early childhood tuberculosis
DESCRIPTION
This presentation is a case based discussion detailing the importance of a high index of suspicion for Tuberculosis based on clinical pictureTRANSCRIPT

Early
CHILDHOOD TUBERCULOSIS
Gopakumar Hariharan
Senior Registrar, NPICU
Royal Hobart Hospital,
Tasmania, Australia

Introduction
• Case scenario
• Mode of transmission
• Pathophysiology
• Investigations
• Treatment
• Complications

Case Scenario
• 3 months old
• Apnea and respiratory distress
• CXR- Miliary patttern suggestive of TB
• Mum- open case- cavitating lesion of lungs – AFB
positive
• Choroid Tubercles
• On ATT ; Managed in Adult ICU

Tuberculosis
• Chronic infection – Mycobacterium Tuberculosis
• Major public health problem
• Pulmonary and extrapulmonary

Russia, India, Southeast Asia, sub-
Saharan Africa, and parts of Latin America
( 95%)

Portal of entry for tuberculosis
• Inhalation of Tubercle bacilli in >95% (M.TB) – Reservoir( infected person)
• Ingestion of milk containing Bovine Tubercle bacilli (M. bovis)
• Contamination of superficial skin or mucous membrane lesion with tubercle bacilli
• Congenital infection when mother has lymphohematogenous spread during pregnancy ORtuberculous endometritis

Epidemiology
• Host Factors
• Age : all ages affected, congenital is rare
• Malnutrition : more susceptible
• Intercurrent infections : e.g. measles, whooping cough
• Environment : overcrowding, inadequate ventilation,
damp, insanitary and unhygienic conditions

Primary tuberculous infection
Primary Focus (Ghon’s focus)
• At the site of first implantation
• Usually single and Subpleural
• In most, - heals and disappears, or
- fibroses or calcifies.
Localized inflammatory Process

Primary complex
Primary Complex:
• Primary focus + Hilar lymphnodes + draining lymphatics ( Tuberculous lymphangitis)
• Complications arise more commonly from regional adenitis than from the primary focus
Progressive primary tuberculosis
• Apparently healed focus or nodes may contain viable
organisms for many years.
• During 1st 4-8 weeks, organisms are disseminated in the blood
stream directly or via lymphatic duct – involves multiple
organs
• Progression of TB depends on the age of the child, number of
tubercle bacilli, and host resistance ( HIV )

Complications of the primary
focus
1. Rupture of focus into pleural space causing serous effusion ( more than 5 years)
2. Rupture of focus into bronchus causing cavitation
3. Enlarged focus, sometimes laminated or “coin” shadow

Complications of regional nodes
1. Incomplete (ball-valve) bronchial obstruction, emphysema of middle & lower lobes
2. Complete bronchial obstruction, collapse of right lower lobe
3. Erosion of node into bronchus & segmental consolidation
4. Rupture of node into pericardium: tuberculouspericardial effusion

Bronchial complications
1. Stricture of bronchus at
site of erosion
2. Cylindrical bronchiectasis
in area of old collapse
3. Wedge shadow: contracture
& fibrosis of segmental
lesion
4. Linear scar of fibrosis
following segmental lesion
Endobronchial TB – wheeze
Fever, troublesome cough, dyspnea, wheezing and cyanosis

Symptoms
• Primary complex – mild fever, anorexia, weight
loss, decreased activity, cough
• Progressive primary complex – high grade fever,
cough.
• Expectoration and hemoptysis – usually associated
with cavity and ulceration of bronchus.
• Abnormal chest signs – decreased air entry,
dullness, creps

Miliary tuberculosis
• Most common within 1st 3 to 6 months after infection
• Due to heavy hematogenous spread of tubercle bacilli
• Onset: Insidious, with
Fever and weight loss
Palpable liver and/or spleen
Tachypnoea with normal chest findings

Miliary tuberculosis
• Hematogenous dissemination - progressive development of small lesions throughout the body, with tubercles in the
• lung, spleen, liver,
• bone marrow, heart, pancreas
• brain, choroid, skin
Radiologic diagnosis:
• “Snow storm” appearance (Multiple small lung nodules 1mm size and above in both lung fields).

