early improvement in carotid plaque echogenicity by ... of the vessel wall into the lumen.27...
TRANSCRIPT

Circulation JournalOfficial Journal of the Japanese Circulation Societyhttp://www.j-circ.or.jp
yperglycemia is associated with an increased risk of in-hospital death and cardiac complications in pa-tients with acute myocardial infarction (AMI) and
with or without known diabetes mellitus (DM).1–5 Previous reports4–6 have suggested that hyperglycemia is associated with microvascular dysfunction, vascular inflammation, a pro-thrombotic state, endothelial dysfunction and impaired myo-cardial glucose use, all of which potentially worsen myocardial ischemia. The rapid resolution of hyperglycemia is associated with early improvement of in-hospital cardiac complications in patients with AMI.4,5,7–9 It is known that rupture or instabil-ity of plaques rich in lipid and inflammatory cells importantly contribute to occlusive vascular events.10 However, it remains unknown whether vulnerable coronary plaques may be rap-idly stabilized in parallel with early blood glucose lowering to reduce cardiac events in patients with acute coronary syn-dromes (ACS) and hyperglycemia.
Recent studies10–12 support the concept that plaque instabil-ity is not merely a local vascular occurrence, but rather that plaque instability exists simultaneously at multiple sites in the systemic vascular bed. Thus, it is possible that coronary plaque
vulnerability may be assessed by evaluating plaque character-istics in other vessels such as the carotid arteries. We and others have assessed the composition of carotid plaques using ultrasound with integrated backscatter (IBS) analysis.13–17 Fi-brosis and calcification in the carotid plaque give a high IBS value, whereas macrophage-rich lesions and lipid deposition give a low IBS value.16–19 We have shown that ultrasound evaluation of plaque echolucency is useful for monitoring the efficacy of therapy using statins or thiazolidinediones on ath-eroma vulnerability in carotid plaques13–15 and that carotid plaque echolucency is associated with vulnerable coronary plaques.15
Acarbose, an α-glucosidase inhibitor, is an oral antidiabetic agent that has been shown to be as efficacious as other com-monly used antidiabetic agents.20–23 Given that acarbose has a relatively modest efficacy of blood glucose lowering and min-imal drug-drug interactions,23 it rarely induces severe hypo-glycemic episodes when used in combination with other an-tidiabetic medications. Acarbose may be useful for glucose management in AMI patients with known type 2 DM, because management of glucose levels within a given range and with minimal risk of hypoglycemia is recommended for the treat-
H
Received January 4, 2012; revised manuscript received January 29, 2012; accepted January 30, 2012; released online March 27, 2012 Time for primary review: 12 days
Department of Internal Medicine ІІ, University of Yamanashi, Faculty of Medicine, Chuo, JapanMailing address: Kiyotaka Kugiyama, MD, PhD, Department of Internal Medicine II, University of Yamanashi, Faculty of Medicine, 1110
Shimokato, Chuo 409-3898, Japan. E-mail: [email protected] doi: 10.1253/circj.CJ-11-1524All rights are reserved to the Japanese Circulation Society. For permissions, please e-mail: [email protected]
Early Improvement in Carotid Plaque Echogenicity by Acarbose in Patients With Acute Coronary Syndromes
Mitsumasa Hirano, MD, PhD; Takamitsu Nakamura, MD, PhD; Jyun-ei Obata, MD, PhD; Daisuke Fujioka, MD, PhD; Yukio Saito, MD, PhD; Ken-ichi Kawabata, MD, PhD; Kazuhiro Watanabe, MD; Yosuke Watanabe, MD; Kiyotaka Kugiyama, MD, PhD
Background: The resolution of hyperglycemia is associated with suppression of in-hospital cardiac complications in patients with acute coronary syndromes (ACS). This study evaluated carotid artery plaque echolucency using ultrasound in patients with ACS and type 2 diabetes mellitus (DM) to determine whether acarbose, an α-glucosidase inhibitor, may rapidly stabilize unstable atherosclerotic plaques.
Methods and Results: ACS patients with type 2 DM and carotid plaques (n=44) were randomly assigned to treat-ment with acarbose (150 or 300 mg/day, n=22) or a control group (no acarbose, n=22). Acarbose treatment was initiated within 5 days after the onset of ACS. Unstable carotid plaques were assessed by measuring plaque echo-lucency using carotid ultrasound with integrated backscatter (IBS) before, and at 2 weeks, 1 and 6 months after the initiation of treatment. An increase in the IBS value reflected an increase in carotid plaque echogenicity. As results, the IBS value of echolucent carotid plaques showed a significant increase at 1 month and a further increase at 6 months after treatment in the acarbose group, but there was minimal change in the control group. The increase in IBS values was significantly correlated with a decrease in C-reactive protein levels.
Conclusions: Acarbose rapidly improved carotid plaque echolucency within 1 month of therapy in patients with ACS and type 2 DM.
Key Words: Carotid arteries; C-reactive protein; Plaque vulnerability; Type 2 diabetes mellitus; Ultrasound
Advance Publication by J-STAGE

HIRANO M et al.
ment of hyperglycemia in patients with AMI.24 Acarbose di-rectly targets postprandial hyperglycemia,23 which has been identified as an important cardiovascular risk factor.25 Unlike acarbose, other antidiabetic medications, such as sulfonylureas, have a greater effect on fasting hyperglycemia than on post-prandial hyperglycemia.26 Thus, the goal of the study was to determine whether acarbose treatment in patients with ACS and type 2 DM might have an early benefit in stabilizing un-stable carotid plaques. Carotid ultrasound was used to exam-ine the echolucency of carotid arterial plaques as an index of plaque vulnerability.
