR reduces medication administration and transcription errors’, viewed 18 January 2011, <http://www.ahrq.gov/news/press/pr2010/emarpr.htm>.
Ashish K, Doolan D, Grandt D, Scott T, Bates D 2008, ‘The use of health information technology in seven nations’, Journal of Medical Informatics, vol. 77, no. 12, pp. 848–54.
Australasian Legal Information Institute (AustLII) 2010, ‘Confidentiality – as per Health Services Act 1988 – s. 141(3)(e)’, viewed 27 October 2010, <http://www.austlii.edu.au/au/legis/vic/consol_act/hsa1988161/s141.html>.
Australian Commission on Safety and Quality in Health Care 2010, viewed 21 May 2010, <http://www.safetyandquality.gov.au>.
Australian Council on Healthcare Standards 2009, Piloting innovative accreditation methodologies: patient journey methodologies: final report, Commonwealth Government of Australia, Department of Health and Ageing on behalf of the Australian Commission on Safety and Quality in Health Care, Canberra.
Australian Nursing Federation 2007, Nurses and information technology, Commonwealth Government of Australia, Canberra.
Bates D and Gawande A 2003, ‘Improving safety with information technology’, The New England Journal of Medicine, vol. 348, no. 25, pp. 2526–34.
Beale T, Chen R, Leslie H, Frankel H, Garde S, Sundvall E, Schuler T, van der Linden H 2007, ‘Implementing open EHR’, Ocean Informatics, presentation at MedInfo, 19 August 2007.
Blaya J, Shin S, Yagui M, Yale G, Suarez C, Asencios L, Cegielski J, Fraser H 2007, ‘A web-based laboratory information system to improve quality of care of tuberculosis patients in Peru: functional requirements, implementation and usage statistics’, BMC Medical Informatics and Decision Making, vol. 7, no. 33, doi:10.1186/1472-6947-7-33.
Cannaby S, Wanscher C, Pedersen C, Voss H 2004, The cost benefit of electronic patient referrals in Denmark, published by ACCA and MedCom in collaboration with the European Commission Information Society Directorate.
Chaudhry B, Wang J, Wu S, Maglione M, Mojica W, Roth E, Morton SC, Shekelle PG 2006, ‘Systematic review: impact of health information technology on quality, efficiency, and costs of medical care’, American College of Physicians, Annals of Internal Medicine, vol. 144, pp. 742–52.
Chen R 2009, Towards interoperable and knowledge-based electronic health records using archetype methodology, Department of Biomedical Engineering, Linköping University, Linköping.
Christensen C, Grossman J, Wang J 2009, The innovator’s prescription: a disruptive solution for health care, McGraw Hill Professional, New York.
Committee on Quality of Health Care in America, Institute of Medicine 2001, Crossing the quality chasm: a new health system for the 21st century, The National Academies Press, Washington DC.
Council of Australian Governments 2009, National partnership agreement on e-health, Council of Australian Governments’ 28th meeting, 7 December 2009.
de Graaf J, Vlug A, van Boven G 2007, ‘Dutch virtual integration of healthcare information’, Methods of Information in Medicine, vol. 46, no.4, pp. 458–62.
Deloitte 2008, National e-health strategy, National E-Health and Information Principal Committee, Canberra.
Department of Health 2010a, Patient safety indicators: AusPSI, State Government of Victoria, Melbourne.

Electronic medical record benefits
Page 16
Department of Health 2010b, HealthSMART HL7 2.4 implementation guide, State Government of Victoria, Melbourne.
Department of Health 2010c, HealthSMART clinical systems overview, State Government of Victoria, Melbourne.
Department of Health 2010d, HealthSMART common technology infrastructure overview, State Government of Victoria, Melbourne.
Department of Health 2011, Victorian Health Priorities Framework 2012–2022, State Government of Victoria, Melbourne.
Department of Human Services 2008, Redesigning Hospital Care Program: framework for health services, State Government of Victoria, Melbourne.
Ehsani J, Jackson T, Duckett S 2006, ‘The incidence and cost of adverse events in Victorian hospitals 2003–2004’, Medical Journal of Australia, vol. 184, no. 11, pp. 551–55.
Fickenscher K 2009, ‘Clinical transformation: turning rhetoric into reality’, presentation, Indian Institute of Health Management Research viewed 21 May 2010, <http://www.iihmrdelhi.org/health%20conclave/DR.%20KEVIN.pdf>.
Fickenscher K 2010, ‘The value of clinical transformation’, Strategic Initiatives, Dell Services, viewed 18 January 2011, <http://i.dell.com/sites/content/public/solutions/healthcare/en/Documents/clinical-transformation.pdf>.
Garde S 2006, ‘Archetypes: the building blocks for electronic health records’, Central Queensland University, presentation, Austin Centre for Applied Clinical Informatics, viewed 18 January 2011, <www.acaci.org.au/resources/informatics/austin_openEHR_Garde_compressed.pdf>.
