effectively operating the household model by steve shields © action pact holdings, llc
TRANSCRIPT
Effectively Operating the Household Model
By Steve Shields© Action Pact Holdings, LLC
13 Years Ago-• Less than 5 organizations with less than 30
households
Today-• More than 300 organizations with more than
1500 households
• Still less than one percent of total nursing home accommodation supply

13 years ago we weren't sure, now we are…
• Hundreds are doing it, thousands are considering it, and a handful don’t know what it is. Most are having difficulty navigating the course required.
• Which group do you want to belong to?

Regulatory Considerations
• Pioneering organizations have taken a lot of the initial regulatory risk
• CMS is on board and fully backs the household model• Regulations are still up to the particular surveyor’s
interpretation which can create friction• However, CMS has stated to providers and surveyors that
any violation should be the start of the discussion between provider and regulator – in other words the surveyor’s first word should never be their final word
• Slowly, but surely, moving toward a regulatory environment where resident directed care is required
The establishment of a healthy and sustainable home comes though the integrated balance of:
Resident directed life Leadership (values driven and resource bearing) Organizational structure (decentralized self-led teams) Physical environment (reflects home) Financial sustainabilityThese aspects, kept in balance, produces the business plan and framework for sure-footed transformation

The Essential Elements
1. The household is each resident’s home and sanctuary 2. The people who live here direct their own lives, individually
and collectively.3. The boundaries of the person and his/her home are clear
and respected as a matter of course.4. Grace, a shared sense of what is sacred about the house and
its people, is deeply valued, consciously created and preserved. Ritual, spontaneity, friendship, spirituality, celebration, recreation, choice, interdependence, art and humor are all manifestations of a culture of grace.
5. The people who live here are loved and served by a responsive, highly valued, decentralized, self-led service team that has responsibility and authority.

The Essential Elements (continued)6. Leadership is a characteristic, not a position. Leaders support and
are supported by values-driven, resource bearing principles and practices as a way for each person to actualize his or her full potential.
7. All systems, including treatments, exist to support and serve the person, within the context of his or her life pursuits
8. We build strong community with one another, our family, our neighbors and our town. Each household is part of a neighborhood of houses, dedicated to continuous learning.
9. The physical building and all it amenities are designed to be a true home. Institutional creep in design and culture is treated as a wolf at the door.
10. The establishment of a healthy and sustainable home comes through the integrated balance of resident-driven life, leadership, organizational structure, physical environment and financial sustainability.

Values Driven, Resource Bearing Leadership
Belief Shaping & Alignment to VisionGrowing Skills and JudgmentOvercoming mis-used hierarchy and silo thinking Understanding that new models and new ways of
operating require new development, framework, strategic sequencing and decision making processes
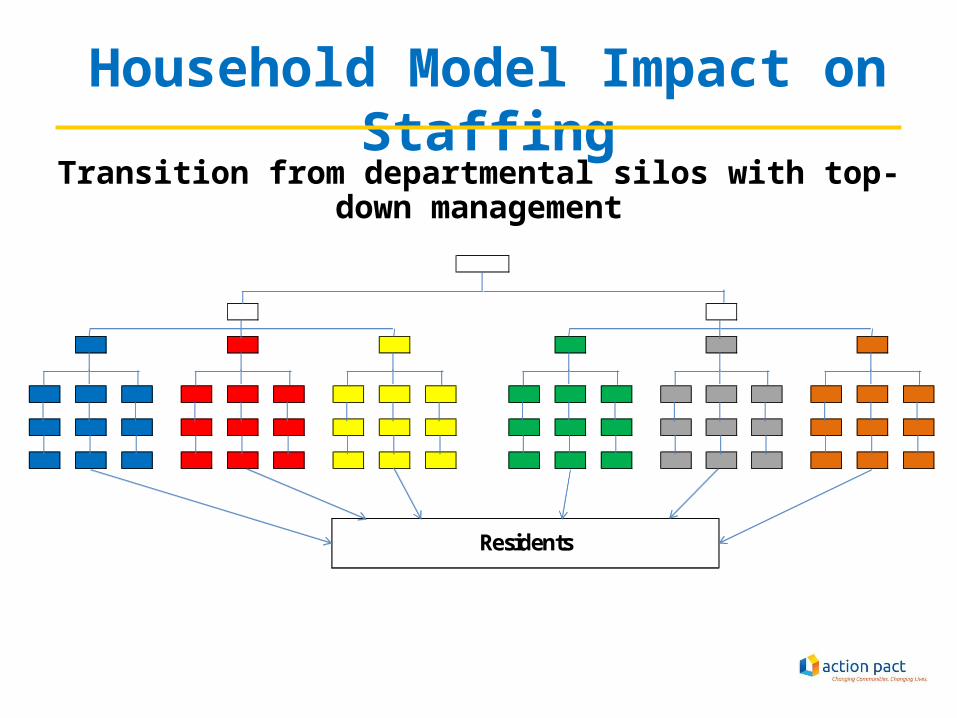
Household Model Impact on StaffingTransition from departmental silos with top-down management
Residents

