early identification & intervention asd, adhd and ... · please make sure you have signed the...
TRANSCRIPT

Early identification
& intervention –
ASD, ADHD and behavioural
difficulties in children and
young peopleDr. Denise McConnellogue
Clinical Psychologist
Primary Behaviour Service / WLMHT CAMHS
Objectives:
To be able to identify early signs of a neurodevelopmental condition by
comparing to how we expect children to develop normally.
To be aware of why it is important to ask more questions if behavioural
difficulties are reported.
To be confident about what to do if you think a child may be presenting with
early signs of ASD or ADHD.
To know how to discuss a referral for specialist assessment with parents and
obtain informed consent.
To have a clear understanding of key information to include with the referral.
To understand what to expect after making a referral and post investigation.
To understand what to expect from services.
Registration & Evaluation form
Please make sure you have signed the registration list
Please complete the ‘PRE’ section of the training evaluation form now if you
haven’t already (4 questions on the first page only)
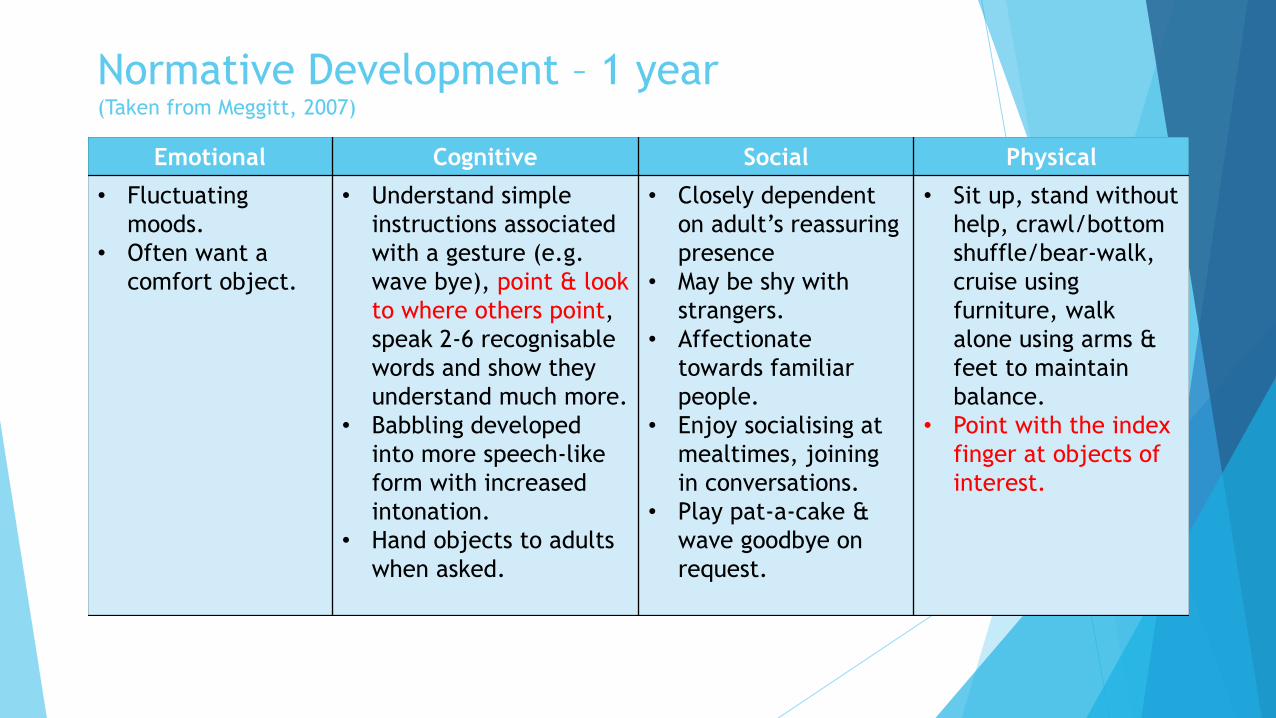
Normative Development – 1 year(Taken from Meggitt, 2007)
Emotional Cognitive Social Physical
• Fluctuating
moods.
• Often want a
comfort object.
• Understand simple
instructions associated
with a gesture (e.g.
wave bye), point & look
to where others point,
speak 2-6 recognisable
words and show they
understand much more.
• Babbling developed
into more speech-like
form with increased
intonation.
• Hand objects to adults
when asked.
• Closely dependent
on adult’s reassuring
presence
• May be shy with
strangers.
• Affectionate
towards familiar
people.
• Enjoy socialising at
mealtimes, joining
in conversations.
• Play pat-a-cake &
wave goodbye on
request.
• Sit up, stand without
help, crawl/bottom
shuffle/bear-walk,
cruise using
furniture, walk
alone using arms &
feet to maintain
balance.
• Point with the index
finger at objects of
interest.