Grossman J 2008, ‘Disruptive innovation in health care: challenges for engineering’, The Bridge, vol. 38, no. 1, pp. 10–16.
Hauck K and Zhao X 2011, How dangerous is a day in hospital? A model of adverse events and length of stay for medical inpatients, Imperial College London, London, UK and Monash University, Melbourne, Australia.
Health Level 7 2010, viewed 18 January 2011, <http://www.hl7.org/>.
Hillestad R, Bigelow J, Bower A, Girosi F, Meili R, Scoville R, Taylor R 2005, ‘Can electronic medical record systems transform health care?: potential health benefits, savings, and costs’, Health Affairs, vol. 24, no. 5, pp. 1103–17.
HIMSS Analytics 2008, ‘The EMR adoption model (EMRAM)’, HIMSS Analytics, LLC, viewed 17 June 2011, <http://www.himssanalytics.org/docs/emram.pdf>.
Hopper K and Jacobs P 2009, ‘Halting the sepsis cascade’, The Cerner Quarterly, vol. 5, no. 1, pp. 15–23.
Kaplan C 2002, ‘The millions that a major computer manufacturer almost saved’, Proceedings of the Fourth Annual Simulation Solutions Conference, Institute of Industrial Engineers, Norcross, GA.
Kohn L, Corrigan J, Donaldson M 2000, To err is human: building a safer health system, The National Academies Press, Washington DC.
Lisby M, Nielsen LP, Mainz J 2005, ‘Errors in the medication process: frequency, type, and potential’, International Journal for Quality in Health Care, vol. 17, no. 1, pp. 15–22.
Morrison B and Bird B 2003, ‘A methodology for modelling front office and patient care processes in ambulatory health care’, Simulation Conference 2003, vol. 2, pp. 1882–86.
Murphy E, Oxencis C, Klauck J, Meyer D, Zimmerman J 2009, ‘Medication reconciliation at an academic medical center: implementation of a comprehensive program from admission to discharge’, American Journal of Health-System Pharmacy, vol. 66, no. 23, pp. 2126–31.
Page 17
National E-Health Transition Authority 2010a, ‘eHealth: why eHealth?’, viewed 16 February 2011, <http://www.ehealthinfo.gov.au/what-is-e-health/why-e-health/>.
National E-Health Transition Authority 2010b, ‘Data specifications and structured document templates: guide for use’, viewed 24 August 2011, <http://www.nehta.gov.au/>.
Paneth-Pollak R, Schillinger JA, Borrelli JM, Handel S, Pathela P, Blank S 2010, ‘Using STD electronic medical record data to drive public health program decisions in New York City’, American Journal of Public Health, vol. 100, no. 4, pp. 586–90, doi:10.2105/AJPH.2009. 175349.
Reid PW, Compton D, Grossman J, Fanjiang G 2005, Building a better delivery system: a new engineering/healthcare partnership, Committee on Engineering and the Health Care System, Institute of Medicine and National Academy of Engineering, The National Academies Press, Washington DC.
Rotter T, Kinsman L, James E, Machotta A, Gothe H, Willis J, Snow P, Kugler J 2010, ‘Clinical pathways: effects on professional practice, patient outcomes, length of stay and hospital costs’, Cochrane Database of Systematic Reviews, vol. 3, art. no. CD006632, doi: 10.1002/14651858. CD006632.pub2.
Schuler R 2010, ‘The smart grid: a bridge between emerging technologies, society, and the environment’, The Bridge, vol. 40, no. 1, pp. 42–49.
Standards Australia Limited 2010, ‘Standards Australia eHealth’, viewed 18 January 2011, <http://www.e-health.standards.org.au/Home/Publications.aspx>.
Vergidis K, Tiwari A, Majeed B 2008, ‘Business process analysis and optimization: beyond reengineering’, IEEE Transactions on Systems, Man, and Cybernetics—Part C: Applications and Reviews, vol. 38, no. 1, pp. 69–82.

Electronic medical record benefits
Page 18
Appendix 3: Other references Australian Bureau of Statistics 2008, Population projections, Australia, 2006 to 2101, cat. 3222.0 Australian Government, Canberra.
Australian Institute of Health and Welfare 2009, Australian hospital statistics 2007–08, Health services series, no. 33, cat. HSE 71, Canberra.
Bartlett C, Boehncke K, Wallace V, Johnstone-Burt A 2010, ‘Optimising e-health value: using an investment model to build a foundation for program success’, Booz & Company Inc., viewed 21 May 2010, <http://www.booz.com/media/file/Optimising_e-Health_Value.pdf>.
