east midlands corporate governance network, february 2017, nottingham
TRANSCRIPT

East Midlands corporate governance networkFebruary 2017, Nottingham
The Integrated Support andAssurance Process (ISAP)Rachel Whitaker21 February 2017
Content
• What is the ISAP and what is its purpose?• To whom and when does the ISAP apply?• 4 key checkpoints• Timeframe of the ISAP process• KLOES• Example questions and submission content• Governance arrangements• Handy tips

What is the ISAP?
• ISAP is the new guidance published by NHS Englandand NHS Improvement.
• The guidance sets out a streamlined assuranceprocess to support the procurement of complexhealthcare contracts.
The Purpose of the ISAP
• The guidance has been developed in response tothe collapsed contract commissioned by theCambridgeshire and Peterborough CCG with UnitingCare Partnership in 2015.
• Identified 7 key lessons
• Applying the ISAP will help guide localcommissioners, manage risk and provide assurance.

To whom does the ISAP apply?
• The ISAP applies to commissioners procuring noveland complex contracts– CCGs– NHS England

When will the ISAP apply
All novel and complex procurements and specificallyif:• contract forms risk sharing arrangements.
• If the calculations of the contract value are takinga previously unused approach.
• If potential providers are creating new legalentities involving new organisations.

Models that will be caught by theISAP• Multispecialty community providers (MCP)• Primary and acute care systems (PACS)• Accountable Networks• Contracts with population based OR significant
levels of payment conditional on outcomes• Any contracts aiming to integrate a range of
services
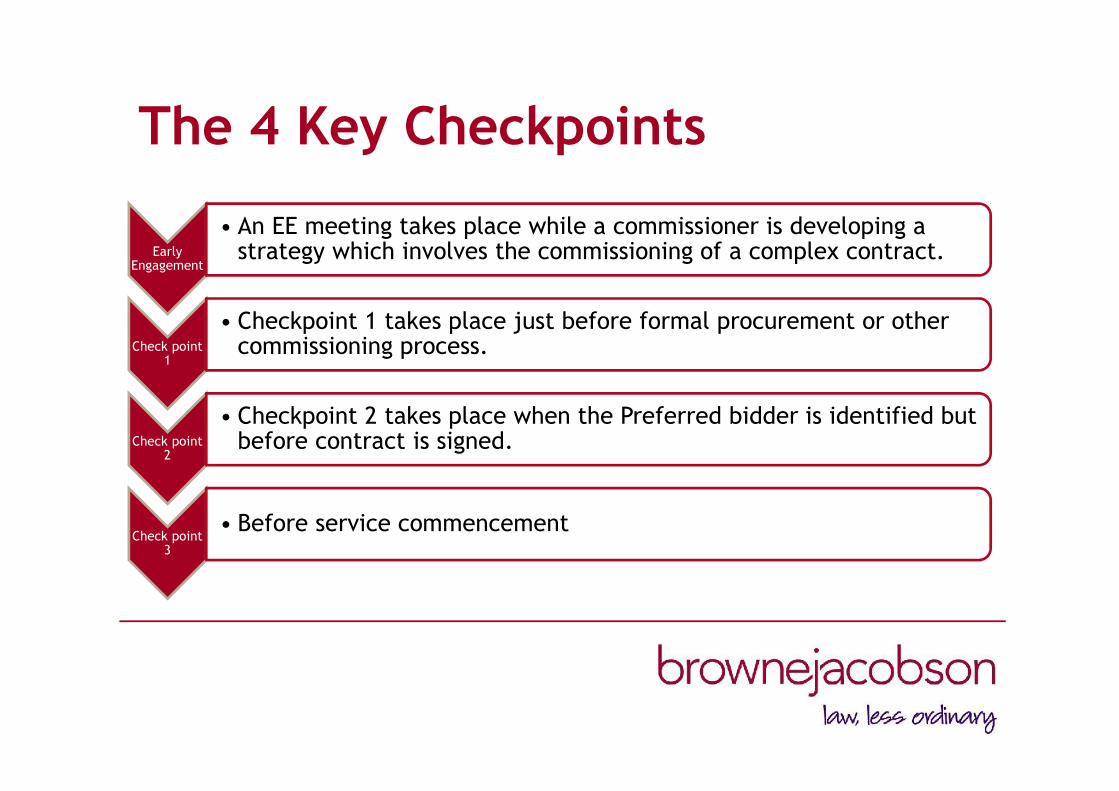
The 4 Key Checkpoints
EarlyEngagement
• An EE meeting takes place while a commissioner is developing astrategy which involves the commissioning of a complex contract.
Check point1
• Checkpoint 1 takes place just before formal procurement or othercommissioning process.
Check point2
• Checkpoint 2 takes place when the Preferred bidder is identified butbefore contract is signed.
Check point3
• Before service commencement