Normative Development – 2 years
Emotional Cognitive Social Physical
• Beginning to express
how they feel.
• Impulsive & curious
about their
environment.
• May be clingy &
dependant at times
& self reliant &
independent at
others.
• Often feel frustrated
when unable to
express themselves
(half 2yr olds have
tantrums almost
every day).
• Now speak over 200
words.
• Still repeat words
spoken to them
(echolalia).
• May omit opening or
closing consonants
‘us for ‘bus’.
• Follow simple
instructions and
requests (e.g. please
bring me the book).
• Recognise familiar
people in photos .
• Listen to general
conversation with
interest.
• Provide comfort
when other babies
cry.
• Want to share songs,
conversation,
rhymes and more.
• Can run safely
avoiding obstacles.
• Draw circles, lines &
dots .
• Enjoy picture books.
• Can copy a vertical
line & a ‘v’ shape.
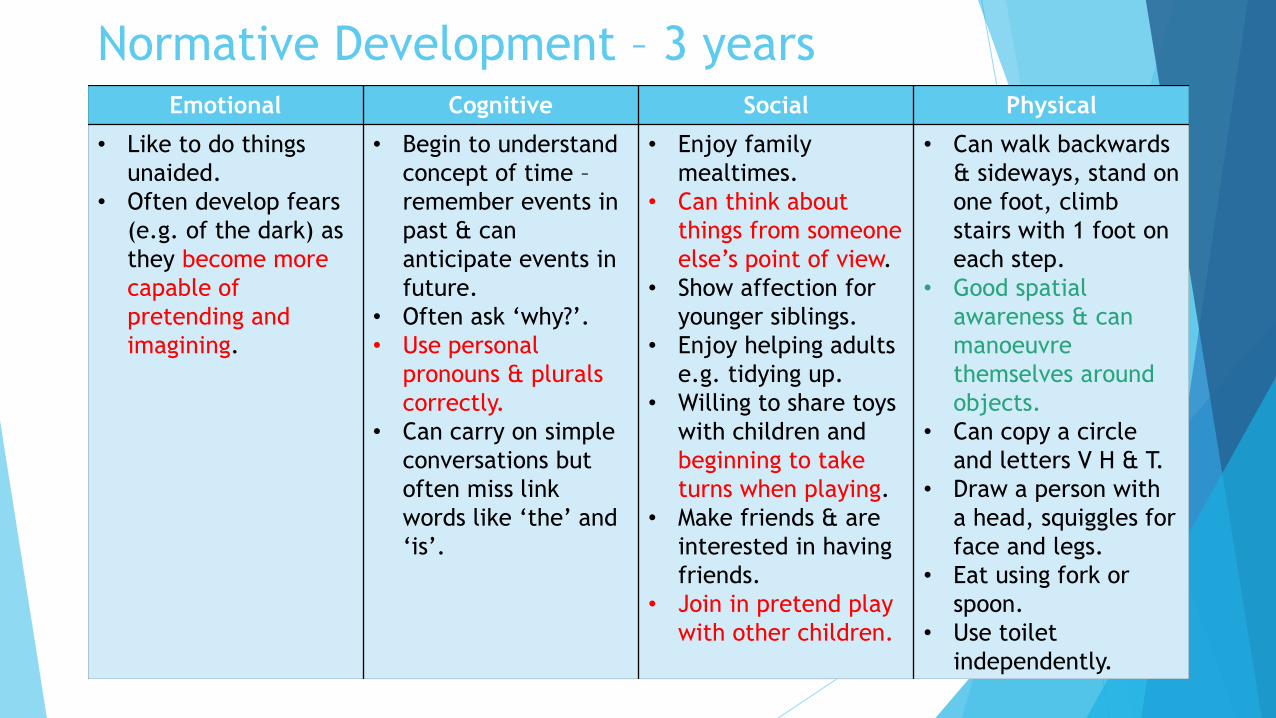
Normative Development – 3 yearsEmotional Cognitive Social Physical
• Like to do things
unaided.
• Often develop fears
(e.g. of the dark) as
they become more
capable of
pretending and
imagining.
• Begin to understand
concept of time –
remember events in
past & can
anticipate events in
future.
• Often ask ‘why?’.
• Use personal
pronouns & plurals
correctly.
• Can carry on simple
conversations but
often miss link
words like ‘the’ and
‘is’.
• Enjoy family
mealtimes.
• Can think about
things from someone
else’s point of view.
• Show affection for
younger siblings.
• Enjoy helping adults
e.g. tidying up.
• Willing to share toys
with children and
beginning to take
turns when playing.
• Make friends & are
interested in having
friends.
• Join in pretend play
with other children.
• Can walk backwards
& sideways, stand on
one foot, climb
stairs with 1 foot on
each step.
• Good spatial
awareness & can
manoeuvre
themselves around
objects.
• Can copy a circle
and letters V H & T.
• Draw a person with
a head, squiggles for
face and legs.
• Eat using fork or
spoon.
• Use toilet
independently.

