ecgs and acute cardiac events workshop dr. stewart mcmorran consultant in accident and emergency mb,...
Post on 21-Dec-2015
218 views
TRANSCRIPT

ECGs and Acute Cardiac Events Workshop
Dr. Stewart McMorran
Consultant in Accident and Emergency
MB, BCh, MRCS, FFAEM

Objectives
• Emergency management of common cardiac events
• ST elevation MIs
• Tachyarrhythmias
• Bradyarrhythmias
• Overview of management
• Interactive case discussions
National Service Framework
• NSF for coronary artery disease established 2000• Relevant to emergency medicine – need for timely
reperfusion therapy• Door to needle time of 30 mins• Call to needle time of 60 mins• Results …
– 75% eligible patients thrombolysed within 30 minutes of hospital arrival

Impact of NSF
• Emphasis on timely delivery of reperfusion therapy
• Thrombolysis – most places• Percutaneous Coronary Intervention:
– Primary – limited availability
– Rescue – local policy; if less than 50% resolution in ST segment elevation after 90 minutes
• Coronary artery bypass graft

Impact on first line services
• Timely assessment of chest pain in A&E
• Extended skills of paramedics
• Availability of Air Ambulances


ECG Lead Placement

Wall affected Leads Artery involved
Reciprocal changes
Anterior V2-4 LAD II, III, aVF
Anterolateral I, aVL, V3-6 LAD, circumflex
II, III, aVF
Anteroseptal V1-4 LAD
Inferior II, III, aVF RCA I, aVL
Lateral I, aVL, V5-6 circumflex II, III, aVF
Posterior V7-9 RCA V1-3
Right ventricular
RV4-6 RCA

Criteria for thrombolysis
• Chest pain, onset within last 12 hours plus any of:• ST elevation 2 mm or more in two contiguous
chest leads• ST elevation 1 mm or more in two contiguous
limb leads• Dominant R wave and ST depression in V1-3• New LBBB





Posterior MI
• Dominant R wave chest leads V1-3
• ST depression chest leads V1-3
• Turn ECG upside down and back to front – see typical changes of STEMI
• Alternatively …– Posterior leads V7-9



Left Bundle Branch Block and MI
• ST segment elevation more than 1 mm concordant (same direction) as QRS complex
• ST segment depression more than 1 mm in V1,2,3• ST segment elevation more than 5 mm discordant
(opposite direction) from QRS complex• Sgarbossa E et al. NEJM 1996 Feb 22:334(8)
481-7


Pericarditis
• Widespread ST elevation (in leads looking at inflamed epicardium)
• Reciprocal depression in aVR and V1
• ST segment saddle shaped (concave upwards)
• No Q waves

ST segment high take off
• Normal variant• High take off or early repolarisation or J point
elevation• Younger patients• Usually follows an S wave• T wave maintains independent wave form• No reciprocal ST segment depression• If in doubt, compare with earlier ECGs

Arrhythmias - principles of treatment
• Choice of intervention
- drugs vs. electricity
• How symptomatic is patient
– How urgent is need for action

Choice of intervention
• Drugs:– Not always reliable
– Side effects
– Every anti-arrhythmic is potentially pro-arrhythmic
• Electricity:– Reliable
– Patient considerations
– Environmental considerations

How symptomatic is patient
• Signs of poor cardiac output– Heart rate
• Too fast – depends on rhythm
• Too slow – depends on patient
– Systolic blood pressure < 90 mm Hg– Chest pain– Breathlessness– Altered level of consciousness


