early rehabilitation in the icu: do we still need chest ... rehabilitation in the icu: do we still...
TRANSCRIPT

Early Rehabilitation in the ICU: Do We Still Need Chest Physiotherapy?
Michelle Kho, PT, PhD
Assistant Professor, School of Rehabilitation Science, McMaster University
Adjunct Assistant Professor, Department of Physical Medicine and Rehabilitation, Johns Hopkins University
November 12, 2013

Financial Interest Disclosure
• I have no conflict of interest.
• Funding – Canadian Institutes of Health Resarch
Overview of today’s talk
A resource issue
Review of evidence
Practical considerations

We have a potentially serious supply and demand problem in Canada:
Landry et al., Human Resources for Health 2007, 5:23.
1991 - 2005
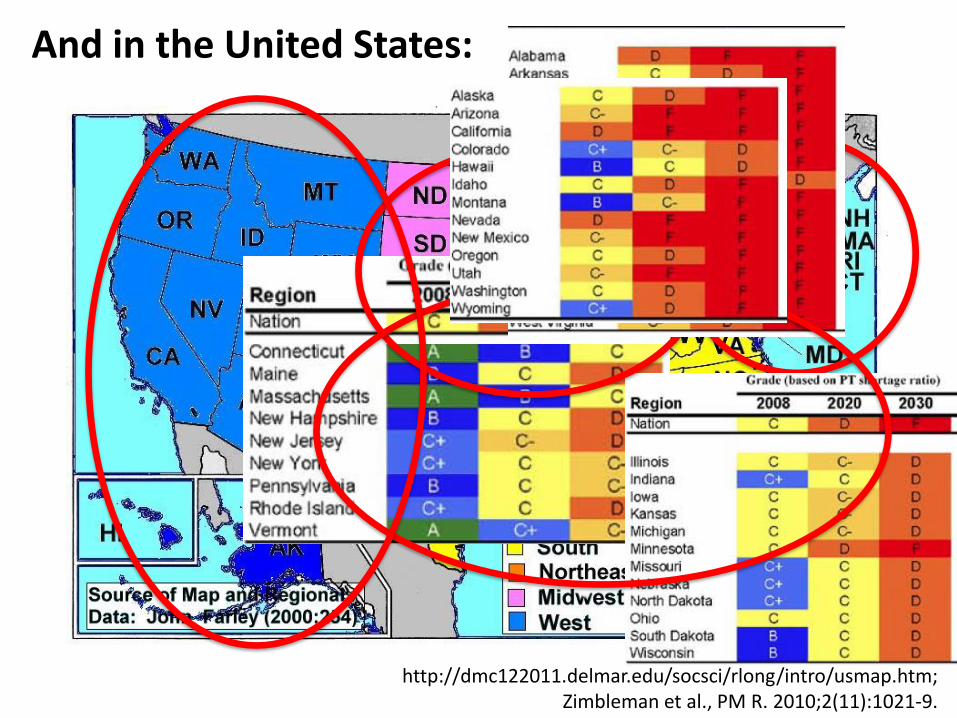
And in the United States:
http://dmc122011.delmar.edu/socsci/rlong/intro/usmap.htm; Zimbleman et al., PM R. 2010;2(11):1021-9.
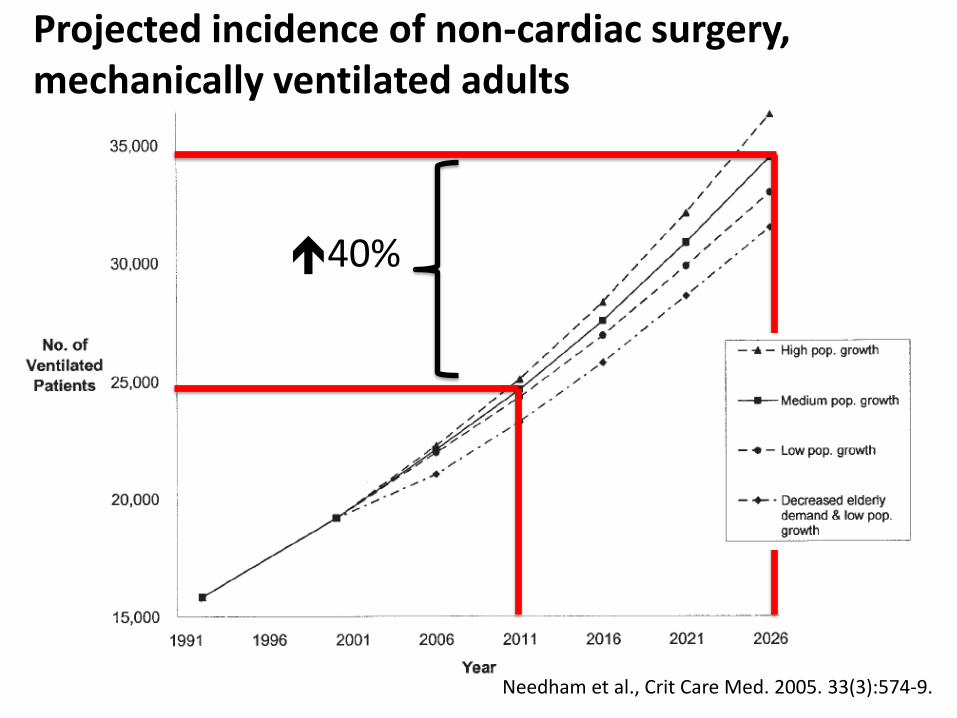
Needham et al., Crit Care Med. 2005. 33(3):574-9.
