effective 12-18-2006 emergency medical...
TRANSCRIPT
Effective 12-18-2006
EMERGENCY MEDICAL SERVICES RULES OF THE
DEPARTMENT OF HEALTH CHAPTER 64E-2, FLORIDA ADMINISTRATIVE CODE (F.A.C.)
EMERGENCY MEDICAL SERVICES 64E-2.001 Definitions 64E-2.002 Basic Life Support Service License - Ground 64E-2.003 Advanced Life Support Service License - Ground 64E-2.004 Medical Direction 64E-2.005 Air Ambulances 64E-2.006 Neonatal Interfacility Transfers 64E-2.007 Vehicle Permits 64E-2.008 Emergency Medical Technician 64E-2.009 Paramedic 64E-2.0094 Voluntary Inactive Certification 64E-2.0095 Involuntary Inactive Certification 64E-2.010 Examinations 64E-2.012 Drivers 64E-2.013 Records and Reports 64E-2.015 Prehospital Requirements for Trauma Care 64E-2.016 Trauma Transport Protocols Approval and Denial Process 64E-2.017 Adult Trauma Scorecard Methodology 64E-2.0175 Pediatric Trauma Scorecard Methodology 64E-2.018 Trauma Registry 64E-2.019 Trauma Agency Formation Requirements 64E-2.020 Trauma Agency Plan Approval and Denial Process 64E-2.021 Trauma Agency Implementation and Operation Requirements 64E-2.022 Apportionment of Trauma Centers
within a Trauma Service Area (TSA) 64E-2.023 Trauma Center Requirements
64E-2.024 Process for the Approval of Trauma Centers
64E-2.025 Extension of Application Period 64E-2.026 Certificate of Approval 64E-2.027 Process for Renewal of Trauma Centers 64E-2.028 Site Visits and Approval 64E-2.029 Application by Hospitals Denied Approval 64E-2.030 Emergency Medical Services Grants Procedures 64E-2.031 Do Not Resuscitate Order (DNRO)
Form and Patient Identification Device 64E-2.032 Certificate of Public Convenience and Necessity
64E-2.033 Convicted Felons Applying for EMT or Paramedic Certification or Recertification
64E-2.034 Inspections 64E-2.035 Emergency Treatment of Insect Stings 64E-2.036 Training Programs 64E-2.037 Security of Medications 64E-2.038 Cardiopulmonary and Advanced
Cardiac Life Support Courses 64E-2.039 Guidelines for Automated External
Defibrillators (AED) in State Owned or Leased Facilities
64E-2.040 Funding for Verified Trauma Centers
EFFECTIVE 12-18-2006 Emergency Medical Services
2
64E-2.001 Definitions. In addition to the definitions provided in Sections 395.401, 395.4001, 401.107, and 401.23, F.S., the following definitions apply to these rules: (1) Abbreviated Injury Score (AIS-90) - means a consensus derived, anatomically based system that classifies individual injuries by body region on a 6-point ordinal severity scale ranging from 1 to 6. The methodology for determining AIS-90 Code is found in the "Abbreviated Injury Scale 1990 – Update 98,” which is incorporated by reference and is available from the Association for the Advancement of Automotive Medicine, P.O. Box 4176, Barrington, IL 60011-4176. (2) Application - means a completed application form, as specified by the department, together with all documentation required by these rules and the required fee. (3) Burn - means a tissue injury resulting from excessive exposure to thermal, chemical, electrical or radioactive agents.
(4) Certification Examination – means an examination developed or adopted by the department to be used for the purpose of testing the ability to practice as a Florida licensed emergency medical technician or paramedic.
(5) Chief – means the chief of the department’s Bureau of EMS.
(6) Controlled Substances – means those drugs listed in Chapter 893.03, F.S. and the “designer drugs” referred to in Chapter 893.035, F.S.
(7) Conviction – means a determination of guilt of a felony in any court of competent jurisdiction which is the result of trial of the entry of a plea of guilty or a plea of nolo contendere, regardless of whether adjudication is withheld.
(8) Department – means the Florida Department of Health (DH), Bureau of Emergency Medical Services, 4052 Bald Cypress Way, Bin C18, Tallahassee, Florida 32399-1738. (9) Emergency Medical Services Provider – means any entity licensed in the state of Florida to provide air, or ground ambulance, whether basic life support (BLS) or advanced life support (ALS), and whether a non-transportation or a transportation service. (10) Glasgow Coma Scale Score - means the neurological assessment developed by G. Teasdale and B. Jennitte in "Assessment of Coma and Impaired Consciousness: A Practical Scale" Lancet, 1974; 2: 81-84, which is incorporated by reference and available from the department. (11) ICD-9-CM - means the “International Classification of Disease, 9th Revision, Clinical Modification”, March, 1989, U.S. Department of Health and Human Services Publication No. (PHS)
89-1260; an internationally applied method by which diseases or groups of medical conditions or injuries are coded for the purpose of statistical analyses. This book is incorporated by reference and available for purchase from the American Hospital Association, Central Office on ICD-9-DM, 1-800-242-2626, AHA, Post Office Box 92683, Chicago, IL 67675-2683. (12) Injury Severity Score (ISS) - means the sum of the squares of the highest AIS-90 code in each of the three most severely injured body regions. The method for computing ISS is found in the "Abbreviated Injury Scale 1990 – Update 98." (13) Neonatal Ambulance - means an ALS permitted vehicle which is designated solely to interfacility transports of neonates to a Level II or Level III neonatal intensive care unit. (14) Neonatal Transport - means the transport of any neonate requiring emergency transfer from a hospital licensed under Chapter 395 F.S., to a Level II or Level III neonatal intensive care unit. (15) Neonate - means an infant less than 28 days of life and or less than 5 kg. (16) “Operate”, “Operates” or “Operation” - means providing, offering to provide, soliciting, or advertising prehospital or interfacility ALS services or BLS transportation services as further described in Rule 64E-2.032, F.A.C. (17) Patient Care Record – means the record used by each EMS provider to document patient care, treatment and transport activities that at a minimum includes the information required under paragraphs 64E-2.003(5)(a)(b), Rule 64E-2.013, subsection 64E-2.015(5), subsections 64E-2.017(5), (6), (7), 64E-2.0175(4), F.A.C. (18) Pediatric Trauma Patient - means a trauma patient with anatomical and physical characteristics of a person 15 years of age or younger. (19) Training Program - means an educational institution having one designated program director, one designated medical director, and single budget entity; for the purposes of providing EMT or paramedic education programs, as approved by the department. (20) Trauma - means a blunt, penetrating or burn injury caused by external force or violence. (21) Trauma Alert - means a notification initiated by EMS informing a hospital that they are en route with a patient meeting the trauma alert criteria. (22) Trauma Alert Patient - means a person whose primary physical injury is a blunt, penetrating or burn injury, and who meets one or more of the adult trauma scorecard criteria in Rule 64E-2.017, F.A.C., or the pediatric trauma scorecard criteria in Rule 64E-2.0175, F.A.C.

EFFECTIVE 12-18-2006 Emergency Medical Services
3
(23) Trauma Patient - means any person who has incurred a physical injury or wound caused by trauma and who has accessed an emergency medical services system. (24) Trauma Registry - means a statewide database which integrates medical and system information related to trauma patient diagnosis and the provision of trauma care by prehospital, hospital, and medical examiners. (25) Trauma Transport Protocols (TTPs) - means a document which describes the policies, processes and procedures governing the dispatch of vehicles, and the triage and transport of trauma patients. Specific Authority 381.0011(13), 395.401, 395.4025(13), 395.405, 401.121, 401.35 FS. Law Implemented 381.0011, 395.401, 395.4001, 395.4015, 395.402, 395.4025, 395.403, 395.404, 395.4045, 395.405, 401.121, 401.211, 401.23, 401.25, 401.35, 401.435 FS. History-New 11-29-82, Amended 4-26-84, 3-11-85, 11-2-86, 4-12-88, 8-3-88, 8-7-89, 6-6-90, Formerly 10D-66.485, Amended 12-10-92, 11-30-93, 10-2-94, 1-26-97. Formerly 10D-66.0485. Amended 08-04-98, 07-14-99, 02-20-00, 11-3-02, 06-09-05, 10-24-05. 64E-2.002 Basic Life Support Service License - Ground. (1) To obtain a license or renewal each applicant shall submit an application to the department on DH Form 631, October 05, Ground Ambulance Service Provider License Application. This form is incorporated by reference and is available from the department, as defined by subsection 64E-2.001(8), F.A.C.
(2) The department shall issue a license to any applicant who: (a) Furnished evidence of insurance coverage for claims arising out of injury or death of persons and damage to the property of others resulting from any cause for which the owner of said business or service would be liable. Each motor vehicle shall be insured for the sum of at least $100,000 for injuries to or death of any one person arising out of any one accident; the sum of at least $300,000 for injuries to or death of more than one person in any one accident; and, for the sum of at least $50,000 for damage to property arising from any one accident. Government operated service vehicles shall be insured for the sum of at least $100,000 for any claim or judgment and the sum of $200,000 total for all claims or judgments arising out of the same occurrence. Every insurance policy or contract for such insurance shall provide for the payment and satisfaction of any financial judgment entered against the operator and present insured, or any
person driving the insured vehicle. All such insurance policies shall provide for 30-day cancellation notice to the department. (b) Obtained a Certificate of Public Convenience and Necessity (COPCN) consistent with the requirements of Rule 64E-2.032, F.A.C. (3) Each BLS provider shall ensure and document in its employee records that each of its EMTs and paramedics hold a current certification from the department. (4) Every provider, except those exempted in paragraph 64E-2.006(1)(a), F.A.C., shall ensure that each EMS vehicle permitted by the department, when available for call, shall be equipped and maintained as approved by the medical director of the service in the vehicle minimum equipment list. The vehicle minimum equipment list shall include, at a minimum, one each of the items listed in Table I and shall be provided to the department upon request.

EFFECTIVE 12-18-2006 Emergency Medical Services
4
TABLE I
GROUND VEHICLE BLS MEDICAL EQUIPMENT AND SUPPLIES
1. Bandaging, dressing, and taping supplies: a. Adhesive, silk, or plastic tape- assorted sizes. b. Sterile 4x4 inch gauze pads. c. Triangular bandages. d. Roller gauze. e. ABD (minimum 5x9 inch) pads. 2. Bandage shears. 3. Patient restraints, wrist and ankle. 4. Blood pressure cuffs: infant, pediatric, and adult. 5. Stethoscopes: pediatric and adult. 6. Blankets. 7. Sheets (not required for non-transport vehicle.) 8. Pillows with waterproof covers and pillow cases or disposable single use pillows (not required for non-transport vehicle). 9. Disposable blanket or patient rain cover. 10. Long spine board and three straps or equivalent. 11. Short spine board and two straps or equivalent. 12. Adult and Pediatric cervical immobilization devices(CID), approved by the medical director of the service. 13. Padding for lateral lower spine immobilization of pediatric patients or equivalent. 14. Portable oxygen tanks, "D" or "E" cylinders, with one regulator and gauge. Each tank must have a minimum pressure of 1000 psi and liter flow at 15 liters per minute. 15. Transparent oxygen masks; adult, child and infant sizes, with tubing. 16. Sets of pediatric and adult nasal cannulae with tubing. 17. Hand operated bag-valve mask resuscitators, adult and pediatric accumulator, including adult, child and infant transparent masks capable of use with supplemental oxygen. 18. Portable suction, electric or gas powered, with wide bore tubing and tips which meet the minimum standards as published by the GSA in KKK-A 1822E specifications. 19. Extremity immobilization devices. Pediatric and Adult. 20. Lower extremity traction splint. Pediatric and Adult. 21. Sterile obstetrical kit to include, at minimum, bulb syringe, sterile scissors or scalpel, and cord clamps or cord-ties. 22. Burn sheets. 23. Flashlight with batteries. 24. Occlusive dressings. 25. Oropharyngeal airways. Pediatric and Adult. 26. Installed oxygen with regulator gauge and wrench, minimum "M" size cylinder (minimum 500 PSI) with oxygen flowmeter to include a 151pm setting,(not required for non-transport vehicles). Other installed oxygen delivery systems, such as liquid oxygen, as allowed by medical director. 27.Gloves - suitable to provide barrier Sufficient quantity, protection for biohazards. sizes and material for all crew
members.
EFFECTIVE 12-18-2006 Emergency Medical Services
5
28. Face Masks -both surgical and Sufficient quantity, sizes, and material respiratory protective. for all crew members. 29. Rigid cervical collars as approved in writing by the medical director and available for review by the department. 30. Nasopharyngeal airways, pediatric and adult. 31. Approved biohazardous waste plastic bag or impervious container per chapter 64E-16, F.A.C. 32. Safety goggles or equivalent meeting A.N.S.I. Z87.1 One per crew member. standard. 33. Bulb syringe separate from obstetrical kit. 34. Thermal absorbent reflective blanket. 35. Multitrauma dressings. 36. Pediatric length based measurement device for equipment selection and drug dosage. Specific Authority 381.0011, 395.405, 401.121, 401.25, 401.35 FS. Law Implemented 381.0011, 395.401, 395.4015, 395.402, 395.4025, 395.403, 395.404, 395.4045, 401.23, 401.24, 401.25, 401.252, 401.26, 401.27, 401.281, 401.30, 401.31, 401.321, 401.34, 401.35, 401.41, 401.411, 401.414, 401.421 FS. History-New 11-29-82, Amended 4-26-84, 3-11-85, Formerly 10D-66.49, Amended 4-12-88, 8-3-88,12-10-92, 10-2-94, 1-26-97. Formerly 10D-66.049. Amended 8-4-98, 1-3-99, 11-19-01, 12-18-06.
EFFECTIVE 12-18-2006 Emergency Medical Services
6
64E-2.003 Advanced Life Support Service License - Ground. (1) To obtain a license or renewal each applicant for an ALS license shall submit to the department DH Form 631, October 05, Ground Ambulance Service Provider License Application, which is incorporated by reference and available from the department, as defined by section 64E-2.001(8), F.A.C. (2) Each ALS provider shall ensure and document in its employee records that each of its EMTs or paramedics hold a current certification from the department. (3) Each ALS provider shall ensure that a current copy of all standing orders authorized by the medical director shall be available in each of the provider’s vehicles; for review by the department; to each of the provider’s paramedics; and supplied to each physician designated by the medical director to receive a copy. (4) Each ALS permitted vehicle, when available for call, shall be equipped and maintained as approved by the medical director of the service in the vehicle minimum equipment list. The vehicle minimum equipment list shall include, at a minimum, one each of the items listed in Table I and II, and shall be provided to the department upon request, except those exempted in paragraph 64E-2.006(1)(a), F.A.C. Substitutions are allowed with signed approval from the medical director and written notification to the department. (5) The medical director may authorize an EMT instead of the paramedic or licensed physician to attend a BLS patient on an ALS permitted ambulance under the following conditions: (a) The medical director determines what type of BLS patient may be attended by an EMT and develops standing orders for use by the EMT when attending the type of BLS patients identified. The on scene paramedic shall conduct the primary patient assessment to determine if the patient’s condition meets the criteria in the standing orders for BLS care. This survey shall be documented on the patient care record and shall identify the paramedic who conducted the survey. (b) The patient care record for any patient care or transport shall clearly state whenever an EMT attends the patient. (c) The provider shall maintain and have accessible for review by the department documentation of compliance with the above requirements.
(6) ALS Nontransport:
(a) Unless otherwise specifically exempted, each advanced life support nontransport vehicle, when personnel are providing advanced life support treatment or care, must be staffed with a certified paramedic or licensed physician. (b) A permitted advanced life support nontransport vehicle may operate as a basic life support emergency vehicle when the vehicle is not staffed by a certified paramedic or licensed physician and only in lieu of placing the unit completely out of service. When such advanced life support nontransport vehicle is operating under this section, the vehicle must be staffed with at least one person who must be an emergency medical technician, and shall carry portable oxygen, airway adjuncts, supplies and equipment as determined by the medical director of the licensed service.
1. Each service provider having permitted vehicles operating pursuant to this section shall log changes in vehicle status.
2. Vehicles operating pursuant to this section shall not display markings indicating advanced life support (other than permit sticker) when responding as basic life support emergency vehicle. (c) Unless otherwise specifically exempted, the following advanced life support non-transport vehicles when personnel are providing emergency treatment or care, must be staffed, at a minimum, with a certified paramedic or licensed physician:
1. Advanced life support vehicles that respond to requests to provide emergency treatment or care during special events or activities or in locations where access by permitted transport vehicles is restricted or limited.
2. Advanced life support vehicles that respond to requests to provide emergency treatment or care in vehicles that cannot accommodate two persons, due to design and construction of the vehicle.
3. Advanced life support vehicles under 13,000 pounds gross vehicle weight that respond to requests to provide emergency treatment or care and are met at the scene by other concurrently responding permitted vehicles. Examples include vehicles that respond to requests to provide emergency treatment or care within a gated or restricted community that is established pursuant to Chapter 190, F.S.; vehicles that respond to requests to provide emergency treatment or care which are owned or operated by counties or municipalities established pursuant to Chapters 125 or 166, F.S.; or vehicles that respond to requests to provide emergency treatment and care which are owned or operated by advanced life support services licensees. Vehicles staffed pursuant to this section shall operate in accordance with a certificate of public convenience and necessity.

EFFECTIVE 12-18-2006 Emergency Medical Services
7
4. Advanced life support non-transport vehicles over 13,000 pounds gross vehicle weight that respond to requests to provide emergency treatment or care. Vehicles staffed pursuant to this section shall operate in accordance with a certificate of public convenience and necessity.
(d) Vehicles staffed pursuant to paragraph 64E-2.003(6)(c), F.A.C., may respond to requests for medical assistance in accordance with Section 252.40, F.S., or in accordance with a mutual aid agreement executed pursuant to Rule 64E-2.032, F.A.C.
(e) Nothing herein shall prohibit an on duty certified EMT or paramedic who arrives on scene from initiating emergency care and treatment at the level of their certification prior to the arrival of other responding vehicles.
(7) Advanced life support non-transport vehicles staffed pursuant to paragraph 64E-2.003(6)(c), F.A.C., are not required to carry the equipment and supplies identified in Table III or V. Such vehicles when personnel are providing advanced life support treatment or care, or when responding to calls in an ALS capacity shall at a minimum carry portable oxygen, defibrillation equipment, airway management supplies and equipment, and medications and fluids authorized by the medical director of the licensed service.
EFFECTIVE 12-18-2006 Emergency Medical Services
8
TABLE II
GROUND VEHICLE
ALS EQUIPMENT AND MEDICATIONS
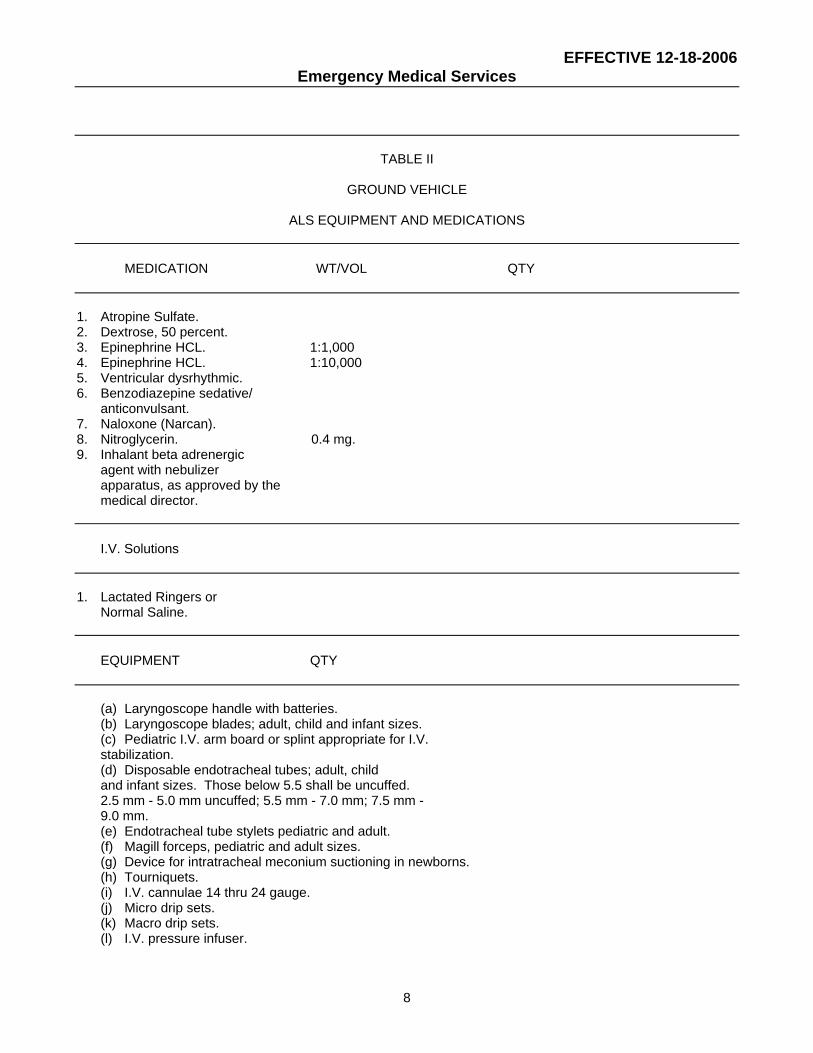
MEDICATION WT/VOL QTY 1. Atropine Sulfate. 2. Dextrose, 50 percent. 3. Epinephrine HCL. 1:1,000 4. Epinephrine HCL. 1:10,000 5. Ventricular dysrhythmic. 6. Benzodiazepine sedative/ anticonvulsant. 7. Naloxone (Narcan). 8. Nitroglycerin. 0.4 mg. 9. Inhalant beta adrenergic agent with nebulizer apparatus, as approved by the medical director. I.V. Solutions 1. Lactated Ringers or Normal Saline. EQUIPMENT QTY (a) Laryngoscope handle with batteries. (b) Laryngoscope blades; adult, child and infant sizes. (c) Pediatric I.V. arm board or splint appropriate for I.V. stabilization. (d) Disposable endotracheal tubes; adult, child and infant sizes. Those below 5.5 shall be uncuffed. 2.5 mm - 5.0 mm uncuffed; 5.5 mm - 7.0 mm; 7.5 mm - 9.0 mm. (e) Endotracheal tube stylets pediatric and adult. (f) Magill forceps, pediatric and adult sizes. (g) Device for intratracheal meconium suctioning in newborns. (h) Tourniquets. (i) I.V. cannulae 14 thru 24 gauge. (j) Micro drip sets. (k) Macro drip sets. (l) I.V. pressure infuser.
EFFECTIVE 12-18-2006 Emergency Medical Services
9
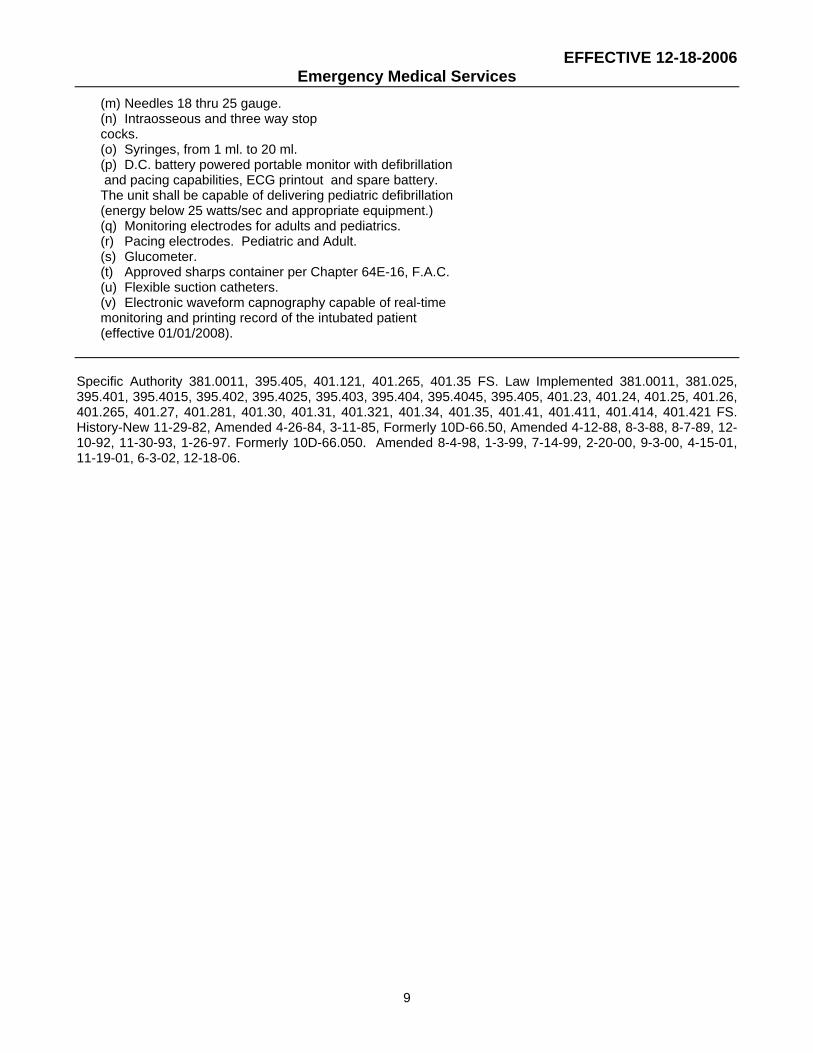
(m) Needles 18 thru 25 gauge. (n) Intraosseous and three way stop cocks. (o) Syringes, from 1 ml. to 20 ml. (p) D.C. battery powered portable monitor with defibrillation and pacing capabilities, ECG printout and spare battery. The unit shall be capable of delivering pediatric defibrillation (energy below 25 watts/sec and appropriate equipment.) (q) Monitoring electrodes for adults and pediatrics. (r) Pacing electrodes. Pediatric and Adult. (s) Glucometer. (t) Approved sharps container per Chapter 64E-16, F.A.C. (u) Flexible suction catheters. (v) Electronic waveform capnography capable of real-time monitoring and printing record of the intubated patient (effective 01/01/2008). Specific Authority 381.0011, 395.405, 401.121, 401.265, 401.35 FS. Law Implemented 381.0011, 381.025, 395.401, 395.4015, 395.402, 395.4025, 395.403, 395.404, 395.4045, 395.405, 401.23, 401.24, 401.25, 401.26, 401.265, 401.27, 401.281, 401.30, 401.31, 401.321, 401.34, 401.35, 401.41, 401.411, 401.414, 401.421 FS. History-New 11-29-82, Amended 4-26-84, 3-11-85, Formerly 10D-66.50, Amended 4-12-88, 8-3-88, 8-7-89, 12-10-92, 11-30-93, 1-26-97. Formerly 10D-66.050. Amended 8-4-98, 1-3-99, 7-14-99, 2-20-00, 9-3-00, 4-15-01, 11-19-01, 6-3-02, 12-18-06.

