effect of air pollution on children
TRANSCRIPT

SympoSium: Social paediatricS
Effect of air pollution on childrenNeeta Kulkarni
Jonathan Grigg
Abstractair pollution is a major threat to child health. children are particularly
vulnerable to the damaging effects of air pollution because their lungs
are growing and their innate defences against inhaled pollutants may be
impaired. this review focuses on the effects of ‘outdoor’ pollutants from
combustion of fossil fuels, but it is important to note that air pollution
from the combustion of biomass fuels in or near homes is one of the
most important global environmental threats to child health.
Keywords air pollution; children; respiratory disease
Basic concepts
Epidemiological studies strongly suggest that air pollution dam-ages child health. Toxic effects occur mainly at the air–tissue interface of the lung, but effects on other organs may also be important.
Types of air pollution: traffic and industrial emissions are main contributors to ‘outdoor’ air pollution in the ‘developed’ world. ‘Indoor’ air pollution from the burning of biomass (wood, dung, leaves) or cruder fossil fuels (coal) is significant in the ‘develop-ing’ world. Transitional economies such as China have the worst of both worlds: high levels of indoor and outdoor air pollutants.
Most of the key studies on health effects have been done in the developing world and focus on the effects of traffic-associated air pollution. Common mechanisms for health effects related to biomass and fossil fuel may allow extrapolation of these studies to children in the developing world.
What is air pollution? air pollution is a mixture of multiple toxic chemicals and gases, with varying composition depending on the source and meteorological conditions. Most attention has been focused on inhalable particulate matter (PM), oxides of nitrogen, sulphur dioxide, ozone, and volatile organic compounds. In the UK, these key pollutants are monitored for regulatory purposes by local authorities to maintain air quality levels (Figure 1).
Neeta Kulkarni MD is a Locum Consultant Paediatrician at Leicester
Primary Care Trust and a Honorary Research Fellow at the University of
Leicester, Leicester, UK.
Jonathan Grigg MD is the Professor of Paediatric Respiratory and
Environmental Medicine at Barts and the London School of Medicine
and Dentistry, London, UK.
paediatricS aNd cHild HealtH 18:5 23
In epidemiological studies, it is difficult to ascertain which pollutants mediate adverse health effects because pollutants from the same source (e.g. cars) tend to be inter-related. This is not a problem if interventions reduce all emission components (e.g. congestion charging), but is an issue if interventions target only one component of the pollutant mix (e.g. particle traps on car exhausts). Data are therefore required from a range of stud-ies, using: • experimental human exposures to specific pollutants (e.g. die-
sel exhaust particles) • markers of exposure to the emissions from specific sources
(e.g. distance of home to a main road) • cellular and molecular responses to in vitro exposures.In the UK, the National Ambient Air Quality standards aim to pro-tect the health of the public (www.defra.gov.uk/environment/airquality/strategy/pdf/air-qualitystrategy-vol1.pdf). Monitoring equipment is located throughout the country and the resulting outputs (Figure 1) reflect variations in ‘background’ exposure of many individuals in a single city. They do not capture the impor-tant component of personal exposure from small local variations in exposure (e.g. from walking down a main road).
Specific air pollutants
PM: airborne PM is a mixture of many subclasses of pollutants, with diverse chemical composition and size distribution. Health effects can be influenced by chemical composition and particle size; ultrafine particles (100 nm) are particularly toxic to cells.
PM is produced by incomplete combustion of fossil fuels (primary) and their chemical reactions in the atmosphere (sec-ondary). The major constituents of fossil-fuel derived PM are sulfate, nitrate, ammonium, chloride, elemental and organic carbon,1,2 a mix seen in urban air worldwide. Smaller particles tend to deposit in the lower respiratory tract. For this reason, regulations on air quality focus on PM of aerodynamic diameter less than 10 μm (PM10). The concentration of PM10 is usually reported as micrograms per cubic metre (μg/m3) of air. PM not derived from fossil fuel (mainly from wind-blown dusts) mainly fall above the PM10 criterion, and are filtered out in the upper airway.
