effects of physical activity on psychological variables in ...€¦ · effects of physical activity...
TRANSCRIPT

Pediatric Exercise Science, 1994, 6, 406-423 O 1994 Human Kinetics Publishers, Inc.
Effects of Physical Activity on Psychological Variables in Adoiescents
Karen J. Calfas and Wendell C. Taylor
To identify the most consistent relationships among psychological variables and physical activity in youth (ages 11-21 years), 20 articles on depression, anxiety, stress, self-esteem, self-concept, hostility, anger, intellectual func- tioning, and psychiatric disorders were reviewed. Physical activity was con- sistently related to improvements in self-esteem, self-concept, depressive symptoms, and anxietylstress. The effect sizes were +.12, -.15, and -.38 for self-esteemlself-concept, stresslanxiety, and depression, respectively. The evidence for hostilitylanger and academic achievement was inconclusive. No negative effects of physical activity were reported. The literature suggests that physical activity in youth is psychologically beneficial. More research is needed to confirm previous findings. Adolescents should engage in moder- ate or vigorous aerobic activity approximately three times per week for a total of at least 60 minutes per week.
In historical times, a healthy mind in a healthy body was a valued concept of Greek tradition. In contemporary times, the mind-body unity is evident in concepts such as high-level wellness, optimal health, and holistic medicine. Both the historical and contemporary perspectives emphasize the importance of psychological and mental health, as well as physical health. Therefore, in addition to the physical effects of activity, it is important to review the research on the psychological effects of physical activity in adolescents. No comprehensive reviews on the psychological effects of physical activity in adolescents (ages 11-21) were found.
Psychological and mental health can be defined in a variety of ways. For the purpose of this review, the psychological variables of primary interest are depression, anxiety, stress, self-esteem, self-concept, hostility, anger, intellectual functioning, and psychiatric disorders defined by the Diagnostic and Statistical Manual of Mental Disorders (DSM-111-R, 1).
These variables were selected for several reasons. First, the literature on the psychological effects of physical activity on adults suggests that these vari- ables are important (2, 3, 4). Significant relationships with these variables have been documented in studies with adults. Second, the selected variables cover a
Karen J. Calfas is with the Department of Health Promotion at San Diego State University, San Diego, California 92182-0567. Wendell C. Taylor is with the School of Public Health at the University of Texas-Houston, Health Science Center, Houston, TX 77225.

Psychological Variables - 407
range of effects from maintaining psychological and mental health to ameliorating and managing psychiatric disorders. The range of variables permits the review of nonclinical and clinical adolescent populations and of preventive and therapeutic measures. Third, the selected variables are appropriate for the developmental level of our age group (ages 11-21), Self-esteem and academic performance (intellectual functioning) are salient concerns for this age group. Moreover, de- pression, suicide, and psychiatric disorders are prevalent in this age group (5). Fourth, several variables can show either positive or negative psychological effects from participation in physical activity (e.g., stress, self-esteem, anxiety). In summary, the selected psychological variables provide a range and balance to review the positive and negative psychological effects of physical activity in both nonclinical and clinical populations.
Method of Review
Index Medicus and social science data bases were searched over the last 10 years for studies or review articles regarding physical activity or exercise and psychological variables including depression, anxiety, stress, self-esteem, self- concept, hostility, anger, intellectual functioning, and psychiatric disorders. Also, we conducted personal retrieval searches. Studies included in this review were identified by these search techniques and relevant references before 1983 were included.
We used several criteria to select and classify studies. Studies that included subjects in the 11- to 21-year-old age range were included in the review. Studies that had a significant proportion of subjects in the age range of interest were also included if they had good scientific merit. Studies including apparently healthy adolescents were of particular interest. Studies examining adolescents with psychological problems or diagnosed with psychological illnesses were included in the High-Risk Populations section of this review. This review focuses on studies that used a randomized controlled, a prospective observational, or a cross-sectional observational design. We excluded conclusions drawn from case reports and expert opinion. Data from unpublished studies and dissertations were not included.
Results and Discussion
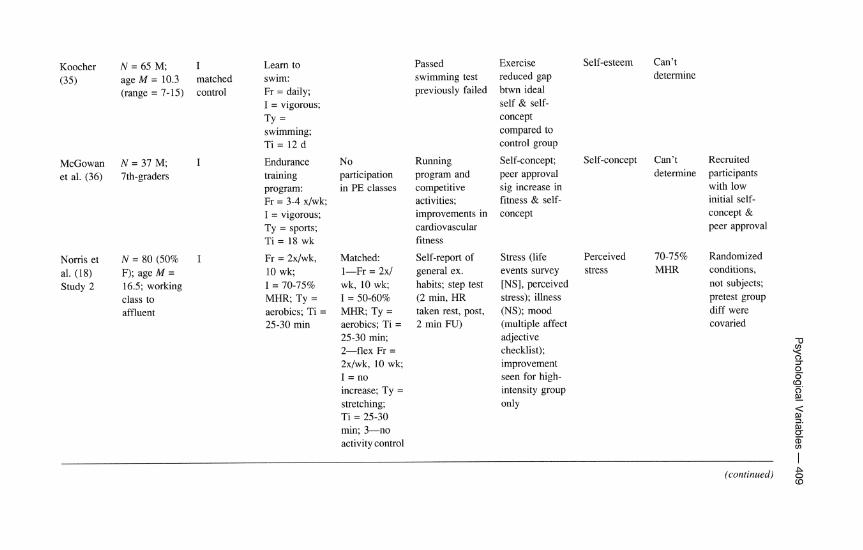
Characteristics of the studies included in this review are described in Table 1. Subjects are classified by age, gender, socioeconomic status, and ethnicity when reported. Study design is classified by level of evidence collected, including (a) Level I, a randomized controlled trial or quasi-experimental design; (b) Level IIA, a prospective observational study, or (c) Level IIB, cross-sectional observational study. Physical activity measures and interventions are described, including the frequency, intensity, type, and time (FITT) where possible. Charac- teristics of intervention and control groups are specified. Dependent variables of psychological function are identified. Particular attention was given to possible dose-response relationships.
As Table 1 indicates, there is a general lack of experimental research on the psychological effects of physical activity among adolescents. Regarding