EFFECTIVE 12-18-2006 Emergency Medical Services
10
64E-2.004 Medical Direction. (1) Each ALS, BLS or air ambulance provider shall maintain on file for inspection and copying by the department its current contract for a medical director by which it employs or independently contracts with a physician qualified pursuant to this section to be its medical director. (2) There is no standard format for a medical director's contract, however, in drafting such an instrument, the following provisions may be addressed: (a) Name and relationship of the contracting parties. (b) A list of contracted services inclusive of medical direction, administrative responsibilities, professional membership, basic and advanced life support review responsibilities, and reporting requirements. (c) Monetary consideration inclusive of fees, expenses, reimbursement, fringe benefits, clerical assistance and office space. (d) Termination clause. (e) Renewal clause. (f) Provision for liability coverage. (g) Effective dates of the contract. (3) Qualifications: (a) A medical director shall be a Florida licensed M.D. or D.O. (b) In addition to all other provisions applicable to medical directors in this rule, an air ambulance medical director shall be knowledgeable of the aeromedical requirements of patients and shall evaluate each patient in person or by written protocol prior to each interfacility transfer flight for the purpose of determining that the aircraft, flight and medical crew, and equipment meet the patient's needs. (c) A medical director shall be board certified and active in a broad-based clinical medical specialty with demonstrated experience in prehospital care and hold an ACLS certificate or equivalent as determined in Chapter 64E-2.032, F.A.C. Prehospital care experience shall be documented by the provider. (d) A medical director shall demonstrate and have available for review by the department documentation of active participation in a regional or statewide physician group involved in prehospital care. (4) Duties and Responsibilities of the Medical Director: (a) Develop medically correct standing orders or protocols which permit specified ALS and BLS procedures when communication cannot be established with a supervising physician or when any delay in patient care would potentially threaten the life or health of the patient. The medical director shall issue standing orders and protocols
to the provider to ensure that the provider transports each of its patients to facilities that offer a type and level of care appropriate to the patient's medical condition if available within the service region. The medical director or his appointee shall provide continuous 24-hour-per-day, 7-day-per-week medical direction which shall include in addition to the development of protocols and standing orders, direction to personnel of the provider as to availability of medical director "off-line" service to resolve problems, system conflicts, and provide services in an emergency as that term is defined by Section 252.34(3), F.S. (b) Develop and implement a patient care quality assurance system to assess the medical performance of paramedics and EMTs. The medical director shall audit the performance of system personnel by use of a quality assurance program to include but not limited to a prompt review of patient care records, direct observation, and comparison of performance standards for drugs, equipment, system protocols and procedures. The medical director shall be responsible for participating in quality assurance programs developed by the department. (c) With the exception of BLS medical directors each ALS or air ambulance service medical director shall possess proof of current registration as a medical director, either individually or through a hospital, with the U.S. Department of Justice, DEA, to provide controlled substances to an EMS provider. DEA registration shall include each address at which controlled substances are stored. Proof of such registration shall be maintained on file with each ALS or air ambulance provider and shall be readily available for inspection. (d) Ensure and certify that security procedures of the EMS provider for medications, fluids and controlled substances are in compliance with Chapters 499 and 893, F.S., and Chapter 64F-12, Florida Administrative Code. (e) Create, authorize and ensure adherence to, detailed written operating procedures regarding all aspects of the handling of medications, fluids and controlled substances by the provider. (f) Notify the department in writing of each substitution by the EMS provider of equipment or medication. (g) Assume direct responsibility for: the use by an EMT of an automatic or semi-automatic defibrillator; the performance of airway patency techniques including airway adjuncts, not to include endotracheal intubation, by an EMT; and on routine interfacility transports, the monitoring and maintenance of non-medicated I.V.s by an EMT. The medical director shall ensure that the EMT is trained to perform these procedures; shall establish written protocols for the performance of

EFFECTIVE 12-18-2006 Emergency Medical Services
11
these procedures; and shall provide written evidence to the department documenting compliance with provisions of this paragraph. (h) An EMT employed by a licensed ALS provider is authorized to start a non-medicated IV under the following conditions: 1. A non-medicated IV is initiated only in accordance with department approved protocols of the licensed ALS provider’s medical director. These protocols must include a requirement that the non-medicated IV be initiated in the presence of a Florida certified paramedic (of the same licensed provider) who directs the EMT to initiate the IV.
2. If the licensed ALS provider elects to utilize EMTs in this capacity, the licensed EMS provider shall ensure that the medical director provides training at least equivalent to that required by the 1999 U.S. D.O.T. EMT-Intermediate National Standard Curriculum relating to IV therapy which is incorporated by reference and available from the Superintendent of Documents, Post Office Box 371954, Pittsburgh, PA 15250-7954. The licensed EMS provider shall document successful completion of such training in each EMTs training file and make documentation available to the department upon request.
(i) Ensure that all EMTs and paramedics are trained in the use of the trauma scorecard methodologies as provided in Rule 64E-2.017, F.A.C., for adult trauma patients and Rule 64E-2.0175, F.A.C., for pediatric trauma patients. (j) Develop and revise when necessary TTPs for submission to the department for approval. (k) Participate in direct contact time with EMS field level providers for a minimum of 10 hours per year. Notwithstanding the number of EMS providers served by the medical director, direct contact time shall be a minimum of 10 hours per year per medical director, not per provider. (l) If he is a medical director of a training program: 1. Be responsible for the instruction of the Department of Transportation (DOT) approved training program for EMTs and paramedics. 2. Have substantial knowledge of the qualifications, training, protocols, and quality assurance programs for the training facility. 3. Maintain current instructor level training in Advanced Cardiac Life Support (ACLS), or equivalent, or Advanced Trauma Life Support (ATLS), maintain provider level training in International Trauma Life Support (ITLS) or Prehospital Trauma Life Support (PHTLS); and Advanced Pediatric Life Support (APLS), Pediatric Advanced Life Support (PALS) or Pediatric Education for Prehospital Professionals (PEPP).
4. Act as a liaison between training centers, local EMS providers and hospitals. 5. Participate in state and local quality assurance and data collections programs. 6. The EMS training center shall by contract, require such medical director to be available 4 hours per month for classroom teaching or review of student performance, and participate in direct contact time with EMS field level providers for a minimum of 10 hours per year. Notwithstanding the number of training center or EMS providers served by the medical director, direct contact time shall be a minimum of 10 hours per year per medical director, not per training center. 7. Participate in the recruitment, selection, and orientation of instructors and preceptors. 8. Participate in student selection, mid-term evaluation and final practical examination of students. (5) The medical director of a licensed EMS provider may authorize paramedics under his or her supervision to perform immunizations pursuant to a written agreement with a County Health Department in the county in which the immunizations are to be performed. Should the medical director elect to utilize paramedics in this capacity, he or she shall verify on DH Form 1256, Certification of Training, July 98, which is incorporated by reference and available from the department, that each paramedic authorized to administer immunizations has completed training consistent with that of other staff giving immunizations in the County Health Department as required by the Director of that County Health Department. Specific Authority 381.0011, 395.405, 401.265, 401.272, 401.35, 499.05 FS. Law Implemented 401.23, 401.24, 401.25, 401.26, 401.265, 401.27, 401.281, 401.2915, 401.30, 401.34, 401.35, 401.41, 401.411, 499.005 FS. History-New 8-7-89, Amended 6-6-90, 12-10-92, 3-19-95, 1-26-97. Formerly 10D-66.0505. Amended 08-04-98, 01-03-99, 02-20-00, 4-15-01, 11-19-01, 06-09-05, 10-24-05, 12-18-06. 64E-2.005 Air Ambulances. (1) Each applicant for an air ambulance license shall pay the required fee as specified in Section 401.34(1)(j), F.S., and submit an application to the department on DH Form 1575, October 05, Air Ambulance Service License Application which is incorporated by reference and available from the department. The air ambulance license shall automatically expire 2 years from the date of issuance.

EFFECTIVE 12-18-2006 Emergency Medical Services
12
(2) Each air ambulance applicant or provider, pursuant to subsection 64E-2.013(1), F.A.C., shall maintain on site and make available to the department at license application, license application renewal, change of insurance carrier or policy renewal, and documentation of the following minimum insurance coverage: (a) Each aircraft shall be insured for the sum of at least $100,000 for injuries to or death of any one person arising out of any one accident and the sum of at least $300,000 for injuries to or death of more than one person in any one accident. Any such policy on a leased aircraft must identify both the owner and the lessee of the aircraft. (b) In lieu of the insurance required in (2)(a), the provider or applicant may furnish a certificate of self-insurance establishing that the provider or applicant has a self-insurance plan to provide coverage identical to what is required in (2)(a) and that the plan has been approved by the Department of Insurance. (3) Each licensed air ambulance shall have emergency protocols which address at least, emergency procedures when the aircraft is overdue, when radio communications cannot be established, or when aircraft location cannot be verified. Each licensed rotary wing air ambulance shall document at least every 15 minutes of flight while en route to and from the patient's location. (4) Each provider shall maintain in each paramedic’s employment file documentation of successful completion of an initial air crew member (ACM) education program that was conducted in accordance with the 1988 United States (U.S.) Department of Transportation (DOT) Air Medical Crew-Advanced National Standard Curriculum (NSC), which is incorporated by reference and is available for purchase from AAMS; 526 King Street, Suite 415, Alexandria, VA 22314; 703-836-8732. Each provider shall ensure and shall document in its employee records that each EMT and paramedic which it employs holds a current certification from the department. (5) Each air ambulance provider shall establish a safety committee. The committee shall: (a) consist of a membership to include: one pilot, one flight medical crew member, the provider's medical director, one hospital administrator if the provider is a hospital based program, and a representative of a quality assurance division if one exists; (b) develop safety procedures for the provider; (c) meet at least quarterly to review safety policies, procedures, unusual occurrences, safety
issues, and audit compliance with safety policies and procedures; (d) communicate the results of the safety audit to all program personnel; and (e) record minutes of the meeting and retain them on file for 2 years. (6) Each prehospital air ambulance provider shall staff the aircraft with a minimum of one person who shall be a paramedic who meets the criteria in subsection 64E-2.005(4), F.A.C. (7) Every air ambulance maintained by an air ambulance provider shall meet the structural, equipment and supply requirements listed in Table III. (8) Each prehospital rotary wing air ambulance when available for call shall meet the structural requirements listed in Table IV, and shall be equipped as approved by the medical director of the service in the aircraft minimum equipment list. The aircraft minimum equipment list shall include, at a minimum, one each of the items listed in Table IV and shall be provided to the department upon request.

EFFECTIVE 12-18-2006 Emergency Medical Services
13
TABLE III
AIR AMBULANCE
Structural, Equipment and Supply Requirements
ITEM QTY.
Aircraft Requirements
1. Entrance large enough to allow loading of a patient.
2. Interior large enough for two medical crew members.
3. Cabin illumination of 40 foot-candles at patient level.
4. FAA approved stretcher system with 2 straps. 5. Isolated aircraft cockpit to protect
pilot from in-flight interference. 6. Each aircraft shall be equipped with
FAA approved communication equipment that operates on frequencies which allow the flight and medical crew to communicate with ground and landing zone medical support exclusive of the air traffic control system.
7. No smoking sign. 8. External search light with a minimum of 400,000
candle power illumination at 200 feet separate from the aircraft landing lights, movable 90 degrees longitudinally, 180 degrees laterally and capable of being controlled from inside the aircraft (Helicopter only).
Medical Equipment Requirements 1. Oxygen sufficient for duration of flight. 2. Oxygen administration equipment. 3. Oropharyngeal airways. Pediatric and adult. 4. Hand operated bag-valve mask resuscitators, adult and pediatric
accumulator, including adult, child and infant transparent masks capable of use with supplemental oxygen.
5. Equipment suitable to determine blood pressure of the adult and pediatric patient during flight.
6. Approved sharps container per Chapter 64E-16, F.A.C.
7. Approved biohazardous waste plastic bag or impervious container per
EFFECTIVE 12-18-2006 Emergency Medical Services
14
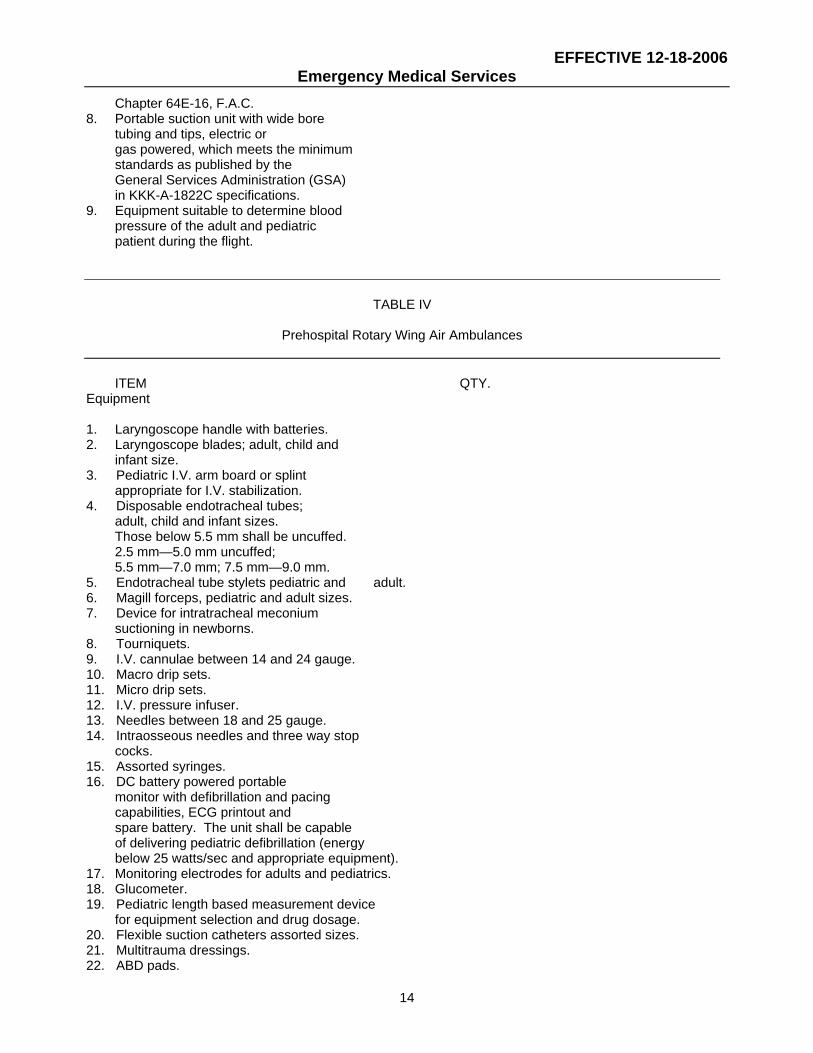
Chapter 64E-16, F.A.C. 8. Portable suction unit with wide bore
tubing and tips, electric or gas powered, which meets the minimum
standards as published by the General Services Administration (GSA) in KKK-A-1822C specifications.
9. Equipment suitable to determine blood pressure of the adult and pediatric patient during the flight.
TABLE IV
Prehospital Rotary Wing Air Ambulances
ITEM QTY. Equipment
1. Laryngoscope handle with batteries. 2. Laryngoscope blades; adult, child and
infant size. 3. Pediatric I.V. arm board or splint
appropriate for I.V. stabilization. 4. Disposable endotracheal tubes;
adult, child and infant sizes. Those below 5.5 mm shall be uncuffed. 2.5 mm—5.0 mm uncuffed; 5.5 mm—7.0 mm; 7.5 mm—9.0 mm.
5. Endotracheal tube stylets pediatric and adult. 6. Magill forceps, pediatric and adult sizes. 7. Device for intratracheal meconium
suctioning in newborns. 8. Tourniquets. 9. I.V. cannulae between 14 and 24 gauge. 10. Macro drip sets. 11. Micro drip sets. 12. I.V. pressure infuser. 13. Needles between 18 and 25 gauge. 14. Intraosseous needles and three way stop
cocks. 15. Assorted syringes. 16. DC battery powered portable
monitor with defibrillation and pacing capabilities, ECG printout and spare battery. The unit shall be capable of delivering pediatric defibrillation (energy below 25 watts/sec and appropriate equipment).
17. Monitoring electrodes for adults and pediatrics. 18. Glucometer. 19. Pediatric length based measurement device
for equipment selection and drug dosage. 20. Flexible suction catheters assorted sizes. 21. Multitrauma dressings. 22. ABD pads.

EFFECTIVE 12-18-2006 Emergency Medical Services
15
23. Sterile gauze pads. 24. Adhesive tape assorted sizes. 25. Patient restraints, wrist and ankle. 26. Soft roller bandages. 27. Bandage shears. 28. Sterile obstetrical kit to include,
at minimum, bulb syringe, sterile scissors or scalpel, and cord clamps or cord ties.
29. Burn sheets. 30. Flashlight with batteries. 31. Vaseline gauze. 32. Gloves—latex or other suitable
material for all crew members. 33. Face masks for all crew members. 34. Naso and oropharyngeal airways, assorted sizes. 35. Safety goggles or equivalent meeting
A.N.S.I. Z87.1 standard. 36. Bulb syringe separate from obstetrical kit. 37. Thermal, absorbent, reflective blanket. 38. Standing orders. 39. Electronic waveform capnography capable
of real-time monitoring and printing record of the intubated patient (effective 01/01/2008).
MEDICATION WT./VOL. 1. Atropine Sulfate. 2. Dextrose 50 percent. 3. Epinephrine HCL. 1:1,000 1 4. Epinephrine HCL. 1:10,000 5. Ventricular dysrhythmic. 6. Sodium Bicarbonate. 50 mEq. or 44.6. mEg. 7. Naloxone (Narcan). 1 mg./ml. 2 mg. amp. 8. Nitroglycerin. 0.4 mg 9. Benzodiazepine sedative/ anticonvulsant. 10. Inhalant beta adrenergic
agent of choice with nebulizer apparatus, as approved by the medical director.
I.V. Solutions 1. Lactated Ringers
or Normal Saline. Specific Authority 381.0011, 401.25, 401.251, 401.265, 401.35 FS. Law Implemented 381.0011, 395.405, 401.23, 401.24, 401.25, 401.251, 401.252, 401.26, 401.27, 401.30, 401.31, 401.321, 401.34, 401.35, 401.41, 401.411 401.414, 401.421 FS. History-New 11-29-82, Amended 4-26-84, 3-11-85, Formerly 10D-66.51, Amended 4-12-88, 8-3-88, 8-7-89, 12-10-92, 11-30-93, 10-2-94, 1-26-97. Formerly 10D-66.051. Amended 1-3-99, 9-3-00, 4-15-01, 12-18-06.