Ozone (O3) is formed from the action of sunlight on oxides of nitrogen and volatile organic compounds, and is classified as a ‘secondary’ pollutant (i.e. not directly emitted from combustion sources). Ozone has diurnal and seasonal variations. Assessing the independent effect of ozone on child health in epidemio-logical studies is relatively easy because concentrations do not always correlate with other pollutants derived from fossil fuels.
Nitrogen oxides: the most important nitrogen species to be emit-ted from combustion of fossil fuel is nitric oxide (NO). Within a few seconds, nitric oxide reacts with ozone to form nitrogen dioxide, nitric acid and nitrate particles. For some children, a major source of exposure to nitrogen dioxide is from domestic gas stoves.3
Volatile organic compounds are mainly from road traffic and exist in vapour form. Benzene and 1,3-butadiene are of most concern because they are potent genotoxic carcinogens.4
8 © 2008 elsevier ltd. all rights reserved.
SympoSium: Social paediatricS
Date
PM10 particulates (no gravimetric conversion) (roll24 means)
Va
lue
07 Oct 14 Oct 21 Oct 23 Oct0
30
25
20
15
10
5
Date
Nitrogen dioxide (ppb) (roll24 means)
Va
lue
07 Oct 14 Oct 21 Oct 23 Oct0
42
35
28
21
14
7
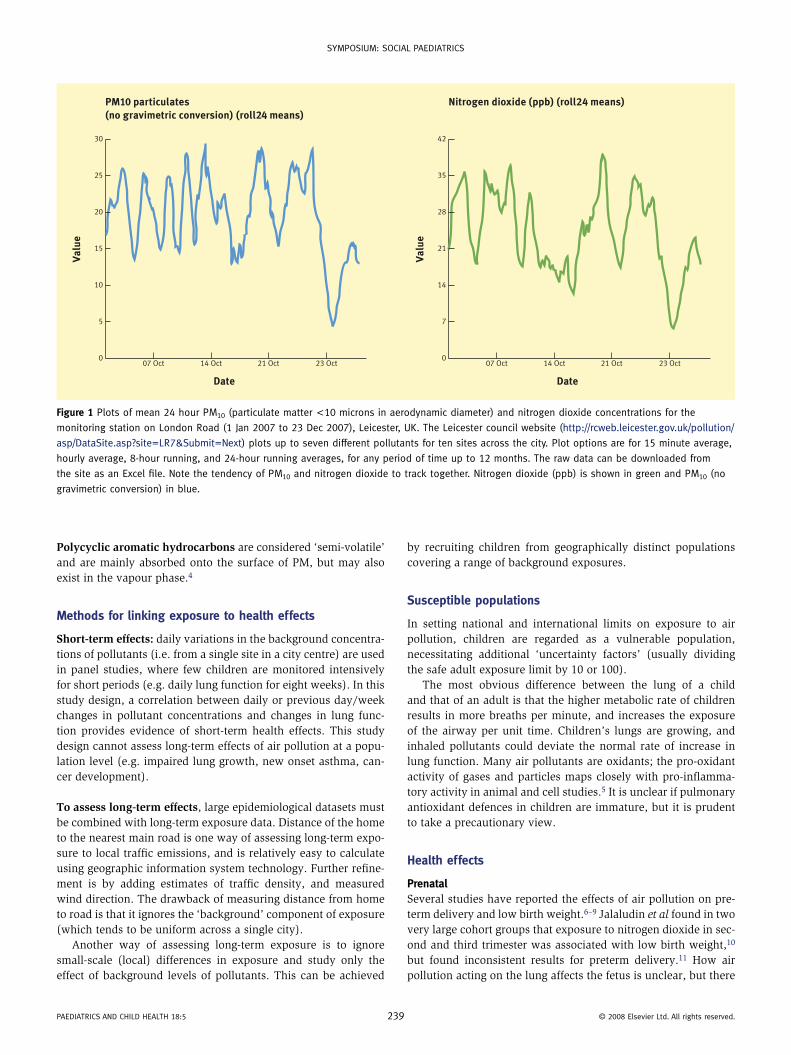
Figure 1 plots of mean 24 hour pm10 (particulate matter <10 microns in aerodynamic diameter) and nitrogen dioxide concentrations for the
monitoring station on london road (1 Jan 2007 to 23 dec 2007), leicester, uK. the leicester council website (http://rcweb.leicester.gov.uk/pollution/
asp/dataSite.asp?site=lr7&Submit=Next) plots up to seven different pollutants for ten sites across the city. plot options are for 15 minute average,
hourly average, 8-hour running, and 24-hour running averages, for any period of time up to 12 months. the raw data can be downloaded from
the site as an excel file. Note the tendency of pm10 and nitrogen dioxide to track together. Nitrogen dioxide (ppb) is shown in green and pm10 (no
gravimetric conversion) in blue.