Silos within the institution produce visible outcomes that we have learned to become insensitive to and cannot correlate to
lack of service-line integration
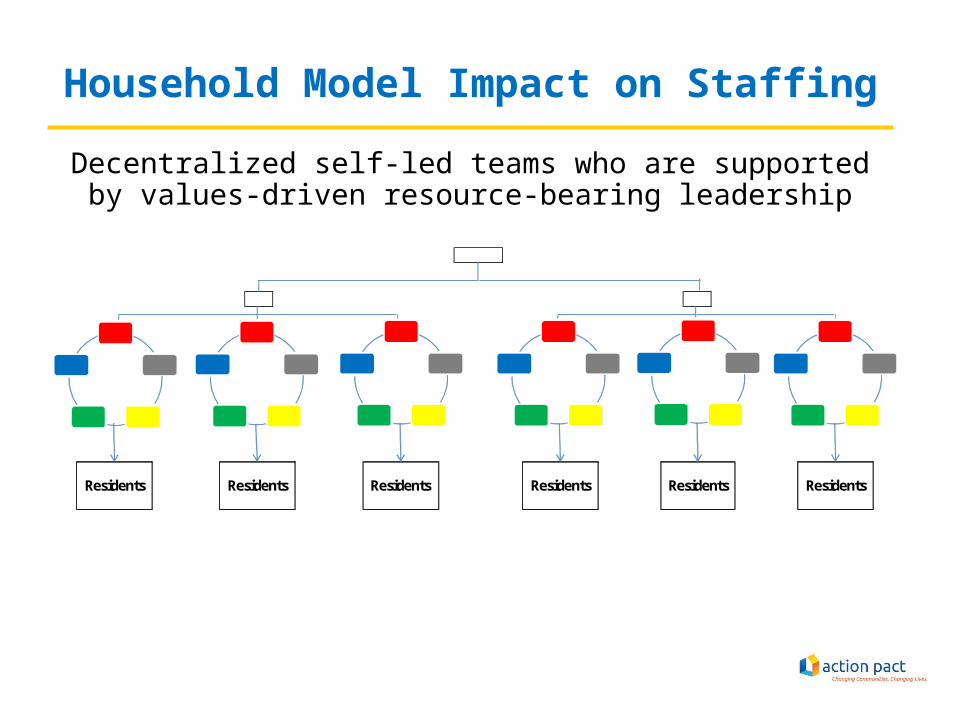
Household Model Impact on StaffingDecentralized self-led teams who are supported by values-driven
resource-bearing leadership
Residents Residents Residents Residents Residents Residents
Household Model Impact on Staffing
• Comprehensive training must occur to transition from departmentally siloed workers to versatile workers Organizational training to create a framework for culture change Cross training of staff to extent possible
• CNA’s receive dietary, housekeeping and activities training• Dietary aides receive CNA and activities training• Etc
Office/Department staff come out from behind the walls and are assigned to houses• 80/20 Rule