Table 1 Study Characteristics and Results on the Relation of Physical Activity (PA) and Psychological Variables in Adolescents
Signif. mental health
Citation Subjects Design Intervention Control Measure Effect outcomes Dose Comments $
Apparently healthy population g 9 Bahrke & N = 65 (54% I Fr = one Read for 15 HR measured Anx (STAI NS Smith (34) F); age M = exercise min; busy before, after PA, children) less
10.6 (SD = session; work for 15 10 min after PA anx from end of 3); white, I = monitored; min activity to FU; middle class Ty = walk/mn; no diff betw.
Ti = 15 min. groups
Berger et N = 305 (65% I Fr = 3x/wk; Relaxation Exercise pulse Stress (profile Depression, al. (17) F); age M = random I = 65-80%; resp. 20 min rates, pulse rate of mood states) anxiety, and
20.0 assignment Ty =jogging; 5 dlwk; duration, self- hostility Ti = 20 min control: no monitor PA
treatment frequency
Gender effect for stress (F > M); continued practice to maintain benefits
Holloway N = 59 F; age I Fr = 3x/wk, NR Measured best Self-efficacy Self- Can't Pretest group et al. (26) M = 16 quasi- 12 wk; I =
experimental nonaerobic; Ty = wt training; Ti = 1 hr/class
single rep max (physical self- esteem & determine diff on some in free wt squat, efficacy, effectiveness efficacy bench press, & physical variables arm curl strength, and (measured in Tx self-efficacy group only) test);
effectiveness (Eating Disorder Inventory)
Koocher N = 65 M; I Learn to (35) age M = 10.3 matched swim:
(range = 7-15) control Fr = daily; I = vigorous; Tv =
McGowan N = 37 M; I et al. (36) 7th-graders
Noms et N = 80 (50% I al. (18) F); age M = Study 2 16.5; working
class to affluent
swimming; Ti = 12 d
Passed Exercise Self-esteem Can't swimming test reduced gap determine previously failed btwn ideal
self & self- concept compared to control group
Endurance No Running Self-concept; Self-concept Can't Recruited training participation program and peer approval determine participants program: in PE classes competitive sig increase in with low Fr = 3-4 xlwk; activities; fitness & self- initial self- I = vigorous; Ty = sports; Ti = 18 wk
Fr = 2x/wk, Matched: 10 wk; 1-Fr = 2x/ I = 70-75% wk, 10 wk; MHR; Ty = I = 50-60% aerobics; Ti = M R . Ty = 25-30 min aerobics; Ti =
25-30 min; 2-flex Fr = 2x/wk, 10 wk;
increase; Ty = stretching; Ti = 25-30 min; 3-no activity control
improvements in concept cardiovascular fitness
concept & peer approval
Self-report of Stress (life Perceived 70-75% Randomized general ex. events survey stress MHR conditions, habits; step test [NS], perceived not subjects; (2 min, HR stress); illness pretest group taken rest, post, (NS); mood diff were 2 min FU) (multiple affect covaried
adjective TI checklist); 0)
improvement 2 7
seen for high- % co. intensity group o
EL only
3 1. nl rr (D V)
(continued) g (D