Polycyclic aromatic hydrocarbons are considered ‘semi-volatile’ and are mainly absorbed onto the surface of PM, but may also exist in the vapour phase.4
Methods for linking exposure to health effects
Short-term effects: daily variations in the background concentra-tions of pollutants (i.e. from a single site in a city centre) are used in panel studies, where few children are monitored intensively for short periods (e.g. daily lung function for eight weeks). In this study design, a correlation between daily or previous day/week changes in pollutant concentrations and changes in lung func-tion provides evidence of short-term health effects. This study design cannot assess long-term effects of air pollution at a popu-lation level (e.g. impaired lung growth, new onset asthma, can-cer development).
To assess long-term effects, large epidemiological datasets must be combined with long-term exposure data. Distance of the home to the nearest main road is one way of assessing long-term expo-sure to local traffic emissions, and is relatively easy to calculate using geographic information system technology. Further refine-ment is by adding estimates of traffic density, and measured wind direction. The drawback of measuring distance from home to road is that it ignores the ‘background’ component of exposure (which tends to be uniform across a single city).
Another way of assessing long-term exposure is to ignore small-scale (local) differences in exposure and study only the effect of background levels of pollutants. This can be achieved
paediatricS aNd cHild HealtH 18:5 2
by recruiting children from geographically distinct populations covering a range of background exposures.
Susceptible populations
In setting national and international limits on exposure to air pollution, children are regarded as a vulnerable population, necessitating additional ‘uncertainty factors’ (usually dividing the safe adult exposure limit by 10 or 100).
The most obvious difference between the lung of a child and that of an adult is that the higher metabolic rate of children results in more breaths per minute, and increases the exposure of the airway per unit time. Children’s lungs are growing, and inhaled pollutants could deviate the normal rate of increase in lung function. Many air pollutants are oxidants; the pro-oxidant activity of gases and particles maps closely with pro-inflamma-tory activity in animal and cell studies.5 It is unclear if pulmonary antioxidant defences in children are immature, but it is prudent to take a precautionary view.
Health effects
PrenatalSeveral studies have reported the effects of air pollution on pre-term delivery and low birth weight.6–9 Jalaludin et al found in two very large cohort groups that exposure to nitrogen dioxide in sec-ond and third trimester was associated with low birth weight,10 but found inconsistent results for preterm delivery.11 How air pollution acting on the lung affects the fetus is unclear, but there
39 © 2008 elsevier ltd. all rights reserved.

SympoSium: Social paediatricS
is strong evidence that air pollutants can influence other organs apart from the lung: • experimental exposure of adults to inhaled particles increases
exercise-induced cardiac ST-segment depression12
• exposure of non-allergic pregnant mice to inert or toxic envi-ronmental air particles causes increased allergic susceptibility in offspring.13
A possible explanation for the association between air pollution and low birth weight is that soluble mediators (e.g. polycyclic aromatic hydrocarbons) released into the systemic circulation from particles impacting at the air–tissue interface impair pla-cental function.
Lung functionOf the potential adverse effects of air pollution of child respira-tory health, the effect of air pollution on lung function is the most robust. Many cross-sectional and longitudinal epidemiological studies suggest that inhalation of PM and gases from the combus-tion of fossil fuel have a deleterious effect on the lung function of normal children.14–18
Studies: a landmark study by Gauderman et al14 prospectively followed up a cohort of 1759 children (average age 10 years) for more than eight years. Differences in the background levels of O3, NO2 and PM in 12 communities in California, USA, were used as markers of long-term exposure (i.e. differences in small-scale local exposure were not assessed). Lung function growth was assessed by repeated spirometric measurements.