General Staffing Descriptions Household Coordinator (Can be anyone that displays leadership
characteristics; generally a non-nurse)– Responsible for overall non-clinical care of household, including food service,
housekeeping, personal care and activities– Does scheduling for household– Partners with the Household Nurse Leader to build teamwork and assure a good
household life– Coordinates hiring and other HR functions of the household together with HR
and each specific disciplines’ mentor Household Nurse Leader (Generally an RN)
– This is a combined job with another nurse leader function such as RAI Specialist or Assistant Director of Nursing
– Responsible for overall clinical care of household residents– Manages clinical quality in the household– Partners with Household Coordinator to build teamwork and assure a good
household life
General Staffing Descriptions (Continued)
Nurses (Generally LPN’s)– Pass and manage medications– Do treatments – Assess condition and needs– Assist with dining, personal care and activities
Nursing Assistants (Generally CNA’s)– Provide personal care– Assist with dining; assist with food preparation and service– Launder resident/guest clothing as needed– Assist with housekeeping– Initiate and assist with spontaneous and planned activities
General Staffing Descriptions (Continued)
Homemakers (Generally housekeeping, activities, or dietary workers)– Prepare and serve food; do housekeeping– Initiate and assist with spontaneous and planned activities
Social Worker – May serve multiple households– Guides household team members in helping to assure the
social/emotional well-being of residents/guests– Participates in assessing and care planning
Each employee not assigned to a Household would adopt a Household and spend time in that Household lending a helping hand and building relationships with the residents and staff
The Physical Environment Reflects Home
Spatial RelationshipsHome is in the DetailsKitchenSquare Footage and Capacity (size of house & number of houses)


Design Driving Principles• Operating Philosophies• Spatial Relationships• Circulation Arteries• Indoor/Outdoor Entrances• Access to Out of Doors• Food Service• Storage / Utility Rooms• Staff work spaces• Increase/Decrease in Census• Spa vs. Resident Room Bathing• House Sizes / Types of Houses
Operating Philosophies Sanctity of Home – boundaries of each home must be
respected as in a neighborhood of individual houses Degrees of privacy– What makes your home safe and comfortable?
• Public spaces• Semi-private spaces• Private spaces
– To what degree a visitor can enter the spaces in your home depends on your relationship with that person
– Need to restore these boundaries in order to provide a real home to elders
Design as if it were your Home, not someone else’s Home
Indoor/Outdoor Entrances• Do you have a preference if you enter each house
from the outside or from an inside-the-building entrance?
• Current plant layout will influence this• Either way you will still have a front door to each
house• Affects how people and food/supplies circulate
around the campus• Can impact how the campus is viewed by the
external world



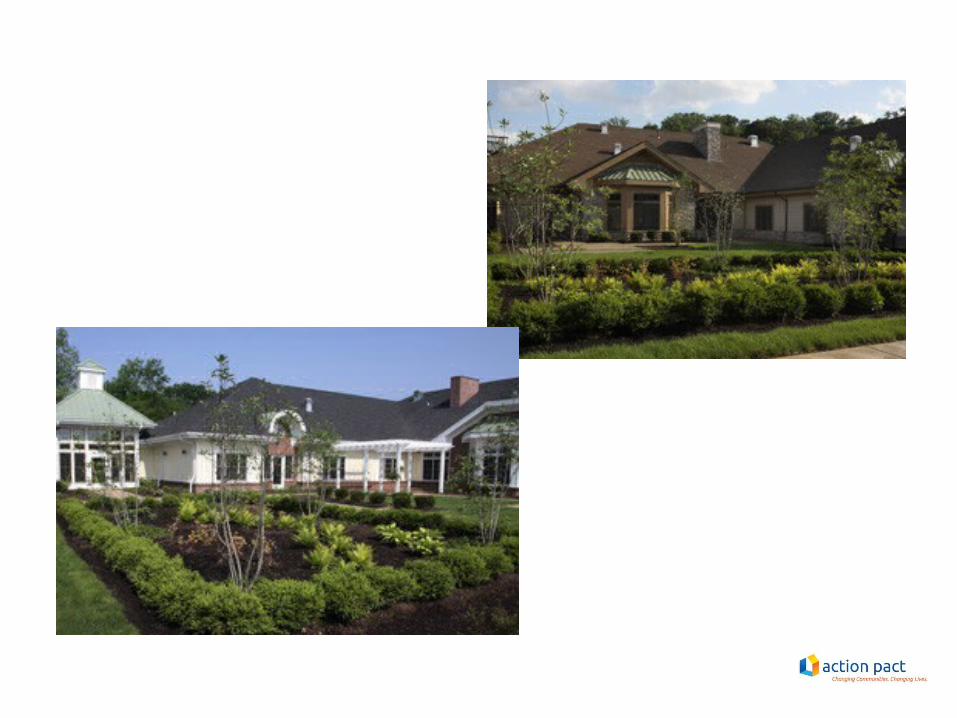
Access to Out of Doors
• Access to the outside is an important aspect of life
• Access to the outside should be through a public side of the house, not through a bedroom hallway
• Out of Doors space can take many forms – patio, garden, courtyard, screened-in porch, etc.

