editorial board - bosnian journal of basic … · editorial board editorial in chief: zuli} irfan...
TRANSCRIPT

2 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
EDITORIAL BOARD
Editorial in chief:Zuli} Irfan
Deputy editor:Selak Ivan
Secretary:Emina Naka{-I}indi}
Technical editor:Selvi} Faruk
Members:Dilberovi} FarukHad`ovi} SafetJadri}-Winterhalter MiraKulenovi} HuseinMihaljevi} MilenaNikolin BrankoPleho AmirPotkonjak DubravkaSinanovi} OsmanSu{i} Husein[alaka Abdul-Umid
ADVISORY BOARD:
Muji} Muzafer, PresidentBerberovi} LjubomirGruji}-Vasi} JelaHad`ovi} SabiraHamamd`i} MuhidinKonjhod`i} FarukLoga SlobodanMulabegovi} Ned`adNikulin AleksandarPuji} Zdravko
Contents:
EDITORIAL . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
ARTIFICIAL CREATION OF GENETICALLYIDENTICAL INDIVIDUALS - REPRODUCTIVE CLONING . . . .5
(Ljubomir Berberovi})
OBSERVING OF THE ASYMMETRY OFHIPPOCAMPAL FORMATION ON PATIENTSWITH COMPLEX PARTIAL ATTACKS . . . . . . . . . . . . . . . . . . .18
(Aida Sara~ - Had`ihalilovi}, Faruk Dilberovi})
TYPE IV COLLAGEN IMMUNOREACTIVITY OFBASEMENT MEMBRANE ININFLAMMATORY-REGENERATIVE AND DYSPLASTICLESIONS OF THE FLAT COLONIC MUCOSA . . . . . . . . . . . . .30
Svjetlana Radovi}, Ivan Selak, Mirsad Babi},
@eljka Kne`evi}, Zora Vukobrat-Bijedi}
PROXIMAL CONVOLUTED TUBULES OF THERATS KIDNEY - A STEREOLOGICAL ANALYSIS . . . . . . . . . .36
Selma Ali~elebi}
DETERMINATION OF THE EXTRACTIONEFFICIENCY OF POLYCYCLIC AROMATICHYDROCARBONS FROM AIRBORNEPARTICULATE MATTER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .40
Miroslav [ober, Branko Nikolin
SIMULTANEOUS ABUSE OF DIFFERENT PSYCHOACTIVESUBSTANCES AMONG ADOLESCENTS . . . . . . . . . . . . . . . . .44
Amira Red`i}, Ifeta Li~anin, Sanja Kro{njar
CO-RELATION BETWEEN RISK FACTORS OFFALLS DOWN AND THE BERG BALANCESCALE IN ELDERLY PEOPLE (THIRD AGE) . . . . . . . . . . . . . .50
Avdiæ Dijana, Škrbo Armin
DOSSIER FOR MARKETING AUTHORIZATIONIN THE EUROPEAN UNION . . . . . . . . . . . . . . . . . . . . . . . . . . .57
Maida Todi}
EXPERIMENTAL DESIGN - BASIC CONSIDERATIONS . . . . .62
Edina Vrani}
INSTRUCTIONS FOR PREPARATION OF MANUSCRIPTS . . .65
UDRU@ENJE BAZI^NIHMEDICINSKIH ZNANOSTIFBIH SARAJEVOASSOCIATION OF BASIC MED-ICAL SCIENCES FBIH SARAJEVO
Predsjednik: Prof. Dr. Irfan Zuli}
Adresa redakcije:Glavni i odgovorni urednik:Prof. Dr. Irfan Zuli}Medicinski fakultetInstitut za farmakologiju^ekalu{a 90 SarajevoTel./Fax: 441 813, 441 895

3Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Editorial
Topical issues in the Association of Basic Medical Sciences
Since December 2002, when the latest number of the Bosnian Journal of Basic Medical Sciences was poublished tillthis day, Symposium "Scientific, ethical and religious dilemmas over the status of human cloning" has been held - thefield which attracts intensively the attention of scientists, and producing plenty of issues that have become significantnot only for scientists but for the modern man too.
Undoubtedly, achievements in cloning, genetic engineering and molecular biology in general often precede the corre-sponding social standpoints. Besides, the field of human cloning contains controversies and significant conceptual con-fusions with respect to implication of results and application of technologies of reproductive and therapeutic cloning.
In the field of medicine cloning methods should serve for solving specific health issues, but today it has turned to bethe issue of cloning of individuals. This interferes with the some significant possibilities of therapeutic and repro-ductive medicine.
As these issues arouse huge interest between scientists, so that we considered appropriate to include in every follow-ing edition one of the overview article given at scientific symposium held on 15 February, the PROGRAM of whichwe are presenting to you herein.
Sarajevo, 15 February 2003Scientific symposium"Scientific, ethical and religious dilemmas over the status of human embryo and its cloning"
09:00 - 09:30 a.m. Opening of symposium and introductory remarks. Cloning-dilemmas, third millennium and where to go on. Doc. Faris Gavrankapetanovi}, M.D.
09:30 - 09:55 a.m. Cloning as a field of genetic engineeringAcademician Ljubomir Berberovi}
09:55 - 10:30 a.m. Pros and cons cloning Ph.D. Kre{imir Paveli}, M.D.10:30 - 11:00 a.m. Possibility of monitoring the earliest developmental phases of human embryo with 3-D and
4-D ultrasounds. Ph.D. Asim Kurjak, M.D.11:00 - 11:10 a.m. Break11:00 - 11:30 a.m. Functional genomics in prenatal diagnostics and therapy
Ph.D. Kre{imir Paveli}, M.D.11:30 - 11:50 a.m. Legal, ethical, scientific and religious dilemmas over the status of human embryo and its
characteristics Ph.D. Asim Kurjak, M.D.11:50 - 12:10 p.m. Cloning - philosophic, ethical and religious considerations Ph.D. Enes Kari}, M.D.12:10 - 1:10 p.m. Discussion
Editor in chiefProfessor Irfan Zuli}, Ph.D., M.D.
Sarajevo, III 2003.
UDRU@ENJE BAZI^NIH MEDICINSKIH ZNANOSTI FEDERACIJE BOSNE I HERCEGOVINEASSOCIATION OF BASIC MEDICAL SCIENCES OF FEDERATION OF BOSNIA & HERZEGOVINA

4 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.

During the second half of the previous century, biologistswere continuously searching for the answers to the ques-tions about the creation of genetically identical individu-als. From the very first ideas (Spemann, 1938) and theearly reports on the attempts and successes in the repro-ductive cloning (Briggs and King, 1952; Stewart et al.,1958) to the recent news about the first cloned baby birth(published informally at the end of 2002), that topic gath-ered a significant scientific and non-scientific attention.All assertions about human cloning resounded as a sen-sation and made a particular public unrest, even thoughit was in fact an operation based on the existence ofalready well known scientific postulations, theories andexperimental results. In spite of whether human individ-uals were cloned or not (many scientists expressed seri-ous reserves regarding the above mentioned news), awider public interest in cloning, its importance and pro-cedures and a new technology practical possibilitiesincreased significantly.
Clones and cloning
Clones and cloning are words with numerous differentmeanings in biological terminology. There are a lot ofambiguities, inconsistencies and obscurities in theBosnian language in the usage of words "clone andcloning"
Term "clone" primarily refers to the group of geneticallyidentical individuals (Bains, 1998), that is a group ofindividuals with the same hereditary basis. In the nature,such individuals originate from a specific type of repro-duction - reproductive cloning. The primary significationof cloning is the creation of such individuals and groups.However, there is also the clonal reproduction of cells inthe organism. The elementary natural way of the clonalsystem creation is an equal (equational, homeo-type) celldivision - mitosis in eukaryotes or binary fusion inprokaryotes. The groups of genetically identical biologi-cal systems (cells or organisms) originating from thesame progenitor arise throughout processes of mitosisand binary fusion (King and Stansfield, 1997). Differentforms of "vegetative reproduction" (when a completenew organisms originate from the multi-cellular bodyfractions, mostly plants) are also representing a sort ofcloning.
In Bosnian language, there is a need to distinguish themeaning of "klona" and "klon". "Klona" (feminine) inBosnian refers to a natural group of live beings with onlyone common progenitor and with the equal individualgenetic material, while "klon" (masculine) is pertainingto the individual biological systems originating from thecloning process (clonal reproduction).
Clonal reproduction is not only a matter of reproductionof living systems, but also it refers to the informationalmacromolecules, especially to DNA (deoxyribonucleicacid). Equiproductivity (a capability for the identicalreproduction or duplication) of DNA molecules is in facta basis of the equiproductivity of supra-molecular struc-tures in all biological systems (e.g. chromosomes), andof the whole biological systems of different organisingand complexity levels (from cells to organisms).Identical reproduction, natural or artificial, is based onthe auto-replication of hereditary molecules - DNA mol-ecules.
Thanks to the enormous technical progress in the genemanipulating, that is, DNA molecule manipulating("Genetic Engineering"), it is possible to create DNAsequences replications in any desired amounts. The mosteffective technology is the so called polymerase chainreaction - PCR, which was shortly after its discovery(Mullis and Falcona, 1987) introduced into the world-wide laboratory use. The advantage of PCR procedure isits potential to provide million and milliard replicationsof the chosen DNA fragment out of the minimal initialamounts in a short time (Mullis, 1990). Term "clonedDNA" refers to the DNA fragments that are passivelyreproduced in the receptor system and incorporated in avector ("travelling DNA", King and Stansfield, 1997).Biological systems may multiply specifically preparedforeign DNA molecules, when incorporated in the differ-ent "DNA carriers" - vectors.
Types of cloning
From the expert point of view, the most precise definitionof term "cloning" comprises all procedures pertaining tothe artificial, identical reproduction of the biologicalstructures (systems), from biological macromolecules tosupra-molecular cellular structures, complete cells, cel-lular lines (tissues) and finally the whole organisms.
Artificial creation of geneticallyidentical individuals - reproductive cloning(Review Article)
Ljubomir Berberovi}Faculty of Science, University of Sarajevo
5Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.

6 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
It is correct to assume that artificial cloning experimentsare a form of genetic engineering, a discipline of scien-tific research that comprises all direct manipulating pro-cedures dealing with the hereditary material, that is,genes and biological structures comprising the genes(Berberovi}, 2002). Basic genetic engineering principlesand types are frequently aligned according to the amountof manipulated genetic material (table 1), in accordancewith a classical, standard and well established mutationclassification (Ayala and Kiger, 1984).
The simplest and the most popular typology of the artifi-cial cloning operations is based on what is the systemwhich is the object of manipulation, or which is the aimof the clonal reproduction. Therefore, it is possible todistinguish cloning on the molecular level (cloning ofgenes or DNA sequences), cloning on the cellular level(cloning of the entire basic biological systems, i. e. cells),and cloning on the organism level (creation of the com-plete, whole multi-cellular organisms). This typology is,in fact, based on the organisation levels of manipulatedbiological structures and the target cloning systems, andit significantly corresponds to the basic types of geneticengineering systematisation (Table 1).
Cloning of the cells and organisms is most preciselydefined as a subfield of the genome engineering.Genome engineering encompasses operations dealingwith integral sets of chromosomes (genes). Genomeengineering can be divided into several different formsof the direct manipulation of the entire genomes (Table2), which are frequently connected with the parasexualindividual reproduction or maintenance and modificationof the cell cultures. Lately, interest is attracted by theexperiments in the somatic genomes cloning realm thatincludes all well known operations of the creation ofwhole organisms from the body cells genetic material.
General typology of the cloning forms may be based ondifferent principles and performed according to the dif-ferent criteria. As presented in the Table 3, a typology ispossible to distinguish primarily between cellular andorganism cloning (bearing in mind that genes or DNAmolecules might be purposely reproducible also, whatwould be called gene or molecular cloning). After thenews was spread in the public about the possibilities forthe clone creation by the usage of material of the humanorigin, a new cloning typology based on the particularprocedure aims was established (Table 4). Reproductivecloning is the cloning of organisms, a procedure carriedout with purpose to create genetically identical individu-als. Reparative (therapeutic) cloning is targeted towardsidentical reproduction of cells with strictly medical pur-poses of specific tissues and organs production (Cibelliet al., 2002).
A special form of the organism cloning or parasexualreproduction is a technique of the fragmentation ofembryo in early phase of its development (most often amorula phase). Embryo cells have totipotent sets ofgenes and can induce development of numerous geneti-cally identical embryos - i. e. monozygotic twins(Willandsen, 1979). This is a base of "embryo transfer"technique, which includes implanting of embryos to cho-sen "surrogate mother" (Moses, 1987). This techniquecan be practicably useful in cattle breeding and it is alsowidely used in experimental cloning procedures.Although some procedures of embryo transfer are neces-sary for genetic engineering cloning experiments, thecreation of individuals with identical hereditary basisthroughout embryo fragmentation does not belong(according to the accepted definition) to the field of thehereditary material direct manipulation. It would ratherbelong to the vegetative reproduction methods than tothe organism cloning as sector of genome engineering.
Biological theory oforganism cloning
Modern biological theory explains identical reproductionof biological systems, cells or organisms, through factthat each somatic cell is characterised by the totipoten-cy (omni potency) of its genetic material. Experimentshave confirmed that somatic genomes (if we neglect rel-atively rare somatic mutations) remained unaffected dur-ing the individual development (Alberts et al., 1994).Differentiation processes are based on the selective acti-vation and deactivation of the genes or groups of genes,but not on the material changing of their structure.
Theory of the genetic omnipotency of the somatic cellshas gradually maturated together with the deepening ofknowledge about processes involved in the cellular divi-sion. A long while ago it has been noticed that the essen-tial of equiproductivity of the cell, as a fundamental livesystem, is the equiproductivity of chromosomes -supramolecular structure containing the majority of thehereditary material or DNA molecules, as key carriers ofthe biological invariance ( duplication "non varietur";Monod, 1970). Mitosis as equal (equational, homeotype)cell division, characteristic for the somatic cells, denotesan accurate chromosome and gene duplication and pre-cise separation of the duplication products. Principally, itis how all somatic cells originate, and they all, regardlessof their own functional differentiation, contain the samediploid chromosomal set (n pairs of homologous chro-mosomes or 2n chromosomes - Chart 1).
Key position in the sexual reproduction processes isoccupied by another type of cellular division -meiosis(reductive, heterotype division). Meiosis is essential forthe creation of sexual cells - gametes. Gametes contain

7Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
haploid chromosomal set, n chromosomes. Gametesoriginate from the special line of the somatic, diploidcells - gametogonies. Gametogonial cells divide throughmeiosis, a division consisting of the one duplication fol-lowed by two chromosome separations (segregation, firstand second meiosis). Crucial moment of meiosis is thephenomenon of conjugation: pairs of homologous chro-mosomes of the diploid set fuse and form bivalents(tetrads). Thus, the chromosomal number is halved, sothat gametes, after the two anaphase separations oftetrads, contain single, haploid chromosomal set (see thecorresponding part of Chart 1). Fusion of two gametesduring the fertilisation process gives the first diploid cellof the new being - a zygote. After that, zygote is dividedthroughout serial of equal divisions to form all othersomatic cells - the whole multicellular organism.
Reproductive cloningbasic procedures
Three most important procedures in the artificial cloningexperiments are: (1) removal of the genetic material fromrecipient system, (2) donor genetic material isolation and(3) donor genetic material transfer (implantation) in therecipient system. Finally, after all the mentioned proce-dures, recipient remains without its own chromosomesand genes while it receives a complete foreign genome.Biological essentials of the cloning process with the cor-responding variants and adequate terminology is synthet-ically presented in Chart 1. All of the mentioned mainphases of the somatic genome cloning, together withsolutions (technical) that may differ in some singulari-ties, are presented in Chart 1. Oocyte, in the finale phase of its maturation or maturedoocyte, and embryo cell of early differentiation stages inthe embryonic development (from zygote to blastocyst)represent universal recipient systems in the organismcloning procedures. Starting operation in all of thealready performed cloning experiments of higher animals(reproductive cloning of the somatic genome) has beenenucleation of the recipient oocyte, in which, somatic cellnucleus (diploid chromosomal set - Chart 2) is to beimplanted. A method different from this one was per-formed during the very first cloning experiments on high-er plants with intention to present a possibility to "coax"single diploid cells of vegetative cup to develop into anintegral being, understanding special environment andspecific stimulations (Steward et al., 1958; Steward et al.,1958b). It is theoretically possible, of course, to performprocess of enucleation on the plant material, as well.
Enucleation (removal of the nucleus) may be performedin different ways, out of which, methods of high reputeare: (1) mechanical removal (microsurgical intervention)or (2) removal by ultraviolet radiation. Both techniqueswere validated and confirmed throughout cloning exper-
iments in amphibians (Briggs and King, 1952, Elsdale etal., 1960). The usage of laser technique is also pre-dictable. All established cloning experiments in mam-mals were performed by mechanical enucleation of therecipient system; only a few early animal cloning exper-iments were performed with UV light application(Elsdale et al., 1960). Cloning experiments withoutoocyte enucleation, i. e. with implantation of the foreigndiploid nucleus in the oocyte with the intact haploidnucleus, were not completely unsuccessful (Fischberg et.al, 1958). Nevertheless, this technique is not practicedany more.
An idea of oocyte enucleation with diploid nucleusimplantation as a possible experimental proof of the the-oretical postulate of somatic cell genetic materialomnipotency and a draft of the appropriate experimentwere published at the end of thirties of the previous cen-tury (Spemann, 1938). Subsequent molecular-geneticresearches explained in details somatic cell omnipotencyphenomenon, providing a full theoretical basis for thesomatic genome cloning.
Hereditary material for implantation process is takenfrom the different tissue donor cells, embryonic or adult,which were previously sustained and monitored in theculture. Different types of donor tissues were used for thereproductive cloning experiments in mammals (Table 5).
Removal of the donor cell nucleus is performed mechan-ically (by micropipettes). This microsurgical procedure isvery similar to the process of enucleation. Occasionally,dissected parts of protoplasm with metaphase chromo-somes were used for the transfer. It is considered thatsuch procedure improve the prospects for the successfulexperiment because it excludes donor cytoplasmic fac-tors that might affect donor chromatin reprogramming(Prather, 2000).The integration of donor genetic material with enucleat-ed oocyte is done by microinjection or fusion. Diploidnucleus extirpation may be immediately followed bymicroinjection into the recipient. Fusion process has tobe stimulated by electroimpulses, chemicals, Sendaivirus (alleviates membranous inter-permeability) or othermethods. In any case, after the formation of pronuclearpseudozygote, stimulation is to be performed in order toprovoke divisions and embryonic development. For thatpurpose, weak electric impulses are applied in order toimitate stimulating activity of spermatozoids (Campbellet al., 1997).
Chronology of the reproductivecloning successes
In early phases of the cloning technology developmentall researches were performed on amphibians. Hereditary

material of the embryonic (larval) cells was used for theimplantation (Briggs and King, 1952; Fischberg et al.,1958). In the later experiments, cellular nuclei of higherlevels of the larval development were used for the trans-plantation process. The first completely realised experi-ment on animal cloning from the entirely differentiatedcells was carried out by the creation of adult fertile frogs(Xenopus laevis) from the intestinal mucous cells of tad-pole (Table 6, Gurdon and Uehlinger, 1996).
The first mammal ever cloned from the cell of an adultorganism was a famous sheep"Dolly", born on July 5,1996 (Campbell et al., 1996). Details on experiment werepublished a bit later (Wilmut et al., 1997). From that timetill the last days of the year 2002 about ten differentmammal clones were successfully created. Greatestattention was attracted by the very fist cloning experi-ments of the individual species (Table7).
In the reproductive cloning of mammals the first experi-ments haven been frequently characterised by discover-ing some significant features in the theoretical andmethodological assumptions of cellular and organismcloning. In the case of "Dolly" the procedure compriseda "quiescence" of somatic genome, which was aimed tobe fused with enucleated oocyte, i. e. - G1 phase of thecellular cycle was artificially prolonged. This idea waslater on successfully applied in practice by many of themammal cloning practitioners. "Quiescence" wasachieved by the reduction of nourishing substances con-centration in the medium used for cultivation of thedonor cells, in order to reduce informative RNA synthe-sis (Wilmut, 1998). Nevertheless, further experimentswere successful even without introduction of the "quies-cence" method (Cibelli et al., 1998), so that nowadaysboth procedures are frequently co-applied.
While performing the first successful mice cloning(Wakayama et al., 1998), significant innovations wereintroduced in practice. Extirpated diploid nucleus wasincorporated in oocyte by microinjection (micropipette).The importance of this novelty procedure was that theoperation of donor genetic material transfer becameremarkably faster and safer and a new possibility of masspseudozygote creation was initiated. Oophoric heap cellsor "cumulus cells" (cellular group with a particular rolein the realising of oocyte releasing from follicle) wereused as donor cells having all attributes of suitable donorgenetic material. Similar methods were subsequentlyutilised by many other researchers who performed co-administering procedures of the alleviation of fusion(electrostimulation). The first success in cloning ofhuman cells was achieved similarly (Cibelli et al, 2002).Double transfer technique by which donor genetic mate-rial was successively transplanted into two enucleatedoocytes of different maturation stages attained a promi-
nent success also (Polejaeva et al., 2000). Experimentalmethods in mammal cloning differ regarding the devel-opmental stages of the used enucleated oocytes. Besidemature oocyte, oocytes in finale stages of maturation andzygotes were used for the somatic nucleus implantation(see Charts 1 and 2). Oocytes extirpated from the femalegenital tract were taken from appropriately hormonallytreated individuals. The extirpation was than followed bythe short cultivation process or the oocyte was immediateprepared for the somatic nucleus transfer (enucleation).All this procedure variants were proved usable and thevariants include an adequate adjustment of the other pro-cedural components of the experiments.
In general, experimental techniques are numerous anddifferent in many their phases. Variations are not oftenconsiderable although their inter-differentiation is impor-tant especially with regard to the specific systematicposition of the experimental species.
Scope and results of reproductivecloning experiments
Concerning the fact that the first mammal organism evercreated from genetic material of the adult organism bodycells was born in 1996, it is safe to conclude that the his-tory of mammal cloning is not long. However, in themean time about ten different mammal species have beensuccessfully cloned (Table 7, 8 and 9). Scope and resultsof reproductive cloning experiments are presented inTables 8, 9 and 10 and they show specially calculatedinformation's based on the data published in one com-piled statistics (Paterson, 2002).
Still, according to the incomplete information on previ-ous experiments, it is obvious that thousand cells havealready been experimentally cultivated and almost 15000 cloned embryos implantation in surrogate mothers (afemale individual who should give birth to the clonedindividuals) have been performed. However, accordingto the statistics, (Paterson, 2002) less than 400 clonedindividuals survived initial post-natal hours, taking inconsideration all mammal species and all types of exper-iments (Table 9). There is no doubt that further cloningoperations are constantly performed in scientific labora-tories all over the world, what will result in improvedcloning techniques and methods and consequently inincreased number of created clones and comprisedspecies.
If we consider "effectiveness" as a ratio between numberof live-born individuals and number of activatedpseudozygotes, an average cloning experiment efficacyis about 1% (Byrne and Gurdon, 2002), and it can beassessed as low. A rather significant variations regard-ing individual experiment results (operation phases) have
8 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.

to be noticed (Table 9). Nevertheless, the final results are:rather equivalent and show mostly low values of conven-tional effectiveness indexes (Table 9). The explanationfor such results has not yet been fully elucidated. Mostprobably, a high congenital anomalies incidence isamong the causes a low cloning effectiveness.Congenital defects incidence was found to be 12% incloned mice and 8% in cloned goats (Wilmut, 2001), andthose percentages significantly exceed the anomalies fre-quency in the natural sexual reproduction in humans,which amounts approximately to around 3% (Waitzmanet al., 1994).
It is obvious that every phase of the experimental cloningis characterised by low efficacy. The percentage of acti-vated pseudozygotes is rarely over 30% while the record-breaking percentages of experimental successes (69.4%,Wells et al. 1999) are exceptions. From the group of"synthetic" embryos implanted into surrogate mothersonly 3% were born alive, as calculated according to thecorresponding results gathered from 59 experiments thatcomprise all species mentioned in Table 9, or in anotherword, the loss in final experimental phase exceeds 96%.Nevertheless, it is interesting to notice that overall effec-tiveness percentage is highly correlative to the number ofperformed experiments on the corresponding animalspecies (Table10). This suggests that in the future wemay expect an improved cloning effectiveness and con-sequently - a rapid progress in the field of cloning.
Cloning and social responibilities
Achievements in cloning, even in those "older" fields ofgenetic engineering, are frequently far ahead of someimportant elements of natural-scientific or social-scien-tific theories. Social-scientific field is characterised by ahuge conceptual chaos regarding reproductive and thera-peutic cloning results and technologies. In another word,cloning is a researching field where possibilities and per-spectives for the practical usage of experimental resultsfind a considerable non-readiness of the society to acceptthese results, specially regarding the terminology anddefinitions of legislative and custom low elements andlawful regulative of medical services and procedures.Cloning is opening a new field of possibilities for the res-olution of concrete medical and other problems and ques-tions, a sensitive field that is temporarily without organ-ised relations in social communities.
It does not surprise that the first reactions on the newcognition regarding scientific potentials and possibilitiesin the field of cloning are mostly negative and charac-terised by the sort of fear and distrust. Regardless of afew attempts of the strict prohibition on further organismcloning work, experiments have been carried on and thefirst individual examples of practical application of
newly discovered cloning techniques have been carriedout. Anyhow, all crucial elements of biological theory asa base of the cloning experiments have already beenproved providing an unquestionable promise of furtherdevelopment in the field of cloning. It is necessary tomention that the difference between reproductive andreparative cloning is not still clearly characterized, so itneed to be reliably defined and legally demarcated if wewant to congregate positive public opinions on the thera-peutic cloning.
Newly founded perspectives in cloning of human beingsand tissues (farm of organs) are opening a numerous ofethical questions that mind scientists and public all overthe world. Regarding that, a simple principle has to befollowed: a science and its realisation in practice willimplement everything possible to be implemented on thepresent level of development of the knowledge. Any for-mal ban will not stop development of the scientificresearches. The society should clearly define all legal andother measures in order to prevent the misuses of the newscientific findings and their applications. The control ofthe scientific results is only a scientific concern. Britishscientist Maurice H. F. Wilkins, 1962 Nobel PrizeLaureate in Physiology or Medicine for discoveries con-cerning the molecular structure of DNA (together withCrick and Watson), gave once an instructive statement:"Science with technology is the only way to keep out ofhunger, illness and pre-term deaths". We think that theabuse of science origins from the wrong politics. Judson(1970) said: "My personal opinion is that politics iswrong, but science and politics are so tightly related thathardly to be separated".
"Cloned organism is a new type of biological being suchlike has never been seen in the nature" stated once Mr.Ronald Green, an honourable expert in bioethics. At thefirst news about the possibilities of therapeutic and repro-ductive cloning of the human material (Cibelli et al.,2002), Mr. Green warned that the world was fronting theenormous problems (Green, 2002) that had to be imme-diately solved if society and its structures would like tomeet the new scientific perspectives as ready as possible.
9Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.

