ecg workshop - heart group gp/ecg... · ecg workshop nezar amir. myocardial ischemia . ... exam is...
TRANSCRIPT

ECG Workshop
Nezar Amir

Myocardial Ischemia

ECG InfarctECG in STEMI is dynamic & evolving

Common causes of ST shift

Infarct Localisation• Left main artery occlusion:
o diffuse ST-depression with ST elevation in AVRo very high risk
• Anterior wall:o ST elevation V1-V4. LAD. (often tachycardia)
• Inferior wall: o ST elevation II, III, AVF. o 80% RCA (elevation III>II; depression > I or in AVL), or RCX
( in 20%). (often bradycardic due to sinus node or AV node ischemia)
• Right ventricle infarct:o ST elevation in V4R.
• Posterior wall: o high R and ST-depression in V1-V3
• Lateral wall: o ST elevation in lead I, AVL, V6.o LAD (D-branch)

Differential diagnosis of ST
elevation
1:LVH
2:LBBB
3: Pericarditis
4: High Potassium
5: Acute AS infarct
6:: Acute AS infarct + RBBB
7: Brugada syndrome
Case Studies

Sixty year old male with epigastric pain associated with nausea
and vomiting. Chronic smoker. HbA1c of 65. BP is 90/70
1. Patient has acute pericarditis
2. Patient sustained acute MI and
needs to be transferred to hospital
3. RV infarct is likely complication of
this infarct
5. Emergency angioplasty is
highly likely required in the
coming 60 minutes
6. Heart block is likely
complication
Q. All of the following are true, except?

Same patient had right-sided leads showing RV infarct

Q-WAVES
• Q waves are electrically silent areas
• Sign of old MI
• Pathological Q
– Locations
• Any in V2-V3
• >=0.03s and >0.1mV deep in other leads
– Two contiguous leads

72 year old man presented for a well check
1. Referral to hospital, this patient
had MI
2. Risk factor assessment and
referral to cardiac services ETT
and echocardiography
3. No action, this ECG is normal
Q. The following are appropriate actions

Q-Waves

55 year old male smoker, presented with central chest pain of 60
minutes. Patient was apprehensive and diaphoretic, BP; 100/60,
exam is otherwise normal.
1. Patient sustained inferior STEMI
2. Patients sustained posterior
STEMI
3. Patient sustained anterolateral
STEMI
4. Immediate transfer on P1
ambulance is mandatory
5. Pain relief, morhpine, GTN
and 600mg of chewable
aspirin should be given
Q. The following statement(s) in regards to ECG are true, except;

12 months later, the patient had an echocardiogram, and he comes
back asking you to look up the result before him being seen by his
cardiologist. He requested an ECG for reassurance
1. New LBBB
2. Persistent ST elevation with
biphasic T wave in the anterior
leads
4. You predict that he would have a large
septal scar on his echocardiogram
5. Patient had another STEMI, consider
immediate transfer to hospital
Q. The findings on the ECG are;

48 year old healthy male presented with severe left-sided chest pain.
The patient needed 15mg of Morhpine. 1st Troponin was negative.
1. Obtain CT scan to exclude aortic
dissection
2. Obtain echocardiogram to look for
regional wall motion abnormalities
3. Obtain urgent second Troponin
4. Review all primary data, including history,
family history , CXR, and blood test
5. Request psychiatrist support, this patient is
a drug seeker
Q. The following are appropriate actions;

• CT showed no dissection- done 10 minutes after arrival
• 2nd Troponin showed no change from 1st- time between the 2 tests
in 45 minutes
• Patient is a father of three, farmer. Bloods and CXR are normal
• Urgent echocardiogram was obtained



ST elevation in the absence of an aMI
• Pericarditis/myocarditis.• Left ventricular hypertrophy (LVH)• Physiological/benign ST elevation• Cardiac aneurysm• Hyperkalemia• LBBB• HCM

50 year old healthy banker presenting for routine medical check.
Asymptomatic. Non-smoker, no family history of cardiac disease
1. RBBB
2. LBBB
3. Old anterior MI with aneurysm
4. LVH
5. Pericarditis
Q. The best description for the ECG is;