Miliary TB
Millets- 1 to 3 mm

X ray
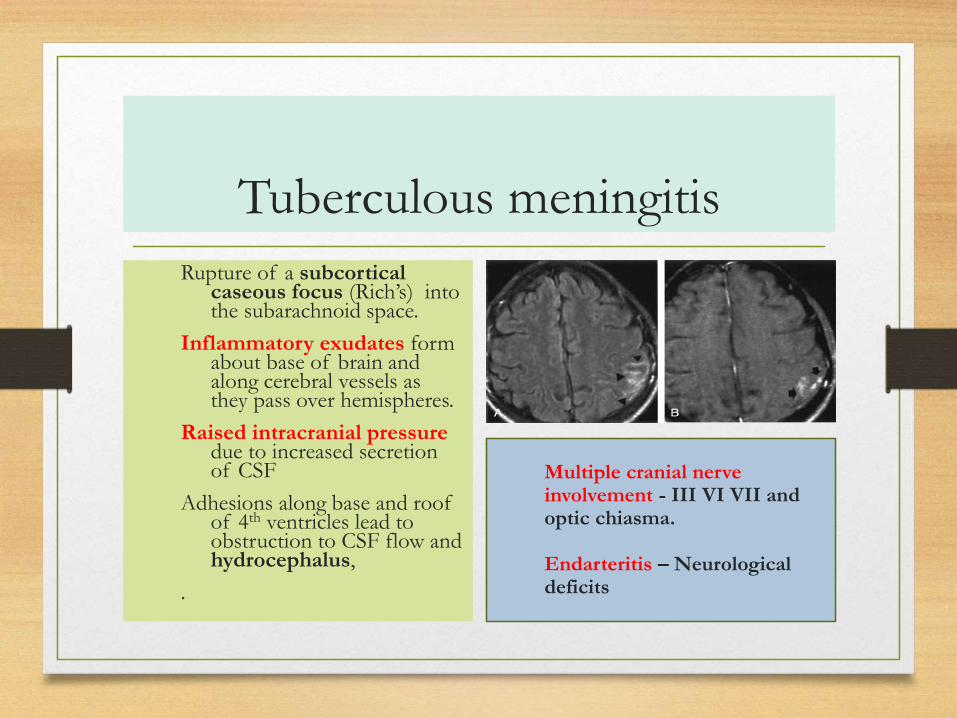
Tuberculous meningitis
Rupture of a subcortical caseous focus (Rich’s) into the subarachnoid space.
Inflammatory exudates form about base of brain and along cerebral vessels as they pass over hemispheres.
Raised intracranial pressure due to increased secretion of CSF
Adhesions along base and roof of 4th ventricles lead to obstruction to CSF flow and hydrocephalus,
.
Multiple cranial nerve involvement - III VI VII and optic chiasma.
Endarteritis – Neurological deficits

Diagnosis of TB meningitis
• Signs of meningeal irritation
• X-ray chest
• CT scan – basal exudates, inflammatory granulomas etc
• Tuberculin testing
• Retinoscopy for choroidal tubercles
• Lumbar puncture
Elevated CSF pressure(30 – 40cm h2o)
Cobweb Coagulum/ pellicle on standing
100 – 500 WBCs / cu.mm
>40 mg% protein
Low / Normal sugar
AFB smear & culture
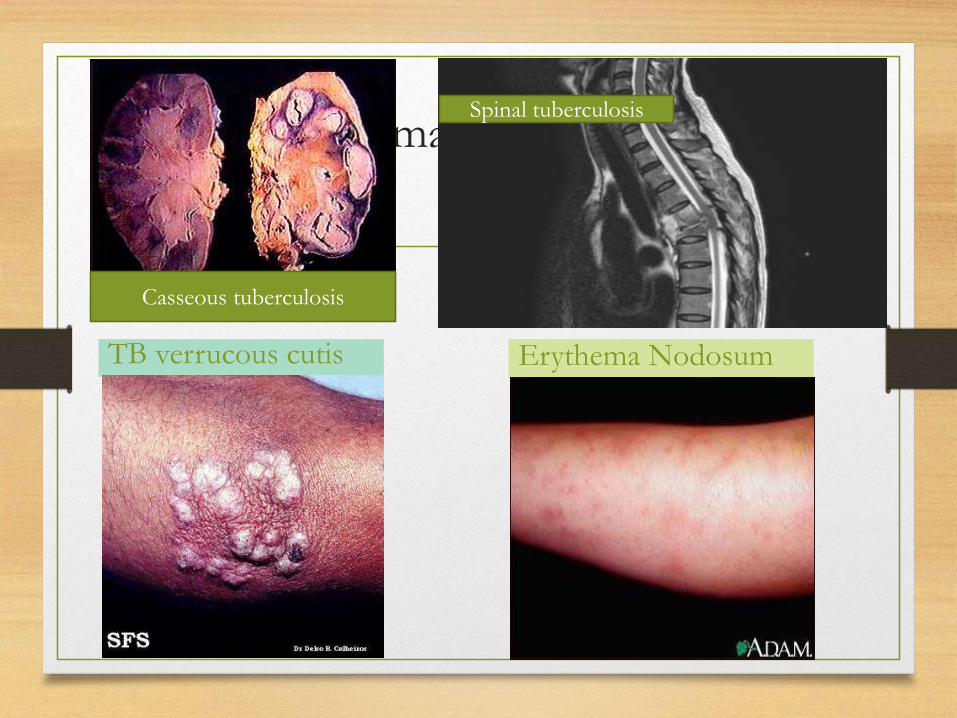
Skin manifestations
TB verrucous cutis Erythema Nodosum
Casseous tuberculosis
Spinal tuberculosis