10 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
GENETICENGINEERING
GENE (DNA) ENGINEERINGSingle gene material manipulation, i.e. molecular manipula-tion or manipulation with the molecular fragments of nucle-ic acids (DNA, RNA)
CHROMOSOMEENGINEERING
Manipulation with the natural groups of allied genes, i.e.manipulation with the chromosomal fragments or entire sin-gle chromosomes
GENOME ENGINEERING
Manipulation with the entire hereditary material of cellularnucleus, when the primary manipulation objectives are thewhole haploid sets of genes (genomes), i.e. entire geneticcompositions
Table 1. Basic typology of the genetic engineering operations and procedures
GENOMICENGINEERING
INDUCTION OF GENOMICMUTATIONS
Haploidy induction
Polyploidy induction
SOMATIC HYBRIDISATIONHomospecific
Heterospecific
SOMATIC GENOMESCLONING
Parasexual reproduction
Culture of embryonic (and definitive) tissues
Table 2. Typology of the main forms of genomic engineering
Table 3. Directions and forms of cloning of dyploid cells genetic material
Table 4. Genome-engineering cloning of human material(basic typology according to the operation objectives)
Cellular Identical reproduction of cells Cultures of cell lineages
«Twinning» of embryos (Embryo-twinning)
«Para-genomic-engineering» cloning
Blastomere separation (Embryo segmentation)
SOMATIC GENOMES
CLONING
Organismic
«Genomic-engineering» cloning
Nuclear somatic transfer - NST
Operation objective
Reparative therapeutic) Identical reproductions of cells, tissues Cloning by somatic
nucleus transfer (SNT) Reproductive Identical reproduction of individuals

11Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Table 5. An overview of the types of cells that were used as donors of hereditary material in mammalreproductive cloning experiments
Table 6. An overview of the development and technical results in enucleation technique in amphibiancloning (frogs)
DONOR CELLS
CUMULUS CELLS 2, 3, 4, 6, 7 FIBROBLASTS 2, 3, 5, 7, STRATUM GRANULOSUM
CELLS1, 4, 5, 7
MAMMARY GLAND CELLS 1, 3 TUBA UTERINA EPITHELIUM 3 1 — Sheep UTERINE EPITHELIUM 3 2 — Mouse
ADULT
ORMANISM
MYOCYTES 3 3 — Bovine SERTOLI'S CELLS 2 4 — Goat FIBROBLASTS 3, 5 5 — Pig HEPATOCYTES 3 6 — Rabbit NEW-BORN
TESTIS CELLS 3 7 — Cat FIBROBLASTS 1, 2, 3, 4, 5 GONAD CELLS 2NEUROCYTES 2SOMATIC CELLS 3, 4, 5 GAMETOGONIA CELLS 3
FOETUS
HEPATOCYTES 3
EXPERIMENT
SPECIES RECIPIENT
CELLSDONOR CELLS RESULT
AUTHORS
Rana
pipiens
Unfertilised, mechanically
enucleated oocyte
Embryonic cells (blastula)
Embryos till neurula stage
Briggs & King, 1952
Rana
pipiens
Unfertilised, mechanically
enucleated oocyte
Embryonic cells (stages till late gastrula)
Larvae (mostly
abnormal) King & Briggs, 1955
Xenopus
laevis
Unfertilised oocyte (without
enucleation)
Embryonic cells (blastula do gastrula stages)
Embryos and larvae (7%
normal) Fischberg et al. 1958
Xenopus
laevis
Unfertilised, enucleated
(UV light) oocyte Larval intestinal cells - Elsdale et al., 1960
First transfer Intestinal larva cells
Xenopus
laevisEnucleated
oocytes Second(serial)transfer
First transplant cells (blastula—neurula)
Normal imaginative
tissues
Gurdon, 1962
Xenopus
laevis
UV light enucleated,
unfertilised oocyte Intestinal epithelium tadpole cells
Fertile adult
frogs
Gurdon & Uehlinger, 1966
Xenopus
laevisThe same Adult erythrocytes and keratocytes Tadpole Gurdon, 1973

12 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Table 7. A chronological overview of the successful experiments in mammal reproductive cloning fromadult organism cells
EXPERIMENTAL DATA
CLONED SPECIES,
RECOURCE
(AUTHORS)
DONOR CELLS DIMENSION OF
EXPERIMENT BIRTH TIME
SHEEP
Ovis aries
(Campbell et al., 1997)
Mammal gland cells (culture)
277 embryos 29 implantations 13 pregnancies
July 5th, 1996 (“Dolly”)
MOUSE
Mus musculus
(Wakayama et al.,1998)
Nuclei of cultivated cells of oophoric cumulus
(cumulus cells)
Larger number of injected oocytes («track cloning»)
October, 1997 (“Cumulina”, with numerous others)
BOVINE
Bos taurus
(Kato et al., 1998)
Cultivated cells of oophoric cumulus and tuba uterina
epithelial cells
125 fusions (both donor types) 38 (18+20) blastocysts 10 implantations in
5 surrogate mothers
July, 1998. (8 calves, from both types of somatic cells)
GOAT
Capra hircus
(Baguisi et al., 1999)
Nuclei of foetal somatic cells
285 fusions 120 embryos, 38 surrogates
25 pregnancies
February, 1999 ( 3 goats)
PIG
Sus scrofa domestica
(Onishi et al., 2000)
Fibroblast nuclei of 24-hours foetus
(primary culture)
210 electro-fusions 110 embryos 4 surrogates
July, 2000 (“Xena”)
GAUR
Bos gaurus
(Vogel, 2001) Epithelial cell of adult male
44 embryos 32 surrogates 8 pregnancies
January, 2001 (“Noah”)
CAT
Felis domestica
(Shin et al., 2002)
Cumulus-cells (primary culture)
87 embryos 8 surrogates
2 pregnancies
December, 2001 (“Cc”, “Sisi”)
RABBIT
Oryctolagus cuniculus
(Chesne et al., 2002) Adult somatic cells ? Mart, 2002

13Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Table 8. An overview of results of successful experiments in mammal reproductive cloning(July, 1996 - December, 2002).
Table 9. A compiled overview of the successes in each experimental phase of mammal cloning
Treated oocytes
Transfers
of NT
embryos
Surrogate
mothers
Number of
pregnancies
Born-alive
individuals
Living
newborns Species
a b c d e f
SHEEP > 2 300 427 177 106 36 13
MOUSE > 19 000 8 311 ? ? 196 141
BOVINE > 6 200 1 450 3 146 917 256 181
GOAT > 2 000 945 103 27 38 30
PIG > 8 500 2 639 39 13 19 16
RABBIT approximately 2 000 1 000 64 10 6 4
GAUR ? 44 32 8 1 0
CAT ? 87 8 2 1 1
The cloning experiment is defined as "successful" if resulted in at least one born-alive individual. Numbers mostly rep-resent either approximate estimation (column "a") or incomplete information.
a - Number of enucleated oocytes (or pro-nuclear zygotes) with transferred somatic genomesb - Number of pseudozygotes with implanted by somatic nucleus, activated and in the form of embryos of
different (early) developmental stages transferred into surrogate mothersc - Number of surrogate mothers with implanted embryosd - Number of conceived surrogate mothers e - Number of born-alive individuals in the parturition momentf - Number of birth-survived individuals
Embryos of NT
oocytes Born-alive
Cloning efficacy Number of successful experiments
Species
a b c d
GOAT 10.5—30.4 (6)
3.3 — 17.5 (6)
0.4 — 4.3 (6)
7
MOUS 16.4—55.1 (9)
1,1 — 23.3 (13)
0.2 — 5.8 (12)
13
BOVINE 4.6 — 69.4 (16)
2.7 — 83.3 (24)
0.3 — 5.0 (24)
28
GOAT 32.1 (1)
1.3 — 13.2 (8)
0.7 — 7.2 (7)
8
PIG 9.5 (1)
0.3 — 0.9 (6)
0.1 — 0.9 (6)
7
RABBIT ? 0.6 0.3 1
GAUR ? ? ? 1
CAT ? 1.1 ? 1

14 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Numbers in brackets are indicating a number of experiments evidenced in available information database
a - Percentage of enucleated recipients with implanted somatic nucleus that were successfully activated(activated to develop).
b - Percentage of born-alive individuals from embryos implanted into surrogate mothers
c - Number of born-alive individuals expressed as a percentage of the total number ofoocytes implanted with the somatic cell genetic material
d - "Successful" is considered to be an experiment that resulted in born-alive individuals and "separate" is each authorised and separately published work dealing with different types of donor cells
Table 10. Correlation between number of reproductive cloning successful experiments and number ofborn-alive individuals originated from the embryos developed from pseudo-zygotes and implanted intosurrogate mothers.
Chart 1. Biological basis of cloning
SpeciesNumber of successful
experimentsPercentage of born-alive individuals
SHEEP 6 8.4 %
MOUSE 13 2.4 %
BOVINE 24 17.7 %
GOAT 8 4.0 %
PIG 6 0.7 %
RABBIT 1 0.6 %
CAT 1 0.1 %
EMBRYONIC
DEVELOPMENT
nI+n
2
2nI
2nII
2nI 2nI
ENUCLEATION
2nI
2nII
nIV
nIInII
nI nI nI nI
nI
ZYGOTE PSEUDOZYGOTE
ENUCLEATED ZYGOTE
2
n
PRONUCLEAR ZYGOTE
TRANSFER
MITOSIS MEIOSIS
.

15Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Chart 2. An overview of the main elements and procedures in development of pseudozygote by somaticcell genetic material transfer into the enucleated oocyte
DIPLOID
CELL
OOCYTE
CULTURE
ENUKLEATED
RECIPIENT
PSEUDOZYGOTE
EMBRYONIC
DEVELOPMENT
Enucleation
Nuclear
transfer
Extirpation
Activation
Stimulation
DONOR RECIPIENT

16 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
References
Alberts B., Bray D., Lewis J., Raff M., Roberts K. & Watson J. D. (1994). Molecular Biology of The Cell (ThirdEdition). Garland Publishing Inc., New York.
Ayala F. J. & Kiger J. A. Jr. (1984). Modern Genetics (Second Edition). The Benjamin/ Cummings PublishingCompany, Inc., Menlo Park (Cal.)-Reading (Mass.)-London-Amsterdam-Don Mills-Ontario-Sydney.
Baguisi A., Behboody E., Melican D. T., Pollock J. S., Destrempes M. M., Cammuso C., Williams J. L., Mims S:D., Porter C. A., Midura P., Palacios M. J., Ayres S. L., Denniston R. S., Hayes M. L., Ziomek C. A., Meade H. M.,Godke R. A., Gavin W. G., Overstr�m E. W.& Echelard Y. (1999). Production of goats by somatic cells nucleartransfer. Nature Biotechnology 17:456-461.
Bains W. (1998). Biotechnology - From A to Z. Oxford University Press, Oxford-New York-Tokyo.
Berberovi} Lj. (2001). Pravci i oblici geneti~koin`enjerskih istra`ivanja. Na{a {kola, 47:55-64.
Briggs R. & King T. (1952). Transplantation of living nuclei from blastula cells into enucleated frogs' eggs.Proceedings Nat. Acad. Sci., 38:455-463.
Byrne J. A. & Gurdon J. B. (2002). Commentary on human cloning. Differentiation 69:154-157.
Campbell K. H. S., McWhir J., Ritchie W. A. & Wilmut I. (1997). Sheep cloned by nuclear transfer from a culturedcell line. Nature 385:810-813.
Chesne P., Adenot P. G., Viglietta C., Baratte M., Boulanger L. & Renard J. P. (2002). Cloned rabbits produced bynuclear transfer from adult somatic cells. Nature Biotechnology 20(4):366-369.
Cibelli J. B., Lanza R. P., West M. D. & Ezzell C. (2002). The first human cloned embryo. Scientific American286(1):44-51.
Cibelli J. B., Stice S. L., Golueke P. J., Kane J. J., Jerry J., Blackwell C., Ponce de Leon F. A. & Robl J. M. (1998).Cloned transgenic calves produced from non-quiescent foetal fibroblasts. Science 280:1256-1258).
Elsdale T. R., Gurdon J. B. & Fischberg M. (1960). A description of the technique for nuclear transplantation inXenopus laevis. Journal of Embryol. and Exp. Morph. 8:437.
Fischberg M., Gurdon J. B. & Elsdale T. R. (1958). Nuclear transplantation in Xenopus laevis. Nature 181:424.Green R. M. (2002). New type of biological entity. Scientific American 286:48-50.
Gurdon J. B. (1973). Gene Expression During Cell Differentiation. Oxford University Press, Oxford.
Gurdon J. B. & Uehlinger V. (1966). "Fertile" intestine nuclei. Nature 210:1240-1241.
Judson H. F. (1979). The Eighth Day of Creation. Simon and Schuster, New York.
Kato Y., Tani T., Sotomaru Y., Kurokawa K., Kato J., Doguchi H., Yasue H. & Tsunoda Y. (1998). Eight calvescloned from somatic cells of a single adult. Science 282:2095-2098.
King R. C. & Stansfield W. D. (1997). A Dictionary of Genetics (Fifth Edition). Oxford University Press, Oxford-New York.
King T. J. & Briggs R. (1955). Changes in the nuclei of differentiating gastrula cells as demonstrated by nucleartransplantation. Proceedings Nat. Acad. Sci. USA 41:321-325.

17Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Monod J (1970). Le hasard et la nécessité (Essai sur la philosophie naturelle de la biologie moderne). Editions duSeuil, Paris.
Moses P. B. (1987). Gene transfer methods applicable to agricultural organisms. (In - "Agricultural Biotechnology- Strategies for National Competitiveness", pp 149-192). National Academy Press, Washington D. C.
Mullis K. B. (1990). The unusual origin of the Polymerase Chain Reaction. Scientific American 262:56-65; April1990.
Mullis K. B. & Falcona F. (1987). Specific synthesis of DNA in vitro via a polymerase chain reaction. Methods inEnzymology 155:335-350.
Onishi A., Iwamoto M., Akita T., Mikawa S., Takeda K., Awata T., Hanada H. & Perry A. C. F. (2000). Pig cloningby microinjection of foetal fibroblasts nuclei. Science 289:1188-1190.
Paterson L. (2002). In - I. Wilmut: Gene Expression and Development. Roslin Institute, Midlothian (UK).
Polejaeva I. A., Chen S., Vaught T. D., Page R. L., Mullins J., Ball S., Dai Y., Boone J., Walker S., Ayares D. L.,Colman A. & Campbell K. H. S. (2000). Cloned pigs produced by nuclear transfer from adult somatic cells. Nature407:86-90.
Prather R. S. (2000). Pigs are pigs. Science 289:1886-1887.
Shin T., Kraemer D., Pryor J., Liu I., Rugila J., Howe L., Buck S., Murphy K., Lyons I. & Westhusin M. (2000). Acat cloned by nuclear transplantation. Nature 415:859.
Spemann H. (1938). Embryonic Development and Induction. Hafner, New York.
Steward F. C., Mapes M. O. & Smith J. (1958a). Growth and organized development of cultured cells. I - Growthand division of freely suspended cells. American J. of Botany 45:693.
Steward F. C., Mapes M. O. & Mears K. (1958b). Growth and organized development of culture cells. II -Organization in cultures grown from freely suspended cells. American J. of Botany 45:709.
Vogel G. (2001). Cloned gaur a short-lived success. Science 291:409.
Waitzman N. J., Romano P. S. & Scheffler R. M. (1994). Estimates of the economic costs of birth defects. Inquiry31:188-205.
Wakayama T., Perry A. C., Zuccotti M., Johnson K. R. & Yanagimachi R. (1998). Full-term development of micefrom enucleated oocytes injected with cumulus cell nuclei. Nature 394:369-374.
Wells D. N., Misica P. M. & Day A. M. (1999). Production of cloned calves following nuclear transfer wit cultureadult mural granolosa cells. Biology of Reproduction 60:996-1005.
Willadsen S. M. (1979). A method for culture of micromanipulated sheep embryos and its use to produce monozy-gotic twins. Nature 277:298-300.
Wilmut I., Schnieke A. E., McWhir J. Kind A. J. & Campbell K. H. S. (1997). Viable offspring derived from foetaland adult mammalian cells. Nature 385:810-813.
Wilmut I. (1998). Cloning for medicine. Scientific American 279:30-35.
Wilmut I. (2001). Somatic Cell Nuclear Transfer (Cloning) Efficiency. Roslin Institute, Midlothian (UK).

Abstract
Lobus limbicus is anatomical basis for explaining thetemporal epilepsy because it not only includes the focusof infection of temporal lobe but also the frontal lobe, andwith it we can explain many of the phenomenon's of theepilepsy (hallucinations, the change of the effects, and soon.).The goal of this assignment was to explore the asymme-try of hippocampal formation on the patients with com-plex partial attacks.The results show that the least number of patients withepilepsy have a symmetric (same) size of the hippocam-pal formation both from the left and the right side. Thenumber is statistically significantly lower than the num-ber of patients with epilepsy who has asymmetric (differ-ent size) hippocampal formation both from the left andthe right side. By the direction of asymmetry the differ-ence in the number of patients with epilepsy isn't statisti-cally significant. Coefficient. of asymmetry shows thatthe asymmetry on the left side is more common to men,while it is distributed evenly on sides, left and right inwomen. Testing of significance in age differencesdepends on the sim. / asim. of the hippocampal formationof both the right and the left side of coronal slice is a sta-tistical significance. While with axial and sagittal slices,we have a statistical significance between a women and aman on the level of the course of asymmetry.So, the use of MRI technique in examining asymmetry ofthe hippocampal formation, that we used on this asym-metry, we suggest it as an template of future examina-tions in a sense of shedding light of the anatomical func-tions that is located on the basis of neuropsychiatrics dys-functions.Keywords: limbic system, hippocampal formation,asymmetry, temporal epilepsy
Introduction
In the limbic system visceral functions are integral withemotional behaviour. That shows best a clinical picture ofthe complex partial attack with the vegetative, psychi-atric (dysfunction of the sensible behaviour) and motoredsymptoms (oral automatism). The importance of hip-pocampus and the surrounding structures in the electricalactivity is best shown with the fact that its damage caus-es abnormal electrical activity in the brain- epilepsy.The results of many psychological studies on patients
with epilepsy show that the psychological deficit is muchlarger in the group of patients with well-known organ eti-ological factor. Pathology of left temporal lobe someconnect with the verbal dysfunction and with learningdysfunctions, wail pathology of the right temporal lobeare conditioning disturbances timing templates and rela-tionships.Bilateral injury on the temporal lobe that has a greataffect on an amygdaloidal complex they cause a series ofbehavioural changes named Kluver - Bucy syndrome. Itis visible on patients as a result of trauma of temporallobe or After surgical operation on the temporal lobe due toepilepsy. Kluver - Bucy syndrome is characterized by thefollowing. The patient can no longer recognize objects bysite (optical agnosia); he can have a significant tactile andhearing agnosia. There is a tendency that he examinesobject by mouth or that he smells them. Than, the patientcan have a tendency to observed cloud surroundings con-stant and he can also overreact on optical stimulations.Patient often doesn't show hate of fear, even when that isnecessary. Patient can also over eat, even when he is nothungry, or he can eat object that are not edible. Often it isalso present hipper sexuality, amnesia, dementia andaphasia; it all depends of the present of damage on thetemporal lobe.
Lobus limbicus is anatomical basis for explaining thetemporal epilepsy because it not only includes the focusof infection of temporal lobe but also the frontal lobe, andwith it we can explain many of the phenomenon's of theepilepsy (hallucinations, the change of the effects, and soon.). Many bodily functions have their rhythm and theyare done in cycles of different length. Most often 24-hourly cycles (ex. bodily temperature oscillation, urina-tion etc). The role of "biological hourly" that regulatesthese rhythms is a part of the limbic system.There fore, psychomotoric epilepsy is frequently con-nected with epil. focused in temporal region, witch isproven with EEG. Experience tells us that all patientswith a focus in the frontal temporal region have a psy-chomotor type of epilepsy. For understanding the tempo-ral epilepsy electro stimulation of the temporal cortexand medial part of temporal structures in a man is impor-tant. Electro stimulation of the lateral and upper part oftemporal lobus on both sides in a mail can cause halluci-nations, that is, complex visual and hearing scenes frompast (as a sequence of a film), a patient are aver of the
18 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Observing of the asymmetry of hippocampalformation on patients with complex partial attacks
Aida Sara~ - Had`ihalilovi}, Faruk Dilberovi}Department of Anatomy, Faculty of Medicine, University of Sarajevo, ^ekalu{a 90

present. The memory of past stops as the electro stimula-tion stops, but it recurs with the replica of electro stimu-lation.
Stimulation of the superior temporal girus can causehearing hallucinations. Electro stimulation of upper partand lateral part of temporal cortex can cause interpretiveillusions, that is, patients present time in time of stimula-tion wrongly interpreted.
Illusions of recognizing, that is, present experience isexperienced as unreal and unknown. They occur as theresult of stimulation of both side of temporal cortex.Illusions of emotions that are the emotions of fear, lone-liness, sorrowed or discuss are accomplished by stimu-lating cortex in the frontal part of parties of temporallobus.
Materials and Methods
As a material for construction of this study we used 35MRI scan in all three projections: horizontal (axial),frontal (coronal) and sagitall patients with epilepsy (com-plex partial attacks). Methods of work include measuringthe size of hippocampal formations in all three projec-tions (axial, coronal and sagittal) 35 patients with epilep-sy (complex partial attacks).
MRI scans are done on MAGNET IMPACT SIEMENS1.0 TESLA in T1 relaxation (TR 500 - 600 / TE 15 / fieldof view 180 x 260, the fatness layer SL 5 mm) and T2relocation (TR 4000 / TE 90 field of view 188 x 250 foraxial and 173 x 230 for coronal, 210 x 240 for sagittalscans in 5 mm layer). Dual sequences are used PD andT2. In PD TR is 4000, and TE 22. We used a head - neckspiral, as well as a head spiral.
On the horizontal (axial), frontal (coronal) and sagittalMRI scans we observed the position and identified a hip-pocampal formation on the level of temporal lobe of thebrain.
On sagittal scans we observed the relation between hip-pocampal formation versus insula. On some sagittalscans we can see a joined hippocampo-amigdaliod zone.
For the size measurement of hippocampal formation andtheir comparison from right to left we used a program ofevaluation- distance on the MRI from the Institute ofRadiology of Clinical Centre in Sarajevo. We tested 35patients with epilepsy, 19 patients male and 16 femalepatients, approximate age 40.8 for males with standarddeviation of 18.37 years and approximate age 27.1 forfemales with standard deviation of 11,68 years.The size of hippocampal formation is measurement in allthree projections: horizontal (axial), frontal (coronal) and
sagittal from right and left. All values of hippocampalformation are given in centimetres.
For hippocampal formation in all three projections (axial,coronal and sagittal) are met in:
1. The number of patients with epilepsy according tosymmetry/asymmetry on the right and left side
2. Analysis of patients with epilepsy by the approxi-mate size of left and right side. Significant difference is tested with t-test
3. Distribution of patients with epilepsy towards thedifferent between the right and left side.The results are shown it tables and diagrams
4. The approximate age of patients with epilepsytowards symmetry / asymmetry from the right andleft side.Significant difference is tested by t-test
Methods of statistical analysis used in this assignmentare:
1. Arithmetic middle 2. Standard deviation 3. Standard failure 4. Median 5. Mod6. Chi-square test 7. t - test differences of arithmetical middle 8. t - test proportionally 9. Coefficient of asymmetry
19Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.