66 year old male with near syncope. Cardiac exam showed systolic
murmur radiating to the carotids. BP is 110/70. No family history of SCD.
1. LVH
2. LBB
3. NSTEMI
4. Old MI with Q waves
5. Pericarditis
Q. The best description for the ECG is;
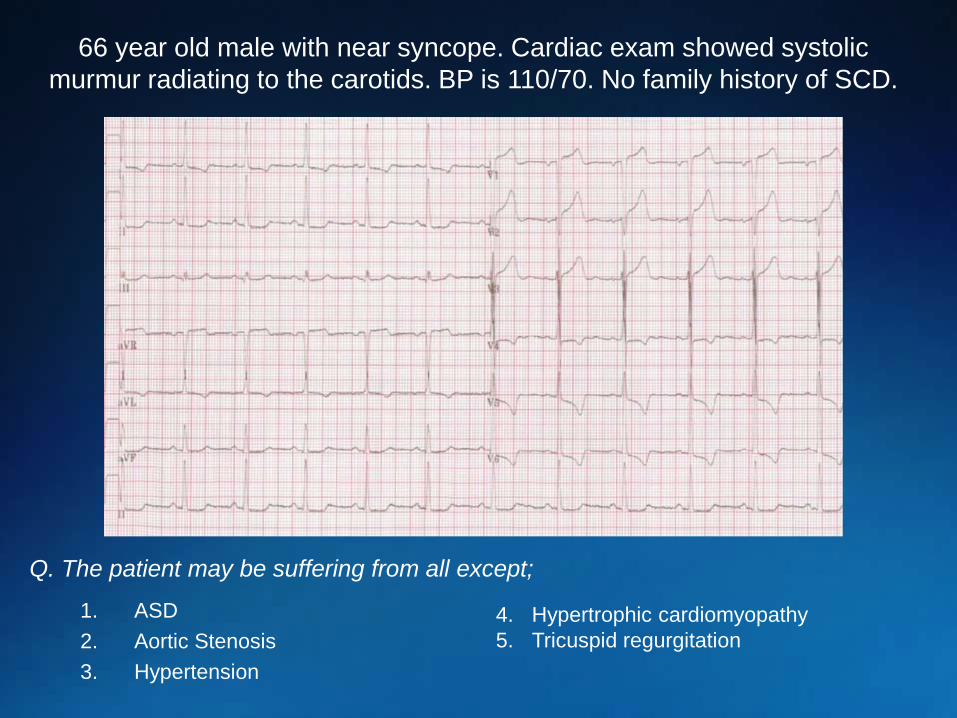
66 year old male with near syncope. Cardiac exam showed systolic
murmur radiating to the carotids. BP is 110/70. No family history of SCD.
1. ASD
2. Aortic Stenosis
3. Hypertension
4. Hypertrophic cardiomyopathy
5. Tricuspid regurgitation
Q. The patient may be suffering from all except;

