educational slide set hpsc october 2014 antimicrobial resistant enterobacteriaceae
TRANSCRIPT

Educational Slide Set HPSC
October 2014
Antimicrobial Resistant Enterobacteriaceae

Presentation Outline
1. What are Enterobacteriaceae?2. What do we mean by the term ‘antimicrobial resistant
Enterobacteriaceae’?3. What do we know about antimicrobial resistant
Enterobacteriaceae in Ireland & Europe?4. Why is this important?5. How can we help prevent the spread of antimicrobial
resistant Enterobacteriaceae?
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

What are Enterobacteriaceae?• A collective term used to describe many of the
different types of bacteria, which are normally found in the gut/bowel/enteric tract:– E. coli– Klebsiella spp.– Proteus mirabilis– Enterobacter cloacae
• Their presence mostly represents a state of ‘carriage’/colonisation’
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

Enterobacteriaceae• In a vulnerable person, they can cause infection: e.g., presence of
wound, invasive device, critical illness, immunocompromise• Common causes of community-acquired and healthcare-associated
infections (HCAI):– Urinary tract infections (UTI) – cystitis, pyelonephritis– Wound and surgical site infections– Healthcare-associated pneumonia– Bloodstream infections (BSI)– Septic shock
• Potentially fatal infections in vulnerable patients
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)
How do we treat infections caused by Enterobacteriaceae?
• Sometimes the immune system can’t control infection on its own: ANTIMICROBIALS may be needed to kill the Enterobacteriaceae
• Three major antimicrobial classes are commonly used for treating infections caused by Enterobacteriaceae:• Beta (β) lactams• Fluoroquinolones – ciprofloxacin, ofloxacin• Aminoglycosides – gentamicin, tobramycin, amikacin
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

What are β lactams?• Penicillin• Amoxicillin• Flucloxacillin• Piperacillin-tazobactam• Co-amoxiclav
• Cefuroxime3rd generationcephalosporins:• Cefotaxime• Ceftriaxone• Ceftazidime
• Aztreonam(acts on Gram-negativeaerobic bacteria only)
• Meropenem• Ertapenem
β lactams bind to proteins on the bacterial cell wall and kill bacteria by disrupting cell wall synthesis
β lactam ring
β lactam ring
β lactam ring
β lactam ring
• A large family of antimicrobials sharing the common property of a β lactam ring
• Over the years, more sophisticated types of β lactams developed to overcome bacteria developing resistance to each type
• No new types of β lactams developed in recent decades and no new types expected to be available in the next decade
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

What are carbapenems?
• A group of powerful “last resort” β lactam antimicrobials (e.g., meropenem)
• Carbapenems must be reserved for treatment of: – Severe infection in critically ill patients – Infections caused by Enterobacteriaceae with
resistance to other antimicrobial classes• Carbapenems should generally only be prescribed
on the advice of an infection specialist: clinical microbiologist or infectious diseases physician
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

How do Enterobacteriaceae become resistant to β lactams?
• Enterobacteriaceae acquire the gene to produce enzymes ‘β lactamases’ which destroy β lactam antimicrobials
• The more powerful the β lactamase enzyme, the more types of β lactam antimicrobial it can destroy
Penicillinases
Extended-spectrum β lactamases
Carbapenemases
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)
What are ESBLs?• Extended Spectrum β Lactamases• Enzymes produced by Enterobacteriaceae, which
destroy most β lactams, including 3rd generation cephalosporins
• The remaining β lactam which is reliable for treating ESBL infection is a carbapenem (e.g., meropenem)
• The gene for making ESBLs is carried on mobile genes (plasmids), which are easily swapped between different types of Enterobacteriaceae
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

What are carbapenemases?
• Even more broadly-acting enzymes produced by Enterobacteriaceae, which destroy VIRTUALLY ALL β lactams, including carbapenems
• This leaves few antimicrobials available to treat infection caused by these bacteria
• The gene for making carbapenemases is also easily swapped between different types of Enterobacteriaceae
• Also known as carbapenemase-producing or carbapenem resistant Enterobacteriaceae ‘CRE’
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