Normative Development – 5 yearsEmotional Cognitive Social Physical
• Definite likes &
dislikes.
• Dress & undress
alone.
• Ask about abstract
words (e.g. what does
beyond mean).
• Recognise their name
& attempt to write it.
• Talk about past,
present & future &
have a good sense of
time.
• Fluent in speech &
mostly grammatically
correct.
• Love to be read
stories & then act
them out later alone
or with friends.
• Enjoys jokes &
riddles.
• Show sympathy &
comfort friends who are
hurt.
• Choose their own friends
• Understand social rules
(e.g how to greet
someone).
• Instinctively help other
children when they are
distressed.
• Enjoy team games.
• Play complicated games
with miniature objects
(small world play).
• Enjoy elaborate pretend
play with others.
• Play alone or with
others.
• Increased agility,
can run, climb,
dodge and skip.
• Good balance &
coordination.
• Can use a knife &
fork competently.
• Can draw a person
with a head, body,
arms, legs, nose,
mouth & eyes.
• Can do jigsaw
puzzles with
interlocking pieces.

Normative Development – 7 yearsEmotional Cognitive Social Physical
• Learn how to
control their
emotions.
• Realise that
they can keep
their own
thoughts private
& hide their
true feelings.
• Begin to think in
terms of who
they are but
also who they
would like to
be.
• Express
themselves in
speech &
writing.
• Perform simple
calculations in
their head.
• Begin to
understand how
to tell the time.
• Are able to
arrive at logical
conclusions & to
understand
cause & effect.
• May be able to speak
up for themselves
(e.g. when visiting
dentist).
• Form close
friendships, mostly
with their own sex.
• Engage in complex
cooperative play,
using more people,
props and ideas.
• Have a clear sense of
right & wrong –
realise it is wrong to
hurt other people
physically.
• Can ride a 2
wheeled bike or use
roller skates.
• Increased stamina,
swimming, skating,
gymnastics.
• Skilful in catching &
throwing ball using
one hand.
• Able to control their
speed when running
& can swerve to
avoid collision.

Autism Spectrum Disorder (ASD):
• Autism is a lifelong developmental disability that affects social and
communication skills. People with an ASD may find it difficult to understand
how the world and people around them operate and find it hard to interact.
“Reality to an autistic person is a confusing mass of events, people, places,
sounds and sights. There seems to be no clear boundaries, order or meaning to
anything. A large part of my life is spent trying to work out the pattern behind
everything.” (a person with autism)

ASD - The triad of impairment
(Lorna Wing)
Sensory-
Motor
Processing
Difficulties

Causes of Autism:
Genetic:
Researchers at Autism Research Centre in Cambridge have identified a group of 8-15 genes thought to be responsible for autism
Autism is known to run in families – 1 in 20 chance of a sibling also being diagnosed if one child in the family already has the condition
Environmental Factors:
Possible triggers include being born before 35 weeks of pregnancy but no conclusive evidence has been found
Other health conditions: (associated with ASD)
Infantile Spasms
Other rare genetic conditions such as Fragile X, Retts Syndrome or Tuberous Sclerosis
Misconceptions about the causes of ASD:
The MMR vaccine
The way a person has been brought up
Diets such as eating wheat or dairy products

http://www.nhs.uk/Conditions/Autistic-spectrum-disorder/Pages/Causes.aspx
https://www.theguardian.com/society/2017/jul/08/david-mitchell-son-autism-
diagnosis-advice
Early signs of ASD
Social interaction difficulties:
Poor turn taking skills / not able to share
Lack of reciprocity in their social relationships – difficulty in building a to and fro conversation
Limited use of language
Few if any relationship repairing skills
Exceptional knowledge around their areas of interest – will talk excessively about this if given the
chance
Not interested in their partners point of view or interests
Appear aloof/less interested in others (making it more difficult for them to develop friendships)
May experience difficulty in relating to others
May try to initiate social contact but not understand ‘social rules’.
Social interaction Clip from Kennedy Krieger Institute (04:24-05:58)
https://www.youtube.com/watch?v=YtvP5A5OHpU
Early signs of ASD
Communication difficulties:
Use of gestures are limited
Stiff/awkward body posture
“unstreetwise” presentation
Poor quality of rapport
Poor eye contact or has a staring quality
Comprehension difficulties
Can make abrupt and/or insensitive comments
Narrow range of conversational topics
Difficulty in conveying feelings
Speech abnormalities, includes:
Language development delay (some but not all cases)
Overly formal and stilted language, but with poor comprehension
Difficulties with specific concepts such as time words, emotions
Misinterpretation of implied meaning – eg, sarcasm, not be able to inference

Early signs of ASD
Communication difficulties:
Better in 1:1 but unable to manage group situations
Volume, rate of speech (prosidy) – may talk with a squeaky voice, not be able to
moderate volume, talk too fast etc.
Poor communication style – may either not join in or cut across topic of
conversation
Limited use of language

Communication
Clip from Kennedy Krieger Institute (05.59-07:57)
https://www.youtube.com/watch?v=YtvP5A5OHpU

Early signs of ASD
Imagination and flexibility:
Find abstract thinking difficult – eg. Concepts about God/death
Have a limited range of imaginative activities
Not initiating or joining in with pretend play
Focus on minutiae/detail rather than the bigger picture – eg. Wheels on a car
Pursue activities in a rigid and repetitive way
Hand flapping/spinning/rocking
Develop an obsessive interest in a specific interest –eg. Timetables, dinosaurs, spiders
Early signs of ASD
Imagination & flexibility:
Have difficulty separating fact from fiction
Not realise that other people have their own thoughts/feelings and agendas
which may differ from their own.
Find it difficult to accept another’s point of view (poor theory of mind)
Rigidity in thought and/or behaviour – have to do things in a particular way
Lack the ability to generate new ideas spontaneously or decide which actions to
carry out.

