ecmo in endocrine emergency
TRANSCRIPT
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 181SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
wwwnaturecomscientificreports
Highlighting Indication of
extracorporeal membrane
oxygenation in endocrine
emergenciesAnne Chao1 Chih-Hsien Wang2 Hao-Chun You2 Nai-Kwoun Chou2 Hsi-Yu Yu2Nai-Hsin Chi2 Shu-Chien Huang2 I-Hui Wu2 Li-Jung Tseng2 Ming-Hsien Lin2 amp Yih-Sharng Chen2
Extracorporeal membrane oxygenation (ECMO) has been repeatedly used to rescue patients with
cardiopulmonary arrest However its clinical utility in endocrine emergencies remains unclear
Herein we describe a case series of 12 patients presenting with refractory shock secondary to
endocrine emergencies who were rescued by ECMO support Patients were identied between 2005
and 2012 from our ECMO registry The diagnostic distribution was as follows pheochromocytoma
crisis (n= 4) thyroid storm (n= 5) and diabetic ketoacidosis (n= 3) The initial presentation of
pheochromocytoma crisis was indistinguishable from acute myocardial infarction (AMI) and
frequently accompanied by paroxysmal hypertension and limb ischemia Thyroid storm was
characterized by hyperbilirubinemia and severe gastrointestinal bleeding whereas neurological
symptoms were common in diabetic ketoacidosis The clinical outcomes of patients with endocrine
emergencies were compared with those of 80 cases with AMI who received ECMO because of
cardiogenic shock The cardiac function and the general conditions showed a signicantly faster
recovery in patients with endocrine emergencies than in those with AMI We conclude that ECMO
support can be clinically useful in endocrine emergencies The screening of endocrine diseases should
be considered during the resuscitation of patients with refractory circulatory shock
Extracorporeal membrane oxygenation (ECMO) is a treatment used to temporarily replace the unctiono the heart andor lungs over an extended period o time to allow or organ recovery Several studies havereported the successul use o ECMO to rescue patients with cardiopulmonary arrest in a wide spectrumo different etiologies including acute respiratory distress syndrome1 drug intoxication2 acute myocardi-tis3 burns4 acute myocardial inarction (AMI)5 post-cardiotomy shock 6 and severe cardiomyopathy 78
Endocrine emergencies ndash including pheochromocytoma crisis (PC) thyroid storm (S) and dia-betic ketoacidosis (DK) ndash are rare but potentially lie-threatening conditions i not recognized early andmanaged properly Te treatment o endocrine emergencies remains challenging even with the arma-mentarium o modern intensive care technologies especially in patients with cardiopulmonary ailureand major organ dysunction Although ECMO may provide mechanical pulmonary and circulatorysupport in patients reractory to conventional therapies to date only a ew cases o its use in endocrineemergencies have been reported in the literature9ndash16 Herein we describe a case series o 12 patientspresenting with reractory shock secondary to endocrine emergencies who were successully rescued by
1Department of Anesthesiology National Taiwan University Hospital College of Medicine National Taiwan
University Hospital Taipei Taiwan 2Department of Surgery National Taiwan University Hospital College of
Medicine National Taiwan University Hospital Taipei Taiwan These authors contributed equally to this work
Correspondence and requests for materials should be addressed to Y-SC (email yschen1234gmailcom)
Received 26 March 2015
Accepted 28 July 2015
Published 24 August 2015
OPEN
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 28
wwwnaturecomscientificreports
2SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
ECMO support We also compared their clinical outcomes with those o 80 cases with AMI who receivedECMO because o cardiogenic shock
MethodsStudy approval was obtained by our Institutional Review Board (No 201404079 RIN) which waivedthe requirement or inormed consent because o the retrospective nature o the study Among thepatients aged 16 years or older who received ECMO and reported to our hospital-based ECMO registryduring the period January 2005ndashDecember 2012 we retrospectively reviewed the data o those whopresented with reractory shock due to endocrine emergencies Te indications or ECMO included
catecholamine-reractory shock and ailed conventional cardiopulmonary resuscitation Te circuit andmanagement o ECMO have been described previously 58 Following completion o ECMO presumeddiagnoses were confirmed by reviewing all o the clinical and laboratory data Because some cases wereinitially incorrectly diagnosed a careul analysis o all clinical records was perormed beore includingthe patient in the study
We identified 12 cases presenting with reractory shock secondary to endocrine emergencies success-ully rescued by ECMO support Te diagnostic distribution was as ollows PC (n= 4) S (n= 5) andDK (n= 3) PC was identified through plasma and urinary catecholamines and metanephrines testingand imaging confirmation o adrenal lesions compatible with pheochromocytoma S was diagnosed onthe basis o serum thyroid hormone levels and traditional signs and symptoms o a thyrotoxic state Tediagnosis o DK was made in presence o uncontrolled hyperglycemia metabolic acidosis and increasedtotal blood ketone concentrations either with or without a history o type 1 diabetes mellitus Te ol-lowing variables were collected in all participants age sex initial clinical presentation final diagnosistime taken to identiy the etiology initial sepsis-related organ ailure assessment (SOFA) score17 ECMO
duration pre- and post-ECMO inotropic equivalent (IE= dopaminetimes 1+ dobutaminetimes 1+ norepi-nephrinetimes 100+ epinephrinetimes 100 all expressed in micro gkgmin) post-ECMO blood pressure valuesbiochemical data hormone levels and length o stay in the intensive care unit Te main outcome meas-ures included neurological conditions at discharge survival duration o ECMO and the occurrence ocomplications afer ECMO Because the clinical presentation o several patients with endocrine emer-gencies closely resembled AMI we compared their general characteristics and outcomes with those o 80cases with AMI (aged le 65 years) who received ECMO because o cardiogenic shock
ResultsTe flow o patients through the study is depicted in Fig 1 During the period January 2005ndashDecember2012 a total o 1180 patients were rescued with ECMO [1027 with veno-arterial (VA) ECMO and 153with veno-venous (VV) ECMO] according to our registry data We identified 12 patients presenting withreractory shock secondary to endocrine emergencies (PC n= 4 S n= 5 and DK n= 3) who wererescued by ECMO support Te clinical outcomes o patients with endocrine emergencies were com-
pared with those o 80 cases with AMI who received ECMO because o cardiogenic shock Endocrineemergencies represented 1 o all cases treated with ECMO (12 o VA ECMO) Te clinical course ispresented separately or each endocrine emergency
Pheochromocytoma crisis We identified our patients with PC Te presentation o PC mimickedAMI with palpitations chest pain abnormal electrocardiographic findings and elevations o cardiacenzymes (ables 1 and 2) Not surprisingly most patients with PC were initially misdiagnosed as havingan acute coronary syndrome Tree PC patients (PC-1 PC-2 and PC-4) had a bystander-witnessedout-o-hospital cardiac arrest and ECMO was initiated during cardiac pulmonary resuscitation (CPR)in the emergency department Patient PC-3 presented with an intractable cardiogenic shock requir-ing ECMO to allow or organ recovery Paroxysmal hypertension was identified in all o these patientsollowing ECMO implantation All o the patients in the PC group underwent coronary angiographyPatients PC-1 PC-2 and PC-3 had normal coronary angiography which led to the suspicion o pheo-chromocytoma Because o a 50 stenosis in the lef circumflex artery patient PC-4 was initially treated
as having an AMI and weaned off ECMO support afer 48 h under stable hemodynamic conditions Anepisode o pulseless ventricular tachycardia occurred 2 h later requiring resumption o CPR and ECMOBecause o the extreme blood pressure fluctuations a diagnosis o PC was suspected Patients PC-1 andPC-3 experienced a severe lower leg compartment syndrome despite placement o a distal perusioncatheter to prevent limb ischemia In patient PC-1 the emoral-emoral VA ECMO was converted toa central ECMO afer median sternotomy avoiding urther worsening o limb ischemia Patient PC-3underwent a below-knee amputation o the lef leg Te patients received abdominal computed tomog-raphy scans to localize the tumor and confirm the diagnosis All PC patients underwent adrenalectomyafer discharge rom the intensive care unit the only exception being PC-4 who reused surgery
Thyroid storm Five patients with S were identified throughout the study period All o them hada history o hyperthyroidism the only exception being S-1 (in whom S was suspected because onormal angiographic findings) Most patients with S were initially misdiagnosed as having AMI orsevere congestive heart ailure Teir rapid clinical deterioration required emergency ECMO supportHyperbilirubinemia was evident in all o the S patients whereas patient S-2 and S-4 developed
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 38
wwwnaturecomscientificreports
3SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
massive gastrointestinal bleeding Under ECMO support and anti-thyroid drug therapy the cardiac unc-tion o our o the 5 S patients started recovering between day 3 and day 4 Tey were subsequentlyweaned off ECMO Patient S-1 died o multi-organ ailure while receiving ECMO whereas patient S-2
eventually died o liver ailure Patient S-4 suffered rom Gravesrsquo ophthalmopathy resulting in exposurekeratopathy o the lef eye which eventually required penetrating keratoplasty
Diabetic ketoacidosis All o the three patients with DK were ound unresponsive at home PatientsDK-1 and DK-3 had a diagnosis o type 1 diabetes mellitus but their compliance with insulin therapywas poor Patient DK-2rsquos relatives denied any known medical history Patients DK-1 and DK-2 wereadmitted to the emergency department with out-o-hospital cardiac arrest Patient DK-3 required ECMObecause o proound hypothermia and hypotension unresponsive to aggressive fluid replacement andhigh-dose catecholamine administration Te presence o uncontrolled hyperglycemia metabolic aci-dosis and increased total blood ketone concentrations led to a diagnosis o DK Because patient DK-1was also diagnosed with community-acquired pneumonia that progressed to acute respiratory distresssyndrome both VA and VV ECMO support were indicated VA and VV ECMO were stopped 200 h and381 h afer initiation respectively Te patient eventually developed gangrene o the distal parts o all ourlimbs and died o septic shock and multiple organ ailure Spontaneous circulation in patient DK-2 did
not return despite ECMO support Patient DK-3 was successully resuscitated and eventually recovered
Comparison between endocrine emergencies and AMI PC and S were requently undistin-guishable rom AMI at presentation Despite lower sepsis-related organ ailure assessment (SOFA) scoresin the AMI group heart unction and clinical outcomes did not differ significantly rom those o patientswith endocrine emergencies AMI patients required higher doses o inotropic agents to stabilize theirhemodynamic status and their lef ventricular ejection unction remained poor Te ECMO weaningsuccess rates or patients with AMI and endocrine emergencies were 70 and 83 respectively Patientswith AMI required the ollowing subsequent interventions coronary bypass surgery (n= 26) repair oa ruptured ventricular septal deect (n= 4) implantation o a lef ventricular assist device (n= 3) car-diorrhaphy ollowing removal o ECMO and heart transplantation (n= 1) Te neurological outcomesdid not differ significantly between the two groups Eighty percent o the patients who survived an AMIhad a cerebral perormance category (CPC) score o 1 which was ound in 83 o those who survivedan endocrine emergency (able 3)
Figure 1 Flow diagram of patients with endocrine emergencies who were rescued by extracorporeal
membrane oxygenation Abbreviations ARDS acute respiratory distress syndrome AMI acute myocardial
inarction CMP cardiomyopathy DK diabetic ketoacidosis ECMO extracorporeal membrane oxygenationPCS post-cardiotomy shock PE pulmonary embolism PC pheochromocytoma crisis PH pulmonaryhypertension S thyroid storm x lung transplantation VA veno-arterial VV veno-venous
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 48
wwwnaturecomscientificreports
4SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
CaseAge(y) Sex Initial presentation Past history Initial diagnosis
Day ofdiagnosis Endocrine data Survival
Pheochromocytoma crisis Urine VMADopaEpiNE
PC1 25 F Dyspnea palpitations cold sweats Myocarditis AMImyocarditis 28 1531851283 Yes
PC2 52 M Chest pain Hypertension AMI 6 207217146858 Yes
PC3 40 M Chest pain Hypertension AMI 3 64349833342162 Yes
PC4 65 M Chest pain palpitations HBV carrier AMI 4 11278791208 Yes
Diabetic ketoacidosis Blood glucoseketone bodies
DK1 16 F Fever loss o consciousness 1DM Septic shock 1 770+ No
DK2 34 M Fever drowsiness Nil Septic shock 1 150559 No
DK3 28 F Loss o consciousness 1DM DK 1 99436 Yes
Tyroid storm Free 43SH
S1 47 M Palpitations exertional dyspnea Gout AMI 3 426927004 No
S2 43 M DyspneaGravesrsquo disease alcohol
liverTyroid stormCHF 4 242237003 No
S3 37 FDry cough night sweating alteration
o consciousnessGravesrsquo disease CHF 1 75-003 Yes
S4 42 MPalpitations dyspnea nausea
deliriumGravesrsquo ophthalmopathy Tyroid storm 1 24722lt 001 Yes
S5 33 F Fever shortness o breath Hyperthyroidism Tyroid storm 1 45425lt 001 Yes
Table 1 Demographic and clinical characteristics of patients with endocrine emergencies who were
rescued by extracorporeal membrane oxygenation Abbreviations M male F emale y years HBVhepatitis B virus AMI acute myocardial inarction 1DM type 1 diabetes mellitus CHF congestive heart
ailure Dopa dopamine (normal range 50ndash450 micro gmiddotday minus1) Epi epinephrine (normal range lt 224micro gmiddotday minus1)NE norepinephrine (normal range 121ndash855 micro gmiddotday minus1) ree 4 thyroxine (normal range 089ndash176 ngdL) 3 triiodothyronine (normal range 84ndash172 ngdL) SH thyroid-stimulating hormone (normal range
04ndash4micro IUmL) VMA vanillomandelic acid (normal range 1ndash7 mgmiddotday minus1)
PC (n= 4) DK (n= 3) TS (n= 5)
SOFA score (range) 13 (9ndash18) 137 (8ndash17) 15 (13ndash18)
Extracorporeal cardiopulmonaryresuscitation n 3 2 3
Inotropic index microgkgmin 283 568 355
IABP n 2 1 2
pH (range) 730 (71ndash736) 712 (663ndash739) 724 (714ndash739)
Blood lactate mmolL (range) 103 (87ndash11) 625 (50ndash75) 96 (35ndash12)
Initial CK UL (range) 15725 (501ndash3796) 2253 (348ndash2576) 7143 (259ndash1574)
Initial CK-MB UL (range) 862 (15ndash290) 211 (14ndash32) 426 (21ndash75)
Initial troponin-I micro gL (range) 370 (09ndash79) 058 (05ndash07) 035 (002ndash11)
Serum sodium mEqL (range) 1413 (138ndash144) 1463 (131ndash155) 143 (128ndash149)
Serum BUN mgdL (range) 169 (14ndash249) 471 (375ndash524) 294 (196ndash755)
Serum creatinine mgdL (range) 21 (08ndash28) 23 (21ndash26) 16 (11ndash240)
Serum bilirubin mgdL (range) 09 (04ndash140) 067 (012ndash15) 72 (26ndash1450)
Serum AS UL (range) 6435 (52ndash2183) 109 (15ndash239) 24645 (195ndash6195)
Serum AL UL (range) 6572 (47ndash2183) 43 (10ndash73) 761 (44ndash2267)
Table 2 Clinical characteristics of patients with endocrine emergencies at the time of ECMO
implantation Abbreviations AS aspartate aminotranserase AL alanine aminotranserase BUNblood urea nitrogen CK creatine kinase DK diabetic ketoacidosis IABP intra-aortic balloon pump PCpheochromocytoma crisis SOFA sepsis-related organ ailure assessment S thyroid storm
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 58
wwwnaturecomscientificreports
5SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
PC (n= 4) DK (n= 3) TS (n= 5) AMI (n= 80)