EFFECTIVE 12-18-2006 Emergency Medical Services
16
64E-2.006 Neonatal Interfacility Transfers. (1) Neonates requiring critical care interfacility transport to a Level II or Level III Neonatal Intensive Care Unit shall be transported in either a neonatal ambulance or a permitted ALS or BLS transport ambulance or aircraft. (a) A neonatal ambulance shall meet the requirements listed in Table V, paragraphs 64E-2.006(1)(c) and (d) and subsections 64E-2.006(2) and (3), F.A.C., and shall be exempt from meeting the equipment and medical supplies listed in Rule 64E-2.002, Table I, F.A.C., and in Rule 64E-2.003, Table II, F.A.C. (b) When a permitted BLS or ALS ambulance is used to transport a neonate, the sending neonatologist or physician and EMS provider's medical director shall ensure that the level of care, staffing, and equipment is commensurate to the needs of the neonate being transported. (c) The neonatal ambulance as defined in subsection 64E-2.001(13), F.A.C., shall have exterior wording or marking which identifies that the ambulance is only for neonatal transport. The wording shall be such that the public cannot mistake a neonatal vehicle as an ambulance for general patient care. (d) Any EMS provider operating a permitted neonatal ambulance for transporting neonates to a Level II or Level III Neonatal Intensive Care Unit shall contract with a neonatologist or have the hospital's staff neonatologist assigned as the provider's medical director.
EFFECTIVE 12-18-2006 Emergency Medical Services
17
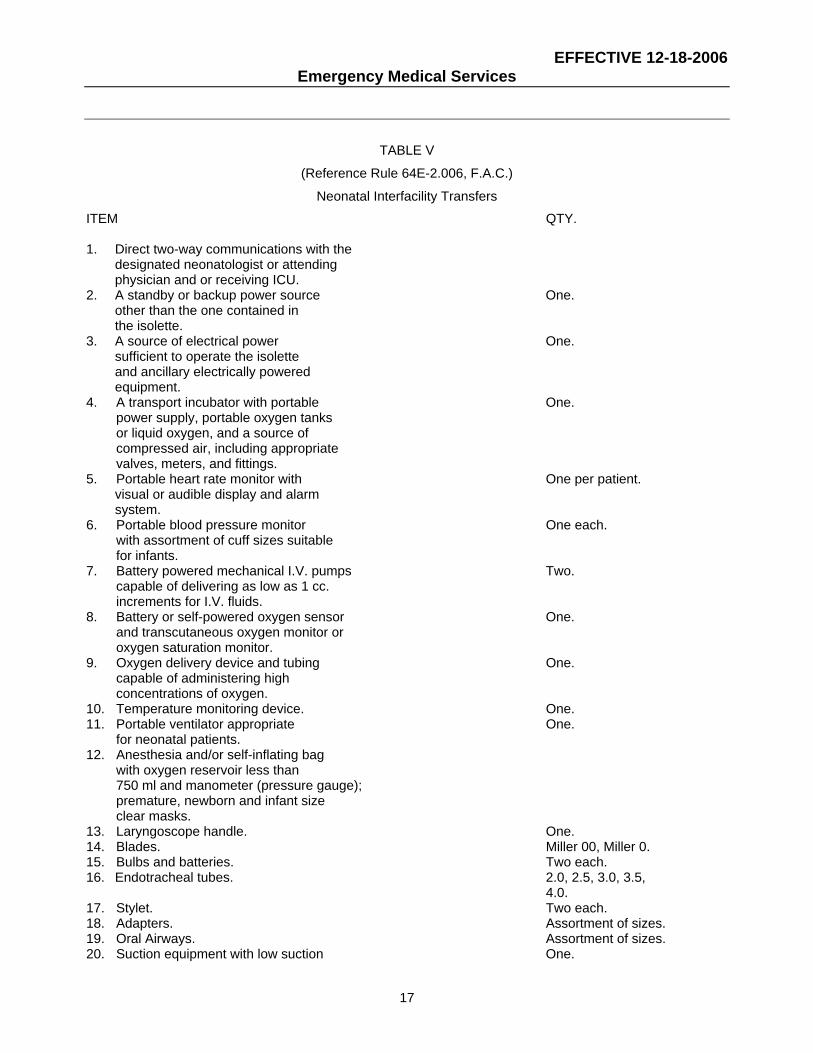
TABLE V
(Reference Rule 64E-2.006, F.A.C.)
Neonatal Interfacility Transfers
ITEM QTY. 1. Direct two-way communications with the designated neonatologist or attending physician and or receiving ICU. 2. A standby or backup power source One. other than the one contained in the isolette. 3. A source of electrical power One. sufficient to operate the isolette and ancillary electrically powered equipment. 4. A transport incubator with portable One. power supply, portable oxygen tanks or liquid oxygen, and a source of compressed air, including appropriate valves, meters, and fittings. 5. Portable heart rate monitor with One per patient. visual or audible display and alarm system. 6. Portable blood pressure monitor One each. with assortment of cuff sizes suitable for infants. 7. Battery powered mechanical I.V. pumps Two. capable of delivering as low as 1 cc. increments for I.V. fluids. 8. Battery or self-powered oxygen sensor One. and transcutaneous oxygen monitor or oxygen saturation monitor. 9. Oxygen delivery device and tubing One. capable of administering high concentrations of oxygen. 10. Temperature monitoring device. One. 11. Portable ventilator appropriate One. for neonatal patients. 12. Anesthesia and/or self-inflating bag with oxygen reservoir less than 750 ml and manometer (pressure gauge); premature, newborn and infant size clear masks. 13. Laryngoscope handle. One. 14. Blades. Miller 00, Miller 0. 15. Bulbs and batteries. Two each. 16. Endotracheal tubes. 2.0, 2.5, 3.0, 3.5, 4.0. 17. Stylet. Two each. 18. Adapters. Assortment of sizes. 19. Oral Airways. Assortment of sizes. 20. Suction equipment with low suction One.
EFFECTIVE 12-18-2006 Emergency Medical Services
18
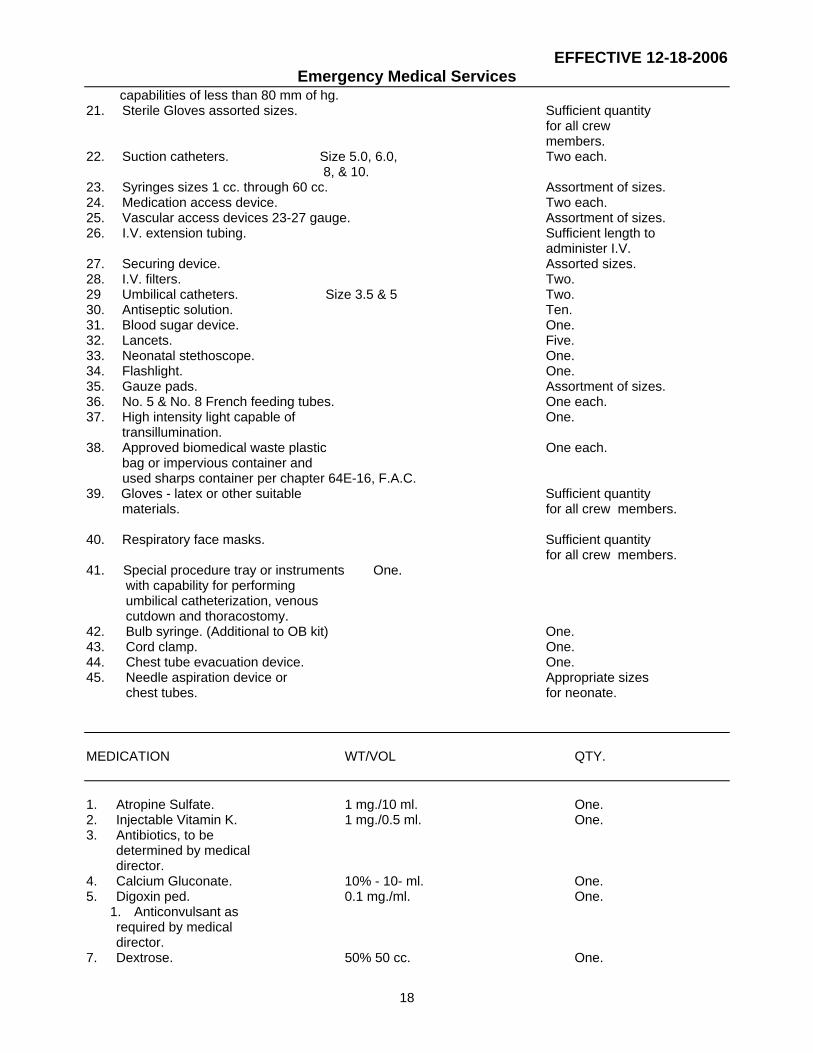
capabilities of less than 80 mm of hg. 21. Sterile Gloves assorted sizes. Sufficient quantity for all crew members. 22. Suction catheters. Size 5.0, 6.0, Two each. 8, & 10. 23. Syringes sizes 1 cc. through 60 cc. Assortment of sizes. 24. Medication access device. Two each. 25. Vascular access devices 23-27 gauge. Assortment of sizes. 26. I.V. extension tubing. Sufficient length to administer I.V. 27. Securing device. Assorted sizes. 28. I.V. filters. Two. 29 Umbilical catheters. Size 3.5 & 5 Two. 30. Antiseptic solution. Ten. 31. Blood sugar device. One. 32. Lancets. Five. 33. Neonatal stethoscope. One. 34. Flashlight. One. 35. Gauze pads. Assortment of sizes. 36. No. 5 & No. 8 French feeding tubes. One each. 37. High intensity light capable of One. transillumination. 38. Approved biomedical waste plastic One each. bag or impervious container and used sharps container per chapter 64E-16, F.A.C. 39. Gloves - latex or other suitable Sufficient quantity
materials. for all crew members.
40. Respiratory face masks. Sufficient quantity for all crew members.
41. Special procedure tray or instruments One. with capability for performing umbilical catheterization, venous cutdown and thoracostomy. 42. Bulb syringe. (Additional to OB kit) One. 43. Cord clamp. One. 44. Chest tube evacuation device. One. 45. Needle aspiration device or Appropriate sizes chest tubes. for neonate. MEDICATION WT/VOL QTY. 1. Atropine Sulfate. 1 mg./10 ml. One. 2. Injectable Vitamin K. 1 mg./0.5 ml. One. 3. Antibiotics, to be determined by medical director. 4. Calcium Gluconate. 10% - 10- ml. One. 5. Digoxin ped. 0.1 mg./ml. One.
1. Anticonvulsant as required by medical director. 7. Dextrose. 50% 50 cc. One.
EFFECTIVE 12-18-2006 Emergency Medical Services
19
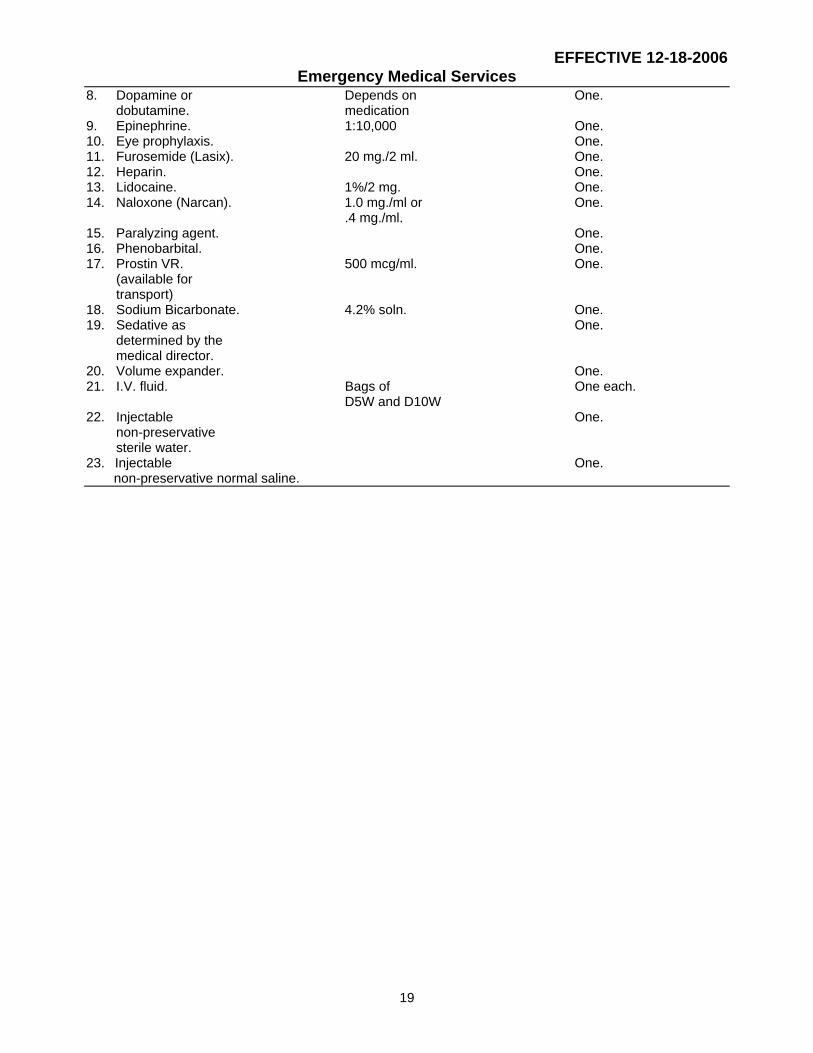
8. Dopamine or Depends on One. dobutamine. medication 9. Epinephrine. 1:10,000 One. 10. Eye prophylaxis. One. 11. Furosemide (Lasix). 20 mg./2 ml. One. 12. Heparin. One. 13. Lidocaine. 1%/2 mg. One. 14. Naloxone (Narcan). 1.0 mg./ml or One. .4 mg./ml. 15. Paralyzing agent. One. 16. Phenobarbital. One. 17. Prostin VR. 500 mcg/ml. One. (available for transport) 18. Sodium Bicarbonate. 4.2% soln. One. 19. Sedative as One. determined by the medical director. 20. Volume expander. One. 21. I.V. fluid. Bags of One each. D5W and D10W 22. Injectable One. non-preservative sterile water. 23. Injectable One. non-preservative normal saline.

EFFECTIVE 12-18-2006 Emergency Medical Services
20
(2) Each permitted ambulance or neonate ambulance when transporting a neonate to a Level II or Level III Neonatal Intensive Care Unit shall be staffed with a minimum of two persons. One person shall be a registered neonatal nurse, the second person shall be either a neonatal registered respiratory therapist (RT), or a paramedic or a registered neonatal nurse. The staffing for each neonate transport shall be determined by the licensee's medical director in conjunction with the attending physician and the neonatologist. A physician can be substituted for any team member. (a) The provider shall assure the RN is licensed in accordance with Chapter 464, F.S.; have a minimum of 4,000 hours RN experience, which includes 2,000 hours of Level II or Level III Neonatal Intensive Care Unit (NICU) nursing experience; and have American Heart Association (AHA) Neonatal Resuscitation Program (NRP) Certification or an equivalent certification and successfully complete a neonatal transport stabilization program within 2 years prior to application to neonatal transport, approved in writing by a medical director; and, accompany a minimum of six neonatal transports prior to staffing a neonatal transport as the only RN in attendance. (b) The provider shall assure the RT is registered by the National Board of Respiratory Care with a minimum of 2,000 hours of Level II or Level III NICU experience or be certified as a RT with a minimum of 3,000 hours of Level II or Level III NICU experience; and have AHA NRP Certification or an equivalent certification and successfully complete a neonatal transport stabilization program within 2 years prior to application to neonatal transport, approved in writing by a medical director; and, accompany a minimum of six neonatal transports prior to staffing a transport as the only RT in attendance. (c) The provider shall assure the paramedic is a Florida licensed paramedic with a minimum of 2,000 hours of Level II or Level III Neonatal Intensive Care unit experience; or be a Florida paramedic with a minimum of 3,000 hours experience; and have AHA NRP Certification or an equivalent certification and successfully complete a neonatal transport stabilization program within 2 years prior to application to neonatal transport, approved in writing by a medical director; and, accompany a minimum of six neonatal transports prior to staffing a neonatal transport. (d) A neonatologist or a licensee's medical director may make medical staff substitutions with individuals of comparable skills when the condition of the neonate warrants such substitution.
(3) Treatment protocols for the management of the neonatal patient from the responsible neonatologist shall accompany each neonatal transport. Specific Authority 381.0011, 383.19, 395.405, 401.251(6), 401.35 FS. Law Implemented 381.001, 383.15, 395.405, 401.24, 401.25, 401.251, 401.252, 401.26, 401.265, 401.27, 401.30, 401.31, 401.35, 401.41, 401.411, 401.414, 401.421 FS. History-New 11-30-93, Amended 1-26-97. Formerly 10D-66.0525. Amended 8-4-98, 9-3-00, 12-18-06. 64E-2.007 Vehicle Permits. (1) Each application for a ground vehicle permit shall be on DH Form 1510, May 98, Application for Vehicle Permit(s). Each application for an aircraft permit shall be on DH Form 1576, May 98, Application for Air Ambulance Permit. These forms are incorporated by reference and available from the department. All applications shall be accompanied by the required fee as specified in Section 401.34(1)(c),(k), F.S. (2) When it is necessary for a permitted vehicle to be out of service for routine maintenance or repairs, a substitute vehicle meeting the same transport capabilities and equipment specifications as the out-of-service vehicle may be used for a period of time not to exceed 30 days. If the substitute vehicle needs to be in service for longer than 30 days, the agency must seek written approval from the department. An unpermitted vehicle cannot be placed into service, nor can a BLS vehicle be used at the ALS level, unless it is replacing a vehicle that has been temporarily taken out of service for maintenance. When such a substitution is made, the following information shall be maintained by the provider and shall be accessible to the department: (a) Identification of permitted vehicle taken out of service. (b) Identification of substitute vehicle. (c) The date on which the substitute vehicle was placed into service and the date on which it was removed from service and the date on which the permitted vehicle was returned to service. (3) All transport vehicles permitted to licensed services must meet the vehicle design specifications, except for color schemes and insignias, as listed in United States General Services Administration (GSA)-KKK-1822, Federal Specifications for Ambulances as mandated by Section 401.35(1)(d), F.S.,