Early signs of ASDSensory:
Many people with autism have sensory processing difficulties that lead them to under or over respond to sensory stimuli in their environment.
Hypo (under-stimulated) hyper (over-stimulated)
7 senses
Vestibular / movement - Situated in inner ear - provides information about where our body is in space and its speed, direction and movement.
Proprioception / body awareness - Situated in muscles and joints - provides information about our body position.
Auditory / hearing - Situated in the inner ear – tells us about sounds and noises in our environment. Important for speech and language.
Vision / sight - Situated in the retina of the eye – sight helps us to define objects, people, colours, contrasts and spatial boundaries.
Olfactory / smell - Situated in the nose - most primitive sense and the first sense we rely upon.
Gustatory / taste - Receptors positioned on the tongue – tells us about different tastes – sweet, sour, bitter, salty and spicy.
Touch - Situated in the skin. Assists us to relate to touch, pressure, pain and temperature (hot and cold)
Sensory difficulties - clips
Clip: Can you make it to the end (NAS video) – http://www.autism.org.uk/get-
involved/tmi/about.aspx
Clip: Make it stop (NAS video) - http://www.autism.org.uk/get-involved/tmi/film.aspx
Clip: How many questions can you answer (NAS video) - http://www.autism.org.uk/get-
involved/tmi/take%20the%20test.aspx
ASD NICE guidance (2011)
Prevalence about 1% of children
Intellectual disability occurs in approximately 50% of young people with
autism.
Approximately 70% of people with ASD also meet diagnostic criteria for at least
one other (often unrecognised) psychiatric disorder, e.g. Anxiety disorder,
depression, OCD.
Core ASD behaviours typically present in early childhood but features are not
always apparent until circumstances of the child change.
Children & young people with certain coexisting conditions (such as
intellectual disability) are less likely to be diagnosed with ASD.

Autism in girls – what to look out for…….Social Interaction:
Girls tend to be more socially motivated to be socially interactive but their friendships may be characterised by an inability to maintain friendships
They may appear excessively shy, avoid interacting with others or making the first move socially.
They can gravitate towards older or younger girls.
May seem uncomfortable during conversation – poor eye contact, lack of social understanding of rules or will want to dominate conversation around their chosen themes.
May only have one close friend. If she has more than one, she may either be on the periphery of their group or will want to lead the group and play.
May play appropriately with toys and engage in pretend/imaginative play with others.
Can show empathy and compassion (be caring) but may be confused by non-verbal signals from others.
May have difficulty fitting in with peers due to clothing and hairstyle choices.
Girls commonly get described as ‘shy’.
They can often create an elaborate fantasy world.
They may be seen as imaginative, but their play, like boys is often repetitive with the same narrative running through.
Social Communication:
She may have an exceptional vocabulary.
Girls are better at masking their symptoms – they will mimic (without understanding) or watch and copy what other girls do. They may not initiate social contact but can ‘go through the motions’ of how they are expected to behave.
Consequently, they may converse in predictable and ‘scripted’ ways.
They can struggle with non-verbal aspects of communication such as body-language and tone of voice.
They may have difficulty dealing with unexpected verbal responses.
Social Imagination:
Parents may perceive their daughter as ‘odd’ but not be able to put their finger on the difference.
Imaginative play does exist, but it is intense in nature, often focused on stereotypical female interests, such as dolls, make-up, animals and celebrities – which is why girls with ASD may not seem that different to females not on the spectrum.
The key is the intensity and quality of these special interests, which are exclusive, all-consuming and experienced in detail
Often have difficulties in moving on from their toys/clothes from when they were younger.
May play with dolls or toys well beyond the typical age for these items.
Behavioural Symptoms:
They are often less disruptive than boys
Girls can develop friendships, but moving into adolescence, the differences between
neurotypical girls and ASD girls becomes greater which may lead to higher rates of
anxiety and/or depression.
http://autism.lovetoknow.com/Aspergers_in_Girls (this has an embedded
video on ‘aspergirls’
https://spectrumnews.org/features/deep-dive/the-lost-girls/
http://www.autisminpink.net/ also has embedded video better than the
other one as made by NAS
https://everydayaspie.wordpress.com/2016/05/02/females-with-aspergers-
syndrome-checklist-by-samantha-craft/amp/