Age years (range) 455 (25ndash65) 26 (16ndash34) 404 (33ndash47) 538 (31ndash65)
Male sex n () 3 (75) 1 (333) 3 (60) 75 (94)
CPR n () 3 (75) 2 (66) 3 (60) 55 (687)
ECMO duration hour (range) 1025 (447ndash1625) 1345 (09ndash3818) 82 (19ndash1156) 117 (54ndash475)
Ventilator support day (range) 14 (6ndash22) 177 (1ndash51) 10 (4ndash26) 177 (1ndash95)
ICU length o stay day (range) 208 (6ndash28) 180 (0ndash51) 118 (5ndash26) 216 (1ndash147)
Initial SOFA score (range) 13 (9ndash18) 137 (8ndash17) 15 (13ndash18) 104 (3ndash18)
MAP Day 1 mmHg (range) 120 (101ndash137) 97 (96ndash99) 84 (63ndash101) 74 (30ndash144)
Day 3 (range) 121 (91ndash146) 85 (84ndash86) 113 (104ndash126) 76 ( 920ndash112)
Day 6 (range) 130 (116ndash145) 99 (99) 114 (93ndash132) 88 (61ndash118)
Pre-ECMO IE micro gkgmin 283 568 355 214
IE day 3 (range) 47 (21ndash70) 324 (324) 46 (0ndash184) 241 (0ndash810)
IE day 6 (range) 14 (0ndash54) 115 (115) 0 (0) 82 (0ndash318)
Patients using inotropes at day 6n ()
1 (25) 1 (33) 0 (0) 50 (625)
Initial CK UL (range) 15725 (501ndash3796) 2253 (348ndash2576) 714 (259ndash1574) 2413 (41ndash28480)
CK day 3 (range) 14589 (1528ndash47829) 385 (385) 83645 (515ndash4446) 58084 (77ndash66274)
CK day 6 (range) 22637 (530ndash13721) 4496 (4496) 501 (114ndash888) 31634 (33ndash36621)
Initial CK-MB UL (range) 862 (15ndash290) 211 (14ndash32) 426 (21ndash75) 172 (42ndash23198)
CK-MB day 3 (range) 3892 (909ndash10031) 522 (522) 535 (396ndash646) 1321 (15ndash1782)
CK-MB day 6 (range) 66 (157ndash207) 26 (26) 451 (407ndash494) 504 (12ndash3089)
Initial n-I microgL (range) 370 (9ndash79) 058 (05ndash07) 035 (002ndash11) 19 (001ndash100)
n-I day 3 (range) 161 (94ndash244) 04 (04) 12 (05ndash18) 377 (044ndash94)
n-I day 6 (range) 22 (126ndash31) Not available Not available 161 (031ndash33)
Lactate in 24 h mmolL (range) 103 (87ndash11) 625 (50ndash75) 96 (35ndash12) 89 (1ndash35)
Dialysis patients n 3 1 1 36
IABP (at implantation) 2 1 1 25 (32)
Bilirubin day 3 mgdL (range) 13 (10ndash19) 09 (09) 106 (20ndash248) 25 (04ndash122)
Bilirubin day 6 (range) 17 (14ndash18) 55 (55) 195 (567ndash269) 35 (06ndash213)
LVEF day 2 (range) 377 (30ndash43) 54 (54) 24 (20ndash40) 33 (7ndash68)
LVEF day 6 (range) 61 (50ndash67) 62 (62) 55 (38ndash64) 374 (18ndash65)
Weaned off ECMO () 4 (100) 2 (667) 4 (80) 56 (70)
Complications
Limb ischemia 2 1 0 6
Massive GI bleeding 0 1 2 1
Corneal erosion 0 0 1 0
ARDSPneumonia 0 1 0 8
Reinstitution o ECMO 1 0 0 1
Severe brain insult 23
Further intervention
CABG n 0 0 0 26
Repair VSDwall n 0 0 0 4
VAD n 0 0 0 3
Heart transplantation n 0 0 0 1
Adrenalectomy n 3 0 0 0
Cause o mortality
Sepsis-related MOF 0 1 0 7
Hepatic ailure MOF 0 0 1 0
Cardiogenic shock 0 1 1 28
Continued
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 68
wwwnaturecomscientificreports
6SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
Discussiono the best o our knowledge this report constitutes the largest series to date describing the outcomeso patients presenting with reractory shock caused by endocrine emergencies (ie PC S and DK)rescued by ECMO support A total o 12 cases were identified in our registry rom 2005 to 2012 indicat-ing that the incidence o endocrine emergencies is low but not negligible Pheochromocytoma has been
estimated to be present in approximately 03 o all patients undergoing evaluation or secondary causeso hypertension18 Moreover S and DK accounts or 2 and 86 o all hospital admissions in patientswith thyrotoxicosis and type 1 diabetes mellitus respectively 1920 In general endocrine emergencies canhave a rapid and aggressive clinical course and pose significant diagnostic challenges (because they canmimic either AMI or acute congestive heart ailure) Endocrine emergencies are not common and prob-ably misdiagnosed in many cases and the clinical value o ECMO support in their clinical managementremains unclear Notably ollowing our report o a patient with PC who was successully rescued byECMO in January 20089 seven additional cases were described (a finding that illustrates the magnitudeo the potential underestimation as well as a recent increase in awareness)10ndash16
In the current series all patients with PC did not have a known history o pheochromocytoma Temain diagnostic eatures o PC consisted o extreme blood pressure fluctuations in presence o patentcoronary arteries on angiography Compared with AMI patients inotropic agents were more rapidlytapered and myocardial unction recovered significantly more quickly in PC However two o the ourpatients with PC (50) developed limb ischemia a percentage which was significantly higher than those
observed in both the DK (one patient 33) and AMI (six patients 75) groups (able 3) o our knowl-edge a total o 12 cases o pheochromocytoma-associated peripheral limb ischemia have been reportedto date21 In this scenario early recognition and treatment o pheochromocytoma through adrenalectomyor alpha-adrenergic blocking agents is paramount to reduce the risk o devastating limb ischemia
In this series most patients with S were initially misdiagnosed as having AMI or severe conges-tive heart ailure Hyperbilirubinemia was a common finding in S patients most likely caused by adirect hepatotoxic effect o excess thyroid hormones andor hepatic congestion resulting rom thyroidstorm Although anti-thyroid drugs (eg propylthiouracil) can cause cholestatic liver injury previousstudies conducted in S patients have shown that jaundice can successully respond to anti-thyroidmedications2223 Consequently the timely detection o S is crucial to the successul preservation oliver unction
Blood glucose levels are routinely checked in all o the patients admitted to our emergency depart-ment with disturbances o consciousness Te diagnosis o DK can be easily established upon admissionin presence o hyperglycemia metabolic acidosis and increased serum or urine ketones In generaldelays to seek medical care and the presence o sepsis andor coma have adverse consequences or DKpatientsrsquo clinical outcomes
In the current study AMI patients had lower SOFA scores and higher levels o cardiac enzymes thanthose with endocrine emergencies Notably the lef ventricular ejection unction and the clinical out-comes were poorer in patients with AMI than in those with endocrine emergencies rescued by ECMO(able 3) Similarly the number o patients who required long-term inotropic agents was higher in theAMI group
aken together there are three main findings rom the current single-center study 1) endocrineemergencies are rare but not negligible events 2) patients with endocrine emergencies presenting withacute reractory shock can be successully rescued by ECMO support and 3) screening o endocrineemergencies is essential in patients with acute reractory shock requiring mechanical support Albeitpreliminary in nature because o the small sample size our results may stimulate urther studies on thecost-benefits analysis o routine screening o thyroid hormones catecholamines and metanephrines inpatients presenting with acute circulatory collapse in need o ECMO support
PC (n= 4) DK (n= 3) TS (n= 5) AMI (n= 80)
Brain death 0 0 0 3
ARDS 0 0 0 2
Survival to discharge () 4 (100) 1 (333) 3 (60) 40 (50)
Survivors with CPC I n () 4 (100 ) 1 (100) 2 (667) 32 (80)
Table 3 Comparisons of patients with endocrine crisis and acute myocardial infarction rescued
with ECMO support Abbreviations AMI acute myocardial inarction ARDS acute respiratory distresssyndrome CABG coronary artery bypass surgery CK creatine kinase CPC cerebral perormance categoryCPR cardiac pulmonary resuscitation DK diabetic ketoacidosis GI gastrointestinal IABP intra-aortic
balloon pumping ICU intensive care unit IE inotropic equivalents LVEF lef ventricular ejection ractionMAP mean arterial pressure MOF multiple organ ailure PC pheochromocytoma crisis SOFA sepsis-related organ ailure assessment n-I troponin-I S thyroid storm VAD ventricular assist device VSD
ventricular septal deect
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 78
wwwnaturecomscientificreports
7SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
ConclusionsSuccessul management o endocrine emergencies depends on prompt recognition correction o theunderlying hormone alterations and immediate treatment o shock Unortunately numerous patientspresenting with endocrine emergencies have an unknown previous history o hormone imbalanceTereore the screening o endocrine emergencies is important in these patients Herein we have shownthat ECMO support is clinically useul in patients diagnosed with endocrine emergencies presenting withacute circulatory ailure Because medical care is extremely challenging in this scenario the awareness othe clinical value o ECMO among physicians managing patients with endocrine emergencies may helpimprove clinical outcomes
References1 Pee983147 G J et al Efficacy and economic assessment o conventional ventilatory support versus extracorporeal membrane
oxygenation or severe adult respiratory ailure (CESA983122) a multicentre randomised controlled trial Lancet 374 1351ndash1363(2009)
2 Baud F J Megarbane B Deye N amp Leprince P Clinical review Aggressive management and extracorporeal support or drug-induced cardiotoxicity Crit Care Doi 101186cc5700 (2007)
3 Chen Y S et al 983122escue or acute myocarditis with shoc983147 by extracorporeal membrane oxygenation Ann Torac Surg 68 2220ndash2224 (1999)
4 Chou N 983115 et al Application o extracorporeal membrane oxygenation in adult burn patients Artif Organs 25 622ndash626 (2001)5 Chen Y S et al Cardiopulmonary resuscitation with assisted extracorporeal lie-support versus conventional cardiopulmonary
resuscitation in adults with in-hospital cardiac arrest an observational study and propensity analysis Lancet 372 554ndash561(2008)
6 983115o W J et al Extracorporeal membrane support or adult postcardiotomy cardiogenic shoc983147 Ann Torac Surg 73 538ndash545(2003)
7 Ariza-Soleacute A et al Ventricular support With Extracorporeal Membrane Oxygenation A New 983122escue Alternative or 983122eractoryCardiogenic Shoc983147 983122ev Esp Cardiol 66 501ndash503 (2013)
8 Chen Y S et al Analysis and results o prolonged resuscitation in cardiac arrest patients rescued by extracorporeal membraneoxygenation J Am Coll Cardiol 41 197ndash203 (2003)
9 Chao A Yeh Y C Yen S amp Chen Y S Phaeochromocytoma crisis ndash a rare indication or extracorporeal membraneoxygenation Anaesthesia 63 86ndash88 (2008)
10 Suh I W et al Catastrophic catecholamine-induced cardiomyopathy mimic983147ing acute myocardial inarction rescued byextracorporeal membrane oxygenation (ECMO) in pheochromocytoma J 983115orean Med Sci 23 350ndash354 (2008)
11 Ezri Golan A Sasson L amp 983122ozenman Y Pheochromocytoma induced ulminant cardiogenic shoc983147 ollowing laparoscopicsalpingectomy successully managed with extracorporeal membrane oxygenation Jurnalul 983122omacircn de Anestezie erapie Intensivatilde 16 154ndash158 (2008)
12 983122itter S Guertler Meier C A amp Genoni M Cardiogenic shoc983147 due to pheochromocytoma rescued by extracorporealmembrane oxygenation Interact Cardiovasc Torac Surg 13 112ndash113 (2011)
13 Noorani A Vuylste983147e A Lewis C Parameshwar J amp Catarino P A moribund athlete Lance 380 74 (2012)14 Ghassam S et al Successul extracorporeal membrane oxygenation treatment or pheochromocytoma-induced acute cardiac
ailure AJEM 30 1017e1ndash1017e3 (2012)15 Banfi C et al Central extracorporeal lie support in pheochromocytoma crisis Ann Torac Surg 93 1303ndash1305 (2012)16 Sheinberg 983122 et al Case 1ndash2012 A perect storm atality resulting rom metoclopramide unmas983147ing a pheochromocytoma and
its management J Cardiothorac Vasc Anesth 26 161ndash115 (2012)17 Vincent J L et al Te SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysunctionailure On behal
o the Wor983147ing Group on Sepsis-983122elated Problems o the European Society o Intensive Care Medicine Intensive Care Med 22 707ndash710 (1996)
18 Streeten D H Anderson G H Jr amp Wagner S Effect o age on response o secondary hypertension to specific treatment Am J Hypertens 3 360ndash365 (1990)
19 983115earney amp Dang C Diabetic and endocrine emergencies Postgrad Med J 83 79ndash86 (2007)20 983122ingel M D Management o hypothyroidism and hyperthyroidism in the intensive care unit Crit Care Clin 17 59ndash74 (2001)21 Lutchman D Buchholz S amp 983115eightley C Pheochromocytomandashassociated critical peripheral ischemia Intern Med J 40 150ndash159
(2010)22 Hull 983115 et al wo cases o thyroid storm-associated cholestatic jaundice Endocr Pract 13 478ndash480 (2007)23 Hambleton C et al Tyroid storm complicated by ulminant hepatic ailure Case report and literature review Ann Otol 983122hinol
Laryngol 22 679ndash682 (2013)
AcknowledgementsTis study was partially supported by the National Science Council (102-2325-B-002-009 101-2325-B-002-009 100-2314-B-002-018-MY2 and 100-2325-B-002-009) Ministry o Science and echnologyaiwan and partially unded by the National aiwan University Hospital MG 213 und
Author ContributionsAC HYY and YSC study design AC CHW and HJY draf o the manuscript tables and figuresNKC LJ NHC and MHL data collection and analysis AC and NHC manuscript editingNKC HYY MHL CHW and HJY literature review and data checking SCH IHW and YSCcritical revision o the manuscript or important intellectual content All authors final approval o themanuscript
Additional InformationCompeting financial interests Te authors declare no competing financial interests
How to cite this article Chao A et al Highlighting indication o extracorporeal membraneoxygenation in endocrine emergencies Sci Rep 5 13361 doi 101038srep13361 (2015)
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 88
wwwnaturecomscientificreports
8SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
Tis work is licensed under a Creative Commons Attribution 40 International License Teimages or other third party material in this article are included in the articlersquos Creative Com-
mons license unless indicated otherwise in the credit line i the material is not included under theCreative Commons license users will need to obtain permission rom the license holder to reproducethe material o view a copy o this license visit httpcreativecommonsorglicensesby40

8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 28
wwwnaturecomscientificreports
2SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
ECMO support We also compared their clinical outcomes with those o 80 cases with AMI who receivedECMO because o cardiogenic shock
MethodsStudy approval was obtained by our Institutional Review Board (No 201404079 RIN) which waivedthe requirement or inormed consent because o the retrospective nature o the study Among thepatients aged 16 years or older who received ECMO and reported to our hospital-based ECMO registryduring the period January 2005ndashDecember 2012 we retrospectively reviewed the data o those whopresented with reractory shock due to endocrine emergencies Te indications or ECMO included
catecholamine-reractory shock and ailed conventional cardiopulmonary resuscitation Te circuit andmanagement o ECMO have been described previously 58 Following completion o ECMO presumeddiagnoses were confirmed by reviewing all o the clinical and laboratory data Because some cases wereinitially incorrectly diagnosed a careul analysis o all clinical records was perormed beore includingthe patient in the study
We identified 12 cases presenting with reractory shock secondary to endocrine emergencies success-ully rescued by ECMO support Te diagnostic distribution was as ollows PC (n= 4) S (n= 5) andDK (n= 3) PC was identified through plasma and urinary catecholamines and metanephrines testingand imaging confirmation o adrenal lesions compatible with pheochromocytoma S was diagnosed onthe basis o serum thyroid hormone levels and traditional signs and symptoms o a thyrotoxic state Tediagnosis o DK was made in presence o uncontrolled hyperglycemia metabolic acidosis and increasedtotal blood ketone concentrations either with or without a history o type 1 diabetes mellitus Te ol-lowing variables were collected in all participants age sex initial clinical presentation final diagnosistime taken to identiy the etiology initial sepsis-related organ ailure assessment (SOFA) score17 ECMO