Table 1 (continued)
0 Signif.
mental health I
Citation Subjects Design Intervention Control Measure Effect Dose Comments outcomes s? $ n,
Rape (37) N = 42 M, I Fr = NR; No activity Self-report Depression Depression Self-selection & age = 18-25; matched I = NR; frequency (Beck potential a European controls, Ty = running; distance of Depression confound 0' t
Americans cross- Ti = 15 milwk running Inventory); 7
sectional observational
Brown & N = 364 F; IL4 NIA Siege1 (38) age M = 14 prelposttest
(7th-1 lth grade); mostly white upper & upper-middle class
runners less depressed than nonexercisers
Self-report of Stress (life time spent in events); health 14 activities (seriousness of (aerobic & illness rating nonaerobic) scale); PA not
con. with stress or illness at pre- or posttest
Folkins et N = 137 (50% IIA Fr = 2x/wk, Fr = 2x/wk, Timed 1.75 mi Self-confidence/ Depression al. (39) F); );I. college controls not 15 wk; I = 15 wk; I = run, resting HR personal (F only),
students randomized, NR; Ty = NR; Ty = golf adjustment anxiety (F post scores walk/jog; Ti = or archery; (adjective check only), self- NR 25-35 min Ti = NR list); anxiety, confidence
(goal) jogging depression (F only), course (multiple affect sleep
adjective checklist); work efficiency, sleep (self-report over last week)
Can't determine
PreTx diff betw. groups; gender diff may be mediated by baseline levels; posttest scores for control goup NR

Hawkins N = 98 M; IIA & Gruber age M = 10.7
(40) (range 9-12)
Observed little league baseball one season
Scanlan & N = 205 M; IIA Observed 16 N/A Passer (29) age = 11-12 measured teams of
preseason, soccer players pregame, postgame
Sharp & N = 65 M: IIA Fr = 2xIwk; Reilley age = 18-23 correlation I = NR, Ty =
(41) of pre- and aerobic posttraining conditioning; scores; corr Ti = 45 min of change scores
Participation in little league baseball program for an entire season; weekly games and practice on other days
Outcome of game (score); self-report of fun during game; perception of importance of win to coach
12 min run VOzmax
Self-esteem (improved after one season)
Anxiety (sport competition anx test, STAI for children); self- concept (Piers- Hanis self concept scale); losing players had anx after game; baseline anx, level of fun & importance of win to coach predicted
Personality, depression (Minnesota Multi-Phasic Personality Inventory); fitness (-) corr wldepr.; change in fitness corr wlchange on MMPI
Hostility Can't determine
Anxiety Can't determine
Depression; Can't some determine components of personality
(continued)

Table 1 (continued) 2 N
Signif. mental health
I
Citation Subjects Design Intervention Control Measure Effect outcomes Dose Comments 0,
m
Brown & N = 220 F; IIB NIA NIA Self-report type, Stress (schedule Depression, Can't g Lawton age M = 14 intensity, of recent life anxiety determine 'I
(42) (range = 1 1 - duration events); health Q 4
17); white, (seriousness of upper-middle illness rating class scale);
depression (Multiple Affect Adjective Checklist); vigorous PA corr. w/less depr; infrequent PA corr w/more vulnerability to stress & illness
Dyer & N = 59 (46% IIB corr NIA NIA Crouch (9) F); age = 18-
24
Self-report running
Mood: Depression, No. mi/ depression, anxiety wk did anger, confusion, fatigue, tension; runners more
not differentiate mood outcome
(+) mood than nonrunners; no diff for frequent/ advanced vs. novice runners

