effects of captopril therapy on endogenous fibrinolysis in ...clonal antibodies against ihe relevant...
TRANSCRIPT

arterial intima (4). Impaired endogenous fibri sis is associated wi
increased risk of ~ntravascu~a of the ~b~no~ytjc system is
From the Cardiovascular Research Unit, University of Edinburgh and tDepar#ment of ~aemato~ogy, Royal Infirmary, Edinburgh, Scotland; and *Department of Medicine, University of Newcastle upon Tyne, Newcastle upon Tyne, England, United Kingdom. This work was supported by tbe Chest, Heart and Stroke Association, Edinburgh, Scotland, and by the British Diabetic Association, London, England. Supplies of placebo and captopril were kindly donated by Bristol-Meyers Squibb Pharmaceuticals Ltd, London, England, who did not provide any financial support.
Manuscript received November 24, 1993; revised manuscript received Jan ary 2. 1994.
Dr. Robert A Wright, Department of Car- diology, Royal Iniirmary, I, Lauriston Place, Edinburgh EH3 9YW. United Kingdom.
CiB4 by the American College of Cardiology
tissue-type ~~asminogen activator ( o~ant inh~ni~or, pias increased levels of t marker of risk for c
healthy men (7), in patients wit angina (8,9) and in patients with myocardia~ infarc 10) and most have been
morality in with coro- nary artery disease (II). Elevated levels of plasm activator inbibitor type 1 activity have been identi young survivors of myocard~al infarction (1%) and we shown to be associated with an increased risk ofre~nfarctio (13). Studies in normal subjects (14) and in patients with angina (15) have shown a correlation between levels of fasting insulin and both t-PA activator and
gen activator inbib~tor type t Angiotensin-conveying enzyme i to improve hy~er~nsul~nemia in
nous infusion of angiotensin II results in an increase in plasma levels of plasminogen activator inhibitor type 1 (19),
07351097/94/$7.00

6% WRIGHT ET AL. SAW Vol. 24, No. 1
EFFECTS OF CAPTOPRIL ON FIBRINOLYSIS July 1!994:67-73
I. Details of the Index Myocardia! Infarction in the 15 Patients
No. of .Pts or Mean Value (range)
Cigarette smoker 3
Family history of IHD 3 Anterior site 8
Inferior site 7
Q wave I4
streptokinase therapy 14
peal; creatine kii (W/liter) I.900 (476-4,259) CatWhoracic ratio 0.48 (0.40-OS)
LVEF at 6 wk 0.37 (0.28-0.42)
a ischemic heart disease; LVEF = lefi ventricular ejection fraction; tients.
providing a link between the renin-angiotensin system and risk of thrombosis and an alternative path by which angiotensin-converting enzyme inhibitors might influence fibrinolysis.
We investigated the hypothesis that the angiotensin- converting enzyme inhibitor captopril might modify endog- enous fibrinolysis in men after myocardial infarction that is uncomplicated by clinically manifest heart failure, arrhyth- mia and recurrent ischemia.
Subjects. Eighteen men ~75 years old and with their first myocardial infarction were recruited 6 weeks after admis- sion to hospital. in addition to a typical history, subjects had to show pathologic Q waves on the electrocardiogram (ECG) or to have had a peak creatine kinase (CR) level MOO ILJWter, or both. Patients with a history of hyperten- sion or diabetes mellitus were excluded. All patients had been taki cardioselective beta-adrenoceptor blocking
nt and mg of asp ;n daily from the time of admission to hospital. and no other medication was permitted. None had previously taken an angiotensinconverting enzyme in- hibitor. At the time of recruitment a full clinical assessment was made, and a chest radiograph, symptom-limited tread- mill exercise test and radionuclide ventriculogram were performed. Any patient with clinical or radiologic signs of heart failure or evidence of ischemia or arrhythmia requiring additional therapy was excluded, and only those considered to have made an uncomplicated recovery from their infarc- tion and without other significant illness were admitted to the study. Three patients were excluded from analysis: one patient whose compliance was <!N% by tablet count (75%), one patient whose beta-blocker was withdrawn by his gen- erai practitioner during the study and one who moved to a different city during the study and was unwilling to continue with study medication. Details of the index admission to hospital for the 15 patients are given in Table 1.