Time frame of the ISAP process
Earlyengagement1week
Check point 11 month
Check point 31 month
Check point 2
2-3 months
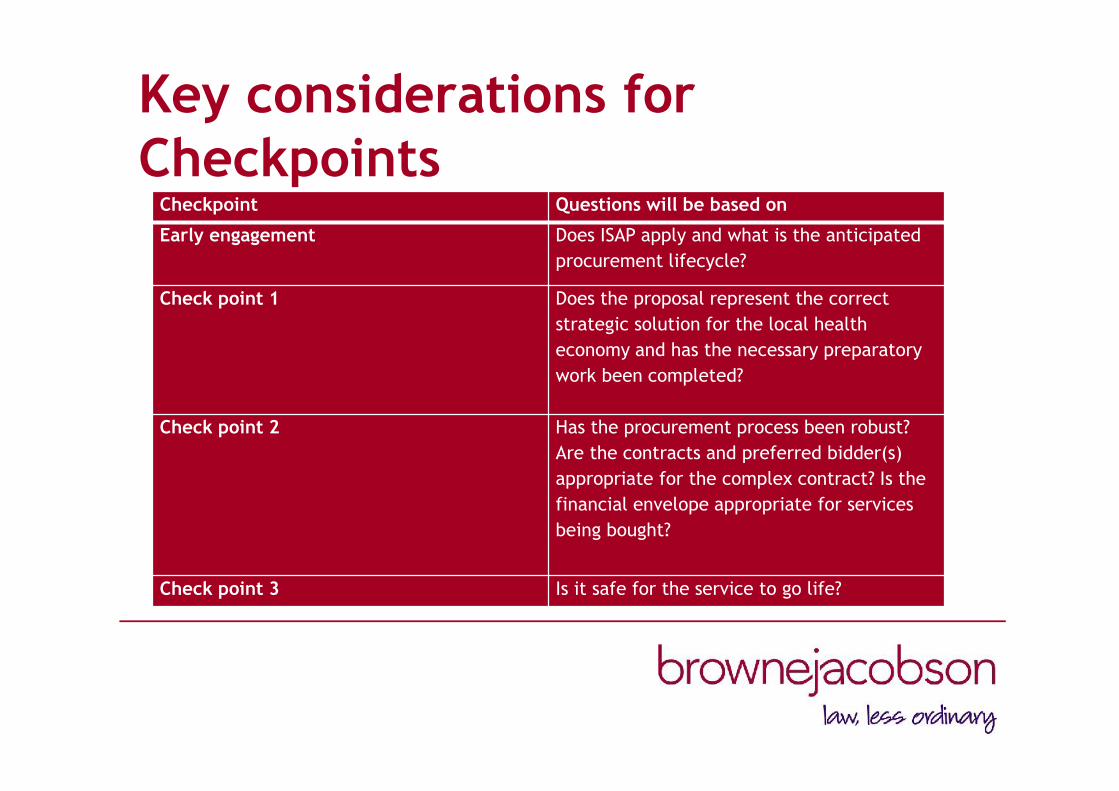
Key considerations forCheckpoints
Checkpoint Questions will be based on
Early engagement Does ISAP apply and what is the anticipatedprocurement lifecycle?
Check point 1 Does the proposal represent the correctstrategic solution for the local healtheconomy and has the necessary preparatorywork been completed?
Check point 2 Has the procurement process been robust?Are the contracts and preferred bidder(s)appropriate for the complex contract? Is thefinancial envelope appropriate for servicesbeing bought?
Check point 3 Is it safe for the service to go life?
Key Lines of Enquiry (KLOES)
• Feedback and outcomes will be provided at the endof each checkpoint.
• KLOES will be structured questions, which willestablish the risk profile of the complex contract ateach check point. It will form the basis of NHSEngland and NHS Improvement’s assessment.
• KLOES will affect commissioners and providers
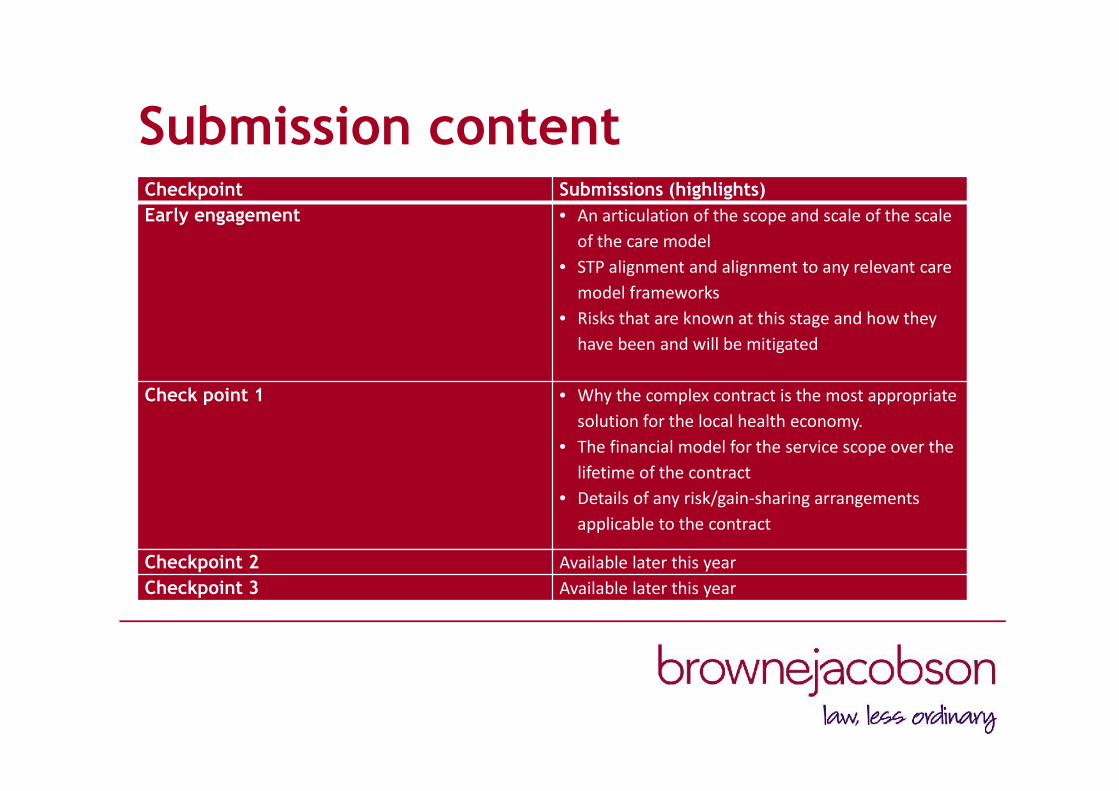
Submission contentCheckpoint Submissions (highlights)Early engagement • An articulation of the scope and scale of the scale
of the care model• STP alignment and alignment to any relevant care
model frameworks• Risks that are known at this stage and how they
have been and will be mitigated
Check point 1 • Why the complex contract is the most appropriatesolution for the local health economy.
• The financial model for the service scope over thelifetime of the contract
• Details of any risk/gain-sharing arrangementsapplicable to the contract
Checkpoint 2 Available later this yearCheckpoint 3 Available later this year
Governance arrangements
• At each check point, submissions fromcommissioner must first be assured by theirrespective governing body or board. Thisinformation needs to be presented in an accessibleway.
• Commissioners will seek from providers assurancethat all submissions have been agreed by theirboard.
Handy tips
• Speak to NHS England before the EarlyEngagement.
• Know who the regional contacts are and who thecentral contacts are (especially for contracts).
• Keep an open dialogue with NHS Englandthroughout the process.