Noms et N = 147 (52% IIB con N/A NIA al. (18) F); age M =
14 (range = 13-17); working class to affluent
Self-report of Stress (life Depression, Can't ex, habits in events); illness predicted determine organized (seriousness of stress sports & others illness rating (mean, SD NR) scale): mood
(Multiple Affect Adjective Check List); neg low corr betw stress and PA (-.23)
High-risk population
Brown et N = 27 (41% I Aerobics & Regular PE al. (27) F); age M = randomly regular PE:
16.5; working assigned Fr = 3x/wk, 9 class to classes pre, wk; I = NR, affluent; mid, Ty = running/ psychiatric in- posttesting aerobics; Ti = patients; Dx = 4 wk FU NR dythymia conduct disorder
One mile run Depression time, resting (Beck HR, recovery Depression HR, BMI Inventory),
mood (Profile of Mood States); self-efficacy (self-efficacy questionnaire); no diff at post or 4 wk FU; some changes
Can't 60% dropped determine out of study:
baseline diff not controlled in subsequent analyses; midpoint changes may be due to regression to the mean & baseline diff
noted at midpoint betw groups <
- (continued)
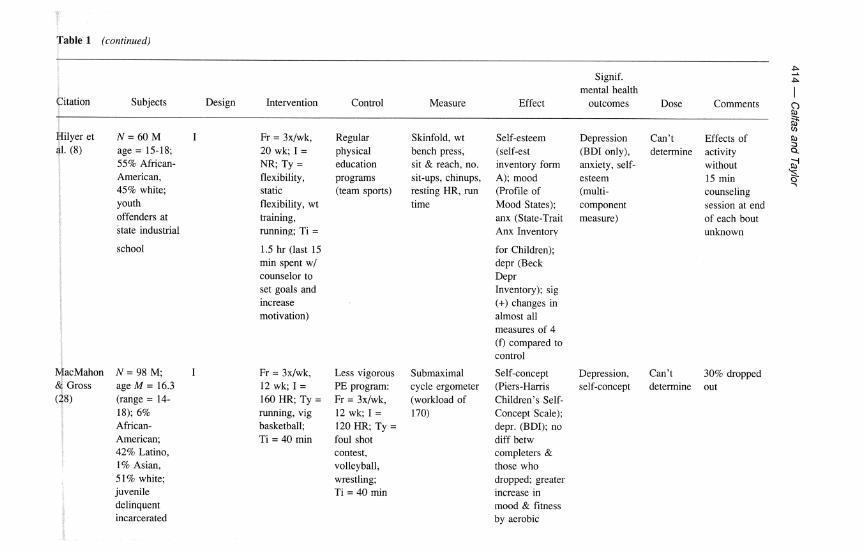
Table 1 (continued)
Signif. 5 P
mental health Citation Subjects Design Intervention Control Measure Effect outcomes
I Dose Comments 0
Hilyer et N = 60 M I al. (8) age = 15-18;
55% African- American, 45% white; youth offenders at state industrial
school
MacMahon N = 98 M; I & Gross age M = 16.3 (28) (range = 14-
18); 6% African- American; 42% Latino, 1% Asian, 51% white; juvenile
Fr = 3x/wk, 20 wk; I = NR; Ty = flexibility, static flexibility, wt training, running; Ti =
1.5 hr (last 15 min spent w/ counselor to set goals and increase motivation)
Regular Skinfold, wt Self-esteem physical bench press, (self-est education sit & reach, no. inventory form programs sit-ups, chinups, A); mood (team sports) resting HR, run (Profile of
time Mood States); anx (State-Trait Anx Inventory
Fr = 3x/wk, Less vigorous 12 wk; I = PE program: 160 HR; Ty = Fr = 3x/wk, running, vig 12 wk; I = basketball; 120 HR, Ty = Ti = 40 min foul shot
contest, volleyball, wrestling; Ti = 40 min
for Children); depr (Beck Depr Inventory); sig (+) changes in almost all measures of 4 (Q compared to control
G Depression Can't Effects of P,
(BDI only), determine activity ii anxiety, self- without 2 esteem 15 min %
4 (multi- counseling component session at end measure) of each bout
unknown
Submaximal Self-concept Depression, Can't 30% dropped cycle ergometer (Piers-Harris self-concept determine out (workload of Children's Self- 170) Concept Scale);
depr. (BDI); no diff betw completers & those who dropped; greater increase in mood & fimess by aerobic
delinquent incarcerated

group; change in fitness not corr wlchange in self-concept or mood
MacMahon N = 54 M; I Fr = 5 d/wk, Fr = 5 d/wk, Random sample Self-concept Self-concept Higher Improvement & Gross age M = 9.7 randomized 20 wk; I = 20 wk; I = were monitored (Piers-Harris intensity in self-concept (19) (range = 7.1- controlled HR > 160 HR < 150 for HR to verify Children's Self- group did more
12.75); middle pre, posttest bpm; Ty = bpm without intensity level; Concept Scale) better associated class; ave. or distance sustained fitness: validated this with above ave. running, elevation in submaximal sample, read participation intelligence, aerobic dance, HR; Ty = testing using aloud (74->80 in PA than
Watters Watters (43)
learning disabled
soccer; Ti = slow relay cycle ergometer percentile vs. 25 min races, dodge (load raised HR 67->68); acad.
ball, to 170) achieve (Wide volleyball; Range Achieve Ti = 25 min Test); motor
prof. (Buininks- Oseretsky Test of motor prof.); body comp
& N = 5 autistic I Fr = 11 tot. TV watching; Observation Self-stirnulatory M, age = 9-1 1 counter- sessions; homework behaviors (e.g.,
balanced I = NR; academic rocking, hand conditions; Ty = jogging; condition subject as Ti = 8-10 min own control
flapping, mouthing) were reduced (M = 32.7%) after the physical exercise condition vs. the academic and TV conditions
with improvements in fitness
Self- Can't Unwanted stimulatory determine behaviors behavior reduced 2
Y 0 T
% '0. 0 E
Note. NR = not reported. F = female; M = male. Fr = frequency; I = intensity; Ty = type; Ti = time. Tx = treatment. For design, I = controlled trial; IIA = prospective observational study; IIB = cross-sectional observational study.