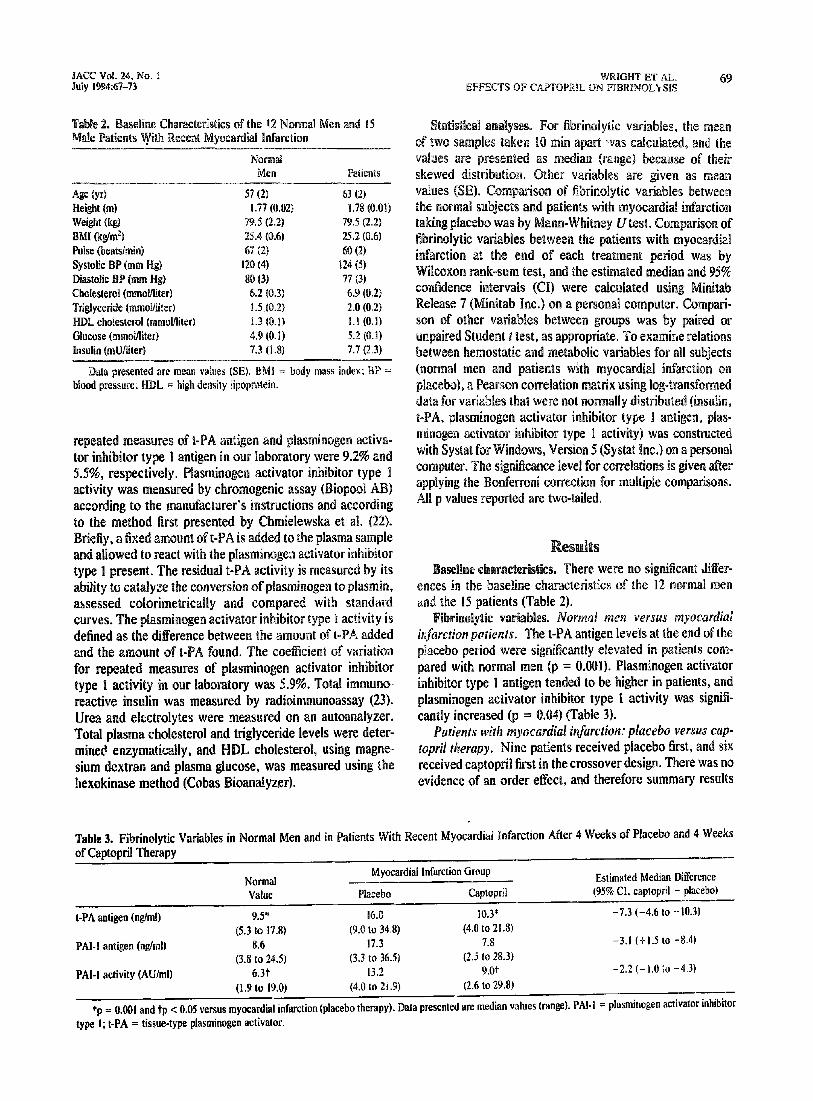
To provide comparison for fibrinolytic variables, 12 nor- mal men similar in age to the patients were identified at
random from the Lot these men gave a his tension or diabetes medication. They all normal IZlead ECG.
on one occasion only i each d-week treatment
The patients lay recumbent, and a 16-G intravenous cannul was inserted into a large antecubital vein aud flushed wit saline solution. Thick minutes later, 5 ml of blood was drawn and discarded. A further 10 ml of blood was drawn into potassium citrate anticoagu~aat for fibrinolytic assays; 10 ml into lithium heparin for immunoreactive insulin, urea and electrolytes; 2.5 ml into fluoride oxalate for glucose; and 10 ml into a plain glass tube for serum lipoproteins. Ten minutes later a further 5 ml of blood was drawn and discarded, and an additional IO-ml sample for fibrinolytic assays was drawn into potassium citrate. The samples for fibrinolytic assays and insulin were placed into melting ice. Within 1 h, plasma was separated by centrifugation (20 min at 2,000 x g and +C), immediately frozen in dry ice and stored at -4OC.