40%
Projected incidence of non-cardiac surgery, mechanically ventilated adults
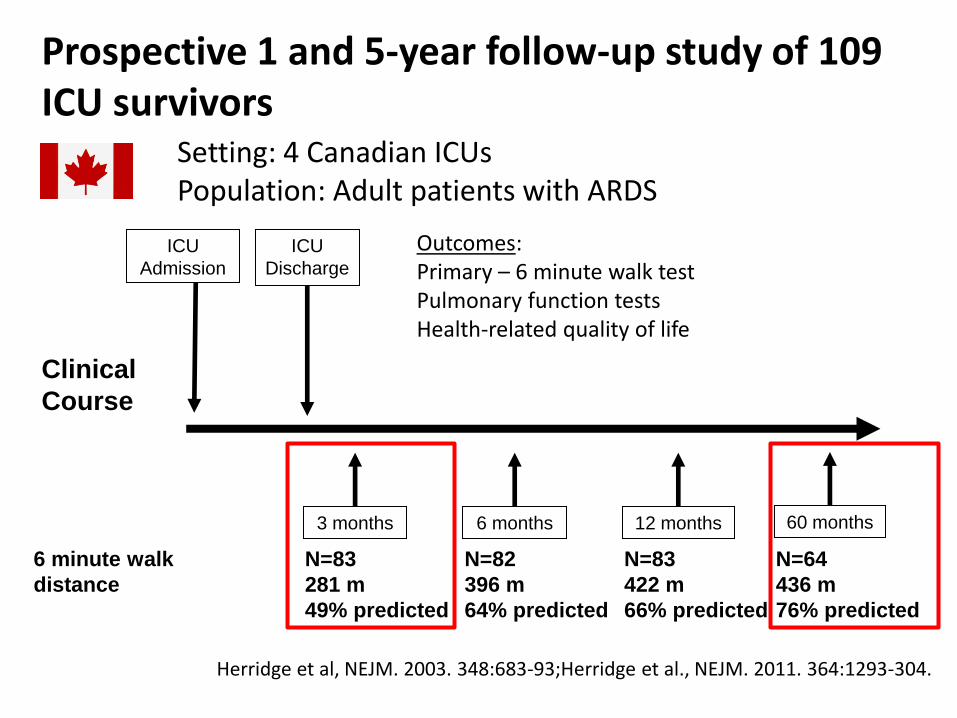
Prospective 1 and 5-year follow-up study of 109 ICU survivors
Clinical
Course
ICU
Discharge
ICU
Admission
Setting: 4 Canadian ICUs Population: Adult patients with ARDS
3 months 6 months 12 months
Outcomes: Primary – 6 minute walk test Pulmonary function tests Health-related quality of life
60 months
N=83
281 m
49% predicted
N=83
422 m
66% predicted
6 minute walk
distance
N=82
396 m
64% predicted
N=64
436 m
76% predicted
Herridge et al, NEJM. 2003. 348:683-93;Herridge et al., NEJM. 2011. 364:1293-304.

Prospective 1 year study of 545 ICU survivors
Clinical
Course
ICU
Discharge
ICU
Admission
6 months
Outcomes: Primary – SF-36 (V2) Physical function domain Secondary – Physical, psychological, & cognitive function; quality of life; employment status
12 months
Needham et al., BMJ. 2013. 346:f1532.