EFFECTIVE 12-18-2006 Emergency Medical Services
21
applicable to the year of the manufacture of the vehicle. (4) All licensed providers applying for an initial air ambulance aircraft permit after January 1, 2005, shall submit to the department a valid airworthiness certificate (unrestricted), issued by the Federal Aviation Administration, for each permitted aircraft, prior to issuance of the initial permit. Aircraft replacements are subject to the initial application process. Specific Authority 381.0011, 401.35 FS. Law Implemented 381.001, 381.0205, 401.23, 401.24, 401.25, 401.251, 401.26, 401.27, 401.30, 401.31, 401.34, 401.35, 401.41, 401.411, 401.414 FS. History-New 11-29-82, Amended 4-26-84, 3-11-85, Formerly 10D-66.53, Amended 4-12-88, 12-10-92, 11-30-93, 1-26-97. Formerly 10D-66.053. Amended 01-03-99, 12-18-06. 64E-2.008 Emergency Medical Technician.
(1) Qualifications and Procedures for Certification pursuant Section 401.27, F.S. - To be qualified for EMT certification, an individual must:
(a) 1. successfully complete an initial EMT training program conducted in accordance with the 1994 U.S. DOT EMT-Basic National Standard Curriculum, which is incorporated by reference and is available for purchase from the Government Printing Office by telephoning 202-512-1800 or writing to the Government Printing Office, Superintendent of Documents, Post Office Box 371954, Pittsburg, PA 15250-7954, or
2. if out of state or military trained in accordance with the 1994 U.S. DOT EMT-Basic National Standard Curriculum, currently hold a valid EMT certification from the National Registry of Emergency Medical Technicians or another U.S. state or territory which has the certifying authority to submit to the department DH Form 1164, April 05 Statement of Good Standing which is incorporated by reference and available from the department, as defined by section 64E-2.001(8), F.A.C.,
(b) apply for and pass Florida EMT certification examination on DH Form 1583, April 05, Emergency Medical Technicians Initial Certification Application which is incorporated by reference and available from the department, as defined by section 64E-2.001(8), F.A.C., and
(c) possess a high school diploma or a General Education Development (GED) diploma.
(2) Renewal Certification - To be eligible for renewal certification as an EMT an individual shall submit DH Form 622, April 05, EMT/Paramedic Renewal Certification Application, which is incorporated by reference and available from the
department; and within 2 years prior to the expiration date of his or her EMT certification complete one of the following:
(a) Complete 30 hours of EMT refresher training based on the 1996 U.S. DOT EMT-Basic National Standard Refresher Curriculum, an additional 2 hours of HIV AIDS refresher training, in accordance with Section 381.0034, F.S.; and maintain a current CPR card as provided in Section 401.27(4)(e)2., F.S., and Rule 64E-2.038, F.A.C. CPR shall be included in the 30 hours of refresher training, provided that the CPR training is taken with a continuing education provider recognized by the department pursuant to Section 401.2715, F.S. The 1996 U.S. DOT EMT-Basic National Standard Refresher Curriculum shall be the criteria for department approval of refresher training courses. The department shall accept either the affirmation of a licensed EMS provider’s medical director; or a certificate of completion of refresher training from a department approved Florida training program or a department approved continuing education provider as proof of compliance with the above requirements. The 1996 U.S. DOT EMT-Basic National Standard Refresher Curriculum is incorporated by reference and available for purchase from the Government Printing Office by telephoning 202-512-1800 or writing to the Government Printing Office, Superintendent of Documents, Post Office Box 371954, , PA 15250-7954.
(b) Successfully pass the EMT certification examination during the current certification cycle; and complete 2 hours of HIV AIDS refresher training, in accordance with Section 381.0034, F.S.; and maintain a current CPR BLS card for the professional rescuer. Prior to taking the examination, a candidate shall submit DH Form 1583, April 05, Emergency Medical Technicians Initial Certification Application to the department so as to be received by the department in accordance with the published examination application deadlines which may be obtained by contacting the department, as defined by section 64E-2.001(8), F.A.C., and pay the required fees.
(c) Satisfactorily complete the first semester of the paramedic training course at a department approved Florida training center pursuant to Section 401.2701, F.S. within the current 2-year certification cycle. Complete 2 hours of HIV AIDS refresher training in accordance with Section 381.0034, F.S., and also maintain a current CPR card for the professional rescuer.
(d) An individual must provide to the department, upon request, proof of compliance with the requirements in this section.
EFFECTIVE 12-18-2006 Emergency Medical Services
22
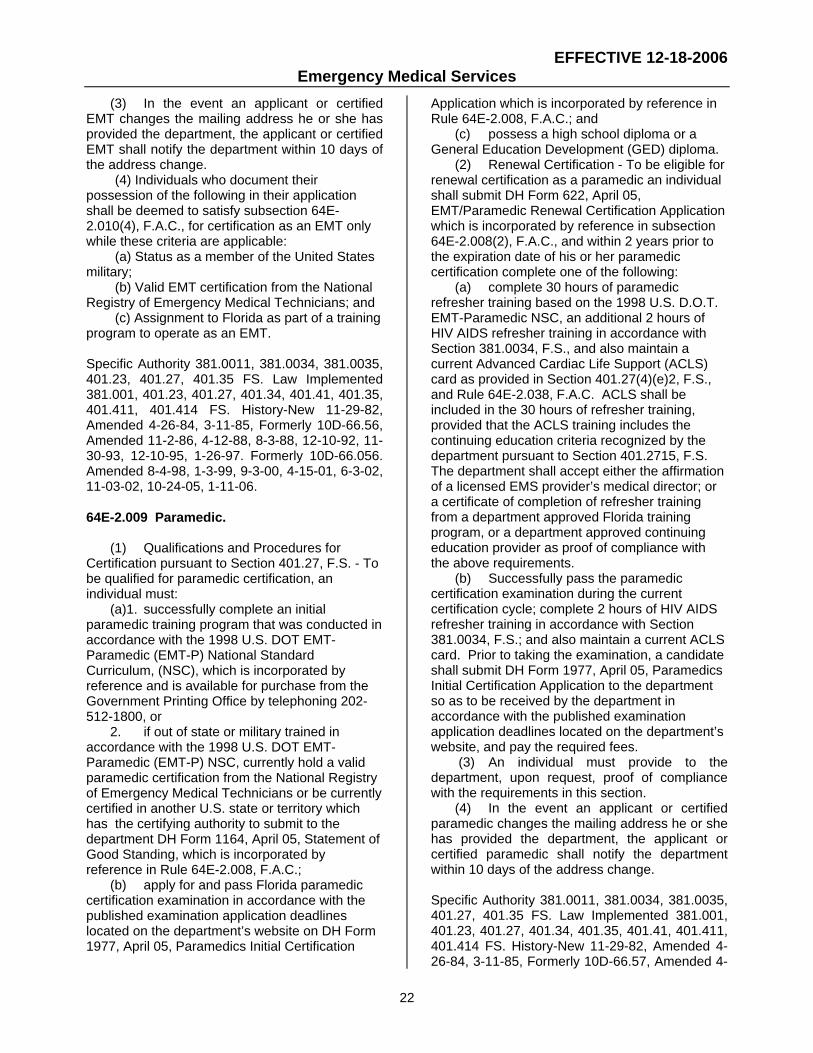
(3) In the event an applicant or certified EMT changes the mailing address he or she has provided the department, the applicant or certified EMT shall notify the department within 10 days of the address change.
(4) Individuals who document their possession of the following in their application shall be deemed to satisfy subsection 64E-2.010(4), F.A.C., for certification as an EMT only while these criteria are applicable:
(a) Status as a member of the United States military;
(b) Valid EMT certification from the National Registry of Emergency Medical Technicians; and
(c) Assignment to Florida as part of a training program to operate as an EMT. Specific Authority 381.0011, 381.0034, 381.0035, 401.23, 401.27, 401.35 FS. Law Implemented 381.001, 401.23, 401.27, 401.34, 401.41, 401.35, 401.411, 401.414 FS. History-New 11-29-82, Amended 4-26-84, 3-11-85, Formerly 10D-66.56, Amended 11-2-86, 4-12-88, 8-3-88, 12-10-92, 11-30-93, 12-10-95, 1-26-97. Formerly 10D-66.056. Amended 8-4-98, 1-3-99, 9-3-00, 4-15-01, 6-3-02, 11-03-02, 10-24-05, 1-11-06. 64E-2.009 Paramedic.
(1) Qualifications and Procedures for
Certification pursuant to Section 401.27, F.S. - To be qualified for paramedic certification, an individual must:
(a)1. successfully complete an initial paramedic training program that was conducted in accordance with the 1998 U.S. DOT EMT-Paramedic (EMT-P) National Standard Curriculum, (NSC), which is incorporated by reference and is available for purchase from the Government Printing Office by telephoning 202-512-1800, or
2. if out of state or military trained in accordance with the 1998 U.S. DOT EMT-Paramedic (EMT-P) NSC, currently hold a valid paramedic certification from the National Registry of Emergency Medical Technicians or be currently certified in another U.S. state or territory which has the certifying authority to submit to the department DH Form 1164, April 05, Statement of Good Standing, which is incorporated by reference in Rule 64E-2.008, F.A.C.;
(b) apply for and pass Florida paramedic certification examination in accordance with the published examination application deadlines located on the department’s website on DH Form 1977, April 05, Paramedics Initial Certification
Application which is incorporated by reference in Rule 64E-2.008, F.A.C.; and
(c) possess a high school diploma or a General Education Development (GED) diploma.
(2) Renewal Certification - To be eligible for renewal certification as a paramedic an individual shall submit DH Form 622, April 05, EMT/Paramedic Renewal Certification Application which is incorporated by reference in subsection 64E-2.008(2), F.A.C., and within 2 years prior to the expiration date of his or her paramedic certification complete one of the following:
(a) complete 30 hours of paramedic refresher training based on the 1998 U.S. D.O.T. EMT-Paramedic NSC, an additional 2 hours of HIV AIDS refresher training in accordance with Section 381.0034, F.S., and also maintain a current Advanced Cardiac Life Support (ACLS) card as provided in Section 401.27(4)(e)2, F.S., and Rule 64E-2.038, F.A.C. ACLS shall be included in the 30 hours of refresher training, provided that the ACLS training includes the continuing education criteria recognized by the department pursuant to Section 401.2715, F.S. The department shall accept either the affirmation of a licensed EMS provider’s medical director; or a certificate of completion of refresher training from a department approved Florida training program, or a department approved continuing education provider as proof of compliance with the above requirements.
(b) Successfully pass the paramedic certification examination during the current certification cycle; complete 2 hours of HIV AIDS refresher training in accordance with Section 381.0034, F.S.; and also maintain a current ACLS card. Prior to taking the examination, a candidate shall submit DH Form 1977, April 05, Paramedics Initial Certification Application to the department so as to be received by the department in accordance with the published examination application deadlines located on the department’s website, and pay the required fees.
(3) An individual must provide to the department, upon request, proof of compliance with the requirements in this section.
(4) In the event an applicant or certified paramedic changes the mailing address he or she has provided the department, the applicant or certified paramedic shall notify the department within 10 days of the address change.
Specific Authority 381.0011, 381.0034, 381.0035, 401.27, 401.35 FS. Law Implemented 381.001, 401.23, 401.27, 401.34, 401.35, 401.41, 401.411, 401.414 FS. History-New 11-29-82, Amended 4-26-84, 3-11-85, Formerly 10D-66.57, Amended 4-

EFFECTIVE 12-18-2006 Emergency Medical Services
23
12-88, 8-3-88, 12-10-92, 11-30-93, 12-10-95, 1-26-97. Formerly 10D-66.057. Amended 8-4-98, 1-3-99, 9-3-00, 4-15-01, 6-3-02, 11-03-02, 10-24-05. 64E-2.0094 Voluntary Inactive Certification. An EMT or paramedic who is currently certified can place their certificate on inactive status by sending a written request to the department and paying a fee of $50. Any EMT or paramedic whose certificate has been placed on inactive status shall not function as an EMT or paramedic until such time as he or she has completed the following requirements for reactivating the certificate: (1) A certificate holder whose certificate has been on inactive status for 12 months or less can activate his or her certificate by submitting a written request to the department for activation and receiving written approval. Pay a late renewal fee of $50. (a) For an EMT, send verification of having a current American Heart Association Basic Life Support Course or an American Red Cross Professional Rescuer CPR course completion certificate and meet the continuing education requirements identified in paragraph 64E-2.008(2)(a), F.A.C. (b) For a paramedic, send verification of a current American Heart Association Advanced Cardiac Life Support (ACLS) course completion certificate and meet the continuing education requirements identified in paragraph 64E-2.009(2)(a), F.A.C. (2) An EMT whose certificate has been on inactive status for more than 1 year can activate his or her certificate by completing the following: (a) 30 hours of EMT refresher training which shall be based on the 1996 U.S. DOT EMT-Basic National Standard Refresher Curriculum and 2 hours of human immunodeficiency virus and acquired immune deficiency syndrome (HIV AIDS) training. The 1996 U.S. DOT EMT-Basic National Standard Refresher Curriculum is incorporated by reference in Rule 64E-2.008, F.A.C. The training: 1. Shall have been completed after the EMT certificate was placed on inactive status and have been completed no more than 2 years prior to the date of receipt of the request for return to active status; and, 2. Shall have been completed at a department approved EMT training program or have been approved by the medical director of a licensed EMS provider. (b) Hold a current CPR card pursuant to Section 401.27(4)(e)1., and Rule 64E-2.038,
F.A.C., or equivalent pursuant to Rule 64E-2.038, F.A.C. (c) Complete a field internship. The internship shall be completed under the auspices of an EMS training program or a licensed ambulance service’s medical director. Upon completion of the field internship, the certificate holder must provide the department with a signed statement from the medical director attesting that the certificate holder completed a field internship program in which he or she demonstrated the ability to assume patient care responsibilities. (d) Pass the EMT certification examination. Should the applicant fail the examination, he or she must meet requirements for initial certification. (e) After completion of the above requirements, submit to the department: 1. DH Form 622, April 05, EMT/Paramedic Renewal Certification Application which is incorporated in subsection 64E-2.008(2), F.A.C. 2. DH Form 1583, April 05, Emergency Medical Technicians Initial Certification Application, which is incorporated by reference in Rule 64E-2.008, F.A.C. (3) A paramedic whose certificate has been on inactive status for more than 1 year can activate his or her certificate by completing the following: (a) 30 hours of paramedic refresher training which shall be based on the 1998 U.S. DOT EMT-Paramedic NSC, which is incorporated by reference in Rule 64E-2.009, F.A.C., and 2 hours of human immunodeficiency virus and acquired immune deficiency syndrome (HIV AIDS) training. The training: 1. Shall have been completed after the paramedic certificate was placed on inactive status and have been completed no more than 2 years prior to the date of receipt of the request for return to active status; and, 2. Shall have been completed at a department approved paramedic training program or have been approved by the medical director of a licensed EMS provider. (b) Hold a current ACLS card pursuant to Section 401.27(4)(e)2., F.S., and Rule 64E-2.038, F.A.C., or equivalent pursuant to Rule 64E-2.038, F.A.C. (c) Complete a field internship. The internship shall be completed under the auspices of an EMS training program or a licensed ambulance service’s medical director. Upon completion of the field internship, the certificate holder must provide the department with a signed statement from the medical director attesting that the certificate holder completed a field internship

EFFECTIVE 12-18-2006 Emergency Medical Services
24
program in which he or she demonstrated the ability to assume patient care responsibilities. (d) Pass the paramedic certification examination. Should the applicant fail the examination, he or she must meet the requirements for initial certification. (e) After completion of the above requirements, submit to the department: 1. DH Form 622, April 05, EMT/Paramedic Renewal Certification Application which is incorporated by reference in subsection 64E-2.008(2), F.A.C. 2. DH Form 1977, April 05, Paramedic Initial Certification Application which is incorporated by reference in Rule 64E-2.008, F.A.C. Specific Authority 401.27, 401.35 FS. Law Implemented 401.27, 401.34, 401.35 FS. New 8-4-98. Amended 1-3-99, 9-3-00, 4-21-02, 6-3-02. 11-3-02, 10-24-05. 64E-2.0095 Involuntary Inactive Certification. (1) An EMT or paramedic certificate that is not renewed at the end of the 2-year certification period shall automatically revert to an inactive status for a period of 180 days. (2) Such certificates may be reactivated if the applicant submits the renewal certification fee required by Section 401.34, F.S., and a late renewal fee of $25 and the following items to the department: (a) DH Form 622, April 05, EMT/Paramedic Renewal Certification Application, which is incorporated by reference in subsection 64E-2.008(2), F.A.C. (b) Verification of having met one of the recertification requirements contained in subsection 64E-2.008(2) or 64E-2.009(2), F.A.C. The requirements for recertification shall be completed before the end of the 180-day inactive certification period. (3) An application for recertification received by the department more than 180 days after the expiration date of the certificate shall be denied. Such certificate holder is ineligible for recertification and must meet the requirements for initial certification. Specific Authority 401.27, 401.35 FS. Law Implemented 401.27, 401.34, 401.35 FS. New 8-4-98. Amended 1-3-99, 9-3-00, 4-15-01, 10-24-05. 64E-2.010 Examinations.
(1) Grade Notification – The department shall notify each candidate of the examination results. If a candidate fails the certification examination developed or required by the department, he or she shall be notified by the department of, examination review, and appeal rights and procedures. (2) Examination Review. (a) A candidate who failed the examination shall notify the department, in writing, that he or she desires an examination review within 21days of the date indicated on the failure notice and include the required review fee of $50 payable by cashier’s check or money order to the department. Upon receipt of payment, the department shall notify the candidate of a review appointment. (b) Each candidate, who has taken and failed the examination, shall have the right to review the examination booklet and a copy of his or her answer sheet. (c) The candidate’s attorney can be present at the review. (d) Examination reviews shall be conducted in the presence of a representative of the department and scheduled at a location designated by the department. The review shall be conducted between 8:00 a.m. and 5:00 p.m., Monday through Friday, excluding official state holidays. A candidate shall attend only one review per examination administration. If the candidate is scheduled for an examination review date and fails to appear, the review fee shall be forfeited. (e) The candidate shall be allowed one-half the time allowed for the original administration of the examination to review the examination materials provided. Neither the candidate nor the attorney shall be allowed to bring any material for documenting or recording any test material into the review session. (f) A representative of the department shall remain with the candidate throughout the review process. The representative shall inform the candidate that the representative cannot defend the examination, attempt to answer or refute any question during the review. (g) The candidate shall be instructed that he or she is exercising his or her right of review. (h) Any candidate who fails the examination and attends an examination review, pursuant to this section, shall not be eligible for reexamination for at least 30 days after the examination review. (4) Examination Requirements: (a) Pursuant to paragraph 401.27(4)(d), F.S., the examination required for certification as an EMT is the National Registry Emergency
EFFECTIVE 12-18-2006 Emergency Medical Services
25
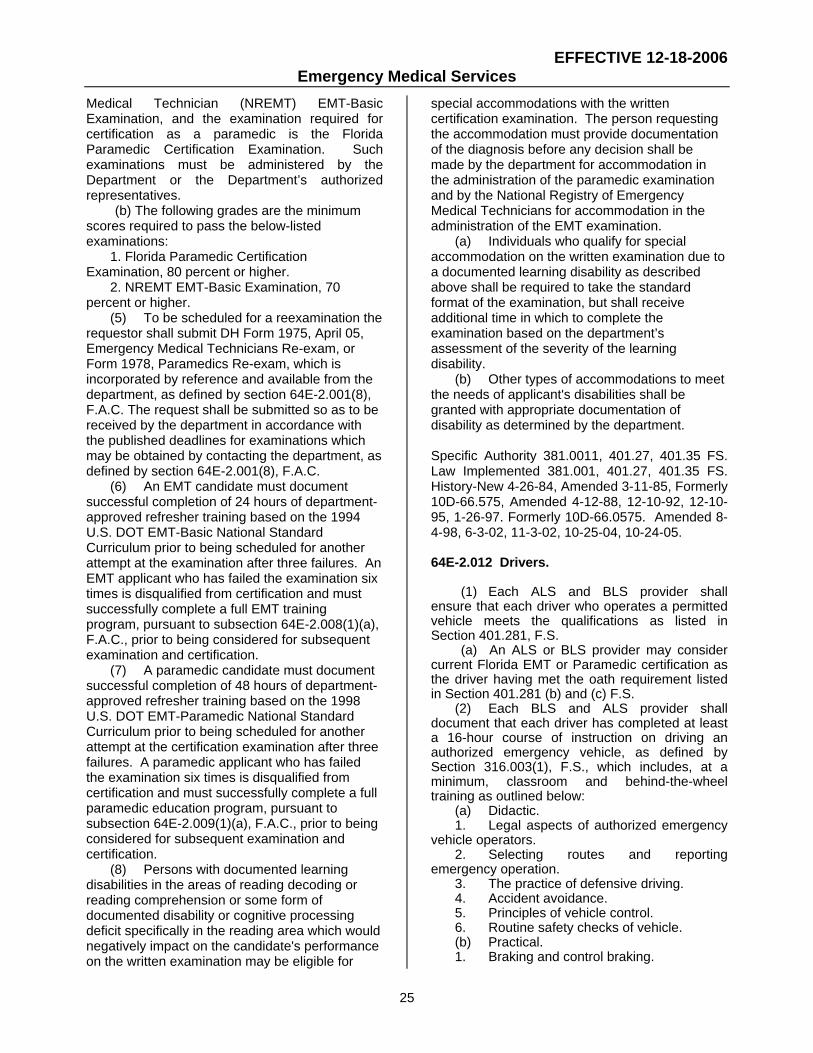
Medical Technician (NREMT) EMT-Basic Examination, and the examination required for certification as a paramedic is the Florida Paramedic Certification Examination. Such examinations must be administered by the Department or the Department’s authorized representatives. (b) The following grades are the minimum scores required to pass the below-listed examinations:
1. Florida Paramedic Certification Examination, 80 percent or higher.
2. NREMT EMT-Basic Examination, 70 percent or higher. (5) To be scheduled for a reexamination the requestor shall submit DH Form 1975, April 05, Emergency Medical Technicians Re-exam, or Form 1978, Paramedics Re-exam, which is incorporated by reference and available from the department, as defined by section 64E-2.001(8), F.A.C. The request shall be submitted so as to be received by the department in accordance with the published deadlines for examinations which may be obtained by contacting the department, as defined by section 64E-2.001(8), F.A.C. (6) An EMT candidate must document successful completion of 24 hours of department-approved refresher training based on the 1994 U.S. DOT EMT-Basic National Standard Curriculum prior to being scheduled for another attempt at the examination after three failures. An EMT applicant who has failed the examination six times is disqualified from certification and must successfully complete a full EMT training program, pursuant to subsection 64E-2.008(1)(a), F.A.C., prior to being considered for subsequent examination and certification. (7) A paramedic candidate must document successful completion of 48 hours of department-approved refresher training based on the 1998 U.S. DOT EMT-Paramedic National Standard Curriculum prior to being scheduled for another attempt at the certification examination after three failures. A paramedic applicant who has failed the examination six times is disqualified from certification and must successfully complete a full paramedic education program, pursuant to subsection 64E-2.009(1)(a), F.A.C., prior to being considered for subsequent examination and certification. (8) Persons with documented learning disabilities in the areas of reading decoding or reading comprehension or some form of documented disability or cognitive processing deficit specifically in the reading area which would negatively impact on the candidate's performance on the written examination may be eligible for
special accommodations with the written certification examination. The person requesting the accommodation must provide documentation of the diagnosis before any decision shall be made by the department for accommodation in the administration of the paramedic examination and by the National Registry of Emergency Medical Technicians for accommodation in the administration of the EMT examination. (a) Individuals who qualify for special accommodation on the written examination due to a documented learning disability as described above shall be required to take the standard format of the examination, but shall receive additional time in which to complete the examination based on the department’s assessment of the severity of the learning disability. (b) Other types of accommodations to meet the needs of applicant's disabilities shall be granted with appropriate documentation of disability as determined by the department. Specific Authority 381.0011, 401.27, 401.35 FS. Law Implemented 381.001, 401.27, 401.35 FS. History-New 4-26-84, Amended 3-11-85, Formerly 10D-66.575, Amended 4-12-88, 12-10-92, 12-10-95, 1-26-97. Formerly 10D-66.0575. Amended 8-4-98, 6-3-02, 11-3-02, 10-25-04, 10-24-05. 64E-2.012 Drivers. (1) Each ALS and BLS provider shall ensure that each driver who operates a permitted vehicle meets the qualifications as listed in Section 401.281, F.S. (a) An ALS or BLS provider may consider current Florida EMT or Paramedic certification as the driver having met the oath requirement listed in Section 401.281 (b) and (c) F.S. (2) Each BLS and ALS provider shall document that each driver has completed at least a 16-hour course of instruction on driving an authorized emergency vehicle, as defined by Section 316.003(1), F.S., which includes, at a minimum, classroom and behind-the-wheel training as outlined below: (a) Didactic. 1. Legal aspects of authorized emergency vehicle operators. 2. Selecting routes and reporting emergency operation. 3. The practice of defensive driving. 4. Accident avoidance. 5. Principles of vehicle control. 6. Routine safety checks of vehicle. (b) Practical. 1. Braking and control braking.

EFFECTIVE 12-18-2006 Emergency Medical Services
26
2. Backing; road position, fender judgement and steering technique. 3. Slalom; steering technique and chassis set. 4. Steering technique during a skid; a skid pad is optional. 5. Turn-around-steering technique; fender judgement, road position, controlled braking, controlled acceleration, understeer, oversteer and chassis set. Specific Authority 401.35 FS. Law Implemented 401.27, 401.281, 401.35, 401.411 FS. History-New 11-29-82, Amended 4-26-84, 3-11-85, Formerly 10D-66.59, Amended 4-12-88, 12-10-92. Formerly 10D-66.059, Amended 12-18-06. 64E-2.013 Records and Reports. (1) Each provider shall be responsible for supervising, preparing, filing and maintaining records and for submitting reports to the department as requested. All records shall be handled in such a manner as to ensure reasonable safety from water and fire damage and to be safeguarded from unauthorized use. Any records maintained by the provider as required by these rules shall be accessible to authorized representatives of the department and shall be retained for a period of at least 5 years except as otherwise specified in this rule. Each provider shall maintain the following administrative records: (a) Vehicle registration, copy of past department inspection reports, proof of current vehicle permit, and proof of current insurance coverage.
(b) Personnel records for each employee, to include date of employment, training records, employee application, documentation of current certification, and confirmation that each driver is in compliance with Section 401.281, F.S. (c) Copy of up-to-date department approved TTPs. (2) Each EMS provider shall ensure that an accurate and complete patient care record was prepared for each instance in which a patient was transported to a hospital. The transporting EMS provider shall have the complete and accurate patient care record as defined in subsection 64E-2.001(17), F.A.C., and required in Rule 64E-2.013, F.A.C., available upon request within 24 hours of the time the vehicle was originally dispatched in response to the request for emergency medical assistance.
(3) The accurate and complete patient care record shall include all known information listed
below and the known information defined under subsection 64E-2.001(17), F.A.C.:
(a) Date of call; (b) Time of call; (c) The service name; (d) Incident ID number; (e) Lead crew signature or
identification number; (f) Service name for any other licensed
service providing care; (g) Name for first responder agency; (h) The patient’s full name or unique
identification number if the name is unknown;
(i) The patient’s age; (j) Patient assessment information
(e.g., airway, breathing, circulation, pupils, skin and vitals) taken on scene and en route with times taken for vitals;
(k) The initial vitals taken by a non-transport service before the arrival of the transport unit;
(l) The patient’s medical history, current medications; allergies, and chief complaint;
(m) Interventions attempted (e.g., airway, breathing, circulation, and secondary interventions) and
(n) Medication(s) administered including the time, medication, dose and route.
(4) Non-transporting vehicle personnel shall
provide information pertinent to the patient's identification, patient assessment and care provided to the patient to the transporting vehicle personnel at the time the responsibility of the patient is transferred to the transporting service.
(5) Transporting vehicle personnel shall provide recorded information to the receiving hospital personnel at the time the patient is transferred that contains all known pertinent incident, patient identification and patient care information. (6) Each EMS provider shall maintain a copy of the patient care record as defined in subsection 64E-2.001(17), F.A.C., for a period of at least 5 years. This copy is considered to be the copy of record, shall contain an original signature by the lead crew member or an identification number assigned to the lead crew member and is certifiable as a true copy. (7) Each licensed EMS provider is responsible for quality review for completeness and accuracy of their own patient care records.