Handy tips continued
• NHS regional teams are not yet familiar with theISAP process, the process is still evolving
• Get sign off on your project timelines at an earlystage.

Any questions?
Rachel Whitaker Associate, Commercial [email protected]: 0115 976 6538 M: 07920 257152

The General Data ProtectionRegulation
“The Highlights”

Introduction
• Change in 2018 – despite Brexit• A significant overhaul to DP legislation• Substantial and ambitious• A flavour of the changes• What action is required• Where to get further guidance
Changed concepts
• Transparency and Consent• Subject access, rectification and portability• Regulated Data• Pseudonymisation• Personal Data Breach• Data Governance• Enhanced Rights
Transparency and Consent
• The need to provide extensive informationabout the processing of personal data– Clear concise notices– General transparency obligation, and– Specified information to be provided
• Stricter conditions for obtaining consent– Intelligible– Informed– unambiguous

Subject access, rectificationand portability
• Information required on demand• Data portability• Time-bound• Legality of processing

Regulated Data
• Personal and sensitive data – includinggenetic and biometric data

Pseudonymisation
• The technique of processing personal datain such a way that it can no longer beattributed to a specific data subject withoutthe use of additional information, whichmust be kept separately and be subject totechnical and organisational measures toensure non-attribution.
Personal Data Breach
• A general personal data breach notificationregime
• Processors must report to controllers –controllers must report to their supervisoryauthority & (in some cases) data subjects
• Fines for non-compliance up to the higherof 2% of turnover or €10 million

Data Governance
• A wide range of measures to reduce therisk of breaching GDPR
• Accountability measures• Appointment of a Data Protection Officer

Enhanced Rights
• Rights to erasure and restriction ofprocessing

What should you be doing?
• Awareness• Information you hold• Privacy Notices• Individuals’ rights• Subject Access Requests• Legal basis for processing

What should you be doing (2)?
• Consent• Children• Data Breaches• DP by design• DP OfficersWho in your organisation is doing this, andhow far have they got…?