SF-36 Physical Function 82(9) 51(32) 55(32)
SF-36 Mental Health 76(3) 64(26) 65(25)
“Substantial” PTSD 26% (122/514) 23% (107/487)
Employed 52% (116/223) 52% (116/223)
Outcomes
Mean (SD) ICU LOS: 14(12); Hospital LOS: 22(16)
Norms
Setting: 41 US ICUs Population: Adult pts with ARDS in NHLBI EDEN RCT
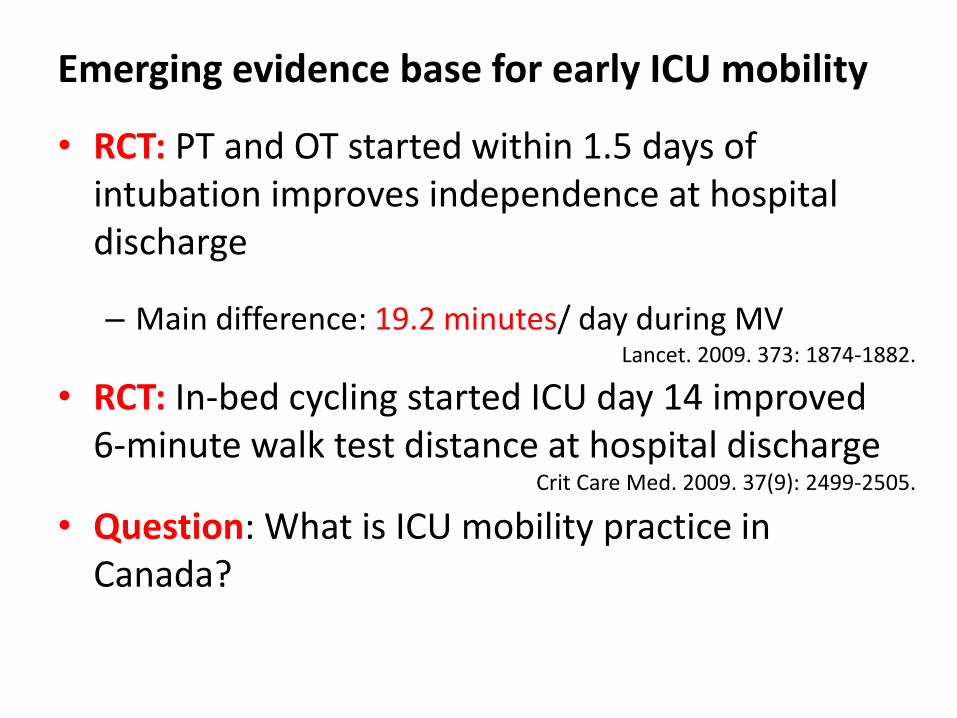
Emerging evidence base for early ICU mobility
• RCT: PT and OT started within 1.5 days of intubation improves independence at hospital discharge
– Main difference: 19.2 minutes/ day during MV
• RCT: In-bed cycling started ICU day 14 improved 6-minute walk test distance at hospital discharge
• Question: What is ICU mobility practice in Canada?
Crit Care Med. 2009. 37(9): 2499-2505.
Lancet. 2009. 373: 1874-1882.
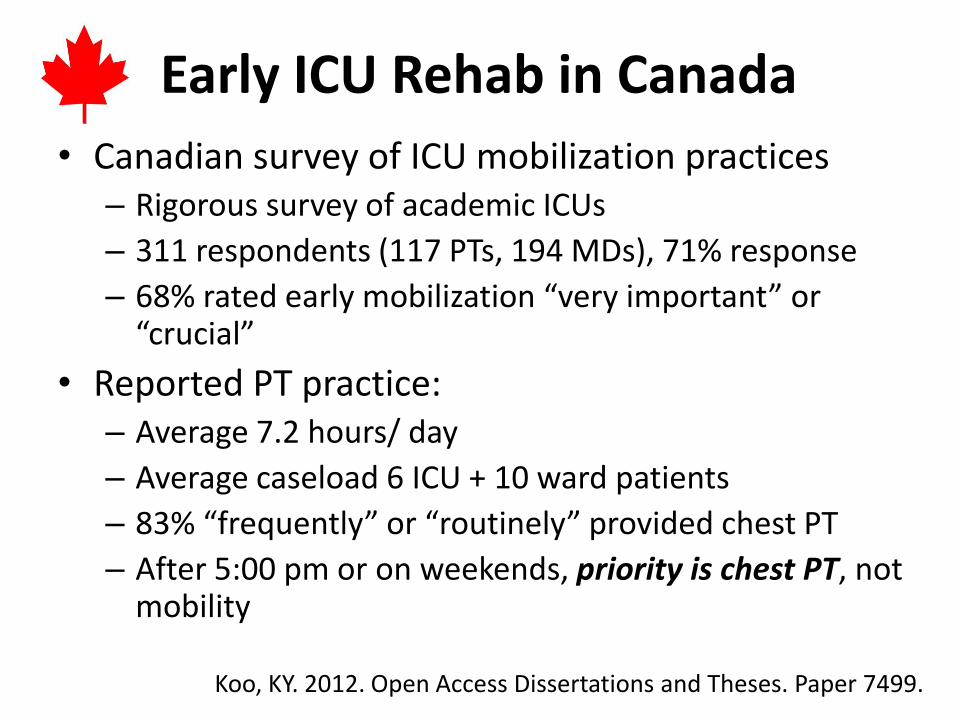
Early ICU Rehab in Canada
• Canadian survey of ICU mobilization practices – Rigorous survey of academic ICUs
– 311 respondents (117 PTs, 194 MDs), 71% response
– 68% rated early mobilization “very important” or “crucial”
• Reported PT practice: – Average 7.2 hours/ day
– Average caseload 6 ICU + 10 ward patients
– 83% “frequently” or “routinely” provided chest PT
– After 5:00 pm or on weekends, priority is chest PT, not mobility
Koo, KY. 2012. Open Access Dissertations and Theses. Paper 7499.
What is the evidence for chest physiotherapy in patients receiving
mechanical ventilation?