41 6 - Calfas and Taylor
apparently healthy adolescents, we identified seven studies that used an experi- mental or quasi-experimental design, five that used a prospective observational design, and three that used a cross-sectional observational design. Studies of adolescents at risk included two of incarcerated youths, one study of psychiatric inpatients, one of learning disabled individuals, and one of autistic participants. All studies of populations at risk used a Level I research design.
We have the most confidence drawing conclusions from experimental studies, which represent over half of the studies reviewed. Most of these studies compared a fitness training program to a no-activity or low-activity group. The Level I1 studies generally measured change in a psychological variable of interest before and after acute or programmatic activity, or they correlated psychological and activity variables cross-sectionally.
We calculated effect sizes for all Level I studies where experimental and control group means and standard deviations were provided. Effect size was calculated by subtracting the control group mean from the experimental group mean and dividing the difference by the pooled estimate of the standard deviation (6, 7). Effect sizes were calculated separately for outcome variables of interest. Of the seven Level I studies of apparently healthy adolescents, effect sizes were calculated for two studies. Of the five Level I studies of at-risk adolescents, effect sizes were calculated for three studies. The effect sizes for each type of outcome variable are shown in Figure 1. While these effect sizes are calculated using a small number of studies and should be interpreted with caution, they demonstrate a moderate and positive relationship between physical activity and various psycho- logical outcomes. For each example, participation in physical activity is associated with increases in self-esteem and decreases in stress/anxiety and depression.
Psychological Impact of Physical Activity Generally, the studies report moderate evidence that physical activity is psycho- logically beneficial for youth. The most consistent effect was for self-esteem/
a 4 3 2 2 w m Y
0 3
8 .r 0 4 -.I5 8 S ~ H - esteem concept
B StresslAnxieIy
8
Effect Size
Figure 1 - Average effect size in reviewed studies of psychological variables.

Psychological Variables - 417
self-concept and anxietylstress variables. Eight of the 11 studies addressing anxietylstress variables found a positive relationship or experimental effect of activity such that physical activity was associated with reductions in anxiety and stress. For example, flexibility training reduced anxiety in an ethnically diverse group of adolescent boys (8). Similarly, runners were found to have low anxiety (9). Perceived stress was lower among participants of a vigorous activity program compared to those of a moderate activity program. In a recent review of primarily adult data, Petruzzello et al. (10) found that only aerobic physical activity pro- duced reductions in anxiety and that the effects were generally independent of subject characteristics.
Nine of the 10 studies addressing self-esteem, self-concept, or self-efficacy also found a positive relationship or experimental effect. Self-esteem and self- concept have been studied as important predictors of many types of human behavior, ranging from academic performance to antisocial activities, and these variables may mediate other psychological states. Physical activity can contribute to improvements in self-concept and self-esteem (1 1, 12, 13). In fact, self-concept has been described as the variable with the "highest payoff" in physical activity and personality research (14).
Two important reviews (12, 13) describe and evaluate the literature related to self-esteem and physical activity. In studies with children typically younger than the age range for this review, Gruber (12) evaluated the relationship between physical activity and self-esteem in 84 articles. Using meta-analytic techniques, Gruber concluded that handicapped children (e.g., emotionally disturbed, trainable mentally retarded, economically disadvantaged, educable mentally retarded) ex- perience large improvements in their self-concepts as a result of physical activity. Typically, handicapped children begin enrichment programs with lower self- concepts than do nonhandicapped children. While nonhandicapped children show improvements in self-concept as a result of physical activity, handicapped children show the greatest improvement in self-concept. Additionally, Gruber concluded that participants in physical fitness and aerobic activities show greater improve- ments in self-esteem than do participants in programs of creative movement (e.g., dance, mime) or sports skills (e.g., gymnastics, soccer).
Sonstroem (13) documented the scientific limitations in 16 studies of exer- cise and self-esteem, including adolescent and adult participants. Because the results were consistently positive, in spite of experimental shortcomings, Sonstroem concluded that participants in exercise programs report significant increases in self-esteem scores.
In the 11-21 age group, physical activity can play a unique role in self- esteem enhancement. Mastery experiences and successes with physical activity can be meaningful in improving self-esteem, particularly during the develop- mental stage of adolescence. Moreover, the duration and type (e.g., aerobic vs. nonaerobic) of physical activity may be an important factor in enhancing self- esteem, More research is needed in this area.
Of studies addressing depressed mood, 9 of 11 studies found a positive relationship or experimental effect. Exercise has an antidepressant effect for mild to moderate forms of depression in adults (15). In a meta-analysis of adults and children, North et al. (16) found exercise to be a better antidepressant than relaxation and other enjoyable activities, and exercise was most effective when combined with psychotherapy. North et al. (16) also found that subjects requiring