© Action Pact Development, LLC

Food Service• Kitchen is the heart of the home – very
important element of design and operations• Design decisions will put a ceiling on what
can be done in the house versus what has to be done in central kitchen
• If you can design with no ceiling, this can allow competencies to grow over time and allows for great flexibility, but can increase upfront cost
Food Service (continued)
Household Options for Food Service– Prepared and cooked in central kitchen; delivered to
household kitchen and served there– Prepared in central kitchen and delivered to household
kitchen; household kitchen cooks the food and serves it– Prepared, cooked, and served in the household kitchen
Can be any combination of the three options and can vary by house (i.e. can cook breakfast to order in the houses, but not the other two meals)

Food Service (continued)
What does a household model kitchen look like?– Household kitchen
• Looks like your personal home kitchen• Resident refrigerator, sinks, counters, cabinets, etc• Stoves can be a fire safety issue and it is very important to think
through– If cooking is done in the house, commercial hood and fire
prevention solutions would be required
– Pantry• Industrial elements are kept here out of sight
– Food storage shelving, industrial refrigeration, three hole sink, commercial dishwasher


Storage / Utility Rooms Even though we are designing it as a
residential home, there are still areas that are necessary to meet regulations and storage needs
Incorporate these rooms throughout the house– Storage areas for supplies and equipment– Clean and soiled utility– Residential washer / dryer area– Medication storage / dispensing
Staff Work Areas How do we provide work areas for staff?– Generally the Household philosophy is to sprinkle work
stations throughout the house– Don’t generally design dedicated offices for specific
individuals within the household, but we do seek office adjacencies where possible• Eats up valuable square footage• We want the household workers to be out in the house with the
residents• Can utilize multi-purpose rooms – such as the den or private dining
room – as staff meeting space when necessary• Full recognition of need for privacy, at times, and adequate space for
work

Increase / Decrease in Census Depends on a variety of factors– What will be retrofit vs. new construction?– Is your market over or under supplied?– Do you currently have a lot of semi-private rooms and
little space to work with?– Do you have land available for new construction?– Can you pay for the physical modifications without
the benefit of increased revenue from adding census?
Spa vs. Resident Room Bathing
• How is facility currently set up?• Making sure each house has a spa that can
provide a warm and relaxing bathing experience is ideal
• Are there existing bathrooms that can be converted in an economic fashion?
• Private Ensuites when possible
House Sizes Number of residents per house– If it is a retrofit, will be driven somewhat by
architectural layout, but we do need to set some parameters
– There is no “right” number – it depends on a variety of factors
– Culturally, houses from 10 to 20 work• While some think 10-12 is best, they don’t seem to provide the
best “life” – there are fewer residents and staff from which you can choose to
build relationships with– Staff call-offs become a real issue– Total number of staff in the house is very low which can inhibit the
creation of “life”• When you get above 20-22, it starts to become difficult to
maintain the culture
House Sizes Number of residents per house (con’t)
– Financially (for staffing ratio reasons), houses of 16 – 25 work best• There is a minimum number of staff needed in a house at
any one time regardless of number of residents• The greater the number of residents, the lower staff per
resident ratio you can achieve– If you overlap best cultural and financial
outcomes, the range of residents per house is best between 16-20.
Types of Houses Can create specialized houses based on certain
resident needs– Memory Support– Short-term stay rehab– Houses can be very flexible for future specialized needs
Households do have residents of varying acuities though– Doesn’t make sense to stratify residents based on level
of care – would need to move them as they became more frail
– Residents should choose homes based on who they love, not their physical condition
© Action Pact Development, LLC
– Where one’s
good life continues
Households