Terminology: What is chest physiotherapy?
Ventilator
hyperinflation
percussion
vibration
suctioning
All are interventions to improve respiratory function, which can be delivered by a registered physiotherapist or other members
of the critical care team.
Stiller. Chest. 2013. 144(3):825-47.
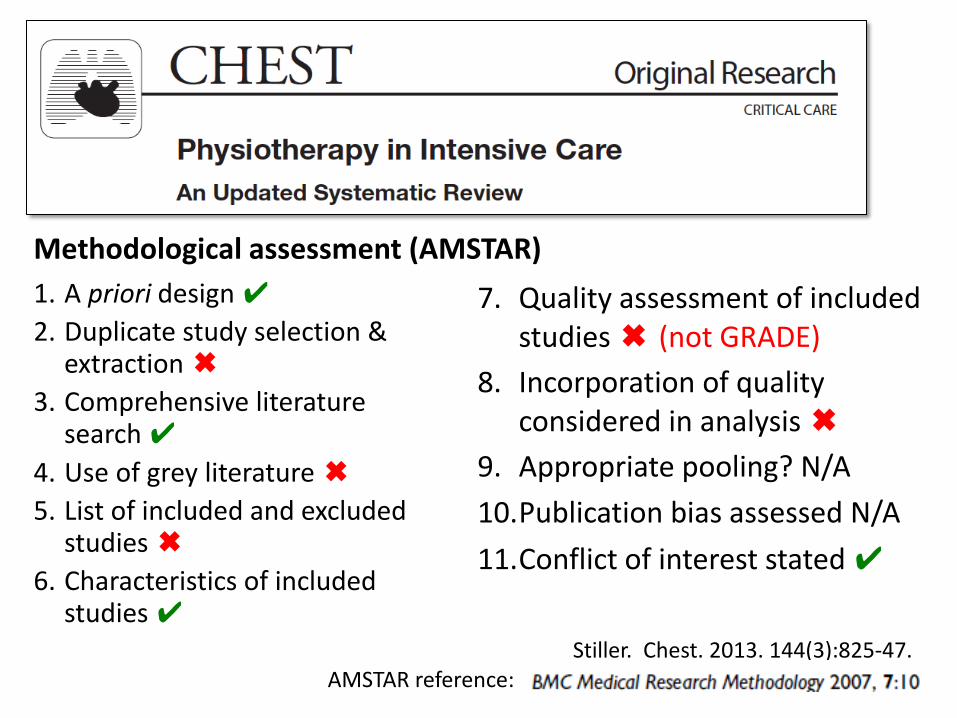
1. A priori design ✔
2. Duplicate study selection & extraction ✖
3. Comprehensive literature search ✔
4. Use of grey literature ✖
5. List of included and excluded studies ✖
6. Characteristics of included studies ✔
7. Quality assessment of included studies ✖ (not GRADE)
8. Incorporation of quality considered in analysis ✖
9. Appropriate pooling? N/A
10.Publication bias assessed N/A
11.Conflict of interest stated ✔
Methodological assessment (AMSTAR)
AMSTAR reference:
Stiller. Chest. 2013 Sep;144(3):825-47.
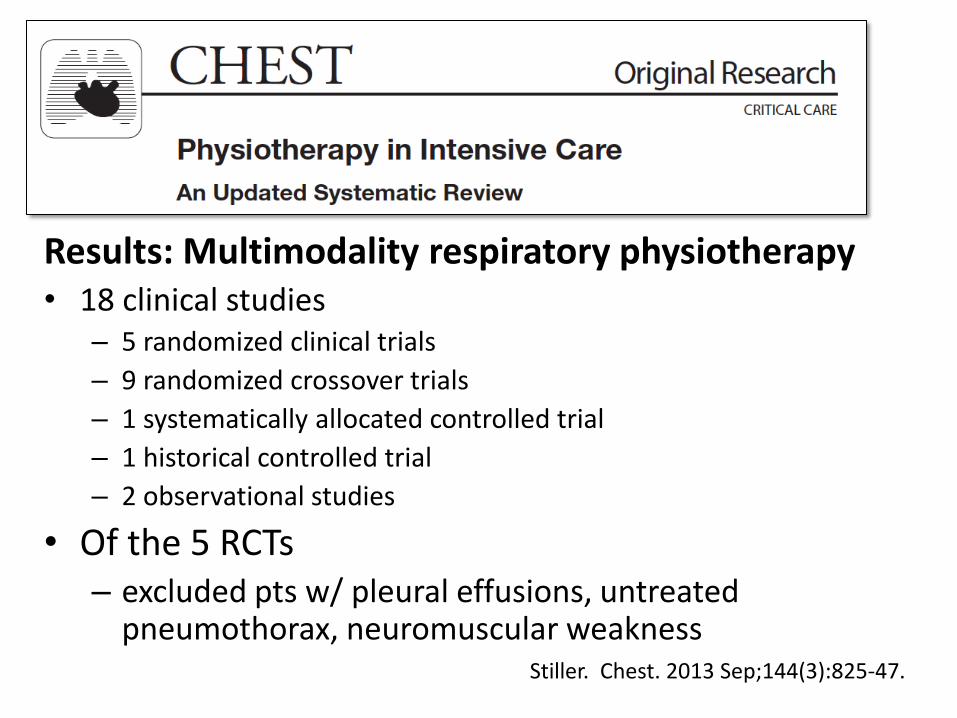
Results: Multimodality respiratory physiotherapy • 18 clinical studies
– 5 randomized clinical trials
– 9 randomized crossover trials
– 1 systematically allocated controlled trial