Results
20 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Male Female TOTAL
Number in % Number in % Number in %
SYMMETRY: hippocampal formation on the right and left side of the axial slice of the same length
3 15.79 2 12.50 5 14.29
Total: 16 84.21 14 87.50 30 85.71
Out of that:
The right side
longer than the
left side
5 26.32 7 43.75 12 34.28
ASYMMETRY
hippocampal formation on the right and the left side of the axial slice of the different lengths
The left side
longer than the
right side
11 57.89 7 43.75 18 51.43
T0TAL: 19 100.00 16 100.00 35 100.00
MRI analisis of pacients with epylepsi
A. Hippocampal formation on the axial (horisontal) MRI scanes
Picture 1 Axial MRI scans -the slice on ahippocampal formation level
The difference in the number of patients with epilepsy in the relation to the length of the hippocampal formation on theleft and on the right side of the horizontal slice is statistical significant. The least number of patients has the symmet-rical length of hippocampal formation from the right and the left side, while the most number of patients has the hip-pocampal formation from the left side of the axial slice longer then the one from the right.
The value of Chi-square test is: ChiSq = 7.225, The level of assurement is p < 0.05.
Picture 2 Axial MRI scans -length of hippocampalformation from the right and the left side
Table 1 Shows patient with epilepsy towards simetry/asimetry hippocampal formation from right and lefton the axial slice

21Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
The coefficient shows it is a slight asymmetry to the left, except for women were the asymmetry on the left side isshown the asymmetry of the right side
The statistical of significant difference between the man and the woman in a group of patients in witch the length ofhippocampal formation from the left side axial slice larger on the right. The value of t- test is: t = 3.305, the level ofassurement is p < 0.01.
The number of pacients with epilepsy
Graph 1 Distribution of patients with epilepsy towards difference between the lengths of hippocampal for-mation from the right and the left side
Table 2 The patients with epilepsy towards the approximate length of hippocampal formation from theright and the left
Table 3 Average age of patients with epilepsy according to symmetry / asymmetry of hippocampal for-mation at the right and left side of the axial slice
4
5
9
5
4
5
3
-0,5
i v
iše
-0,3
- -
0,4
-0,1
- -
0,2 0
0,1
- 0
,2
0,3
- 0
,4
0,5
i v
iše
u cm
Male Female
Right side Left side Right side Left side
Arithmetic middle 3.42 cm 3.57 cm 3.23 cm 3.18 cm
Standard deviation S.D. 0.40 cm 0.55 cm 0.38 cm 0.41 cm
Standard failure S 0.092 0.13 0.095 0.102
Median Me 3.49 cm 3.575 cm 3.3 cm 3.1 cm
Coefficient of asymmetry -0.504 -0.027 -0.592 +0.598
xx
Male Female TOTAL
In a
yearS.D.
In a
yearS.D.
In a
yearS.D.
TOTAL 40.8 18.37 27.1 11.68 34.6 17.09 SYMMETRY: hippocampal formation on the right side and on the left side of axial slice of the same length
39.0 9.64 32.0 14.14 36.2 9.43
Total: 39.12 18.36 26.2 11.91 33.1 16.96
Out of that:
The right side
longer than the
left side
29.2 12.67 29.3 15.69 29.3 13.29
ASYMM-ETRY:
hippocampal formation on the axial slice of the different length
The left side
longer than the
right side
43.6 20.09 23.1 7.93 35.7 18.57
x x x

22 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
B. Hippocompal formation on the coronal (frontal) MRI slices
Picture 3 Coronal MRI scans -a slice on the levelof the frontal part of hippocampal formation
Picture 4 Coronal MRI scans -the width of the hip-pocampal formation on the left and the right side
Table 4 Shows patients with epilepsy towards symmetry/asymmetry hippocampal formation from rightand left on the coronal slice
Male Female TOTAL
Number In % Number in % Number In %
SYMMETRY: hippocampal formation on the right side and on the left side of the coronal slice of the same width
7 36.84 2 12.50 9 25.71
Total: 12 63.16 14 87.50 26 74.29
Out of that:
The right side
wider than the
left side
6 31.58 11 68.75 17 48.58
ASYMMETRY:
hippocampal formation on the right sine and on the left side of the coronal slice of the different width
The left side
wider than the
right side
6 31.58 3 18.75 9 25.71
TOTAL: 19 100.00 16 100.00 35 100.00
Number of epilepsy patients with symmetric (same width) of hippocampal formation at the left and right side on thecoronal slice significantly is smaller than the epilepsy patient with asymmetrical (different width) of hippocampal for-mation from the left and right side
The value of Chi-square test is: ChiSq =8.257; the level of assurement is p < 0.01.

23Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
The number of pacients with epilepsy
Graph 2 Distribution of patients with epilepsy towards difference of hippocampal formation from the rightand the left side on the coronal slice
4
3
2
9
8
3 3 3
-0,3
-0,2
-0,1 0
0,1
0,2
0,3
0,4
i v
iše
u cm
Table 5 The patients with epilepsy towards the approximate width of hippocampal formation from theright and the left
Male Female
Right side Left side Right side Left side
Arithmetic middle 1.974 cm 1.958 cm 2.056 cm 1.975 cm
Standard deviation S.D. 0.338 cm 0.258 cm 0.179 cm 0.216 cm
Standard failure S 0.078 0.0592 0.045 0.0541
Median Me 2.11 cm 2.11 cm 2.15 cm 2.05 cm
Coefficient of asymmetry -1.208 -1.768 -1.570 -1.039
xx
Coefficient of asymmetry shows asymmetry on the left side, for both sides (left and right) and for both sex.
Table 6 Average age of patients with epilepsy according to symmetry / asymmetry of hippocampal for-mation at the right and left side of the coronal slice
Male Female TOTAL
In a
year
S.D. In a
year
S.D. In a
year
S.D.
TOTAL 40.8 18.37 27.1 11.68 34.6 17.09
SYMMETRY: hippocampal formation on the right and on the left side of the coronal slice of the same width
47.71 19.04 23.0 2.82 42.22 18.66
Total: 34.08 14.68 27.71 12.36 30.65 13.83
Out of that:
The right side
wider than the
left side
34.0 17.49 28.36 13.35 30.35 14.27
ASYMMETRY:hippocampal formation on the right and on the left side of the coronal slice of the different width The left side
wider than the
right side
34.16 14.52 25.33 12.34 31.22 12.97
x x x
Difference in age average between patient with symmetric value of width of hippocampal formation at the right andleft side of coronal slice and patients with asymmetric values, is statistically significant on the level of assurement p< 0.10. The value of t-test is : t=1.703.

24 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
C. Hippocampal formation on the sagitall MRI slices
Picture 5 Sagittal MRI scans -slice on the levelof the parahippocampal girus and the hippocam-
pal formation
Picture 6 Sagittal MRI scans -the measurements for the hippocampal formations onthe right and the left side

25Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Table 7 Shows patients with epilepsy towards symmetry/asymmetry hippocampal formation from rightand left on the sagitall slice
Male Female TOTAL
In a
year
S.D. In a
year
S.D. In a
year
S.D.
TOTAL 40.8 18.37 27.1 11.68 34.6 17.09
SYMMETRY: hippocampal formation on the right and on the left side of the coronal slice of the same width
47.71 19.04 23.0 2.82 42.22 18.66
Total: 34.08 14.68 27.71 12.36 30.65 13.83
Out of that:
The right side
wider than the
left side
34.0 17.49 28.36 13.35 30.35 14.27
ASYMMETRY:hippocampal formation on the right and on the left side of the coronal slice of the different width The left side
wider than the
right side
34.16 14.52 25.33 12.34 31.22 12.97
x x x
Number of patient with epilepsy with symmetric (same length) of hippocampal formation at the right and left side ofsagittal slice is significantly smaller by statistics from number of patient with epilepsy with different leght of hip-pocampal formation at the right and left side. The value of Chi-square test is: ChiSq = 24.028 while level of assure-ment is p < 0.001
The number of pacients with epilepsy
Graph 3 Distribution of patients with epilepsy towards difference between the length of hippocampal for-mation from the right and the left side
2 2
3
5
3
8 8
2 2
-0,7
i v
iše
cm
-0,5
- -
0,6
cm
-0,3
- -
0,4
cm
-0,1
- -
0,2
cm 0
0,1
– 0
,2 c
m
0,3
– 0
,4 c
m
0,5
– 0
,6 c
m
0,7
– 0
,8 c
m

26 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Table 8 The patients with epilepsy towards the approximate length of hippocampal formation from theright and the left
Male Female
Right side Left side Right side Left side
Arithmetic middle 4.16 cm 4.11 cm 4.20 cm 4.14 cm
Standard deviation S.D. 0.43 cm 0.42cm 0.37 cm 0.53 cm
Standard failure S 0.099 cm 0.096 0.093 0.118
Median Me 4.15 cm 4.12 cm 4.15 cm 4.1 cm
Coefficient of asymmetry +0.090 -0.044 +0.408 +0.214
xx
Coefficient of asymmetry shows asymmetry on the right side. Excuse is asymmetry for the mails left side - whichasymmetry is on left side
Table 9 Average age of patients with epilepsy according to symmetry / asymmetry of hippocampal forma-tion at the right and left side of the sagittal slice
Male Female TOTAL
In a
yearS.D.
In a
yearS.D.
In a
yearS.D.
SYMMETRY:hippocampal formation on the right and on the left side of the sagittal slice of the same length
19.5 3.5 30.0 0 23 5.72
Total: 41.41 16.62 26.93 12.0 34.62 16.34
Out of that:
The right side
longer than the
left side
41.36 18.94 29.56 13.5 36.05 17.73
ASYMMETRY:hippocampal formation on the right and on the left side of the sagittal slice of the different length
The left side
longer than the
right side
41.5 11.18 23.0 7.85 32.37 13.37
x x x
The difference in average age between mail and female in group of patient which hippocampal formation is longer fromthe left side in compare to the right side is statistically significant. The value of t test is: t = 3.317; the level of assure-ment is p < 0.05.

27Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Discussion
The locating of the precise location of the incorrectanatomical function that is in the basis of the neurologi-cal and psychiatric dysfunctions just recently became thesubject of intensive research in this field. In that sense itis important to apply structural and functional techniquesof MRI, for future pinpointing of the problems in work-ing with epilepsy. There for, MRI offers the most sensi-tive volumetric measurements of hippocampal formation. R. C. Peterson et al. - 2000 (22) proves that MRI - hip-pocampal formation precisely shows structural-function-al relationship between the deficit of memory and hip-pocampal damage with the sector of normal ageing ofdementia. Authors underline, that the hippocampal sizescan be precisely sensitive as the diagnostically tech-niques in early uncovering of the degenerative diseasesas it is in AD. In the work of N. Bernasconi et al. - 2001(3) it is shown that the hippocampal sclerosis is mostoften pathology that can be found in the basis of epilep-sy of temporal lobe (ETR) that doesn't react to pharma-ceuticals. Authors show that the usual MRI medical find-ings on patients with epilepsy with ETR hippocampalatrophy. Also, they emphasize the cause / effect relation-ship between the formation of hippocampal sclerosis, andits vivo relationship with hippocampal atrophy with theexistence of temperature convulsions in the picture ETR.Tuuli Salmenpera et al. - 2000 (29) proves that the statusepileptics doesn't always lead to progressive lessening ofthe size of the structure in the medial temporal lobe onmatured patients that have been treated without hospital-ization, with already known protocol for quick relieffrom the attacks. There for the authors emphasize that theserial showing of the magnetic resonance (MRI) offers atool for following the temporal progression of the cere-bral damage that follows the status of epileptics thru thelife. Authors also emphasize the presence of the progres-sive hippocampal damage on MRI after the prolongedstatus epileptics and the resistant one to the drugs. Andfinally, an emphasize on doing the aetiology, that is theacute or chronically of the process. On the basis of the analysis of our results connected withthe size of the hippocampal formation in all three pro-jections (axial, coronal and sagittal), in the group ofpatients with epilepsy we can conclude in the followingway:
1. In all three slices the least number of patients withepilepsy have a symmetric (same) size of the hippocam-pal formations from the left and the right side. That num-ber is statistically significantly lower than the number ofpatients with epilepsy with asymmetric (different size)hippocampal formations from both sides. By the way ofasymmetry the difference in the number of patients withepilepsy isn't statistical significant, except with axialslice, were we have the largest number of patients with
hippocampal formation on the left side longer than on theright (51.43 %).
2. With all three slices in the approximate size of the hip-pocampal formation from the right and left sides isn't sta-tistically significant in men nor in women, except in axialslice were we have the difference between the approxi-mate size of hippocampal formation on the left sidebetween the men and a women is statistical significant,that is the same in the text before.
3. When it comes to the coefficient of asymmetry itshows that the asymmetry on the left side is more oftenin men, wail women have the same distribution on bothsides.
4. The testing of the significance differences in approxi-mate ageing of patients depends on the sim./ asim. hip-pocampal formation from the right and the left sides ofcoronal slice is stat. sign. Wail in axial and sagittal slice,we have a statistically significant between the womenand a man on the level of asymmetry:
a) With the axial slice in the group of patients thathave the longer hippocampal formation on theleft side - males are older than women.
b) With the sagittal slice in the group of patientswith the longer hippocampal formation on theleft side - males are older than women.
Conclusions
On basis of our analysis we can conclude:
1. Every one of analyzed asymmetry shows the samecharacteristics in the group, in witch we emphasize vari-ations.
2. We also emphasize the importance of presence of con-ciseness in individual characteristics of every one of theparameters in the shading light on asymmetry of hip-pocampal formation.
3. We have to be careful about what projection we arerefusing to as being watched hippocampal formationbecause the results will depend on that. We can suggestthe prospective studies in more projections because of thevalue of the statistically significant conclusions.
4. MRI - volumetric measurement have their value.
5. Usage of MRI techniques in examining the asymmetryof hippocampal formation, that we used, we suggest asthe studies in the future research in the sense of the shad-ing light on the anatomical functions that are on the basisof neuropsychiatry dysfunctions.

28 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
References
1. Bilir E., Craven W., Hugg J., Gilliam F., Martin R., Faught E., KuznieckyVolumetric MRI of the limbic system: anatomic determinants, Neuroradiology. 40(3):138-44, 1998 Mar.
2. Baxendale SA., Van Paesschen W., Thompson PJ., Duncan JS., Shorvon SD., Connelly A.:The relation between quantitative MRI measure of hippocampal Structure and the intracarotid amobarbitaltest, Epilepsia. 38( 9 ): 998-1007, 1997 Sep.
3. Bernasconi N., Bernasconi A., Caramanos Z., Dubeau F., Richardson J., Andermann F., Arnold D. L.:Entorhinal cortex atrophy in epilepsy patients Exhibiting normal hippocampal volumes, Neurology, 56:1335 – 1339, 2001.
4. Belin P., Zilbovicius M., Crozier S., Thivard L., Fontaine A., Masure MC., Samson Y.:Lateralization of speech and auditory temporal processing, Journal of Cognitive Neuroscience, 10 ( 4 ): 536– 40, 1998 Jul.
5. Cahill L., Haier RJ., Fallon J., Alkire MT., Tang C., Keator D., Wu J., McGaugh JL.:Amygdala activity at encording correlated with long-term, free Recall of emotional information,Proceedings of the National Academy of Sciences of the USA. 93 ( 15 ): 8016-21, 1996 Jul.
6. Chronister R. B., Hardy S. G. P.: The Limbic System, chapter thirty, 444 – 454, 2000.7. Dalby MA., Elbro C., Stodkilde – Jorgensen H.: Temporal lobe asymmetry
and dyslexia: an in vivo study using MRI, Brain & Language. 62 (1): 51-69, 1998 Mar.8. Dilberovi} F., Kulenovi} A., Kundurovi} Z., Sara~ – Had`ihalilovi} A.:
Contribution to detection of the corpus amygdaloideum using magnetic resonance, XV Congress of theInternational Federation of Associations of Anatomists and IV International Malpighi Symposium, Rome,September, 11 -16, 1999.
9. Dilberovi} F., Kulenovi} A., Sara~ – Had`ihalilovi} A., Kadeni} Z.:Prikaz limbi~kih struktura u temporalnom re`nju velikog mozga metodom MRI i CT, Prvi KongresRadiologa Bosne i Hercegovine, Sarajevo, 14 – 16 Oktobar, 1999.
10. Dilberovi} F., F. Ov~ina, V. ^erkez: Hipokamp i amigdaloidni kompleks u pacova i ma~aka, FoliaAnatomica Jug.: 11 – 20, 1982.
11. Dalagija F., Be{li} [., Vobornik S.: Magnetna Rezonanca, Medicinski `urnal, 1 – 11, Supplement 2000.12. Elaine N. Marieb: Neural Integration – Higher Mental functions, Human Anatomy and Physiology, third
edition: 489 – 500, 1995.13. Had`iselimovi} H., M. ^uš: Konfiguracija lobanjske baze ~ovjeka u odnosu na izgled njenog okcipitalnog
dijela, Gl. Antr. Dr. Jug.: Br. 1:41 – 54, 1964.14. Had`iselimovi} H.: O asimetriji ~ovje~ijeg mozga, Radovi – ANU Odjeljenja medicinskih nauka,
Sarajevo, LI 1974.15. Had`iselimovi} H., ^uš M.: The appearance of internal structures of the brain in relation to configuration
of the human skull, Acta anat. 63, 289 – 299, 1966. 16. Had`iselimovi} H., Ru`di} N.: Appearance of the base of the brain in relation to the configuration of
human skull, Acta anat. 65, 146 – 156, 1966.17. Had`iselimovi} H., And`eli} M.: On the appearance of some interior brain structures in relation to the
exterior configuration of the brain, Acta anat. 63, 289 – 299, 1966.18. Kantard`i} D`: Kognitivnin poreme}aji, Epilepsija i psihi~ki poreme}aji, 44 – 52, Sarajevo, 1997.19. Malcom B. Carpenter: Gross Anatomy of the Brain, Core Text of Neuro-anatomy, third edition: 23-
28,1985.20. Malcom B. Carpenter: Olfactory Pathways, Hippocampal Formation and the Amygdala, Core Text of
Neuroanatomy, third edition: 331 – 347, 1985.21. Merhemi} Z., Dalagija F., Kadeni} Z., Sulejmanpaši} G., Prevljak S., Konjhod`i} F.: Po~etna iskustva
sa aparatom za magnetnu rezonancu od 1,0 Tesla u neuroradiologiji, Medicinski `urnal, 32 – 36,Supplement 2000.
22. Petersen R. C. et al.: Memory and MRI – based hippocampal volumes in aging and AD, Neurology, 54: 581 –587, 2000.
23. Pruessner JC., Collins DL., Pruessner M., Evans AC.: Age and gender predict volume decline in the anterior and posterior hippocampus in early adulthood, Journal of Neuroscience., 21 ( 1 ): 194 – 200, 2001 Jan 1.

29Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
24. Sara~ – Had`ihalilovi} Aida: Asymmetry of palate in relation of asymmetry of neurocranium, TheEleventh European Anatomical Congress Timisoara – Romania, September 10 – 13, 1998.
25. Sara~ – Had`ihalilovi} Aida: Asymmetry of the brain and his blood – vessels, XV Congress of theInternational Federation of Associations of Anatomists and IV International Malpighi Symposium, Rome,September 11 – 16, 1999.
26. Steinmetz H.: Structure, functional and cerebral asymmetry: in vivo morphometry of the planum tempo-rale, Neuroscience & Bio-behavioural Reviews. 20 ( 4 ): 587 – 91, 1996 Winter.
27. Stephan G. Waxman: The Limbic System, Correlative Neuroanatomy, twenty – third edition: 246 – 258,1996.
28. Stephan G. Waxman: Higer Cortical Functions, Correlative Neuroanatomy, twenty – third edition: 275 –286, 1996.
29.Tuuli Salmenpera, Reetta Kalviainen, Kaarina Partanen, Esa Mervaala, Asla Pitkanen: MRI volume-try of the hippocampus, amygdala, entorhinal cortex, and perirhinal cortex after status epilepticus, EpilepsyResearch 40: 155 – 170, 2000.
30. Von Gunten A., Fox NC., Cipolotti L., Ron MA.: A volumetric study of hippocampus and amygdala indepressed patients with subjective memory problems, Journal of Neuropsychiatry and ClinicalNeurosciences, 12 ( 4 ):493 – 8, 2000 Feb.
31. Wolf H., Grunwald M., et al.: Hippocampal volume discriminates between normal cognition, question-able and mild dementia in the elderly, Neuro-biology of Aging. 22 ( 2 ): 177 – 86, 2001 Mar – Apr.