Assays. All fibrinolytic assays were performed at the same time after completion of the study. Assays for t-PA and plasminogen activator inhibitor type 1 antigen were by a two-site enzyme-linked immunosorbent assay (Biopool AB) and were performed as instructed by the manufacturer, according to the method of Ranby et al. (21) in which plasma samples are incubated in microtiter plates coated with mono- clonal antibodies against ihe relevant antigen, unbound antigens are washed off, and bound antigen is detected by addition of a second specific antibody conjugated to horse- radish peroxidase. Standard curves were constructed using purified antigen diluted in plasma to known concentrations. The amount of t-PA and plasminogen activator inhibitor type 1 antigen in samples was deduced by comparing absorbance with the standard curve. The coefficients of variation for
Normal &Ien
57 43
1.77 (0.02) 79.5 (2.f) 25.4 (0.6) 67 12)
77 (31 6.9 (0.2)
1.5 .(0.2) 2.0 (0.2) 1.3 U-l.%) 1.1 (0.l) 4.9 1O.n) 5.2 (0.1) 7.3 (1 .$I 7.7 (2.3)
II = body mass index;
s
were no sigmi~ca~t Ji
assessed c~~~~~~et~ica~~y and compared with standard ~~~~t~~ type 1 activ e amount of t-PA
and the amount of t-PA hmd. The CO for repeated measures Of ~las~~~~~em type 1 activity in our laboratory was 5.
nsulin was measured by radioimmunoassay (23). electrolytes were seasoned m an autoanalyzer.
Total plasma cholesterol and triglyceride levels were deter- mined enzymatically, and HDL cholesterol, using magne- sium dextran and plasma glucose, was measured using the hexokinase method (Cobas Bioanalyzer).
nsrmal men (p = 0.00 i~~i~it~~ type B antigen tended to be higher in patients, and plasminogen activator inhibitor type 1 activity was signifi- cantly increased (p = 0.03) (Table 3).
Pahms with myscardi~l hzjarctim: placebo versus cap- topril thcrqy. Nine patients received placebo first, and six
received captopril first in the crossover design. There was 110 evidence d an order etfect, and therefore summary resuks
.
Table 3. Fibrinolytic Variables in Nornmal Eaen and in Patients With Recent Myocardial Infarction After 4 Weeks of Placebo and 4 Weeks of Captopril Therapy
Normal hnyocardial Infarction Group Estimated Median Difference
Value Placebo Captopril (95% Cl, caplopril - placebo)
t-PA antigen (nglml) 9.5” 16.0 10.3* -7.3 (-4.6 to -10.3)
(5.3 to 17.8) (9.0 to 34.8) (4.0 to 21.8)
PAI-1 antigen @/ml) 8.6 17.3 7.8 -3.8 (+ 1.5 IO -8.4)
(3.8 to 24.5) (3.3 to 36.51 (2.5 to 28.3)
PAL1 activity (AU/ml) 6.3.t 13.2 9.0t -2.2 (- 1.0 ;o -4.3)
(1.9 LO 19.0) (4.0 to 2 i 3) (2.6 to 29.81
*p = 0.001 and tp < 0.05 versus myocardial infarction (placebo therapy). Data presented are median values (range). PAI-1 = plasminogen activator inhibitor
type 1; t-PA = tissue-type plasminogen activator.

70 WRIGHT ET AL. EFFECTS OF CAPTOPRIL ON FIBRINOLYSIS
PAi- Anti$en (q/ml) PAL1 Activity (AU/ml)
are presented combined in Taboo 3; i~~ivi~~al results are rorrela given in Figure II. with fa
Tissue-@pa plasminogerr activator antigen. After 4
weeks of therapy with captopril compared with 4 weeks of placebo, there was a highly si nificant decrease in t-PA (p = O&01), with a median reduction of 46% (95% C1 -29% to -64%). Fourteen patients showed a reduction, and one showed a small increase.
Phminqen activator inhibitor type ! antigen. After captopril therapy compared with, placebo therapy, 10 pa- tients showed a decrease in ~las~~~n~e~ activator inhibitor type 1 antigen, one patient showed no change, and four patients showed an increase. There was no overall sig~ifi- cant effect, although there was a median reduction of 18% (C9% to -49%. p = 0.17).
P~astni~~~en activator inhibitor type 1 activil.v. After captopril therapy, there was a significant reduction in plas-
activator inhibitor type 1 activity (p = 0.02), with a (-8% to -33%); 13 patients inogen activator inhibitor type 1
ents with myocardial infarction: therapy. After 4 weeks of therapy
with placebo compared to 4 weeks of captopril, there was no significant effect on blood pressure or plasma urea, electro- lyte, lipoprotein, glucose or insulin levels (Table 4).
acute myocardial infzction. In addition, we have shown in double-blind, ~!acebo-controlled, randomized crossover study that 4 weeks of treatment with captopril(75 mg d is associated with a significant decrease in t-PA antigen plasmi~ogen activator inhibitor type 1 activity. Angiotensin- converting enzyme inhibitors have not previously been reported to have an effect on fibrinolytic variables, and this may help to explain why their use is associated with a reduction in risk of coronary thrombosis.