– 1 historical controlled trial
– 2 observational studies
• Of the 5 RCTs – excluded pts w/ pleural effusions, untreated
pneumothorax, neuromuscular weakness
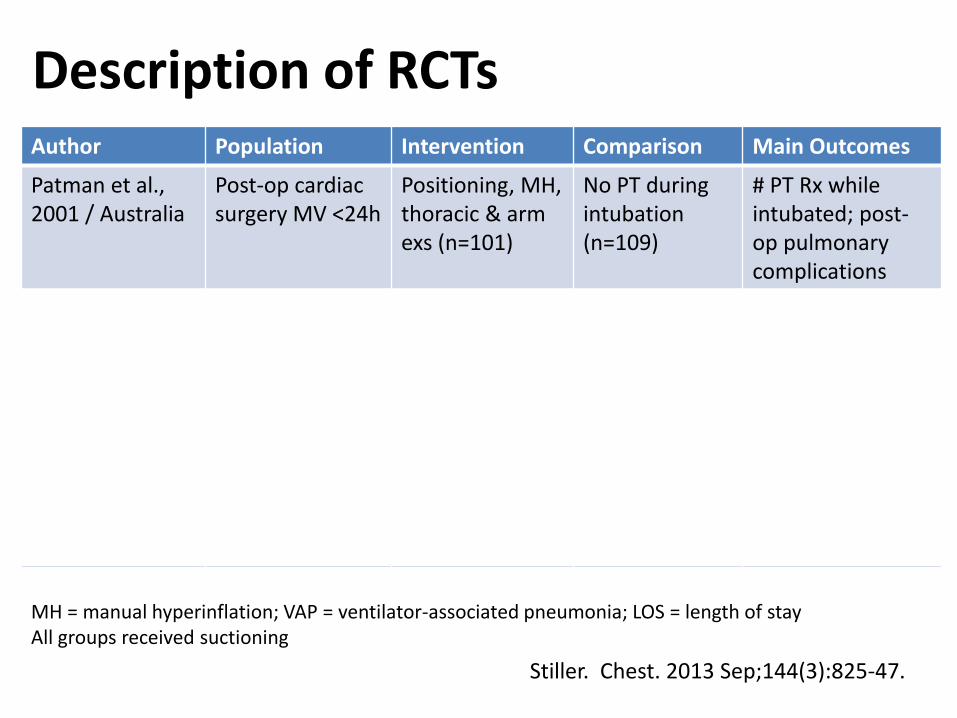
Author Population Intervention Comparison Main Outcomes
Patman et al., 2001 / Australia
Post-op cardiac surgery MV <24h
Positioning, MH, thoracic & arm exs (n=101)
No PT during intubation (n=109)
# PT Rx while intubated; post-op pulmonary complications
Patman et al., 2009 / Australia
Acquired brain injury >24 h MV
Targeted positioning, MH 6x30min q24h until weaned (n=72)
General positioning, MH (n=72)
1°: VAP 2°: LOS, MV duration, mortality
Barker et al. 2002 / UK
Acute lung injury & MV
1: 1 Rx of positioning, 6 MH breaths, (n=7); 17 min
2: Routine care (n=5); 5 min 3: Positioning (n=5); 15 min
Oxygenation, dynamic compliance, & hemodynamics
MH = manual hyperinflation; VAP = ventilator-associated pneumonia; LOS = length of stay All groups received suctioning
Description of RCTs
Stiller. Chest. 2013 Sep;144(3):825-47.