MethodsStudy PatientsThis study enrolled 44 patients (mean age 65±11 years, range 43–79 years, 35 males) from 112 consecutive patients with ACS who were admitted to Yamanashi University Hospital from December 2008 to April 2010. The inclusion criteria included previously known type 2 DM and the presence of carotid intima-media thickness (IMT) ≥1.1 mm with protru-sion of the vessel wall into the lumen.27 Patients with severe carotid stenosis (≥50%) were excluded because they have a high risk of ischemic stroke. Type 2 DM was defined accord-ing to the criteria of the American Diabetic Association.28 ACS was diagnosed by the presence of acute ischemic symptoms lasting ≥20 min within 48 h before admission to hospital, and electrocardiographic changes consistent with ACS.29 AMI was diagnosed when creatine kinase-MB levels increased to at least twice the upper limit of normal or when troponin T levels were >0.1 ng/ml. Patients without AMI were considered to
have unstable angina pectoris. All of the patients with ACS had successful reperfusion therapy with percutaneous coro-nary intervention immediately after admission to Yamanashi University Hospital. Exclusion criteria were as follows: (1) use of α-glucosidase inhibitor during the preceding 6 months, (2) history of hepatic disease, (3) chronic renal dysfunction (serum creatinine level >2.0 mg/dl), (4) major surgery and trauma or serious infectious disease within the previous 4 weeks, (5) history of hypersensitivity to acarbose, (6) cardio-genic shock or pulmonary edema (Killip classification ≥II or Forrester classification ≥II) at admission, (7) low left ventricu-lar ejection fraction on echocardiography (<40%), or (8) stroke at admission.
The present study also included 50 patients with stable coro-nary artery disease (CAD), carotid plaque (IMT ≥1.1 mm) and type 2 DM. None of the patients with stable CAD had had any episodes of angina at rest and no changes in the frequency of angina in the previous year. These patients with stable CAD were selected to match the traditional risk factors for athero-sclerosis of the patients with ACS, and they were examined to compare biomarkers and carotid ultrasound parameters at baseline with the ACS patients. The baseline clinical charac-teristics and medication usage are shown in Tables 1 and 2, respectively. All female patients were postmenopausal, and not on any hormone replacement therapy. Written informed consent was given by all patients before the study. This study was approved by the institution’s ethics committee. The inves-tigation conformed to the principles outlined in the 1975 Dec-laration of Helsinki.
Table 1. Comparison of Baseline Characteristics of the Study Patients With ACS or CAD
ACS patients (n=44)Stable CAD (n=50)
Acarbose (n=22) Control (n=22)
Age (years) 65±10 65±11 65±10
Sex (male %) 82 77 76
AMI (%) 82 73 –
Hypertension (%) 73 68 70
Smoking (%) 77 73 72
BMI (kg/m2) 25.0±3.9 24.9±3.8 24.7±3.7
No. of diseased vessels 1.7±0.8 1.8±0.8 1.8±0.7
LVEF (%) 53.3±8.4* 54.1±9.2* 65.3±8.4
LDL-C (mg/dl) 132±29 139±36 136±28
Triglyceride (mg/dl) 127 (89, 168) 118 (74, 169) 120 (80, 169) HDL-C (mg/dl) 42±8 43±9 44±7
Glucose at admission (mg/dl) 239±93 236±88 –
Fasting glucose (mg/dl) 170±60 163±31 161±36
Postprandial glucose (mg/dl) 238±79 240±53 237±61
IRI (μU/ml) 7.4 (4.5, 12.3) 9.6 (4.6, 14.3) 8.2 (4.4, 13.2)
HOMA-IR 2.5 (1.7, 5.1) 2.7 (1.2, 4.3) 2.6 (1.4, 4.7) Hemoglobin A1c (%) 8.0±1.8 8.1±1.7 7.9±1.7
CRP (mg/dl) 0.89 (0.29, 1.15)* 0.93 (0.45, 1.25)* 0.09 (0.05, 0.15)
Calibrated IBS (dB) –18.2±3.7* –18.4±4.0* –14.3±2.6
IMTmax (mm) 1.79±0.48 1.73±0.42 1.69±0.38
Data are expressed as the mean value ± SD, median and interquartile range (25th and 75th percentiles) or % of patients.*P<0.05, vs. stable CAD; Hypertension, blood pressure ≥140/90 mmHg or taking antihypertensive medication; Smoking, >10 cigarettes/day for >1 year.ACS, acute coronary syndrome; CAD, coronary artery disease; BMI, body mass index; LVEF, left ventricular ejection fraction on echocardiography; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein choles-terol; IRI, immunoreactive insulin; HOMA-IR, homeostasis model assessment of insulin resistance; CRP, C-reactive protein; IMT, intima-media thickness.
Advance Publication by J-STAGE
Carotid Plaque Echogenicity and Acarbose in ACS
Study ProtocolThe study patients with ACS were all treated with standard medical therapy and were randomly allocated, using random numbers generated by a computer, into a group treated with acarbose (n=22) or a control group that was treated without acarbose (n=22). Acarbose treatment was initiated within 5 days after the onset of ACS. Patients in both groups were pro-spectively followed for 6 months. The daily dose of acarbose was initially 150 mg, and the dose was increased to 300 mg at 2 months after the start of treatment when the hemoglobin A1c (HbA1c) level was ≥7.5% 2 months after enrollment. Antidia-betic medications other than α-glucosidase inhibitor were per-mitted in both groups, but the types of antidiabetic medica-tions were maintained throughout the study after the allocation of acarbose. In the control group, the increase in the dosage of the antidiabetic medications was permitted when the HbA1c level was ≥7.5% 2 months after enrollment. Carotid ultra-sound and blood sampling were performed on the morning after an overnight fast in the same manner before, and at 2 weeks, 1 month and 6 months of treatment. All patients re-ceived the standardized cardiac medications shown in Table 2 during the follow-up period.