Table 4. Effect of 4 Weeks of Placebo and 4 Weeks of Captopril Therapy on Other Variables
era meta Based on combined results from normal men and
patients with myocardial infarction treated with beta- blockers, aspirin and placebo, Table 5 shows the Pearson correlation coefficients between fibrinolytic variables and plasmaglucose, insulin and lipid levels. After adjustment for muhiple comparisons, the correlations between t-PA antigen and plasminogen activator inhibitor type 1 activity (r = 0.61, p = 0.027) and between plasminogen activator inhibitor type 1 antigen and plasminogen activator inhibitor type 1 activity (r = 0.673, p = 0.005) remained significant. Plasminogen activator inhibitor type 1 activity also showed significant
Placebo Caplopril
Systolic BP (mm Hg) II7 (4) 114 (4) Diastolic BP (mm Hg) 69 (3) 6g (4) Urea (mmol!liter) 6.3 (0.3) 6.5 (0.4) Sodium (mmoUliter) 141(I) 141 (1) Potassium (mmol/lited 4.1 (0.1) 4.1 (0.1) Crcatinine (~0Uiiter) 105 (3) 105 (3) Cholesterol (mmoMiter1 6.9 (0.2) 6.8 (0.2) Trigiyctride (mmoyliter) 2.0 (0.2) 2.2 (0.3) HDL cholesterol (mmoMiter) 1.1 (0.1) I.1 (0.0 Glucose (mmohliter) 5.3 (0. I) 5.2 (0.2) Insulin (mU&ter) 7.7 (2.3) 6.8 (1.4)
Data presented are mean values (SE). Abbreviations as in Table 2.
JACC Vol. 24. No. 1 July 1 :6Y-73
Tissue-type Plasminogen acti- ) autiBern levels and plasmin-
ogen activator inhibitor type I (FM-I) antigen and activity levels in 15 patients with recent, ~~co~~~cated ~yoca~dia~
tion treated for 4 weeks witn pla-
olytic system, a3 shown

PALl antigen 0.484 - - PAI- activity 0.610” 0.673: - Fasting issulin 0.173 0.526 0.591’ Fasting ~I,IW,.= -8. ^^^^ 0.26Q 0.035 0.392 Total cbo~estero~ 0.259 0.068 0.283 Total ~~~iyce~de 0.477 0.424 0.594* HDL cholesterol -0.475 -0.460 -0.394
*p < 0.05. tp < 0.01 after Bonferroni correction. Abbreviations as in Tables 2 and 3.
with reinfarct~~~ ha
predict mQr~ality over a 7-y r follow-up (1 I). An earlier study of young SUrviVQrs of found higher levels of t-PA a
tor type I activity tRan con&01 subjects, and a of further iRfarcti0~ was predicted by increase
lasminogen activator j~bib~~or type 1 activity in study in which tissue-type asmi~oge~ activator antigen
has been a consistent ~~d~og antigen and ~lasminoge~ activator iub~bitor type 1
mi~oge~ activator inhibitor t I activity disease,
It should be noted that the results of assays that measure levels of antigen include inactive complexes of t-PA with ~la§minogeo activator in- hibitor type 1, and therefore it is valuable to have measures of both antigen and activity.
It might initially be thought that antigen would suggest a decreased indicating a more active fibrinolytic system. One hypothesis that could help to explain these observations is that in- creased secretion of these molecules, measured by t.he levels of antigen detected, reflects a respopse to stimuli that promote thrombosis and that it is these that increase the risk of subsequent thrombotic occlusive events. This by is supported by evidence that both thrombosis and pharma- cologic thrombolysis increase circulati evels of plasmin- ogen activator inhibitor type I (24) and expression of the plasminogen activator inhibitor type 1 gene within the endo- thelium (25). It is likely that increased circulating plasmino- gen activator inhibitor type 1 stimulates release of t-PA, which is supported by the strong correlation between t-PA
activator ~~b~bito
ults indicate that factors o
otensin system may play a more direct role in the control of endogenous fibrinolysis (19). In a study
crtensive subjects, an intravenous infusion of angio- a significant increase in plasmi pe 1 antigen with no effect on t
ngiotensin-converting enzyme i ion of angiotensin II, they might be expected crease in levels of plasminogen activator
inhibitor type 1, but this would not explain the decrease in t-PA. Angiotensin-converting enzyme inhibitors also influ- ence the kinin system and lead to increased levels of
bradyk~Ri~ (29). Tissue-type p~asmi~oge~ activator is pri- marily secreted from ~dothelium~ from which its release is enhanc inin (3Q). Two possible explanations for the a y with our observahs are the duration of treatment in our study compared with the short-term elects of bradykinin infusion in ~x~e~~e~ta~ models and our failure to measure the activity of t-PA in a.ddition to s concentration.