What do we mean by multi-drug resistant (MDR) Enterobacteriaceae?
• Term used when Enterobacteriaceae have become resistant to at least two different antimicrobial classes:– Resistant to β lactams mainly due to production of either ESBLs
and/or carbapenemasesAND
– Resistant to a fluoroquinolone (e.g., ciprofloxacin)AND/OR
– Resistant to an aminoglycoside (e.g., gentamicin)• There are extremely limited treatment options for
infection caused by MDR-Enterobacteriaceae
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

AGENT RESULT
Amoxicillin RESISTANT
Co-amoxiclav RESISTANT
Cefuroxime RESISTANT
Cefotaxime RESISTANT
Ceftazidime RESISTANT
Piperacillin/tazobactam RESISTANT
Aztreonam RESISTANT
Meropenem RESISTANT
Ciprofloxacin RESISTANT
Gentamicin SUSCEPTIBLE
Tobramycin RESISTANT
Amikacin RESISTANT
Tigecycline RESISTANT
Colistin SUSCEPTIBLE
What does this mean for a patient with infection?• Microbiology laboratory report for
a patient who developed a wound infection caused by a MDR-Enterobacteriaceae, called Klebsiella pneumoniae
Resistant to all the β lactams: including 3rd generationcephalosporins (ESBL production) & carbapenem(carbapenemase production = CRE)
ALSO resistant to a fluoroquinolone – ciprofloxacin
ALSO resistant to some aminoglycosides – tobramycin & amikacin
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

What does this mean for the patient?• Infection caused by antimicrobial resistant Enterobacteriaceae (e.g.,
ESBL or CRE) more likely to result in patient harm or death than if caused by antimicrobial susceptible bacteria
• Why?– Patients with ESBL/CRE infections may already be very ill or
vulnerable to infection– There could be a delay in detecting that infection is caused by
ESBLs or CRE = delay in starting patient on optimal antimicrobial treatment
– Infections more difficult to treat because very few suitable options available – risk of toxic side effects with some drugs
– Longer hospital stay, longer recovery time, delayed return to normal life/work, increased cost to patient & healthcare system
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)
What do we know about antimicrobial resistant Enterobacteriaceae in Ireland & Europe?
• Information on one of the most significant infection types; bloodstream infection (BSI) is collected by every microbiology laboratory & reported to the HPSC
• The two commonest types of Enterobacteriaceae that cause BSI are:– E. coli– Klebsiella pneumoniae
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

BSI caused by Enterobacteriaceae: Ireland
2010 2011 2012 2013
Number of cases of E. coli BSI 2170 2210 2449 2530
% of E. coli BSI that were ESBL positive 6.1 7.5 8.6 10.5
% of E. coli BSI that were MDR 11.7 13 13.5 14.8
Number of cases of Klebsiella pneumoniae BSI
326 312 345 326
% of K. pneumoniae BSI that were ESBL positive
5 5.6 8.8 18.4
% of K. pneumoniae BSI that were MDR 2.2 3.2 5.2 11.7
Source: HPSC EARS-Net data
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

Carbapenemase producing Enterobacteriaceae (CPE or CRE) in Ireland
• 2009: CRE first detected in Ireland• March 2011: Laboratory detection of CRE became
notifiable• September 2011: Invasive CRE infection added to updated
Notifiable Infectious Disease Regulations• 2011: CRE enhanced surveillance scheme launched• 2012: National Carbapenemase Producing
Enterobacteriaceae Reference Laboratory Service (CPEaRLS) established at GUH
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

CRE in Ireland
Number of confirmed carbapenemase producing (CRE) cases
Data source
2011 39 HPSC enhanced CRE surveillance
2012 32 HPSC enhanced CRE surveillance
2013 48 CPEaRLS report
Data represents reference laboratory-confirmed cases of carbapenemase-producingEnterobacteriaceae (CRE) from clinical (sterile and non-sterile sites)
& screening (rectal swab or faeces) specimens
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

What is the surveillance data telling us?• Monitoring antimicrobial resistance in Enterobacteriaceae
in Ireland and Europe, shows a worrying increase, particularly in the past five years
• ESBL, CRE and multi-drug resistant (MDR) Enterobacteriaceae are detected with increasing frequency in acute hospitals and long-term care facilities across Ireland
• Patients and residents are frequently transferred between these settings
• Antimicrobial use is a major driver of antimicrobial resistance
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