Carotid UltrasoundA carotid ultrasound examination was performed in the ultra-sound laboratory using an 11.0-MHz, linear-array transducer (SONOS-5500, Phillips, Andover, MA, USA) in the morning after an overnight fast before treatment; and after 2 weeks, 1 month and 6 months of treatment.13–15 The measurements were performed by 2 well-trained researchers (J.O., T.N.) who did not have any information about the randomization or clinical characteristics of the study patients. IMT was defined as the distance from the leading edge of the lumen-intima interface to the leading edge of the media-adventia interface on a longi-tudinal image of each carotid artery. Atherosclerotic plaque was defined as a lesion with a focal IMT ≥1.1 mm, which re-sulted in a localized protrusion of the vessel wall into the lumen. Maximal IMT (IMTmax) was defined as the greatest axial thickness in the carotid arteries. Subsequently, we mea-sured the IBS value of all plaques, as described previously.13–15 For each plaque, conventional high resolution, B-mode im-ages were obtained, followed by the acquisition of 60 IBS images. Atherosclerotic plaques were analyzed using the man-ual definition mode to outline the region of interest (ROI). The average power of the IBS signal within the ROI was measured and displayed in decibels for a total of 60 frames. In the case of heterogeneous plaques, we excluded excessively high echo-genic areas with acoustic shadowing, which indicated calcifi-cation in the ROI. We adopted the adventitia as the reference object and then expressed the relative IBS value of the intima-media complex as the difference in IBS values between the intima-media and adventitia (calibrated IBS=intima-media IBS value – adventitia IBS value). In each patient, we selected the plaque with the most echolucent calibrated IBS value among all carotid plaques at baseline as the target plaque for monitoring the calibrated IBS value during treatment. The exact distance of the target plaque from the bifurcation of the common carotid artery or a site of arterial calcification was recorded as a landmark in each patient to ensure that the same target plaque was measured during treatment. Also, the head positions and probe positions during the examinations were recorded in each patient. Measurement of IMTmax and cali-brated IBS was performed twice during each session in all patients, and the averaged value of the 2 measurements was used for further analyses. The inter- and intraobserver vari-
abilities for repeated measurements of the calibrated IBS value were 0.3±0.3 dB and 0.5±0.4 dB, respectively. An increase in IBS value reflects an increase in carotid plaque echogenicity.
Laboratory ExaminationsVenous blood samples were obtained from all patients after a 12-h overnight fast at the same time points used for the ultra-sound assessment of carotid plaques. After the blood sampling and ultrasound examination in the fasting condition, all study patients had the same test breakfast (500 kcal) consisting of 75 g carbohydrate, 24 g protein and 12 g fat, supplied by the hospital. At 2 h after taking the test meal, blood samples were again obtained for measurement of postprandial glucose lev-els. High sensitive C-reactive protein (CRP) levels in the fast-ing plasma were assayed by rate nephelometry (Dade Behring, Marburg, Germany). The serum total cholesterol and triglyc-eride concentrations were measured enzymatically, and the serum high-density lipoprotein cholesterol (HDL-C) concen-tration was measured by heparin-Ca2+/Ni2+ precipitation. Low-density lipoprotein cholesterol levels were calculated by the Friedewald’s formula. Plasma insulin levels (immunoreactive insulin; IRI) were determined by an enzyme immunoassay (Tosoh, Tokyo, Japan). The plasma glucose concentration was determined with an autoanalyzer using the glucose oxidase method. The homeostasis model assessment of insulin resis-
Table 2. Comparison of Frequencies of Medication Usage at Admission and During 6 Months of Follow-up in Patients With ACS
Acarbose (n=22)
Control (n=22) P value
At admission
Aspirin 5 (23) 7 (32) 0.50
Thienopyridines 4 (18) 2 (9) 0.38
β-blocker 2 (9) 3 (14) 0.63
CCB 8 (36) 7 (32) 0.75
ACEI or ARB 10 (45) 10 (45) –
Statin 5 (23) 6 (27) 0.73
SU 7 (32) 6 (27) 0.74
Pioglitazone 6 (27) 4 (18) 0.47
Biguanide 1 (5) 1 (5) –
Insulin 3 (14) 4 (18) 0.68
During 6 months follow-up
Aspirin 22 (100) 22 (100) –
Thienopyridines 21 (95) 19 (86) 0.29
β-blocker 5 (23) 6 (27) 0.73
CCB 14 (64) 13 (59) 0.76
ACEI or ARB 17 (77) 18 (82) 0.71
Statin 17 (77) 15 (68) 0.50
Rosuvastatin 2.5 mg/day 7 (32) 6 (27) 0.74
Rosuvastatin 5 mg/day 2 (9) 2 (9) –
Pravastatin 10 mg/day 6 (27) 5 (23) 0.73
Atrovastatin 10 mg/day 2 (9) 2 (9) –
SU 10 (45) 9 (41) 0.76
Pioglitazone 10 (45) 7 (32) 0.35
Biguanide 1 (5) 2 (9) 0.55
Insulin 4 (18) 5 (23) 0.71
Values are expressed as number of patients (%).ACS, acute coronary syndrome; CCB, calcium-channel blocker; ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin II receptor blocker; SU, sulfonylurea.
Advance Publication by J-STAGE
HIRANO M et al.
tance (HOMA-IR) was determined by the following formula: fasting plasma insulin (in μU/ml)×fasting plasma glucose (in mg/dl)/405. Plasma IRI levels and HOMA-IR were measured for the statistical analysis in the study patients taking no insu-lin treatment.
Statistical AnalysisData are expressed as the mean value ± SD, median and inter-quartile range (25th and 75th percentiles) or frequencies (%). The Shapiro-Wilk test showed that the levels of CRP, triglyc-erides, IRI and HOMA-IR were not distributed normally, and therefore these data were log-transformed for statistical analy-sis. The mean value and frequency between 2 groups were compared using a Student’s unpaired t-test and a chi-square analysis, respectively. For comparisons of the mean values be-fore and during treatment, 1-way analysis of variance (ANOVA) was performed followed by a Scheffé test for post-hoc com-parisons. The mean value of lipids, other biochemical param-eters and calibrated IBS values before and during treatment were compared between 2 groups using 2-way ANOVA for repeated measures followed by post-hoc testing. P values were tabulated for duration, group (acarbose vs. control) effects and interaction by 2-way repeated-measures ANOVA. When the
duration effect was significant, differences between time points in each group were compared with a Scheffé test. When the group effect was significant, differences between groups at each time point were compared with a Student’s unpaired t-test. Also, the percent changes in HbA1c and CRP from base-line to either 1 month or 6 months of treatment were not dis-tributed normally, and therefore the relationship of the percent changes in calibrated IBS values with the percent changes in CRP and other biochemical parameters after therapy was ana-lyzed by the Spearman rank correlation test using data from both treatment groups. The independent relationship of the percent changes in calculated IBS with those in the biochemi-cal parameters was examined in the multivariate linear regres-sion analysis using the percent changes in biochemical param-eters as covariates that had a significant relationship with the change in calculated IBS at 6 months treatment in the Spear-man rank correlation test. Statistical significance was defined as P<0.05. Analyses were performed using StatView 5.0 for Windows (Tokyo, Japan) and JMP (SAS Institute Inc, Cary, NC, USA).