Study li lions. Although our results are consistent with previous observations that altered fibrinoiysis is asso-
72 WRIGHT ET AL. EFFECCS OF CAPTOPRIL ON FIBRINOLYSIS
c&d with an increased risk of myocardial infarction and that angiotensin-converting enzyme inhibitors reduce the risk of subsequent coronary thrombosis in patients with first mymwdid infarction, there are a number of limitations to our study. We studied a small, highly selected population for a relatively short period. We included only men <75 years old with a first uncomplicated myocardial infarction. Pa- tients with previous hypertension or diabetes mellitus or with any evidence of heart failure were excluded because these conditions might influence fibrinolysis directly or through associated neurohumoral disturbances. All of our ptients were taking a cardioselective beta-blockbr and aspirin, as is the preferred therapy for patients with myocars dial infarction in the absence of any cont~indication. Nei-
ta-blockers (12,JI) nor assign is thought to i~~ue~c~ Abrinolysis.
Our study did not include any cxumination of t-PA release, such as the venous occlusion test (321, w have provided i~fo~ation on changes in endotbe~i~ func- tion. However, a recent study in diabetic and nondia~tic survivors of myocardial infarction found no difference in levels of t-PA antigen or plasminogen activator inhibitor type I antigen and activity after venous occlusion between pa- tients and control subjects despite significant differences before venous occlusion (33). Finally, we cannot exclude a long-lasting hangover effect from acute infarction that might influence the results of the patient group, although the blood samples for this study were taken at least 12 weeks after the initial event. Mitigating st an acute-phase response persisting are the stable d values, the uncomplicated recovery from infarction in our group and the absence of an order effect in the crossover design. This also a hangover effect from the captopti~ treatment those who received coptopril first, consisten
se to captopril withdrawal (34). ted that fibrinolytic variables are few days after infarction and are
A decrease in the incidence of acute coro- nary syndromes in those receiving angiotensin-coavcrting enzyme inhibitors was a common and unexplained finding in three large placebo-controlled trials in patients with mild left ventricular dysfbnction (l-3). This study has shown for the first time that captopril modifies endogenous fibrinolysis in patients with recent uncomplicated ruyocardial infarction. This may help to explain the reduction in thrombotic risk
~sswiated with the use of smgiotensin-convertinp enzyme inhibitors.
we ~~W~SC the considerable help and expertise of MIX. Catriona smpso% RGN. and Mrs. Frances henhouse. HNC, without whom this WO&
udd m be been possible. Assays of total immunoreactive insulin were Pcltormed by Mrs. fatrici Shearing in the Department of Medicine, Univer- sity of Newcastle upon Tyne, United Ki~@om. We thank Mrs. J. Cunning- ham for preparation of the manuscript.
s
1. The SDLVD Investigators. Effect of enalapril on survival in patients with entricular ejection fractions and congestive heart failure. 19991;325:293-302.
2. Investigators. Effect of enalapril on mortality and the development of heart failure in asymptomatic ventricular ejection fractions. N Engl J Med 1
3. Pfeffer MA. Blaunwald E, Move LA. et al. Effects of caotomil on
4,
5. 6.
7.
8.
9.
10.
II.
I?.
13.
14.
mortality and morbidity in patients with left ventricular dysfun&n after myocardial infarction. N Engl J 2~32~~9-71. Yusuf S, Pepine 0. Garces C. et al. Effect of enalapril on rny~~~~ infarction and unstable angina in patients with low ejection factions.