Abstract
The aim of this research is to establish by immunohisto-chemistry if there is a change in the expression of colla-gen type IV, as a substitute of basement membrane, indevelopment of epithelial dysplasia in chronicallyinflamed colon mucosa.
Methods. Biopsy specimens from 270 patients wereexamined: 74 were classified as inflammatory-regenera-tive and 196 as dysplastic lesions. There were 108 casesof mild dysplasia, 58 cases of moderate and 30 casessevere dysplasia, respectively. Visualisation of collagenIV and its way of expression within basement membraneof glandular crypts was performed by immunohisto-chemistry and then compared with findings in normalcolon mucosa and colon adenocarcinoma tissue.
Results. Changes in the expression of collagen IV com-prised of its focal irregularities, diffuse thinning and/orthickening, focal interruptions or its complete absence. Significant changes in the expression of collagen IV inrelation to normal mucosa already occur in inflammatory-regenerative mucosa. In mild dysplasia, these changesare more intensive in relation to those in inflammatoryaltered mucosa as well as at severe dysplasia in relationto moderate dysplasia. Changes in the expression of col-lagen IV in severe dysplasia are significantly more seri-ous than in moderate dysplasia but are identical to thosein colon adenocarcinoma tissue.
Conclusion. These findings suggest that change in theexpression of collagen IV is in correlation to a degree ofepithelial dysplasia that developed in flat chronicallyinflamed colon mucosa.
Key words: collagen IV, epithelial dysplasia, colonmucosa
Introduction
Basement membrane is a structure that separates connec-tive tissue from parenchymatous cells, endothelium,nerve trunks and myocytes. Five types of proteins, ascomponents of basement membranes (BM) are identifiedby immunohistochemistry: proteoglycane heparin sul-
phate, glycoprotein laminin, collagen type IV, entactinand fibronectin. Presence and distribution of entactin andfibronectin are variable. BM in all tissues develops as aresult of mutual activity of epithelium and extracellularmatrix.. Preservation of its integrity is a reflection ofpreservation of structural and functional relation betweenepithelium and stroma. In colon mucosa BM is primarily product of epithelialcells that lay on it but also of pericryptal fibroblasts thatsurround glandular crypts. Heparin sulphate is exclu-sively produced by epithelial cells, collagen IV by mes-enchymal cells while laminin is produced by both typesof cells. Close contact of epithelial cells and pericryptalfibroblasts is essential for production of aforementionedcomponents as achieved only in normal mucosa.
Abnormalities in biosynthesis and/or in metabolism inBM occur within numerous pathologic processes (1), inwhich either hyper-production or reduction of extracellu-lar matrix develops as a final outcome (2 ). Thickening,thinning or absence of BM might occur in reflection tothese processes and was observed by microscopy.Thinning of BM is mostly present at different malignanttumours (3, 4, 5, 6), inside of which thickening of BMsometimes might be present as well (5,7). Irregularities inthe expression of BM are observed at hyperplastic andmild dysplastic changes of larynx mucosa (8, 9, 2), aswell as at paraneoplastic lesion of bronchial mucosa(4,2).
In this paper we tried to determine a relation between theintensity of changes in collagen IV production and gradeof epithelial dysplasia in flat chronically inflamed colonmucosa.
Material and methods
During the routine endoscopic examination, 2-3 speci-mens of colonic mucosa (always at 30 cm from the anus)were taken with biopsy forceps from each patient after aclinician established the diagnosis of inflammatoryprocess. Total number of patients was 270, out of which208 males and 62 females. All patients were older than 45years (median age 65 years, range 46-82).
As a control group we used biopsy specimens of normal
30 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Type IV collagen immunoreactivity ofbasement membrane in inflammatory-regenerativeand dysplastic lesions of the flat colonic mucosa
Svjetlana Radovi}, Ivan Selak, Mirsad Babi}, @eljka Kne`evi}*, Zora Vukobrat-Bijedi}**Institute of Pathology, Sarajevo University School of Medicine, *General Hospital "Sarajevo",**Gastroenterology Department, Sarajevo University Hospital Centre

colonic mucosa of 40 deceased patients, between 30 and70 years old. There were 26 males and 14 females. Thesespecimens were taken during the autopsy and only whencolonic mucosa showed no sign of inflammatory disease.
From the regular autopsy material also the specimens ofcolon adenocarcinoma from cases with "de novo" carci-noma have been taken. Carcinoma samples were takenfrom 40 deceased patients, between 38 and 76 years old(median age 65), 27 males and 13 females. Carcinomas"de novo" are small carcinomas in colonic flat mucosaranging from 7+/-10 mm in diameter. In 29 cases the sur-face was slightly sagged, in 8 cases slightly elevated andin 3 cases a discrete swelling in the level of mucosa sur-face appeared. In "de novo" carcinoma tissue on serialsections, neither by macroscopic nor by microscopicmethod, the existence of resident adenoma could beestablished.
The specimens were fixed in 10% buffered formalin,embedded in paraffin, cut into 3-5 micrometer sectionsand stained by standard haematoxylin-eosin (HE) andanalysed immunohistochemically by mouse anti humancollagen IV (CIV 22, prediluted, code No: L 1863,DAKO).
Histological criteria were defined to ease differentiationof inflammatory-regenerative and dysplastic changes andgrading of dysplasia intensity (10). According to thesecriteria, dysplastic changes are classified into threegroups (mild, moderate and severe dysplasia). The clas-sification was based on 19 criteria regarding morphologyof lesions, graded on a 1-4 scale with respect to the inten-sity of change. The scores were summed up and theirmean marked as index (I). Numerical values of index Ifor individual categories of changes are:
1.3<I<1.8 for inflammatory-regenerative changes;1.9<I<2.3 for mild dysplasia;2.4<I<2.9 for moderate dysplasia and3.0<I<3.7 for severe dysplasia.
Upon immunohistochemical staining, the evaluation ofbiopsy specimens was performed regarding the expres-sion of collagen fibres. We notified intact fibres (promi-nent and continuous distribution around glands that ispresent in normal mucosa), focal irregularities like redu-plication, thinning and/or thickening of collagen, diffusethinning, diffuse thickening, focal interruptions or com-plete absence. Eventual presence of intracytoplasmaticstaining of epithelium for collagen was also notified.BM under skin epidermis served as a positive control.Deposition of collagen IV in BM of capillary blood ves-sels, nerve fibres and smooth muscles fibres of colonmucosa served as a positive internal control in each spec-imen.
Results
Among biopsy specimens of 270 examined patients,chronic ulcerative colitis was found in 105 patients, lym-phocytic colitis in 40 patients and eosinophilic colitis in25 patients. In 74 cases the changes have been defined asinflammatory-regenerative and in 196 cases as dysplas-tic. Mild dysplasia was found in 108 cases, moderate in58 while severe dysplasia was found in 30 cases (Table1).
Table 1. Classification of morphological changesin colon mucosa of 270 patients with colonicinflammatory-regenerative and dysplastic epitheliallesions
In normal colon mucosa collagen IV is expressed byimunohistochemistry as a linear, intact, prominent struc-ture located immediately between epithelial cells ofglands and lamina propria. Immunoreactivity of epithe-lial cell cytoplasm was not observed in normal mucosa.
Variations in immunohistochmical staining of collagenIV were perceived in the category of inflammatory-regenerative and dysplastic changes as well as in colonadenocarcinoma tissue (Table 2.)
Morphological changes Index* Number of patients
Inflammatory-
regenerative changes
1.3 7
1.4 10
1.5 16
1.6 9
1.7 20
1.8 12
Total 74
Mild dysplasia 1.9 21
2.0 10
2.1 29
2.2 30
2.3 18
Total 108
Moderate dysplasia 2.4 14
2.5 15
2.6 8
2.7 6
2.8 11
2.9 4
Total 58
Severe dysplasia 3.0 5
3.1 9
3.2 4
3.3 6
3.4 2
3.5 2
3.6 2
3.7 0
Total 30
* Index (I) is a numerical estimate of the extent of morphological changes
31Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.

In 40 cases of inflammatory-regenerative changes (54%),(Figure 1.) there were numerous and clearly noticeablefocal interruptions of collagen fibres. In 16 cases (21.6%)they were completely absent and in 6 cases (9.4%) therewere focal irregularities like reduplication, thickeningand/or thinning of fibres. In the rest 12 cases (19.2%) thechanges in BM were not observed. All changes were
always limited to those places in which epithelium waspervaded and disintegrated with inflammatory cell infil-trates where the polymorphs were the dominant cells.
In 95 cases of mild dysplasia (87.9%) (Figure 2.) thechanges in BM were not found. It looked the same wayas BM in normal mucosa. In 8 cases (7.4%) there were
32 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Table 2. Immunohistochemical status of collagen type IV in basement membrane of normal mucosa in40 patients, inflammatory-regenerative and dysplastic flat colon mucosa in 270 patients, and in colonadenocarcinoma in 40 patients
Morphological changes
Distribution of
collagen IV in
BM
Normal
mucosa
N=40
Inflammatory-
regenerative
changes
N=74
Mild
dysplasia
N=108
Moderate
Dysplasia
N=58
Severe
dysplasia
N=30
Colon
Adeno-
carcinoma
N=40
Prominent and
continuous 40 (100%) 12 (19.2%) 95 (87.9%) 0 0 0
Focal
irregularities0 6 (9.5%) 8 (7.4%) 2 (3.4%) 0 2 (5.0%)
Diffuse thinning 0 0 1 (0.9%) 6 (10.3%) 2 (6.6%) 0 Diffuse
thickening 0 0 4 (3.7%) 2 (3.4%) 0 0
Focal
interruptions 0 40 (54.0%) 0 47 (81.0%) 7 (23.3%) 2 (5.0%)
Complete
absence 0 16 (21.6%) 0 1 (1.7%) 21 (70.0%) 36 (90.0%)
Table 2a. Results of Table 2 testing
Morphological groups tested for significance Number
of free
degrees
Value of Hi-
quadrate test
Conclusion on
significance of
differences between
morphological groups
and level of significance
1. Normal mucosa -inflammatory-regenerative changes
2. Normal mucosa - mild dysplasia
3. Normal mucosa - moderate dysplasia
4. Normal mucosa - severe dysplasia
5. Normal mucosa - adenocarcinoma
6. Inflammatory-regenerative changes - mild dysplasia
7. Mild dysplasia - moderate dysplasia
8. Moderate dysplasia - severe dysplasia
9. Severe dysplasia - adenocarcinoma
2
1
2
2
1
4
3
2
1
70.174
3.883
96.893
68.815
72.042
123.431
139.259
53.529
3.788
Significant, p<0.005
Significant, p<0.005
Significant, p<0.005
Significant, p<0.005
Significant, p<0.005
Significant, p<0.005
Significant, p<0.005
Significant, p<0.005
not significant for p<0.05, but significant for p<0.01

irregularities like thickening and/or thinning of collagenIV fibres that preserved their continuity. Diffuse thicken-ing was observed in 4 cases (3.7%), while diffuse thin-ning was observed in only one case (0.9%).
In mild dysplasia (Figure 3.) there was a wide range ofdifferent expressions of collagen IV fibres. Focal inter-ruptions in BM were found in 47 cases (81%), diffusethinning in 6 cases (10.3%) and diffuse thickening andfocal irregularities in 2 cases each (3.4%). In one casesthese fibres in BM were completely missing.
In 21 case of severe dysplasia (70.0%) collagen IV typefibres were completely missing and in 7 cases (23.3%)there were focal interruptions while in 2 cases (6.6%) thediffuse thinning of these fibres within BM was notified.
In 36 cases of colon adenocarcinoma (90.0%), collagen
IV fibres were totally missing from BM of atypical
glands. Focal interruptions and focal irregularities in the
expression of these fibres were found in two cases each
(5.0%).
Differences in the expression of collagen IV fibres in BM
were tested for significance and these results showed
high significance (p<0.005) regarding severity collagen
fibres damage for each following category in comparison
to the previous category of morphological changes
(Table 2a.). Only the differences between severe dyspla-
sia and adenocarcinoma are lees significant (p<0.10) in
relation to the differences between other categories.
33Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Figure l. Focal attenuation and focal interruption of type IV collagen of the basement membrane of glandsof the colon mucosa with inflammatory-regenerative changes (X 250).
Figure 2. Type IV collagen of the basement membrane of glands of the colon mucosa with mild dysplasia(X 100).

Discussion
There is a small number of studies related to changes ofextracellular matrix (ECM) in pre-neoplastic lesions ofdifferent tissues (2, 4, 9). The majority of these studies isfocused on the changes of ECM in tumour tissue. It iswell known that modifications in the expression of extra-cellular matrix are the reflection of disturbed interactionof epithelium and matrix and have a big role in thegrowth and spreading of tumour (1, 3). The biggest num-ber of observations is mostly related to malignanttumours. Findings regarding changes in extracellularmatrix are rather controversial. These studies deal withdestruction and degrading of BM but also with the newsynthesis of BM (9,2). Former findings suggest that neo-plastic cells of well-differentiated carcinomas preserveability of BM components' synthesis, like normal cells(9), which can be induced by mesenchymal cells (4). This paper analysed the ways of expression of collagenIV fibres within BM of inflammatory-regenerative anddysplastically changed flat colonic mucosa. The findingsare then compared with those in normal mucosa andcolon adenocarcinoma tissue.There are significant differences in the expression of col-lagen IV in inflammatory-regenerative mucosa in rela-tion to normal mucosa, reflected in the occurrence offocal irregularities, interruptions and complete lack offibres. These lesions of BM were at the sites with a lot ofinflammatory cell infiltrates dominated with the poly-morphs that were not only close to epithelium but alsotuck into it. In mild dysplasia, the significance of changescompared with aforementioned category was even high-er. With an increase in ED intensity, changes in BM weremore prominent. In moderate dysplasia, in the biggestnumber of cases, we notified focal interruptions, diffusethinning and focal irregularities. In one case collagen IVfibres were completely missing. In severe dysplasia, inthe biggest number of cases these fibres were completely
missing while in a few cases we notified focal interrup-tions of their continuity and diffuse thinning. There wereno differences in the expression of collagen IV fibresbetween cases of severe dysplasia and adenocarcinomatissue. These findings are in correlation with Fosseler-Eckhoffov findings (4), that notified degradation of BMcomponents (fibronectin, collagen III and laminin) in theareas of dysplastic epithelium of bronchial mucosa whichseverity depended on ED degree. In dysplastic lesions,with an increase of their intensity, a quantity of mononu-clear cellular infiltrate also enlarged (macrophages werethe dominant cells), but direct lytical activity of inflam-matory cells on the epithelium was not observed.The findings of collagen IV lesions in inflammatory-regenerative and dysplastic colon mucosa can be theresult of different cellular mechanisms but are still notcompletely solved. Inflammatory cells contain proteaseenzymes (elastases, collagenases and plasminogen acti-vator) that are capable to cause severe damage of extra-cellular matrix (ECM) (11). Collagenasa, enzyme of neu-trophil leukocytes has a direct effect on collagen IVfibres. Collagenases are excreted in inactive zymogenform (as proenzyme), which only later acquire catalyticactivity but the exact mechanism of activation is stillunknown (12). It is the most probable that these injuriesand interruptions of collagen fibres in the category ofinflammatory-regenerative changes are the result of neu-trophils' collagenases activity since this type of cell dom-inated in inflammatory infiltrate. Range of anomalies ofcollagen IV fibres is in correlation with ED intensity.Macrophages were the most numerous inflammatorycells in dysplastic lesions and in stroma of colon adeno-carcinoma but had no direct contact with the epithelium.Since the macrophages are capable of excreting prote-olytic enzymes, which are responsible for digestion ofBM substrate, their possible action on collagen fibres isnot excluded. It is also notified that dysplastic epithelialcells are capable of production and release of collagenas-
34 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Figure 3. Well defined type IV collagen basement bembrane interruption of glands of the colonic mucosawith moderate dysplasia (X 100).

es (13,14), that destroy ECM and in that way they trace apath for tumour cells of their own origin to invade.Dysplastic cells are capable to activate inflammatorycells i.e. macrophages and to stimulate them to releaselysosomal enzymes (15).At chemically induced carcinomas of murine colon,preservation of collagen IV fibres in BM was notified atwell-differentiated adenocarcinomas but only in thoseareas where the pericriptal fibroblasts were in close con-tact with carcinoma cells (16). The areas where there wasno such close contact between these two types of cellswere deprived of collagen IV. Since mesenchymal cellsprimarily produce collagen IV, lack of these fibres inthese cases is interpreted through a loss of close contactbetween these two types of cells (16,17). It is found thatstroma of myofibroblasts around atypical glands of colonadenocarcinoma produce lytic enzymes that lead to BMcomponents' degradation and collagen IV fibres in par-
ticular (17). In a recent research of pericryptal fibroblasts(PCF) in the dysplastic lesions of flat colonic mucosa(18) we notified that a decrease in the number of PCFcorrelated with the increase of ED grade. Therefore areduction in the number of these cells could serve as arisk marker for pre-neoplastic and neoplastic progressionof the lesion.We cannot be certain about the mechanism of observedchanges only on the basis of morphologic indicators andwithout experimental controls. It is not clear whether theabnormalities of BM in ED are the result of cessation incollagen IV production because of pre-neoplasticallychanged epithelium, changes in PCF number or that isbecause increased degradation by specific enzymes orig-inated from mononuclear inflammatory cells. It is alsopossible that all these aforementioned mechanisms areinvolved in these events at the same time.
35Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
References
1.Van Den Hooff A. The part played by the stroma in carcinogenesis. Perspect Biol Med 1984; 27: 498-509.2. Visser R, Van der Beek JMH, Havenith MG, Cleutjens J, M Bosman FT. Immunocytochemical detection of base-
ment membrane antigens in the histopathological evaluation of laryngeal dysplasia and neoplasia.Histopathology 1986;10:171-180.
3. Daneker GW, Piazza AJ, Steele GD, Mercurio AM. Interaction of human colorectal carcinoma cells with base-ment membranes. Arch Surg 1989;124:183-187
4. Fisseler-Eckhoff A, Prebeg M, Voss B, Muller KM. Extracellular matrix in preneoplastic lesions and early cancerof the lung.Path Res Pract 1990;186:95-101.
5. Havenith MG, Arends JW, Simon R, Volovics A, Wiggers T,Bosman T. Type IV collagen immunoreactivity incolorectal cancer. Prognostic value of basement membrane deposition. Cancer 1988;62:2207-2211
6. Nakanishi K, Kawai T, Suzuki M, Torikata C. Bronchogenic squamous cell carcinomas with invasion along alve-olar walls. Histopathology 1996;29:363-368.
7. Lagace R, grimaud JA, Schurch W. Myofibroblastic stromal reaction in carcinoma of the brest: variations of col-lagenous matrix and structural glycoproteins. Virchows Arch (A) 19985;408:49-59.
8. Antonelli AR, Nicolai P, Cappiello J, Peretti G, Molinari Tosatti MP, et al. Basement membrane components innormal, dysplastic, neoplastic laryngeal tissue and metastatic lymph nodes. Acta Otolaryngol 1991;111:437-443.
9. Sakr WA, Zarbo RJ, Jacobs JR, Crissman JD. Distribution of basement membrane in squamous cell carcinoma ofthe head and neck. Hum Pathol 1987;18:1043-1050.
10. Nikulin A, Radovic S. Razrada morfoloških kriterija za dijagnosticiranje displasticnih promjena u sluznici debel-og crijeva (Analysis of morphological criteria for the diagnosis of dysplastic changes in the colon mucosa).Radovi ANUBiH, odjeljenje medicinskih nauka 1991;25:33-43.
11. Campbell EJ, Senior RM, Welgus HG. Extracellular matrix injury during lung inflammation. Chest 1987;92:161-167
12. Bonkhoff H, Wernert N, Dhom G, Remberger K. Basement membranes in fetal, adult normal, hyperplastic andneoplastic human prostate. Virchows Archiv A Pathol Anat 1991;418;375-381.
13. Kao RT, Stern R. Collagenases in human breast carcinoma cell lines. Cancer Res 1986;46:13449-54.14. Kao RT, Stern R. Elastases in human breast carcinoma cell lines. Cancer Res 1986;46:1355-1358.15. Henry N, van Lamsweerde AL, Vaes G. Collagen degradation by metastatic variants of Lewis lung carcinoma:
cooperation between tumour cells and macrophages. Cancer Res 1983;43:5321-532716. Pujuguet P, Hammann A, Martin F, Martin M. Abnormal basement membrane in tuors induced by rat colon can-
cer cells. Gastroenterol 1994;107:701-711.17. Martin M, Pujuguet P, Martin F. Role of stromal myofibroblasts infiltrating colon cancer in tumor invasion. Path
Res Pract 1996; 192:712-717.18. Radovic S, Selak I, Babic M, Bratovic I. Demonstration of percryptal fibroblasts in inflammatory-regenerative
and dysplastic epithelial lesions of the flat colonic mucosa. Adv in Clin Pathol 2001; 5: 139-145

Abstract
Background and Purpose: The aim of this work was toorder quantitative parameters of the proximal convolutedtubules (PCT) in the normal rat kidney cortex. Volumedensity (VV), both surface and specific surface densitytoward interstitium (SVi and SVi/VV) and toward lumen(SVl and SVl/VV) and thickness (T) of tubules epitheliumhave been stereologically ordered. Material and Methods: Stereologically were analysed170 test fields by lattice L36 on the paraffin sections of thethree adult male Wistar rats kidney dyeing by PAS-method. Results: The mean values of the variables analysedwere: VV=76.4% ±0.012; SVi=0.056µm-1 ±0.004;SVl=0.028µm-1 ±0.003; SVi/VV=0.073µm-1 ±0.003;SVl/VV=0.037µm-1 ±0.005; T=18,26µm ±0.897.Conclusions: Stereological methods are making a veryvaluable contribution to science over recent years. Wehave used unbiased stereological counting methods toobtain objective quantitative parameters of the PCTepithelium in the normal rats' kidney cortex.
Key words: kidney, proximal convoluted tubule, stereol-ogy, rat.
Introduction
The nephron is the fundamental structural and functionalunit of the kidney. Each nephron consists of a dilated por-tion, the renal, or malpighian, corpuscle; the proximalconvoluted tubule (PCT); the thin and thick portions ofthe loop of Henle; and the distal convoluted tubule (9).The proximal thick segment of the nephron begins as thePCT at Bowman's capsule; it makes a short turn towardthe cortex and then returns to its site of origin where itfollows a very tortuous or convoluted course. It thenenters a medullar ray and continues as the descendingproximal straight tubule into the pyramid (21). PCT is thelongest, most convoluted tubular part of the nephron (24)about 14 mm in length and 60µm wide in human ren (6). The PCT is lined by simple cuboidal epithelium. Thecylindrical or pyramidal cell of this epithelium has aspherical nucleus and a strongly acidophilic granularcytoplasm. The cell apex, exposed to the lumen of thetubule, exhibits 1-1.3µm long abundant microvilli thatform the so-called brush border. Because of the extensive
interdigitations of the lateral membranes, no discrete cellmargins can be observed with the light microscopebetween cells of the proximal tubule (9, 21). Although all parts of the nephron, as well as the PCT,investigated and described morphologically in detail uptoday, our knowledge of renal quantitative parameters isstill incomplete. The stereology as a method is mainlyused for researches of glomeruli (1, 2, 7, 12, 13, 15, 23).Total numbers of glomeruli were estimated in the normal(4) and experimental (25) rat and in human (8) kidney.Usual techniques of stereological estimates of glomerularcapillaries number and sizes were also used in research-es of glomeruli in experimental conditions (3, 16). Allstudies that have used the technique of Nyengaard andMarcussen (18) to estimate the number of capillary loopscontributed to the increase in total capillary length. Thesestudies include studies of glomerular capillary growth inrats with lithium nephropathy (14), experimental diabet-ic nephropathy (19) and following unilateral nephrecto-my (17). But very little has been published about quanti-tative parameters of the mayor proximal cortical nephronsegments (11, 20, 22).Knowledge of normal quantitative parameters of PCTepithelium is very important and might be useful forcomparison based on objective numerical valuesobtained in investigations of different experimental andpathological conditions. The purpose of this work isbased on the reasons mentioned above. Stereologicalanalyses were performed on normally structured tubularpart of rat's kidney cortex to obtain some main numericalparameters of PCT epithelium. The distal tubules werenot evaluated owing to the difficulties in distinguishingwith sufficient reliability between those structures andcollecting ducts or vessels.
Material and methods
Rat kidneys used in this study were obtained from threeadult male Wistar rats. After fixation in 10% neutralformaldehyde and embedding in paraffin, the 8µm-thicksections were stained by the periodic-acid-Schiff (PAS)reaction. This study was performed by stereological analysis of170 test fields of the ren tissue cortex. The sections forstereological analysis were used systematically and inter-mittently. Counting number was ordered from pilotmeasuring towards De-Hoff's (10) formula in which esti-
36 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Proximal convoluted tubules of the rats kidney- a stereological analysisSelma Ali~elebi}Institute of Histology and Embryology,University of Sarajevo, School of Medicine,^ekalu{a 90, 71 000 Sarajevo, Bosnia and Herzegovina