What is Pathological Demand Avoidance?From: Pathological Demand Avoidance Syndrome – www.pdasociety.org.uk
Understanding Pathological Demand Avoidance Syndrome in Children (2012). Christie, P., Duncan, M., Fidler, R. & Healy, Z.
PDA is not a recognised diagnostic label, nor is it likely to become one in the near future.
CAMHS is only able to ascribe diagnoses to children using the ICD 10 manual soon to be ICD 11.
Although we may see PDA type behaviours, these will be understood as part of the autism spectrum.
Avoidance of and resistance to, the demands of everyday life – ie. demand avoidance. These can range from direct and explicit instructions to the more subtle demands of everyday life.
Any suggestion put to a child can be perceived as a demand.
Underpinning the avoidance is extremely levels of anxiety about conforming to social demands and a strong need for them to be in control, which in turn further heightens their anxiety.
Avoidance can be at all costs: tantrums/meltdowns, panic attacks.
Children with PDA have better social communication skills than others on the spectrum.
They often use these skills to try to avoid demands through negotiation, manipulation or distraction. (Manipulation is used because children with PDA are successful in avoiding demands because they have sufficient social empathy to do so.)
There is surface sociability, but apparent lack of a sense of social identity, pride or shame.
They will present with lability in mood and as impulsive and led by the need to control.
They will be comfortable in role-playing.
Large majority of children with PDA will have some speech and language delay.
Obsessive behaviour, similar to that seen in children with autism.

What might teachers see in the classroom
with PDA? Need to be in control
Explosive behaviour
‘slipping under the radar’ – create an act of ‘doing’/’busy doing nothing’
Threatening language
Poor sense of self-esteem
Expressed desire to be equal or better than
Desiring friendships but inadvertently sabotaging them
Ambivalent about success and enjoyment
Lack of permanence and transfer of learning and experience
Very poor emotional regulation
Variability in behaviour
Extensive involvement in fantasy and role play

How to help with PDA…….
First thing to remember is every interaction, or exchange is a transactional
(two way) process. The adult has to consider their contribution, from which
solutions are possible.
The child ‘can’t help won’t’: the child can’t help the fact that s/he won’t do
it, on this occasion.
Expectations and ground rules: compromise, prioritising, flexibility and
negotiation should be at the core.
Avoid being directive – use invitations or suggestions such as ‘I wonder how
we might….’ or ‘I can’t quite see how to do….’.
Keep calm in the face of disruptive or challenging behaviours. Do not take it
personally.
Be flexible and adaptable: strategies are likely to need changing more
frequently than for a child with autism.

How to help with PDA continued…..
Structured teaching and visual support.
Building on a child’s strengths and interests as learning opportunities.
Using drama and role play.
Monitoring and adjusting use of language – for example, allowing sufficient
time to process information.
Depersonalising demands and requests. Eg. If they are on the computer, use
an electronic timer which plays a pre-recorded message to indicate ‘game
over’.
Consider the learning environment: visual support materials, noise levels,
visual distractions, lighting, given the child space and clearly defined areas.

ASD Vs Attachment difficulties
Heather Moran – the Coventry grid:
Clip of Heather Moran talking about ASD & attachment -http://network.autism.org.uk/knowledge/insight-opinion/interview-
heather-moran
To access the Coventry grid -http://drawingtheidealself.co.uk/drawingtheidealself/Downloads_fil
es/Coventry%20Grid%20Version%202%20-%20Jan%202015.pdf

ASD Classroom Recommendations:
Support to develop social skills through social skills group/nurture
group/social stories.
Child with ASD often learn and respond to information that is presented to
him or her in a visual format. All verbal information should be supported by
visual cues/prompts/slides.
To avoid literal interpretation of language, verbal instructions in class
should be short, specific and clear.
Whole-class instructions may need to be repeated to the individual to
ensure they have understood
Small group work may need to be supported to encourage success and feel
that they are a valuable member of the class.
Give advanced warnings of any change to the usual routine of the class.
Social stories can help with this.
Contact the SENSS team/EP for further support and interventions.

In pairs or small groups…(5 mins)
Have a think about whether you recognise any of these early signs of ASD in
children you have previously worked with?
What might help you keep these early signs in mind for the year ahead?


Attention Deficit Hyperactivity Disorder
(ADHD): ADHD is a combination of overactive, poorly modulated behaviour
with marked inattention and lack of persistent task involvement.
These behaviours must be pervasive across situations and persistentover time and at higher levels than what is expected in a child of the same chronological age (ICD 10).
ADHD is a developmental disorder and there should be a history of symptoms in childhood.
Concentration and attention difficulties can also arise for other reasons (e.g. emotional difficulties, high anxiety level) and may be linked to recent life events (such as parental separation, frequent moving). In this case, difficulties may be more transient and parents may not report historical difficulties with attention and concentration.