AstropT. The b~o:~~ica~ ~~~~~~~a~~~~ ~~~b~~~ys~s. Lancet 1956;2:565-8. Kruitbof EKO, Gudinchet A, ~acbmann F. ~~asrninog~~ activator inhib- itor I and plasm~~8eo activator inhibrtor 2 in various disease states. Thromb Haemostas 1988;59:?-12. ~idker Ph4. Vaughan DE. Stampfer
asmino~en :1165-8. rsen J. A depression of active tissue plasmin-
ogen activator in plasma characterises patients with unstable angina pectoris who develop myocardic: infarction. Eur Heart J 199Ql I:SZS-8. Jansson JH. Nilsson TK. Olofsson ssue ~~asn~~noge~ activator and other risk factors as predictox of ascular events in patient3 with severe angina pectoris. Eur Heart 1X57-61. Gram J. Jespersen J. A selective depression of tissue plasmlna~e~ activator (t-PA) activity in englobM~i~ characteristix a risk group among survivors of acute myocardial infarction. T~~~rnb Haemostas 1%?;57:
son 80. Nilssoo TK. ~d~~:~ve value of tissue plas- mass concentration on long-term mortaliry in patients
artery disease: a 7 year follow up. Circulation 1993;88:
Hamsten A. Wiman 5. De Faire U. Blomback M. increased levels of a rapid itor of tissue plasrn~n~e~ activator in young survivors of myoc in~~ct~o~. N Engl J k&d l985;3~3:~S5~~63. Hamsten A. De Faire U. Walldius 6. et al. Plasminogen activator inhibitor in plasma: risk factor for recurrent myocardial infarction. Lancet 198%2:3-9. Vague P. Juban-Vague I. Aillaud MF. et al. Correlation tx%ween blood Linolytic activity. plasminogen activator inbibitor level. plasma insulin level, and relative body weight in nornxl and obese sigbi~cts. Metabolism 1986:35:250-3. - -
IS. Juhan-Vague 1. Alessi MC. Joly P. et al. Plasma p~sm~~oge~ activator inhibitor-l in angina pectoris; influence of plasma insulin and acute-phase response. Arteriosclerosis 1989393362-7.
16. Alessi MC, Juhan-Vague 1. Kooistra T, Declerck PJ, Collen D. Insulin stimulates the synthesis of plasminogen activator 1 by the hepatocellular cell iine Hep G2. Thromb Haemostas l!J!#f+4cl~=4
17. Kooistra T, Bosma PJ. Tons HAM, vata 4Cil iifig Ar. Leyer P, Princen HMG. Piasminogen activator inhibitor I: biosynthesis and mRNA level are increased by insulin in cultured human hepatocytes. Tbromb Haemo- stas 1989;61:723-8.
18. Pollare T. Lithell H. Beme C. A comparison of the effects of hydrochlo- rothiazide and captopril on glucose and lipid metabolism in patients with hypertension. N Engl J Med 1989;321:868-73.
19. Ridker PM, Gabouty CL, Conlin PR. Seely EW, Williams GH. Vau8han DE. Stimulation of plasmino8en activator inhibitor in vivo by i&ion of angiotensin ii: evidence of a potential intelaction between the renin- aqiotensin system fibrinolytic function. Circulation 1993;87:1969-73.
20. Gram J, KluR C, Jespersen J. Depression of tissue plasminogen activator (t-PA) activity and rise of t-PA inhibition and acute phase reactants in blood of patients with acute myocardial infarction (AME). Thromb Hae- mostas 1987;58:817-21.
21. Ranby M. Bergsdorf N. Nilsson T. ~e~lb~~g 6, Winblad B. Bucht G. Age dependance of tissue plasminogen activator concentrations in plasma. as studied by an improved enzyme linked immunosorbent assay. Clin Chem 1986;32:21605.
22. Chmielewska J, Ranby M, Wiman B. Evidence for a rapid inhibitor to tissue plasminogen activator in plasma. Thromb Res 1983;31:427-36.

JACC Vol. 24, No. 1 July tW&67-73
2.3. ~~ld~e6 JS, She CriticaP variables in the 6adicim serum insulirr using the dailble antibody technic. Diabeks i%5;14:771-9.
Lmcore CL,
Evidence for increased levels of tissue ~~asrni~ogeo activator in
Scbmer G. Diurnal variation of tissue-type s rapid io~i~itor (PAlmI). Circulation 19S(p;79:
30.
31.
32.
33.
34.
a~g~ote~sin converting enzyme ~~~i~~t~oo on c~~c~~at~og and local kitin levels. Am J Cardiol l982;4~140~-4.
ulation of the acute release of tissue-type ~~asm~oo~eo g~~at~ao activation products. Ann
type 1 in patients with 1~4;~279-82.
mmogen activator release during specific assay. Ciin Cbim
Gray RF, Patterson Yudkin JS. Blasminogen activator inhibitor tic and &diabetic survivors of myocardial i
~ Ikram H, Espiner EA. Turner JG. Waemo- rolyte responses to withdrawal of lone-term
captopril t~eatmemt kr failure. Lancet 1981;2:959-61.