EFFECTIVE 12-18-2006 Emergency Medical Services
27
(8) Medication errors and reactions en route shall be reported to the physician who ordered the medication, the receiving physician, and the ALS medical director. (9) Each provider shall maintain a written plan, available for review by the department, for the proper handling, storage, and disposal of biohazardous wastes in accordance with Chapter 64E-16, F.A.C. (10) Each provider shall return his license to the department within 15 calendar days after a change of name or ownership of the service or upon permanently ceasing to provide service. (11) Each air ambulance provider shall maintain documentation describing the service rendered to the patient and cost as part of the patient's record in accordance with Section 401.251(4)(c), F.S. (12) A fixed wing air ambulance provider shall have an air medical crew member document the cabin altitude hourly. The cabin pressure shall be documented on the patient care record. (13) Each provider shall document and submit to the department, the information contained on DH Form 1304, May 02, “EMS Aggregate Prehospital Report and Provider Profile Information Form”, which is incorporated by reference and available from the department as defined and required in DHP 150-445, May 02, “Department of Health, Bureau of Emergency Medical Services (EMS) Instruction Manual for the: EMS Aggregate Pre-hospital and Provider Profile Information Form (DH 1304)”, which is incorporated by reference and available from the department. (a) Reports shall be submitted in accordance with the format and time frame specified in DHP 150-445. Reports received after the due date(s) specified in DHP 150-445 or not in the format specified in DHP 150-445, may not be included in reports published by the department. (b) The non-transporting unit is responsible for providing critical treatment and intervention information as defined in DHP 150-445 to the transporting unit at the time that the responsibility for the patient’s care is transferred to the transporting unit. The transporting unit is required to include counts of all known critical treatments and interventions that were administered or attempted to be administered to the patient prior to their arrival as defined and required in DHP 150-445 as part of their required quarterly submission of DH Form 1304 to the department. Specific Authority 381.0011, 395.405, 401.30, 401.35 FS. Law Implemented 381.001, 381.0205, 395.401-395.405, 401.23, 401.25, 401.27,
401.30, 401.35, 401.411 FS. History-New 11-29-82, Amended 4-26-84, 3-11-85, Formerly 10D-66.60, Amended 11-2-86, 4-12-88, 8-3-88, 12-10-92, 11-30-93, 12-10-95, 1-26-97. Formerly 10D-66.060. Amended 7-14-99, 2-20-00, 4-15-01, 11-3-02, 10-24-05. 64E-2.015 Prehospital Requirements for Trauma Care.
(1) Each EMS provider shall ensure that upon arrival at the location of an incident, an EMT or paramedic shall assess the condition of each adult trauma patient using the adult trauma scorecard methodology to determine the transport destination, as provided in Rule 64E-2.017, F.A.C., and the transport destination of each pediatric patient by using the pediatric trauma scorecard methodology included in Rule 64E-2.0175, F.A.C. (2) Each EMS provider shall transport, or cause to be transported, every trauma alert patient to a trauma center nearest to the location of the incident, unless the distance is not relevant to the length of time for transport due to the use of an air ambulance. Pediatric trauma alert patients shall be transported to the nearest trauma center with pediatric services even if a trauma center without pediatric services is nearer to the location of the incident, except as provided in department-approved TTPs. If a trauma center further from the location of the incident has a special resource(s) that the nearest trauma center does not have, such as burn center or hyper baric chamber, which is needed for the immediate condition of the trauma alert patient, the EMS provider may transport to the trauma center having that special resource(s) even if the trauma center is not nearest to the incident. These exceptions to transporting to the nearest trauma center, or other exceptions the EMS provider wishes to request, shall be addressed in the EMS provider's TTPs which shall be submitted to the department for approval, in accordance with Section 395.4045, F.S. and Rule 64E-2.016, F.A.C. (3) A trauma alert patient may be transported to a hospital other than a trauma center only if the hospital is closer to the scene of the incident, and the patient's immediate condition is such that the patient's life will be endangered if care is delayed by proceeding directly to the trauma center. If an EMS provider intends to transport trauma alert patients to hospitals other than trauma centers under any other circumstances, those circumstances must be described in and authorized by the EMS
EFFECTIVE 12-18-2006 Emergency Medical Services
28
provider's department-approved TTPs, as required in this section. (a) An EMS provider must transport a trauma alert patient to a trauma center, except as may be provided in the EMS provider's department-approved TTPs. For situations for which the EMS provider intends to transport a trauma alert patient to a hospital other than trauma center, as indicated in the provider's or trauma agency’s department-approved TTPs, the EMS provider or trauma agency shall ensure beforehand that the hospital meets the following criteria:
1. Is staffed 24-hours-per-day with a physician and other personnel who are qualified in emergency airway management, ventilatory support, and control of life threatening circulatory problems which shall include but not be limited to placement of endotracheal tubes; establishment of central intravenous lines; and insertion of chest tubes;
2. Has equipment and staff in-hospital and available to conduct chest and cervical spine x-rays; 3. Has laboratory facilities, equipment and staff in-hospital and available to analyze and report laboratory results;
4. Has equipment and staff on call and available to initiate definitive care required by a trauma alert patient within 30 minutes of the patient's arrival at the hospital, or can initiate procedures within 30 minutes of the patients arrival to transfer the trauma alert patient to a trauma center; and
5. Has a written transfer agreement with at least one trauma center. The transfer agreement shall provide specific procedures to ensure the timely transfer of the trauma alert patient to the trauma center. (b) Any exceptions to this requirement shall be included in the EMS provider's TTPs and be approved by the department. (c) Prior to submitting an application for an ALS, BLS or air ambulance license, or to renew such a license, each EMS provider shall request in writing, from the chief executive officer of each hospital (excluding trauma centers) to which the EMS provider intends to transport trauma alert patient's, written documentation that verifies that the hospital meets the requirements provided in paragraph (3)(a) of this section. When submitting TTPs for department approval, EMS providers shall include copies of each letter sent to the chief executive officer of such hospital as well as the response, if any, from the chief executive officer indicating whether the hospital complies with paragraph (3)(a) of this section.
(d) A trauma agency that has developed uniform TTPs may request written documentation from the hospitals in lieu of each EMS provider, in accordance with the requirements of this section. (e) If an EMS provider does not receive a response from a hospital, or if the hospital indicates that it is not in compliance with the criteria in paragraph (3)(a) of this section, the EMS provider shall not deliver a trauma alert patient to that hospital. Any exception must also be included in the EMS provider's department-approved TTPs. (f) If a hospital's compliance with the criteria in paragraph (3)(a) of this section changes during the EMS provider's biennial licensure period, the EMS provider shall submit, within 30 days of becoming cognizant of the change, revised TTPs to the department for approval, in accordance with Rule 64E-2.016, F.A.C. (g) If a hospital to which an EMS provider transports trauma alert patients, as provided in the EMS provider's or trauma agency department-approved TTPs, becomes a trauma center, including those granted provisional status by the department, the EMS provider shall begin immediately transporting trauma alert patients to that trauma center. The EMS provider or trauma agency shall revise and submit TTPs to the department for approval within 30 days of the hospital becoming a trauma center. Within 30 days of an EMS provider or a trauma agency receiving notification that a trauma center intends to discontinue as a trauma center, the EMS provider or trauma agency shall submit revised TTPs to the department for approval, in accordance with Rule 64E-2.016, F.A.C. (4) ALS non-transporting vehicle personnel shall provide to the transporting vehicle personnel complete information about the patient's identity, the initial patient assessment and care provided prior to arrival of the transporting vehicle personnel, at the time that responsibility for the patient is transferred. (5) The EMS provider responsible for the patient shall ensure that a prehospital trauma alert is issued upon determining that a trauma patient meets the requirements of Rules 64E-2.017, and 64E-2.0175, F.A.C. The words "trauma alert" shall be used when notifying the trauma center, or hospital that EMS is en route with a trauma alert patient. The medical director of the EMS provider issuing the trauma alert, or the physician at the receiving trauma center, or hospital, are the only people authorized to change the trauma alert status. The EMS provider issuing the trauma alert shall also provide the trauma center or hospital with information required under subsection 64E-2.013(5), F.A.C., and the information listed below at the time the patient is transferred to the

EFFECTIVE 12-18-2006 Emergency Medical Services
29
personnel of the receiving trauma center or hospital:
(a) Time of injury if different from the time of the call;
(b) Date of injury if different from day of call;
(c) County of injury; (d) County of residence of patient; (e) Cause of injury; (f) Injury site/type; (g) Trauma alert criteria if met as
defined in Rule 64E-2.017 or 64E-2.0175, F.A.C., and
(h) Protective devices if motor vehicle crash, bicycle or marine crash.
The information listed above shall be documented on the patient care record of the transporting unit that delivered the patient in accordance with the requirements of Rule 64E-2.013, F.A.C. (6) Each EMS provider or trauma agency shall submit to the department TTPs for approval as required by the Trauma Transport Protocols Manual, December 2004, which is incorporated by reference and available from the department. Specific Authority 395.4045, 395.405, 401.35 FS. Law Implemented 395.401-395.403, 395.404-395.405, 395.4045, 401.30, 401.35 FS. History-New 8-3-88, Amended 12-10-92, 11-30-93. Formerly 10D-66.100. Amended 8-4-98, 07-14-99, 2-20-00, 11-3-02, 11-24-02, 06-09-05. 64E-2.016 Trauma Transport Protocols Approval and Denial Process. (1) TTPs shall be approved by the EMS provider's or trauma agency’s medical director prior to submission to the department for approval and in accordance with the Trauma Transport Protocols Manual, December 2004, which is incorporated in Rule 64E-2.015, F.A.C. Specific Authority 395.405, 401.35 FS. Law Implemented 395.4045, 395.4045, 401.30, 401.35 FS. History-New 8-3-88, Amended 12-10-92. Formerly 10D-66.101. Amended 11-24-02, 06-09-05. 64E-2.017 Adult Trauma Scorecard Methodology. (1) Each EMS provider shall ensure that upon arrival at the location of an incident, an EMT or paramedic shall: (a) Assess the condition of each adult trauma patient using the adult trauma scorecard methodology, as provided in this section to
determine whether the patient should be a trauma alert. (b) In assessing the condition of each adult trauma patient, the EMT or paramedic shall evaluate the patient’s status for each of the following components: airway, circulation, best motor response (a component of the Glasgow Coma Scale which is defined and incorporated by reference in subsection 64E-2.001(10), F.A.C.), cutaneous, longbone fracture, patient’s age, and mechanism of injury. The patient’s age and mechanism of injury shall only be assessment factors when used in conjunction with assessment criteria included in (3) of this section. (2) The EMT or paramedic shall assess all adult trauma patients using the following criteria in the order presented and if any one of the following conditions are identified, the patient shall be considered a trauma alert patient: a. Airway: The patient receives active airway assistance beyond the administration of oxygen. b. Circulation: The patient lacks a radial pulse with a sustained heart rate greater than 120 beats per minute or has a blood pressure of less than 90 mmHg. c. Best Motor Response (BMR): The patient exhibits a score of four or less on the motor assessment component of the Glasgow Coma Scale, or exhibits the presence of paralysis or there is the suspicion of a spinal cord injury or the loss of sensation. d. Cutaneous: The patient has 2nd or 3rd degree burns to 15 percent or more of the total body surface area, or amputation proximal to the wrist or ankle, or any penetrating injury to the head, neck, or torso (excluding superficial wounds where the depth of the wound can be determined). e. Longbone Fracture: The patient reveals signs or symptoms of two or more long bone fracture sites (humerus, (radius, ulna), femur, (tibia or fibula)). (3) Should the patient not be identified as a trauma alert using the criteria listed in (2) of this section, the trauma patient shall be further assessed using the criteria in (3) of this section and shall be considered a trauma alert patient when a condition is identified from any two of the seven components included in this section. a. Airway: The patient has a respiratory rate of 30 or greater. b. Circulation: The patient has a sustained heart rate of 120 beats per minute or greater. c. BMR: The patient has a BMR of 5 on the motor component of the Glasgow Coma Scale.
EFFECTIVE 12-18-2006 Emergency Medical Services
30
d. Cutaneous: The patient has a soft tissue loss from either a major degloving injury, or a major flap avulsion greater than 5 inches, or has sustained a gun shot wound to the extremities of the body. e. Longbone Fracture: The patient reveals signs or symptoms of a single longbone fracture resulting from a motor vehicle collision or a fall from an elevation of 10 feet or greater. f. Age: The patient is 55 years of age or older. g. Mechanism of Injury: The patient has been ejected from a motor vehicle (excluding any motorcycle, moped, all terrain vehicle, bicycle or the open body of a pick-up truck), or the driver of the motor vehicle has impacted with the steering wheel causing steering wheel deformity. (4) If the patient is not identified as a trauma alert patient after evaluating the patient using the criteria in (2) and (3) of this section, the trauma patient will be evaluated using all elements of the Glasgow Coma Scale. If the patient’s score is 12 or less, the patient shall be considered a trauma alert patient (excluding patients whose normal Glasgow Coma Scale Score is 12 or less, as established by the patient’s medical history or preexisting medical condition when known). (5) Where additional local trauma alert criteria has been approved by the medical director of the EMS service and presented as part of the state TTP approval process, the use of local trauma alert criteria as the basis for calling a trauma alert shall be documented in the patient care record in accordance with the requirements of Rule 64E-2.013, F.A.C. Local trauma assessment criteria can only be applied after the patient has been assessed as provided in (2), (3), and (4) of this section. (6) In the event that none of the conditions are identified using the criteria in (2), (3), (4), or (5) of this section in the assessment of the adult trauma patient, the EMT or paramedic can call a trauma alert if, in his or her judgment, the patient's condition warrants such action. Where EMT or paramedic judgment is used as the basis for calling a trauma alert, it shall be documented in the patient care record in accordance with the requirements of Rule 64E-2.013, F.A.C. (7) The results of the patient assessment shall be recorded and reported in the patient care record in accordance with the requirements of Rule 64E-2.013, F.A.C. Specific Authority 395.4045, 395.405, 401.35 FS. Law Implemented 395.401, 395.4015, 395.402, 395.4025, 395.4045, 395.405, 401.30, 401.35 FS.
History-New 8-3-88, Amended 12-10-92, 11-30-93. Formerly 10D-66.102. Amended 11-4-99, 2-20-00. 64E-2.0175 Pediatric Trauma Scorecard Methodology. (1) Each EMS provider shall ensure that upon arrival at the location of an incident, the EMT or paramedic shall assess the pediatric trauma patient by evaluating the patient’s status for each of the following components: Airway, Consciousness, Circulation, Fracture, Cutaneous and the pediatric patient’s size when used in conjunction with the other components in (3) of this section. The assessment of the pediatric patient using the weight and length parameter and the other components of this section shall be referred to as the Pediatric Trauma Scorecard Methodology. In assessing the pediatric patient, the criteria for each of the components in (2) and (3) of this section shall be used to determine the transport destination for pediatric trauma patients. (2) The EMT or paramedic shall assess all pediatric trauma patients using the following criteria and if any of the following conditions are identified, the patient shall be considered a pediatric trauma alert patient: (a) Airway: In order to maintain optimal ventilation, the patient is intubated, or the patient's breathing is maintained through such measures as manual jaw thrust, continuous suctioning or through the use of other adjuncts to assist ventilatory efforts. (b) Consciousness: The patient exhibits an altered mental status that includes: drowsiness, lethargy, the inability to follow commands, unresponsiveness to voice, totally unresponsive, or is in a coma or there is the presence of paralysis; or the suspicion of a spinal cord injury; or loss of sensation. (c) Circulation: The patient has a faint or nonpalpable carotid or femoral pulse or the patient has a systolic blood pressure of less than 50 mmHg. (d) Fracture: There is evidence of an open long bone (humerus, (radius, ulna), femur, (tibia or fibula)) fracture or there are multiple fracture sites or multiple dislocations (except for isolated wrist or ankle fractures or dislocations). (e) Cutaneous: The patient has a major soft tissue disruption, including major degloving injury, or major flap avulsions or 2nd or 3rd degree burns to 10 percent or more of the total body surface area, or amputation at or above the wrist or ankle, or any penetrating injury to the head, neck or torso (excluding superficial wounds

EFFECTIVE 12-18-2006 Emergency Medical Services
31
where the depth of the wound can be determined). (3) In addition to the criteria listed in (2) of this section, a trauma alert shall be called when a condition is identified from any two of the components included in (3) of this section. (a) Consciousness: The patient exhibits symptoms of amnesia, or there is loss of consciousness. (b) Circulation: The carotid or femoral pulse is palpable, but the radial or pedal pulses are not palpable or the systolic blood pressure is less than 90 mmHg. (c) Fracture: The patient reveals signs or symptoms of a single closed long bone fracture. Long bone fractures do not include isolated wrist or ankle fractures. (d) Size: Pediatric trauma patients weighing 11 kilograms or less, or the body length is equivalent to this weight on a pediatric length and weight emergency tape (the equivalent of 33 inches in measurement or less). (4) In the event that none of the criteria in (2) or (3) of this section are identified in the assessment of the pediatric patient, the EMT or paramedic can call a "Trauma Alert" if, in his or her judgment, the trauma patient's condition warrants such action. Where EMT or paramedic judgment is used as the basis for calling a trauma alert, it shall be documented in the patient care record in accordance wth Rule 64E-2.013, F.A.C. Specific Authority 395.4045, 395.405, 401.35 FS. Law Implemented 395.401, 395.4015, 395.402, 395.4025, 395.4045, 395.405, 401.30, 401.35 FS. History-New 8-4-98. Amended 2-20-00, 9-3-00. 64E-2.018 Trauma Registry. Instructions for completing and submitting data are defined in the Florida Trauma Registry Manual, December 2005, which is incorporated by reference and available from the department, as defined by section 64E-2.001(8), F.A.C. Specific Authority 395.405, 401.35 FS. Law Implemented 395.3025(4)(f), 395.401, 395.4015, 395.402, 395.4025, 395.404, 395.4045, 395.405, 401.30, 401.35 FS. History-New 8-3-88, Amended 12-10-92, 11-30-93. Formerly 10D-66.013. Amended 07-14-99, 11-19-01, 6-3-02, 06-09-05, 04-25-06. 64E-2.019 Trauma Agency Formation Requirements. (1) To form a trauma agency, and for submission of the trauma agency 5 year plan update, a county or counties (if regional), or an
entity with which the county or counties contract for the purpose of trauma service administration shall: (a) Obtain formal authority to create the agency from the county commission of each of the counties in which the agency plans to operate. (b) Establish interlocal agreements between county governments if the proposed agency shall provide service to more than one county. (c) Hold a public hearing and give adequate notice of the hearing to the public in the county or counties in which the proposed trauma agency shall operate. Adequate notice shall consist of publishing the notice, at least 30 days prior to the public hearing, in at least one newspaper of general circulation in each affected county. If a newspaper is not published in a county in which a proposed trauma agency shall operate, adequate notice may be given by publishing the notice in at least one newspaper of general circulation in adjoining affected counties. (d) Develop and submit an original and four copies of the trauma agency plan to the department for review and approval. (2) The trauma agency plan shall contain the following information in the following order: (a) Table of Contents; (b) Population and Geographic Area to be Served. 1. Describe the population and defined geographic area to be served by the trauma agency; 2. Include a map showing the defined geographic area of the proposed trauma agency, each major geographical barrier, all medical facilities, all prehospital ground and air facilities, and all other significant factors that affect the determination of the geographic area boundaries; and 3. Describe the historical patient flow, patient referral, and transfer patterns used to define the geographic areas of the proposed trauma agency. (c) Organizational Structure: 1. Provide a detailed description of the managerial and administrative structure of the proposed agency; 2. Include a table of organization, the names of the board of directors and each member's affiliation, and identify the individuals who will administer or operate the trauma agency, if known; 3. Provide the names, job descriptions and responsibilities of officials who shall be directly responsible for trauma agency personnel, and the names, job descriptions and responsibilities of individuals who shall be responsible for managing and operating the trauma agency on a daily basis; and
EFFECTIVE 12-18-2006 Emergency Medical Services
32
4. Describe in detail the specific authority that trauma agency personnel shall have in directing the operation of prehospital and hospital entities within the purview of the trauma agency, if approved, be it a single or multi-county trauma agency. (d) Trauma System Structure: 1. Describe the operational functions of the system; the components of the system; the integration of the components and operational functions; and the coordination and integration of the activities and responsibilities of trauma centers, hospitals, and prehospital EMS providers; and 2. Include a list of all participating and non-participating trauma care resources within the defined geographical area of the proposed trauma agency and documentation showing that these entities have been given the opportunity to participate in the system. Trauma care resources shall include, but are not limited to, hospitals, trauma centers, prehospital providers, training centers, and planning entities; and 3. Include the proposed trauma agency's recommendation and justification for the number and location of trauma centers required to serve its defined geographical area. (e) Objectives, Proposed Actions, and Implementation Schedule. Provide a description of the objectives of the plan, a detailed list of the proposed actions necessary to accomplish each objective, and a timetable for the implementation of the objectives and action. The timetable shall identify the scheduling of the annual audit and evaluation, including the completion date and submission date to the department. (f) Describe the proposed source of income and anticipated expenses by category for the proposed trauma agency; (g) Describe the proposed trauma agency's fiscal impact on the trauma system which includes a description of any increased costs related to providing trauma care. (h) Transportation System Design: 1. Describe the EMS ground, water, and air transportation system design of the trauma system; and 2. Include trauma patient flow patterns, emergency inter-hospital transfer agreements, and the number, type, and level of service of prehospital EMS providers within the trauma system. (i) TTPs: 1. Provide confirmation that existing department-approved TTPs for each EMS provider, within the defined geographical area of the proposed trauma agency, are accurate and shall be adopted by the proposed trauma agency, pending department approval of the plan;
2. A proposed trauma agency may develop uniform TTPs for department approval that shall be adhered to by all EMS providers that serve the geographic area of the proposed trauma agency. If uniform TTPs are submitted to the department for approval, the TTPs shall include the name of each EMS provider that shall operate according to the uniform TTPs, and proof of consultation with each EMS provider's medical director. TTPs developed and submitted by a proposed trauma agency shall be processed in accordance with Rule 64E-2.016, F.A.C.; and 3. The proposed trauma agency shall provide a copy of any county ordinance governing the transport of trauma patients within the defined geographic area of the proposed trauma agency. (j) Medical Control and Accountability. Identify and describe the qualifications, responsibilities and authority of individuals and institutions providing off-line (system) medical direction and on-line (direct) medical control of all hospitals and prehospital EMS providers operating under the purview of the trauma agency. (k) Emergency Medical Communications: 1. Describe the EMS communication system within the proposed trauma agency's trauma service area; and 2. Describe the proposed trauma agency's compliance with the State of Florida Communications Plan, requirements for normal operating conditions, mass casualty and disaster situations in which commercial power, telephone lines or telephone services are not available, including outages of base stations controlled by leased telephone lines. The specific areas to be addressed are: a. Statewide medical coordination (SMC); b. Local medical coordination (LMC); c. Vehicle dispatch and response (VDR); d. Medical resource coordination; e. Local scene coordination; f. Medical alert paging; g. Communications coverage; h. LMC and VDR channels; i. SMC channel; j. Cellular phone use if applicable; and k. Locations and types of communications equipment within the proposed trauma agency's geographical area. (l) Data Collection. Describe the trauma data management system developed for the purpose of documenting and evaluating the trauma systems operation. (m) Trauma System Evaluation. Describe the methodology by which the proposed trauma agency shall evaluate the trauma system. (n) Mass Casualty and Disaster Plan Coordination. Describe the proposed trauma agency's coordination of the prehospital and
EFFECTIVE 12-18-2006 Emergency Medical Services
33
hospital component's mass casualty and disaster plan for the defined geographic area it represents. (o) Public Information and Education. Describe the proposed trauma agency's programs designed to increase public awareness of the trauma system and public education programs designed to prevent, reduce the incidence of, and care for traumatic injuries within the defined geographic area it represents. (p) Attachments. Include the following: 1. A copy of each contract and agreement entered into by the proposed trauma agency, pending department approval of the proposed trauma agency, for the benefit and operation of the trauma system; and 2. A copy of the public hearing notice and minutes of the hearing. Specific Authority 395.401, 395.405, 401.35 FS. Law Implemented 395.401, 395.4015, 395.402, 395.4025, 395.405, 401.35 FS. History-New 8-3-88, Amended 12-10-92. Formerly 10D-66.104. Amended 11-24-02, 06-09-05. 64E-2.020 Trauma Agency Plan Approval and Denial Process. (1) The department shall, within 30 days of receipt of the formation of a trauma agency and the trauma agency 5 year plan update, review the proposed trauma agency's trauma system plan and notify the proposed trauma agency that the plan is complete, or that there are omissions. If there are omissions, the department shall request the required additional information to be submitted by the proposed trauma agency. (2) The existing or proposed trauma agency shall submit the requested additional information to the department within 30 days of receipt of the notice of omissions. (3) The department shall deem the plan complete upon receipt of the additional information or the expiration of the 30-day time period, whichever occurs first. (4) The department shall review the plan to determine compliance with Chapters 395 and 401, F.S., and Chapters 59A-3 and 64E-2, F.A.C., within 60 days of receipt of the additional information or of the plan being deemed complete. (5) The department shall issue a letter of approval to the existing or proposed trauma agency upon determination that the plan is in compliance with Chapters 395 and 401, .F.S., and Chapters 59A-3 and 64E-2, F.A.C. (6) The department shall issue a letter of denial to the existing or proposed trauma agency upon determination that the plan is not in compliance with Chapters 395 and 401, F.S., and Chapters 59A-3 and 64E-2, F.A.C. The letter
shall specify the deficiencies in the plan and include notification of any right to a hearing pursuant to Section 120.57, F.S. Specific Authority 395.401, 395.405, 401.35 FS. Law Implemented 395.401, 395.4015, 395.402, 95.4025, 395.405,401.35 FS. History-New 8-3-88, Amended 12-10-92. Formerly 10D-66.106. Amended 11-24-02. 64E-2.021 Trauma Agency Implementation and Operation Requirements. (1) To implement a trauma system, a department-approved trauma agency shall: (a) Implement the trauma system in accordance with its department-approved planned timetable for implementation. (b) Submit proposed changes to the department-approved plan to the department for approval, as provided in Rule 64E-2.020, F.A.C. The trauma agency may, at its own risk, institute proposed changes to the plan and submit a request for department approval within 30 days after a change is instituted if a delay in approval would have an adverse impact on the current level of care. The trauma agency's request shall explain how the delay in approval would have adversely affected the current level of care. Each request shall document that affected trauma care resources within the defined geographical area of the agency concur with these proposed changes. (2) Each trauma agency shall operate the trauma system in accordance with the department-approved plan, and shall: (a) Conduct reviews of trauma center applications from any hospital within the defined geographic area of the trauma agency. Submission of a trauma center’s application to the trauma agency by a hospital seeking approval shall be in accordance with the time frames described in paragraph 64E-2.024(1)(c), F.A.C. Results of the trauma agency's review shall be submitted to the department no later than April 7 of each year, in order to be considered by the department. (b) Conduct annual performance evaluations of the trauma system and submit the results to the department for approval, as provided in Rule 64E-2.020, F.A.C. The evaluation report shall be submitted by March 1 following the end of the previous calendar year. This evaluation shall include at least the following: 1. Results of monitoring each EMS provider, trauma center and hospital within the defined geographic area of the trauma agency for compliance with trauma scorecard methodology requirements as provided in Rules 64E-2.017, and 64E-2.0175, F.A.C.