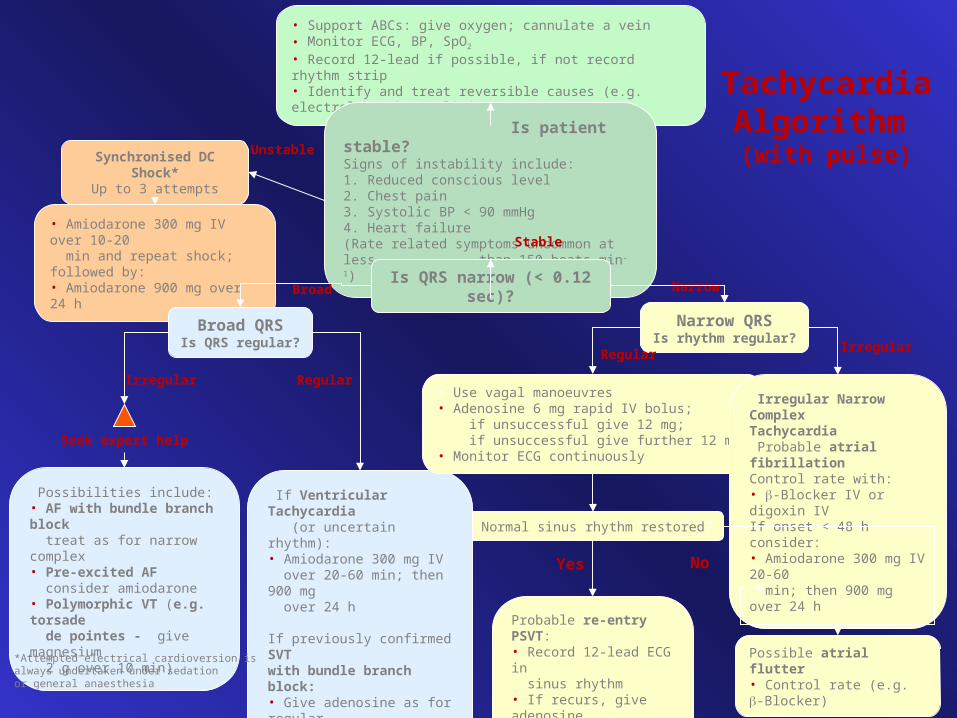
TachycardiaAlgorithm (with pulse)
• Support ABCs: give oxygen; cannulate a vein• Monitor ECG, BP, SpO2
• Record 12-lead if possible, if not record rhythm strip• Identify and treat reversible causes (e.g. electrolyte abnormalities)
Seek expert help
Synchronised DC Shock*Up to 3 attempts
Seek expert help
Normal sinus rhythm restored?
Probable re-entry PSVT:• Record 12-lead ECG in sinus rhythm• If recurs, give adenosine again & consider choice of anti-arrhythmic prophylaxis
If Ventricular Tachycardia (or uncertain rhythm):• Amiodarone 300 mg IV over 20-60 min; then 900 mg over 24 h
If previously confirmed SVT with bundle branch block:• Give adenosine as for regular narrow complex tachycardia
• Amiodarone 300 mg IV over 10-20 min and repeat shock; followed by:• Amiodarone 900 mg over 24 h
Is patient stable?Signs of instability include:1. Reduced conscious level 2. Chest pain3. Systolic BP < 90 mmHg 4. Heart failure(Rate related symptoms uncommon at less than 150 beats min-1)
Is QRS narrow (< 0.12 sec)?Broad Narrow
Narrow QRSIs rhythm regular?
RegularIrregular
Broad QRSIs QRS regular?
• Use vagal manoeuvres• Adenosine 6 mg rapid IV bolus; if unsuccessful give 12 mg; if unsuccessful give further 12 mg.• Monitor ECG continuously
Irregular Narrow Complex Tachycardia Probable atrial fibrillationControl rate with:• -Blocker IV or digoxin IVIf onset < 48 h consider:• Amiodarone 300 mg IV 20-60 min; then 900 mg over 24 h
Irregular Regular
Possibilities include:• AF with bundle branch block treat as for narrow complex• Pre-excited AF consider amiodarone• Polymorphic VT (e.g. torsade de pointes - give magnesium 2 g over 10 min)
Yes No
Possible atrial flutter• Control rate (e.g. -Blocker)
*Attempted electrical cardioversion is always undertaken under sedation or general anaesthesia
Stable
Unstable

Example
• 65 year old male
• Presents to A&E
• Palpitations /chest pain
• MI 3 months ago
• Sa02 95% on high flow oxygen
• PR 190 BP 90/70


How do you know it is VT ?
• May be difficult to distinguish ventricular tachycardia from atrial tachycardia with aberrant conduction e.g. LBBB
• Default position – assume ventricular• Look for confirmatory features:
– capture beats– fusion beats– concordance– extreme axis deviation

Main learning points
• VT is a malignant arrhythmia
• DC cardioversion in presence of adverse signs
• Check electrolytes especially K+ and Mg2+
• Amiodarone anti-arrhythmic of choice

Example
• 25 year old female
• Presents to A&E
• Palpitations
• Sa02 97% on high flow oxygen
• PR 200 BP 110/70