mated number "n" means number of test fields measuringneeded for stereological analyse with 95% confidence.Stereology as the methodology provides meaningfulquantitative descriptions of the geometry of real threedimensional glob structures from measurements that aremade on two dimensional images sampled from the glob(5). Stereological measuring was done on a light micro-scope by the semicircular multipurpose test system L36
after Mertz, at objective magnification x40. Referentspace was the renal cortex and the proximal convolutedtubule epithelium was the investigated phase (Fig.1). We calculated by means of standard stereological proce-dures volume density (VV) of the PCT epithelium, its sur-face density (SVl) and specific surface density (SVl/VV)toward lumen, its surface density (SVi) and specific sur-face density (SVi/VV) toward interstitium and its thickness(T). Statistical evaluation of the data included calculation ofbasic descriptive statistic parameters. We calculatedmean value - σ, standard deviation - SD and standarderror - SE of results obtained for each stereological vari-able.
Results
Results of rat kidney quantitative analyse are presented inTable 1.The results of the stereological analyses have shown thatvolume density (VV) of PCT epithelium varied from0.750 to 0.774µmo in three investigated rats kidneys. Theaverage volume density (σ±1SE) was 0.764± 0.007µmo.Surface density (SVl) of PCT epithelium toward lumen, orluminal surface of epithelium, in three investigated rat'skidneys varied from 0.024 to 0.030µm-1. The averagesurface density (σ±1SE) was 0.028± 0.002µm-1.Surface density (SVi) of PCT epithelium toward intersti-tium, or basal surface of epithelium, varied from 0.052 to0.059 µm-1 in our investigation, and the average value(σ±1SE) of this stereological variable was 0.056±0.002µm-1.Specific surface density (SVl/VV) of PCT epitheliumluminal surface varied from 0.031 to 0.041µm-1, and theaverage value (σ±1SE) was 0.037± 0.003µm-1.
Specific surface density (SVi/VV) of PCT epitheliumtoward interstitium varied from 0.070 to 0.076µm-1, andthe average value (σ±1SE) was 0.073± 0.002µm-1.Thickness (T) of PCT epithelium in three investigatedrats kidneys varied from 17.440 to 19.218µm,and theaverage value (σ±1SE) was 18.261±0.518µm.
Discussion
The present results indicate that the useful informationcan be obtained about rat kidney by stereological investi-gation. The only requirement was to recognise and dis-tinguish the proximal convoluted tubules epitheliumfrom the other structures in the renal cortex. Sections inour investigation were stained by the periodic-acid-Schiff(PAS) reaction because previous morphologic descrip-tions (9) pointed at a well-developed, PAS-positive base-ment membrane around the proximal convoluted tubuleand at its microvillar brush border lined by a PAS-posi-tive cell coat (a structure rich in glycoproteins). We havedescribed the estimation of volume density, surface den-sity, specific surface density and thickness as an exampleof using of stereological methods.Volume density, as a relative stereological variable,denoting how much of the volume is taken up byresearched phase. The results of our stereological analysehave shown that the volume part of proximal convolutedtubules epithelium was 76.4% of the rats renal cortex.Surface density, as a relative stereological variable,denoting how much space a certain surface had taken upwhen compared to the volume unit. In our investigationthe average surface density of luminal surface of proxi-mal convoluted tubules epithelium (SVl) was 0.028±0.002µm-1 and the average value of its surface towardinterstitium (SVi) was much greater (0.056± 0.002µm-1).Specific surface density denotes how a certain surfacechanges in comparison to its volume. Specific surfacedensity (SVl/VV) of proximal convoluted tubules epitheli-um luminal surface was 0.037± 0.003µm-1 and the spe-cific surface density of proximal convoluted tubulesepithelium toward interstitium (SVi/VV) was much greaterand that 0.073± 0.002µm-1. The mean thickness of 18.261µm of PCT epithelium
37Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Table 1 The main morphometric parameters of epithelium of the rat renal proximal convoluted tubules
Kidney VV SVi SVl SVi/ VV SVl/ VV T
1. 0.774 0.059 0.030 0.076 0.038 17.440
2. 0.750 0.052 0.030 0.070 0.041 18.124
3. 0.767 0.056 0.024 0.073 0.031 19.218
0.764 0.056 0.028 0.073 0.037 18.261
SD 0.012 0.004 0.003 0.003 0.005 0.897
SE 0.007 0.002 0.002 0.002 0.003 0.518
mean value - σ, standard deviation - SD, standard error - SE

obtained in our study is compatible with observation thatthe thin part of the loop of Henle, which is a continuationof the proximal convoluted tubule, has an external diam-eter of about 12µm, the smaller collecting tubules have adiameter of approximately 40µm and the diameter of thecollecting ducts reaches 200µm near the papillae (9) andwith observation that proximal convoluted tubule isabout 60µm wide in human ren (6). Our findings are alsocompatible with previous findings of Kazimierezak et al.(11). They measured diameters of the cortical proximaland distal tubules of the unilaterally nephrectomized andthe control male, four weeks old, Wistar rats by an eye-piece with inserted scale. They have indicated a progres-sive increase in diameter of the cortical tubules betweenthe second and the twenty-eighth days of experiment.The diameter of PCT increased from 32µm to 42µm. Themean thickness of 18.261µm of PCT epithelium obtainedin our study indirectly corroborates their findings of PCTdiameter because their experimental animals were muchyounger than adult animals in our investigation.
Despite differences in the stereological techniques andanimal age, sex and weight, our results are quantitativelyvery similar to those of Seyer-Hansen et al. (22) andPfaller et al. (20) and indirectly corroborate theirs. Seyer-Hansen et al. (22) studied different rats' renal structuresduring the initial phases of compensatory renal hypertro-phy. Their measurements were made both on intact andon nephrectomized animals. They estimated volume frac-tions of proximal tubular cells and lumina with cortex asthe reference volume, the average luminal and external
diameter of the proximal tubulus and average proximaltubulus cell height as half the difference between the twodiameters. In intact control animals tubule cell volumewas 345±14mm3, luminal diameter was 19.2±2µm andepithelial cell height was 10.2±1µm. Pfaller et al. (20)studied the compensatory hypertrophy in different renalcortical structures in rats 10 and 21 days after unilateralnephrectomy and in sham controls by quantitative mor-phological/stereological analysis and found the PCTresponds with "radial" hypertrophy (thickening of thetubular epithelial wall), while the DCT undergoes"length" hypertrophy (increase of tubular length withoutthickening of the tubular wall and without an increase innumber of cells). Absolute volume of epithelial PCTcompartments contained in the renal cortex was about310ml. Absolute surface areas of the luminal (3.4m2) andbasolateral (2.3m2) PCT cell membrane domains con-tained in the renal cortex were determined in sham con-trols. The enlargement in PCT epithelial volume isaccompanied by changes in the total luminal and basolat-eral membrane surface areas of cortical tubule segments.Although they didn't directly measure, they conclude anincrease in the thickness of the PCT epithelial cell layer.In conclusion, the present findings have confirmed previ-ous morphologic findings, identified some new andimportant correlations, and suggested some correlationsthat may emerge as statistically significant once addi-tional kidneys have been analysed. Meanwhile, theknowing of normal quantitative parameters of proximalconvoluted tubules epithelium is important for extendingour total knowledge about ren.
38 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Figure 1 Proximal convoluted tubule (H) in the normal rat' kidney cortex (stained by PAS method, x180)

39Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
References
1. Bendsten,T.F., Nyengaard,I.R.: Unbiased estimation of particle number using sections-on historical per-spective with special reference to the stereology of glomeruli, Journ Microsc, 1989; 153/1,
2. Bertram,J.F.: Analysing renal glomeruli with the new sterology, Int Rev Cytol, 1995; 161:111-72, 3. Bertram,J.F.; Cahill,M.M.: Glomerular capillary growth and cellular hyperplasia in a model of focal and
segmental glomerulosclerosis, Image Anal Stereol, 2000; 19:109-112,4. Bertram,J.F. et al.: Total numbers of glomeruli and individual glomerular cell types in the normal rat kid-
ney, Cell Tissue Res, 1992; 270:37-45,5. DeHoff, R.T.: Probes, populations, samples, measurements and relations in stereology, Image Anal Stereol,
2000; 19:1-8.6. Duan~i},V.: Osnove histologije ~ovjeka, Medicinska knjiga Beograd-Zagreb, 1986,7. Hinchliffe,S.A. et al.: The effect of intrauterine growth retardation on the development of renal nephrons,
Br J Obstet Gynaecol, 1992; 99:296-301,8. Johnson,K.J. et al.: Estimating total glomerular number in human kidneys with a physical dissector/ frac-
tionator combination, Image Anal Stereol, 2000; 20:105-108,9. Junqueira,L.C. et al.: Basic histology, 7th edition, Appleton & Lange, Connecticut,1992,
10. Kali{nik,M.: Temelji stereologije, Acta stereologica, 1985; 4:1-148,11. Kazimierezak,J. et al.: Morphometric and enzyme Histochemical behaviour of the kidney of young rats
before and after unilateral nephrectomy, Histochemistry, 1976, 46:107-120,12. Langley-Evans,S.C. et al.: Foetal exposure to a maternal low protein diet impairs nephrogenesis and pro-
moted hypertension in the rat, Life Sci,1999; 64:965-74,13. Mackensen-Haen,S. et al.: Contribution on the correlation between morphometric parameters gained from
the renal cortex and renal function in IgA nephritis, Lab Invest, 1988; 52/2:239-45,14. Marcussen,N. et al.: Compensatory growth of glomeruli is accomplished by an increased number of
glomerular capillaries, Lab Invest, 1994; 70:868-74,15. Merlet-Benichou,C. et al.: Intrauterine growth retardation leads to a permanent nephron deficit in the rat,
Pediatr Nephrol, 1994; 8:175-80,16. Nyengaard,J.R.: The quantitative development of glomerular capillaries in rats with special reference to
unbiased stereological estimates of their number and sizes, Microvasc Res,1993a; 45:243-61,17. Nyengaard,J.R.: Number and dimensions of rat glomerular capillaries in normal development and after
nephrectomy, Kidney Int, 1993b; 43:1049-57,18. Nyengaard,J.R., Marcussen,N.: The number of glomerular capillaries estimated by an unbiased and effi-
cient stereological method, J Microsc, 1993; 171:27-37,19. Nyengaard,J.R., Rasch,R.: The impact of experimental diabetes mellitus in rats on glomerular capillary
number and sizes, Diabetologia, 1993; 36:189-94,20. Pfaller,W. et al.: Quantitative morphology of renal cortical structures during compensatory hypertrophy,
Exp Nephrol, 1998, 6:308-319,21. Ross,M.H. et al.: Urinary system In: Histology. A Text and Atlas 3rd ed. Williams & Wilkins, Baltimore,
Maryland, pp 558-94, 1995,22. Seyer-Hansen,K. et al.: Stereology of the rat kidney during compensatory renal hypertrophy, Acta
path.microbiol.immunol.scand. Sect.A.,1985, 93:9-12,23. Washizava,K. et al.: Morphometric changes in glomerular anionic sites during aminonucleoside nephrosis,
Acta Path Jap, 1989; 39/8:558,24. Wheather,P.R. et al.: Urinary system In: Functional Histology, A text and colour atlas,2nd edition,
Churchill Livingstone, Edinburgh, London, Melbourne and New York, pp 236-58, 1989,25. Zimanyi, M.A. et al.: Nephron number in the offspring of rats fed a low protein diet during pregnancy,
Image Anal Stereol, 2000; 19:219-22.

Abstract
Polycyclic aromatic hydrocarbons are common environ-mental pollutants that reach atmosphere in the form ofaerosol adsorbed on soot, ash and dust. Having in mindits carcinogenic and mutagenic effects most countrieshave regulations concerning their estimation in environ-mental samples. In this work we have investigatedextraction efficiency of several polycyclic aromatichydrocarbons from flying particles collected on glass fib-ber filters. Efficiency of extraction of different durationin Soxhlet apparatus, ultrasonic bath and boiling tolueneunder reflux were compared. It has been established thatcompounds having two or three condensed rings are lostduring evaporation of toulene that was used as a solvent.For compounds having five or more condensed ringsextraction in ultrasonic bath and boiling toluene usingmagnetic stirrer and reflux are the most efficient.Key words: polycyclic aromatic hydrocarbons, extrac-tion, Soxhlet apparatus, ultrasonic bath, reflux, gas chro-matography
Introduction
Polycyclic aromatic hydrocarbons (PAH) are group oforganic compounds whose molecules are composed oftwo, three or more six-member, sometimes five-memberrings condensed in linear or angular form. These com-pounds are formed during incomplete combustion of fos-sil fuels, in home furnaces and automobile exhaust, aswell as in different industrial processes like production ofcoke, iron aluminium or crude oil refineries (1,2). Owingto its relatively high boiling points, they reach atmos-phere in the form of aerosol, adsorbed on the ash, soot ordust. PAHs having two or three rings might be present ingas phase and solid phase simultaneously. Polycyclicaromatic hydrocarbons are very stabile in the environ-ment showing tendency to cumulate and they can betransferred through food chain. Particular interest thatthese compounds attract is due to their distinct carcino-genic and mutagenic effect. In fact, they are the firstdescribed chemical carcinogens. By the end of the 18th
century British physician Percival Pott describedincreased incidence of scrotum cancer among Londonchimneysweepers, which was attributed to soot. Later,during the second decade of 20th century PAHs wereidentified in the soot (3). Mechanism of carcinogenicimpact of PAHs is based on its metabolic transformation
involving cytochrom-dependent monooxygenazes thatgive dihydrodioles which can be further oxydized givingrise to substances that can have stable carbonium ion (4).Due to expressive nucleophylic properties of carboniumions, these metabolites are covalently bonded to cellmacromolecules including nucleic acids, which can givemutations and further can be converted in pre-neoplasticor neoplastic lesion (5).Nowadays the most of developed countries have strictregulations concerning PAHs. At the same time they areclassified among persisting organic pollutants that havespecific treatment (6). All of this demand application ofsensitive and reliable analytical methods for its determi-nation in food, water and environmental samples.Extraction procedure is the first step in every analyticalmethod that strongly influence on the overall sensitivity,accuracy and precision. Up to date different extractionprocedures of PAHs from particulate matter have beenpublished (7, 8). These methods involve the use of dif-ferent solvents in Soxhlet apparatus (9), use of ultrasonicbath (10, 11), extraction with supercritical fluids (12,13),exraction with ionic tenzides (14) or extraction assistedby micro waves (15). However, only few publicationsdeal with comparison of efficiency of different extractionprocedures. This is why we have investigated and com-pared extraction efficiencies of relatively simple proce-dures suitable to be used in modestly equipped laborato-ries.
Material and methods
In this work we have investigated extraction in ultrason-ic bath lasting 30 minutes and 3 hours, extraction in boil-ing toluene with magnetic stirrer under the reflux lasting30 minutes and 3 hours and extraction in Soxhlet appara-tus lasting 5 hours. In all experiments was used toluenesupplied by Kemika, Zagreb. Ultrasonic bath of 100 Wpower and 30 kHz frequencies was supplied by Iskra,Kranj and magnetic stirrer with hot plate MM 510 byTehtnica, @eleznik. Following polycyclic aromatichydrocarbons were investigated: naphthalene, acenaph-thylene, acenaphtene, fluorene, phenatrene, anthracene,pyrene, fluorantene chryzene, benz(a)anthracene,benzo(a)pyrene and dibenz(a,h)anthracene. All standardswere purity pro analysis, supplied by Fluka. Methylstearate was used as internal standard and was purchasedthrough Micromass, Manchester.Extract clean up was performed using XAD-2 resin,
40 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Determination of the extraction efficiency of polycyclicaromatic hydrocarbons from airborne particulate matterMiroslav [ober, Branko NikolinFaculty of Pharmacy, University of Sarajevo^ekalu{a 90, Sarajevo

according to modified method, originally described bySpitzer (16). The resin was purchased from SigmaFeinbiochemica, Heidelberg and was prepared accordingto procedure previously described by [ober and Nikolin(17, 18). Clean up was performed as follows. Fraction ofpolar compounds was first eluted using ethanol (suppliedby Kemika, Zagreb), followed by fraction of aliphaticcompounds eluted by n-hexane (Merck, Darmstadt) andethanol. Finally, fraction with aromatic compounds waseluted with toluene. Toluene fraction was spiked withinternal standard, evaporated to dryness at 40 oC underthe stream of nitrogen, reconstituted in exactly 100 µL oftoluene and subjected for further chromatographic analy-sis. Quantification of polycyclic aromatic hydrocarbons wasperformed by gas chromatography on semi polar capil-lary column DB-5, 30 m x 0.32 mm purchased fromJ&W Scientific. Gas chromatograph was Dani 3800 HRequipped with flame ionisation detector and helium wasused as a carrier gas with flow rate of 1 mL/min.Temperature program started at 110 oC, hold for 10 min-utes, then heated to 280 oC with rate of 3 oC/min.Chromatograms were registered on Perkin Elmer 56recorder with 10 mV input sensitivity.Determination of all compounds was performed usinginternal standard method, with calibration curve.Results of extraction efficiency were analysed by analy-sis of variance to find out whether significant differencebetween groups exists or not.Concerning the fact that standard reference material wasnot available, it was necessary to prepare samples of air-borne particulate matter with exact concentration of poly-cyclic aromatic hydrocarbons. To do so, we collected air-borne particles in city of Zenica during winter period,when emission is the highest. Samples were collected byLIB sampling device supplied by SAG Apparate undGerateban, Ottobrun, Freilinger und Ritschel, GmbH.Flying particles were collected on glass fibber filtersSartorius type SM 134 00. Each sample was collected for24 hours with 350 m3 mean volume of air passed throughthe filter. After sampling, filters were extracted in Soxhletapparatus for 24 hours using toluene, with approximate-ly 5 cycles per hour. After drying in the air and dessica-tor, each filter was cut out in 8 equal parts. Two partswere separately extracted and extracts checked forresidues of organic compounds by gas chromatography.Other parts of the filter were spiked by the means ofHamilton RNE 25 precision syringe with standard solu-tion containing amounts of PAHs listed in table 1.
Each sample prepared on such way was dried at roomtemperature and kept in dessicator until extraction. Extraction in ultrasonic bath was performed in durationof 30 minutes and 3 hours. Due to technical limitations,ultrasonic vibrations were applied in 15 minutes inter-vals, followed by 10 minutes break. That means that 30
Table 1: Amounts of substances used in experi-ment
minutes of effective extraction lasted 40 minutes and 3hours of effective extraction lasted almost 6 hours.Extraction in boiling toluene was performed using mag-netic stirrer with hot plate, under reflux, lasting 30 min-utes and 3 hours.Extraction in Soxhlet apparatus was also performed usingtoluene, with approximately 5 cycles per hour. In each case extract was protected from direct sunlight, toavoid photo oxidation.
Results and discussion
In this experiment toluene was chosen as solvent due toits similarity with investigated substances. In few otherpublications authors used benzene, but we chose toluenefor reasons of its lover toxicity. Unfortunately, due totoluene's relatively high boiling point (111 oC) most oflow volatile PAHs were lost during procedure of sampleevaporation. It has been established that naphthalene,acenaphthylene and acenaphthene are completely lost aswell as most of phenantrene and anthracene and signifi-cant amount of pyrene and fluorene. Fortunately, thesecompounds have negligible biological activity, so pro-posed extraction procedures still might be used for analy-
Substance Amount
Naphthalene 3,46 µg
Acenaphthylene 3,09 µg
Acenaphtene 3,58 µg
Fluorene 3,55 µg
Phenantrene 3,70 µg
Anthracene 3,48 µg
Fluorantene 3,41 µg
Pyrene 3,17 µg
Benz(a)anthracene 3,21 µg
Chryzene 3,95 µg
Benz(a)pyrene 3,25 µg
Dibenz(a,h)anthracene 3,73 µg
41Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.

sis of carcinogenic PAHs. These are compounds with 5 ormore condensed rings and it was shown that their extrac-tion efficiency ranges from 42.55% to 80.52%.In table 2 are shown mean results of six individual sam-ples from each group, analysed in duplicate (table 2).
Analysis of variance was used to test significance of dif-ference among results in one group and between groups.It has been established that results of groups C and D sig-nificantly differ from groups A and B, but there is no sig-nificant difference among them. Results of group E aresignificantly different from results of groups C and D inthe case of benz(a)anthracene, benzo(a)pyrene anddibenz(a,h)anhtracene. Extraction efficiency of chrysenein group C is significantly different from all other results.In other words it means that extraction in boiling toluenelasting 3 hours is the most appropriate for extraction ofchrysene. But in case of pyrene, extraction in ultrasonicbath lasting 3 hours is the most effective.Results for extraction efficiency of phenantrene differfrom all other. However it was previously stated that
most of the phenantrene was lost during evaporation pro-cedure, so figures in table might reflect this lost morethen difference in extraction procedure. To avoid lose oflow boiling substance it would be necessary to switchbetween toluene to another low volatile solvent.Methylene chloride might be appropriate choice.In the experiment described in this work it has beenestablished that the most effective procedures are extrac-tion in boiling toluene using magnetic stirrer and refluxlasting 3 hours and extraction in ultrasonic bath lasting 3hours. However, extraction in boiling toluene has priori-ty over extraction in ultrasonic bath, due to previouslydescribed technical limitations that make actual extrac-tion time almost 6 hours. Extraction in Soxhlet apparatusgives somewhat cleaner extracts compared with extrac-tion in boiling toluene, since magnetic stirrer destroysglass fibber filter and extract contains particles of filter. Due to significant loses of low volatile substancesthrough evaporation procedure; it should be reconsideredswitch between toulene and another solvent with lowerboiling point.
42 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Table 2: Extraction efficiency of five different procedures for PAHs extraction
Percent of recovery Compound name
A B C D E
Phenantrene 9.98 11.07 11.12 12.48 12.15
Anthracene 12.25 12.76 16.64 16.74 14.81
Fluorantene 29.05 28.55 29.65 29.66 29.05
Pyrene 27.85 28.00 30.25 36.74 29.18
Benz(a)anthracene 66.41 70.83 76.93 77.55 65.90
Chyzene 65.95 66.41 80.52 71.34 70.46
Benzo(a)pyrene 42.55 41.94 58.34 54.50 51.19
Dibenz(a,h)anthracene 34.33 34.87 65.03 62.37 55.76
Legend:A = Extraction in boiling toluene, using magnetic stirrer and reflux lasting 30 minutesB = Extraction in ultrasonic bath lasting 30 minutesC = Extraction in boiling toluene, using magnetic stirrer and reflux lasting 3 hoursD = Extraction in ultrasonic bath lasting 3 hoursE = Extraction in Soxhlet apparatus lasting 5 hours
43Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
References
1. Nikolaou K., Masclet P., Monsev G. Sources and chemical reactivity of polycyclic aromatic hydrocarbonsin the atmosphere - a critical review. Sci Tot Eviron. 1984; 32: 103-132
2. Quilliam M.A., Lunt M.S., Kaiser-Farrel C., McCalla D.R., Sheldrake C.P., Kerr A.A., Lockington J.N.,Gibson E.S. Identification of polycyclic aromatic compounds in mutagenic emission from steel casting.Biomedical Mass Spectrom. 1985; 12: 143-150
3. Pitot H.C. III, Dragan Y.P. Chemical carcinogenesis. In: Cassaret and Doul'ss Toxicology: The basic sci-ence of poisons, fifth edition, Klaase C.D. Ed. McGraww-Hill, New Yourk 1996
4. Cavalieri E.L., Rogan E.G. The approach to understanding aromatic hydrocarbon carcinogenesis: The cen-tral role of radical cations in metabolic activation. Pharmacol Ther 1992; 55: 183-199
5. Larssen B.S. Interaction between chemicals and melanin. Pigment Cell Res 1993; 67: 127-1336. United Nations Economic Commission for Europe: New Protocol on Persistent Organic Pollutants, Aarhus,
Denmark February 1998.7. Junk G.A., Richard J.J. Extraction of organic compounds from solid samles. Anal Chem 1986; 58: 962-9658. Griest W.H., Yeatts L.B. Jr, Caton J.E. Recovery of polycyclic aromatic hydrocarbons sorbed on fly ash for
quantitative determination. Anal Chem 1980; 52: 199-2019. Lee F.S.C., Schuetzle D. Handbook of polycyclic aromatic hydrocarbons, Bjorseth A. Ed. Marcel dekker,
New York, 198310. Golden C., Sawick E. Extraction of organic compounds from particulate matter using ultrasonication. Int j
Environ Chem 1975; 4: 9-1311. Pereira P.A., De Andrade J.B., Miguel A.A. Determination of 16 priority polycyclic aromatic hydrocarbons
in particulate matter by HRGC-MS after extraction by sonication. Anal Sci 2001; 17: 1229-123112. Hawthorne S.B., Miller D.J. Extraction and recovery of polycyclic aromatic hydrocarbons from environ-
mental solids using supercritical fluids. Anal Chem 1987; 59: 1705-170813. Termodynamic and kinetic model for the extraction of essential oil from suvoy and polycyclic aromatic
hydrocarbons from soil with hot water and supercritical CO2. Kubatova A., Jansen B., Vaudoisot J-F.,Hawthorne B. J Chromatogr A 2002; 975: 175-188
14. Merino F., Rubio S., Perez-Bendito D. Acid-induced cloud point extraction and preconcentration of poly-cyclic aromatic hydrocarbons from environmental solid samples. J Chromatogr A 2002; 962: 1-8
15. Bruno P., Caselli M., de Gennaro G., de Rienzo M., Traini A. Analysis of polycyclic aromatic hydrocar-bons in the atmospheric particulate - focused microwaves for a faster extraction method. J Environ Monit2000; 2: 223-227
16. Spitzer T. Clean-up of polycyclic aromatic hydrocarbons from air particulate matter on XAD-2. JChromatogr 1982; 237: 273-278
17. M. [ober, B. Nikolin. Policikli~ki aromatski ugljikovodici u atmosferi grada Zenice. Arhiv za higijenu radai toksikologiju 1990; 41: 297-304
18. M. [ober Analitika fotooksidacionih produkata policikli~kiha aromaskih spojeva u atmosferi. Ph.D Thesis,Faculty of Pharmacy, University of Sarajevo 1996