duration pre- and post-ECMO inotropic equivalent (IE= dopaminetimes 1+ dobutaminetimes 1+ norepi-nephrinetimes 100+ epinephrinetimes 100 all expressed in micro gkgmin) post-ECMO blood pressure valuesbiochemical data hormone levels and length o stay in the intensive care unit Te main outcome meas-ures included neurological conditions at discharge survival duration o ECMO and the occurrence ocomplications afer ECMO Because the clinical presentation o several patients with endocrine emer-gencies closely resembled AMI we compared their general characteristics and outcomes with those o 80cases with AMI (aged le 65 years) who received ECMO because o cardiogenic shock
ResultsTe flow o patients through the study is depicted in Fig 1 During the period January 2005ndashDecember2012 a total o 1180 patients were rescued with ECMO [1027 with veno-arterial (VA) ECMO and 153with veno-venous (VV) ECMO] according to our registry data We identified 12 patients presenting withreractory shock secondary to endocrine emergencies (PC n= 4 S n= 5 and DK n= 3) who wererescued by ECMO support Te clinical outcomes o patients with endocrine emergencies were com-
pared with those o 80 cases with AMI who received ECMO because o cardiogenic shock Endocrineemergencies represented 1 o all cases treated with ECMO (12 o VA ECMO) Te clinical course ispresented separately or each endocrine emergency
Pheochromocytoma crisis We identified our patients with PC Te presentation o PC mimickedAMI with palpitations chest pain abnormal electrocardiographic findings and elevations o cardiacenzymes (ables 1 and 2) Not surprisingly most patients with PC were initially misdiagnosed as havingan acute coronary syndrome Tree PC patients (PC-1 PC-2 and PC-4) had a bystander-witnessedout-o-hospital cardiac arrest and ECMO was initiated during cardiac pulmonary resuscitation (CPR)in the emergency department Patient PC-3 presented with an intractable cardiogenic shock requir-ing ECMO to allow or organ recovery Paroxysmal hypertension was identified in all o these patientsollowing ECMO implantation All o the patients in the PC group underwent coronary angiographyPatients PC-1 PC-2 and PC-3 had normal coronary angiography which led to the suspicion o pheo-chromocytoma Because o a 50 stenosis in the lef circumflex artery patient PC-4 was initially treated
as having an AMI and weaned off ECMO support afer 48 h under stable hemodynamic conditions Anepisode o pulseless ventricular tachycardia occurred 2 h later requiring resumption o CPR and ECMOBecause o the extreme blood pressure fluctuations a diagnosis o PC was suspected Patients PC-1 andPC-3 experienced a severe lower leg compartment syndrome despite placement o a distal perusioncatheter to prevent limb ischemia In patient PC-1 the emoral-emoral VA ECMO was converted toa central ECMO afer median sternotomy avoiding urther worsening o limb ischemia Patient PC-3underwent a below-knee amputation o the lef leg Te patients received abdominal computed tomog-raphy scans to localize the tumor and confirm the diagnosis All PC patients underwent adrenalectomyafer discharge rom the intensive care unit the only exception being PC-4 who reused surgery
Thyroid storm Five patients with S were identified throughout the study period All o them hada history o hyperthyroidism the only exception being S-1 (in whom S was suspected because onormal angiographic findings) Most patients with S were initially misdiagnosed as having AMI orsevere congestive heart ailure Teir rapid clinical deterioration required emergency ECMO supportHyperbilirubinemia was evident in all o the S patients whereas patient S-2 and S-4 developed
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 38
wwwnaturecomscientificreports
3SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
massive gastrointestinal bleeding Under ECMO support and anti-thyroid drug therapy the cardiac unc-tion o our o the 5 S patients started recovering between day 3 and day 4 Tey were subsequentlyweaned off ECMO Patient S-1 died o multi-organ ailure while receiving ECMO whereas patient S-2
eventually died o liver ailure Patient S-4 suffered rom Gravesrsquo ophthalmopathy resulting in exposurekeratopathy o the lef eye which eventually required penetrating keratoplasty
Diabetic ketoacidosis All o the three patients with DK were ound unresponsive at home PatientsDK-1 and DK-3 had a diagnosis o type 1 diabetes mellitus but their compliance with insulin therapywas poor Patient DK-2rsquos relatives denied any known medical history Patients DK-1 and DK-2 wereadmitted to the emergency department with out-o-hospital cardiac arrest Patient DK-3 required ECMObecause o proound hypothermia and hypotension unresponsive to aggressive fluid replacement andhigh-dose catecholamine administration Te presence o uncontrolled hyperglycemia metabolic aci-dosis and increased total blood ketone concentrations led to a diagnosis o DK Because patient DK-1was also diagnosed with community-acquired pneumonia that progressed to acute respiratory distresssyndrome both VA and VV ECMO support were indicated VA and VV ECMO were stopped 200 h and381 h afer initiation respectively Te patient eventually developed gangrene o the distal parts o all ourlimbs and died o septic shock and multiple organ ailure Spontaneous circulation in patient DK-2 did
not return despite ECMO support Patient DK-3 was successully resuscitated and eventually recovered
Comparison between endocrine emergencies and AMI PC and S were requently undistin-guishable rom AMI at presentation Despite lower sepsis-related organ ailure assessment (SOFA) scoresin the AMI group heart unction and clinical outcomes did not differ significantly rom those o patientswith endocrine emergencies AMI patients required higher doses o inotropic agents to stabilize theirhemodynamic status and their lef ventricular ejection unction remained poor Te ECMO weaningsuccess rates or patients with AMI and endocrine emergencies were 70 and 83 respectively Patientswith AMI required the ollowing subsequent interventions coronary bypass surgery (n= 26) repair oa ruptured ventricular septal deect (n= 4) implantation o a lef ventricular assist device (n= 3) car-diorrhaphy ollowing removal o ECMO and heart transplantation (n= 1) Te neurological outcomesdid not differ significantly between the two groups Eighty percent o the patients who survived an AMIhad a cerebral perormance category (CPC) score o 1 which was ound in 83 o those who survivedan endocrine emergency (able 3)
Figure 1 Flow diagram of patients with endocrine emergencies who were rescued by extracorporeal
membrane oxygenation Abbreviations ARDS acute respiratory distress syndrome AMI acute myocardial
inarction CMP cardiomyopathy DK diabetic ketoacidosis ECMO extracorporeal membrane oxygenationPCS post-cardiotomy shock PE pulmonary embolism PC pheochromocytoma crisis PH pulmonaryhypertension S thyroid storm x lung transplantation VA veno-arterial VV veno-venous
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 48
wwwnaturecomscientificreports
4SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
CaseAge(y) Sex Initial presentation Past history Initial diagnosis
Day ofdiagnosis Endocrine data Survival
Pheochromocytoma crisis Urine VMADopaEpiNE
PC1 25 F Dyspnea palpitations cold sweats Myocarditis AMImyocarditis 28 1531851283 Yes
PC2 52 M Chest pain Hypertension AMI 6 207217146858 Yes
PC3 40 M Chest pain Hypertension AMI 3 64349833342162 Yes
PC4 65 M Chest pain palpitations HBV carrier AMI 4 11278791208 Yes
Diabetic ketoacidosis Blood glucoseketone bodies
DK1 16 F Fever loss o consciousness 1DM Septic shock 1 770+ No
DK2 34 M Fever drowsiness Nil Septic shock 1 150559 No
DK3 28 F Loss o consciousness 1DM DK 1 99436 Yes
Tyroid storm Free 43SH
S1 47 M Palpitations exertional dyspnea Gout AMI 3 426927004 No
S2 43 M DyspneaGravesrsquo disease alcohol
liverTyroid stormCHF 4 242237003 No
S3 37 FDry cough night sweating alteration
o consciousnessGravesrsquo disease CHF 1 75-003 Yes
S4 42 MPalpitations dyspnea nausea
deliriumGravesrsquo ophthalmopathy Tyroid storm 1 24722lt 001 Yes
S5 33 F Fever shortness o breath Hyperthyroidism Tyroid storm 1 45425lt 001 Yes
Table 1 Demographic and clinical characteristics of patients with endocrine emergencies who were
rescued by extracorporeal membrane oxygenation Abbreviations M male F emale y years HBVhepatitis B virus AMI acute myocardial inarction 1DM type 1 diabetes mellitus CHF congestive heart
ailure Dopa dopamine (normal range 50ndash450 micro gmiddotday minus1) Epi epinephrine (normal range lt 224micro gmiddotday minus1)NE norepinephrine (normal range 121ndash855 micro gmiddotday minus1) ree 4 thyroxine (normal range 089ndash176 ngdL) 3 triiodothyronine (normal range 84ndash172 ngdL) SH thyroid-stimulating hormone (normal range
04ndash4micro IUmL) VMA vanillomandelic acid (normal range 1ndash7 mgmiddotday minus1)
PC (n= 4) DK (n= 3) TS (n= 5)
SOFA score (range) 13 (9ndash18) 137 (8ndash17) 15 (13ndash18)
Extracorporeal cardiopulmonaryresuscitation n 3 2 3
Inotropic index microgkgmin 283 568 355
IABP n 2 1 2
pH (range) 730 (71ndash736) 712 (663ndash739) 724 (714ndash739)
Blood lactate mmolL (range) 103 (87ndash11) 625 (50ndash75) 96 (35ndash12)
Initial CK UL (range) 15725 (501ndash3796) 2253 (348ndash2576) 7143 (259ndash1574)
Initial CK-MB UL (range) 862 (15ndash290) 211 (14ndash32) 426 (21ndash75)
Initial troponin-I micro gL (range) 370 (09ndash79) 058 (05ndash07) 035 (002ndash11)
Serum sodium mEqL (range) 1413 (138ndash144) 1463 (131ndash155) 143 (128ndash149)
Serum BUN mgdL (range) 169 (14ndash249) 471 (375ndash524) 294 (196ndash755)
Serum creatinine mgdL (range) 21 (08ndash28) 23 (21ndash26) 16 (11ndash240)
Serum bilirubin mgdL (range) 09 (04ndash140) 067 (012ndash15) 72 (26ndash1450)
Serum AS UL (range) 6435 (52ndash2183) 109 (15ndash239) 24645 (195ndash6195)
Serum AL UL (range) 6572 (47ndash2183) 43 (10ndash73) 761 (44ndash2267)
Table 2 Clinical characteristics of patients with endocrine emergencies at the time of ECMO
implantation Abbreviations AS aspartate aminotranserase AL alanine aminotranserase BUNblood urea nitrogen CK creatine kinase DK diabetic ketoacidosis IABP intra-aortic balloon pump PCpheochromocytoma crisis SOFA sepsis-related organ ailure assessment S thyroid storm
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 58
wwwnaturecomscientificreports
5SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
PC (n= 4) DK (n= 3) TS (n= 5) AMI (n= 80)
Age years (range) 455 (25ndash65) 26 (16ndash34) 404 (33ndash47) 538 (31ndash65)
Male sex n () 3 (75) 1 (333) 3 (60) 75 (94)
CPR n () 3 (75) 2 (66) 3 (60) 55 (687)
ECMO duration hour (range) 1025 (447ndash1625) 1345 (09ndash3818) 82 (19ndash1156) 117 (54ndash475)
Ventilator support day (range) 14 (6ndash22) 177 (1ndash51) 10 (4ndash26) 177 (1ndash95)
ICU length o stay day (range) 208 (6ndash28) 180 (0ndash51) 118 (5ndash26) 216 (1ndash147)
Initial SOFA score (range) 13 (9ndash18) 137 (8ndash17) 15 (13ndash18) 104 (3ndash18)
MAP Day 1 mmHg (range) 120 (101ndash137) 97 (96ndash99) 84 (63ndash101) 74 (30ndash144)
Day 3 (range) 121 (91ndash146) 85 (84ndash86) 113 (104ndash126) 76 ( 920ndash112)
Day 6 (range) 130 (116ndash145) 99 (99) 114 (93ndash132) 88 (61ndash118)
Pre-ECMO IE micro gkgmin 283 568 355 214
IE day 3 (range) 47 (21ndash70) 324 (324) 46 (0ndash184) 241 (0ndash810)
IE day 6 (range) 14 (0ndash54) 115 (115) 0 (0) 82 (0ndash318)
Patients using inotropes at day 6n ()
1 (25) 1 (33) 0 (0) 50 (625)
Initial CK UL (range) 15725 (501ndash3796) 2253 (348ndash2576) 714 (259ndash1574) 2413 (41ndash28480)
CK day 3 (range) 14589 (1528ndash47829) 385 (385) 83645 (515ndash4446) 58084 (77ndash66274)
CK day 6 (range) 22637 (530ndash13721) 4496 (4496) 501 (114ndash888) 31634 (33ndash36621)
Initial CK-MB UL (range) 862 (15ndash290) 211 (14ndash32) 426 (21ndash75) 172 (42ndash23198)
CK-MB day 3 (range) 3892 (909ndash10031) 522 (522) 535 (396ndash646) 1321 (15ndash1782)
CK-MB day 6 (range) 66 (157ndash207) 26 (26) 451 (407ndash494) 504 (12ndash3089)
Initial n-I microgL (range) 370 (9ndash79) 058 (05ndash07) 035 (002ndash11) 19 (001ndash100)
n-I day 3 (range) 161 (94ndash244) 04 (04) 12 (05ndash18) 377 (044ndash94)
n-I day 6 (range) 22 (126ndash31) Not available Not available 161 (031ndash33)
Lactate in 24 h mmolL (range) 103 (87ndash11) 625 (50ndash75) 96 (35ndash12) 89 (1ndash35)
Dialysis patients n 3 1 1 36
IABP (at implantation) 2 1 1 25 (32)
Bilirubin day 3 mgdL (range) 13 (10ndash19) 09 (09) 106 (20ndash248) 25 (04ndash122)
Bilirubin day 6 (range) 17 (14ndash18) 55 (55) 195 (567ndash269) 35 (06ndash213)
LVEF day 2 (range) 377 (30ndash43) 54 (54) 24 (20ndash40) 33 (7ndash68)
LVEF day 6 (range) 61 (50ndash67) 62 (62) 55 (38ndash64) 374 (18ndash65)
Weaned off ECMO () 4 (100) 2 (667) 4 (80) 56 (70)
Complications
Limb ischemia 2 1 0 6
Massive GI bleeding 0 1 2 1
Corneal erosion 0 0 1 0
ARDSPneumonia 0 1 0 8
Reinstitution o ECMO 1 0 0 1
Severe brain insult 23
Further intervention
CABG n 0 0 0 26
Repair VSDwall n 0 0 0 4
VAD n 0 0 0 3
Heart transplantation n 0 0 0 1
Adrenalectomy n 3 0 0 0
Cause o mortality
Sepsis-related MOF 0 1 0 7
Hepatic ailure MOF 0 0 1 0
Cardiogenic shock 0 1 1 28
Continued
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 68
wwwnaturecomscientificreports
6SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
Discussiono the best o our knowledge this report constitutes the largest series to date describing the outcomeso patients presenting with reractory shock caused by endocrine emergencies (ie PC S and DK)rescued by ECMO support A total o 12 cases were identified in our registry rom 2005 to 2012 indicat-ing that the incidence o endocrine emergencies is low but not negligible Pheochromocytoma has been
estimated to be present in approximately 03 o all patients undergoing evaluation or secondary causeso hypertension18 Moreover S and DK accounts or 2 and 86 o all hospital admissions in patientswith thyrotoxicosis and type 1 diabetes mellitus respectively 1920 In general endocrine emergencies canhave a rapid and aggressive clinical course and pose significant diagnostic challenges (because they canmimic either AMI or acute congestive heart ailure) Endocrine emergencies are not common and prob-ably misdiagnosed in many cases and the clinical value o ECMO support in their clinical managementremains unclear Notably ollowing our report o a patient with PC who was successully rescued byECMO in January 20089 seven additional cases were described (a finding that illustrates the magnitudeo the potential underestimation as well as a recent increase in awareness)10ndash16
In the current series all patients with PC did not have a known history o pheochromocytoma Temain diagnostic eatures o PC consisted o extreme blood pressure fluctuations in presence o patentcoronary arteries on angiography Compared with AMI patients inotropic agents were more rapidlytapered and myocardial unction recovered significantly more quickly in PC However two o the ourpatients with PC (50) developed limb ischemia a percentage which was significantly higher than those
observed in both the DK (one patient 33) and AMI (six patients 75) groups (able 3) o our knowl-edge a total o 12 cases o pheochromocytoma-associated peripheral limb ischemia have been reportedto date21 In this scenario early recognition and treatment o pheochromocytoma through adrenalectomyor alpha-adrenergic blocking agents is paramount to reduce the risk o devastating limb ischemia
In this series most patients with S were initially misdiagnosed as having AMI or severe conges-tive heart ailure Hyperbilirubinemia was a common finding in S patients most likely caused by adirect hepatotoxic effect o excess thyroid hormones andor hepatic congestion resulting rom thyroidstorm Although anti-thyroid drugs (eg propylthiouracil) can cause cholestatic liver injury previousstudies conducted in S patients have shown that jaundice can successully respond to anti-thyroidmedications2223 Consequently the timely detection o S is crucial to the successul preservation oliver unction