44 year old with chronic renal failure on hemodialysis. Mild SOB. ECG obtained
1. Elevated CK
2. STEMI
3. Fluid overload
4. Hyperkalemia
5. Hypernatremia
Q. The most likely explanation;
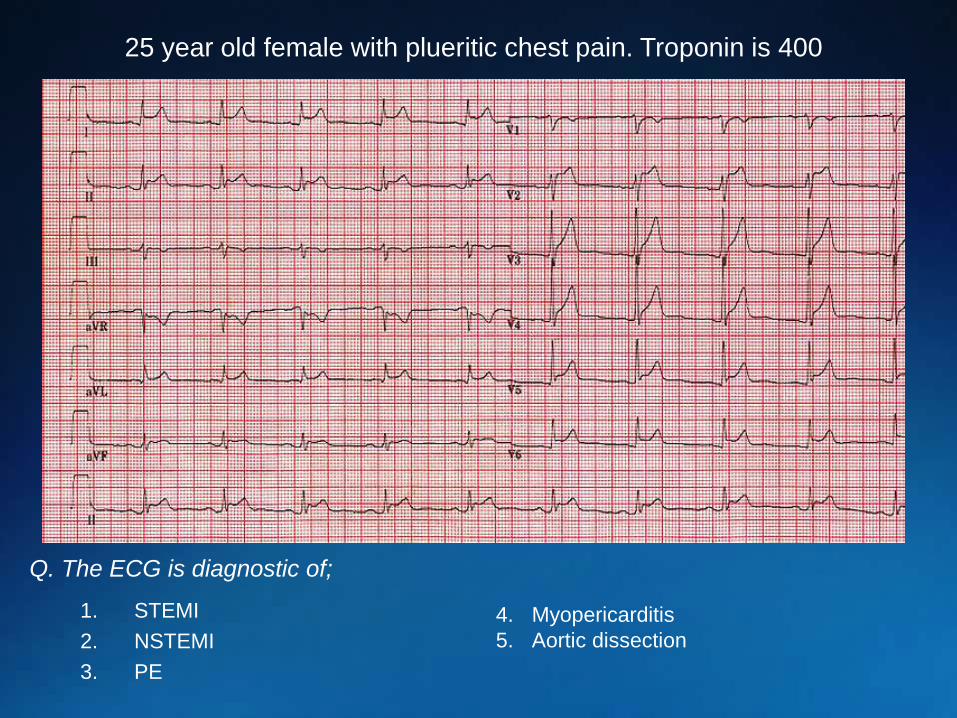
25 year old female with plueritic chest pain. Troponin is 400
1. STEMI
2. NSTEMI
3. PE
4. Myopericarditis
5. Aortic dissection
Q. The ECG is diagnostic of;

1. Normal variant early repolarization pattern
2. Physiologic sinus arrhythmia
3. Normal AV conduction
4. Left axis deviation
5. Transition zone in lead V3
Q. This ECG from an 18 year old male shows all of the following, except;

Non-ST Elevation
Infarction
Note the ST
depression
and T-wave
inversion in
leads V2-V6.
Here’s an ECG of an evolving non-ST elevation MI:
Question:What area of
the heart is
infarcting?
Anterolateral

Case 3; The ECG is from a 64 year old
Caucasian male referred by the primary
care physician to the cardiac outpatient
clinic because of a very abnormal ECG.
The patient is asymptomatic, without
any sort of chest pain, dyspnea,
palpitations, or previous syncope or
dizzy spells.
The BP is 130/80 mmHg and there are
not murmurs on auscultation.

1. Urgent hospital admission for coronary
arteriography
2. Urgent angiographic CT scan to exclude
pulmonary embolism
3. Consider this ECG as a normal variant and
reassure the patient accordingly
4. Nothing, this is a typical artifact originating from
a poor connection of the Wilson terminal to the
ground
5.None of the above
Q. What would you do?;

ECGs similar to this one can be seen in:
1. Athletes of African or Afro-American origin without the
phenotype of hypertrophic cardiomyopathy: our patient is
Caucasian and is not an athlete, but a 64 year old male in
whom his primary care physician obtained a routine ECG
2. Severe hypertensive heart disease: the blood pressure in this
patient was normal
3. Valvular aortic stenosis: there were no heart murmurs on
auscultation
4. Hypertrophic cardiomyopathy: the absence of murmurs should
prompt us to consider a non-obstructive hypertrophic
cardiomyopathy

cMR

Case 4; The ECG is from a 53 year old male with a history of high blood pressure for the last couple of years. He is overweight and has mild hyperglycemia.
He is referred by the primary care physician to the cardiac outpatient clinic because of a history of episodes of palpitations during the last 3 months, unrelated to exercise, of a very short duration, two or 3 times per month.
On auscultation there is a 2/6 systolic murmur along the left sternal border and a wide splitting of the second heart sound.

1.Chest X ray
2.2D ECHO
3.Holter recording
4.CT scan
5.Cardiac MRI
Q. What would you do first?;



THANK YOU