Reduced growth of forced expiratory volume in one second (FEV1) was associated with exposure to NO2 (P = 0.005) and inhalable PM (P = 0.04); no effects were found for O3. These associations remained significant after adjustment for several potential confounders and effect modifiers. The reduction in lung function growth associated with air pollution resulted in reduced attainment of adult lung function. For example, the estimated proportion of 18-year-olds with a ratio of observed to expected FEV1 of <80% was 7.9% in high-exposure communities, com-pared with 1.6% in low-exposure communities.
A large cohort study of 3170 children from a city with very high levels of air pollutants (Mexico City, Mexico) concluded that deficits in FEV1 and forced vital capacity growth are significantly associated with PM10, O3 and NO2.19
PM: the inter-relation between pollutants makes it difficult to ascertain the most important components, but the view is that PM (particularly ultrafine PM) is the most toxic to respiratory health. The long-term heath effects of reduced lung function growth are not defined, but the concern is that children growing up in high-pollution areas will suffer increased morbidity and mortality if they develop conditions such as chronic obstructive pulmonary disease.
Local variations in air pollution: the Gauderman et al study14 used differences in background air pollution between geographi-cally distinct communities as a maker of differences in individual exposure, but local variations in air pollution are important.
In a recent study, the authors used a novel method of assess-ing individual exposure to assess the effect on background and local pollution on lung function. The amount of carbon (marker
paediatricS aNd cHild HealtH 18:5 24
for inhaled PM10) in lower airway macrophages from healthy children (Figure 2) was quantified; an increase of 1.0 μm2 in macrophage carbon content was associated with a reduction of 17% in FEV1. An association between the amount of alveolar macrophage carbon and modelled exposure to locally generated particles (mainly from nearby roads) was also found.20
The importance of locally generated air pollution was recently highlighted by a follow-up of the Gauderman et al study.21 The researchers found that, independent of the background pollutant level, children living within 500 metres of the freeway have decreased: • annual growth of forced expiratory volume in 1 sec (%
predicted FEV1) • FVC • maximal mid-expiratory flow rate (MMEF).Thus, decreased lung growth is associated with the background level of air pollutants (affects all children in a geographically defined area) and locally generated pollution (only affects chil-dren living near main roads). Reduced lung growth associated with air pollution appears to be partly reversible. For exam-ple, E Avol et al22 studied children who moved into higher or lower areas of pollution in the Southern California community study. Children who moved to lower levels of exposure of PM10 showed a significant increase in growth of MMEF, particularly if they remained in a lower-exposure community for more than 3 years.
The mechanism for pollutant-induced impairment of lung growth is unclear. It may be mediated by persistent short-term injury. In a systematic review of 22 panel studies in children aged 6–11 years, pooled data analyses show that short-term increases in ambient PM are associated with small, but significant, changes in lung function.18
Respiratory symptomsSmall, albeit significant, decrements in lung function in normal children may have little clinical significance, but there is good
Figure 2 airway macrophage from a healthy child, showing carbon areas
(phagocytosed pm10). macrophages were obtained by induced sputum,
stained with diff-Quik and imaged under oil-immersion lens.
0 © 2008 elsevier ltd. all rights reserved.

SympoSium: Social paediatricS
evidence from cohort and panel studies that air pollution is asso-ciated with an increased prevalence of respiratory symptoms.
Weiland and Forastiere23 summarized the evidence available in 2005 for asthma and allergies in children for the WHO. They concluded that sufficient evidence links an increased incidence of the following to air pollution: • cough • asthma exacerbations • deficits in lung function.There is very little evidence for increased incidence or prevalence of asthma and air pollution in general.
The authors recently reported a higher prevalence of cough without cold in a cohort of 4400 preschool children,24 with increased exposure to locally generated PM pollution (mainly from roads). In a study carried out in the Netherlands, wheeze- and doctor-diagnosed asthma were significantly more in school-children living 100 m from the freeway.25 In a UK study, children living within 150 m from the main road had increasing risk of wheeze (odds ratio 1.08), with most risk localized to those living within 90 m of a main road.26 The adverse effect of living near a road has not been consistently found.27,28 One explanation for these inconsistent data is that distance from a road is an imper-fect maker of exposure to locally generated air pollution, particu-larly in school age children, who spend significant time away from the home address. Studies combining modelled exposure to locally generated air pollutants at home and at school addresses with measured background levels are urgently needed.