Causes of ADHD:
Genetics
ADHD tends to run in families.
Strong genetic factors – parents and siblings of a child with ADHD are 4 to 5 times likely to have ADHD, but the way it is inherited is likely to be complex and not due to a single gene
Brain Function and structure
Research has identified a number of possible differences in the brains of people with ADHD including differences in the frontal lobe (responsible for decision making and moral judgements) and an imbalance in some of the neurotransmitters or chemical which help the brain to work properly
Other possible causes:
Being born premature (before 37 weeks) and having a low birthweight
Brain damage either whilst in the womb or in the first few years of life
Drinking alcohol/mis-using drugs and smoking

3 subtypes of ADHD:
1. Inattentive subtype
2. Impulsive / hyperactive subtype
3. Combined subtype
What is ADHD?
Clip: (7:42 mins)
https://www.youtube.com/watch?v=0Wz7LdLFJVM
Core features of ADHD:
Attention Problems
Impulsivity
Hyperactivity
Early signs of ADHD:
Attentional Problems:
Avoids tasks that require sustained mental effort.
Inattention and distractibility (by self or environment).
Difficulties in sustaining attention (unless supervised) and not listening.
Difficulties in organising and following instructions and completing tasks.
Fails to closely attend to work and makes careless mistakes.
Losing things and forgetfulness.
Impulsivity:
Difficulties in waiting their turn.
Blurting out answers before questions are completed.
Interrupting conversations or games.
Doesn’t learn from mistakes.
Poor judgement in self-awareness and therefore fails to anticipate situations.
Poor sense of road safety/danger.
Early signs of ADHD:
Hyperactivity:
Fidgety
Runs about or climbs excessively/inappropriately.
Always on the go.
Trouble staying seated.
Talks incessantly.
Inappropriately noisy/boisterous.
ADHD NICE guidance (2016)
Based on narrower criteria of ICD-10, hyperkinetic disorder is estimated to
occur in 1-2% of children & young people in the UK.
Based on broader criteria of DSM-IV, ADHD is thought to affect 3-9% of school
aged children & young people in the UK (NICE, 2016).
Common co-existing conditions in children with ADHD are disorders of mood,
conduct, learning, motor-control and communication and anxiety disorders
(NICE, 2016).
What’s it like to have ADHD?
Clip: https://www.youtube.com/watch?v=Hl7Ro1PUJmE&feature=youtu.be
(2 min 15 secs)
Children’s descriptions of how ADHD affects them
What might the teachers see in the
classroom? Primary Schools
Children with ADHD may:
Struggle with continuing with tasks such as writing or colouring for very long
Move from one activity to the other without finishing anything
Not enjoy playing with toys or games and prefer active games
Appear not to hear you when you speak to them and may forget when you have asked
them to do something
Fidget constantly, make noises and talk all the time
Be easily distracted by others
Be impulsive and prone to accidents
Hate to wait and will do anything to avoid being bored
Interrupt when people are talking and struggle to wait for their turn in class

What might the teachers see in the
classroom? High Schools
Children with ADHD may:
Be less physically active and fidgety but still struggle to concentrate for
extended periods – internal restlessness

Classroom Recommendations for ADHD: Write out the most important 3-5 class rules for the child on his/her desk.
Ensure instructions are broken down and repeated and that instructions have been understood.
Highlight any key words needed to focus on in the work.
Break work into manageable chunks. Eg. First 3 questions then seek further instructions from the teacher or TA.
Alternatively, ask the child to complete his/her work for timed chunks, eg. 10 minutes and then come and seek help. Try different timers to see if this makes a difference.
Try giving the child a specific number of lines to write into – use a highlighter to mark out the number of lines.
To reduce calling out, encourage the child to count to 5 in his head first.
Children with ADHD often manage best if they are sat at the front, faced forward with little visual distractions around their table.
Use a range of fidget toys to see if this helps – change fidget toys regularly.
Allow the child to stand up to write if that enables him/her to keep to task.
Use visual aids to support learning – colour coded boxes for planning of tasks or spidergrams to get their ideas down on paper.
Try and give immediate feedback on behaviour whether positive or negative.
Try not to remove lunch play as this is likely to impact behaviour in the afternoon.
Reading – if a problem can be encouraged by alternating being read to and reading to the child.
Use a ruler to highlight sentences that need to be read.

In pairs or small groups…(5 mins)
Have a think about whether you recognise any of these signs of ADHD in
children you have previously worked with?
What would you do if you thought a child was showing signs of ASD or ADHD?