Calver J, Brameld KJ, Preen DB, Alexia SJ, Boldy DP, McCaul KA 2006, ‘High-cost users of hospital beds in Western Australia: a population-based record linkage study’, Medical Journal of Australia, vol. 184, no. 8, pp. 393–97.
Canada Health Infoway 2009, ‘Making health information work better for Canadians’, Corporate Business Plan 2009–2010, viewed 26 May 2010, <http://www.infoway-inforoute.ca/flash/ar-bp/en/bp/index.html>.
Commonwealth Government of Australia 2010, ‘Budget 2010–11, part 2: expense measures’, viewed 24 May 2010, <http://www.budget.gov.au/2010-11/content/bp2/html/bp2_expense-13.htm>.
Department of Health 2009, Definitive data report 2008–09, Funding Policy and Data Hospital and Health Service Performance Division (internal use only), State Government of Victoria, Melbourne.
Department of Health 2010e, Better skills, best care: workforce design strategy, State Government of Victoria, Melbourne.
Department of Human Services 1998, PRS/2 manual part A: definitions and system parameters, State Government of Victoria, Melbourne.
Eber R, Laxminarayan R, Perencevich E, Malani A 2010, ‘Clinical and economic outcomes attributable to healthcare-associated sepsis and pneumonia’, Archive of Internal Medicine, vol. 170, no. 4, pp. 347–53.
Gogler J, Hullin C, Vaughan V, Searle C 2010, ‘The chaos in primary nursing data: good information reduces risk’, Electronic Journal of Health Informatics, vol. 5, no. 1, e. 6.
Health Information Technology 2010, Electronic health records and meaningful use, The Office of the National Coordinator for Health Information Technology, US Department of Health and Human Service, Washington DC.
HISA 2010, ‘Health Informatics Society of Australia’, viewed 9 June 2010, <http://www.hisa.org.au/>.
Hugh L 2010, ‘Electronic medication management’, Health informatics – an overview, IOS Press, Amsterdam, pp. 157–68.
Kaiser Permanente 2010, ‘Kaiser Permanente completes electronic health record implementation’, press release, 3 March 2010, viewed 26 May 2010, <http://xnet.kp.org/newscenter/pressreleases/nat/2010/030310ehrcomplete.html>.
Kolodner R 2005, ‘Statement of Robert M. Kolodner’, US Department of Veterans Affairs, viewed 26 May 2010, <http://www4.va.gov/OCA/testimony/hgrc/050929RK.asp>.
KPMG 2009, ‘Health workforce in Australia and factors for current shortages’, Australian Health Workforce Taskforce, viewed 20 May 2010, <http://www.nhwt.gov.au/publications.asp>.
Krizner K 2004, ‘Clinical transformation initiative starts with a total vision’, Managed Healthcare Executive, viewed 24 May 2010, <http://managedhealthcareexecutive.modernmedicine.com/mhe/Technology/Clinical-transformation-initiative-starts-with-a-t/ArticleStandard/Article/detail/127457>.

Page 19
McGrath K, Bennett D, Ben-Tovim D, Boyages S, Lyons N, O’Connell T 2008, ‘Implementing and sustaining transformational change in healthcare: lessons learnt about clinical process redesign’, Medical Journal of Australia, vol. 188, no. 6, pp. S32–35.
Mental Health Council of Australia 2007, ‘Access to health services by people with mental illness’, Australian Human Rights Commission, viewed 20 May 2010 <http://www.hreoc.gov.au/disability_rights/health/mhca.doc>.
National e-Health Transition Authority 2010c, ‘NEHTA sets direction for electronic messaging in health’, viewed 24 May 2010, <http://www.nehta.gov.au/media-centre/nehta-news/423-nehta-sets-direction-for-electronic-messaging-in-health>.
National e-Health Transition Authority 2010d, ‘Coordinated care: what is a PCEHR?’, viewed 6 October 2010, <http://www.nehta.gov.au/coordinated-care/what-is-a-pcehr>.
Nictiz 2008, eHealth in the Netherlands, National IT institute for Healthcare, Netherlands.
PM Hut 2010, ‘Project management approach for business process improvement’, viewed 24 May 2010, <http://www.pmhut.com/project-management-approach-for-business-process-improvement>.
Wikipedia 2010, ‘VistA’, viewed 26 May 2010, <http://en.wikipedia.org/wiki/VistA>.
Wikipedia 2010, ‘Business process improvement’, viewed 24 May 2010, <http://en.wikipedia.org/wiki/Business_process_improvement>.
WorldVistA 2010, ‘VistA History’, viewed 26 May 2010, <http://worldvista.org/AboutVistA/VistA_History>.
Young P, Olsen L, McGinnis J 2010, ‘Value in healthcare: accounting for cost, quality, safety, outcomes, and innovation’, Roundtable on evidence-based medicine, Institute of Medicine, The National Academies Press, Washington DC.