Previous literature showed that acarbose treatment may potentially improve HOMA-IR by 20–30% in patients with type 2 DM.30 On the basis of the correlation between changes
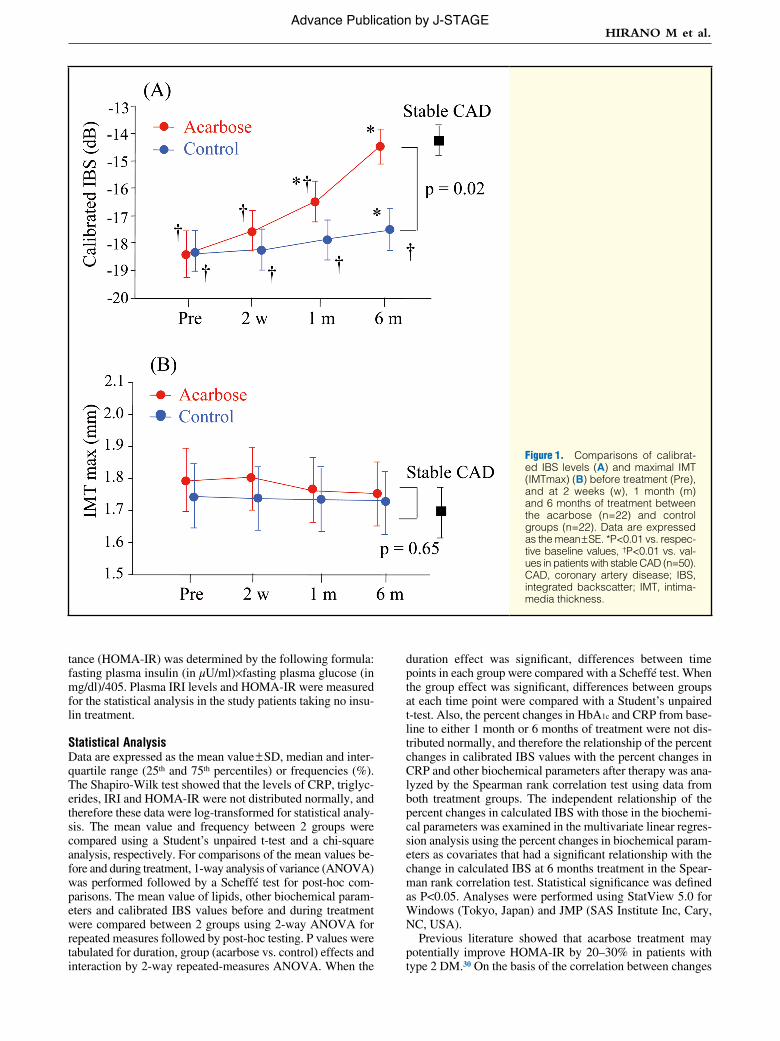
Figure 1. Comparisons of calibrat-ed IBS levels (A) and maximal IMT (IMTmax) (B) before treatment (Pre), and at 2 weeks (w), 1 month (m) and 6 months of treatment between the acarbose (n=22) and control groups (n=22). Data are expressed as the mean ± SE. *P<0.01 vs. respec-tive baseline values, †P<0.01 vs. val-ues in patients with stable CAD (n=50). CAD, coronary artery disease; IBS, integrated backscatter; IMT, intima-media thickness.
Advance Publication by J-STAGE
Carotid Plaque Echogenicity and Acarbose in ACS
in HOMA-IR and calibrated IBS value in our previous study,13 we proposed that acarbose would increase the calibrated IBS value by approximately 25% after 6 months of treatment. Power analysis showed that given this effect size (25%), a probability of type-I error of 0.05 (2-tailed), a power of 0.8, and an expected SD of the calibrated IBS values of 2.0 dB, the minimum required sample size needed was 20 patients in each group.
ResultsComparison of Pretreatment Data in Patients With ACSThe daily dose of acarbose was increased to 300 mg at 2 months after the start of treatment in 10 patients in the acar-bose group, and the dose remained at 150 mg during the 6 months of treatment in the remaining 12 patients. All of the study patients completed the trial, and there were no adverse events related to acarbose. None of the study patients had re-current cardiovascular events or obvious heart failure during the 6 months of follow-up. The blood glucose levels at admis-sion were similar between the acarbose and control groups (Table 1). The 2 treatment groups had similar profiles for traditional risk factors, calibrated IBS values, IMTmax, and levels of CRP and fasting and postprandial glucose that were collected on the day after admission (Table 1). Both treatment groups had hyperglycemia in the fasting and postprandial conditions (Table 1). The use of antihypertensive, lipid-low-ering, antiplatelet and antidiabetic medications, except acar-bose at administration and at 6 months of the follow-up, was similar between the 2 groups (Table 2).