)
Phlyctenular conjunctivitis
Cervicitis, salpingitis, infertility
Tuberculous otitis with multiple perforations
Scrofula

Choroid Tuberculosis
Tubercles of choroid (with
miliary TB)
Panophtalmitis
Exudative retinal detachment
Responds well to treatment

Wallgren A.The time table of Tuberculosis. Tubercle 1948;29:245-251

Direct tests for tuberculosis
• Ziehl-Neelsen staining for AFB in clinical specimens (sputum, gastric juice, biopsy)
• AFB culture on Lowenstein-Jensen solid medium (4 weeks)
• PCR amplification of targeted mycobacterial DNA sequences
• DNA probes: fluorescence in situhybridization assays

Other tests
• PCR – rapid results ( antigen/ antibodies)
• Serodiagnosis – ELISA
• QuantiFERON- TB test (QFT) – for diagnosing latent TB. Based on IFN-gamma released from sensitized lymphocytes.ELISPOT
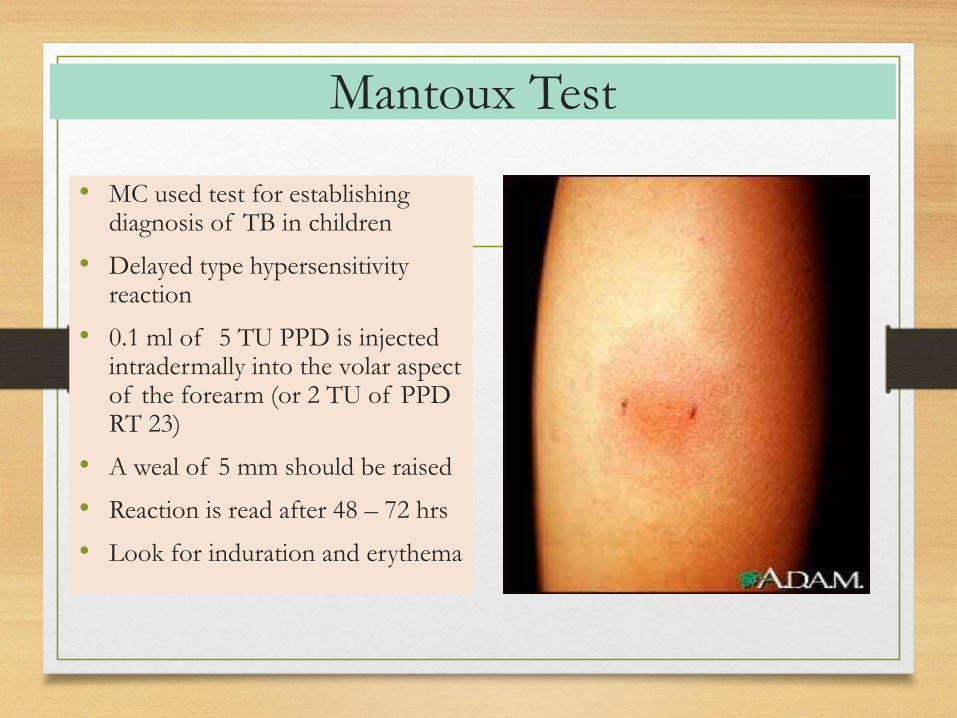
Mantoux Test
• MC used test for establishing diagnosis of TB in children
• Delayed type hypersensitivity reaction
• 0.1 ml of 5 TU PPD is injected intradermally into the volar aspect of the forearm (or 2 TU of PPD RT 23)
• A weal of 5 mm should be raised
• Reaction is read after 48 – 72 hrs
• Look for induration and erythema