As discussed above, another way of linking exposure to health effects is to look for an association between daily (or another time period) changes in the background level of air pollution and changes in a health-related variable. Daily fluctuations of back-ground levels of PM10 were associated with: • acute respiratory hospital admissions in children • absences from school and kindergarten • increased use of asthma medications.29
Brauer et al30 assessed associations of traffic-related air pollu-tion and development of respiratory symptoms in first four years of life in a birth cohort (n = 4000). Elevated adjusted odds ratios per interquartile pollution range for wheeze (OR 1.2 for soot) and doctor-diagnosed asthma (1.3) were found.
As a part of Children’s Health Study in California, 265 out of 3535 children followed up for five years reported new diagnosis of asthma.31 In communities with high concentrations of O3, the relative risk of developing asthma in children playing three or more sports was 3.3 (95% CI 1.9 to 5.8), compared with children playing no sports.
Lee et al32 correlated hospital admissions for asthma in chil-dren ≤18 years of age with daily mean concentration of PM10, PM2.5, NO2, SO2 and O3. There was a significant increase in asthma admission rate with change of these pollutants except for SO2.
In summary, even with imperfect measures of individual exposure, fossil fuel pollutants are associated with increased respiratory symptoms in children.
InfectionThe effect of air pollution on vulnerability to bacterial and viral infections has received less attention.
In a study based in Rome, increased hospital admissions (4%) due to acute respiratory infections in children aged 0–14 years
paediatricS aNd cHild HealtH 18:5 24
were found to be associated with NO2;33 a recent study from Aus-tralia and New Zealand reported that increased hospital admis-sions for pneumonia and acute bronchitis in children aged less than 4 years are associated with high levels of NO2 and PM2.5.34
The most convincing data come from studies in the develop-ing world, where young children are exposed to very high levels of PM and gases from the burning of ‘crude’ fossil fuels (e.g. coal) and biomass (e.g. wood, dung). Indoor smoke is estimated to cause two million excess deaths per year,35 a major propor-tion of these in those aged less than 5 years.36 These deaths are predominately due to smoke-induced vulnerability to acute lower respiratory tract infection.37 Indoor smoke may act directly by attenuating innate immune defences to bacterial pathogens, or indirectly by decreasing anti-viral defences (which in turn increases vulnerability to secondary bacterial infection).
Current challenges
Some of the challenges of epidemiological studies are related to exposure measurement and multiple confounding factors. Expo-sure depends on activity patterns, which can vary significantly between individuals living in same geographical area. Indoor pollutants must be considered when interpreting data. Because of ethical considerations, controlled exposure studies cannot be conducted in children, and biomarkers of exposure are needed. These will come from a more detailed understanding of the cel-lular and molecular mechanisms for the disparate pollutant-induced health effects seen in children.
Future research
The mechanism of increased susceptibility in children (particu-larly those with chronic respiratory conditions such as asthma and cystic fibrosis) must be understood. A complete understand-ing of the mechanism(s) for air pollution-induced health effects at the cellular level would strengthen the epidemiological asso-ciations (and possibly guide policy makers). The newer methods of assessing airway inflammation non-invasively (e.g. induced sputum, exhaled NO, exhaled breath condensate) may provide new insights into this mechanism.
For the more esoteric associations (e.g. PM10 and low birth weight), paediatricians should convince their obstetric colleagues that research into air pollution is important. Examples of joint investigations would be a panel study to assess the association between: • daily changes in placental blood flow and background PM10
• birth weight and living near a main road.The mechanism of impaired pulmonary host defence mecha-
nisms must be understood because acute respiratory infections are associated with biomass exposure.38 Many of the components of biomass- and fossil fuel-derived air pollution are similar, and insights obtained in the developing world may be applicable to the developed world.
For clinicians
Clinicians should inform children and parents of the possible adverse effects of air pollution. Parents, particularly of children with chronic respiratory conditions, should access local air
1 © 2008 elsevier ltd. all rights reserved.