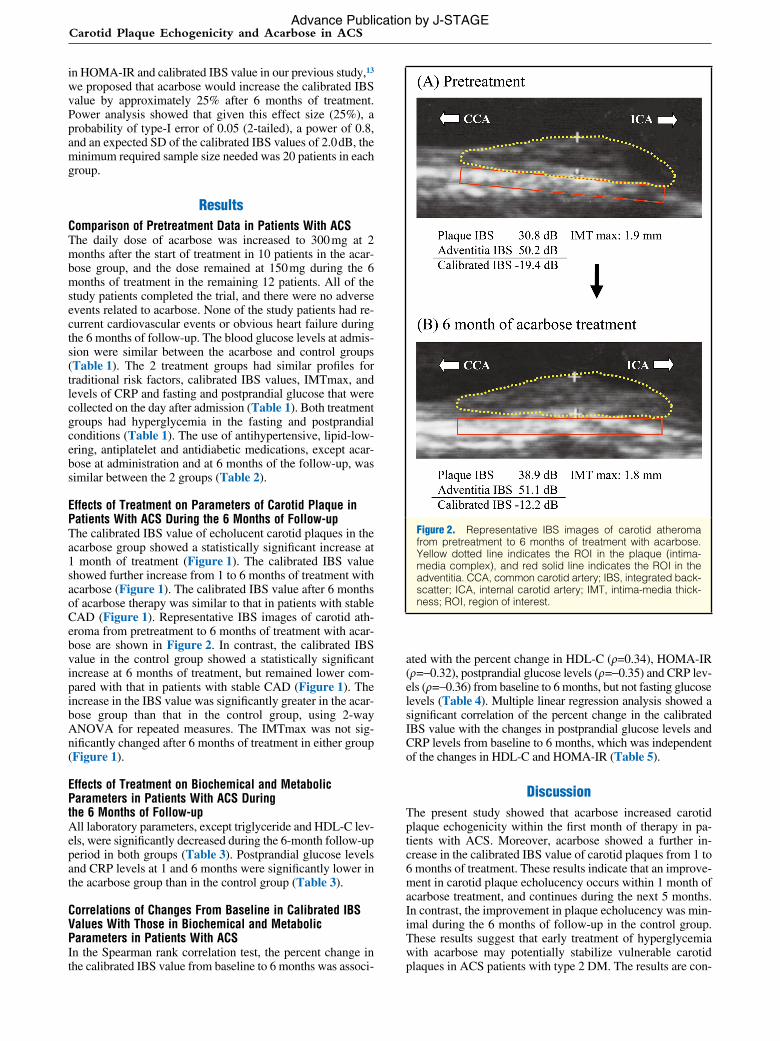
Effects of Treatment on Parameters of Carotid Plaque in Patients With ACS During the 6 Months of Follow-upThe calibrated IBS value of echolucent carotid plaques in the acarbose group showed a statistically significant increase at 1 month of treatment (Figure 1). The calibrated IBS value showed further increase from 1 to 6 months of treatment with acarbose (Figure 1). The calibrated IBS value after 6 months of acarbose therapy was similar to that in patients with stable CAD (Figure 1). Representative IBS images of carotid ath-eroma from pretreatment to 6 months of treatment with acar-bose are shown in Figure 2. In contrast, the calibrated IBS value in the control group showed a statistically significant increase at 6 months of treatment, but remained lower com-pared with that in patients with stable CAD (Figure 1). The increase in the IBS value was significantly greater in the acar-bose group than that in the control group, using 2-way ANOVA for repeated measures. The IMTmax was not sig-nificantly changed after 6 months of treatment in either group (Figure 1).
Effects of Treatment on Biochemical and Metabolic Parameters in Patients With ACS During the 6 Months of Follow-upAll laboratory parameters, except triglyceride and HDL-C lev-els, were significantly decreased during the 6-month follow-up period in both groups (Table 3). Postprandial glucose levels and CRP levels at 1 and 6 months were significantly lower in the acarbose group than in the control group (Table 3).
Correlations of Changes From Baseline in Calibrated IBS Values With Those in Biochemical and Metabolic Parameters in Patients With ACSIn the Spearman rank correlation test, the percent change in the calibrated IBS value from baseline to 6 months was associ-
ated with the percent change in HDL-C (ρ=0.34), HOMA-IR (ρ=−0.32), postprandial glucose levels (ρ=−0.35) and CRP lev-els (ρ=−0.36) from baseline to 6 months, but not fasting glucose levels (Table 4). Multiple linear regression analysis showed a significant correlation of the percent change in the calibrated IBS value with the changes in postprandial glucose levels and CRP levels from baseline to 6 months, which was independent of the changes in HDL-C and HOMA-IR (Table 5).
DiscussionThe present study showed that acarbose increased carotid plaque echogenicity within the first month of therapy in pa-tients with ACS. Moreover, acarbose showed a further in-crease in the calibrated IBS value of carotid plaques from 1 to 6 months of treatment. These results indicate that an improve-ment in carotid plaque echolucency occurs within 1 month of acarbose treatment, and continues during the next 5 months. In contrast, the improvement in plaque echolucency was min-imal during the 6 months of follow-up in the control group. These results suggest that early treatment of hyperglycemia with acarbose may potentially stabilize vulnerable carotid plaques in ACS patients with type 2 DM. The results are con-
Figure 2. Representative IBS images of carotid atheroma from pretreatment to 6 months of treatment with acarbose. Yellow dotted line indicates the ROI in the plaque (intima-media complex), and red solid line indicates the ROI in the adventitia. CCA, common carotid artery; IBS, integrated back-scatter; ICA, internal carotid artery; IMT, intima-media thick-ness; ROI, region of interest.
Advance Publication by J-STAGE

HIRANO M et al.
sistent with previous reports4,5,7,8 that the clinical benefit of glycemic treatment was observed early during hospitalization in patients with ACS.