Blood glucose levels are routinely checked in all o the patients admitted to our emergency depart-ment with disturbances o consciousness Te diagnosis o DK can be easily established upon admissionin presence o hyperglycemia metabolic acidosis and increased serum or urine ketones In generaldelays to seek medical care and the presence o sepsis andor coma have adverse consequences or DKpatientsrsquo clinical outcomes
In the current study AMI patients had lower SOFA scores and higher levels o cardiac enzymes thanthose with endocrine emergencies Notably the lef ventricular ejection unction and the clinical out-comes were poorer in patients with AMI than in those with endocrine emergencies rescued by ECMO(able 3) Similarly the number o patients who required long-term inotropic agents was higher in theAMI group
aken together there are three main findings rom the current single-center study 1) endocrineemergencies are rare but not negligible events 2) patients with endocrine emergencies presenting withacute reractory shock can be successully rescued by ECMO support and 3) screening o endocrineemergencies is essential in patients with acute reractory shock requiring mechanical support Albeitpreliminary in nature because o the small sample size our results may stimulate urther studies on thecost-benefits analysis o routine screening o thyroid hormones catecholamines and metanephrines inpatients presenting with acute circulatory collapse in need o ECMO support
PC (n= 4) DK (n= 3) TS (n= 5) AMI (n= 80)
Brain death 0 0 0 3
ARDS 0 0 0 2
Survival to discharge () 4 (100) 1 (333) 3 (60) 40 (50)
Survivors with CPC I n () 4 (100 ) 1 (100) 2 (667) 32 (80)
Table 3 Comparisons of patients with endocrine crisis and acute myocardial infarction rescued
with ECMO support Abbreviations AMI acute myocardial inarction ARDS acute respiratory distresssyndrome CABG coronary artery bypass surgery CK creatine kinase CPC cerebral perormance categoryCPR cardiac pulmonary resuscitation DK diabetic ketoacidosis GI gastrointestinal IABP intra-aortic
balloon pumping ICU intensive care unit IE inotropic equivalents LVEF lef ventricular ejection ractionMAP mean arterial pressure MOF multiple organ ailure PC pheochromocytoma crisis SOFA sepsis-related organ ailure assessment n-I troponin-I S thyroid storm VAD ventricular assist device VSD
ventricular septal deect
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 78
wwwnaturecomscientificreports
7SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
ConclusionsSuccessul management o endocrine emergencies depends on prompt recognition correction o theunderlying hormone alterations and immediate treatment o shock Unortunately numerous patientspresenting with endocrine emergencies have an unknown previous history o hormone imbalanceTereore the screening o endocrine emergencies is important in these patients Herein we have shownthat ECMO support is clinically useul in patients diagnosed with endocrine emergencies presenting withacute circulatory ailure Because medical care is extremely challenging in this scenario the awareness othe clinical value o ECMO among physicians managing patients with endocrine emergencies may helpimprove clinical outcomes
References1 Pee983147 G J et al Efficacy and economic assessment o conventional ventilatory support versus extracorporeal membrane
oxygenation or severe adult respiratory ailure (CESA983122) a multicentre randomised controlled trial Lancet 374 1351ndash1363(2009)
2 Baud F J Megarbane B Deye N amp Leprince P Clinical review Aggressive management and extracorporeal support or drug-induced cardiotoxicity Crit Care Doi 101186cc5700 (2007)
3 Chen Y S et al 983122escue or acute myocarditis with shoc983147 by extracorporeal membrane oxygenation Ann Torac Surg 68 2220ndash2224 (1999)
4 Chou N 983115 et al Application o extracorporeal membrane oxygenation in adult burn patients Artif Organs 25 622ndash626 (2001)5 Chen Y S et al Cardiopulmonary resuscitation with assisted extracorporeal lie-support versus conventional cardiopulmonary
resuscitation in adults with in-hospital cardiac arrest an observational study and propensity analysis Lancet 372 554ndash561(2008)
6 983115o W J et al Extracorporeal membrane support or adult postcardiotomy cardiogenic shoc983147 Ann Torac Surg 73 538ndash545(2003)
7 Ariza-Soleacute A et al Ventricular support With Extracorporeal Membrane Oxygenation A New 983122escue Alternative or 983122eractoryCardiogenic Shoc983147 983122ev Esp Cardiol 66 501ndash503 (2013)
8 Chen Y S et al Analysis and results o prolonged resuscitation in cardiac arrest patients rescued by extracorporeal membraneoxygenation J Am Coll Cardiol 41 197ndash203 (2003)
9 Chao A Yeh Y C Yen S amp Chen Y S Phaeochromocytoma crisis ndash a rare indication or extracorporeal membraneoxygenation Anaesthesia 63 86ndash88 (2008)
10 Suh I W et al Catastrophic catecholamine-induced cardiomyopathy mimic983147ing acute myocardial inarction rescued byextracorporeal membrane oxygenation (ECMO) in pheochromocytoma J 983115orean Med Sci 23 350ndash354 (2008)
11 Ezri Golan A Sasson L amp 983122ozenman Y Pheochromocytoma induced ulminant cardiogenic shoc983147 ollowing laparoscopicsalpingectomy successully managed with extracorporeal membrane oxygenation Jurnalul 983122omacircn de Anestezie erapie Intensivatilde 16 154ndash158 (2008)
12 983122itter S Guertler Meier C A amp Genoni M Cardiogenic shoc983147 due to pheochromocytoma rescued by extracorporealmembrane oxygenation Interact Cardiovasc Torac Surg 13 112ndash113 (2011)
13 Noorani A Vuylste983147e A Lewis C Parameshwar J amp Catarino P A moribund athlete Lance 380 74 (2012)14 Ghassam S et al Successul extracorporeal membrane oxygenation treatment or pheochromocytoma-induced acute cardiac
ailure AJEM 30 1017e1ndash1017e3 (2012)15 Banfi C et al Central extracorporeal lie support in pheochromocytoma crisis Ann Torac Surg 93 1303ndash1305 (2012)16 Sheinberg 983122 et al Case 1ndash2012 A perect storm atality resulting rom metoclopramide unmas983147ing a pheochromocytoma and
its management J Cardiothorac Vasc Anesth 26 161ndash115 (2012)17 Vincent J L et al Te SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysunctionailure On behal
o the Wor983147ing Group on Sepsis-983122elated Problems o the European Society o Intensive Care Medicine Intensive Care Med 22 707ndash710 (1996)
18 Streeten D H Anderson G H Jr amp Wagner S Effect o age on response o secondary hypertension to specific treatment Am J Hypertens 3 360ndash365 (1990)
19 983115earney amp Dang C Diabetic and endocrine emergencies Postgrad Med J 83 79ndash86 (2007)20 983122ingel M D Management o hypothyroidism and hyperthyroidism in the intensive care unit Crit Care Clin 17 59ndash74 (2001)21 Lutchman D Buchholz S amp 983115eightley C Pheochromocytomandashassociated critical peripheral ischemia Intern Med J 40 150ndash159
(2010)22 Hull 983115 et al wo cases o thyroid storm-associated cholestatic jaundice Endocr Pract 13 478ndash480 (2007)23 Hambleton C et al Tyroid storm complicated by ulminant hepatic ailure Case report and literature review Ann Otol 983122hinol
Laryngol 22 679ndash682 (2013)
AcknowledgementsTis study was partially supported by the National Science Council (102-2325-B-002-009 101-2325-B-002-009 100-2314-B-002-018-MY2 and 100-2325-B-002-009) Ministry o Science and echnologyaiwan and partially unded by the National aiwan University Hospital MG 213 und
Author ContributionsAC HYY and YSC study design AC CHW and HJY draf o the manuscript tables and figuresNKC LJ NHC and MHL data collection and analysis AC and NHC manuscript editingNKC HYY MHL CHW and HJY literature review and data checking SCH IHW and YSCcritical revision o the manuscript or important intellectual content All authors final approval o themanuscript
Additional InformationCompeting financial interests Te authors declare no competing financial interests
How to cite this article Chao A et al Highlighting indication o extracorporeal membraneoxygenation in endocrine emergencies Sci Rep 5 13361 doi 101038srep13361 (2015)
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 88
wwwnaturecomscientificreports
8SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
Tis work is licensed under a Creative Commons Attribution 40 International License Teimages or other third party material in this article are included in the articlersquos Creative Com-
mons license unless indicated otherwise in the credit line i the material is not included under theCreative Commons license users will need to obtain permission rom the license holder to reproducethe material o view a copy o this license visit httpcreativecommonsorglicensesby40

8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 38
wwwnaturecomscientificreports
3SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
massive gastrointestinal bleeding Under ECMO support and anti-thyroid drug therapy the cardiac unc-tion o our o the 5 S patients started recovering between day 3 and day 4 Tey were subsequentlyweaned off ECMO Patient S-1 died o multi-organ ailure while receiving ECMO whereas patient S-2
eventually died o liver ailure Patient S-4 suffered rom Gravesrsquo ophthalmopathy resulting in exposurekeratopathy o the lef eye which eventually required penetrating keratoplasty
Diabetic ketoacidosis All o the three patients with DK were ound unresponsive at home PatientsDK-1 and DK-3 had a diagnosis o type 1 diabetes mellitus but their compliance with insulin therapywas poor Patient DK-2rsquos relatives denied any known medical history Patients DK-1 and DK-2 wereadmitted to the emergency department with out-o-hospital cardiac arrest Patient DK-3 required ECMObecause o proound hypothermia and hypotension unresponsive to aggressive fluid replacement andhigh-dose catecholamine administration Te presence o uncontrolled hyperglycemia metabolic aci-dosis and increased total blood ketone concentrations led to a diagnosis o DK Because patient DK-1was also diagnosed with community-acquired pneumonia that progressed to acute respiratory distresssyndrome both VA and VV ECMO support were indicated VA and VV ECMO were stopped 200 h and381 h afer initiation respectively Te patient eventually developed gangrene o the distal parts o all ourlimbs and died o septic shock and multiple organ ailure Spontaneous circulation in patient DK-2 did
not return despite ECMO support Patient DK-3 was successully resuscitated and eventually recovered
Comparison between endocrine emergencies and AMI PC and S were requently undistin-guishable rom AMI at presentation Despite lower sepsis-related organ ailure assessment (SOFA) scoresin the AMI group heart unction and clinical outcomes did not differ significantly rom those o patientswith endocrine emergencies AMI patients required higher doses o inotropic agents to stabilize theirhemodynamic status and their lef ventricular ejection unction remained poor Te ECMO weaningsuccess rates or patients with AMI and endocrine emergencies were 70 and 83 respectively Patientswith AMI required the ollowing subsequent interventions coronary bypass surgery (n= 26) repair oa ruptured ventricular septal deect (n= 4) implantation o a lef ventricular assist device (n= 3) car-diorrhaphy ollowing removal o ECMO and heart transplantation (n= 1) Te neurological outcomesdid not differ significantly between the two groups Eighty percent o the patients who survived an AMIhad a cerebral perormance category (CPC) score o 1 which was ound in 83 o those who survivedan endocrine emergency (able 3)
Figure 1 Flow diagram of patients with endocrine emergencies who were rescued by extracorporeal
membrane oxygenation Abbreviations ARDS acute respiratory distress syndrome AMI acute myocardial
inarction CMP cardiomyopathy DK diabetic ketoacidosis ECMO extracorporeal membrane oxygenationPCS post-cardiotomy shock PE pulmonary embolism PC pheochromocytoma crisis PH pulmonaryhypertension S thyroid storm x lung transplantation VA veno-arterial VV veno-venous
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 48
wwwnaturecomscientificreports
4SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
CaseAge(y) Sex Initial presentation Past history Initial diagnosis
Day ofdiagnosis Endocrine data Survival
Pheochromocytoma crisis Urine VMADopaEpiNE
PC1 25 F Dyspnea palpitations cold sweats Myocarditis AMImyocarditis 28 1531851283 Yes
PC2 52 M Chest pain Hypertension AMI 6 207217146858 Yes
PC3 40 M Chest pain Hypertension AMI 3 64349833342162 Yes
PC4 65 M Chest pain palpitations HBV carrier AMI 4 11278791208 Yes
Diabetic ketoacidosis Blood glucoseketone bodies
DK1 16 F Fever loss o consciousness 1DM Septic shock 1 770+ No
DK2 34 M Fever drowsiness Nil Septic shock 1 150559 No
DK3 28 F Loss o consciousness 1DM DK 1 99436 Yes
Tyroid storm Free 43SH
S1 47 M Palpitations exertional dyspnea Gout AMI 3 426927004 No
S2 43 M DyspneaGravesrsquo disease alcohol
liverTyroid stormCHF 4 242237003 No
S3 37 FDry cough night sweating alteration
o consciousnessGravesrsquo disease CHF 1 75-003 Yes
S4 42 MPalpitations dyspnea nausea
deliriumGravesrsquo ophthalmopathy Tyroid storm 1 24722lt 001 Yes
S5 33 F Fever shortness o breath Hyperthyroidism Tyroid storm 1 45425lt 001 Yes
Table 1 Demographic and clinical characteristics of patients with endocrine emergencies who were
rescued by extracorporeal membrane oxygenation Abbreviations M male F emale y years HBVhepatitis B virus AMI acute myocardial inarction 1DM type 1 diabetes mellitus CHF congestive heart
ailure Dopa dopamine (normal range 50ndash450 micro gmiddotday minus1) Epi epinephrine (normal range lt 224micro gmiddotday minus1)NE norepinephrine (normal range 121ndash855 micro gmiddotday minus1) ree 4 thyroxine (normal range 089ndash176 ngdL) 3 triiodothyronine (normal range 84ndash172 ngdL) SH thyroid-stimulating hormone (normal range
04ndash4micro IUmL) VMA vanillomandelic acid (normal range 1ndash7 mgmiddotday minus1)
PC (n= 4) DK (n= 3) TS (n= 5)
SOFA score (range) 13 (9ndash18) 137 (8ndash17) 15 (13ndash18)
Extracorporeal cardiopulmonaryresuscitation n 3 2 3
Inotropic index microgkgmin 283 568 355
IABP n 2 1 2
pH (range) 730 (71ndash736) 712 (663ndash739) 724 (714ndash739)
Blood lactate mmolL (range) 103 (87ndash11) 625 (50ndash75) 96 (35ndash12)
Initial CK UL (range) 15725 (501ndash3796) 2253 (348ndash2576) 7143 (259ndash1574)
Initial CK-MB UL (range) 862 (15ndash290) 211 (14ndash32) 426 (21ndash75)
Initial troponin-I micro gL (range) 370 (09ndash79) 058 (05ndash07) 035 (002ndash11)
Serum sodium mEqL (range) 1413 (138ndash144) 1463 (131ndash155) 143 (128ndash149)
Serum BUN mgdL (range) 169 (14ndash249) 471 (375ndash524) 294 (196ndash755)
Serum creatinine mgdL (range) 21 (08ndash28) 23 (21ndash26) 16 (11ndash240)
Serum bilirubin mgdL (range) 09 (04ndash140) 067 (012ndash15) 72 (26ndash1450)
Serum AS UL (range) 6435 (52ndash2183) 109 (15ndash239) 24645 (195ndash6195)
Serum AL UL (range) 6572 (47ndash2183) 43 (10ndash73) 761 (44ndash2267)
Table 2 Clinical characteristics of patients with endocrine emergencies at the time of ECMO
implantation Abbreviations AS aspartate aminotranserase AL alanine aminotranserase BUNblood urea nitrogen CK creatine kinase DK diabetic ketoacidosis IABP intra-aortic balloon pump PCpheochromocytoma crisis SOFA sepsis-related organ ailure assessment S thyroid storm
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 58
wwwnaturecomscientificreports
5SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
PC (n= 4) DK (n= 3) TS (n= 5) AMI (n= 80)
Age years (range) 455 (25ndash65) 26 (16ndash34) 404 (33ndash47) 538 (31ndash65)
Male sex n () 3 (75) 1 (333) 3 (60) 75 (94)
CPR n () 3 (75) 2 (66) 3 (60) 55 (687)
ECMO duration hour (range) 1025 (447ndash1625) 1345 (09ndash3818) 82 (19ndash1156) 117 (54ndash475)
Ventilator support day (range) 14 (6ndash22) 177 (1ndash51) 10 (4ndash26) 177 (1ndash95)
ICU length o stay day (range) 208 (6ndash28) 180 (0ndash51) 118 (5ndash26) 216 (1ndash147)
Initial SOFA score (range) 13 (9ndash18) 137 (8ndash17) 15 (13ndash18) 104 (3ndash18)