41 8 - Calfas and Taylor
medical or psychological care demonstrated the largest decreases in depression. This finding is consistent with Gruber's (12) assertion that those with lower levels of initial functioning benefit more from physical activity and may reflect regression to the mean.
Very little evidence was available for hostility/anger and physical activity. The available evidence was inconsistent. One study found a significant decrease in hostilitylanger (17), and another study found no significant difference between experimental and control groups (18). A cross-sectional study found no relation- ship (14). Evidence regarding academic achievement was also sparse. One study found no significant effects on academic performance (19), while another study found that a one-hour increase in physical activity per day improved math perfor- mance of grade-school children (20). In a review, Kirkendall (21) asserted that there is no conclusive evidence regarding the effects of exercise on intellectual development or performance especially in our age group.
Negative Effects of Physical Activity
Notably, no studies reported negative effects of activity. In fact, all changes that were not statistically significant were in the direction expected (i.e., improve- ments). Still, potential negative outcomes of physical activity may include exer- cise abuse, eating disorders, overtraining, and staleness (i.e., competitive athletes who overtrain suffer mood disturbances such as depression) (22,23). In adoles- cents, extreme levels of physical activity can be related to other problems. During primary care visits, it is appropriate to question adolescents who are extremely physically active about possible eating disorders and stress induced by excessive competitive drives. However, a causal relationship between activity and eating disorders is not well documented (24, 25). The potential for negative effects of physical activity merits further study. The available literature suggests that physi- cal activity creates no psychological harm in adolescents.
Type/Dose of Activity
Little is known about the amount of activity most likely to produce psychological benefits. Few studies experimentally controlled for intensity or dose of activity.. One study examined the effect of moderate- versus high-intensity activity, and demonstrated that anxiety and stress were lower for the high-intensity group compared to that of the moderate-intensity group at posttesting (18). Other studies compared high- versus moderate-intensity activity groups or aerobic versus flexi- bility activity groups and found greater improvement on psychological variables for the more aerobic or active conditions. Regarding duration and frequency of activity, Dyer and Crouch (9) found that moderate levels of running (7 miles per week for 5 months) were associated with positive mood to the same extent as more advanced levels of running (56 miles per week for > 5 years). The average duration in studies that found significant effects was 106 min per week (6G125 min per week). The average duration of intervention in studies which found significant effects was 12.8 weeks (1-20 weeks).
Only one study examined the effects of a strength-training program (26). While this study has methodological flaws, there was a general trend for partici- pants in the strength-training program to show greater improvements in total self- efficacy, perceived physical ability, self-presentation, and perceived effectiveness

Psychological Variables - 419
than either the mild cardiovascular training condition or no-activity condition. Since there are very little data that assess dose-response relationships in intensity of training, duration, or frequency, it is inappropriate to draw firm conclusions about dose, given the current state of the literature.
High-Risk Populations
The adult literature supports the use of physical activity as an adjunctive treatment for clinical and subclinical psychological disorders, including depression (16) and anxiety (10). The available data for adolescent populations is insufficient to draw the same conclusions. One study of male and female psychiatric inpatients showed moderate changes in mood as a result of physical activity (27). However, the researchers did not report other psychological interventions that may have been taking place during their hospitalization. Also, the gender effects reported in this study (i.e., girls showed more improvement in depression than boys) may have been mediated by psychiatric diagnosis, in which more girls than boys were diagnosed as dysthymic at baseline.
The two other high-risk studies examined the effect of activity on institution- alized youth offenders (8, 28) and showed a general positive effect on mood and self-esteem. Clearly, these three studies are not representative of the most frequent types of psychological dysfunction seen in the adolescent population. Risk for suicide, substance abuse, and eating disorders are also appropriate targets for potential intervention at either the clinical or subclinical level. The efficacy of physical activity may depend on the psychological condition. More research is needed on physical activity as an adjunct treatment for specific disorders in adolescence.
Limitations
There are several methodological problems with the data reviewed. First, the number of controlled trials in this area is limited. Second, many of the conclusions in the studies were based on a small number of subjects. Attrition was very high in some studies, potentially skewing the results. Third, these studies targeted different psychological variables measured in different ways. It is particularly important for studies to use age-appropriate measures that have been developed and validated for an adolescent population. Fourth, assessing physical activity has unique challenges. Observation is the preferred and most reliable method, but is unrealistic for large groups. Self-report is more easily administered, but may not be accurate. Mechanical devices provide better data than self-report, but may not accurately measure all types of activity. It is important that the measurement of physical activity be well documented and validated.
Most of the studies were conducted with white, middle- or upper-middle- class, urban subjects, making generalizations to other ethnic and socioeconomic groups difficult. Additional research is needed using more subjects, a randomized controlled design, and diverse subject populations, particularly with respect to ethnicity, gender, and socioeconomic status. We recognize that physical activity, as well as psychological states, play different roles in different cultural settings. For this reason, it is often difficult to generalize these results across different ethnic and cultural populations.

Table 2 Recommendations and Summary Findings on Physical Activity and Psychological Variables in Adolescents -I
9 4
Amount of No. Level of Anxiety/ Self-esteem/ Hostility/ dose response Basis for
studies quality Depression stress concept anger data recommendations Recommendatons
General 5-10 I ? ? 7. + Some 65% adolescent data, Fr = 3x/wk; I = adolescent < 5 II A ? t 7 N/A None 15% adult data, 10% modlvig 70% MHR; population < 5 IIB '? t N/A -3 None child data, 10% Ty = aerobic; Ti =
expert opinion 60 min/wk (total)
High-risk 5- 10 I ? + ? N/A Some adolescent
None
population
Note. I = a controlled trial; IIA = a prospective observational study; IIB = cross-sectional observational study. + = no apparent evidence of beneficial trend of PA related to outcome; '? = some apparent evidence of beneficial trend of PA related to outcome. Fr = frequency; I = intensity; Ty = type; Ti = time.