TachycardiaAlgorithm (with pulse)
• Support ABCs: give oxygen; cannulate a vein• Monitor ECG, BP, SpO2
• Record 12-lead if possible, if not record rhythm strip• Identify and treat reversible causes (e.g. electrolyte abnormalities)
Seek expert help
Synchronised DC Shock*Up to 3 attempts
Seek expert help
Normal sinus rhythm restored?
Probable re-entry PSVT:• Record 12-lead ECG in sinus rhythm• If recurs, give adenosine again & consider choice of anti-arrhythmic prophylaxis
If Ventricular Tachycardia (or uncertain rhythm):• Amiodarone 300 mg IV over 20-60 min; then 900 mg over 24 h
If previously confirmed SVT with bundle branch block:• Give adenosine as for regular narrow complex tachycardia
• Amiodarone 300 mg IV over 10-20 min and repeat shock; followed by:• Amiodarone 900 mg over 24 h
Is patient stable?Signs of instability include:1. Reduced conscious level 2. Chest pain3. Systolic BP < 90 mmHg 4. Heart failure(Rate related symptoms uncommon at less than 150 beats min-1)
Is QRS narrow (< 0.12 sec)?Broad Narrow
Narrow QRSIs rhythm regular?
RegularIrregular
Broad QRSIs QRS regular?
• Use vagal manoeuvres• Adenosine 6 mg rapid IV bolus; if unsuccessful give 12 mg; if unsuccessful give further 12 mg.• Monitor ECG continuously
Irregular Narrow Complex Tachycardia Probable atrial fibrillationControl rate with:• -Blocker IV or digoxin IVIf onset < 48 h consider:• Amiodarone 300 mg IV 20-60 min; then 900 mg over 24 h
Irregular Regular
Possibilities include:• AF with bundle branch block treat as for narrow complex• Pre-excited AF consider amiodarone• Polymorphic VT (e.g. torsade de pointes - give magnesium 2 g over 10 min)
Yes No
Possible atrial flutter• Control rate (e.g. -Blocker)
*Attempted electrical cardioversion is always undertaken under sedation or general anaesthesia
Stable
Unstable

Main learning points
• Supraventricular tachycardias are often well tolerated
• Usually younger patients
• Vagal manoeuvres may be successful
• Adenosine is an effective anti-arrhythmic

Wolf Parkinson White

Wolf Parkinson White syndrome
• Uncommon cause of SVT• Presence of accessory pathway (bundle of
Kent)• Characteristic ECG features
– Short PR interval (<120 ms)– Wide QRS (>120 ms)– Delta wave (slurred upstroke)
• Unpredictable response to adenosine

Example
• 55 year old man
• Presents to A&E
• 1 hour history of central chest pain
• Sa02 97% on high flow oxygen
• PR 45 BP 80/50


BRADYCARDIA ALGORITHM(includes rates inappropriately slow for haemodynamic state)
Adverse signs?
• Systolic BP < 90 mmHg• Heart rate < 40 beats min-1
• Ventricular arrhythmias compromising BP• Heart failure
Atropine500 mcg IV
SatisfactoryResponse?
Risk of asystole?
• Recent asystole• Möbitz II AV block• Complete heart block with broad QRS• Ventricular pause > 3s
Interim measures:
• Atropine 500 mcg IV repeat to maximum of 3 mg• Adrenaline 2-10 mcg min-1
• Alternative drugs OR• Transcutaneous pacing
Seek expert helpArrange transvenous pacing
Yes No
Yes
Observe
YesNo

Main learning points
• Bradyarrhythmias may complicate inferior myocardial infarction (RCA supplies AVN)
• Atropine may be effective
• Pacing for symptomatic bradycardias resistant to atropine

Example
• 75 year old female
• Presents to A&E
• Palpitations
• Sa02 95% on high flow oxygen
• PR 175 irreg BP 80/50


Atrial fibrillation Treatment based on risk to patient from the arrhythmia
• High risk– Rate > 150 beats min-1
– Chest pain
– Critical perfusion
• Intermediate risk– Rate 100-150 beats min-1
– Breathlessness
– Poor perfusion
• Low risk– Rate < 100 beats min-1
– Mild or no symptoms– Good perfusion

Main learning points
• Management of AF is complex
• Universal agreement on high risk patients
• Anticoagulation essential to prevent thromboembolic complications

Example
• 35 year old male
• Presents to A&E
• Palpitations
• Sa02 97% on high flow oxygen
• PR 200 BP 110/70


Any Questions?

Summary
• Chest pain is a common cause of attendance to hospital
• Important to recognise STEMI
• Arrhythmias may precede or complicate MI
• Standardised treatment algorithms for initial management