MAP Day 1 mmHg (range) 120 (101ndash137) 97 (96ndash99) 84 (63ndash101) 74 (30ndash144)
Day 3 (range) 121 (91ndash146) 85 (84ndash86) 113 (104ndash126) 76 ( 920ndash112)
Day 6 (range) 130 (116ndash145) 99 (99) 114 (93ndash132) 88 (61ndash118)
Pre-ECMO IE micro gkgmin 283 568 355 214
IE day 3 (range) 47 (21ndash70) 324 (324) 46 (0ndash184) 241 (0ndash810)
IE day 6 (range) 14 (0ndash54) 115 (115) 0 (0) 82 (0ndash318)
Patients using inotropes at day 6n ()
1 (25) 1 (33) 0 (0) 50 (625)
Initial CK UL (range) 15725 (501ndash3796) 2253 (348ndash2576) 714 (259ndash1574) 2413 (41ndash28480)
CK day 3 (range) 14589 (1528ndash47829) 385 (385) 83645 (515ndash4446) 58084 (77ndash66274)
CK day 6 (range) 22637 (530ndash13721) 4496 (4496) 501 (114ndash888) 31634 (33ndash36621)
Initial CK-MB UL (range) 862 (15ndash290) 211 (14ndash32) 426 (21ndash75) 172 (42ndash23198)
CK-MB day 3 (range) 3892 (909ndash10031) 522 (522) 535 (396ndash646) 1321 (15ndash1782)
CK-MB day 6 (range) 66 (157ndash207) 26 (26) 451 (407ndash494) 504 (12ndash3089)
Initial n-I microgL (range) 370 (9ndash79) 058 (05ndash07) 035 (002ndash11) 19 (001ndash100)
n-I day 3 (range) 161 (94ndash244) 04 (04) 12 (05ndash18) 377 (044ndash94)
n-I day 6 (range) 22 (126ndash31) Not available Not available 161 (031ndash33)
Lactate in 24 h mmolL (range) 103 (87ndash11) 625 (50ndash75) 96 (35ndash12) 89 (1ndash35)
Dialysis patients n 3 1 1 36
IABP (at implantation) 2 1 1 25 (32)
Bilirubin day 3 mgdL (range) 13 (10ndash19) 09 (09) 106 (20ndash248) 25 (04ndash122)
Bilirubin day 6 (range) 17 (14ndash18) 55 (55) 195 (567ndash269) 35 (06ndash213)
LVEF day 2 (range) 377 (30ndash43) 54 (54) 24 (20ndash40) 33 (7ndash68)
LVEF day 6 (range) 61 (50ndash67) 62 (62) 55 (38ndash64) 374 (18ndash65)
Weaned off ECMO () 4 (100) 2 (667) 4 (80) 56 (70)
Complications
Limb ischemia 2 1 0 6
Massive GI bleeding 0 1 2 1
Corneal erosion 0 0 1 0
ARDSPneumonia 0 1 0 8
Reinstitution o ECMO 1 0 0 1
Severe brain insult 23
Further intervention
CABG n 0 0 0 26
Repair VSDwall n 0 0 0 4
VAD n 0 0 0 3
Heart transplantation n 0 0 0 1
Adrenalectomy n 3 0 0 0
Cause o mortality
Sepsis-related MOF 0 1 0 7
Hepatic ailure MOF 0 0 1 0
Cardiogenic shock 0 1 1 28
Continued
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 68
wwwnaturecomscientificreports
6SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
Discussiono the best o our knowledge this report constitutes the largest series to date describing the outcomeso patients presenting with reractory shock caused by endocrine emergencies (ie PC S and DK)rescued by ECMO support A total o 12 cases were identified in our registry rom 2005 to 2012 indicat-ing that the incidence o endocrine emergencies is low but not negligible Pheochromocytoma has been
estimated to be present in approximately 03 o all patients undergoing evaluation or secondary causeso hypertension18 Moreover S and DK accounts or 2 and 86 o all hospital admissions in patientswith thyrotoxicosis and type 1 diabetes mellitus respectively 1920 In general endocrine emergencies canhave a rapid and aggressive clinical course and pose significant diagnostic challenges (because they canmimic either AMI or acute congestive heart ailure) Endocrine emergencies are not common and prob-ably misdiagnosed in many cases and the clinical value o ECMO support in their clinical managementremains unclear Notably ollowing our report o a patient with PC who was successully rescued byECMO in January 20089 seven additional cases were described (a finding that illustrates the magnitudeo the potential underestimation as well as a recent increase in awareness)10ndash16
In the current series all patients with PC did not have a known history o pheochromocytoma Temain diagnostic eatures o PC consisted o extreme blood pressure fluctuations in presence o patentcoronary arteries on angiography Compared with AMI patients inotropic agents were more rapidlytapered and myocardial unction recovered significantly more quickly in PC However two o the ourpatients with PC (50) developed limb ischemia a percentage which was significantly higher than those
observed in both the DK (one patient 33) and AMI (six patients 75) groups (able 3) o our knowl-edge a total o 12 cases o pheochromocytoma-associated peripheral limb ischemia have been reportedto date21 In this scenario early recognition and treatment o pheochromocytoma through adrenalectomyor alpha-adrenergic blocking agents is paramount to reduce the risk o devastating limb ischemia
In this series most patients with S were initially misdiagnosed as having AMI or severe conges-tive heart ailure Hyperbilirubinemia was a common finding in S patients most likely caused by adirect hepatotoxic effect o excess thyroid hormones andor hepatic congestion resulting rom thyroidstorm Although anti-thyroid drugs (eg propylthiouracil) can cause cholestatic liver injury previousstudies conducted in S patients have shown that jaundice can successully respond to anti-thyroidmedications2223 Consequently the timely detection o S is crucial to the successul preservation oliver unction
Blood glucose levels are routinely checked in all o the patients admitted to our emergency depart-ment with disturbances o consciousness Te diagnosis o DK can be easily established upon admissionin presence o hyperglycemia metabolic acidosis and increased serum or urine ketones In generaldelays to seek medical care and the presence o sepsis andor coma have adverse consequences or DKpatientsrsquo clinical outcomes
In the current study AMI patients had lower SOFA scores and higher levels o cardiac enzymes thanthose with endocrine emergencies Notably the lef ventricular ejection unction and the clinical out-comes were poorer in patients with AMI than in those with endocrine emergencies rescued by ECMO(able 3) Similarly the number o patients who required long-term inotropic agents was higher in theAMI group
aken together there are three main findings rom the current single-center study 1) endocrineemergencies are rare but not negligible events 2) patients with endocrine emergencies presenting withacute reractory shock can be successully rescued by ECMO support and 3) screening o endocrineemergencies is essential in patients with acute reractory shock requiring mechanical support Albeitpreliminary in nature because o the small sample size our results may stimulate urther studies on thecost-benefits analysis o routine screening o thyroid hormones catecholamines and metanephrines inpatients presenting with acute circulatory collapse in need o ECMO support
PC (n= 4) DK (n= 3) TS (n= 5) AMI (n= 80)
Brain death 0 0 0 3
ARDS 0 0 0 2
Survival to discharge () 4 (100) 1 (333) 3 (60) 40 (50)
Survivors with CPC I n () 4 (100 ) 1 (100) 2 (667) 32 (80)
Table 3 Comparisons of patients with endocrine crisis and acute myocardial infarction rescued
with ECMO support Abbreviations AMI acute myocardial inarction ARDS acute respiratory distresssyndrome CABG coronary artery bypass surgery CK creatine kinase CPC cerebral perormance categoryCPR cardiac pulmonary resuscitation DK diabetic ketoacidosis GI gastrointestinal IABP intra-aortic
balloon pumping ICU intensive care unit IE inotropic equivalents LVEF lef ventricular ejection ractionMAP mean arterial pressure MOF multiple organ ailure PC pheochromocytoma crisis SOFA sepsis-related organ ailure assessment n-I troponin-I S thyroid storm VAD ventricular assist device VSD
ventricular septal deect
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 78
wwwnaturecomscientificreports
7SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
ConclusionsSuccessul management o endocrine emergencies depends on prompt recognition correction o theunderlying hormone alterations and immediate treatment o shock Unortunately numerous patientspresenting with endocrine emergencies have an unknown previous history o hormone imbalanceTereore the screening o endocrine emergencies is important in these patients Herein we have shownthat ECMO support is clinically useul in patients diagnosed with endocrine emergencies presenting withacute circulatory ailure Because medical care is extremely challenging in this scenario the awareness othe clinical value o ECMO among physicians managing patients with endocrine emergencies may helpimprove clinical outcomes
References1 Pee983147 G J et al Efficacy and economic assessment o conventional ventilatory support versus extracorporeal membrane
oxygenation or severe adult respiratory ailure (CESA983122) a multicentre randomised controlled trial Lancet 374 1351ndash1363(2009)
2 Baud F J Megarbane B Deye N amp Leprince P Clinical review Aggressive management and extracorporeal support or drug-induced cardiotoxicity Crit Care Doi 101186cc5700 (2007)
3 Chen Y S et al 983122escue or acute myocarditis with shoc983147 by extracorporeal membrane oxygenation Ann Torac Surg 68 2220ndash2224 (1999)
4 Chou N 983115 et al Application o extracorporeal membrane oxygenation in adult burn patients Artif Organs 25 622ndash626 (2001)5 Chen Y S et al Cardiopulmonary resuscitation with assisted extracorporeal lie-support versus conventional cardiopulmonary
resuscitation in adults with in-hospital cardiac arrest an observational study and propensity analysis Lancet 372 554ndash561(2008)
6 983115o W J et al Extracorporeal membrane support or adult postcardiotomy cardiogenic shoc983147 Ann Torac Surg 73 538ndash545(2003)
7 Ariza-Soleacute A et al Ventricular support With Extracorporeal Membrane Oxygenation A New 983122escue Alternative or 983122eractoryCardiogenic Shoc983147 983122ev Esp Cardiol 66 501ndash503 (2013)
8 Chen Y S et al Analysis and results o prolonged resuscitation in cardiac arrest patients rescued by extracorporeal membraneoxygenation J Am Coll Cardiol 41 197ndash203 (2003)
9 Chao A Yeh Y C Yen S amp Chen Y S Phaeochromocytoma crisis ndash a rare indication or extracorporeal membraneoxygenation Anaesthesia 63 86ndash88 (2008)
10 Suh I W et al Catastrophic catecholamine-induced cardiomyopathy mimic983147ing acute myocardial inarction rescued byextracorporeal membrane oxygenation (ECMO) in pheochromocytoma J 983115orean Med Sci 23 350ndash354 (2008)
11 Ezri Golan A Sasson L amp 983122ozenman Y Pheochromocytoma induced ulminant cardiogenic shoc983147 ollowing laparoscopicsalpingectomy successully managed with extracorporeal membrane oxygenation Jurnalul 983122omacircn de Anestezie erapie Intensivatilde 16 154ndash158 (2008)
12 983122itter S Guertler Meier C A amp Genoni M Cardiogenic shoc983147 due to pheochromocytoma rescued by extracorporealmembrane oxygenation Interact Cardiovasc Torac Surg 13 112ndash113 (2011)
13 Noorani A Vuylste983147e A Lewis C Parameshwar J amp Catarino P A moribund athlete Lance 380 74 (2012)14 Ghassam S et al Successul extracorporeal membrane oxygenation treatment or pheochromocytoma-induced acute cardiac
ailure AJEM 30 1017e1ndash1017e3 (2012)15 Banfi C et al Central extracorporeal lie support in pheochromocytoma crisis Ann Torac Surg 93 1303ndash1305 (2012)16 Sheinberg 983122 et al Case 1ndash2012 A perect storm atality resulting rom metoclopramide unmas983147ing a pheochromocytoma and
its management J Cardiothorac Vasc Anesth 26 161ndash115 (2012)17 Vincent J L et al Te SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysunctionailure On behal
o the Wor983147ing Group on Sepsis-983122elated Problems o the European Society o Intensive Care Medicine Intensive Care Med 22 707ndash710 (1996)
18 Streeten D H Anderson G H Jr amp Wagner S Effect o age on response o secondary hypertension to specific treatment Am J Hypertens 3 360ndash365 (1990)
19 983115earney amp Dang C Diabetic and endocrine emergencies Postgrad Med J 83 79ndash86 (2007)20 983122ingel M D Management o hypothyroidism and hyperthyroidism in the intensive care unit Crit Care Clin 17 59ndash74 (2001)21 Lutchman D Buchholz S amp 983115eightley C Pheochromocytomandashassociated critical peripheral ischemia Intern Med J 40 150ndash159
(2010)22 Hull 983115 et al wo cases o thyroid storm-associated cholestatic jaundice Endocr Pract 13 478ndash480 (2007)23 Hambleton C et al Tyroid storm complicated by ulminant hepatic ailure Case report and literature review Ann Otol 983122hinol
Laryngol 22 679ndash682 (2013)
AcknowledgementsTis study was partially supported by the National Science Council (102-2325-B-002-009 101-2325-B-002-009 100-2314-B-002-018-MY2 and 100-2325-B-002-009) Ministry o Science and echnologyaiwan and partially unded by the National aiwan University Hospital MG 213 und
Author ContributionsAC HYY and YSC study design AC CHW and HJY draf o the manuscript tables and figuresNKC LJ NHC and MHL data collection and analysis AC and NHC manuscript editingNKC HYY MHL CHW and HJY literature review and data checking SCH IHW and YSCcritical revision o the manuscript or important intellectual content All authors final approval o themanuscript
Additional InformationCompeting financial interests Te authors declare no competing financial interests
How to cite this article Chao A et al Highlighting indication o extracorporeal membraneoxygenation in endocrine emergencies Sci Rep 5 13361 doi 101038srep13361 (2015)
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 88
wwwnaturecomscientificreports
8SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
Tis work is licensed under a Creative Commons Attribution 40 International License Teimages or other third party material in this article are included in the articlersquos Creative Com-
mons license unless indicated otherwise in the credit line i the material is not included under theCreative Commons license users will need to obtain permission rom the license holder to reproducethe material o view a copy o this license visit httpcreativecommonsorglicensesby40
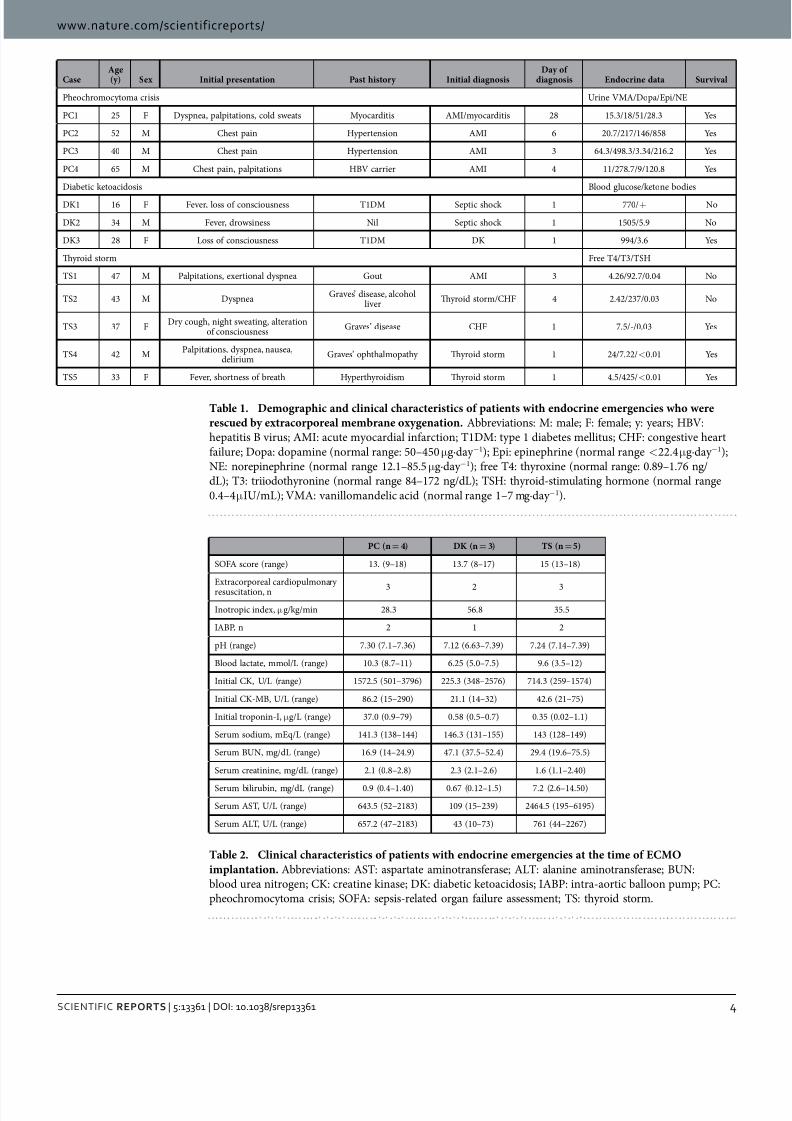
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 48
wwwnaturecomscientificreports
4SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
CaseAge(y) Sex Initial presentation Past history Initial diagnosis
Day ofdiagnosis Endocrine data Survival
Pheochromocytoma crisis Urine VMADopaEpiNE
PC1 25 F Dyspnea palpitations cold sweats Myocarditis AMImyocarditis 28 1531851283 Yes
PC2 52 M Chest pain Hypertension AMI 6 207217146858 Yes
PC3 40 M Chest pain Hypertension AMI 3 64349833342162 Yes
PC4 65 M Chest pain palpitations HBV carrier AMI 4 11278791208 Yes
Diabetic ketoacidosis Blood glucoseketone bodies
DK1 16 F Fever loss o consciousness 1DM Septic shock 1 770+ No
DK2 34 M Fever drowsiness Nil Septic shock 1 150559 No
DK3 28 F Loss o consciousness 1DM DK 1 99436 Yes
Tyroid storm Free 43SH
S1 47 M Palpitations exertional dyspnea Gout AMI 3 426927004 No
S2 43 M DyspneaGravesrsquo disease alcohol
liverTyroid stormCHF 4 242237003 No
S3 37 FDry cough night sweating alteration
o consciousnessGravesrsquo disease CHF 1 75-003 Yes
S4 42 MPalpitations dyspnea nausea
deliriumGravesrsquo ophthalmopathy Tyroid storm 1 24722lt 001 Yes
S5 33 F Fever shortness o breath Hyperthyroidism Tyroid storm 1 45425lt 001 Yes
Table 1 Demographic and clinical characteristics of patients with endocrine emergencies who were
rescued by extracorporeal membrane oxygenation Abbreviations M male F emale y years HBVhepatitis B virus AMI acute myocardial inarction 1DM type 1 diabetes mellitus CHF congestive heart
ailure Dopa dopamine (normal range 50ndash450 micro gmiddotday minus1) Epi epinephrine (normal range lt 224micro gmiddotday minus1)NE norepinephrine (normal range 121ndash855 micro gmiddotday minus1) ree 4 thyroxine (normal range 089ndash176 ngdL) 3 triiodothyronine (normal range 84ndash172 ngdL) SH thyroid-stimulating hormone (normal range
04ndash4micro IUmL) VMA vanillomandelic acid (normal range 1ndash7 mgmiddotday minus1)
PC (n= 4) DK (n= 3) TS (n= 5)
SOFA score (range) 13 (9ndash18) 137 (8ndash17) 15 (13ndash18)
Extracorporeal cardiopulmonaryresuscitation n 3 2 3
Inotropic index microgkgmin 283 568 355
IABP n 2 1 2
pH (range) 730 (71ndash736) 712 (663ndash739) 724 (714ndash739)
Blood lactate mmolL (range) 103 (87ndash11) 625 (50ndash75) 96 (35ndash12)
Initial CK UL (range) 15725 (501ndash3796) 2253 (348ndash2576) 7143 (259ndash1574)