Psychological Variables - 421
Recommendations
Generally, it is difficult to make specific recommendations regarding physical activity for psychological benefits among adolescents. There are few studies, and the quality of the data are poor in some studies. However, despite the methodologi- cal flaws of the research, the overall trend suggests physical activity can be psychologically beneficial for adolescents. Further, there is no evidence that activity causes psychological harm. We recommend that adolescents participate in regular physical activity as specified in Table 2. A good behavioral goal is for adolescents to develop the skills necessary to continue being active throughout their adult years.
Future research should consider the role of the social/psychological context in which the activity occurs. For example, Scanlan and Passer (29) found that soccer players had different psychological responses to presumably the same amount of activity, depending on whether they won or lost a soccer game. Other potential mediating experiences during activity include competition, self- appraisal, expectations about how others appraise one's performance, individual versus group activities, and social support. According to Sage (30), developmental scientists agree that play (activity) is important for social development. However, the popular notion that participation in sports builds character provides an interest- ing cultural context for further exploration.
Rowland (31) reports four potential mediating factors for the effect of physical activity on mental health, including (a) "time out" theory, in which attention is diverted away from stressors; (b) self-significance, in which participa- tion in activity fosters feelings of mastery and competence; (c) control, in which activity is experienced as concrete, and improvements can be clearly seen and achieved; and (d) biochemical changes, in which activity causes chemical changes known to improve mood. The reader is referred to other articles for more thorough discussions of potential mediating factors (10, 11, 15, 32).
In conclusion, the data suggest that physical activity is psychologically beneficial for adolescents. More research is needed to better understand this relationship. The World Health Organization defines health as the comprehensive state of physical, psychological, and social well-being, not merely absence of disease (33). Psychological benefits of activity are as important as physical benefits because psychological well-being contributes to overall health. Learning more about the psychological benefits of physical activity will enable us to better understand the concept of a healthy mind in a healthy body.
References 1. American Psychological Association. Diagnostic and Statistical Manual of Mental
Disorders (3rd ed.). Washington, DC: Author, 1987. 2. Brown, R. Exercise, fitness, and mental health. In: Exercise, Fitness, and Health: A
Consensus of Current Knowledge, C. Bouchard, R.J. Shephard, T. Stephens, J.R. Sutton, and B.D. McPherson (Eds.). Champaign, IL: Human Kinetics, 1990, pp. 607- 633.
3. King, A.C., C.B. Taylor, W.L. Haskell, and R.F. DeBusk. Influence of regular aerobic exercise on psychological health: A randomized controlled trial of healthy middle- aged adults. Health Pych. 8:305-324.

422 - Calfas and Taylor
4. Taylor, C.B., J.F. Sallis, and R. Needle. The relation of physical activity and exercise to mental health. Public Health Rep. 100:195-202, 1985.
5. Shaw, K.R., K.H. Sheehan, and R.C. Fernandez. Suicide in children and adolescents. Adv. Pediatr. 34:3 13-334, 1987.
6. Glass, G., B. McGaw, and M. Smith. Meta-Analysis in Social Research. Beverly Hills, CA: Sage, 1981.
7. Rosner, B. Fundamentals of Biostatistics (2nd ed.). Boston: Duxbury Press, 1986. 8. Hilyer, J.C., D.G. Wilson, C. Dillon, L. Caro, C. Jenkins, W.A. Spencer, & W.
Booker. Physical fitness training and counseling as treatment for youth offenders. J. Couns. Psych. 29:292-303, 1982.
9. Dyer, J.B., and J.G. Crouch. Effects of running on moods: A time series study. Percep. Motor Skills 64:783-789, 1987.
10. Petruzzello, S.J., D.M. Landers, B.D. Hatfield, K.A. Kubitz, and W. Salazar. A meta- analysis on the anxiety-reducing effects of acute and chronic exercise: Outcomes and mechanisms. Sports Med. 11(3):143-182, 1991.
11. Sonstroem, R.J., and W.P. Morgan. Exercise and self-esteem: Rationale and model. Med. Sci. Sport Exerc. 21:329-337, 1989.
12. Gruber, J.J. Physical activity and self-esteem development in children: A meta- analysis. In: Effects of Physical Activity on Children (The American Academy of Physical Education Papers, No. 19), G.A. Stull and H.M. Eckert (Eds.). Champaign, IL: Human Kinetics, 1986, pp. 30-48.
13. Sonstroem, R.J. Exercise and self-esteem. Exerc. Sport Sci. Rev. 12:123-155, 1984. 14. Folkins, C.H., and W.E. Sime. Physical fitness training and mental health. Am. Psych.
9:380-389, 1981. 15. Martinsen, E.W. Benefits of exercise for the treatment of depression. Sports Med.
91380-389, 1990. 16. North, T.C., P. McCullagh, and Z.V. Tran. Effect of exercise on depression. Exerc.
Sport Sci. Rev. 18:379-415, 1990. 17. Berger, B.G., E. Friedmann, and M. Eaton. Comparison of jogging, the relaxation
response, and group interaction for stress reduction. J. Sport Exerc. Psych. 10:431- 447, 1988.
18. Norris, R., D. Carroll, and R. Cochrane. The effects of physical activity and exercise training on psychological stress and well-being in adolescent population. J. Clin. Psych. 36(1):55-65, 1991.
19. MacMahon, J.R., and R.T. Gross. Physical and psychological effects of aerobic exercise in boys with learning disabilities. Dev. Behav. Pediatr. 8(5):274-277, 1987.
20. Shephard, R.J., M. Volle, H. Lavallee, R. LaBarre, J.C. Jequier, and M. Rajic. Required physical activity and academic grades: A controlled study. In: Children and Sport: Pediatric Work Physiology, J. Ilmarinen and I. Valimaki (Eds.). Berlin: Springer- Verlag, 1984, pp. 58-63.
21. Kirkendall, D.R. Effects of physical activity on intellectual development and academic performance. In: Effects of Physical Activity on Children (The American Academy of Physical Education Papers, No. 19), G.A. Stull and H.M. Eckert (Eds.). Champaign, IL: Human Kinetics, 1986, pp. 49-63.
22. Raglin, J.S. Exercise and mental health: Beneficial and detrimental effects. Sports Med. 9:323-329, 1990.
23. Morgan, W.P., D.R. Brown, J.S. Raglin, P.J. O'Connor, and K.A. Ellickson. Psycho- logical monitoring of overtraining and staleness. Br. J. Sports Med. 21(3):107-114, 1987.