Several mechanisms for the improvement in carotid echo-lucency by acarbose treatment may be considered. Although
both postprandial hyperglycemia and fasting hyperglycemia were improved in the control groups as well as the acarbose group, the improvement in postprandial hyperglycemia was more rapid and greater in the acarbose group than in the con-trol group. This is attributed to acarbose treatment because
Table 3. Changes in Lipids and Biochemical Markers During Treatment With and Without Acarbose in Patients With ACS
Acarbose (n=22) Control (n=22)Repeated ANOVA
Duration Group Interaction
LDL-C (mg/dl) P<0.01 P=0.26 P=0.87
Next day 132±29 139±36 2 weeks 119±21 126±31 1 month 108±22* 120±32* 6 months 101±22* 107±30* Triglyceride (mg/dl) P=0.02 P=0.87 P=0.96
Next day 127 (89, 168) 118 (74, 169) 2 weeks 119 (104, 145) 127 (99, 179) 1 month 121 (97, 145) 130 (94, 168) 6 months 107 (97, 125) 113 (88, 160) HDL-C (mg/dl) P<0.01 P=0.33 P=0.97
Next day 42±8 43±9 2 weeks 38±7 40±7 1 month 41±9 44±7 6 months 44±12 46±7 Fasting glucose (mg/dl) P<0.01 P=0.99 P=0.68
Next day 170±60 163±31 2 weeks 137±22* 139±21* 1 month 131±21* 135±21* 6 months 120±18* 121±16* IRI (μU/ml) P=0.01 P=0.30 P=0.76
Next day 7.4 (4.5, 12.3) 9.6 (4.6, 14.3) 2 weeks 6.5 (3.9, 9.3) 9.5 (4.6, 12.1) 1 month 6.8 (4.1, 8.9) 9.2 (5.3, 12.0)*
6 months 5.9 (3.9, 8.8)* 8.1 (4.8, 12.8)*
HOMA-IR P<0.01 P=0.93 P=0.25
Next day 2.5 (1.7, 5.1) 2.7 (1.2, 4.3) 2 weeks 2.4 (1.4, 3.1)* 2.8 (1.5, 3.8) 1 month 2.2 (1.7, 2.9)* 2.4 (1.3, 3.5)* 6 months 2.2 (1.4, 2.6)* 2.1 (1.5, 3.0)* Hemoglobin A1c (%) P<0.01 P=0.43 P=0.14
Next day 8.0±1.8 8.1±1.7 2 weeks 7.7±1.5 7.9±1.4 1 month 7.4±1.2* 7.8±1.3*
6 months 6.9±1.1* 7.4±1.0*
Postprandial glucose (mg/dl) P<0.01 P=0.02 P=0.08
Next day 238±79 240±53 2 weeks 182±37* 210±36*,†
1 month 161±38* 199±34*,†
6 months 145±40* 179±29*,†
CRP (mg/dl) P<0.01 P<0.01 P<0.01
Next day 0.89 (0.29, 1.15) 0.93 (0.45, 1.25) 2 weeks 0.44 (0.09, 0.69)* 0.63 (0.42, 0.95)* 1 month 0.11 (0.06, 0.22)* 0.34 (0.05, 0.66)*,†
6 months 0.05 (0.02, 0.06)* 0.19 (0.14, 0.34)*,†
Data presented are mean value ± SD or median and interquartile range (25th and 75th percentiles).*P<0.05, vs. next day after the admission. †P<0.05, vs. respective time points in the acarbose group. Details of statis-tical methods are described in the text.Abbreviations see in Table 1.
Advance Publication by J-STAGE
Carotid Plaque Echogenicity and Acarbose in ACS
acarbose has been shown to reduce postprandial hyperglyce-mia to a greater extent than other oral antidiabetic agents such as sulfonylureas.23 It has been shown that the circulating levels of pro-inflammatory cytokines and CRP are increased in pa-tients with type 2 DM, but these levels are more greatly as-sociated with post-challenge hyperglycemia than fasting hy-perglycemia.31,32 We and others have shown that postprandial hyperglycemia induces oxidative stress and endothelial dys-function.4,5,33 Postprandial hyperglycemia could induce pro-inflammatory cytokines through oxidative stress-induced ac-tivation of nuclear factor kappa B.4,5 In line with those previous reports, the present study showed that the decrease in CRP levels was greater in the acarbose group than in the control group. Thus, an improvement in postprandial hyperglycemia may lead to a decrease in CRP levels after acarbose treatment. Moreover, the present results showed that an improvement in carotid echolucency was associated with reduction in both postprandial hyperglycemia and CRP levels at 6 months. Therefore, suppression of the inflammatory response after acarbose treatment may at least partly contribute to the im-proved echolucency of carotid plaques in the present study on the basis of the inflammatory features of unstable atheroscle-rotic plaque. At 1 month of treatment, there was not a statisti-cally significant association between the improvement in ca-rotid echolucency and CRP reduction. However, CRP levels at 1 month were reduced more greatly in the acarbose group than in the control group. Thus, the antiinflammatory effect of acarbose may also play a possible role in the improved carotid echolucency in the acarbose group at 1 month, although other medications, including statin and angiotensin II receptor block-ers (ARB) added after enrollment, could potentially contribute to the improvement in carotid echolucency. It has been shown that exposure of the lower small intestine to undigested carbo-hydrate after acarbose leads to an increase in the release of glucagon-like peptide-1 (GLP-1),34 which is known to have antiatherosclerotic effects.35 This may be another potential mechanism for the beneficial effects of acarbose treatment, although the present study did not measure GLP-1 levels.
The present study showed that IMTmax did not signifi-cantly regress during 6 months of therapy with acarbose. These data suggest that plaque stabilization may precede re-gression in plaque size and support the concept10,36 that stabi-lization rather than regression of vulnerable atheroma is more important in the early reduction of coronary events. A previ-
ous report37 showed that acarbose delayed progression of IMT during treatment for more than 1 year, which is not consistent with the present data. The relatively short period of treatment with acarbose may partly explain the lack of suppression of IMTmax in the present study.
Study LimitationsFirst, this study included a relatively small number of patients, which limited the statistical power of the analysis to show small differences between groups. Second, the study included patients with carotid plaque with a maximum IMT ≥1.1 mm,27 but patients with carotid stenosis ≥50% were excluded be-cause of a high risk of ischemic stroke. It remains to be deter-mined whether similar results would be obtained in general patients with AMI. Third, the largest plaque was selected for serial measurement of IBS from among the eligible plaques (≥1.1 mm of IMT) in each patient. It has been shown that plaque progression is affected by shear stress; low shear causes plaque progression at the proximal internal carotid and the bifurcation of the carotid artery.38 Thus, plaque location may have a potential influence on the change in IMTmax and IBS values over the 6 months of follow-up. Fourth, antiplatelet and antihypertensive drugs, including angiotensin-converting en-zyme inhibitors, ARB, statins, and calcium-channel blockers, may contribute to favorable change in carotid plaque echolu-
Table 4. Nonparametric Analysis of Relationship of % Change in Calibrated IBS Values With % Changes in Clinical Parameters From Next Day After Admission to 1 and 6 Months of Treatment in the Study Patients With ACS
1 month 6 months
ρ P value ρ P value
% Change of LDL-C (mg/dl) –0.07 0.65 –0.03 0.83
% Change of triglyceride (mg/dl) –0.21 0.17 –0.09 0.54
% Change of HDL-C (mg/dl) 0.18 0.23 0.34 0.03
% Change of fasting glucose (mg/dl) –0.11 0.49 –0.04 0.79
% Change of IRI (μU/ml) –0.29 0.06 –0.29 0.06
% Change of HOMA-IR –0.26 0.08 –0.32 0.04
% Change of hemoglobin A1c (%) –0.02 0.87 –0.10 0.51
% Change of postprandial glucose (mg/dl) –0.03 0.86 –0.35 0.03
% Change of CRP (mg/dl) –0.09 0.54 –0.36 0.02
Data are expressed as Spearman’s correlation coefficient by rank (ρ ). The data are from patients including the acar-bose treatment group and the control group.IBS, integrated backscatter. Other abbreviations see in Table 1.