Initial CK-MB UL (range) 862 (15ndash290) 211 (14ndash32) 426 (21ndash75)
Initial troponin-I micro gL (range) 370 (09ndash79) 058 (05ndash07) 035 (002ndash11)
Serum sodium mEqL (range) 1413 (138ndash144) 1463 (131ndash155) 143 (128ndash149)
Serum BUN mgdL (range) 169 (14ndash249) 471 (375ndash524) 294 (196ndash755)
Serum creatinine mgdL (range) 21 (08ndash28) 23 (21ndash26) 16 (11ndash240)
Serum bilirubin mgdL (range) 09 (04ndash140) 067 (012ndash15) 72 (26ndash1450)
Serum AS UL (range) 6435 (52ndash2183) 109 (15ndash239) 24645 (195ndash6195)
Serum AL UL (range) 6572 (47ndash2183) 43 (10ndash73) 761 (44ndash2267)
Table 2 Clinical characteristics of patients with endocrine emergencies at the time of ECMO
implantation Abbreviations AS aspartate aminotranserase AL alanine aminotranserase BUNblood urea nitrogen CK creatine kinase DK diabetic ketoacidosis IABP intra-aortic balloon pump PCpheochromocytoma crisis SOFA sepsis-related organ ailure assessment S thyroid storm
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 58
wwwnaturecomscientificreports
5SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
PC (n= 4) DK (n= 3) TS (n= 5) AMI (n= 80)
Age years (range) 455 (25ndash65) 26 (16ndash34) 404 (33ndash47) 538 (31ndash65)
Male sex n () 3 (75) 1 (333) 3 (60) 75 (94)
CPR n () 3 (75) 2 (66) 3 (60) 55 (687)
ECMO duration hour (range) 1025 (447ndash1625) 1345 (09ndash3818) 82 (19ndash1156) 117 (54ndash475)
Ventilator support day (range) 14 (6ndash22) 177 (1ndash51) 10 (4ndash26) 177 (1ndash95)
ICU length o stay day (range) 208 (6ndash28) 180 (0ndash51) 118 (5ndash26) 216 (1ndash147)
Initial SOFA score (range) 13 (9ndash18) 137 (8ndash17) 15 (13ndash18) 104 (3ndash18)
MAP Day 1 mmHg (range) 120 (101ndash137) 97 (96ndash99) 84 (63ndash101) 74 (30ndash144)
Day 3 (range) 121 (91ndash146) 85 (84ndash86) 113 (104ndash126) 76 ( 920ndash112)
Day 6 (range) 130 (116ndash145) 99 (99) 114 (93ndash132) 88 (61ndash118)
Pre-ECMO IE micro gkgmin 283 568 355 214
IE day 3 (range) 47 (21ndash70) 324 (324) 46 (0ndash184) 241 (0ndash810)
IE day 6 (range) 14 (0ndash54) 115 (115) 0 (0) 82 (0ndash318)
Patients using inotropes at day 6n ()
1 (25) 1 (33) 0 (0) 50 (625)
Initial CK UL (range) 15725 (501ndash3796) 2253 (348ndash2576) 714 (259ndash1574) 2413 (41ndash28480)
CK day 3 (range) 14589 (1528ndash47829) 385 (385) 83645 (515ndash4446) 58084 (77ndash66274)
CK day 6 (range) 22637 (530ndash13721) 4496 (4496) 501 (114ndash888) 31634 (33ndash36621)
Initial CK-MB UL (range) 862 (15ndash290) 211 (14ndash32) 426 (21ndash75) 172 (42ndash23198)
CK-MB day 3 (range) 3892 (909ndash10031) 522 (522) 535 (396ndash646) 1321 (15ndash1782)
CK-MB day 6 (range) 66 (157ndash207) 26 (26) 451 (407ndash494) 504 (12ndash3089)
Initial n-I microgL (range) 370 (9ndash79) 058 (05ndash07) 035 (002ndash11) 19 (001ndash100)
n-I day 3 (range) 161 (94ndash244) 04 (04) 12 (05ndash18) 377 (044ndash94)
n-I day 6 (range) 22 (126ndash31) Not available Not available 161 (031ndash33)
Lactate in 24 h mmolL (range) 103 (87ndash11) 625 (50ndash75) 96 (35ndash12) 89 (1ndash35)
Dialysis patients n 3 1 1 36
IABP (at implantation) 2 1 1 25 (32)
Bilirubin day 3 mgdL (range) 13 (10ndash19) 09 (09) 106 (20ndash248) 25 (04ndash122)
Bilirubin day 6 (range) 17 (14ndash18) 55 (55) 195 (567ndash269) 35 (06ndash213)
LVEF day 2 (range) 377 (30ndash43) 54 (54) 24 (20ndash40) 33 (7ndash68)
LVEF day 6 (range) 61 (50ndash67) 62 (62) 55 (38ndash64) 374 (18ndash65)
Weaned off ECMO () 4 (100) 2 (667) 4 (80) 56 (70)
Complications
Limb ischemia 2 1 0 6
Massive GI bleeding 0 1 2 1
Corneal erosion 0 0 1 0
ARDSPneumonia 0 1 0 8
Reinstitution o ECMO 1 0 0 1
Severe brain insult 23
Further intervention
CABG n 0 0 0 26
Repair VSDwall n 0 0 0 4
VAD n 0 0 0 3
Heart transplantation n 0 0 0 1
Adrenalectomy n 3 0 0 0
Cause o mortality
Sepsis-related MOF 0 1 0 7
Hepatic ailure MOF 0 0 1 0
Cardiogenic shock 0 1 1 28
Continued
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 68
wwwnaturecomscientificreports
6SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
Discussiono the best o our knowledge this report constitutes the largest series to date describing the outcomeso patients presenting with reractory shock caused by endocrine emergencies (ie PC S and DK)rescued by ECMO support A total o 12 cases were identified in our registry rom 2005 to 2012 indicat-ing that the incidence o endocrine emergencies is low but not negligible Pheochromocytoma has been
estimated to be present in approximately 03 o all patients undergoing evaluation or secondary causeso hypertension18 Moreover S and DK accounts or 2 and 86 o all hospital admissions in patientswith thyrotoxicosis and type 1 diabetes mellitus respectively 1920 In general endocrine emergencies canhave a rapid and aggressive clinical course and pose significant diagnostic challenges (because they canmimic either AMI or acute congestive heart ailure) Endocrine emergencies are not common and prob-ably misdiagnosed in many cases and the clinical value o ECMO support in their clinical managementremains unclear Notably ollowing our report o a patient with PC who was successully rescued byECMO in January 20089 seven additional cases were described (a finding that illustrates the magnitudeo the potential underestimation as well as a recent increase in awareness)10ndash16
In the current series all patients with PC did not have a known history o pheochromocytoma Temain diagnostic eatures o PC consisted o extreme blood pressure fluctuations in presence o patentcoronary arteries on angiography Compared with AMI patients inotropic agents were more rapidlytapered and myocardial unction recovered significantly more quickly in PC However two o the ourpatients with PC (50) developed limb ischemia a percentage which was significantly higher than those
observed in both the DK (one patient 33) and AMI (six patients 75) groups (able 3) o our knowl-edge a total o 12 cases o pheochromocytoma-associated peripheral limb ischemia have been reportedto date21 In this scenario early recognition and treatment o pheochromocytoma through adrenalectomyor alpha-adrenergic blocking agents is paramount to reduce the risk o devastating limb ischemia
In this series most patients with S were initially misdiagnosed as having AMI or severe conges-tive heart ailure Hyperbilirubinemia was a common finding in S patients most likely caused by adirect hepatotoxic effect o excess thyroid hormones andor hepatic congestion resulting rom thyroidstorm Although anti-thyroid drugs (eg propylthiouracil) can cause cholestatic liver injury previousstudies conducted in S patients have shown that jaundice can successully respond to anti-thyroidmedications2223 Consequently the timely detection o S is crucial to the successul preservation oliver unction
Blood glucose levels are routinely checked in all o the patients admitted to our emergency depart-ment with disturbances o consciousness Te diagnosis o DK can be easily established upon admissionin presence o hyperglycemia metabolic acidosis and increased serum or urine ketones In generaldelays to seek medical care and the presence o sepsis andor coma have adverse consequences or DKpatientsrsquo clinical outcomes
In the current study AMI patients had lower SOFA scores and higher levels o cardiac enzymes thanthose with endocrine emergencies Notably the lef ventricular ejection unction and the clinical out-comes were poorer in patients with AMI than in those with endocrine emergencies rescued by ECMO(able 3) Similarly the number o patients who required long-term inotropic agents was higher in theAMI group
aken together there are three main findings rom the current single-center study 1) endocrineemergencies are rare but not negligible events 2) patients with endocrine emergencies presenting withacute reractory shock can be successully rescued by ECMO support and 3) screening o endocrineemergencies is essential in patients with acute reractory shock requiring mechanical support Albeitpreliminary in nature because o the small sample size our results may stimulate urther studies on thecost-benefits analysis o routine screening o thyroid hormones catecholamines and metanephrines inpatients presenting with acute circulatory collapse in need o ECMO support
PC (n= 4) DK (n= 3) TS (n= 5) AMI (n= 80)
Brain death 0 0 0 3
ARDS 0 0 0 2
Survival to discharge () 4 (100) 1 (333) 3 (60) 40 (50)
Survivors with CPC I n () 4 (100 ) 1 (100) 2 (667) 32 (80)
Table 3 Comparisons of patients with endocrine crisis and acute myocardial infarction rescued
with ECMO support Abbreviations AMI acute myocardial inarction ARDS acute respiratory distresssyndrome CABG coronary artery bypass surgery CK creatine kinase CPC cerebral perormance categoryCPR cardiac pulmonary resuscitation DK diabetic ketoacidosis GI gastrointestinal IABP intra-aortic
balloon pumping ICU intensive care unit IE inotropic equivalents LVEF lef ventricular ejection ractionMAP mean arterial pressure MOF multiple organ ailure PC pheochromocytoma crisis SOFA sepsis-related organ ailure assessment n-I troponin-I S thyroid storm VAD ventricular assist device VSD
ventricular septal deect
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 78
wwwnaturecomscientificreports
7SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
ConclusionsSuccessul management o endocrine emergencies depends on prompt recognition correction o theunderlying hormone alterations and immediate treatment o shock Unortunately numerous patientspresenting with endocrine emergencies have an unknown previous history o hormone imbalanceTereore the screening o endocrine emergencies is important in these patients Herein we have shownthat ECMO support is clinically useul in patients diagnosed with endocrine emergencies presenting withacute circulatory ailure Because medical care is extremely challenging in this scenario the awareness othe clinical value o ECMO among physicians managing patients with endocrine emergencies may helpimprove clinical outcomes
References1 Pee983147 G J et al Efficacy and economic assessment o conventional ventilatory support versus extracorporeal membrane
oxygenation or severe adult respiratory ailure (CESA983122) a multicentre randomised controlled trial Lancet 374 1351ndash1363(2009)
2 Baud F J Megarbane B Deye N amp Leprince P Clinical review Aggressive management and extracorporeal support or drug-induced cardiotoxicity Crit Care Doi 101186cc5700 (2007)
3 Chen Y S et al 983122escue or acute myocarditis with shoc983147 by extracorporeal membrane oxygenation Ann Torac Surg 68 2220ndash2224 (1999)
4 Chou N 983115 et al Application o extracorporeal membrane oxygenation in adult burn patients Artif Organs 25 622ndash626 (2001)5 Chen Y S et al Cardiopulmonary resuscitation with assisted extracorporeal lie-support versus conventional cardiopulmonary
resuscitation in adults with in-hospital cardiac arrest an observational study and propensity analysis Lancet 372 554ndash561(2008)
6 983115o W J et al Extracorporeal membrane support or adult postcardiotomy cardiogenic shoc983147 Ann Torac Surg 73 538ndash545(2003)
7 Ariza-Soleacute A et al Ventricular support With Extracorporeal Membrane Oxygenation A New 983122escue Alternative or 983122eractoryCardiogenic Shoc983147 983122ev Esp Cardiol 66 501ndash503 (2013)
8 Chen Y S et al Analysis and results o prolonged resuscitation in cardiac arrest patients rescued by extracorporeal membraneoxygenation J Am Coll Cardiol 41 197ndash203 (2003)
9 Chao A Yeh Y C Yen S amp Chen Y S Phaeochromocytoma crisis ndash a rare indication or extracorporeal membraneoxygenation Anaesthesia 63 86ndash88 (2008)
10 Suh I W et al Catastrophic catecholamine-induced cardiomyopathy mimic983147ing acute myocardial inarction rescued byextracorporeal membrane oxygenation (ECMO) in pheochromocytoma J 983115orean Med Sci 23 350ndash354 (2008)
11 Ezri Golan A Sasson L amp 983122ozenman Y Pheochromocytoma induced ulminant cardiogenic shoc983147 ollowing laparoscopicsalpingectomy successully managed with extracorporeal membrane oxygenation Jurnalul 983122omacircn de Anestezie erapie Intensivatilde 16 154ndash158 (2008)
12 983122itter S Guertler Meier C A amp Genoni M Cardiogenic shoc983147 due to pheochromocytoma rescued by extracorporealmembrane oxygenation Interact Cardiovasc Torac Surg 13 112ndash113 (2011)
13 Noorani A Vuylste983147e A Lewis C Parameshwar J amp Catarino P A moribund athlete Lance 380 74 (2012)14 Ghassam S et al Successul extracorporeal membrane oxygenation treatment or pheochromocytoma-induced acute cardiac
ailure AJEM 30 1017e1ndash1017e3 (2012)15 Banfi C et al Central extracorporeal lie support in pheochromocytoma crisis Ann Torac Surg 93 1303ndash1305 (2012)16 Sheinberg 983122 et al Case 1ndash2012 A perect storm atality resulting rom metoclopramide unmas983147ing a pheochromocytoma and
its management J Cardiothorac Vasc Anesth 26 161ndash115 (2012)17 Vincent J L et al Te SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysunctionailure On behal
o the Wor983147ing Group on Sepsis-983122elated Problems o the European Society o Intensive Care Medicine Intensive Care Med 22 707ndash710 (1996)
18 Streeten D H Anderson G H Jr amp Wagner S Effect o age on response o secondary hypertension to specific treatment Am J Hypertens 3 360ndash365 (1990)
19 983115earney amp Dang C Diabetic and endocrine emergencies Postgrad Med J 83 79ndash86 (2007)20 983122ingel M D Management o hypothyroidism and hyperthyroidism in the intensive care unit Crit Care Clin 17 59ndash74 (2001)21 Lutchman D Buchholz S amp 983115eightley C Pheochromocytomandashassociated critical peripheral ischemia Intern Med J 40 150ndash159
(2010)22 Hull 983115 et al wo cases o thyroid storm-associated cholestatic jaundice Endocr Pract 13 478ndash480 (2007)23 Hambleton C et al Tyroid storm complicated by ulminant hepatic ailure Case report and literature review Ann Otol 983122hinol
Laryngol 22 679ndash682 (2013)
AcknowledgementsTis study was partially supported by the National Science Council (102-2325-B-002-009 101-2325-B-002-009 100-2314-B-002-018-MY2 and 100-2325-B-002-009) Ministry o Science and echnologyaiwan and partially unded by the National aiwan University Hospital MG 213 und
Author ContributionsAC HYY and YSC study design AC CHW and HJY draf o the manuscript tables and figuresNKC LJ NHC and MHL data collection and analysis AC and NHC manuscript editingNKC HYY MHL CHW and HJY literature review and data checking SCH IHW and YSCcritical revision o the manuscript or important intellectual content All authors final approval o themanuscript
Additional InformationCompeting financial interests Te authors declare no competing financial interests
How to cite this article Chao A et al Highlighting indication o extracorporeal membraneoxygenation in endocrine emergencies Sci Rep 5 13361 doi 101038srep13361 (2015)
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 88
wwwnaturecomscientificreports
8SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
Tis work is licensed under a Creative Commons Attribution 40 International License Teimages or other third party material in this article are included in the articlersquos Creative Com-
mons license unless indicated otherwise in the credit line i the material is not included under theCreative Commons license users will need to obtain permission rom the license holder to reproducethe material o view a copy o this license visit httpcreativecommonsorglicensesby40

8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 58
wwwnaturecomscientificreports
5SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
PC (n= 4) DK (n= 3) TS (n= 5) AMI (n= 80)
Age years (range) 455 (25ndash65) 26 (16ndash34) 404 (33ndash47) 538 (31ndash65)
Male sex n () 3 (75) 1 (333) 3 (60) 75 (94)
CPR n () 3 (75) 2 (66) 3 (60) 55 (687)
ECMO duration hour (range) 1025 (447ndash1625) 1345 (09ndash3818) 82 (19ndash1156) 117 (54ndash475)
Ventilator support day (range) 14 (6ndash22) 177 (1ndash51) 10 (4ndash26) 177 (1ndash95)
ICU length o stay day (range) 208 (6ndash28) 180 (0ndash51) 118 (5ndash26) 216 (1ndash147)
Initial SOFA score (range) 13 (9ndash18) 137 (8ndash17) 15 (13ndash18) 104 (3ndash18)