Further guidance
• Bird & Bird (www.twobirds.com)• ICO (www.ico.org.uk)• IGA (digital.nhs.uk/information-governance-
alliance)
…any questions?

Brexit for Health
Laura Hughes21 February 2017

Where are we now?
• Referendum – 23 June 2016• All change at the top• Miller/Santos – High Court and Supreme Court• White paper Feb 2017• European Union (Notification of Withdrawal) Bill
2016-17 – 2nd reading in HL 20 Feb• Notice under Article 50• The Grand Repeal Bill

Impact on health
• Article 168, section 7, Lisbon Treaty – health is amember state competence
• But…..• Reciprocal access to healthcare through European
Health Insurance Card• Pharmaceuticals• Working hours of Dr’s, recognition of qualifications• Cross-border public health….

• NHSE has set up/is setting up a “Brexit unit”• Health Select Committee heard from Jeremy Hunt
on 24 Jan 2017• Health Select Committee hearing today from panel
of experts about reciprocal healthcarearrangements, and use of staff drawn from the EU

Public health
• European Centre for Disease Control andPrevention – early warning and response system forthe prevention and control of communicablediseases
• Jeremy Hunt indicated that do not want to changeposition in public health
Healthcare professionals
• 130,000 EU nationals working in health and socialcare. 55,400 in the NHS – 5% total workforce (9%hospital doctors and 6% nurses)
• Simon Stevens seeking assurance EU nationals canremain and continue to work in NHS
• Jeremy Hunt says this presents an opportunity for“proper strategic workforce planning”. Priority toensure agreement that EU nationals can remainand continue to work in NHS.

Recognition of qualifications
• European Directive on the recognition ofqualifications – health and social care professionalswho qualified within the EEA automatically havetheir qualifications recognised by relevantregulatory bodies in EEA
• Language and other requirements increase?• Capability of regulators to cope? i.e. Nursing and
Midwifery Council

EU Working Time Directive
• Limits working week to 48 hours and 11 hours restbetween working periods
• Initially junior doctors excluded because ofconcerns re training – phased in by 2009
• Limitations of ECJ case law that on call time at aplace of work even if sleeping counted as working
• Possibly regarded as a good thing – although not byunions…..

• BUT Jeremy Hunt said that it is not the intention ofGovernment to weaken workers rights. Controlover hours was brought in partly to tackleexcessive hours in Dr training.

Reciprocal access to healthcare
• Currently reciprocal access to healthcare in otherEU countries
• Could retain something i.e. Swiss residentsparticipate in European Health Insurance Cardscheme
• EEA and non-perm residents cost NHS £305m perannum, around £220m recoverable. Only £50mrecovered in 2012-13
• Jeremy Hunt says NHS has to get better at recovery

Medicines regulation
• European Medicines Agency – responsible forscientific evaluation of human and veterinarymedicines developed by pharmaceutical companiesfor use in the EU.
• Pharma companies can apply to EMA for centralisedauthorisation, and process is compulsory for sometypes of drug. Companies can apply to nationalmarketing authorities EU simultaneously, orthrough mutual-recognition procedure

• Simon Stevens indicating a preference to remain amember of the EMA

Audit & Governance Workshop
Key updates for CCGs
Annette Tudor (Deputy Director)21st February 2017
• Managing Conflicts of Interest in the NHSPublished 9th February 2017, NHS England
• A Manual for Caldicott GuardiansPublished January 2017, UK Caldicott Guardian Council
• Procedures for clinical commissioning groupsto apply for constitution change, merger ordissolutionPublished 3rd November 2016
• STP Checklist for Governance &EngagementPublished 22nd November, NHS Clinical Commissioners inpartnership with NHS Confederation, National Voices and theCentre for Public Scrutiny,
All information correct at time of production.
The information and opinions expressed within this document areno substitute for full legal advice. It is for guidance only andillustrates the law as at the published date. If in doubt, pleasetelephone us on 0370 270 6000.
© Browne Jacobson LLP 2017 – The information contained withinthis document is and shall remain the property of BrowneJacobson. This document may not be reproduced without the priorconsent of Browne Jacobson.