Do we use many antimicrobials in Ireland?• 80% of antimicrobial use is in
the community setting (primary & long-term care) and use is increasing
• Residents of Irish long-term care facilities three times more likely to be prescribed an antimicrobial than their European counterparts
Sources: HPSC Antimicrobial Consumption Surveillance & ECDC HALT PPS 2010 & 2013
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)
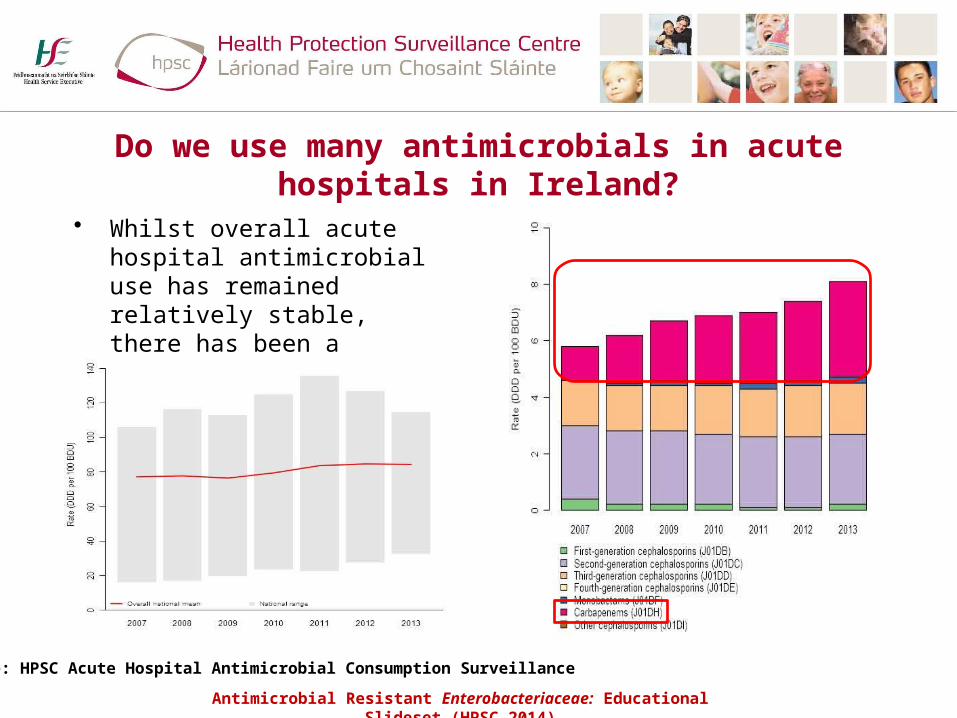
Do we use many antimicrobials in acute hospitals in Ireland?
• Whilst overall acute hospital antimicrobial use has remained relatively stable, there has been a significant increase in carbapenem use in Ireland since 2007
Source: HPSC Acute Hospital Antimicrobial Consumption Surveillance
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)
How do antimicrobial resistant Enterobacteriaceae spread?
• Patient-to-patient OR resident-to-resident– Via contaminated environment, shared toilet facilities– Via hands of healthcare workers, patients/residents and visitors,
where hand hygiene opportunities have not been taken• Hospital-to-hospital OR hospital-to-long-term care facility
– Direct patient/resident transfer– Patients/residents attending more than one hospital
• Country-to-country– Patients repatriated to Irish hospital following illness abroad– Health tourism– International travel – potential to acquire organisms via
contaminated water or food
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

How would we know a person is carrying antimicrobial resistant Enterobacteriaceae?
• Via a positive microbiology result:– Specimen taken to investigate suspected infection (e.g., urine, blood
cultures, sputum, swab etc.)– Specimen taken to screen/check for bowel carriage (e.g., rectal swab or
faeces)– Patient already known to be a carrier from a result obtained during a
prior attendance OR from testing in another healthcare facility• Without a positive microbiology result, we would not know whether
a person is a carrier: – Often asymptomatic bowel carriage and less often implicated as a cause
of infection– Bowel is laden with Enterobacteriaceae: no proven method to eradicate
bowel carriage and carriage often indefinite
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