EFFECTIVE 12-18-2006 Emergency Medical Services
34
2. Results of monitoring each EMS provider, trauma center and hospital within the defined geographic area of the trauma agency for compliance with TTP requirements as provided in Rule 64E-2.015, F.A.C. 3. Collection of data on both prehospital and hospital patient care data, as defined by the trauma agency plan. 4. Documentation of the continuum of care and quality of medical care for all trauma patients from injury through rehabilitation or death. 5. Documentation that all trauma centers in the geographic area of the trauma agency participate in quality improvement process. 6. Results of monitoring for compliance with trauma registry reporting requirements.
(3) Each trauma agency shall have personnel or arrange for management service personnel with clear authority and responsibility to operate the trauma agency. The administrative function of the trauma agency shall not be carried out or performed under the direct supervision of any individual who administers or operates any health care entity in the trauma system, whether a single or multi-county system. Specific Authority 395.405, 401.35 FS. Law Implemented 395.401, 395.4015, 395.402, 395.4025, 395.405, 401.35 FS. History-New 12-10-92. Formerly 10D-66.1065. Amended 8-4-98, 11-19-01, 11-24-02, 06-09-05.
64E-2.022 Apportionment of Trauma Centers within a Trauma Service Area (TSA). (1) The number and composition of TSAs shall be in accordance with Section 395.402, F.S. (2) The number of trauma centers in each TSA shall be in accordance with the maximum number set forth in the table below. Each trauma service area shall have at least one Level I or Level II trauma center position. (3) The number of trauma center positions for each TSA is as follows: TSA Counties Trauma Centers 1 Escambia; Okaloosa; Santa Rosa; Walton 2 2 Bay; Gulf; Holmes; Washington 1 3 Calhoun; Franklin; Gadsden; Jackson; Jefferson; Leon; Liberty; Madison; Taylor; Wakulla 1 4 Alachua; Bradford; Columbia; Dixie; Gilchrist; Hamilton; Lafayette; Levy; Putnam; Suwannee; Union 2 5 Baker; Clay; Duval; Nassau; St. Johns 2 6 Citrus; Hernando; Marion 1 7 Flagler; Volusia 2 8 Lake; Orange; Osceola; Seminole; Sumter 3 9 Pasco; Pinellas 3 10 Hillsborough 2 11 Hardee; Highlands; Polk 3 12 Brevard; Indian River 2 13 DeSoto; Manatee; Sarasota 3 14 Martin; Okeechobee; St. Lucie 1 15 Charlotte; Glades; Hendry; Lee 2 16 Palm Beach 2 17 Collier 1 18 Broward 3 19 Dade; Monroe 6 TOTAL 42

EFFECTIVE 12-18-2006 Emergency Medical Services
35
(4) The trauma center will be assigned by the department according to section 395.402(4), F.S. Specific Authority 395.405 FS. Law Implemented 395.401, 395.4015, 395.402, 395.405 FS. History-New 12-10-92. Formerly 10D-66.1075. Amended 06-09-05, 12-18-06. 64E-2.023 Trauma Centers Requirements. (1) The standards for Level I and Level II trauma centers, are published in DH Pamphlet (DHP) 150-9, December 2004, which is incorporated by reference and available from the department. Trauma Centers must be in full compliance with these standards by July 1, 2000. (2) To be a Level I trauma center, a hospital shall be a state licensed general hospital and shall:
(a) Meet and maintain after receiving provisional status and during the 7 year approval period the standards for a Level I trauma center as provided in DHP 150-9, December 2004;
(b) Meet the site visit requirements described in Rule 64E-2.028, F.A.C.;
(c) Meet and maintain after receiving provisional status and during the 7 year approval period the requirements provided in Rule 64E-2.018, F.A.C., regarding the collecting and reporting of trauma registry data; and (d) Maintain and update at least annually an in-hospital copy of the application that was approved by the department as described in Rule 64E-2.024, F.A.C., so that the application reflects current and accurate information. Documentation used by the trauma center to update the application, but maintained elsewhere between annual application updates shall be immediately available for department review at any time. The application shall be maintained and updated after receiving provisional status and during the 7 year approval period, and organized in the same manner as was required at the time of application. (3) To be a Level II trauma center, a hospital shall: (a) Meet and maintain after receiving provisional status and during the 7 year approval period the standards for a Level II trauma center as provided in DHP 150-9, December 2004; (b) Meet the site visit requirements described in Rule 64E-2.028, F.A.C.; (c) Meet and maintain after receiving provisional status and during the 7 year approval period the requirements provided in Rule 64E-2.018, F.A.C., regarding the collecting and reporting of trauma registry data; and (d) Maintain and update at least annually an in-hospital copy of the application that was approved by the department as described in Rule 64E-2.024, F.A.C., so that the application reflects
current and accurate information. The application shall be maintained and updated after receiving provisional status and during the 7 year approval period, and organized in the same manner as was required at the time of application. (4) To be a pediatric trauma center, a hospital shall:
(a) Meet and maintain after receiving provisional status and during the 7 year approval period the standards for a pediatric trauma center as provided in DHP 150-9, December 2004;
(b) Meet the site visit requirements described in Rule 64E-2.028, F.A.C.;
(c) Meet and maintain after receiving provisional status and during the 7 year approval period the requirements provided in Rule 64E-2.018, F.A.C., regarding the collecting and reporting of trauma registry data; and
(d) Maintain and update at least annually an in-hospital copy of the application that was approved by the department as described in Rule 64E-2.024, F.A.C., so that the application reflects current and accurate information. Documentation used by the trauma center to update the application, but maintained elsewhere between annual application updates shall be immediately available for department review at any time. The application shall be maintained and updated after receiving provisional status and during the 7 year approval period, and organized in the same manner as was required at the time of application. (5) The standards published in DHP 150-9, December 2004, are subject to revision at any time through rule promulgation. Any hospital that has been granted Provisional trauma center status or has been granted a 7 year Certificate of Approval as a trauma center shall comply with all revisions to the standards published in DHP 150-9, beginning on the date the amended rule becomes effective. Specific Authority 395.405 FS. Law Implemented 395.401, 395.4015, 395.402, 395.4025, 395.404, 395.4045, 395.405 FS. History-New 8-3-88, Amended 12-10-92, 12-10-95. Formerly 10D-66.108. Amended 8-4-98, 2-20-00, 6-3-02, 06-09-05. 64E-2.024 Process for the Approval of Trauma Centers. (1) Beginning September 1, 1990, and annually thereafter, the department shall approve trauma centers in accordance with the schedule shown in Table VII; (Unless stated otherwise all dates given by calendar month and day refer to that date each year.) (a) The department shall accept a letter of intent, DH Form 1840, December 2004, "Trauma Center Letter of Intent", which is incorporated by
EFFECTIVE 12-18-2006 Emergency Medical Services
36
reference and available from the department, postmarked no earlier than September 1 and no later than midnight, October 1, from any acute care general or pediatric hospital. The letter of intent is non-binding, but preserves the hospital's right to submit an application by the required due date if an available position, as provided in Rule 64E-2.022, F.A.C., exists in the hospital's TSA. If the hospital does not submit an application by April 1 of the following year, the hospital's letter of intent is void; (b) By October 15, the department shall send to those hospitals submitting a letter of intent an application package which will include, as a minimum, instructions for submitting information to the department for selection as a trauma center, DHP 150-9, December 2004, Trauma Center Standards, which is incorporated by reference in Rule 64E-2.023, F.A.C., and the requested application(s); (c) No later than April 1 of the calendar year following the submission of a letter of intent, a hospital seeking approval as a trauma center shall submit to the department an original and 3 copies of the respective application as indicated below. Each hospital in a TSA with a department-approved local or regional trauma agency shall, at the time a trauma center application is submitted to the department, submit a duplicate of the application to the trauma agency for review. Recommendations from the trauma agency shall be submitted to the department no later than April 7, as provided in Rule 64E-2.021, F.A.C. 1. To apply for approval as a Level I Trauma Center, applicants must submit all forms contained in the Level I Trauma Center Application Manual, December 2004. The manual and the forms contained therein are incorporated by reference and available from the department. The manual contains the following forms: DH Form 2032, December 2004, General Information for Level I Trauma Center Application; DH Form 2032-A, December 2004, Level I Trauma Center Approval Standards Summary Chart; DH Form 2032-B, December 2004, Application for Level I Trauma Center Approval Letter of Certification; DH Form 2032-C, December 2004, Level I Trauma Center Surgical Specialties Certifications; DH Form 2032-D, December 2004, Level I Trauma Center Non-Surgical Specialties Certifications; DH Form 2032-E, December 2004, Level I Trauma Center General Surgeons Commitment Statement; DH Form 2032-F, December 2004, Level I Trauma Center General Surgeons Available for Trauma Surgical Call; DH Form 2032-G, December 2004, Level I Trauma Center Neurosurgeons Available for Trauma Surgical Call; DH Form 2032-H, December 2004, Level I Trauma Center Neurological, Pediatric Trauma and Neurological,
and Neuroradiology Statements; DH Form 2032-I, December 2004, Level I Trauma Center Surgical Specialists On Call and Promptly Available; DH Form 2032-J, December 2004, Level I Trauma Center Emergency Department Physicians; DH Form 2032-K, December 2004, Level I Trauma Center Anesthesiologists Available for Trauma Call; DH Form 2032-L, December 2004, Level I Trauma Center C.R.N.A.s Available for Trauma Call; and DH Form 2032-M, December 2004, Level I Trauma Center Non-Surgical Specialists On Call and Promptly Available. 2. To apply for approval as a Level II Trauma Center, applicants must submit all forms contained in the Level II Trauma Center Application Manual, December 2004. The manual and the forms contained therein are incorporated by reference and available from the department. The manual contains the following forms: DH Form 2043, December 2004, General Information for Level II Trauma Center Application; DH Form 2043-A, December 2004, Level II Trauma Center Approval Standards Summary Chart; DH Form 2043-B, December 2004, Application for Level II Trauma Center Approval Letter of Certification; DH Form 2043-C, December 2004, Level II Trauma Center Surgical Specialties Certifications; DH Form 2043-D, December 2004, Level II Trauma Center Non-Surgical Specialties Certifications; DH Form 2043-E, December 2004, Level II Trauma Center General Surgeons Commitment Statement; DH Form 2043-F, December 2004, Level II Trauma Center General Surgeons Available for Trauma Surgical Call; DH Form 2043-G, December 2004, Level II Trauma Center Neurosurgeons Available for Trauma Surgical Call; DH Form 2043-H, December 2004, Level II Trauma Center Neurological, Pediatric Trauma and Neurological, and Neuroradiology Statements; DH Form 2043-I, December 2004, Level II Trauma Center Surgical Specialists On Call and Promptly Available; DH Form 2043-J, December 2004, Level II Trauma Center Emergency Department Physicians; DH Form 2043-K, December 2004, Level II Trauma Center Anesthesiologists Available for Trauma Call; DH Form 2043-L, December 2004, Level II Trauma Center C.R.N.A.s Available for Trauma Call; and DH Form 2043-M, December 2004, Level II Trauma Center Non-Surgical Specialists On Call and Promptly Available. 3. To apply for approval as a Pediatric Trauma Center, applicants must submit all forms contained in the Pediatric Trauma Center Application Manual, December 2004. The manual and the forms contained therein are incorporated by reference and available from the department. The manual contains the following forms: DH Form 1721, December 2004, General Information
EFFECTIVE 12-18-2006 Emergency Medical Services
37
for Pediatric Trauma Center Application; DH Form 1721-A, December 2004, Pediatric Trauma Center Approval Standards Summary Chart; DH Form 1721-B, December 2004, Application for Pediatric Trauma Center Letter of Certification; DH Form 1721-C, December 2004, Pediatric Trauma Center Surgical Specialties Certifications; DH Form 1721-D, December 2004, Pediatric Trauma Center Non-Surgical Specialties Certifications; DH Form 1721-E, December 2004, Pediatric Trauma Center General Surgeons Commitment Statement; DH Form 1721-F, December 2004, Pediatric Trauma Center General Surgeons Available for Trauma Surgical Call; DH Form 1721-G, December 2004, Pediatric Trauma Center Neurosurgeons Available for Trauma Surgical Call; DH Form 1721-H, December 2004, Pediatric Trauma Center Neurological, Pediatric Trauma and Neurological, and Neuroradiology Statements; DH Form 1721-I, December 2004, Pediatric Trauma Center Surgical Specialists On Call and Promptly Available; DH Form 1721-J, December 2004, Pediatric Trauma Center Emergency Department Physicians; DH Form 1721-K, December 2004, Pediatric Trauma Center Anesthesiologists Available for Trauma Call; DH Form 1721-L, December 2004, Pediatric Trauma Center C.R.N.A.s Available for Trauma Call; and DH Form 1721-M, December 2004, Pediatric Trauma Center Non-Surgical Specialists On Call and Promptly Available. (d) After considering the results of the local or regional trauma agency's recommendations, the department shall, by April 15, conduct a provisional review to determine completeness of the application and the hospital's compliance with the standards of critical elements for provisional status. The standards of critical elements for provisional review for Level I and Level II trauma center applications are specified in DHP 150-9, December 2004, as follows: Level I
STANDARD I. Administrative: A, E, and F; II. Trauma Service: A, B.1, 5, 6, and 9, C,
and D; III. Surgical Services: A, B, C, and D; IV. Non-Surgical Services: A, B, and C; V. Emergency Department: A, B, C.1, D,
and E.4, VI. Operating Room and Post-Anesthesia
Recovery Area: A.1, 2, and 3 and B.1 and 2; VII. Intensive Care Unit and Pediatric
Intensive Care Unit: B, C, D, and E; VIII. Training and Continuing Education
Programs: A, B, and C; IX. Equipment: A, B, C, D, and E;
X. Laboratory Services: A and B; XII. Radiological Services: A, B, and C; XIII. Organized Burn Care: A; XIV. Acute Spinal Cord and Brain Injury
Management Capability: A; XV. Acute Rehabilitative Services: B; XVI. Psychosocial Support Services: A; XVII. Outreach Programs: B, C, and E; XVIII. Quality Management: A through H; XIX. Trauma Research: B;.
Level II STANDARD I. Administrative: A, E, and F; II. Trauma Service: A, B.1, 5, and 6, C, and
D; III. Surgical Services: A, B, C, and D; IV. Non-Surgical Services: A, B, and C; V. Emergency Department: A, B, C.1, D,
and E.4; VI. Operating Room and Post-Anesthesia
Recovery Area: A.1, 2, and 3 and B.1 and 2; VII. Intensive Care Unit: A, B, C, and D; VIII. Training and Continuing Education
Programs: A, B, and C; IX. Equipment: A, B, C, D, and E; X. Laboratory Services: A and B; XII. Radiological Services: A, B, and C; XIII. Organized Burn Care: A; XIV. Acute Spinal Cord and Brain Injury
Management Capability: A; XV. Acute Rehabilitative Services: B; XVI. Psychosocial Support Services: A; XVII. Outreach Programs: B, C, and E; XVIII. Quality Management: A through H;
Pediatric
STANDARD I. Administrative: A, E, and F; II. Trauma Service: A, B.1, 5, 6, and 9, C,
and D; III. Surgical Services: A, B, C, and D; IV. Non-Surgical Services: A, B, and C; V. Emergency Department: A, B, C.1, D,
and E.4; VI. Operating Room and Post-Anesthesia
Recovery Area: A.1, 2, and 3 and B.1 and 2; VII. Pediatric Intensive Care Unit: A, B, C,
and D; VIII. Training and Continuing Education
Programs: A, B, and C; IX. Equipment: A, B, C, D, and E; X. Laboratory Services: A and B; XII. Radiological Services: A, B, and C; XIII. Organized Burn Care: A; XIV. Acute Spinal Cord and Brain Injury
Management Capability: A; XV. Acute Rehabilitative Services: B;
EFFECTIVE 12-18-2006 Emergency Medical Services
38
XVI. Psychosocial Support Services: A; XVII. Outreach Programs: B, C, and E; XVIII. Quality Management: A through H;
(e) No later than April 15, each hospital whose application the department finds to be unacceptable or deficient during the department's provisional review, will be notified in writing of deficiencies and given the opportunity to submit additional clarifying or corrective information. (f) The hospital shall submit the requested information to the department by close of business 5 working days after April 15. Failure to provide the requested information, or failure to successfully address the deficiencies identified by the department, shall result in the denial of the hospital's application. (g) The department shall send written notification to each applicant on or before May 1: 1. The department shall notify each hospital whose application it has found acceptable upon completion of the provisional review that the hospital shall operate as a Provisional trauma center beginning May 1; 2. The department shall inform each hospital whose provisional application it has denied of the remaining deficiencies in the application and shall inform the hospital that it may submit a letter of intent at the beginning of the next approval cycle. (h) The department shall, between May 1 and June 30, complete an in-depth review of all sections of the Provisional trauma center’s application. The department shall notify the hospital of any omissions, deficiencies, or problems and request additional information to be submitted by the hospital. (i) To have additional information considered during the department's in-depth review of the application, the Provisional trauma center shall submit the requested additional information to the department no later than September 1. (j) By September 30, the department shall determine whether the omissions, deficiencies, or problems have been corrected. The department shall notify each Provisional trauma center on or before October 1 of any omissions, deficiencies, or problems that were not resolved by submission of the requested additional information. (k) Provisional trauma centers are subject to a site visit from October 1 to May 30. Any Provisional trauma center that was notified by the department on or before October 1 at the conclusion of the in-depth review that omissions, deficiencies, or problems were not resolved shall be given 30 calendar days from the department's notification following the completion of the site visit to provide additional information, as discussed in Rule 64E-2.028, F.A.C. (l) The department shall deny the application of any Provisional trauma center that has not
corrected the omissions, deficiencies, or problems noted from the in-depth review within 30 calendar days from the department's notification following the completion of the site visit, as provided in Rule 64E-2.028, F.A.C., regardless of the findings of the out-of-state review team regarding the quality of trauma patient care and trauma patient management provided by the Provisional trauma center. (m) By July 1, the department shall approve or deny trauma centers based upon the recommendations of the out-of-state review team, the result of the in-depth review and, if necessary, upon application of the additional criteria in subsection 64E-2.028(10), F.A.C.: 1. The department shall issue the certificate to the hospital upon approval as a trauma center; 2. The department shall issue a letter of denial to each hospital not approved as a trauma center, specifying the basis for denial and informing the hospital of the next available approval cycle, and the hospital's right to an administrative hearing pursuant to Sections 120.57 and 395.4025, F.S. (2) Each hospital denied provisional status or not approved as a trauma center, may, within 30 days of receipt of the denial notice, request a hearing in which to contest the findings of the department. (3) The department shall deny, suspend, or revoke the approval of any Provisional trauma center which misrepresents a material fact in its application for trauma center approval, including the site survey process.
(4) In the event a trauma center terminates its trauma services, it shall give notice of its intent to terminate to the department via a letter signed by its CEO or designee. The letter shall be addressed to the Division, Division of Emergency Medical Operations, and shall reference and comply with chapter 395.4025(8), F.S. The letter shall include an explanation of the specific reason or reasons why the trauma center wants to terminate its trauma services. The termination will be effective 6 months from receipt of the letter by the department unless a longer time is specified in the letter. Upon termination, the hospital shall cease operating or holding itself out as a trauma center. Specific Authority 395.405 FS. Law Implemented 395.1031, 395.401, 395.4015, 395.402, 395.4025, 395.404, 395.4045, 395.405 FS. History-New 8-3-88, Amended 12-10-92, 12-10-95. Formerly 10D-66.109. Amended 8-4-98, 2-20-00, 6-3-02, 06-09-05. 64E-2.025 Extension of Application Period.