SympoSium: Social paediatricS
quality websites (e.g. DEFRA in the UK (www.airquality.co.uk/archive/index.php) for warnings of high levels, and avoid out-door activities during those hours. Whether increasing treatment (e.g. increasing doses of formoterol/budesonide combination) in response to these warnings prevents attacks is unknown. His-tory of possible sources of air pollution (e.g. busy road, factories) should be included in consultations for asthma and other respira-tory illnesses. Increasing awareness among parents and children will increase co-operation and participation in future research. ◆
REFEREnCES
1 Harrison rm, yin J. particulate matter in the atmosphere: which
particle properties are important for its effects on health? Sci Total
Environ 2000; 249: 85–101.
2 Harrison rm, Jones m. the chemical composition of airborne particles
in the uK atmosphere. Science Total Environ 1995; 168: 195–214.
3 ackerman-liebrich u, rapp r. oxides of nitrogen and sulfur.
epidemiological effects of oxides of nitrogen, especially No2. in:
Holgate S, Samet Jm, Koren HS, maynard rl, eds. air pollution and
health. london: academic press, 1999.
4 Harrison rm. Geographical, atmospheric and ground determinants of
air pollution. measurements of concentrations of air pollutants. in:
Holgate S, Samet Jm, Koren HS, maynard rl, eds. air pollution and
health. london: academic press, 1999.
5 Kelly FJ. oxidative stress: its role in air pollution and adverse health
effects. Occup Environ Med 2003; 60: 612–16.
6 Bobak m. outdoor air pollution, low birth weight, and prematurity.
Environ Health Perspect 2000; 108: 173–176.
7 chen l, yang W, Jennison Bl, Goodrich a, omaye St. air pollution
and birth weight in northern Nevada, 1991–1999. Inhal Toxicol
2002; 14: 141–157.
8 lee Be, Ha eH, park HS, et al. exposure to air pollution during
different gestational phases contributes to risks of low birth weight.
Hum Reprod 2003; 18: 638–43.
9 Xu X, ding H, Wang X. acute effects of total suspended particles
and sulfur dioxides on preterm delivery: a community-based cohort
study. Arch Environ Health 1995; 50: 407–15.
10 mannes t, Jalaludin B, morgan G, et al. impact of ambient air
pollution on birth weight in Sydney, australia. Occup Environ Med
2005; 62: 524–30.
11 Jalaludin B, mannes t, morgan G, et al. impact of ambient air
pollution on gestational age is modified by season in Sydney,
australia. Environ Health 2007; 6: 16.
12 mills Nl, tornqvist H, Gonzalez mc, et al. ischemic and thrombotic
effects of dilute diesel-exhaust inhalation in men with coronary
heart disease. N Engl J Med 2007; 357: 1075–82.
13 Fedulov aV, leme a, yang Z, et al. pulmonary exposure to particles
during pregnancy causes increased neonatal asthma susceptibility.
Am J Respir Cell Mol Biol 2008; 38: 57–67.
14 Gauderman WJ, avol e, Gilliland F, et al. the effect of air pollution
on lung development from 10 to 18 years of age. N Engl J Med
2004; 351: 1057–67.
15 Horak Jr F, Studnicka m, Gartner c, et al. particulate matter and
lung function growth in children: a 3-yr follow-up study in austrian
schoolchildren. Eur Respir J 2002; 19: 838–45.
16 Jedrychowski W, Flak e, mroz e. the adverse effect of low levels of
ambient air pollutants on lung function growth in preadolescent
children. Environ Health Perspect 1999; 107: 669–74.
paediatricS aNd cHild HealtH 18:5 2
17 Brunekreef B, Hoek G. the relationship between low-level air
pollution exposure and short-term changes in lung function in dutch
children. J Expo Anal Environ Epidemiol 1993; 3(suppl 1): 117–128.
18 Ward dJ, ayres JG. particulate air pollution and panel studies in
children: a systematic review. Occup Environ Med 2004; 61: e13.
19 rojas-martinez r, perez-padilla r, olaiz-Fernandez G, et al. lung
function growth in children with long-term exposure to air pollutants
in mexico city. Am J Respir Crit Care Med 2007; 176: 377–84.