MAP Day 1 mmHg (range) 120 (101ndash137) 97 (96ndash99) 84 (63ndash101) 74 (30ndash144)
Day 3 (range) 121 (91ndash146) 85 (84ndash86) 113 (104ndash126) 76 ( 920ndash112)
Day 6 (range) 130 (116ndash145) 99 (99) 114 (93ndash132) 88 (61ndash118)
Pre-ECMO IE micro gkgmin 283 568 355 214
IE day 3 (range) 47 (21ndash70) 324 (324) 46 (0ndash184) 241 (0ndash810)
IE day 6 (range) 14 (0ndash54) 115 (115) 0 (0) 82 (0ndash318)
Patients using inotropes at day 6n ()
1 (25) 1 (33) 0 (0) 50 (625)
Initial CK UL (range) 15725 (501ndash3796) 2253 (348ndash2576) 714 (259ndash1574) 2413 (41ndash28480)
CK day 3 (range) 14589 (1528ndash47829) 385 (385) 83645 (515ndash4446) 58084 (77ndash66274)
CK day 6 (range) 22637 (530ndash13721) 4496 (4496) 501 (114ndash888) 31634 (33ndash36621)
Initial CK-MB UL (range) 862 (15ndash290) 211 (14ndash32) 426 (21ndash75) 172 (42ndash23198)
CK-MB day 3 (range) 3892 (909ndash10031) 522 (522) 535 (396ndash646) 1321 (15ndash1782)
CK-MB day 6 (range) 66 (157ndash207) 26 (26) 451 (407ndash494) 504 (12ndash3089)
Initial n-I microgL (range) 370 (9ndash79) 058 (05ndash07) 035 (002ndash11) 19 (001ndash100)
n-I day 3 (range) 161 (94ndash244) 04 (04) 12 (05ndash18) 377 (044ndash94)
n-I day 6 (range) 22 (126ndash31) Not available Not available 161 (031ndash33)
Lactate in 24 h mmolL (range) 103 (87ndash11) 625 (50ndash75) 96 (35ndash12) 89 (1ndash35)
Dialysis patients n 3 1 1 36
IABP (at implantation) 2 1 1 25 (32)
Bilirubin day 3 mgdL (range) 13 (10ndash19) 09 (09) 106 (20ndash248) 25 (04ndash122)
Bilirubin day 6 (range) 17 (14ndash18) 55 (55) 195 (567ndash269) 35 (06ndash213)
LVEF day 2 (range) 377 (30ndash43) 54 (54) 24 (20ndash40) 33 (7ndash68)
LVEF day 6 (range) 61 (50ndash67) 62 (62) 55 (38ndash64) 374 (18ndash65)
Weaned off ECMO () 4 (100) 2 (667) 4 (80) 56 (70)
Complications
Limb ischemia 2 1 0 6
Massive GI bleeding 0 1 2 1
Corneal erosion 0 0 1 0
ARDSPneumonia 0 1 0 8
Reinstitution o ECMO 1 0 0 1
Severe brain insult 23
Further intervention
CABG n 0 0 0 26
Repair VSDwall n 0 0 0 4
VAD n 0 0 0 3
Heart transplantation n 0 0 0 1
Adrenalectomy n 3 0 0 0
Cause o mortality
Sepsis-related MOF 0 1 0 7
Hepatic ailure MOF 0 0 1 0
Cardiogenic shock 0 1 1 28
Continued
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 68
wwwnaturecomscientificreports
6SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
Discussiono the best o our knowledge this report constitutes the largest series to date describing the outcomeso patients presenting with reractory shock caused by endocrine emergencies (ie PC S and DK)rescued by ECMO support A total o 12 cases were identified in our registry rom 2005 to 2012 indicat-ing that the incidence o endocrine emergencies is low but not negligible Pheochromocytoma has been
estimated to be present in approximately 03 o all patients undergoing evaluation or secondary causeso hypertension18 Moreover S and DK accounts or 2 and 86 o all hospital admissions in patientswith thyrotoxicosis and type 1 diabetes mellitus respectively 1920 In general endocrine emergencies canhave a rapid and aggressive clinical course and pose significant diagnostic challenges (because they canmimic either AMI or acute congestive heart ailure) Endocrine emergencies are not common and prob-ably misdiagnosed in many cases and the clinical value o ECMO support in their clinical managementremains unclear Notably ollowing our report o a patient with PC who was successully rescued byECMO in January 20089 seven additional cases were described (a finding that illustrates the magnitudeo the potential underestimation as well as a recent increase in awareness)10ndash16
In the current series all patients with PC did not have a known history o pheochromocytoma Temain diagnostic eatures o PC consisted o extreme blood pressure fluctuations in presence o patentcoronary arteries on angiography Compared with AMI patients inotropic agents were more rapidlytapered and myocardial unction recovered significantly more quickly in PC However two o the ourpatients with PC (50) developed limb ischemia a percentage which was significantly higher than those
observed in both the DK (one patient 33) and AMI (six patients 75) groups (able 3) o our knowl-edge a total o 12 cases o pheochromocytoma-associated peripheral limb ischemia have been reportedto date21 In this scenario early recognition and treatment o pheochromocytoma through adrenalectomyor alpha-adrenergic blocking agents is paramount to reduce the risk o devastating limb ischemia
In this series most patients with S were initially misdiagnosed as having AMI or severe conges-tive heart ailure Hyperbilirubinemia was a common finding in S patients most likely caused by adirect hepatotoxic effect o excess thyroid hormones andor hepatic congestion resulting rom thyroidstorm Although anti-thyroid drugs (eg propylthiouracil) can cause cholestatic liver injury previousstudies conducted in S patients have shown that jaundice can successully respond to anti-thyroidmedications2223 Consequently the timely detection o S is crucial to the successul preservation oliver unction
Blood glucose levels are routinely checked in all o the patients admitted to our emergency depart-ment with disturbances o consciousness Te diagnosis o DK can be easily established upon admissionin presence o hyperglycemia metabolic acidosis and increased serum or urine ketones In generaldelays to seek medical care and the presence o sepsis andor coma have adverse consequences or DKpatientsrsquo clinical outcomes
In the current study AMI patients had lower SOFA scores and higher levels o cardiac enzymes thanthose with endocrine emergencies Notably the lef ventricular ejection unction and the clinical out-comes were poorer in patients with AMI than in those with endocrine emergencies rescued by ECMO(able 3) Similarly the number o patients who required long-term inotropic agents was higher in theAMI group
aken together there are three main findings rom the current single-center study 1) endocrineemergencies are rare but not negligible events 2) patients with endocrine emergencies presenting withacute reractory shock can be successully rescued by ECMO support and 3) screening o endocrineemergencies is essential in patients with acute reractory shock requiring mechanical support Albeitpreliminary in nature because o the small sample size our results may stimulate urther studies on thecost-benefits analysis o routine screening o thyroid hormones catecholamines and metanephrines inpatients presenting with acute circulatory collapse in need o ECMO support
PC (n= 4) DK (n= 3) TS (n= 5) AMI (n= 80)
Brain death 0 0 0 3
ARDS 0 0 0 2
Survival to discharge () 4 (100) 1 (333) 3 (60) 40 (50)
Survivors with CPC I n () 4 (100 ) 1 (100) 2 (667) 32 (80)
Table 3 Comparisons of patients with endocrine crisis and acute myocardial infarction rescued
with ECMO support Abbreviations AMI acute myocardial inarction ARDS acute respiratory distresssyndrome CABG coronary artery bypass surgery CK creatine kinase CPC cerebral perormance categoryCPR cardiac pulmonary resuscitation DK diabetic ketoacidosis GI gastrointestinal IABP intra-aortic
balloon pumping ICU intensive care unit IE inotropic equivalents LVEF lef ventricular ejection ractionMAP mean arterial pressure MOF multiple organ ailure PC pheochromocytoma crisis SOFA sepsis-related organ ailure assessment n-I troponin-I S thyroid storm VAD ventricular assist device VSD
ventricular septal deect
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 78
wwwnaturecomscientificreports
7SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
ConclusionsSuccessul management o endocrine emergencies depends on prompt recognition correction o theunderlying hormone alterations and immediate treatment o shock Unortunately numerous patientspresenting with endocrine emergencies have an unknown previous history o hormone imbalanceTereore the screening o endocrine emergencies is important in these patients Herein we have shownthat ECMO support is clinically useul in patients diagnosed with endocrine emergencies presenting withacute circulatory ailure Because medical care is extremely challenging in this scenario the awareness othe clinical value o ECMO among physicians managing patients with endocrine emergencies may helpimprove clinical outcomes
References1 Pee983147 G J et al Efficacy and economic assessment o conventional ventilatory support versus extracorporeal membrane
oxygenation or severe adult respiratory ailure (CESA983122) a multicentre randomised controlled trial Lancet 374 1351ndash1363(2009)
2 Baud F J Megarbane B Deye N amp Leprince P Clinical review Aggressive management and extracorporeal support or drug-induced cardiotoxicity Crit Care Doi 101186cc5700 (2007)
3 Chen Y S et al 983122escue or acute myocarditis with shoc983147 by extracorporeal membrane oxygenation Ann Torac Surg 68 2220ndash2224 (1999)
4 Chou N 983115 et al Application o extracorporeal membrane oxygenation in adult burn patients Artif Organs 25 622ndash626 (2001)5 Chen Y S et al Cardiopulmonary resuscitation with assisted extracorporeal lie-support versus conventional cardiopulmonary
resuscitation in adults with in-hospital cardiac arrest an observational study and propensity analysis Lancet 372 554ndash561(2008)
6 983115o W J et al Extracorporeal membrane support or adult postcardiotomy cardiogenic shoc983147 Ann Torac Surg 73 538ndash545(2003)
7 Ariza-Soleacute A et al Ventricular support With Extracorporeal Membrane Oxygenation A New 983122escue Alternative or 983122eractoryCardiogenic Shoc983147 983122ev Esp Cardiol 66 501ndash503 (2013)
8 Chen Y S et al Analysis and results o prolonged resuscitation in cardiac arrest patients rescued by extracorporeal membraneoxygenation J Am Coll Cardiol 41 197ndash203 (2003)
9 Chao A Yeh Y C Yen S amp Chen Y S Phaeochromocytoma crisis ndash a rare indication or extracorporeal membraneoxygenation Anaesthesia 63 86ndash88 (2008)
10 Suh I W et al Catastrophic catecholamine-induced cardiomyopathy mimic983147ing acute myocardial inarction rescued byextracorporeal membrane oxygenation (ECMO) in pheochromocytoma J 983115orean Med Sci 23 350ndash354 (2008)
11 Ezri Golan A Sasson L amp 983122ozenman Y Pheochromocytoma induced ulminant cardiogenic shoc983147 ollowing laparoscopicsalpingectomy successully managed with extracorporeal membrane oxygenation Jurnalul 983122omacircn de Anestezie erapie Intensivatilde 16 154ndash158 (2008)
12 983122itter S Guertler Meier C A amp Genoni M Cardiogenic shoc983147 due to pheochromocytoma rescued by extracorporealmembrane oxygenation Interact Cardiovasc Torac Surg 13 112ndash113 (2011)
13 Noorani A Vuylste983147e A Lewis C Parameshwar J amp Catarino P A moribund athlete Lance 380 74 (2012)14 Ghassam S et al Successul extracorporeal membrane oxygenation treatment or pheochromocytoma-induced acute cardiac
ailure AJEM 30 1017e1ndash1017e3 (2012)15 Banfi C et al Central extracorporeal lie support in pheochromocytoma crisis Ann Torac Surg 93 1303ndash1305 (2012)16 Sheinberg 983122 et al Case 1ndash2012 A perect storm atality resulting rom metoclopramide unmas983147ing a pheochromocytoma and
its management J Cardiothorac Vasc Anesth 26 161ndash115 (2012)17 Vincent J L et al Te SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysunctionailure On behal
o the Wor983147ing Group on Sepsis-983122elated Problems o the European Society o Intensive Care Medicine Intensive Care Med 22 707ndash710 (1996)
18 Streeten D H Anderson G H Jr amp Wagner S Effect o age on response o secondary hypertension to specific treatment Am J Hypertens 3 360ndash365 (1990)
19 983115earney amp Dang C Diabetic and endocrine emergencies Postgrad Med J 83 79ndash86 (2007)20 983122ingel M D Management o hypothyroidism and hyperthyroidism in the intensive care unit Crit Care Clin 17 59ndash74 (2001)21 Lutchman D Buchholz S amp 983115eightley C Pheochromocytomandashassociated critical peripheral ischemia Intern Med J 40 150ndash159
(2010)22 Hull 983115 et al wo cases o thyroid storm-associated cholestatic jaundice Endocr Pract 13 478ndash480 (2007)23 Hambleton C et al Tyroid storm complicated by ulminant hepatic ailure Case report and literature review Ann Otol 983122hinol
Laryngol 22 679ndash682 (2013)
AcknowledgementsTis study was partially supported by the National Science Council (102-2325-B-002-009 101-2325-B-002-009 100-2314-B-002-018-MY2 and 100-2325-B-002-009) Ministry o Science and echnologyaiwan and partially unded by the National aiwan University Hospital MG 213 und
Author ContributionsAC HYY and YSC study design AC CHW and HJY draf o the manuscript tables and figuresNKC LJ NHC and MHL data collection and analysis AC and NHC manuscript editingNKC HYY MHL CHW and HJY literature review and data checking SCH IHW and YSCcritical revision o the manuscript or important intellectual content All authors final approval o themanuscript
Additional InformationCompeting financial interests Te authors declare no competing financial interests
How to cite this article Chao A et al Highlighting indication o extracorporeal membraneoxygenation in endocrine emergencies Sci Rep 5 13361 doi 101038srep13361 (2015)
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 88
wwwnaturecomscientificreports
8SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
Tis work is licensed under a Creative Commons Attribution 40 International License Teimages or other third party material in this article are included in the articlersquos Creative Com-
mons license unless indicated otherwise in the credit line i the material is not included under theCreative Commons license users will need to obtain permission rom the license holder to reproducethe material o view a copy o this license visit httpcreativecommonsorglicensesby40

8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 68
wwwnaturecomscientificreports
6SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
Discussiono the best o our knowledge this report constitutes the largest series to date describing the outcomeso patients presenting with reractory shock caused by endocrine emergencies (ie PC S and DK)rescued by ECMO support A total o 12 cases were identified in our registry rom 2005 to 2012 indicat-ing that the incidence o endocrine emergencies is low but not negligible Pheochromocytoma has been
estimated to be present in approximately 03 o all patients undergoing evaluation or secondary causeso hypertension18 Moreover S and DK accounts or 2 and 86 o all hospital admissions in patientswith thyrotoxicosis and type 1 diabetes mellitus respectively 1920 In general endocrine emergencies canhave a rapid and aggressive clinical course and pose significant diagnostic challenges (because they canmimic either AMI or acute congestive heart ailure) Endocrine emergencies are not common and prob-ably misdiagnosed in many cases and the clinical value o ECMO support in their clinical managementremains unclear Notably ollowing our report o a patient with PC who was successully rescued byECMO in January 20089 seven additional cases were described (a finding that illustrates the magnitudeo the potential underestimation as well as a recent increase in awareness)10ndash16
In the current series all patients with PC did not have a known history o pheochromocytoma Temain diagnostic eatures o PC consisted o extreme blood pressure fluctuations in presence o patentcoronary arteries on angiography Compared with AMI patients inotropic agents were more rapidlytapered and myocardial unction recovered significantly more quickly in PC However two o the ourpatients with PC (50) developed limb ischemia a percentage which was significantly higher than those
observed in both the DK (one patient 33) and AMI (six patients 75) groups (able 3) o our knowl-edge a total o 12 cases o pheochromocytoma-associated peripheral limb ischemia have been reportedto date21 In this scenario early recognition and treatment o pheochromocytoma through adrenalectomyor alpha-adrenergic blocking agents is paramount to reduce the risk o devastating limb ischemia