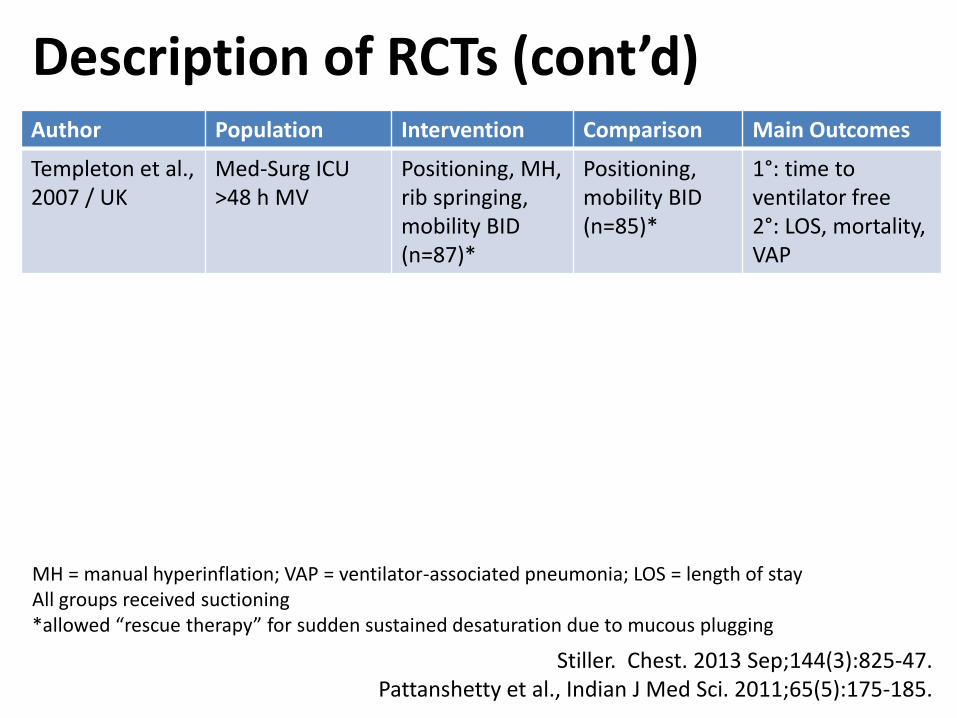
Author Population Intervention Comparison Main Outcomes
Templeton et al., 2007 / UK
Med-Surg ICU >48 h MV
Positioning, MH, rib springing, mobility BID (n=87)*
Positioning, mobility BID (n=85)*
1°: time to ventilator free 2°: LOS, mortality, VAP
Pattanshetty et al. 2010 / India
ICU >48 h MV Positioning, MH, chest vibration BID until weaned (n=50)
MH BID until weaned (n=50)
1°: VAP 2°: LOS, mortality
Pattanshetty et al., 2011 / India NEW
ICU >48 h MV Same as above; (n=87)
Same as above; (n=86)
1°:“recovery rate” 2°: LOS, VAP
MH = manual hyperinflation; VAP = ventilator-associated pneumonia; LOS = length of stay All groups received suctioning *allowed “rescue therapy” for sudden sustained desaturation due to mucous plugging
Description of RCTs (cont’d)
Stiller. Chest. 2013 Sep;144(3):825-47. Pattanshetty et al., Indian J Med Sci. 2011;65(5):175-185.
GRADE = Grades of Recommendation Assessment, Development and Evaluation
CMAJ 2003, BMJ 2004, BMC 2004, BMC 2005,
AJRCCM 2006, Chest 2006, BMJ 2008
2 part framework:
1. Quality of Evidence
2. Strength of recommendations
“Extent to which we are confident that an estimate of effect is correct.”
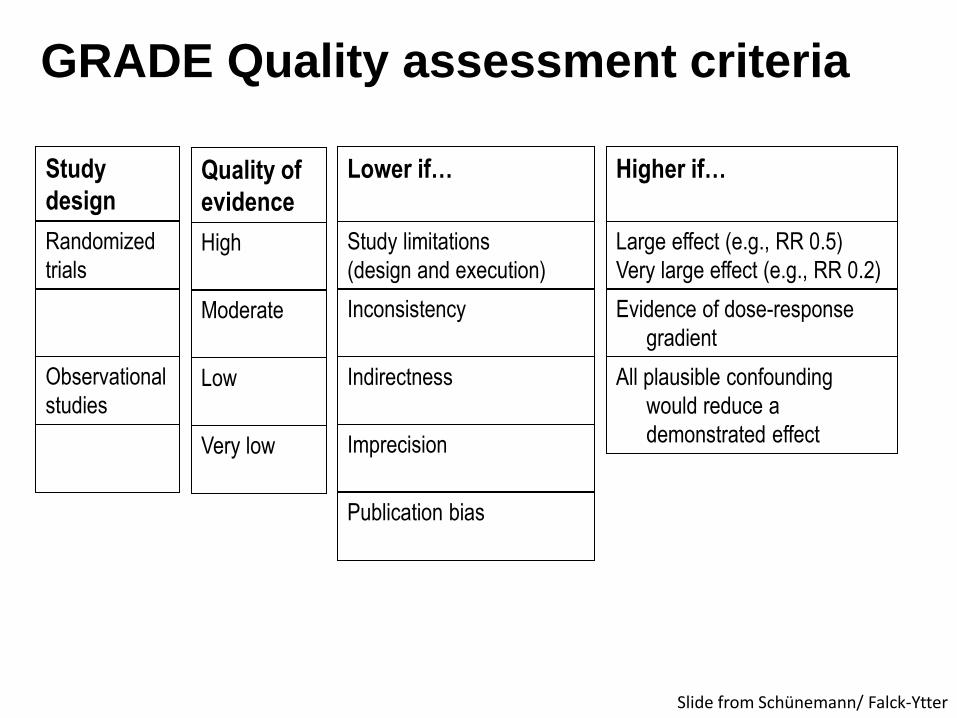
GRADE Quality assessment criteria
Lower if…
Quality of
evidence
High
Moderate
Low
Very low
Study limitations
(design and execution)
Inconsistency
Indirectness
Imprecision
Publication bias
Observational
studies
Study
design
Randomized
trials
Higher if…
Large effect (e.g., RR 0.5)
Very large effect (e.g., RR 0.2)
Evidence of dose-response
gradient
All plausible confounding
would reduce a
demonstrated effect
Slide from Schünemann/ Falck-Ytter

GRADE Quality Assessment
Of 6 parallel group RCTs (n=816 patients),
• Most evidence low to very low quality (⊕⊕⊝⊝)
• Reasons for downgrading
– Imprecision (small sample sizes)
– Indirectness (differences in interventions)
– Inconsistent results
– Study design limitations • Outcomes assessors not blinded to group
• Overall weaknesses in study reporting
GRADE Interpretation: Our confidence in the effect is limited: The true effect may be substantially different from the estimate of the effect.