Psychological Variables - 423
24. Dishman, R.K. Exercise and sport psychology in youth 6 to 18 years of age. In: Perspectives in Exercise Science and Sports Medicine: Vol. 2 . Youth Exercise and Sport, C.V. Gisolfi and D.R. Lamb (Eds.). Indianapolis: Benchmark, 1989, pp. 47- 97.
25. Yates, A., K. Leehy, and C.M. Shisslak. Running: An analogue to anorexia? N. Engl. J. Med. 308:251-255, 1983.
26. Holloway, J.B., A. Beuter, and J.L. Duda. Self-efficacy and training for strength in adolescent girls. J. Appl. Soc. Psych. 18:699-719, 1988.
27. Brown, S.W., M.C. Welsh, E.E. Labbe, W.F. Vitulli, and P. Kulkarni. Aerobic exercise in the psychological treatment of adolescents. Percep. Motor Skills 74:555-560, 1992.
28. MacMahon, J.R., and R.T. Gross. Physical and psychological effects of aerobic exercise in delinquent adolescent males. Sports Med. 142:1361-1366, 1988.
29. Scanlan, R.K., and M.W. Passer. Factors related to competitive stress among male youth sport participants. Med. Sci. Sports 10:103-108, 1978.
30. Sage, G.H. The effects of physical activity on the social development of children. In: Effects of Physical Activity on Children (The American Academy of Physical Education Papers, No. 19), G.A. Stull and H.M. Eckert (Eds.). Champaign, IL: Human Kinetics, 1986, pp. 22-29.
31. Rowland, T.W. Exercise and Children's Health. Champaign, IL: Human Kinetics, 1990, pp. 161-180.
32. Morgan, W.P. Psychogenic factors and exercise metabolism: A review. Med. Sci. Sports Exerc. 17:309-316, 1985.
33. World Health Organization. The First Ten Years of the World Health Organization. Geneva: Author, 1958.
34. Bahrke, M.S., and R.G. Smith. Alterations in anxiety of children after exercise and rest. Am. Correct. Ther. J . 39:90-94, 1985.
35. Koocher, G.P. Swimming, competence, and personality change. J. Personality Soc. Psych. 18:275-278, 1971.
36. McGowen, R.W., B.O. Jarman, and D.M. Pedersen. Effects of a competitive endurance training program on self-concept and peer approval. J. Psych. 86:57-60, 1974.
37. Rape, R.N. Running and depression. Percep. Motor Skills 64: 1303- 13 10, 1987. 38. Brown, J.D., and J.M. Siegel. Exercise as a buffer of life stress: A prospective study
of adolescent health. Health Psych. 7:341-353, 1988. 39. Folkins, C.H., S. Lynch, and M.M. Gardner. Psychological fitness as a function of
physical fitness. Arch. Phys. Med. Rehab. 53(11):503-508, 1972. 40. Hawkins, D.B., and J.J. Gruber. Little league baseball and players' self-esteem. Percep.
Motor Skills 55:1335-1340, 1982. 41. Sharp, M.W., and R.R. Reilley. The relationship of aerobic physical fitness to selected
personality traits. J. Clin. Psych. 31:428-432, 1975. 42. Brown, J.D., and M. Lawton. Stress and well-being in adolescence: The moderating
role of physical exercise. J. Human Stress 12:125-131, 1986. 43. Watters, R.G., and W.E. Watters. Decreasing self-stirnulatory behavior with physical
exercise in a group of autistic boys. J. Autism Dev. Disord. 10:379-383, 1980.