Table 5. Multivariate Linear Regression Models of Relationship of % Change in Calibrated IBS Values With % Changes in Clinical Parameters From Next Day After Admission to 6 Months of Treatment in the Study Patients With ACS
Β P value
% Change of HDL 0.12 0.41 % Change of HOMA-IR –0.22 0.11 % Change of postprandial glucose –0.29 0.04 % Change of CRP –0.38 0.007
Data are expressed as standardized regression coefficient (β). Clinical parameters were selected as independent variables because they had a significant relation with the % change in cali-brated IBS values in the Spearman’s correlation test in Table 4. The data are from patients including the acarbose treatment group and the control group.Abbreviations see in Tables 1,4.
Advance Publication by J-STAGE
HIRANO M et al.
cency,39,40 although there was no significant difference in the number of patients given these drugs at baseline and also at 6 months of the follow-up between both groups.
ConclusionsAcarbose rapidly improved carotid plaque echolucency within 1 month of therapy initiation in patients with ACS and type 2 DM. This may reflect the early clinical benefits of treatment of hyperglycemia in patients with ACS. However, the present results are preliminary and should be confirmed by further studies with a larger number of study patients.
AcknowledgmentsThis study was supported by Grants-in-Aid for (B)(2)-15390244 and (B)-19390209, Priority Areas (C) “Medical Genome Science 15012222” from the Ministry of Education, Culture, Sports, Science, and Technology, and by Health and Labor Sciences Research Grants for Comprehensive Re-search on Aging and Health (H15-Choju-012), Tokyo, Japan.
DisclosuresWe have no conflicts of interest or financial disclosures to declare in conjunction with the publication of this work.
References 1. Capes SE, Hunt D, Malmberg K, Gerstein HC. Stress hyperglycae-
mia and increased risk of death after myocardial infarction in patients with and without diabetes: A systematic overview. Lancet 2000; 355: 773 – 778.
2. Stranders I, Diamant M, van Gelder RE, Spruijt HJ, Twisk JW, Heine RJ, et al. Admission blood glucose level as risk indicator of death after myocardial infarction in patients with and without diabe-tes mellitus. Arch Intern Med 2004; 164: 982 – 988.
3. Wong VW, Ross DL, Park K, Boyages SC, Cheung NW. Hypergly-cemia: Still an important predictor of adverse outcomes following AMI in the reperfusion era. Diabetes Res Clin Pract 2004; 64: 85 – 91.
4. Zarich SW, Nesto RW. Implications and treatment of acute hyper-glycemia in the setting of acute myocardial infarction. Circulation 2007; 115: e436 – e439.
5. Ceriello A, Zarich SW, Testa R. Lowering glucose to prevent adverse cardiovascular outcomes in a critical care setting. J Am Coll Cardiol 2009; 53(Suppl): S9 – S13.
6. Marfella R, Siniscalchi M, Esposito K, Sellitto A, De Fanis U, Romano C, et al. Effects of stress hyperglycemia on acute myocardial infarc-tion: Role of inflammatory immune process in functional cardiac outcome. Diabetes Care 2003; 26: 3129 – 3135.
7. Malmberg K. Prospective randomised study of intensive insulin treat-ment on long term survival after acute myocardial infarction in pa-tients with diabetes mellitus. DIGAMI (Diabetes Mellitus, Insulin Glucose Infusion in Acute Myocardial Infarction) Study Group. BMJ 1997; 314: 1512 – 1515.
8. Goyal A, Mahaffey KW, Garg J, Nicolau JC, Hochman JS, Weaver WD, et al. Prognostic significance of the change in glucose level in the first 24 h after acute myocardial infarction: Results from the CARDINAL study. Eur Heart J 2006; 27: 1289 – 1297.
9. Kosiborod M, Inzucchi SE, Krumholz HM, Masoudi FA, Goyal A, Xiao L, et al. Glucose normalization and outcomes in patients with acute myocardial infarction. Arch Intern Med 2009; 169: 438 – 446.
10. Libby P. Current concepts of the pathogenesis of the acute coronary syndromes, Circulation 2001; 104: 365 – 372.
11. Goldstein JA, Demetriou D, Grines CL, Pica M, Shoukfeh M, O’Neill WW. Multiple complex coronary plaques in patients with acute myo-cardial infarction. N Engl J Med 2000; 343: 915 – 922.
12. Rothwell PM, Villagra R, Gibson R, Donders RC, Warlow CP. Evi-dence of a chronic systemic cause of instability of atherosclerotic plaques. Lancet 2000; 355: 19 – 24.
13. Hirano M, Nakamura T, Kitta Y, Yano T, Kobayashi T, Sano K, et al. Rapid improvement of carotid plaque echogenicity within 1 month of pioglitazone treatment in patients with acute coronary syndrome. Atherosclerosis 2009; 203: 483 – 488.
14. Nakamura T, Obata JE, Kitta Y, Takano H, Kobayashi T, Fujioka D, et al. Rapid stabilization of vulnerable carotid plaque within 1 month of pitavastatin treatment in patients with acute coronary syndrome.
J Cardiovasc Pharmacol 2008; 51: 365 – 371.15. Watanabe K, Sugiyama S, Kugiyama K, Honda O, Fukushima H,
Koga H, et al. Stabilization of carotid atheroma assessed by quantita-tive ultrasound analysis in non hypercholesterolemic patients with coronary artery disease. J Am Coll Cardiol 2005; 46: 2022 – 2030.
16. Takiuchi S, Rakugi H, Honda K, Masuyama T, Hirata N, Ito H, et al. Quantitative ultrasonic tissue characterization can identify high-risk atherosclerotic alteration in human carotid arteries. Circulation 2000; 102: 766 – 770.