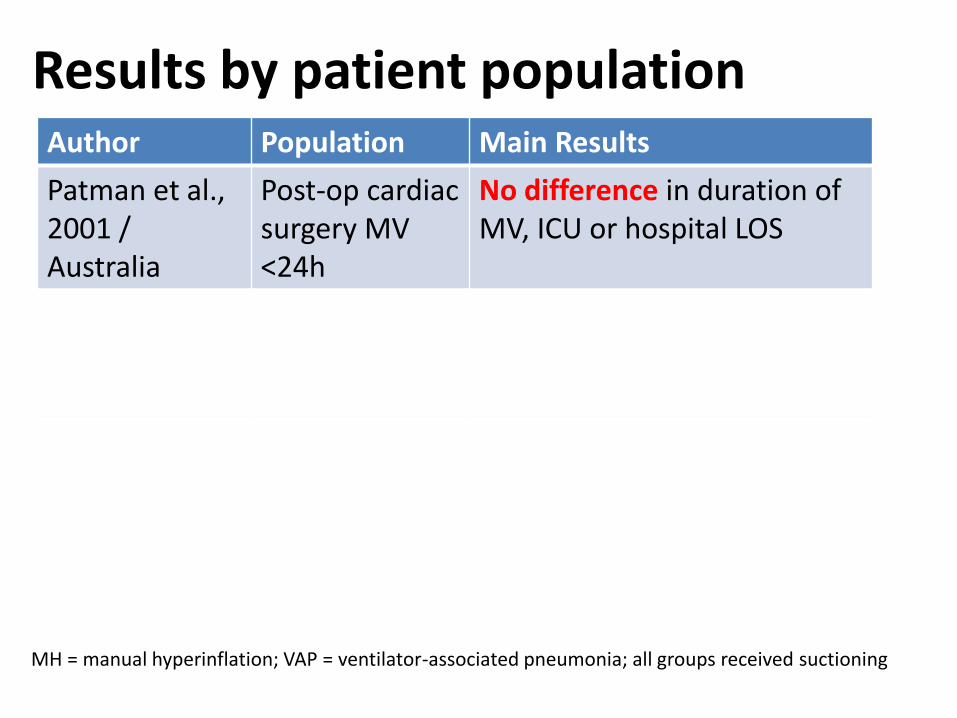
Author Population Main Results
Patman et al., 2001 / Australia
Post-op cardiac surgery MV <24h
No difference in duration of MV, ICU or hospital LOS
Patman et al., 2009 / Australia
Acquired brain injury >24 h MV
1°: VAP – no difference 2°: LOS, MV duration, mortality - no difference
Barker et al. 2002 / UK
Acute lung injury & MV
Oxygenation, dynamic compliance, & hemodynamics
MH = manual hyperinflation; VAP = ventilator-associated pneumonia; all groups received suctioning
Results by patient population
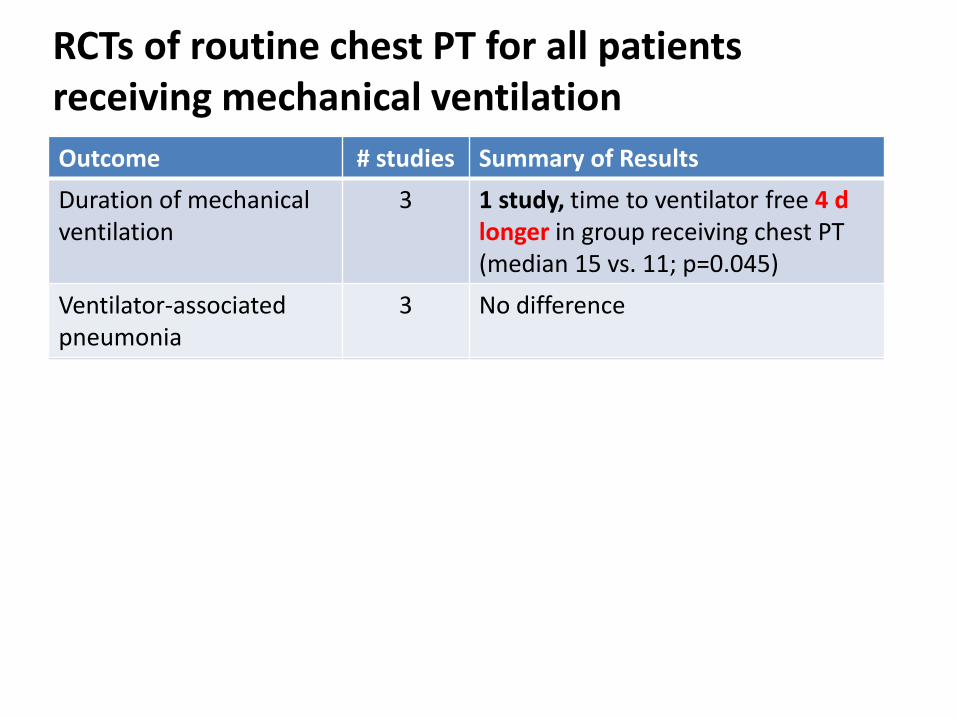
Outcome # studies Summary of Results
Duration of mechanical ventilation
3 1 study, time to ventilator free 4 d longer in group receiving chest PT (median 15 vs. 11; p=0.045)
Ventilator-associated pneumonia
3 No difference
ICU LOS 2 No difference
Hospital LOS 2 • 1 study, 3.2 days longer in group receiving chest PT (p=0.000)
• 1 study, no difference
Mortality 2 • 1 study, lower in group receiving chest PT (12/50 vs. 25/51, p=0.007)
• 1 study, no difference
RCTs of routine chest PT for all patients receiving mechanical ventilation