Behavioural Difficulties High number of children referred for support with behavioural difficulties
show significant indicators of a neurodevelopmental condition that warrant
specialist assessment.
42 % of children open to Clinical Psychology in the Primary Behaviour Service
referred for further assessment of ASD / ADHD (Sept 15–July 16)
If the main difficulty is ‘behaviour’, consider asking for more information

Parenting intervention
If you are seeing a child that is demonstrating behavioural difficulties or early signs of a neurodevelopmental condition…consider referring them for a parenting intervention.
Regardless of the underlying reason for the difficulties, parenting groups provide a useful space to support parents with:
Improving positive interactions with their child
Understanding their child’s behaviour
Using praise and rewards
Behaviour management and discipline strategies
Understanding the importance of consistency
Understanding the importance of their own self care
This is likely to be a helpful intervention for parents and children regardless of the underlying reason for the difficulties.
If you think a parent may struggle to access a group, there may be more individualised support available

“I don’t need to go to a parenting group!”
Well begun is half done!
Think about how you approach a parent and don’t ask them
to ‘go to a parenting group’
Talk to them about the things they are struggling with and
explain how things in the group might be beneficial to them
Say it’s a group for parents or use some other name but try
to avoid saying ‘parenting group’ or ‘parenting class’ as it
can evoke ideas about being seen a bad or useless parent.
Normalise their experience – all parents struggle, there’s no
guidebook and no one gets it right all the time. Emphasise
the group is about pooling resources & parents sharing ideas
Say its about taking time out to be able to see clearer and
make a plan rather than make it up on the spot when
adrenaline is flowing.

What to do if you think a child may have
a neurodevelopmental condition:
Discuss with your manager/supervisor/SENCO
Hypothesising – it could be a neurodevelopmental condition but lets get more information
How severe are the difficulties?
How long have they been present?
How pervasive are the difficulties? Are they across contexts?
ADHD – 2 or more important settings
But why might parents report no difficulties at home?
What else could it be?
Consider factors that are associated with an increased prevalence of ASD and ADHD - e.g. for ASD -
sibling with ASD, intellectual disability, gestational age less than 35 weeks etc (see NICE, 2011)
Try strategies to see if they make a difference
Consider watchful waiting for up to 10 weeks if concerns about ADHD (NICE, 2016)

If you still think it may be a
neurodevelopmental condition…
Refer for parenting intervention
Parent-training/education programmes are usually the first-line treatment for
parents and carers of pre-school children and children and young people of school
age with ADHD and moderate impairment (NICE, 2016)
Discuss with member of ASD / ADHD assessment team (NDS or CDT)
Referral to agencies for further assessment
EP
OT – sensory needs / SLT
CDT – ASD assessment IF child is 0-6 years old but no ADHD assessments for under 7’s
NDS – ASD assessment IF child is 6+ years old & ADHD assessments

Discussing the referral with the parent and
getting consent
Discuss your concerns in terms of strengths and weaknesses
“So we have talked about how X is really good at maths and
completing tasks by himself and we have talked about some
of the things he seems to find more difficult, like
communicating with others, socialising with peers and talked
about how he can get quite stuck doing activities he likes
and seems to find it difficult to think flexibly. This pattern of
strengths and difficulties could be indicative of social
communication difficulties or an autism spectrum disorder.
Have you heard of social communication difficulties or
autism spectrum disorder before? What do you know about it
already? What do you think? Have you thought about this?”

Discussing the referral with the parent
and getting consent
Don’t be afraid to say ‘autism spectrum disorder’ – the parent may get a
shock when they go to the first CAMHS appointment if they do not know this is
what the assessment appointment is for. Clarify any confusion and talk about
it being a spectrum.
It may be helpful to explain that you are NOT giving a diagnosis of ASD/ADHD
but you think it might be helpful to have this further assessed by the
specialist team.
Explain what will happen on referral to the ASD/ADHD assessment team if
they are referred.
Key information to include with the referral to NDS ASD:
Parental Consent.
Descriptions of behaviours that you have seen within the ‘Triad of Impairment’, social communication/interaction; communication (verbal and non-verbal); flexibility of thought and behaviour.
What has been done so far to support the young person’s learning?
Have any other professionals been involved in the young person’s care/education?
ADHD:
NB. NICE guidelines for ADHD recommend a period of watchful waiting by the GP as well as parents attending a recognised parenting programme before referral to CAMHS Tier 3.
Parental Consent.
Descriptions of behaviours that you have seen regarding hyperactivity; impulsivity; inattention.
What has been done so far to support the young person’s learning?
What other professionals have been involved and in what capacity?
The better the information you provide, the more likely the referral will be accepted!

Waiting for the assessment…
NDS referrals are not subject to the 18 week deadline
Children can wait 12 + months for the assessment to be completed
Continue to involve relevant services and put things in place for the child
or young person while waiting for the assessment to be finished. Try
strategies!
Do not wait for this assessment to be finalised before applying for an
Education Health Care (EHC) plan – describe the needs and difficulties you
are seeing when applying.
If you are concerned about the child or young persons mental health or feel
they are at risk while they are on the waiting list, contact the service you
referred them to and discuss your concerns.
What will happen if the child is referred
to CDT or NDS?
The child and parent may be invited in for several appointments.
The assessment may involve:
Talking to the parent to get a developmental history for the child and a good
understanding of their early history
Doing a play based assessment with the child
A group observation (a clinician observing the child interact with other children all
invited in to the clinic)
An observation of the child in their school
Asking the parent and child’s school to complete some questionnaires
Discussion with other agencies already involved in supporting the child