20 Kulkarni N, pierse N, rushton l, Grigg J. carbon in airway
macrophages and lung function in children. N Engl J Med 2006;
355: 21–30.
21 Gauderman WJ, Vora H, mcconnell r, et al. effect of exposure to
traffic on lung development from 10 to 18 years of age: a cohort
study. Lancet 2007; 369: 571–7.
22 avol el, Gauderman WJ, tan Sm, london SJ, peters Jm. respiratory
effects of relocating to areas of differing air pollution levels. Am J
Respir Crit Care Med 2001; 164: 2067–72.
23 World Health organisation. effects of air pollution on children’s
health and development—a review of the evidence. Geneva: WHo,
2005.
24 pierse N, rushton l, Harris rS, et al. locally generated particulate
pollution and respiratory symptoms in young children. Thorax 2006;
61: 216–20.
25 van Vliet p, Knape m, de Hartog J, et al. motor vehicle exhaust
and chronic respiratory symptoms in children living near freeways.
Environmental Research 1997; 74: 122–32.
26 Venn aJ, lewis Sa, cooper m, Hubbard r, Britton J. living near a
main road and the risk of wheezing illness in children. Am J Respir
Crit Care Med 2001; 164: 2177–80.
27 livingstone ae, Shaddick G, Grundy c, elliott p. do people living
near inner city main roads have more asthma needing treatment?
case-control study. BMJ 1996; 312: 676–7.
28 Wilkinson p, elliott p, Grundy c, et al. case-control study of hospital
admission with asthma in children aged 5–14 years: relation with
road traffic in north west london. Thorax 1999; 54: 1070–4.
29 american thoracic Society. Health effects of outdoor air pollution.
committee of the environmental and occupational Health assembly
of the american thoracic Society. Am J Respir Crit Care Med 1996;
153: 3–50.
30 Brauer m, Hoek G, Smit Ha, et al. air pollution and development of
asthma, allergy and infections in a birth cohort. Eur Respir J 2007;
29: 879–88.
31 mcconnell r, Berhane K, Gilliland F, et al. asthma in exercising
children exposed to ozone: a cohort study. Lancet 2002; 359: 386–91.
32 lee Sl, Wong WHS, lau yl. association between air pollution and
asthma admission among children in Hong Kong. Clin & Exp Aller
2006; 36: 1138–46.
33 Fusco d, Forastiere F, michelozzi p, et al. air pollution and hospital
admissions for respiratory conditions in rome, italy. Eur Respir J
2001; 17: 1143–50.
34 Barnett aG, Williams Gm, Schwartz J, et al. air pollution and child
respiratory health: a case-crossover study in australia and New
Zealand. Am J Respir Crit Care Med 2005; 171: 1272–8.
35 Bruce N, perez-padilla r, albalak r. indoor air pollution in
developing countries: a major environmental and public health
challenge. Bull World Health Organ 2000; 78: 1078–92.
36 Smith Kr, Samet Jm, romieu i, Bruce N. indoor air pollution in
developing countries and acute lower respiratory infections in
children. Thorax 2000; 55: 518–32.
42 © 2008 elsevier ltd. all rights reserved.

SympoSium: Social paediatricS
37 ezzati m, Kammen d. indoor air pollution from biomass combustion
and acute respiratory infections in Kenya: an exposure-response
study. Lancet 2001; 358: 619–24.
38 Grigg J. effect of biomass smoke on pulmonary host defence
mechanisms. Paediatric Respiratory Reviews 2007; 8: 287–91.
Practice points
• children (particularly those with chronic respiratory
conditions) are more susceptible to adverse effects of air
pollution
paediatricS aNd cHild HealtH 18:5 24
• traffic and industry are major sources of air pollution in the
developed world
• exposure to biomass smoke is a leading cause of mortality
and morbidity in children in developing world
• reduction in lung function growth is a well-documented
adverse effect
• air pollution is associated with exacerbation of asthma
• routine history-taking for respiratory conditions should
include possible sources of air pollution in or near the home
or school
• Further research to understand the cellular mechanisms of
adverse effects in children is required
3 © 2008 elsevier ltd. all rights reserved.