Abstract
Although the drug abuse has been evidenced in every ageof the human life, it seems that its occurrence is crucialduring adolescence period with its well-known conse-quences on the further personality development.Adolescents like to experiment with risky lifestyles with-out adequate knowledge about their possible harmfuleffects and consequences. International experiences haverepresented that early onset of the risky behaviour pre-disposes young persons for serious problems in social,psychological and physical future lives.It has been noticed that adolescents like to combine dif-ferent psychoactive substances. Therefore the aim of thisstudy was to present the most important and the mostactual substances abused by young adolescents togetherwith the substance characteristics. This research included 600 adolescents with the sameprevalence regarding age, sex and living zone (rural-urban).Our research showed that simultaneous abuse of variousharmful psychoactive substances (polydrug abuse) is themost common (tobacco smoking and cannabis consump-tion in 75% of cases, alcohol consumption and cannabisconsumption in 80% of cases).
Key words: adolescence, genetic factors, biogenetic fac-tors, cannabis, tobacco, alcoholism, Bosnia andHerzegovina.
Introduction
Drug abuse is sociopathological phenomenon thatdestroys social, economical and family life of the person.In the middle of 20th century new modern psychophar-macological medicines were discovered - drugs with thesignificant influence on the consumer's mental andbehaviour status. Therefore, these medicines were namedpsychoactive or psychotropic substances. In the majority
of cases, the use of psychopharmacological medicines isnot under the control of medical professionals. Cases ofthe "self-medication" are very frequent, as well as numer-ous evidences when individuals, especially adolescents,experiment on themselves with a combined abuse of dif-ferent psychotropic substances in order to experiencetheir effects. This kind of behaviour often leads towardsaddiction syndrome with unpredictable consequences(1).Psychoactive substance abuse implicates the psychoac-tive substance consumption in maladaptive manner dur-ing the period longer that one month. It differs from thepsychoactive substance addiction syndrome because itdoes not comprise abstinence symptoms. Usually it leadsto physical or mental health impairment. Although thedrug abuse has been evidenced in every age of the humanlife, it seems that its occurrence is crucial during adoles-cence period with its well-known consequences on thefurther personality development. Adolescents like toexperiment with risky lifestyles without adequate knowl-edge about their possible harmful effects and conse-quences. International experiences have represented thatearly onset of the risky behaviour predisposes young per-sons for serious problems in social, psychological andphysical future lives.As a country in transition, Bosnia and Herzegovina hasall characteristics of the post-war society with numerousrisk factors for the psychoactive substance abuse (2). Theusage of narcotics, psychoactive substances (especiallycannabis products), antiparkinson agents, glue, solvents,rarely heroin and seldom cocaine and LSD-25 wasnoticed during the year 1996. Unfortunately, exact dataon the prevalence of psychoactive substances addictionhave not been precisely evidenced, even in developedcountries with highly organised health services and otherfollowing aspects of the social and health care. The rea-son for that is that drug abuse problem is very dynamicand changeable according to the prevalence of the illegaldrug abuse, patterns of the drug abuse throughout time,
44 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Simultaneous abuse of different psychoactivesubstances among adolescentsAmira Red`i}*, Ifeta Li~anin**, Sanja Kro{njar***
* Department of Biology with Human Genetics, Faculty of Medicine, University of Sarajevo, ^ekalu{a 90, Bosnia and Herzegovina; E-mail: [email protected]
** Psychiatric Clinic of Clinical Centre of University of Sarajevo, Bolni~ka 25, Bosnia and Herzegovina;E-mail: [email protected]
*** Bosnalijek, Pharmaceutical and Chemical Joint Stock Company, Juki}eva 55, Sarajevo, Bosnia and HerzegovinaE-mail: [email protected]

history of the drug consumption and development of theassociated social problems. Psychoactive substanceabuse exact data are usually gathered from the curedaddict medical registers in health services, by the mortal-ity prevalence data related to the drug abuse and through-out the police reports (2). These are three groups of the drug abuse aetiological fac-tors: Psychoactive substance type together with its effect,addict personality and social environment (social fac-tors). Psychoactive substance type ad its effect have animportant role in substance abuse among young people.
General drug abuse risk factors according to Newcombare:
1. Cultural-social: Law that promotes drug abuse,social standards that promote drug abuse, drugavailability, unusually difficult economic condi-tions, parents and family members substanceabuse, positive attitude towards substance abuse inthe family;
2. Interpersonal: Model for deviant behaviour (parentabuse of psychoactive substances), conflictsbetween parents or friends;
3. Biogenetic: Genetic factors responsible for the vul-nerability (psychological vulnerability to substanceeffects, personality characteristics, low self-esteemand risky behaviour predisposition). Positive fami-ly anamnesis regarding drug addiction (childrenfrom the alcoholic families are two to four timesmore predisposed to develop some type of addic-tion in comparison to children from the non-alco-holic families). In this group of factors it is verydifficult to differentiate genetic from the environ-mental component. Genetics is also very importantin some psychiatric disorders especially in someaffective disorders highly related to the drug abuse(e.g. bipolar affective disorder). These disordersare more frequently registered within population ofaddicts than within general population.
4. Psychosocial: prolonged risky behaviour with earlyonset, inappropriate and bad school behaviour andfinal educational result, insurgent behaviour, posi-tive attitude towards drug abuse, addiction onset inearly life age, conflicts and disturbed interpersonalrelations in the family (it is more likely that chil-dren will start to use alcohol or drugs in familieswhere parents do not control children at all or infamilies with too strict and inconsistent discipline).Also, it is well known, that if parents abuse psy-choactive substances children become addictsmore frequently.
There are many psychoactive substance classifications,but due to practical reasons we use to divide them intothree major groups: The first group is presenting all sub-
stances with sedative effect, the second group is nervoussystem stimulating substances and the third group is sub-stances with hallucinating effects (3, 4, 5).Usually, addicts combine drugs with different substancessuch as alcohol, sedatives and hypnotics what can causesevere physical and mental impairments. Liver impair-ment, for example, can affect another drug metabolismby causing of prolonged sedative effect during the simul-taneous usage of alcohol and sedatives. Sedative effects of alcohol have been used in order toreduce anxiety or depression, but also to straighteneffects of other substances consumed concomitantly withalcohol. Alcohol has ability to impair other substancemetabolism including sedatives, cocaine and opiates. Ithastens cocaine metabolism with resulting accumulationof its metabolites. For that reason alcohol has a hepato-toxic effect. Adolescents mostly abuse marihuana and alcohol, butalso marihuana and depressants in the form of tablets."Speedball" is when stimulants are used in combination
with opiates. Recently, the new form of smoking stimu-lant known as "ice" is in use. It can induce a rapid andhigh drug concentration in the brain with resulting pro-longed intoxication (12-24 hours). During the intoxica-tion phase, "ice" consumers often have psychotic symp-toms related to the violent behaviour. "Ice" abuse is indramatic increase in California and Hawaii. Considering all facts mentioned above, our research goalwas to estimate the frequency of various psychoactivesubstances simultaneous abuse.
Methodology
Type of researchThe study type was prospective and epidemiological-analytical.
SampleThis research included 600 adolescents in total, 200 fromTuzla Canton (100 from Elementary Schools and 100from High Schools) and 400 from Sarajevo Canton (200from Elementary Schools and 200 from High Schools).The average age of participants was between 12 to 17years with equal prevalence regarding the sex and resi-dence location. (rural-urban).
Research instrumentsThe collection of necessary information we performed bythe "Q2000" test, a questionnaire founded in the period1990-1991 and dealing with the drug abuse problem.This test was scientifically validated and accepted inmany countries. "Q2000" test contains a wide spectrumof the questions relating to the all aspects of adolescentlife, including health education, life style and behaviourin school. The questionnaire is anonymous and voluntarybased. Our investigation preparation and "Q2000" test"
45Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
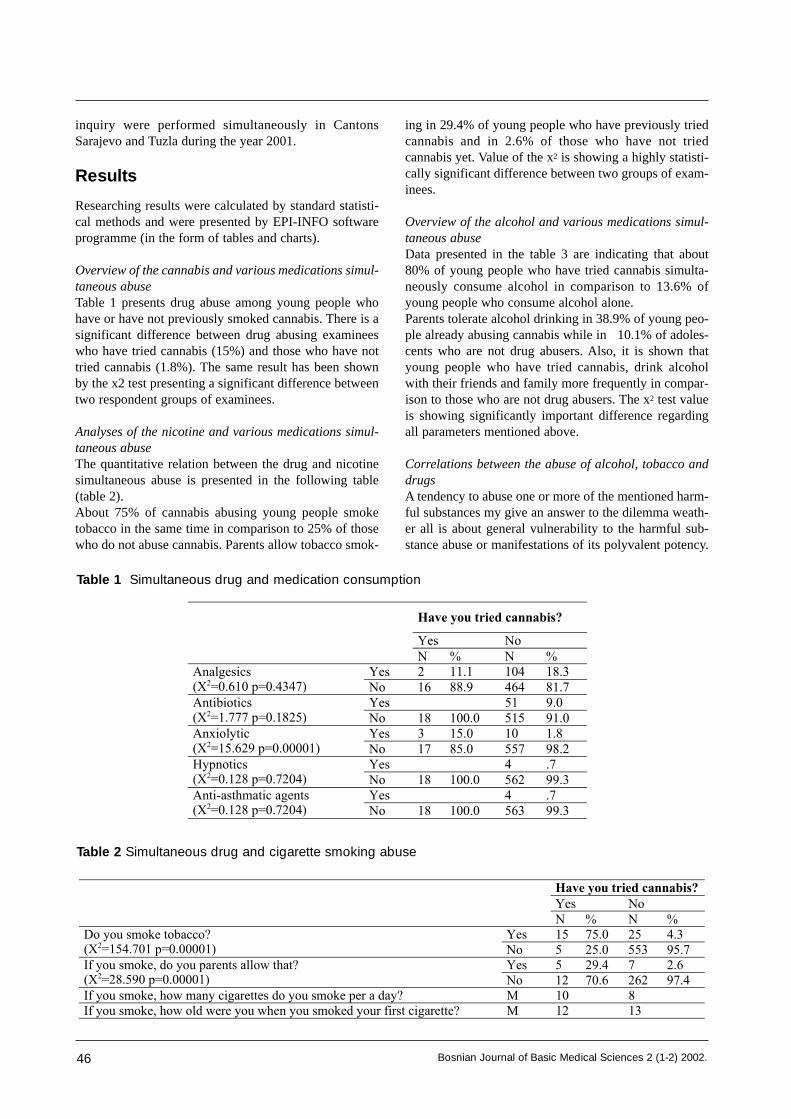
inquiry were performed simultaneously in CantonsSarajevo and Tuzla during the year 2001.
Results
Researching results were calculated by standard statisti-cal methods and were presented by EPI-INFO softwareprogramme (in the form of tables and charts).
Overview of the cannabis and various medications simul-taneous abuseTable 1 presents drug abuse among young people whohave or have not previously smoked cannabis. There is asignificant difference between drug abusing examineeswho have tried cannabis (15%) and those who have nottried cannabis (1.8%). The same result has been shownby the x2 test presenting a significant difference betweentwo respondent groups of examinees.
Analyses of the nicotine and various medications simul-taneous abuse The quantitative relation between the drug and nicotinesimultaneous abuse is presented in the following table(table 2). About 75% of cannabis abusing young people smoketobacco in the same time in comparison to 25% of thosewho do not abuse cannabis. Parents allow tobacco smok-
ing in 29.4% of young people who have previously triedcannabis and in 2.6% of those who have not triedcannabis yet. Value of the x2 is showing a highly statisti-cally significant difference between two groups of exam-inees.
Overview of the alcohol and various medications simul-taneous abuse Data presented in the table 3 are indicating that about80% of young people who have tried cannabis simulta-neously consume alcohol in comparison to 13.6% ofyoung people who consume alcohol alone. Parents tolerate alcohol drinking in 38.9% of young peo-ple already abusing cannabis while in 10.1% of adoles-cents who are not drug abusers. Also, it is shown thatyoung people who have tried cannabis, drink alcoholwith their friends and family more frequently in compar-ison to those who are not drug abusers. The x2 test valueis showing significantly important difference regardingall parameters mentioned above.
Correlations between the abuse of alcohol, tobacco anddrugsA tendency to abuse one or more of the mentioned harm-ful substances my give an answer to the dilemma weath-er all is about general vulnerability to the harmful sub-stance abuse or manifestations of its polyvalent potency.
46 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Table 1 Simultaneous drug and medication consumption
Have you tried cannabis?
Yes No N % N %
Yes 2 11.1 104 18.3 Analgesics (X2=0.610 p=0.4347) No 16 88.9 464 81.7
Yes 51 9.0 Antibiotics (X2=1.777 p=0.1825) No 18 100.0 515 91.0
Yes 3 15.0 10 1.8 Anxiolytic (X2=15.629 p=0.00001) No 17 85.0 557 98.2
Yes 4 .7 Hypnotics (X2=0.128 p=0.7204) No 18 100.0 562 99.3
Yes 4 .7 Anti-asthmatic agents (X2=0.128 p=0.7204) No 18 100.0 563 99.3
Table 2 Simultaneous drug and cigarette smoking abuse
Have you tried cannabis?
Yes No N % N %
Yes 15 75.0 25 4.3 Do you smoke tobacco? (X2=154.701 p=0.00001) No 5 25.0 553 95.7
Yes 5 29.4 7 2.6 If you smoke, do you parents allow that? (X2=28.590 p=0.00001) No 12 70.6 262 97.4 If you smoke, how many cigarettes do you smoke per a day? M 10 8 If you smoke, how old were you when you smoked your first cigarette? M 12 13

Following tabular review is showing a high positive cor-relation between different substance abuse, includingcorrelation between tobacco and alcohol abuse, tobaccoand drug abuse and alcohol and drugs abuse as well. Allresults obtained during our investigation are indicatingthat there is a genetic and phylogenetic tendency tosimultaneous polyvalent harmful substance abuse.Table 4. is presenting a highly significant correlationbetween tobacco and drug abuse, but also between alco-hol and drug abuse and alcohol and tobacco abuse.
Discussion
Literature data undeniably indicate that simultaneousabuse of different harmful substances is very common.Our investigation results are corresponding to the litera-
ture data. We discovered that young people who abusedcannabis frequently consumed alcohol or psychothera-peutics in the same time, and vice versa, which implicat-ed the presence of all variations of the simultaneous, dif-ferent substance abuse. Petraitis and Flay tested the USA population aged 12years and older (1997-1999), and found out that 14.8 mil-lion Americans used illegal drugs from which 6.7% wereaged 12 years and older. The most frequently abused drugwas cannabis (75%), cannabis in combination with otherharmful substances (18%) and other drugs (25%). It wasconcluded that 6.4 Americans were abusing other harm-ful substances with or without cannabis (7).Psychotherapeutic agent abuse in Americans was presentas follows: Painkillers 2.6 million, tranquillisers 11 mil-lion, CNS stimulants 0.9 million and sedatives 0.2 mil-
47Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Table 3 Simultaneous drug and alcohol abuse
Have you tried cannabis?
Yes Yes
N % N %
Yes 16 80.0 77 13.6 Do you drink alcohol beverages?
(X2=63.920 p=0.00001) No 4 20.0 490 86.4
Yes 7 38.9 43 10.1 If you are drinking alcohol, do your parents allow that?
(X2=14.330 p=0.00001) No 11 61.1 383 89.9
If you are drinking alcohol, how old were you when
you had your first alcohol beverage? Mean 12 12
How often do you drink alcohol with your friends? Daily or almost daily 2 10.0 2 .5
Couple times a week 3 15.0 How often do you drink alcohol with your family?
(X2=19.688 p=0.00001) Couple times a year 2 10.0 30 7.2
Couple times a week 1 5.0 3 .7
Couple times per month 1 5.0 5 1.2
Once a month 1 5.0 5 1.2
How often do you drink alcohol alone?
(X2=0.140 p=0.9866)
Couple times a year 2 10.0 8 1.9
Couple times a week 3 15.0 1 .2
Couple times per month 1 5.0 3 .7 How often do you get drunk?
(X2=2.708 p=0.2582) Couple times a year 5 25.0 10 2.3
Table 4 Correlations
Do you smoke
cigarettes?
Do you drink
alcohol beverages?
Have you tried
cannabis?
Spearman rho .390(**) .509(**)
P .000 .000 Do you smoke
cigarettes? N 587 598
Spearman .390(**) .330(**)
P .000 .000 Do you drink
alcohol
beverages? N 587 587
Spearman rho .509(**) .330(**)
P .000 .000
Spearman
rho
Have you tried
cannabis? N 598 587
** Correlation is significant on the level 0.01

lion Americans. About 1.5 million young people (12years) abused cocaine (0.7%) while hallucinogens wereabused by the 0.4% of young people. Analgesic abuse hasbeen in increase from 1980-ties till present time. In theyear 1990 the prevalence of the analgesic abuse amongyoung people aged from 12 to 17 years increased for6.3/1000 while the result for the year 1999 was32.4/1000. The final conclusion was that most frequentlyabused illegal substance among American adolescentswas cannabis (44% among high school adolescents) (8,9). Gilligan and the group of authors investigated tobaccosmoking and highly risky behaviour with the purpose toestablish the relation between cigar smoking, cigarettesmoking and alcohol drinking among adolescents agedfrom 10 to 15 years. Adolescents who smoked tobaccomore frequently abused some other tobacco products andalcohol beverages (10). Concurrent abuse of different psychoactive substanceswas investigated by many authors with the conclusion
that tobacco smoking and alcohol drinking were predic-tive for the drug abuse (11).Our investigation revealed that adolescents most fre-quently abused cannabis.
Conclusion
Young people use to combine various psychoactive sub-stances (>75% combine cannabis with alcohol drinkingand cigarette smoking) very frequently. Our researchrevealed a significant positive correlation towards poly-abuse of various psychoactive substances indicating anexistence of the genetic or phylogenetic liability towardsconcurrent polyvalent harmful substances abuse.It is conspicuous that parents support their children in apassive way to consume psychoactive substances (par-ents allow alcohol drinking: in children who smokecannabis - 38.9%; in children who do not abuse drugs -10.1%).
48 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
References
1. Loga, S. Sudska psihopatologija, Sarajevo; Fakultet kriminalisti~kih nauka, 1999: 70-98.
2. Sinanovi}, O. Ovisnost o drogama. Tuzla: Medicinski fakultet; Behrambegova medresa; 2001: 9-42, 131-
140.
3. Loga, S. Klini~ka psihijatrija. Sarajevo/Tuzla: Medicinski fakultet, 1999: 151-179.
4. Harold, I. Kaplan, Benjamin, J. Sadock, MD: Comprehensive Textbook of Psychiatry/ VII. 7th ed. Vol. 2
Chapter 33 Child Psychiatry, 2000: pgs: 2151-2169. Baltimore: Williams and Wilkins.
5. Lewis, M. eds. Child and Adolescent Psychiatry: A Comprehensive Textbook. 2nd ed. Baltimore;
Philadelphia; London etc. Williams & Wilkins Section VI/ Syndromes, 1996: page 736-751.
6. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders (4th ed).
Washington, DC, American Psychiatric Association, 1994.
7. Petraitis, J., Flay, B. R., Miller, T. D, Torpy, E. J., Greiner, B. Illicit Substance Use Among Adolescents: A
Matrix of Prospective Predictors. Substance Use and Misuse, No 33, 1999: pp. 2561-604.
8. Dignan, M. B., Steckler, A., Block, G. D. Prevalence of Health-Risk Behaviour among Seventh Grade stu-
dents in Carolina. South Med J, 2000 Mar: 79(3): 295-8, 302.
9. Magnusson, D., Stattin, H., Allen, V. Differential Maturation among Girls and its Relations to Social
Adjustment: A longitudinal Perspective, J Clin Psychiatry, 1999: 49: 3-6.
10. Gilligan, C., Lyons, N., Hanmer, T. Making Connections. Cambridge, Mass and London: Harvard
University Press, 1990.
11. Johnson, P. B., Boles, S. M., Kleber, H. D. The Relationship Between Adolescents Smoking and Drinking
and Likely Estimates of Illicit Drug Use. J Addict Dis; 19 (2), 2000: 75-81.

49Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Abstract
This study encompassed 77 randomly assigned partici-pants of both sexes and older than 65 of age. Every par-ticipant was questioned in his/her own house and com-pletely familiarized with the methodology and the aimsof the questionnaire. Out of 27 men, data on falls down were provided by 4participants (14.81%): one of them lived alone whilethree of them lived in their families. Out of 50 women,data on falls down were provided by 17 (34%) partici-pants: 9 of them lived in their families and 8 lived alone.Out of all living alone women 44% fell down twice ormore during this study in comparison to 20% of livingalone men.Regarding the values of the score of risk factors obtainedthroughout the questionnaire and the Berg balance scale,there are statistically significant differences between menand women (p < 0.005, i.e. p < 0.01), as well as partici-pants that have never fallen down (p < 0.001, i.e. p <0.01), while regarding the life style (living alone or in thefamily) there are no statistically significant differences (P> 0.05). Nowadays, the Berg balance scale is the mostfrequently used questionnaire that is, in total, significant-ly superior to other ever utilized tests.Average values of results obtained throughout the Bergbalance scale in this study are statistically significantlyhigher in men and those participants who did not providedata on falls down, while regarding the life style there areno statistically significant differences.Key words: risk factor of falling down, Berg balancescale, third age of life
Introduction
Rapid industrialization and urbanization, as well as rapidprogress in technique put third aged people on the mar-gin of interest of health institutions. On the other hand,the progress of civilization (improvement of general,economic, social and health condition, as well as betterworking conditions, progress in technique) causes pro-longed average lifetime. It is assumed that an averagelifetime of people in developed countries was approxi-mately 85 years of age (year 2000) (1). Body balance andmoving require a very complex relation between percep-tive, neuromuscular and cardiovascular functions, as wellas an ability of fast adaptation to the requirements of theenvironment. In biomechanical sense, human walk is
actually a loss and a regaining of the body balance in themanner that it is re-established before it would becomedisordered during the fall down. With age, body balanceis weakening while staggering process advances. Theresult of this is vulnerability that makes elderly personinclined to fall down when facing additional burden toany of the formerly mentioned functions. Thus, a simplefall down may result in serious problems such as pneu-monia or myocardial attack. Hypothetically, age weaken-ing of the sensory systems induces a rise in order tostrengthen the signals that come from these systems andeverything in order to ensure necessary information forthe control of the body posture (2).
Aim of the work
Aim of this work was to conduct a questionnaire aboutfall down risk factors and the Berg balance scale in orderto find out the co-relation between results of falls downrisk factors and the Berg balance scale.
Participants and themethods of research
The study was clinical and consisted of manipulative,prospective and control exams. The research itselfencompassed 77 randomly assigned participants of bothsexes, all older than 65 years. Each participant was ques-tioned in his/her own house and absolutely familiarizedwith methodology and aims of the research. Six monthlater, a control review was done and all participants weredivided into two groups: a group without falls down anda group with falls down. In this manner, the group with-out falls down presented a control group while the groupwith falls down presented a tested group. Research inclu-sion criteria were: age over 65 years and ability to movewith or without a device (stick). Research exclusion cri-teria were: death of the participant during the study orappearance of an illness that might affect participantfunctional ability during the research period. All patientswere examined by a physiatrist. There was a separatequestionnaire for the each participant about risk factors(Annex 1). The questionnaire consisted of 22 questions,which were rated in dichotomised manner ("yes" or"no"). The summary of positive answers presents the rel-ative index of fall down risk. This evaluation is based onthe observation of the researcher, patients' answers anddata from available medical documentation. The Berg
Co-relation between risk factors of falls down and theBerg balance scale in elderly people (third age)Avdiæ Dijana1, Škrbo Armin2
1 - Orthopaedic and Trauma Clinic "KCU Sarajevo"2 - Faculty of Pharmacy, Sarajevo

50 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
balance scale was conducted in each patient (3, 4, 5, 6)(Annex 2). Otherwise, the Berg balance scale consists of14 tasks being scored based on the previously set criteria.Primarily, the performance of each task was demonstrat-ed to each patient. The necessary equipment included astopwatch, centimetre tape, chair and armchair, as well asa small chair which height co-related to the averageheight of foot-lift while walking. Maximum Berg balancescale score is 56 and indicates an excellent body balance. Results were statistically analysed according to SPSSprogram version 9.0, and presented in tables and graphs.Following parameters were determined for each clinicaltest: frequencies and measures of central tendency, speci-ficity, sensitivity, positive and negative predictive value,percentage of false positive and false negative results. Ttest values indicate that all examined variables statistical-ly significantly differ. In order to uncover the individualvariables predictive for fall down, a logistic regressiveanalysis was performed while the depending variable wasrepresented by datum on fall down 0 (0 - no fall, 1 - witha fall).
Results
77 participants were included in the study: 27 men(35.06%) and 50 women (64.94%). Distribution of ques-tioned participants according to the sex is shown inGraph 1.
Graph 1 Distribution of questioned participantsaccording to the sex
Average age was 71.23 ± 5.63 (ranging from 65 to 90years): for women 71.22 ± 5.80 (ranging from 65 to 90years), and for men 72.67 ± 5.26 years (ranging from 65to 82 years). During the study period, 21 participants(27.27%) fell down twice or more times, while the samenumber of participants provided data on only one falldown. Out of 27 men, data on falls down were providedby 4 participants (14.81%) - one living alone and threeliving in their families. Out of 50 women, the data onfalls down were provided by 17 participants (34%) - 9 ofthem living in their families and 8 living alone. Data onfalls down, related to the sex and life style (living aloneor within a family), are shown in Table 1. Average value of the risk factor score gained throughoutthe questionnaire and the results of the Berg balancescale are shown in Tables 2-4.
50
27
Women Men
Table 1 Distribution of participants according to the data on falls down and related to the life style and sex
Fall (n) No fall (n) TOTAL (n) PARAMETER
M F MF M F MF M F MF Living alone 1 8 9 4 10 14 5 18 23 Living in a family 3 9 12 19 23 42 22 32 54 Total 4 17 21 23 33 56 27 50 77
Table 2 Average values of the risk factor score and the Berg balance scale according to the sex
PARAMETER Men Women Total
Risk factor score 2.59 ± 3.35 5.32 ± 3.71 4.36 ± 3.80
Berg balance scale 50.7 ± 13.8 42.5 ± 15.0 45.4 ± 15.0
Table 3 Average values of the risk factor score and the Berg balance scale according to the life style
PARAMETER Lives alone Lives in a family Total
Risk factor score 4.87 ± 3.75 4.15 ± 3.83 4.36 ± 3.80
Berg balance scale 44.6 ± 14.4 45.7 ± 15.4 45.4 ± 15.0
Table 4 Average values of the risk factor score and the Berg balance scale according to data on falls down
PARAMETER Fall No fall Total
Risk factor score 8.33 ± 3.07 2.88 ± 2.87 4.36 ± 3.80
Berg balance scale 35.5 ± 17.1 49.1 ± 12.4 45.4 ± 15.0

51Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Graph 2 Average value of the Berg balance scale
Regarding risk factor score gained throughout the ques-tionnaire and the Berg balance scale there are statistical-ly significant differences between men and women, aswell as between participants who fell down and thosewho did not, while there are no statistically significantdifferences regarding their life style (living alone or in afamily) (Tables 5-7).
Discussion
The study encompassed 77 participants of both sexeswith average life age of 71.73 ± 5.63 years (ranging from
65 to 90 years), who were randomly assigned. Everypatient was questioned in his/her house and was familiar-ized with the methodology and aims of the study. Thepercentage of women was 64.94% (50 female partici-pants) while the percentage of men was 35.06% (27 maleparticipants), which is in accordance with this populationgroup demographic data in our conditions. 1 In otherstudies, sex structure differs, so Harada and colleagues(7) stated that women represented 87% of participants intheir questioned group. Average value of the risk factor score and the Berg bal-ance scale were statistically significantly differentaccording to the sex and fall down data in contrast to thelife style.Clinical methods of evaluation that are in use nowadaysare especially suitable for the screening process sincethey can uncover specific damages and they can be car-ried out by both medical and previously trained non-med-ical staff (8). After such screenings, further expert evalu-ation is to be performed. In the practice, most usuallyused are following tests: Berg balance scale4, B-POMAtest (9) and "Get-up and Go" test (10, 11). There is excel-lent co-relation between these tests, but the Berg balancescale in overall superior in comparison to other two men-tioned tests (12).Shumway-Cook and colleagues (13) constructed a verysimple model for the prediction of fall down based on theBerg balance scale test results and data on body balancemalfunction. Sensitivity of that model is 91%, character-istics are 82%, which means that 20 out of 22 personsfrom the fall down group will be correctly classified, that
46,83
50,89
44,64 45,17
47,54
39,95
49,41
0
10
20
30
40
50
60
total men women alone family fall no fall
Table 5 Testing of the significance of the each test differences between men and women
PARAMETER T-test value Freedom degrees Stat. significance
Risk factor score 3.183 75 p < 0.005
Berg balance scale 2.346 75 p < 0.01
Table 6 Testing of the significance of the each test differences between participants who lived alone andthose who lived in the family
PARAMETER T-Test Value Freedom degrees Stat. significance
Risk factor score 0.761 75 N.S. p > 0.05
Berg balance scale 0.286 75 N.S. p > 0.05
Table 7 Testing of the significance of the each test differences between participants who fell down andthose who did not fall down
PARAMETER T-test value Freedom degrees Stat. significance
Risk factor score 7.298 75 p < 0.001
Berg balance scale 3.828 75 p < 0.001

52 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
is 18 out of 22 persons without data on falls down will becorrectly classified.The conclusion of authorswas that every third aged person with the Berg balance
scale score below 40 needed an adequate physical treat-ment.Average values of the results gained throughout the Bergbalance scale in this study are statistically significantlyhigher in men and participants who provided no dataabout falls down, while statistically significant differ-ences regarding the life style were not observed. Theseresults are co-relating to literature data (4, 8, 12, 13, 15).Many participants categorically stated that they could notperform some of the tasks (keeping body balance whileturning for 360 degrees), and for their performance, apartfrom the proper explanation, a longer verbal support wasneeded. This result is in accordance with the result ofStudenski and colleagues (16), who published that elder-ly people with recent fall down experience were moreunstable than people from the similarly aged controlgroup (performance of the postural test of one-leg stand-ing and turning around).The Berg balance scale did not reveal significant prob-lems in performing Romberg test, though the literatureproves two opposite opinions. Briggs and colleagues(17), differently from Heitmann and colleagues (18),have found no difference between the leaning time of thethird aged persons during the Romberg test performanceand one-leg standing in comparison to the data on fallsdown.
Conclusions
1. Regarding the risk factor score gained throughout thequestionnaire and the Berg balance scale results, thereare statistically significant differences between menand women (p < 0.005, i.e. p < 0.01), as well as par-ticipants who did not fall down (p < 0.001, i.e. p <0.01), while there are no statistically significant dif-ferences regarding the life style (alone or in family)(p > 0.05).
2. Clinical methods of evaluation that are in use nowa-days are especially suitable for the screening processsince they can uncover specific damages and they canbe carried out by both medical and previously trainednon-medical staff.
3. After such screenings, further expert evaluation is tobe performed.
4. The Berg balance scale is nowadays mostly used inthe practice and in overall superior in comparison tothe other tests that are being used.
5. Average values of the results gained throughout theBerg balance scale in this study are statistically sig-nificantly higher in men and in participants who pro-vided no data about falls down, while statistically sig-nificant differences regarding the life style were notobserved.

53Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
References
1. Gavranovi} M. and ass. Clinical Geriatrics. International Peace Centre, Sarajevo, 1997; 13-5.2. Stelmach GE, Zelaznik HN, Lower D. The influence of aging and attentive demands on recovery from
postural instability. Aging 1900; 2(2): 155-61.3. Berg K, Wood-Dauphinee S, Williams JI, et al. Measuring balance in the elderly: validation of an instru-
ment. Can J Public Health 1992; 73: 1073-80.4. Berg K, Wood-Dauphinee S, Williams JI, et al. Measuring balance in the elderly: preliminary development
of an instrument. Physiotherapy Canada. 1989; 41: 304-11.5. Berg K, Wood-Dauphinee S, Williams JI. The balance scale scale: assessment with elderly residents and
patients with acute strike. Scand J Rehabil Med 1995; 27(1): 27-36.6. Riddle DL, Stratford PW. Interpreting validity indexes for diagnostic tests: an illustration using the Berg
Balance Test. Phys Ther. 1999; 79:939-948. 7. Horak FB, Nashner LM, Diener HC. Postural strategies associated with somatosensory and vestibular loss.
Exp Brain Res. 1990; 82: 167-77.8. Harada N, Chiu V, Damron-Rodriquez J, et al. Screening for balance and mobility impairment in elderly
individuals living in residential care facilities. Phys Ther. 1995; 75(6): 462-9.9. Tinetti ME. Performance-oriented assessment of mobility problems in elderly patients. J Am Geriatr Soc.
1986; 34(2): 119-26.10. Mathias S, Nayak USL, Isaacs B. Balance in elderly patients: the "Get-up and Go" test. Arch Phys Med
Rehabil. 1986; 67: 387-9.11. Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling
older adults using the Timed Up & Go Test. Phys Ther. 2000;80:896-903. 12. Berg K, Maki B, Williams JI, et al. Clinical and laboratory measures of postural balance in an elderly pop-
ulation. Arch Phys Med Rehabil. 1992; 73: 1073-80.13. Shumway-Cook A, Baldwin M, Polissar LN, et al. Predicting the probability for falls in community-
dwelling older adults. Phys Ther. 1997; 77(8): 812-9.14. Berg K. Balance and its measure in the elderly: a review. Physiotherapy Canada. 1989; 41: 240-6.15. Raîche M, Hébert R, Prince F, Corriveau H. Screening older adults at risk of falling with the Tinetti bal-
ance scale. Lancet. 2000; 356 (9234): 1001-2.16. Studenski S, Duncan PW, Chandler J. Postural responses and effector factors in persons with unexplained
falls: results and methodological issues. J Am Geriatr Soc. 1991; 39: 229-34.17. Briggs RC, Gossman MR, Birch R, et al. Balance performance among non-institutionalized elderly
women. Phys Ther. 1989; 69: 748-56.18. Heitmann DK, Gossman MR, Shaddeau SA, Jackson JR. Balance performance and step width in non-insti-
tutionalized, elderly, female fallers and non-fallers. Phys Ther. 1989; 69: 923-31.

54 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Questionnaire
Name and Family Name:Age: Sex:Body Weight: Body Height: Blood Pressure:Lives alone: Lives in a family:Leading diagnosis (group of illnesses):Remark:
RISK FACTORS
1. For conduct of two or more activities(cooking, laundry wash, dressing, walking, …) help needed YES NO
2. For conduct of two or more manipulative activities(shopping, use of telephone, handling money, Taking medications,) help needed YES NO
3. Had fracture or malfunction of hip, knee or foot YES NO4. Has visible joint consequences of mentioned states YES NO 5. Uses a helping device for walking (stick, walker, …) YES NO6. Physical activity limited to basic house works YES NO7. Describes him/herself as a scared person YES NO8. Complaining of dizziness YES NO9. Complaining on troubles with balance YES NO10. Having complaints connected to postural hypotension YES NO11. Fell once or twice during this year YES NO12. Fell more than twice during this year YES NO13. Was any care needed after the fall? YES NO14. Did the fall(s) result in fracture? YES NO15. Is he/she generally afraid of falling? YES NO16. Afraid of falling in the house (bathroom, kitchen…) YES NO17. Afraid of falling outside (public transport, stairway, street…) YES NO18. Does he/she avoid leaving house for the fear of falling? YES NO19. Does he/she have 3 or more health malfunctions asking for regular health checks? YES NO20. Do these malfunctions require house visits by medical staff? YES NO 21. Does he/she have some of the following illnesses that might result in a fall? YES NO
• Neurological (e.g. cancer, peripheral neuropathy, multiple sclerosis, lupus…)• Cardiovascular (e.g. postural hypo tension)• Muscle-skeleton (e.g. total joint prosthetics implant)• Sensory (e.g. damages to sight)• Other (amputation, Parkinson disease, Alzheimer disease)
22. Does he/she take medications potentially dangerous from aspects of falling? YES NO• Antihypertensive agents• Narcoleptics• Hypnotics/anxiolytics• Antiarrhythmic agents• Antiparkinson agents• Analgesics/anti-inflammatory/anti-rheumatics• Vasoregulators
Total answers ___ ___

55Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
The Berg balance scale
The performance of each task is to be demonstrated to the patient. The necessary equipment included a stop-watch, centimetre tape, chair and armchair, as well as a small chair which height co-related to the average heightof foot-lift while walking. Maximum Berg balance scale score is 56 and indicates an excellent body balance.
Instructions for certain tasks:
1. Please stand up. Try that without leaning on your arms.2. Please stand for 2 minutes without holding onto anything.3. Please sit down for 2 minutes with your arms crossed.4. Please sit down.5. Please move from the armchair to the chair and then vice versa.6. Please close your eyes and stand still for 10 seconds.7. Please put your feet together and stand without holding onto anything.8. Please raise your hand (patient may choose which one) to 900. Stretch your fingers and touch forwards
as much as you can. Measurer will measure the distance from the starting position.9. Please from the standing position raise your slippers that are in front of you.10. Please turn around and look over your left and then over your right shoulder.11. Please turn for 3600. Make a short break and repeat it backwards.12. Please rise on the small chair with your both feet (first one foot than another).
Repeat four times with each foot.13. Please put one foot exactly in front of the other (patient may choose) or the heel of your foot as much as
it is possible in front of the other foot your toes as it does not affect your stability.14. Please stand without holding onto anything one leg (patient may choose) as long as it is possible.
NAME AND FAMILY NAME:DATE:EVALUATION: start
DESCRIPTION OF THE TASK SCORES (0-4)
1. Sitting to standing __2. Standing without holding __3. Sitting without holding __4. From standing to sitting __5. Transfers __6. Standing with eyes closed __7. Standing with feet together __8. Catching forward with stretched arm __9. Lifting items from the floor __10. Turning for looking back __11. Turning for 360 degrees __12. Putting another foot on a small chair __13. Standing with one leg in front of another __14. Standing on one foot __
TOTAL _____

56 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Abstract
Extensive and complete documentation must be present-ed for marketing authorization of a medicinal product inthe EU. Presented documentation should prove quality,safety and efficacy of the medicinal product. It is ensuredthat the applicant supplies the authorities with completeinformation. The legislation in Federation of Bosnia andHerzegovina has also taken more steps towards thoseEuropean directions.
The presentation and content of the dossier in theEuropean Union has been redefined. The "old" EU for-mat will be replaced with the Common TechnicalDocument (EU CTD format) agreed in 2000, within theInternational Conference on Harmonization framework.These two formats are intended to coexist during thetransition period until July 2003. The CTD is an interna-tionally agreed upon format for the preparation of a wellstructured presentation for applications to be submitted toregulatory authorities in the three ICH regions of Europe,US and Japan.
Key words: marketing authorization, application dossier,domestic laws
Introduction
The centralized and mutual recognition proceduresbecame applicable in the EU from 1995. In order toachieve the free movement of medicinal products withinthe Community, a Committee for the ProprietaryMedicinal Products is set up. The Committee has aresponsibility to examine any question relating to granti-ng, variation, suspension or withdrawal of marketingauthorization in EU. In order to obtain authorization toplace a medicinal product on the market, an applicationshall be made by the competent authority of the MemberState concerned, and followed by the particulars and doc-uments (1):
- Information about the applicant and, where applica-ble, about the manufacturer;
- Name of the medicinal product;- Qualitative and quantitative particulars of all the
constituents of the medicinal product;- Description of the manufacturing method;- Therapeutic indications, contraindications and
adverse effects;
- Posology, pharmaceutical form, method and route ofadministration and expected shelf life;
- Reasons for any precautions and safety measures,with an indication of any potential risk presented bythe medicinal product for the environment;
- Description of the control methods employed by themanufacturer;
- Results of the physical-chemical biological ormicrobiological tests, toxicological and pharmaco-logical tests, clinical tests;
- A Summary of the product characteristics, packag-ing and labelling information, with a packageleaflet;
- A document showing that the manufacturer isauthorized in his own country to produce medicinalproducts;
- Copies of the authorizations obtained in anotherMember State or in the third country, with a list ofMember States in which an application for authori-zation submitted is under examination, accompa-nied with particulars and information about thisprocess.
The European Commission and the European Agency forthe Evaluation of Medicinal Products published Therules governing medicinal products in the EuropeanUnion. Volume 2B in this series is dealing with the pres-entation and content of the application dossier.
Volume 2B was first published as a separate volume in1998. It provides guidance for the compilation of dossierfor applications for European marketing authorizations.This EU format of dossier will be replaced with newupdate in July 2003. Format of the Common TechnicalDocument (CTD) was internationally agreed upon for-mat for the preparation of a well-structured presentationfor applications to be submitted to regulatory authoritiesin the three ICH regions of Europe, US and Japan (3).
Correlation between old and newformat of the application dossier
According to the Common Technical Document applica-tion dossier should be presented in five Modules:
- Module 1, Administrative and prescribing informa-tion;
- Module 2, CTD Summaries;- Module 3, Quality;
Dossier for marketing authorization in the European UnionMaida Todi}Institute of Pharmacology, Clinical Pharmacology and Toxicology "Pavel Stern",Faculty of Medicine, University of Sarajevo,

57Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
- Module 4, Non-clinical study reports;
- Module 5, Clinical study reports.
The content of the Module 1 is defined in consultations
with authorities of the Member State, and Modules 2, 3,
4 and 5 are intended to be common for all regions. The
first Module is containing regional and national informa-
tion. The old EU format was composed of 4 parts. First
part includes administrative information, prescribing
information and Expert reports on the chemical, pharma-
ceutical and biological documentation, toxico-pharmaco-
logical documentation and clinical documentation. The
content of this Part is divided into Modules 1 and 2 of the
EU CTD format (table 1).
Table 1 Correlation between old and new way of presentation of the application dossier in the EU (Part I -Module 1 and 2) and FBiH
FB H Old EU format
(NTA, Vol. 2B Ed.1998)
EU CTD format
(NTA, Vol.2B, Ed.2001)
Code of legislation on
drugs, Marketing
authorization
PART I
SUMMARY OF THE DOSSIER
MODULE 1
ADMINISTRATIVE AND
PRESCRIBING INFORMATION
Application
Certificate of quality of the medicinal product, that proves authorization of the product in the country of manufacture and respecting the GMP rules
List of the countries where the authorization is obtained, with the current prices
Certificate of Manufacturers authorization for the name of the medicinal product
Package Leaflet text;
The way of safe disposal of expired drug
Comprehensive Table of Content
Application Form
Summary of Product Characteristics, Labelling and Package Leaflet
Information about the Experts
Specific Requirements for different types of applications
Annex 1, Environmental risk assessment
Annex 2, Orphan medicinal products/ Demonstration of significant benefit
MODULE 2
COMMON TECHNICAL
DOCUMENT SUMMARIES
The information from the Summaries is in the Expert reports on the chemical, pharmaceutical and biological documentation, toxicological-pharmacological documentation and clinical documentation, that are requested with the considered documentation
Administrative data and Table of Contents for remainder of the dossier
Summary of Product Characteristics, Packaging, Labelling and Package Leaflet
Expert Report on the chemical, pharmaceutical and biological documentation, with Product profile, Critical Assessment, Information on the Expert, Tabular Formats and the Written Summaries
Expert Report on the toxicological-pharmacological documentation, with Product profile, Critical Assessment, Information on the Expert, Tabular Formats, Tabular Overview and the Written Summaries
Expert Report on the clinical documentation, with Product profile, Critical Assessment, Information on the Expert, Tabular Formats and the Written Summaries
Overall Table of Contents of Modules 2,3, 4 and 5
Introduction
Quality Overall Summary
Non-clinical Overview
Clinical Overview
Non-clinical Summary (Pharmacology, Pharmacokinetics and Toxicology Written and Tabulated Summaries)
Clinical Summary (Summary of bio-pharmaceutics and associated analytical methods, of clinical pharmacology studies, clinical efficacy, clinical safety, Synopses of individual studies)