17. Waki H, Masuyama T, Mori H, Maeda T, Kitade K, Moriyasu K, et al. Ultrasonic tissue characterization of the atherosclerotic carotid ar-tery: Histological correlates or carotid integrated backscatter. Circ J 2003; 67: 1013 – 1016.
18. Grønholdt ML, Nordestgaard BG, Bentzon J, Wiebe BM, Zhou J, Falk E, et al. Macrophages are associated with lipid-rich carotid ar-tery plaques, echolucency on B-mode imaging, and elevated plasma lipid levels. J Vasc Surg 2002; 35: 137 – 145.
19. Shepard RK, Miller JG, Wickline SA. Quantification of atheroscle-rotic plaque composition in cholesterol-fed rabbits with 50-MHz acoustic microscopy. Arterioscler Thromb 1992; 12: 1227 – 1234.
20. Chiasson JL, Josse RG, Gomis R, Hanefeld M, Karasik A, Laakso M; STOP-NIDDM Trial Research Group. Acarbose treatment and the risk of cardiovascular disease and hypertension in patients with impaired glucose tolerance: The STOP-NIDDM trial. JAMA 2003; 290: 486 – 494.
21. Hanefeld M, Cagatay M, Petrowitsch T, Neuser D, Petzinna D, Rupp M. Acarbose reduces the risk for myocardial infarction in type 2 diabetic patients: Meta-analysis of seven long-term studies. Eur Heart J 2004; 25: 10 – 16.
22. Ceriello A, Taboga C, Tonutti L, Giacomello R, Stel L, Motz E, et al. Post-meal coagulation activation in diabetes mellitus: The effect of acarbose. Diabetologia 1996; 39: 469 – 473.
23. Hanefeld M. Cardiovascular benefits and safety profile of acarbose therapy in prediabetes and established type 2 diabetes. Cardiovasc Diabetol 2007; 6: 20.
24. Kosiborod M, Deedwania P. An overview of glycemic control in the coronary care unit with recommendations for clinical management. J Diabetes Sci Technol 2009; 3: 1342 – 1351.
25. DECODE Study Group, the European Diabetes Epidemiology Group. Glucose tolerance and cardiovascular mortality: Comparison of fast-ing and 2-hour diagnostic criteria. Arch Intern Med 2001; 161: 397 – 405.
26. Baron AD. Postprandial hyperglycaemia and alpha-glucosidase in-hibitors. Diabetes Res Clin Pract 1998; 40(Suppl): S51 – S55.
27. Nguyen-Thanh HT, Benzaquen BS. Screening for subclinical coro-nary artery disease measuring carotid intima media thickness. Am J Cardiol 2009; 104: 1383 – 1388.
28. Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Report of the expert committee on the diagnosis and clas-sification of diabetes mellitus. Diabetes Care 2003; 26: S5 – S20.
29. Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE Jr, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarc-tion: A report of the Am College of Cardiology/Am Heart Associa-tion Task Force on Practice Guidelines (Writing Committee to Re-vise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non ST-Elevation Myocardial Infarction). Circula-tion 2007; 116: e148 – e304.
30. Kim MK, Suk JH, Kwon MJ, Chung HS, Yoon CS, Jun HJ, et al. Nateglinide and acarbose for postprandial glucose control after opti-mizing fasting glucose with insulin glargine in patients with type 2 diabetes. Diabetes Res Clin Pract 2011; 92: 322 – 328.
31. Festa A, D’Agostino R Jr, Tracy RP, Haffner SM. C-reactive protein is more strongly related to post-glucose load glucose than to fasting glucose in non-diabetic subjects: The Insulin Resistance Atheroscle-rosis Study. Diabet Med 2002; 19: 939 – 943.
32. Cardellini M, Andreozzi F, Laratta E, Marini MA, Lauro R, Hribal ML, et al. Plasma interleukin-6 levels are increased in subjects with impaired glucose tolerance but not in those with impaired fasting glucose in a cohort of Italian Caucasians. Diabetes Metab Res Rev 2007; 23: 141 – 145.
33. Kawano H, Motoyama T, Hirashima O, Hirai N, Miyao Y, Sakamoto T, et al. Hyperglycemia rapidly suppresses flow-mediated endothe-lium-dependent vasodilation of brachial artery. J Am Coll Cardiol 1999; 34: 146 – 154.
34. Qualmann C, Nauck MA, Holst JJ, Orskov C, Creutzfeldt W. Glu-cagon-like peptide 1 (7–36 amide) secretion in response to luminal sucrose from the upper and lower gut: A study using alpha-glucosi-dase inhibition (acarbose). Scand J Gastroenterol 1995; 30: 892 – 896.
Advance Publication by J-STAGE

Carotid Plaque Echogenicity and Acarbose in ACS
35. Chilton R, Wyatt J, Nandish S, Oliveros R, Lujan M. Cardiovascular comorbidities of type 2 diabetes mellitus: Defining the potential of glucagonlike peptide-1-based therapies. Am J Med 2011; 124(Suppl): S35 – S53.
36. Nissen SE, Gurley JC, Grines CL, Booth DC, McClure R, Berk M, et al. Intravascular ultrasound assessment of lumen size and wall morphology in normal subjects and patients with coronary artery disease. Circulation 1991; 84: 1087 – 1099.
37. Hanefeld M, Chiasson JL, Koehler C, Henkel E, Schaper F, Temelkova-Kurktschiev T. Acarbose slows progression of intima-media thick-ness of the carotid arteries in subjects with impaired glucose toler-
ance. Stroke 2004; 35: 1073 – 1078.38. Solberg LA, Eggen DA. Localization and sequence of development
of atherosclerotic lesions in the carotid and vertebral arteries. Circu-lation 1971; 43: 711 – 724.
39. Ambrose JA, Martinez EE. A new paradigm for plaque stabilization. Circulation 2002; 105: 2000 – 2004.
40. Sano K, Nakamura T, Hirano M, Kitta Y, Kobayashi T, Fujioka D, et al. Comparative study of bezafibrate and pravastatin in patients with coronary artery disease and high levels of remnant lipoprotein. Circ J 2010; 74: 1644 – 1650.
Advance Publication by J-STAGE