EFFECTIVE 12-18-2006 Emergency Medical Services
39
(1) Any hospital may request that the department grant up to 18 months additional time to complete its application to become a trauma center if the hospital determines prior to submitting an application that the hospital cannot meet all of the standards of critical elements as provided in paragraph 64E-2.024(1)(d), F.A.C. The standards of critical elements provided in paragraph 64E-2.024(1) (d), F.A.C., are the only standards for which an extension shall be considered. The request for extension must also comply with the requirements provided in this section. (2) To be considered for an extension, a hospital must submit an application in accordance with the requirements in Rule 64E-2.024, F.A.C., together with a request for extension. The request for extension must contain the following: (a) the specific date the hospital desires to have the department begin the provisional review of the hospital's application; (b) a reference to each standard, or specific part of a standard, in DHP 150-9, December 2004, Trauma Center Standards, which is incorporated by reference in Rule 64E-2.023, F.A.C., that the hospital is unable to meet; (c) for each standard, or specific part of a standard, that the hospital is unable to meet, a detailed and separate explanation as to why the standard, or specific part of a standard, cannot be met; and (d) an action plan that describes the major activities planned to meet each standard, or specific part of a standard, and the completion date for each activity. (3) The department shall, by April 15, conduct a review of the hospital's extension request for completeness and to determine any deficiencies. (4) No later than April 15, hospitals with extension requests found to be incomplete or deficient will be notified in writing of the deficiencies or incomplete sections, and shall be given the opportunity to submit additional clarifying or corrective information. (5) The hospital shall submit the requested information to the department no later than 5 working days after receipt of the department's notification. Failure to provide the requested information or failure to address the deficiencies or incomplete information identified by the department shall result in the denial of the hospital's extension request. (6) The department shall notify the hospital on or before May 1 of the approval or denial of the hospital's extension request. If the extension is granted, the department shall provide written notification to the hospital of the beginning and ending dates of the extension.
(7) The department shall make a final determination on whether to approve or deny a hospital's extension request only after the provisional review of all other trauma center applications in the hospital's TSA are completed, and it has been determined that the number of trauma centers and Provisional trauma centers in the hospital's TSA is less than the allocated number of positions available for that TSA. (8) If the hospital's request for extension is denied, the hospital may, within 30 days of receipt of the notification of denial, request a hearing to contest the decision of the department, in accordance with Chapter 120.57, F.S. (9) The hospital may modify any date for completion of a major activity in the department-approved action plan discussed in (d) of this section without prior department approval. When any date for completion of a major activity is modified by the hospital, the hospital must provide an updated action plan to the department. The hospital must complete all major activities within the extension period granted by the department. The department will not begin the provisional review of the hospital's application for approval as a trauma center at the end of the extension period, or earlier at the request of the hospital, unless the hospital can substantiate completion of all major activities in the action plan. The department may conduct a site visit to determine the hospital's compliance with the approved action plan. (10) The department shall begin a provisional review of the hospital's trauma center application on the date the hospital specified in the extension request, as approved by the department. The hospital may request that the department begin the provisional review earlier than the date specified in the extension request if the hospital completes all action steps before the expiration of the approved extension period. The department's provisional review of the hospital's application shall be conducted in accordance with the timeframes for processing the application provided in section 64E-2.024, F.A.C., but will not coincide with the dates provided in that section. (11) The hospital shall ensure that the trauma center’s application provided at the time the hospital submitted the extension request is current on the date the department begins the provisional review. (12) A hospital receiving an extension greater than 12 months shall have its extension terminated if the number of trauma centers or Provisional trauma centers in the hospital's TSA equals the number of available positions allocated to the TSA, resulting in the denial of its application and the department will inform the applicant of its right to a Section 120.57, F.S., hearing regarding this denial. (13) The department shall complete an in-depth review of the application of each hospital

EFFECTIVE 12-18-2006 Emergency Medical Services
40
that received an extension and became a Provisional trauma center within 90 days of the hospital receiving provisional status according to the following schedule: (a) The department shall review the application and inform the Provisional trauma center of any omissions, deficiencies, or problems within 30 days of the date the department begins the in-depth review; (b) The Provisional trauma center may provide additional information in response to the department's notice of omissions, deficiencies, or problems within 30 days of receipt of the department's notification. If the Provisional trauma center does not provide additional information within 30 days, the department shall inform the Provisional trauma center of any omissions, deficiencies, or problems that were not corrected at the conclusion of the in-depth review. (c) If the Provisional trauma center submits additional information, the department shall review the additional information and inform the Provisional trauma center of any remaining omissions, deficiencies, or problems that were not corrected at the conclusion of the in-depth review. (14) A hospital approved by the department as a Provisional trauma center following an approved extension period, shall receive a site visit during the next scheduled site visit phase. The hospital shall operate as a Provisional trauma center no less than 6 consecutive months prior to the site visit. Specific Authority 395.405 FS. Law Implemented 395.401, 395.4015, 395.402, 395.4025, 395.404, 395.4045, 395.405 FS. History-New 12-10-92, 12-10-95. Formerly 10D-66.1095. Amended 8-4-98, 2-20-00, 6-3-02, 06-09-05.

41
Table VII Reference Section 64E-2.024, F.A.C.
PROCESS FOR APPROVAL OF TRAUMA CENTERS
Task SEP
OCT
NOV
DEC
JAN
FEB
MAR
APR
MAY
JUN
JUL
AUG
SEP
OCT
NOV
DEC
JAN
FEB
MAR
APR
MAY
JUN
JUL
Hospitals Submit Letters of Intent
DH Sends Applications to Hospitals
Hospitals Complete Applications
Hospitals Submit Applications
Preliminary Review of Applications by DH
Hospitals Respond to Deficiencies
Hospitals Informed of Provisional Status
In-Depth Review of Applications by DH
Revised Applications Submitted by Provisional Trauma Centers
DH Final Review of Applications
Provisional Trauma CentersNotified of In-Depth Review
Findings
DH Conducts Site Visit Quality of Care Assessments
DH Approves Trauma Centers
DH Notifies Hospitals of Approval as Trauma Centers

42
64E-2.026 Certificate of Approval. Each hospital approved as a trauma center shall be issued a DH Form 2032-Z, December 2004, Level I Trauma Center Certificate of Approval, DH Form 2043-Z, December 2004, Level II Trauma Center Certificate of Approval, or DH Form 1721-Z, December 2004, Pediatric Trauma Center Certificate of Approval, which are incorporated by reference and available from the department. The certificates shall include:
(1) The date effective and the date of termination;
(2) The hospital's name; and (3) The approved trauma center level. Specific Authority 395.4025, 395.405 FS. Law Implemented 395.401, 395.4015, 395.402, 395.4025, 395.404, 395.4045, 395.405 FS. History-New 8-3-88, Amended 12-10-92. Formerly 10D-66.110. Amended 02-20-00, 4-15-01, 06-09-05. 64E-2.027 Process for Renewal of Trauma Centers (1) At least 14 months prior to the expiration of the trauma center’s certification, the department shall send, to each trauma center that is eligible to renew, a blank DH Form 2032R, December 2004, Trauma Center Application to Renew, which is incorporated by reference and available from the department, in accordance with the provisions of this section. Within 15 calendar days after receipt, the trauma center choosing to renew its certification shall submit to the department the completed DH Form 2032R, December 2004. (2) All renewing trauma centers shall receive an on-site survey after the department’s receipt of the completed DH Form 2032R, December 2004. The department shall notify each trauma center of the results of the site survey within 30 working days from completion of the site survey. If the trauma center desires to provide additional information regarding the results of the site survey to the department to be considered, the information must be provided in writing and be received by the department within 30 calendar days of the hospital’s receipt of the department’s notice. If the trauma center elects not to respond to the department’s notice within 30 calendar days, the department shall make the final determination of approval or denial based solely on information collected during the applicant’s site survey. (3) At least 45 days prior to the expiration of the certification, the department shall simultaneously notify each facility in writing of their approval or denial to renew. If approved, this renewal certification shall be for a period of 7 years beginning the day after the current certification expires.
(4) A trauma center which does not desire to be re-approved shall follow the notification provisions of Section 395.4025(8), F.S. Specific Authority 395.4025, 395.405 FS. Law Implemented 395.401, 395.402, 395.4025, 395.404, 395.4045, 395.405 FS. History-New 8-3-88, Amended 12-10-92, 1-23-96. Formerly 10D-66.111. Amended 3-15-98, 2-20-00, 06-09-05. 64E-2.028 Site Visits and Approval. (1) Each Provisional trauma center shall receive an on-site evaluation to determine whether the hospital is in substantial compliance with standards published in DHP 150-9, December 2004, Trauma Center Standards, which is incorporated by reference in Rule 64E-2.023, F.A.C., and to determine the quality of trauma care provided by the hospital. (2) The on-site evaluation shall be conducted by a review team of out-of-state reviewers with knowledge of trauma patient management as evidenced by experience in trauma care at a trauma center approved by the governing body of the state in which they are licensed. (3) All Provisional trauma centers shall receive a site visit between October 1 of each year and June 1 of the following year. (4) The reviewers shall assess each applicant hospital's compliance with the standards published in DHP 150-9, December 2004, by means of direct observation, review of call schedules, and review of patient charts. Reviewers also shall assess the quality of trauma patient care and trauma patient management by reviewing facility trauma mortality data, by reviewing patient charts and by reviewing trauma case summaries and minutes of trauma quality management committee meetings pursuant to Standard XVIII of DHP 150-9, December 2004. (5) Evaluation of the Quality of Trauma Patient Care and Trauma Patient Management: (a) The reviewers shall judge the quality of trauma patient care and the quality of trauma patient management in each Provisional trauma center by analyzing each facility's trauma patient care and trauma patient outcomes, by reviewing trauma patient charts and by evaluating the effectiveness of the trauma quality management program through reviews of trauma case summaries and minutes of trauma quality management committee meetings. (b) Evaluations of trauma patient care and trauma patient management will also be conducted using trauma patient data collected from the hospital trauma registry and the Florida Trauma Registry from the time the hospital received provisional trauma center status through the date of the on-site review. Trauma patient data may also be collected from the emergency department patient log, audit filter log, or quality management committee minutes. The patient

43
population for review shall be selected on the basis of Injury Severity Scores (ISS). The ISS shall be determined using Abbreviated Injury Scaling (AIS-90). If the Provisional trauma center has an in-hospital trauma registry which computes the ISS using the International Classification of Disease, 9th Revision, Clinical Modification (ICD-9-CM), the computer program shall contain AIS-90 as a component of the program. (c) Patient charts to be reviewed shall be selected by the department from cases meeting the criteria listed in Standard XVIII B.2, published in DHP 150-9, December 2004. A minimum of 75 cases shall be selected for review in each facility. If the cases total less than 75, then all cases are subject to review. (d) Patient charts shall be reviewed to identify factors related to negative patient outcome or compromised patient care. When such factors are identified, trauma case reviews by the medical director of the trauma service or the trauma nurse coordinator, as well as minutes of trauma quality management committee meetings, shall be reviewed to determine if corrective action was taken by the trauma service and appropriate peer review committees within the facility. (e) Reviewers shall study the trauma case reviews and trauma quality management committee meeting minutes to evaluate the overall effectiveness of the quality management program. (6) The reviewers shall rate a Provisional trauma center which they have reviewed as either acceptable, acceptable with corrections, or unacceptable. The rating shall be based on each facility's substantial compliance with the standards published in DHP 150-9, December 2004, and upon the performance of each Provisional trauma center in providing acceptable trauma patient care and trauma patient management which resulted in acceptable patient outcomes. (7) The department shall evaluate the results of the site visit review and the in-depth application review of each Provisional trauma center between June 1 and July 1. All applicant hospitals shall be notified simultaneously of their approval or denial to become a trauma center on or before July 1. The department's selection will be based on the results of the site visit and the in-depth application review. In those situations in which there are more trauma centers, Provisional trauma centers than available positions in the TSA, the criteria in paragraph (11) of this section shall be applied for final selection. (8) The department shall notify each Provisional trauma center of the results of the site visit within 30 working days from completion of the site visit. The department shall include in the notice any problems that the Provisional trauma center was informed of at the conclusion of the department's in-depth application review. If the Provisional trauma center desires to provide additional information regarding the results of the site visit or in-depth application review to the department to be considered during the final
evaluation between June 1 and July 1, the information must be provided in writing and be received by the department within 30 calendar days of the hospital's receipt of the department's notice. If the Provisional trauma center elects not to respond to the department's notice within 30 calendar days, the department shall make the final determination of approval or denial based solely on information collected during the applicant's site visit and in-depth application review. (9) Site Visits may be conducted at any reasonable time at the discretion of the department at any Provisional trauma center or trauma center by the department staff or reviewers to: (a) verify information provided pursuant to section (8); and (b) ensure each trauma center maintains substantial compliance with trauma center standards, quality of trauma patient care, and quality of trauma patient management. (10) Section 395.4025(12), F.S., makes confidential and exempt from the provisions of Section 119.07(1), F.S., not only patient care, transport or treatment records and patient care quality assurance proceedings, but also records or reports made or obtained pursuant to Sections 119.07(3)(v), 395.3025(4)(f), 395.401, 395.4015, 395.402, 395.4025, 395.403, 395.404, 395.4045 and 395.405, F.S. The department identifies the confidential and exempt records included within the authority of these laws to be the following: (a) patient care, transport or treatment records; (b) patient care quality assurance proceedings, records, or reports; (c) any site survey instrument of the department, its agents, or surveyors in any form; (d) any site survey findings of the department; and (e) a hospital’s response to the department’s site survey findings. (11) If the number of Provisional trauma centers found eligible for selection by the department in a given TSA exceeds the number permitted, as provided in subsection 64E-2.022(3), F.A.C., the following criteria shall be applied independently and consecutively to all Provisional trauma centers in the TSA until application of the criteria results in the number of trauma centers authorized in subsection 64E-2.022(3), F.A.C., for that TSA. When that occurs, the remaining criteria shall not be considered. The criteria to be applied are as follows: (a) A hospital recommended to be a trauma center in the department-approved local or regional trauma agency plan pursuant to subparagraph 64E-2.019(2)(d)3., F.A.C., shall be given approval preference over any hospital which was not recommended. (b) A hospital shall be given selection preference based on the level of service they intend to provide according to the following sequence:

44
1. A Provisional Level I trauma center will be given preference over a Provisional Level II trauma center with pediatrics, a Provisional Level II trauma center, and a Provisional pediatric trauma center; 2. A Provisional Level II trauma center with pediatrics will be given preference over a Provisional Level II trauma center and a Provisional pediatric trauma center; and 3. A Provisional Level II trauma center will be given preference over a Provisional pediatric trauma center in TSA having only one allocated trauma center position, and in a TSA with more than one allocated trauma center position if there already exist an approved Level I trauma center, Level II trauma center with pediatrics, or a pediatric trauma center; or if in the instant selection process a Level I trauma center Level II trauma center with pediatrics, or pediatric trauma center is to be selected. (c) An applicant hospital in a geographic location that is most conducive to access by the greatest number of people to be served within a TSA shall be given preference for selection. (d) A hospital representing the best geographic distribution with respect to terrain, population served and projected service population in a given TSA shall be given preference for selection. (e) A hospital which, according to the most recent complete year of Agency for Health Care Administration data, shows a higher level of commitment of care to the service area, as evidenced by the ratio of non-paying to paying patients, shall be given preference for approval. (12) The department shall inform in writing each Provisional trauma center denied approval as a trauma center of its opportunity to request a hearing in which to contest the denial in accordance with Section 120.57, F.S. Specific Authority 395.4025, 395.405 FS. Law Implemented 395.401, 395.4015, 395.402, 395.4025, 395.404, 395.4045, 395.405 FS. History-New 8-3-88, Amended 12-10-92, 10-2-94, 12-10-95. Formerly 10D-66.112. Amended 8-4-98, 2-20-00, 6-3-02, 06-09-05. 64E-2.029 Application by Hospital Denied Approval. Any hospital that was not approved as a trauma center based on the application of criteria in Rule 64E-2.028, F.A.C., may submit a completed Letter of Intent DH Form 1840, December 2004, postmarked no earlier than September 1 and no later than midnight October 1 of the following year. Specific Authority 395.4025, 395.405 FS. Law Implemented 395.401, 395.4015, 395.402, 395.4025, 395.404, 395.4045, 395.405 FS. History-New 8-3-88, Amended 12-10-92, 12-10-95. Formerly 10D-66.113. Amended 2-20-00, 06-09-05.
64E-2.030 Emergency Medical Services Grants Procedures. (1) In order to apply for a matching emergency medical services grant, applicants shall submit DH Form 1767, June 02, EMS Matching Grant Application contained in the EMS Matching Grant Program Application Packet, June 02. This application packet is incorporated by reference and available from the department. The application packet contains the following forms which are also incorporated by reference and available from the department: DH Form 1767, EMS Matching Grant Application, June 02, DH Form 1767P, Request for Grant Fund Distribution, June 02, DH Form 1684A, EMS Grant Program Expenditure Report, June 02, DH Form 1684C, EMS Grant Program Change Request, June 02, DH Form 1767G, Matching Grants Evaluation Worksheet, June 02. (2) The department shall advertise grant availability in the Florida Administrative Weekly (FAW). The FAW notice shall establish the deadline for submission of applications. Following the review by the grant review team and approval by the Secretary of the Department of Health, the department shall publish in the FAW the date, time, and location of the posting of the grant awards. (3) All grant award decisions shall be posted on a date and time certain at a specific location in Tallahassee, Florida. All grant award notices shall be published on the Bureau of Emergency Medical Services website at www.doh.state.fl.us/ems, at the date and time established in the FAW notice as outlined in (2) above. (4) All matching grant applications submitted to the department shall have the envelope or other container marked in large bold letters “EMS GRANT APPLICATION”. Upon receipt of the completed application the department shall date stamp the application and it shall remain unopened until the official opening date published in the FAW. (5) The grant review team for matching grant applications eligible for a grant of 75% of approved budgets shall consist of at least five persons appointed by the Chief. The Chief shall appoint a minimum of three department staff to review rural applications eligible for a grant of at least 90% of their approved budgets. (6) In order to apply for a county award grant, applicants shall submit DH Form 1684, EMS County Grant Application, June 02, contained in the EMS County Grant Program Application Package, June 02. This application packet is incorporated by reference and available from the department. The application packet contains the following forms which are also incorporated by reference and available from the