In this series most patients with S were initially misdiagnosed as having AMI or severe conges-tive heart ailure Hyperbilirubinemia was a common finding in S patients most likely caused by adirect hepatotoxic effect o excess thyroid hormones andor hepatic congestion resulting rom thyroidstorm Although anti-thyroid drugs (eg propylthiouracil) can cause cholestatic liver injury previousstudies conducted in S patients have shown that jaundice can successully respond to anti-thyroidmedications2223 Consequently the timely detection o S is crucial to the successul preservation oliver unction
Blood glucose levels are routinely checked in all o the patients admitted to our emergency depart-ment with disturbances o consciousness Te diagnosis o DK can be easily established upon admissionin presence o hyperglycemia metabolic acidosis and increased serum or urine ketones In generaldelays to seek medical care and the presence o sepsis andor coma have adverse consequences or DKpatientsrsquo clinical outcomes
In the current study AMI patients had lower SOFA scores and higher levels o cardiac enzymes thanthose with endocrine emergencies Notably the lef ventricular ejection unction and the clinical out-comes were poorer in patients with AMI than in those with endocrine emergencies rescued by ECMO(able 3) Similarly the number o patients who required long-term inotropic agents was higher in theAMI group
aken together there are three main findings rom the current single-center study 1) endocrineemergencies are rare but not negligible events 2) patients with endocrine emergencies presenting withacute reractory shock can be successully rescued by ECMO support and 3) screening o endocrineemergencies is essential in patients with acute reractory shock requiring mechanical support Albeitpreliminary in nature because o the small sample size our results may stimulate urther studies on thecost-benefits analysis o routine screening o thyroid hormones catecholamines and metanephrines inpatients presenting with acute circulatory collapse in need o ECMO support
PC (n= 4) DK (n= 3) TS (n= 5) AMI (n= 80)
Brain death 0 0 0 3
ARDS 0 0 0 2
Survival to discharge () 4 (100) 1 (333) 3 (60) 40 (50)
Survivors with CPC I n () 4 (100 ) 1 (100) 2 (667) 32 (80)
Table 3 Comparisons of patients with endocrine crisis and acute myocardial infarction rescued
with ECMO support Abbreviations AMI acute myocardial inarction ARDS acute respiratory distresssyndrome CABG coronary artery bypass surgery CK creatine kinase CPC cerebral perormance categoryCPR cardiac pulmonary resuscitation DK diabetic ketoacidosis GI gastrointestinal IABP intra-aortic
balloon pumping ICU intensive care unit IE inotropic equivalents LVEF lef ventricular ejection ractionMAP mean arterial pressure MOF multiple organ ailure PC pheochromocytoma crisis SOFA sepsis-related organ ailure assessment n-I troponin-I S thyroid storm VAD ventricular assist device VSD
ventricular septal deect
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 78
wwwnaturecomscientificreports
7SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
ConclusionsSuccessul management o endocrine emergencies depends on prompt recognition correction o theunderlying hormone alterations and immediate treatment o shock Unortunately numerous patientspresenting with endocrine emergencies have an unknown previous history o hormone imbalanceTereore the screening o endocrine emergencies is important in these patients Herein we have shownthat ECMO support is clinically useul in patients diagnosed with endocrine emergencies presenting withacute circulatory ailure Because medical care is extremely challenging in this scenario the awareness othe clinical value o ECMO among physicians managing patients with endocrine emergencies may helpimprove clinical outcomes
References1 Pee983147 G J et al Efficacy and economic assessment o conventional ventilatory support versus extracorporeal membrane
oxygenation or severe adult respiratory ailure (CESA983122) a multicentre randomised controlled trial Lancet 374 1351ndash1363(2009)
2 Baud F J Megarbane B Deye N amp Leprince P Clinical review Aggressive management and extracorporeal support or drug-induced cardiotoxicity Crit Care Doi 101186cc5700 (2007)
3 Chen Y S et al 983122escue or acute myocarditis with shoc983147 by extracorporeal membrane oxygenation Ann Torac Surg 68 2220ndash2224 (1999)
4 Chou N 983115 et al Application o extracorporeal membrane oxygenation in adult burn patients Artif Organs 25 622ndash626 (2001)5 Chen Y S et al Cardiopulmonary resuscitation with assisted extracorporeal lie-support versus conventional cardiopulmonary
resuscitation in adults with in-hospital cardiac arrest an observational study and propensity analysis Lancet 372 554ndash561(2008)
6 983115o W J et al Extracorporeal membrane support or adult postcardiotomy cardiogenic shoc983147 Ann Torac Surg 73 538ndash545(2003)
7 Ariza-Soleacute A et al Ventricular support With Extracorporeal Membrane Oxygenation A New 983122escue Alternative or 983122eractoryCardiogenic Shoc983147 983122ev Esp Cardiol 66 501ndash503 (2013)
8 Chen Y S et al Analysis and results o prolonged resuscitation in cardiac arrest patients rescued by extracorporeal membraneoxygenation J Am Coll Cardiol 41 197ndash203 (2003)
9 Chao A Yeh Y C Yen S amp Chen Y S Phaeochromocytoma crisis ndash a rare indication or extracorporeal membraneoxygenation Anaesthesia 63 86ndash88 (2008)
10 Suh I W et al Catastrophic catecholamine-induced cardiomyopathy mimic983147ing acute myocardial inarction rescued byextracorporeal membrane oxygenation (ECMO) in pheochromocytoma J 983115orean Med Sci 23 350ndash354 (2008)
11 Ezri Golan A Sasson L amp 983122ozenman Y Pheochromocytoma induced ulminant cardiogenic shoc983147 ollowing laparoscopicsalpingectomy successully managed with extracorporeal membrane oxygenation Jurnalul 983122omacircn de Anestezie erapie Intensivatilde 16 154ndash158 (2008)
12 983122itter S Guertler Meier C A amp Genoni M Cardiogenic shoc983147 due to pheochromocytoma rescued by extracorporealmembrane oxygenation Interact Cardiovasc Torac Surg 13 112ndash113 (2011)
13 Noorani A Vuylste983147e A Lewis C Parameshwar J amp Catarino P A moribund athlete Lance 380 74 (2012)14 Ghassam S et al Successul extracorporeal membrane oxygenation treatment or pheochromocytoma-induced acute cardiac
ailure AJEM 30 1017e1ndash1017e3 (2012)15 Banfi C et al Central extracorporeal lie support in pheochromocytoma crisis Ann Torac Surg 93 1303ndash1305 (2012)16 Sheinberg 983122 et al Case 1ndash2012 A perect storm atality resulting rom metoclopramide unmas983147ing a pheochromocytoma and
its management J Cardiothorac Vasc Anesth 26 161ndash115 (2012)17 Vincent J L et al Te SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysunctionailure On behal
o the Wor983147ing Group on Sepsis-983122elated Problems o the European Society o Intensive Care Medicine Intensive Care Med 22 707ndash710 (1996)
18 Streeten D H Anderson G H Jr amp Wagner S Effect o age on response o secondary hypertension to specific treatment Am J Hypertens 3 360ndash365 (1990)
19 983115earney amp Dang C Diabetic and endocrine emergencies Postgrad Med J 83 79ndash86 (2007)20 983122ingel M D Management o hypothyroidism and hyperthyroidism in the intensive care unit Crit Care Clin 17 59ndash74 (2001)21 Lutchman D Buchholz S amp 983115eightley C Pheochromocytomandashassociated critical peripheral ischemia Intern Med J 40 150ndash159
(2010)22 Hull 983115 et al wo cases o thyroid storm-associated cholestatic jaundice Endocr Pract 13 478ndash480 (2007)23 Hambleton C et al Tyroid storm complicated by ulminant hepatic ailure Case report and literature review Ann Otol 983122hinol
Laryngol 22 679ndash682 (2013)
AcknowledgementsTis study was partially supported by the National Science Council (102-2325-B-002-009 101-2325-B-002-009 100-2314-B-002-018-MY2 and 100-2325-B-002-009) Ministry o Science and echnologyaiwan and partially unded by the National aiwan University Hospital MG 213 und
Author ContributionsAC HYY and YSC study design AC CHW and HJY draf o the manuscript tables and figuresNKC LJ NHC and MHL data collection and analysis AC and NHC manuscript editingNKC HYY MHL CHW and HJY literature review and data checking SCH IHW and YSCcritical revision o the manuscript or important intellectual content All authors final approval o themanuscript
Additional InformationCompeting financial interests Te authors declare no competing financial interests
How to cite this article Chao A et al Highlighting indication o extracorporeal membraneoxygenation in endocrine emergencies Sci Rep 5 13361 doi 101038srep13361 (2015)
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 88
wwwnaturecomscientificreports
8SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
Tis work is licensed under a Creative Commons Attribution 40 International License Teimages or other third party material in this article are included in the articlersquos Creative Com-
mons license unless indicated otherwise in the credit line i the material is not included under theCreative Commons license users will need to obtain permission rom the license holder to reproducethe material o view a copy o this license visit httpcreativecommonsorglicensesby40
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 78
wwwnaturecomscientificreports
7SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
ConclusionsSuccessul management o endocrine emergencies depends on prompt recognition correction o theunderlying hormone alterations and immediate treatment o shock Unortunately numerous patientspresenting with endocrine emergencies have an unknown previous history o hormone imbalanceTereore the screening o endocrine emergencies is important in these patients Herein we have shownthat ECMO support is clinically useul in patients diagnosed with endocrine emergencies presenting withacute circulatory ailure Because medical care is extremely challenging in this scenario the awareness othe clinical value o ECMO among physicians managing patients with endocrine emergencies may helpimprove clinical outcomes
References1 Pee983147 G J et al Efficacy and economic assessment o conventional ventilatory support versus extracorporeal membrane
oxygenation or severe adult respiratory ailure (CESA983122) a multicentre randomised controlled trial Lancet 374 1351ndash1363(2009)
2 Baud F J Megarbane B Deye N amp Leprince P Clinical review Aggressive management and extracorporeal support or drug-induced cardiotoxicity Crit Care Doi 101186cc5700 (2007)
3 Chen Y S et al 983122escue or acute myocarditis with shoc983147 by extracorporeal membrane oxygenation Ann Torac Surg 68 2220ndash2224 (1999)
4 Chou N 983115 et al Application o extracorporeal membrane oxygenation in adult burn patients Artif Organs 25 622ndash626 (2001)5 Chen Y S et al Cardiopulmonary resuscitation with assisted extracorporeal lie-support versus conventional cardiopulmonary
resuscitation in adults with in-hospital cardiac arrest an observational study and propensity analysis Lancet 372 554ndash561(2008)
6 983115o W J et al Extracorporeal membrane support or adult postcardiotomy cardiogenic shoc983147 Ann Torac Surg 73 538ndash545(2003)
7 Ariza-Soleacute A et al Ventricular support With Extracorporeal Membrane Oxygenation A New 983122escue Alternative or 983122eractoryCardiogenic Shoc983147 983122ev Esp Cardiol 66 501ndash503 (2013)
8 Chen Y S et al Analysis and results o prolonged resuscitation in cardiac arrest patients rescued by extracorporeal membraneoxygenation J Am Coll Cardiol 41 197ndash203 (2003)
9 Chao A Yeh Y C Yen S amp Chen Y S Phaeochromocytoma crisis ndash a rare indication or extracorporeal membraneoxygenation Anaesthesia 63 86ndash88 (2008)
10 Suh I W et al Catastrophic catecholamine-induced cardiomyopathy mimic983147ing acute myocardial inarction rescued byextracorporeal membrane oxygenation (ECMO) in pheochromocytoma J 983115orean Med Sci 23 350ndash354 (2008)
11 Ezri Golan A Sasson L amp 983122ozenman Y Pheochromocytoma induced ulminant cardiogenic shoc983147 ollowing laparoscopicsalpingectomy successully managed with extracorporeal membrane oxygenation Jurnalul 983122omacircn de Anestezie erapie Intensivatilde 16 154ndash158 (2008)
12 983122itter S Guertler Meier C A amp Genoni M Cardiogenic shoc983147 due to pheochromocytoma rescued by extracorporealmembrane oxygenation Interact Cardiovasc Torac Surg 13 112ndash113 (2011)
13 Noorani A Vuylste983147e A Lewis C Parameshwar J amp Catarino P A moribund athlete Lance 380 74 (2012)14 Ghassam S et al Successul extracorporeal membrane oxygenation treatment or pheochromocytoma-induced acute cardiac
ailure AJEM 30 1017e1ndash1017e3 (2012)15 Banfi C et al Central extracorporeal lie support in pheochromocytoma crisis Ann Torac Surg 93 1303ndash1305 (2012)16 Sheinberg 983122 et al Case 1ndash2012 A perect storm atality resulting rom metoclopramide unmas983147ing a pheochromocytoma and
its management J Cardiothorac Vasc Anesth 26 161ndash115 (2012)17 Vincent J L et al Te SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysunctionailure On behal
o the Wor983147ing Group on Sepsis-983122elated Problems o the European Society o Intensive Care Medicine Intensive Care Med 22 707ndash710 (1996)
18 Streeten D H Anderson G H Jr amp Wagner S Effect o age on response o secondary hypertension to specific treatment Am J Hypertens 3 360ndash365 (1990)
19 983115earney amp Dang C Diabetic and endocrine emergencies Postgrad Med J 83 79ndash86 (2007)20 983122ingel M D Management o hypothyroidism and hyperthyroidism in the intensive care unit Crit Care Clin 17 59ndash74 (2001)21 Lutchman D Buchholz S amp 983115eightley C Pheochromocytomandashassociated critical peripheral ischemia Intern Med J 40 150ndash159
(2010)22 Hull 983115 et al wo cases o thyroid storm-associated cholestatic jaundice Endocr Pract 13 478ndash480 (2007)23 Hambleton C et al Tyroid storm complicated by ulminant hepatic ailure Case report and literature review Ann Otol 983122hinol
Laryngol 22 679ndash682 (2013)
AcknowledgementsTis study was partially supported by the National Science Council (102-2325-B-002-009 101-2325-B-002-009 100-2314-B-002-018-MY2 and 100-2325-B-002-009) Ministry o Science and echnologyaiwan and partially unded by the National aiwan University Hospital MG 213 und
Author ContributionsAC HYY and YSC study design AC CHW and HJY draf o the manuscript tables and figuresNKC LJ NHC and MHL data collection and analysis AC and NHC manuscript editingNKC HYY MHL CHW and HJY literature review and data checking SCH IHW and YSCcritical revision o the manuscript or important intellectual content All authors final approval o themanuscript
Additional InformationCompeting financial interests Te authors declare no competing financial interests
How to cite this article Chao A et al Highlighting indication o extracorporeal membraneoxygenation in endocrine emergencies Sci Rep 5 13361 doi 101038srep13361 (2015)
8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 88
wwwnaturecomscientificreports
8SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
Tis work is licensed under a Creative Commons Attribution 40 International License Teimages or other third party material in this article are included in the articlersquos Creative Com-
mons license unless indicated otherwise in the credit line i the material is not included under theCreative Commons license users will need to obtain permission rom the license holder to reproducethe material o view a copy o this license visit httpcreativecommonsorglicensesby40

8182019 Ecmo in Endocrine Emergency
httpslidepdfcomreaderfullecmo-in-endocrine-emergency 88
wwwnaturecomscientificreports
8SCIENTIFIC REPORTS | 513361 | DOI 101038srep13361
Tis work is licensed under a Creative Commons Attribution 40 International License Teimages or other third party material in this article are included in the articlersquos Creative Com-
mons license unless indicated otherwise in the credit line i the material is not included under theCreative Commons license users will need to obtain permission rom the license holder to reproducethe material o view a copy o this license visit httpcreativecommonsorglicensesby40