What CAMHS teams offer……
Tier 2 includes CAMHS staff based in:
SAFE
PBS
CLiPS
CAMHS-LD
MAST
Parenting
LAC
Connect
Tier 3 includes:
FYPS – Family & Young Person’s Service - 0-13 years
NDS – Neurodevelopmental Service - 6-18 years
PLS – Paediatric Liaison Service - 0-16 years
ACS – Adolescent Community Service - 14-18 years
EDT – Eating Disorders Team – any age
Ealing CAMHS consists of two levels of service delivery: Tier 2 and Tier 3
Tiers are distinguished by the level of severity of presenting problem. For example, low
mood would be referred to SAFE teams, whereas a child who is low in mood and expressing
consistent desire to end their life or who have tried to commit suicide would be Tier 3.
What problems do the T3 teams see….?
Depression with severe indicators
Self Harm – suicide attempt, suicidal ideation, repeated self-harm
Eating Disorders – rapid and sustained weight loss, anorexic behaviour, bulimic patterns
Anxiety Disorders – Significant anxiety, especially OCD and severe phobias
ADHD – Assessment and treatment for ADHD
Behaviour Problems – only as part of another condition
Anger Problems – only as part of another condition
Sleep Problems – only as part of a complex picture or as part of other problems
Low self-esteem – not as the only reason for referral, but part of another problem
Substance Misuse – young people are referred to EASY Project
Enuresis / Encopresis – Not as the only reason for referral
Bereavement, loss and trauma – for pathological grief reactions; PTSD
Divorce and Separation – not unless there is clear evidence of a specified mental health problem
School-based problems – not unless there is clear evidence of a specified mental health problem
Severe Learning Difficulties – usually seen by CAMHS-LD but by NDS if they are in mainstream education
School refusal – not unless there is evidence of or need for an assessment for a mental health problem
Psychosis – Assessment and treatment of all psychotic disorders
Autism Spectrum Disorder – Assessment of children with normal language and intellectual development for ASD including concerns of co-morbid mental health problems

What to expect from services
In CAMHS, children or young people with significant mental health needs are
prioritised; this will be the same for children on the waiting list. If a child or
young person has been diagnosed with ASD or ADHD and doesn’t have
significant mental health needs they can be supported by relevant community
services.
There isn’t a designated service for children or young people who have been
given a diagnosis of ASD or ADHD without significant mental health
difficulties.
Dawn Clegg can provide teaching / training to schools about ASD
Don’t forget about voluntary services:
National Autistic Society (NAS)
National Attention Deficit Disorder Information and Support Service (ADDISS)
Family Lives
Post- investigation – what to expect
The child’s needs will still be the same
A diagnosis may help people understand the child or young persons needs.
This is not necessarily the case and people may still need support to
understand these needs: PDD-NOS
Groups (ASD/ADHD parenting group, parenting groups for conduct disorder)
Drug treatment?
Not recommended for children under the age of 7 years with ADHD
Can be tried for school age children with ADHD with moderate impairment after
parent training and psychological therapies (CBT, social skills training) or those
with severe symptoms
Contact details to discuss referrals
Neurodevelopmental Service (NDS) –
Ealing CAMHS,
1 Armstrong Way
Southall
Middx UB2 4SD
T: 020 8354 8160
Child Development Team (CDT) –
Carmelita House
21-22 The Mall
Ealing
London W5 2PJ
T: 020 8825 8712

Parenting pilot – Sept 2017 – Sept 2018
Your school will be participating in the Ealing-wide Primary School Project to pilot a new type of parent/education programme that is more focused on behavioural issues
Empowering Parents Empowering Communities (EPEC) is an innovative, low cost method of working with communities to ensure that they get effective, evidence based early parenting intervention. It is a collaboration between South London and Maudsley NHS Foundation Trust, Kings College London, Ealing Council and Ealing Clinical Commissioning Group
Two members of your staff at the school will be undertaking the training this term to run a parenting group in both the Spring and Summer Terms. They will be supported by a local Health Care Professional assigned to your school
If you are seeing a child that is demonstrating behavioural difficulties or early signs of a neurodevelopmental condition…consider referring them for a parenting intervention within your school
This is likely to be a helpful intervention for parents and children regardless of the underlying reason for the difficulties
Participating primary schools:
Viking, Selbourne, Hanbrough, Stanhope, Gifford, Little Ealing, Berrymede Junior, John Perryn

Resources:
National Autistic Society: www.nas.org.uk
The Attention Deficit Disorder Information and Support Service (ADDISS):
www.addiss.co.uk

References:
Autism spectrum disorder in under 19s: recognition, referral and diagnosis,
NICE, 2011.
Attention deficit hyperactivity disorder: diagnosis and management, NICE
2008, updated 2016.
Child Development - An illustrated guide – Carolyn Meggit (2007)
Step by step help for children with ADHD – A self-help manual for parents –
Cathy Laver_Bradbury, Margaret Thompson, Anne Weeks, David Daley &
Edmund J. S. Sonuga-Barke (2010).

Evaluation form
Please complete the remainder of the training evaluation form
Thank you!