45
department: DH Form 1684, EMS County Grant Application, June 02, DH Form 1684C, EMS Grant Program Change Request, June 02, DH Form 1684A, EMS Grant Program Expenditure Report, June 02, DH Form 1767P, Request for Grant Fund Distribution, June 02. Specific Authority 401.121 FS. Law Implemented 401.111, 401.113, 401.121 FS. History-New 6-6-90, Amended 12-10-92, 1-26-97. Formerly 10D-66.205. Amended 8-4-98, 11-3-02, 6-9-03. 64E-2.031 Do Not Resuscitate Order (DNRO) Form and Patient Identification Device.
(1) An emergency medical technician or paramedic shall withhold or withdraw cardiopulmonary resuscitation:
(a) upon the presentation of an original or a completed copy of DH Form 1896, Florida Do Not Resuscitate Order Form, December 2004, which is incorporated by reference and available from the department at no cost, or, any previous edition of DH Form 1896; or
(b) upon the presentation or observation, on the patient, of a Do Not Resuscitate Order patient identification device.
(2) The Do Not Resuscitate Order: (a) form shall be printed on yellow paper and
have the words "DO NOT RESUSCITATE ORDER" printed in black and displayed across the top of the form. DH Form 1896 may be duplicated, provided that the content of the form is unaltered, the reproduction is of good quality, and it is duplicated on yellow paper. The shade of yellow does not have to be an exact duplicate;
(b) patient identification device is a miniature version of DH Form 1896 and is incorporated by reference as part of the DNRO form. Use of the patient identification device is voluntary and is intended to provide a convenient and portable DNRO which travels with the patient. The device is perforated so that it can be separated from the DNRO form. It can also be hole-punched, attached to a chain in some fashion and visibly displayed on the patient. In order to protect this device from hazardous conditions, it shall be laminated after completing it. Failure to laminate the device shall not be grounds for not honoring a patient’s DNRO order, if the device is otherwise properly completed.
(3) The DNRO form and patient identification device must be signed by the patient's physician. In addition, the patient, or, if the patient is incapable of providing informed consent, the patient's health care surrogate or proxy as defined in Section 765.101, F.S., or court appointed guardian or person acting pursuant to a durable power of attorney established
pursuant to Section 709.08, F.S., must sign the form and the patient identification device in order for them to be valid.
(4) An emergency medical technician or paramedic shall verify the identity of the patient who is the subject of the DNRO form or patient identification device. Verification shall be obtained from the patient's driver license, other photo identification, or from a witness in the presence of the patient.
(5) During each transport, the EMS provider shall ensure that a copy of the DNRO form or the patient identification device accompanies the live patient. The EMS provider shall provide comforting, pain-relieving and any other medically indicated care, short of respiratory or cardiac resuscitation.
(6) A DNRO may be revoked at any time by the patient, if signed by the patient, or the patient's health care surrogate, or proxy or court appointed guardian or person acting pursuant to a durable power of attorney established pursuant to Section 709.08, F.S. Pursuant to Section 765.104, F.S., the revocation may be in writing, by physical destruction, by failure to present it, or by orally expressing a contrary intent. Specific Authority 381.0011, 401.45(3) FS. Law Implemented 381.0205, 401.45, 765.401 FS History-New 11-30-93. Amended 3-19-95, 1-26-97. Formerly 10D-66.325. Amended 2-20-00, 11-3-02, 06-09-05. 64E-2.032 Certificate of Public Convenience and Necessity.
(1) Each county is empowered pursuant to Section 401.25(2)(d) and (6), F.S., to issue a COPCN to an ambulance service which proposes to operate within that county. (2) The department shall license an ambulance service, and that service may operate in a county in this state, provided the applicant meets the ambulance service requirements of Chapter 401, part III, F.S., and this rule chapter, and provided further that the ambulance service has first obtained a COPCN: (a) From each county in which the ambulance service provides or proposes to provide prehospital ALS services or prehospital BLS transportation services. (b) From each county within which the ambulance service provides or proposes to provide intracounty, interfacility ALS services or interfacility BLS transportation services. (c) From each county where the ambulance service provides or proposes to provide interfacility ALS services or BLS transportation services in which the need for such service either originates or terminates, but not from both the county where the need for such service originates and the county where the need for such service terminates unless the
46
county by ordinance pursuant to Section 401.25(6), F.S., mandates a COPCN for both. (3) All licenses issued by the department shall be for ALS, BLS transport or air ambulance service consistent with the services authorized by the COPCN, if the department requires a COPCN pursuant to this section. If the applicant is not required by the county to have a COPCN to operate in that county, the department shall issue a license in one of the above categories and upon meeting all of the other requirements of Rules 64E-2.002 and .003, F.A.C. (4) Provisions of this section to the contrary notwithstanding, the department shall license an ambulance service which meets the ambulance service requirements of Chapter 401, F.S., part III, and Chapter 64E-2, F.A.C., in any county where the ambulance service provides or proposes to provide services for which a license is required under chapter 401, F.S., part III, where the county does not require a COPCN for such services. (5) An ambulance service licensed by the department is permitted to provide services under its license in a county without first having obtained a COPCN from the governing body of that county, if such service is provided pursuant to and consistent with the terms of a mutual aid agreement with that county, or as part of a coordinated response to a disaster or a mass casualty incident. Pursuant to Section 401.23(16), F.S., a mutual aid agreement must be in writing, must be sanctioned by the governing bodies of the affected counties, and must at a minimum include: (a) The conditions under which the agreement shall be activated. (b) The procedures and medical protocols to be followed during activation. (c) The conditions and process by which the agreed upon services shall be terminated. Specific Authority 401.35 FS. Law Implemented 401.23, 401.25, 401.251, 401.252, 401.33, 401.35, 401.411, 401.414, 401.421 FS. History-New 10-2-94, Amended 1-26-97. Formerly 10D-66.335. Amended 01-03-99. 64E-2.033 Convicted Felons Applying for EMT or Paramedic Certification or Recertification. (1) An applicant for certification or recertification as an EMT or paramedic who has been convicted of or plead no contest, regardless of adjudication, to a felony and has complied with the requirements of Chapter 940, FS., and provides documentation of restoration of Civil Rights shall become certified provided that the requirements of Section 401.27, F.S., and Rule 64E-2.008, F.A.C., for EMT or Rule 64E-2.009, F.A.C., for paramedic have been met and no other basis for denial exists.
(2) The department shall consider an applicant for certification or recertification as an EMT or paramedic with a felony conviction upon their submission of the following documentation: (a) Copy of the judgement of the felony conviction. (b) All probation documents, including the name and telephone number of the probation officer.
(c) Information regarding any additional convictions.
(d) Any and all information related to the conviction, or plea and any and all information in support of the application, which the department deems necessary to base a decision for approval or denial. Specific Authority 401.27, 401.35. Law Implemented 401.27, 401.41, 401.411, 401.414, 401.421. History-New 1-03-99. Amended 11-3-02. 64E-2.034 Inspections (1) Inspections of Emergency Services Providers shall be documented by the department. Neonatal vehicle inspections shall be documented on Neonatal Interfacility Vehicle Inspection Form; DH Form 1831, June 99. This form is incorporated by reference and available from the department.
(2) Violation categories - All equipment, medical supplies, records and procedures required by Florida Statutes and rules are placed in one of three violation categories: Category 1 - life-saving equipment, medical supplies, drugs, records, or procedures; Category 2 - intermediate support equipment, medical supplies, drugs, records or procedures; Category 3 - minimal support equipment, medical supplies records or procedures. These categories shall be used to determine corrective action time frames for deficiencies noted during inspections. The violation categories for each required item are noted on the inspection documentation.
(3) Corrective Action: (a) Corrective Action Time Frames - Based on
the violation category definitions listed above, the following corrective action time frames and administrative action guidelines shall apply: Category 1 - any item in this category found deficient shall require action by the service provider within 24 hours of the inspection to replace or correct the deficiency noted to avoid administrative action by the department; Category 2 - any item in this category found deficient shall require action by the service provider within 5 working days (Monday - Friday) of the inspection to replace or correct the deficiency noted to avoid administrative action by the department;
47
Category 3 - any item in this category found deficient shall require action by the service provider within 10 working days (Monday - Friday) of the inspection to avoid administrative action by the department.
(b) Inspection Corrective Action statement - Upon completion of an inspection in which deficiencies were noted, the EMS provider shall be given DH Form 1831, October 05 Inspection Corrective Action Statement, which is incorporated by reference and available from the department. This form documents the corrective action that must be taken by the EMS provider to correct the inspection deficiencies and the time frames within which the corrective action must be taken. The completed DH form 1831, October 05, and documentation of the corrective action taken, must be received by the department within 14 working days of the inspection. Failure of the EMS provider to submit the corrective action statement or correct identified deficiencies within the required time frames is grounds for disciplinary action under Chapter 401, F.S.
(4) A copy of the Inspection Corrective Action Statement shall be maintained by the provider for a period of 3 years. Specific Authority 401.31, 401.35 FS. Law Implemented 401.31 FS. History New 2-20-00. Amended 9-3-00, 12-18-06. 64E-2.035 Emergency Treatment of Insect Stings. (1) An individual who desires to be certified to administer epinephrine to a person who suffers adverse reactions to insect stings must: (a) Be 18 years of age or older; (b) Have, or reasonably expect to have as a result of occupation or volunteer status, responsibility for at least one other person who has severe adverse reactions to insect stings; and (c) Have successfully completed, within the previous 2 years, a training program in the appropriate procedures for administration of epinephrine to persons who suffer adverse reactions to insect stings. (2) Epinephrine administration training programs shall be conducted by a Florida licensed physician and shall include, at a minimum, 30 minutes of training on the following subjects: (a) Definition of anaphylaxis; (b) Agents which might cause anaphylaxis and the distinction between them, including insect stings, drugs, food and inhalants; (c) Recognition of symptoms of anaphylaxis; (d) Appropriate emergency treatment of anaphylaxis as a result of insect stings; (e) Use of a method of administration of epinephrine, i.e., autoinjector, as a result of insect
stings including demonstration verifying correct technique; (f) Pharmacology of epinephrine including its indications, contraindications, and side effects; (g) Instruction that administration of epinephrine shall be utilized only in the absence of the availability of a physician. (3) The individual shall apply on DH Form 1882, October 2000, Application for Insect Sting Emergency Treatment Certification, which is incorporated by reference and available from the department, and submit documentation of successful completion of the training requirements as outlined in subsection 64E-2.035(1), F.A.C., with the required certification fee of $25 to the department. (4) Certificates of training expire on March 1 of each odd-numbered year. The requirements for and process for renewal of certification are the same as that for initial certification. Specific Authority 381.88(3) FS. Law Implemented 381.88 FS. History-New 9-3-00. Amended 4-15-01. 64E-2.036 Training Programs. (1) Qualifications and procedures for EMT and paramedic training programs in addition to those contained in Section 401.2701, F.S., are as follows: (a) each applicant shall demonstrate that EMT and paramedic students are not subject to call while participating in class, clinical or field sessions. (b) each applicant shall demonstrate that each EMT and paramedic student function under the direct supervision of an EMS preceptor and shall not be in the patient compartment alone during patient transport and shall not be used to meet staffing requirements. (c) each applicant shall receive a scheduled site visit by the department. Any paramedic training program that is accredited by the Committee on Accreditation of Educational Programs for the Emergency Medical Services Professions (CoAEMSP) has the option to request that the department schedule its site visit to the institution in conjunction with the CoAEMSP site visit to avoid duplication of effort and unnecessary interruption of the student learning environment. (d) course directors shall submit a roster of students eligible to take the state certification examination to the department within 14 days after course completion; but not before course completion. This roster shall be signed by the program director. (2) To be approved as an EMT Training Program, an entity shall submit a completed DH Form 1698, October 05, Application for Approval of an Emergency Medical Technician – Basic (EMT-B) Training Program, which is incorporated by reference and available from the department.

48
(3) To be approved as a Paramedic Training Program, an entity shall submit a completed DH Form 1698, October 05, Application for Approval of an Emergency Medical Technician-Paramedic (EMT-P) Training Program, which is incorporated by reference and available from the department. (4) Any changes to the training as approved by the department, shall be submitted to the department for review within 30 days of the change. (5) Commencing with the effective date of this rule and expiring December 1 of even numbered years thereafter, entities not licensed as an emergency medical services provider or a department approved Florida training program shall be approved to conduct EMT or paramedic recertification training providing they meet the requirements contained in Section 401.2715, F.S., and this section. To be approved as an EMS Recertification Training Program, each applicant shall: (a) submit DH Form 1698C, February 2001, Application for Review of Continuing Education Offering which is incorporated by reference and available from the department. (b) submit a non-refundable fee of $300 for approval of continuing education which is valid for a period of 2 years concurrently with the EMT and paramedic recertification cycle. (c) submit the following for each course offering: 1. Behavioral objectives: a. Describe expected learner outcomes in terms that can be evaluated, are attainable and are relevant to current US DOT NSC. b. Determine teaching methodology and plan for evaluation. 2. Subject matter: a. Shall reflect the professional educational needs of the student. b. Currency and accuracy shall be documented by references/ bibliography. 3. Faculty qualifications: a. Provide evidence of academic credentials or expertise in the subject matter. b. When the subject matter includes advanced life support, a physician, nurse or paramedic with expertise in the content area shall be involved in the planning and instruction. 4. Medical Direction: a. Provide evidence of current contract with a physician who has experience in emergency medicine, trauma or appropriate certification in prehospital care. b. Responsibilities of physician shall be clearly stated on contract. 5. Teaching strategies:
a. Learning experiences and teaching methods, relative to emergency medical services, are utilized to achieve the objectives. b. Adult education principles are employed in teaching strategies. c. Time is allowed for each activity to ensure opportunity for each student to meet the objectives. 6. Evaluation methods: Evidence shall be submitted that participants are given an opportunity to evaluate learning experiences, instructional methods, facilities and resources used. 7. Contact hour criteria: a. All offerings shall be at least 50 minutes in length which is equivalent to 1 contact hour. b. Increments of 25 minutes will be accepted if the offering extends beyond 1 contact hour. (6) All training offered for the purpose of recertification of EMTs and paramedics shall be documented through a system of record keeping which shall include: program title, course outline, course objectives, dates offered, name of instructor, contact hours and roster of attendees. Each entity shall submit a roster of students that have completed training to the department within 14 days after completion; but not before course completion. The course director shall sign this roster. (7) Recertification Training Programs, which maintain current approval from the department, and have an assigned approval code, may submit additional courses for approval during the current recertification cycle without paying an additional fee. The training program shall comply with the other requirements contained in subsection 64E-2.036(5), F.A.C. (8) The department shall periodically conduct monitoring site visits to entities conducting recertification training to verify that the training is being documented through record keeping that verifies compliance with the recertification requirements of Rules 64E-2.008 and 64E-2.009, F.A.C., for all training conducted. These training records shall be retained for a minimum of 4 years, which shall include the 2 year period within each certification cycle and the immediate 2 year period following that certification cycle. (9) A medical director’s affirmation of completion of recertification training as provided in Section 401.2715(3), F.S., is the physician’s confirmation that the certificate holder has completed recertification training consisting of at least 30 hours, and is based on the requirements of paragraph 64E-2.008(2)(a), F.A.C., or 64E-2.009(2)(a), F.A.C. Specific Authority 401.27, 401.2715 FS. Law Implemented 401.27, 401.2715 FS. History-New 9-3-00. Amended 4-15-01, 4-21-02, 11-3-02, 12-18-06.
49
64E-2.037 Security of Medications. (1) Each ALS and air ambulance provider shall develop, implement, maintain, and have available for review by the department written operating procedures approved and signed by the medical director for procuring, storing, handling, dispensing, and disposal of all controlled substances, medications, and fluids. (a) These procedures must address the provider’s method for meeting applicable state and federal requirements. (b) Security procedures which include the provider’s method of ensuring against theft, tampering with or contamination of controlled substances, medications, and fluids and the identities and position titles of employees who have access to controlled substances. (c) The amount of each controlled substance, authorized by the medical director, to be in on-site storage.
(d) Documentation procedure for the distribution, disposal, and re-supply of controlled substances, medications, and fluids maintained on site. This procedure shall address on-site and shift change inventory procedures for all controlled substances stocked by the provider and identify a record keeping procedure, which includes inventory schedules for stocking of medical supplies and reporting and resolving any discrepancy found during an inventory. (2) All operating procedures related to controlled substances, medications, and fluids shall be consistent with and meet the minimum federal requirements specified by the United States Department of Justice, Drug Enforcement Administration in Title 21, Code of Federal Regulations, Food and Drugs, Part 1300 to END, Chapter II, April 1, 2000, and minimum state requirements specified in Chapters 499 and 893, Florida Statutes and rules adopted there under. Specific Authority 401.26, 401.35 FS. Law Implemented 401.25, 401.26, 401.35(1) FS. History–New 9-3-00. Amended 11-24-02. 64E-2.038 Cardiopulmonary and Advanced Cardiac Life Support Courses.
(1) Cardiopulmonary resuscitation (CPR) or advanced cardiac life support (ACLS) courses which have been accredited by the Continuing Education Coordinating Board for Emergency Medical Services (CECBEMS) are defined as equivalent to CPR or ACLS courses conducted by the American Heart Association or American Red Cross.
(2) Any public or private entities desiring to conduct CPR or ACLS courses equivalent to those conducted by the American Heart Association or American Red Cross shall have those courses accredited by the CECBEMS and shall maintain CECBEMS accreditation of those courses at all times they are offered and conducted.
(3) Entities shall provide a copy of the letter of approval of accreditation from CECBEMS for each CPR and ACLS course to be recognized and accepted as an equivalent by the Department. A copy of the letter of approval shall be submitted to the Department with a completed DH Form 1938, December 2004, Cardiopulmonary Resuscitation (CPR) or Advanced Cardiac Life Support (ACLS) Course Equivalency Form at least 90 days prior to the offering of the course. This form is incorporated by reference and available from the department. In addition to DH Form 1938 and a copy of the letter of approval each entity shall provide a sample completion card or certificate which shall be issued to students successfully completing the course.
(4) The entity shall provide the student with a course completion card or certificate which is the same as that submitted to the Department which includes: name of entity, course title, date of course, expiration date of the card, name of the instructor and name of the student.
(5) Department approval of the CPR and ACLS courses shall be concurrent with the CECBEMS accreditation of the courses.
Specific Authority 401.35,FS. Law Implemented 401.27, FS. History-New 4-21-02. 64E-2.039 Guidelines for Automated External Defibrillators (AED) in State Owned or Leased Facilities.
(1) Management of any state owned or leased facilities considering the placement of AEDs should seek cooperation of facility personnel and local training, medical, and emergency response resources.
(2) An AED is obtained by a prescription from a licensed physician. The prescription must accompany the order for the AED.
(3) Several elements should be considered to determine the appropriate number, placement, and access system for AEDs. Facility managers should consider:
(a) Physician oversight provided by either a facility’s medical staff or contracted through a designated physician. A physician should be involved as a consultant in all aspects of the program.
50
(b) Response Time: The optimal response time is 3 minutes or less. This interval begins from the moment a person is identified as needing emergency care to when the AED is at the side of the victim. Survival rates decrease by 7 to 10 percent for every minute that defibrillation is delayed.
(c) Lay Responder or Rescuer Training 1. Pursuant to Section 401.2915(1), F.S., all
persons who use an AED shall have the required training.
2. Overall effectiveness of AEDs shall be improved as the number of trained personnel increases. Where possible, facility managers should establish in-house training programs on a routine basis.
3. Cardiopulmonary resuscitation and AED training can be obtained from a nationally recognized organization.
4. In addition to training on use of the AED, it is important for lay responders or rescuers to be trained on the maintenance and operation of the specific AED model in the facility.
5. Training is not a one-time event and formal refresher training should be conducted at least every 2 years. Computer-based programs and video teaching materials permit more frequent review. Facility management should make periodic contact with a training entity to assure that advances in techniques and care are incorporated into their program. In addition to formal annual recertification, mock drills and practice sessions are important to maintain current knowledge and a reasonable comfort level by lay responders or rescuers. The intervals for conducting these exercises should be established in consultation with the physician providing medical oversight.
(d) Demographics of the Facility’s Workforce: Management should examine the make up of the resident workforce and consider the age profile of workers. Facilities hosting large numbers of visitors are more likely to experience an event, and an appraisal of the demographics of visitors should be included in an assessment. Facilities where strenuous work is conducted are more likely to experience an event. Specialty areas within facilities such as exercise and work out rooms should be considered to have a higher risk of an event than areas where there is minimal physical activity.
(e) Physical Layout of Facility: Response time should be calculated based upon how long it will take for a lay responder or rescuer with an AED and walking at a rapid pace to reach a victim. Large facilities and buildings with unusual designs, elevators, campuses with several separate buildings, and physical impediments all present unique challenges. In some larger facilities, it may be necessary to incorporate the use of properly equipped
“golf cart” style conveyances to accommodate time and distance conditions.
(f) Suggestions for proper placement of AEDs: 1. A secure location that prevents or minimizes
the potential for tampering, theft, and or misuse, and precludes access by unauthorized users.
2. An easily accessible position (e.g., placed at a height so those shorter individuals can reach and remove, unobstructed access).
3. A location that is well marked, publicized, and known among trained staff. Periodic “tours” of locations are recommended.
4. A nearby telephone that can be used to call backup, security, or 911.
5. Written protocols addressing procedures for activating the local emergency medical services system. These protocols should include notification of EMS personnel of the quantity, brands, and locations of AEDs within the facility.
6. Equipment stored in a manner whereby the removal of the AED automatically notifies security, EMS, or a central control center. If such automatic notification is not possible, emphasis should be placed on notification procedures and equipment placement in close proximity to a telephone.
(g) It is recommended that additional items necessary for a successful rescue be placed in a bag and be stored with the AED. Following are items that may be necessary for successful utilization of the AED:
1. Simplified directions for CPR and use of the AED
2. Non-latex protective gloves 3. Appropriate sizes of CPR face masks with
detachable mouthpieces, plastic or silicone face shields, one-way valves, or other type of barrier device that can be used in mouth to mouth resuscitation.
4. Pair of medium sized bandages 5. Spare battery and electrode pads 6. Two biohazard or medical waste plastic bags 7. Pad of paper and pen for writing 8. Absorbent towel
Specific Authority Laws of Florida 2001-76, House Bill 1429. Law Implemented Laws of Florida 2001-76, House Bill 1429. History-New 11-3-02.
64E-2.040 Funding for Verified Trauma Centers
(1) For Purposes of s. 318.14, F.S., s. 395.4036, F.S. and this rule, in addition to those terms defined in the Florida Trauma Registry Manual, December 2005, (see 64E-2.018) and elsewhere in these rules, the following definitions also apply:
(a) “Attestation” - means a letter on hospital letterhead, signed under oath consistent with s. 92.50,

51
F.S., by the person with direct or delegated authority to make such a statement, stating that the proceeds received by the hospital under s. 395.4036, F.S., were used in compliance with law.
(b) “Certified trauma center”, “verified trauma center” and “trauma center” - all mean a Level I, Level II or Pediatric Trauma Center.
(c) “Caseload volume”, “trauma caseload volume”, and “volume of trauma cases” - all mean the number of patients served by a trauma center during a calendar year, after 2004, on whom data timely supplied by the trauma center to the trauma registry satisfies the Florida Trauma Registry Manual, December 2005, reporting requirements for determining trauma caseload volume (see page 5 of the manual). Solely for calendar years 2004 and 2005, this definition shall be the number of patients served by a trauma center during the respective calendar year on which data was supplied timely by the trauma center consistent with the Florida Trauma Registry Manual, December 2004.
(d) “Local funding contribution” - means local municipal, county or tax district funding, public or private and public foundation funding and service district organization funding received by a hospital or healthcare system that operates a trauma center.
(e) “Weighted ISS volume” - means (The number of patients in the caseload volume for the previous calendar year with an ISS score of 14 and below) + (3 x the number of patients in the caseload volume for the previous calendar year with an ISS score of 15 and above).
(2) Funds collected under s. 318.14(5), F.S., and s. 318.18(14), F.S., and deposited into the department’s administrative trust fund shall be distributed during the subsequent first calendar quarter and during the subsequent third calendar quarter as follows:
(a) First quarter distribution shall be calculated, consistent with (d) and (e) below, using timely submitted caseload volume data from the year preceding the previous calendar year.
(b) Third quarter distribution shall be calculated, consistent with (d) and (e) below, using timely submitted caseload volume data for the previous calendar year.
(c) All distribution shall be consistent with (2) or upon resolution of all relevant administrative and judicial challenges, whichever is later.
(d) Funds collected under s. 318.14(5), F.S. and deposited into the department’s administrative trust fund shall be distributed to the trauma center as follows: [(.5 x funds)/Current total number of trauma centers)] + [(.5 x funds) x (Caseload volume for the trauma center for the previous calendar year/The sum of caseload volume for all trauma centers during the previous calendar year)].
(e) Funds collected under s. 318.18(14), F.S. and deposited into the department’s administrative trust fund under s. 395.4095(1), F.S., shall be distributed as follows:
1. To each trauma center in a region receiving a local funding contribution as of December 31 of the previous year: (.2 x funds) x (Caseload volume for the trauma center for the previous calendar year/The sum of caseload volume for the previous calendar year for all trauma centers receiving funding under (2)(e)1. of this rule).
2. To each trauma center: [(.4 x funds) x (Caseload volume of the trauma center during the previous calendar year/The sum of caseload volume for all trauma centers during the previous calendar year)].
3. To each trauma center: [.4 x funds) x (The trauma center’s weighted ISS volume/The sum of all trauma centers’ weighted ISS volume)]. Specific Authority 395.4036. Law Implemented 395.4036. History-New 4-25-06.