58 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
The qualitatively different approach can be seen inModule 1, which is including the Environmental riskassessment and Demonstration of significant benefit forOrphan medicinal products in the Annexes. A space forEnvironmental risk assessment describes present attitudein valuing drugs, regarding their influence on the envi-ronment. The task of this evaluation is to discus possiblerisks to the environment from the point of view of prod-ucts use and disposal, with proposition of measures forreducing this risk. In the EU format the Environmentalrisk assessment was divided and placed in Part II or III,depending on the presence of GMOs (genetically modi-fied organisms) in the medicinal product.
There is another change in organization of the dossier inModule 2. Here should be presented the CTDSummaries, prepared by suitably qualified Experts. Theclassical "Expert Report" known from the EU formatdoes not exist here. The term "Expert Report" is main-tained for legal reasons, but the information is given inthe form of Overviews and Summaries.
The Quality Overall Summary present information thatprovides an overview of Module 3, and discus key issuesthat support information from other Modules. The Non-clinical Overview is continuing with presentation ofassessment of the non-clinical evaluation. The quality of
batches of active substance used in this study should bediscussed, so as the effects seen with related products.The Clinical Overview should be a critical analysis of theclinical data. It should include: description of the overallapproach to the clinical development of the medicinalproduct, a brief overview of the clinical findings, an eval-uation of benefits and risks of the medicinal product in itsintended use, and description how the study results sup-port critical parts of the prescribing information.
The content of the Module 3, 4 and 5 is parallel to theinformation from Part 2, 3 and 4 of the EU format.Mentioned parts include chemical, pharmaceutical andbiological documentation, toxicological-pharmacologi-cal documentation and clinical documentation.
The scientific information from both versions of applica-tion dossier can be globally divided on: Quality, Non-clinical and Clinical information. The qualityPart/Module is dealing with the quality of the manufac-ture series and the characteristics of the used test samplesthat can affect the results of evaluation process (table 2).The information on bioequivalence was more present inthe pharmaceutical documentation of EU format and inEU CTD format is primary discussed inside of the clini-cal information and in Biopharmaceutical studies ofModule 5.
Table 2 Correlation between old and new way of presentation of the application dossier in the EU (Part II -Module 3) and in the FBiH
FB H Old EU format
(NTA, Vol. 2B Ed.1998)
EU CTD format
(NTA, Vol.2B, Ed.2001)
Code of legislation on
drugs, Marketing
authorization
PART II
CHEMICAL, PHARMACEUTICAL AND
BIOLOGICAL DOCUMENTATION
MODULE 3
QUALITY
Documentation on laboratory evaluation with Expert Report
Composition of medicinal product, Container, Clinical trial formulae, Development pharmaceutics Method of preparation Control of starting materials (Specifications, routine tests and Scientific data for Active substance and Excipients) Control tests of intermediates Control tests on the finished products (Specifications, routine tests and Scientific data) Stability Bioavaliability/Bioequivalence Data related to the environmental risk assessment for products containing genetically modified organisms (GMOs) Other Information
Module 3 table of contents Body of data Drug substance (General information, Manufacture, Characterization, Control of drug substance, Reference Standards or Materials, Container, Stability) Drug Product (Description and composition, Pharmaceutical Development, Manufacture, Control of excipients, Control of drug product, Reference Standards or Materials, Container, Stability) Appendices Regional Information Literature References
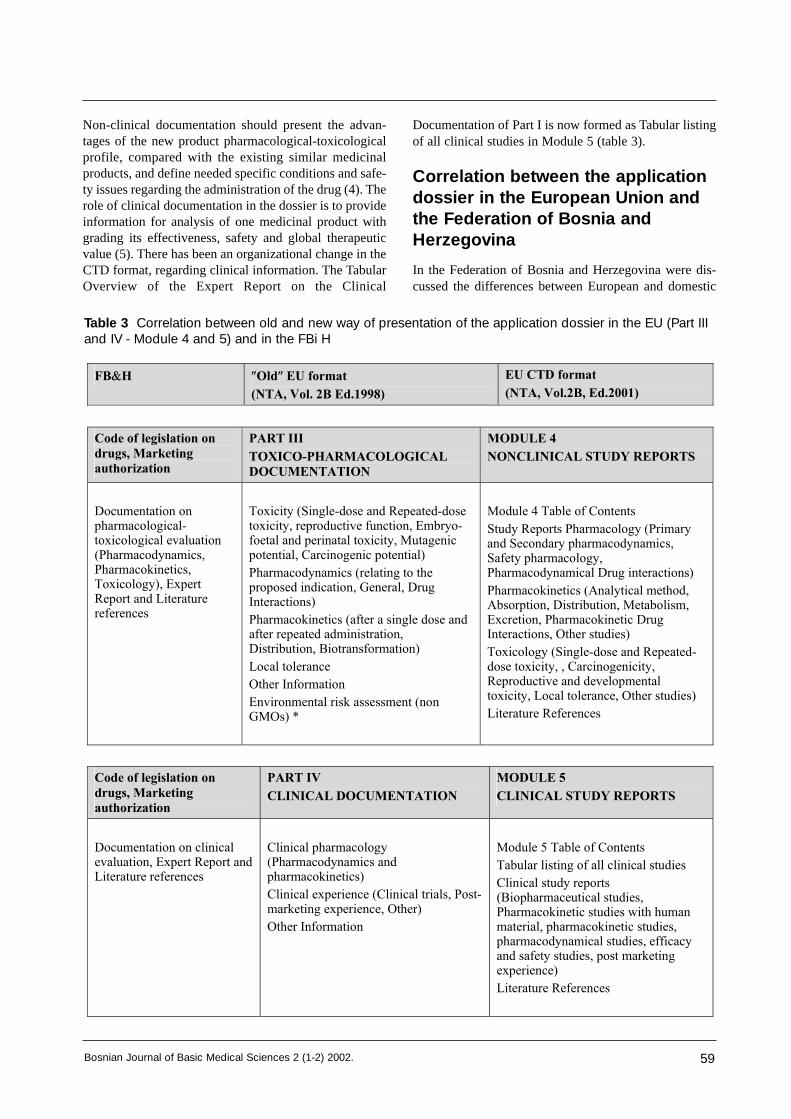
59Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Non-clinical documentation should present the advan-tages of the new product pharmacological-toxicologicalprofile, compared with the existing similar medicinalproducts, and define needed specific conditions and safe-ty issues regarding the administration of the drug (4). Therole of clinical documentation in the dossier is to provideinformation for analysis of one medicinal product withgrading its effectiveness, safety and global therapeuticvalue (5). There has been an organizational change in theCTD format, regarding clinical information. The TabularOverview of the Expert Report on the Clinical
Documentation of Part I is now formed as Tabular listingof all clinical studies in Module 5 (table 3).
Correlation between the applicationdossier in the European Union andthe Federation of Bosnia andHerzegovina
In the Federation of Bosnia and Herzegovina were dis-cussed the differences between European and domestic
Table 3 Correlation between old and new way of presentation of the application dossier in the EU (Part IIIand IV - Module 4 and 5) and in the FBi H
FB H Old EU format
(NTA, Vol. 2B Ed.1998)
EU CTD format
(NTA, Vol.2B, Ed.2001)
Code of legislation on
drugs, Marketing
authorization
PART III
TOXICO-PHARMACOLOGICAL
DOCUMENTATION
MODULE 4
NONCLINICAL STUDY REPORTS
Documentation on pharmacological-toxicological evaluation (Pharmacodynamics, Pharmacokinetics, Toxicology), Expert Report and Literature references
Toxicity (Single-dose and Repeated-dose toxicity, reproductive function, Embryo-foetal and perinatal toxicity, Mutagenic potential, Carcinogenic potential)
Pharmacodynamics (relating to the proposed indication, General, Drug Interactions)
Pharmacokinetics (after a single dose and after repeated administration, Distribution, Biotransformation)
Local tolerance
Other Information
Environmental risk assessment (non GMOs) *
Module 4 Table of Contents
Study Reports Pharmacology (Primary and Secondary pharmacodynamics, Safety pharmacology, Pharmacodynamical Drug interactions)
Pharmacokinetics (Analytical method, Absorption, Distribution, Metabolism, Excretion, Pharmacokinetic Drug Interactions, Other studies)
Toxicology (Single-dose and Repeated-dose toxicity, , Carcinogenicity, Reproductive and developmental toxicity, Local tolerance, Other studies)
Literature References
Code of legislation on
drugs, Marketing
authorization
PART IV
CLINICAL DOCUMENTATION
MODULE 5
CLINICAL STUDY REPORTS
Documentation on clinical evaluation, Expert Report and Literature references
Clinical pharmacology (Pharmacodynamics and pharmacokinetics)
Clinical experience (Clinical trials, Post-marketing experience, Other)
Other Information
Module 5 Table of Contents
Tabular listing of all clinical studies
Clinical study reports (Biopharmaceutical studies, Pharmacokinetic studies with human material, pharmacokinetic studies, pharmacodynamical studies, efficacy and safety studies, post marketing experience)
Literature References

60 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
rules for authorization, and some propositions that are inour country possibilities are adapted. In order to obtainmarketing authorization, Applicant is considered to sub-mit the following to the Regulatory authorities (2):
- Application with basic information aboutManufacturer and medicinal product;
- Documentation on clinical, pharmacological-toxico-logical and laboratory evaluation;
- Certificate of quality of the medicinal productaccording to the World Health Organization rulesfor quality of the products intended for internation-al trade, that proves authorization of the product inthe country of manufacture and that the manufactureprocess was by the rules of the Good manufacturepractice;
- List of the countries where the authorization isobtained, with the current prices;
- Certificate of Manufacturers authorization for thename of the medicinal product;
- Package Leaflet text;- The way of safe disposal of expired drug;- Manufacturers price of the medicinal product;- Samples of the medicinal product.
Conclusion
There are no substantial changes regarding the content of
old and new EU format, but the way of presentation and
organization of the files is redefined. The parts of the
dossier that describes in details all characteristics of the
medicinal product are more strictly defined in the EU
CTD format, so the new way of presenting information
has less space for improvisation.
If we compare the legislation of the content of the appli-
cation dossier in the EU and Federation no substantial
difference in the content of documentation is present. But
application and presented information about the medici-
nal product are more defined and extensive in the dossier
for European Union marketing authorization process.
Generally, our legislation is trying to keep step with EU.
One of the goals of our health management policy is to
develop the legislation in this segment that will corre-
spond to European standards.
References
1. European Commission, The rules governing medicinal products in the European Union, Volume 2, Noticeto applicants for marketing authorization for medicinal product for human use in the Member States of theEuropean Community, Official Journal of the European Communities, November 2001, http//pharmacos.eudra.org/F2/eudralex/vol-2/home.htm.
2. Parliament of Federation of Bosnia and Herzegovina: Code of legislation on drugs. Official Journal ofFederation of Bosnia and Herzegovina, November 2001, Sarajevo.
3. European Commission, The rules governing medicinal products in the European Union, Volume 2, Noticeto applicants, Volume 2B, Presentation and content of the dossier Common Technical Document (CTD),October 2001, Final- Revision 1, Brussels. http //pharmacos.eudra.org/F2/eudralex/vol-2/home.htm.
4. Velja~a M, Role of Expert Reports in Drug Registration in European Community- on Pharmaco-Toxicological Documentation, Medicus, 1997, Vol.6, No.1,121-4.
5. L.Brni} & T Ajhler, Role of Expert Reports in Drug Registration in European Community- on ClinicalDocumentation. Medicus, 1997, Vol.6, No.2, 271-5.

61Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Abstract
Experimental design is a critically important tool forimproving the performance of a manufacturing process.It has also extensive application in the development ofnew processes. It is important to investigate all factorsthat may be of importance and to not be overly influ-enced by past experience, particularly when we are in theearly stages of experimentation or when the process isnot very mature.
Key words: experimental design, experimentation, flu-idized bed
Introduction
The focus of many experiments in pharmaceutical tech-nology is on experiments in physico-chemical character-isation of active substances and excipients, technologicalprocess, drug stability and analysis, new product design,manufacturing process development, and processimprovement. Planning and conducting of the experi-ments and analysing the resulting data has its purpose inobtaining the valid and objective conclusions. In manycases, the objective may be to develop a robust process,that is, a process affected minimally by external sourcesof variability.
Experimental process
The overall experimental process can be divided into anumber of stages:
(1) statement of the problem• what is experiment supposed to achieve;
what is its objective?
(2) the choice of factors to be investigated, and thelevels of those factors which are to be used;
(3) the selection of suitable response • we must be sure that the measurement of the
chosen response will really contribute toachievement of the objective
• the accuracy of the proposed methods ofmeasuring the response must also be considered
(4) the choice of the experimental design• this is often a balance between cost and
statistical validity
• the more an experiment is replicated,the greater is the reliability of the results
• replication increases cost and the experimenter must therefore consider the acceptable degree of uncertainty;
• inextricably linked with this stage is selection of the method to be used to analyze the data
(5) performance of the experiment• the data collection process• this will follow the experimental
design laid down earlier
(6) data analysis• using methods defined earlier
(7) conclusions and recommendations
Too often, the objective of the experiment is imperfectlydefined. It is then discovered that the experimentaldesign is deficient and has provided insufficient and/orinappropriate data for the most effective form of analysisto be carried out. Thus the term "experimental design"must include not only the proposed experimentalmethodology but also the methods whereby the data fromthe experiments are to be analysed. The importance ofconsidering both parts of this definition together cannotbe overemphasized.
Examples
The most important variables for the possible granulationprocess in a fludized bed are given in this article. As wealready know, the granulation process in a fluidized bedis a complex process. There are many process variables(spray rate, inlet airflow rate, inlet temperature, inlet airhumidity, nozzle air pressure, nozzle height) (1) that caninfluence the granule properties. These variables havebeen studied extensively (2,3,4)
The most widely studied granule properties in the litera-ture are: geometric mean granule size, granule size dis-tribution, loose and tap density (Hausner index), granuleflow rate, and loss of drying. (5, 6, 7, 8, 9).
In the experiments on a small scale (10) were shown thatthe inlet temperature, the inlet airflow rate, the spray rateand the nozzle air pressure were the key process variablesdetermining the granule size.
Experimental design - basic considerationsEdina Vrani}Department of Pharmaceutical Technology, University of Sarajevo, Faculty of Pharmacy, ^ekaluša 90, Bosnia and Herzegovina

An increase in inlet temperature, airflow rate or nozzleair pressure reduced granule size whilst the spray rateincreased it. The effect of the inlet air humidity on thegranule size has not been investigated much yet. Oneexpects that an increase of the inlet air humidity willincrease the granule size, because it decreases the waterevaporation capacity of the inlet air and increases thepowder bed moisture content. The latter depends on theequilibrium between liquid supplied by the spray rate andthe inlet air humidity and the evaporation of liquid by theinlet airflow rate and the inlet air temperature. Someauthors (7,8,9) showed that the granule size depends onthe powder bed moisture content. If too much liquid isadded or the evaporation of the liquid is not adequatethan this results in an increase of the powder bed mois-ture content. Above a certain powder bed moisture con-tent the powder bed becomes overwetted and defluidizes(11).
At an increased inlet airflow rate, the powder bed deflu-idizes at higher moisture content due to the increaseddeformation force on the agglomerated granules exer-cised by the airflow.When the evaporation of the liquid is excessive becauseof high inlet flow rate and/or high inlet air temperature orlow supply of liquid by the spray rate, the powder bedmoisture content will be low and a spray dry process willbe obtained where the granule size depends essentially onthe droplet size of the binder (12).
The droplet size is mainly dependent on the nozzle airpressure and the spray rate. Therefore, the granule size isaffected by the following fundamental variables: powderbed moisture content, droplet size of the binder solutionand the deformation force exercised by the airflow. Thesevariables must be controlled between certain ranges inorder to produce granules of a desirable size.According to the disposed scientific references, the fol-lowing variables should be investigated in the design:
• spray rate, • inlet airflow rate, • inlet air temperature • the nozzle air pressure, • the droplet size of the binder solution• granule size distribution, • angle of repose, • loose and tap density (Hausner index), • angle of repose, • and loss on drying
Because of the complexity of the granulation process,experimental design is an appropriate way to investigateit. Experimental designs are widely used in pharmaceuti-cal science. Experimental designs dealing with the gran-ulation process have been applied in the studies (13,14)
Conclusion
Experimental design have found broad application inmany disciplines. In fact, we can view experimentationas part of the scientific process and as one of the ways welearn about how systems or process work. Generally, welearn through a series of activities in which we makeabout a process, perform experiments to generate datafrom process, and then use the information from theexperiment to establish new conjectures, which lead tonew experiment.
Experimental design is a critically important tool forimproving the performance of a manufacturing process.It has also extensive application in the development ofnew processes. The application of experimental designtechniques early in process development can result in:
• improved process yields• reduced variability and closer conformance to
nominal or target requirements• reduced development time• reduced overall costs
The experimenter must choose the factors to be varied inthe experiment, the ranges over which these factors willbe varied, and the specific levels at which runs will bemade. Thought must also be given to how these factorsare to be controlled at the desired values and how theyare to be measured. It is necessary to choose the region ofinterest for each variable (that is, the range over whicheach factor will be varied) and on how many levels ofeach variable to use. Process knowledge is required to dothis.
This process knowledge is usually a combination of prac-tical experience and theoretical understanding. It isimportant to investigate all factors that may be of impor-tance and to not be overly influenced by past experience,particularly when we are in the early stages of experi-mentation or when the process is not very mature.
62 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.

63Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
References
1. Mehta, A.M. Scale-Up Considerations in the Fluid-Bed Process for Controlled-Release Products. Pharm.Tech. 1988; 12: 46-52
2. Lipps, M., Sakr, A.M. Characterization of wet granulation process parameters using response surfacemethodology, 1. Top spray fluidized bed. J. Pharm. Sci. 1994; 83: 937-947
3. Miyamoto, Y., Ogawa, S., Miyajima, M., Sato, H., Takayama, K., Nagai, T. An evaluation of process vari-ables in wet granulation. Drug Dev. Ind. Pharm. 1995; 21: 2213-2225
4. Juslin, L., Ylirusi, J. The effect of raw material and atomizing air pressure on the properties of granulesprepared in a fluidized bed granulator. S.T.P. Phrama. 1996; 6: 328-334
5. Dussert, A., Chulia, D., Jeannin, C., Ozil, P. Parametric study of fluidized-bed granulation of a low densitymicronized powder. Drug Dev. Ind. Pharm. 1995; 21: 1439-1452
6. Vojnovic, D., Moneghini, M., Rubessa, F. Experimental design for a granulation process with "a priori" cri-terias, Drug Dev. Ind. Pharm. 1995; 21: 823-831
7. Watano, S., Morikawa, T., Miyanami, K. Mathematical model in the kinetics of agitation fluidized bedgranulation. Effects of humidity content, damping speed and operation time on granule growth rate. Chem.Pharm. Bull. 1996; 44: 409-415
8. Watano, S., Fukushima, T., Miyanami, K. Heat transfer and granule growth rate in fluidized bed granula-tion. Chem. Pharm. Bull. 1996; 44: 572-576
9. Watano, S., Takashima, H., Sato, Y., Yasutomo, T., Miyanami, K. Measurement of humidity content by IRsensor in fluidized bed granulation. Effects of operating variables on the relationship between granulehumidity content and absorbance of IR spectra. Chem. Pharm. Bull. 1996; 44:1267-1269
10. Rambali, B., Baert, L., Thone, D., Massart, D. L. Using experimental design to optimize the granulationprocess in fluid bed. Drug Dev. Ind. Pharm. 2001; 27: 53-61
11. Parikh, D.M., Bonck, J.A., Mogavero, M. Batch fluid bed granulation. In: Parikh, D.M. (Ed.), Handbook ofpharmaceutical granulation technology. Marcel Dekker, Inc., New York, 1997: pp. 227-302
12. Schaefer, T., Worts, O. Control of fluidized bed granulation. V. Factors affecting granule growth. Arch.Pharm. Chem. Sci. 1978; 6: 69-82
13. Gordon, M.S. Process considerations in reducing tablet friability and their effect on in vitro dissolution.Drug Dev. Ind. Pharm. 1994; 20: 11-29
14. Merkku, P., Lindqvist, A.S., Leiviska, K., Yliruusi, J. Influence of granulation and compression processvariables on flow rate of granules and on tablet properties, with special reference to weight variation. Int.J. Pharm. 1994; 102: 117-125

64 Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.
Submission: Only papers written in correct English areconsidered. Manuscripts must be typewritten in triplicate(with three sets of illustrations of which ones is an origi-nal), double spaced on one side of the paper with a 2,5cm wide margin on top, bottom and both sides, accom-panied by the identical file on a diskette.
Original research papers: Submitted manuscriptsshould be fully documented reports of original research.They must contain significant and original observationsto be critically evaluated.
Short communications: These manuscripts shouldnot exceed 2 printed pages (i.e. 5 manuscript pages),including an abstract essential references and not more 3tables or figures. Short communications should representcomplete, original studies and should be arranged in thesame way as full length manuscripts.
Leading articles and editorials are solicited by theEditorial Board with the aim to bring to the general read-ership pressing topics in life sciences and related envi-ronmental and bioethical dilemmas.
Review articles and viewpoints: Authors who wishto contribute a manuscript to this category are encour-aged to contact the Editor-in-Chief. Reviews should befocused on topics of current interest. View-points shouldoffer a more personalized perspective on a topic that willbe of interest to the general readership. All contributionsto those categories will be subject to editorial review.
Commentaries and letters to the Editor concerningwork published in the journal may also be submitted.They should not exceed 2 manuscript pages includingone table or figures.
CONDITIONS: All manuscripts will be reviewed by theeditor and two referees in order to expedite review,authors may suggest three to five potential reviewerswith their addresses. Manuscripts are received with theexplicit understanding that they are not under simultane-ous consideration by any other publication. A cover letterwith the name, postal address, postal code, telephone, faxand E-mail numbers of the corresponding author mustaccompany each manuscript. This letter must include astatement confirming that all authors concur with thesubmission. The contents of BOSNIAN JOURNAL OFMEDICAL SCIENCES may be reproduced without per-mission provided that credit is given to the journal. It isthe author’s responsibility to obtain permission to repro-duce illustrations, tables, etc. from other publications.
One of the criteria considered in reviewing manuscriptsis the proper treatment of animals. In particular, the useof painful or otherwise noxious stimuli must be carefullyand thoroughly justified. Papers that do not meet thesecriteria will not be accepted for publication.
Preparation of manuscripts
First page - A concise but informative full title of thearticle. Avoid abbreviations and colloquialisms.
Second page -A condensed title (running title) of nomore than 70 letters and spaces. Name(s) of author(s).Write first names in full. Complete address of the laboratory (institution) for eachauthor.
Third page - footnotes to the title, if any. List of anynon-standard abbreviations.
Fourth page - An Abstract (no more than 250 words)must be divided into four separate sections: backgroundand purpose, materials and methods, results and conclu-sions, and should be a factual condensation of the entirework including a statement of its purpose, a cleardescription of the findings and finally a concise presenta-tion of conclusions.
Content of manuscript
Number the remaining pages consecutively and type theauthor’s(s) last name(s) at the top of each page. Write inthe first person (except summary) and the active voicewhenever possible.
Keep the INTRODUCTION brief, stating clearly the pur-pose of the article and its relation to other papers on thesame subject. Do not give an extensive review of litera-ture.
Provide enough information in the MATERIAL ANDMETHODS section to enable other investigators torepeat the experiments.
Report RESULTS clearly and concisely. Do not presentthe same results in tables and illustrations. Exceptionally,results and discussion can be combined in a single sec-tion.
In the DISCUSSION interpret the results, state theirmeaning and draw conclusions. Do not simply repeat theresults.
Start each section on a separate sheet.
Instructions for preparation of manuscripts to be published inextenso in Bosnian Journal of Basic Medical Sciences

SUPPLEMENTS TO MANUSCRIPT
Footnotes: Avoid footnotes
Tables and illustration: Tables and illustrations (bothnumbered in Arabic numerals) should be prepared onseparate sheets. Tables require a heading, and figures alegend. Only good drawings and original photographscan be accepted: negatives or photocopies cannot beused. On the back of each illustration, indicate its num-ber, the author’s name, and “top”.Colour illustrations can now be integrated within the textand are reproduced at the author’s expense. Each tableand illustration must have all the necessary informationto be understood independently of the text.
Submit a drawing twice the final size. Lettering and iden-tifying marks should be clear and eligible after reduction.We prefer either an original drawing in India ink on whitedrawing or tracing paper or an electronic printout.Submit glossy prints of good quality. Write lightly in pen-cil the author’s name and figure number (indicate top) onthe back of each illustration.
Abbreviations: Introduce an abbreviation only whenthe same term occurs three or more times.
References: References are to be cited on a separatepage at the end of the article, numbered according to thecitation order from the text, and marked by Arabicnumerals in brackets. A citation in the text is marked bythe reference related number. All authors are mentioned,if six or less, while if more than six, only three first onesare cited adding et al. Type references on a separate sheet.Cite in sequence authors names and initials, title of arti-cle, name of journal, year of publication, volume numberof journal, and first and last pages.The surnames of the authors followed by initials shouldbe given. There should be no punctuation other than com-mas to separate the authors.Abbreviate journal titles according to the InternationalList of Periodical Title Word Abbreviations, CurrentContents or according to Index Medicus. Material sub-mitted for publication but not yet accepted should benoted as unpublished data and not included in the refer-ence list.
Example for journal citation:Lucin P., Jonji} S. Cytomegalovirus replication cycle. Anoverview. Period biol. 1995; 97:13-26.
Example for book citation:Hukovi} S., Potkonjak D., Zuli} I. Op{ta i specijalna far-makologija sa toksikologijom, Svjetlost, Sarajevo, 1988.
65Bosnian Journal of Basic Medical Sciences 2 (1-2) 2002.