Who might be ‘at-risk’ of carrying resistant Enterobacteriaceae?
1. Patient with prior history of carriage or infection2. Patient who has been in close contact with a patient
diagnosed as being a carrier (e.g., sharing a room or toilet)
3. Patient transferred back to Ireland from foreign healthcare facility (includes Northern Ireland)
4. Patient transferred from another healthcare facility in Ireland: acute hospital or long term care facility
5. Patient admitted to a specialist care area: critical care unit, haematology, oncology, transplant ward
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

How can we help prevent spread of antimicrobial resistant Enterobacteriaceae?
1. Consistent hand hygiene during patient/resident care by all healthcare professionals
2. Look after wounds and medical devices (e.g., drips, catheters) and remove devices as soon as no longer required
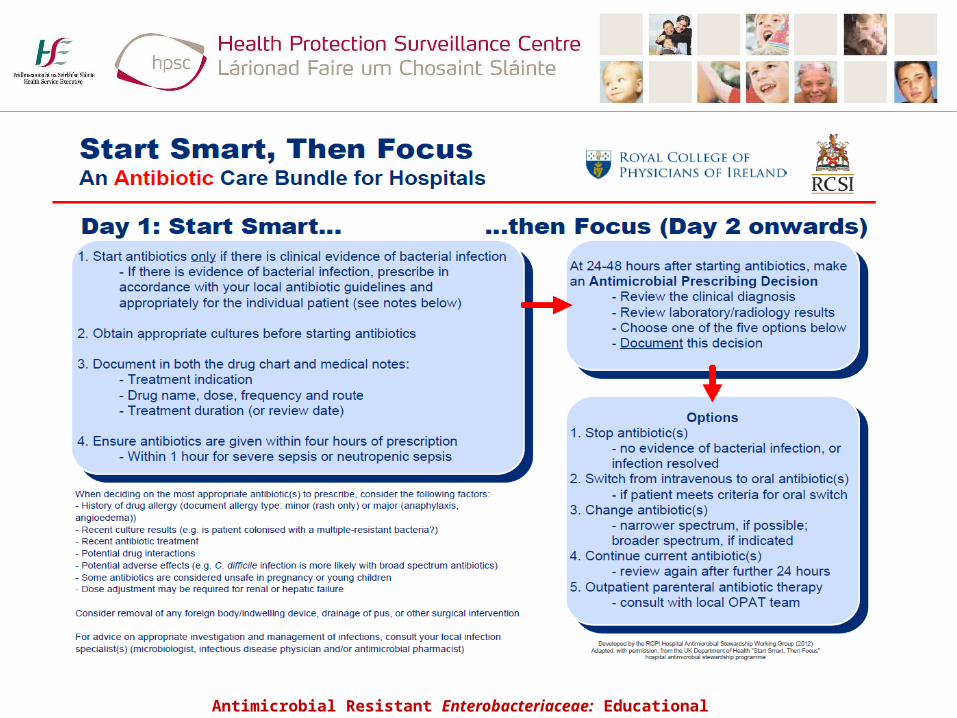
3. Prudent antimicrobial prescribing:– Follow local prescribing guidelines & use the antibiotic care
bundle – right drug, dose, duration– Seek advice from clinical microbiologist/ID physician before
prescribing carbapenems
1,2 & 3 FOR EVERY PATIENT/RESIDENT – EVERY TIMEAntimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

How can we help prevent spread of antimicrobial resistant Enterobacteriaceae?
1. Patients/residents who are already known to be carriers should be cared for using appropriate transmission-based precautions
2. Ensure good communication when patients/residents already known to be carriers are being transferred between clinical areas and between healthcare facilities
3. Use healthcare record alerts and electronic alerts to help staff identify patients/residents who are known to be carriers when they return to the hospital/long-term care facility
4. In the acute hospital setting, ‘at-risk’ patients for bowel carriage should be identified and cared for using appropriate transmission-based precautions, with use of screening specimens to detect bowel carriage, as per national and local laboratory testing guidelines
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)

Thank you for your attentionFurther information available on HPSC website:
Antimicrobial Resistant Enterobacteriaceae: Educational Slideset (HPSC 2014)