Strengths and Limitations of Data
Strengths
Published clinical trials
Published systematic review
Utilization-focused outcomes
Limitations
• Applicability in Canadian setting
• Need more focused study of specific populations / indications
• Need more detailed intervention reporting – Frequency, Intensity, Time, Type
• Need more patient-specific outcomes – E.g., Function
Practical considerations
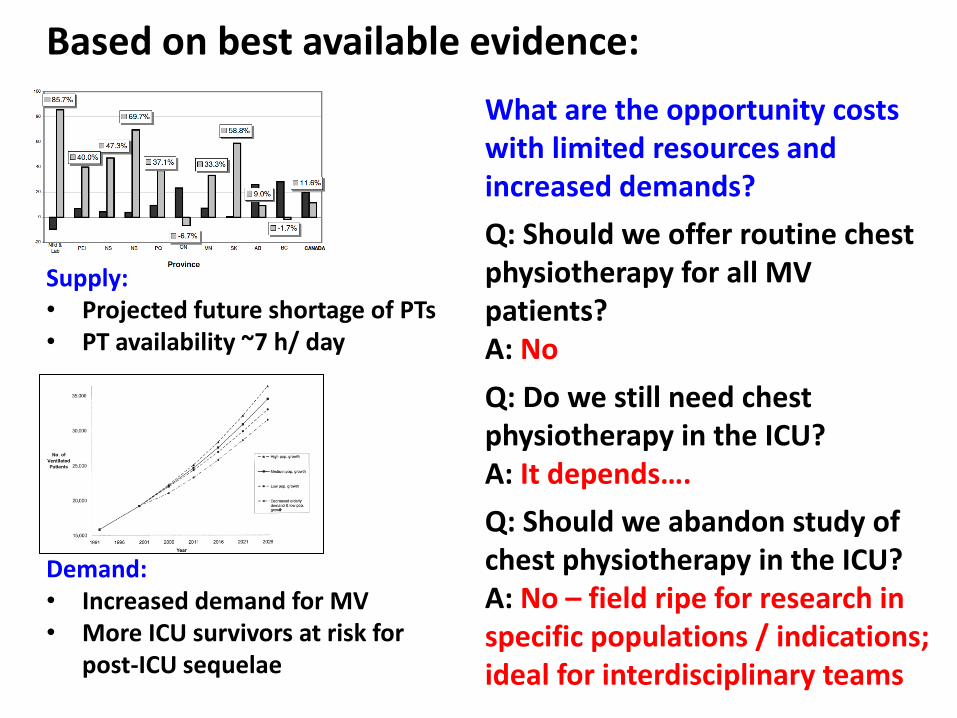
Based on best available evidence:
Supply: • Projected future shortage of PTs • PT availability ~7 h/ day
Demand: • Increased demand for MV • More ICU survivors at risk for
post-ICU sequelae
Q: Should we offer routine chest physiotherapy for all MV patients? A: No
Q: Do we still need chest physiotherapy in the ICU? A: It depends….
Q: Should we abandon study of chest physiotherapy in the ICU? A: No – field ripe for research in specific populations / indications; ideal for interdisciplinary teams
What are the opportunity costs with limited resources and increased demands?

Summary of today’s talk
A resource issue
Review of evidence
Practical considerations [email protected]