Observation and Inference
• 48-72 hours later diameter of induration is measured
transversely to the long axis of the forearm.
• Induration > 10mm is suggestive of natural infection.
• 5-10 mm borderline; considered positive in
immunocompromised host
• <5mm Negative mantoux test does not rule out TB

False Negatives• Test done in incubation period of TB
• For several weeks following measles
• During Corticosteroid therapy
• Overwhelming TB infection (miliary, meningits)
• Severe Malnutrition
• If given Sub Cutaneous instead of Intra dermal
• Inactive Tuberculin

Guidelines for presumptive diagnosis of tuberculosis
Pediatr Infect Dis J 1993;12: 499-504)
A combination of at least 3 of the following:
• Symptoms/signs s/o TB: (fever > 1 mo., cough, weight loss)
• History of close contact with TB
• Positive tuberculin skin test (Mantoux > 10 mm)
• Sputum / gastric juice AFB +ve
• Lymph node / tissue biopsy positivity
• Radiologic features suggestive of TB
• Response to Anti TB Therapy
History of contact = any child who lives in a household with an adult taking ATT or has taken therapy in the past 2 years

Radiology
• In extra pulmonary TB , presence of lesions on chest radiograph supports diagnosis.
• Enlarged lymph nodes in hila, right paratracheal region
• Consolidation in progressive primary disease –heterogenous, poorly marginated with predilection to apical or posterior segments of upper lobe or superior segments of lower lobe.
• Bronchiectasis
• Pleural effusion
• Miliary TB

Treatment for TB
1st line anti-tuberculous drugs• Isoniazid H
• Rifampicin R
• Pyrazinamide Z
• Ethambutol E
• Streptomycin S

Phases of Treatment
• Intensive Phase
• Eliminate bacterial load
• Prevent emergence of drug resistant strains
• Atleast 3 Bactericidal Drugs used
• Continuation Phase
• Continue and complete therapy
• Atleast 2 Bactericidal drugs used
• Steroids
• Anti inflammatory effect – miliary, peritonitis, pericarditis
• TB meningitis

Management of Active TB
( NICE guidelines)
Progressive Pulmonary Tuberculosis and multiple LNE-
2 HRZE + 4 HR ( 6 month )
Meningeal TB
2 HRZE + 10 HR +Prednisolone /Dexamethasone
Prednisolone 1–2 mg/kg, maximum 40 mg with gradual withdrawal of the glucocorticoid considered, starting within 2–3 weeks of initiation


The 5 components of DOTS
Political & administrative commitment
Diagnosis by good quality sputum microscopy
Adequate supply of good quality drugs
Directly observed treatment
Systematic monitoring & Accountability

Prevention
Children with pulmonary TB disease are
rarely infectious due to
• Their pattern of disease,
• Low bacillary load and
• Lack of coughing force

Diagnosing latent TB
• Mantoux testing - household contacts (aged 5 years
and older) of all people with active TB and non-
household contacts (other close contacts for
example, in workplaces and schools).
• Consider Interferon-gamma testing - Mantoux
testing shows positive results, or in people for whom
Mantoux testing may be less reliable, for example
BCG-vaccinated people. ( high specificity)

Contacts – outbreak situation
• Active community surveillance
• Large numbers of people may need to be screened,
consider a single interferon-gamma test for people
aged 5 years and older.
• Preventive Therapy In Mantoux Positive : 6 HR

Healthcare workers
• Offer a Mantoux test to new employees who will be
in contact with patients or clinical materials if the
employees:
• Have not had BCG vaccination (for example, they
are without scar, other documentation or reliable
history).
• Mantoux test is positive, offer an interferon-gamma
test

BCG vaccination for
healthcare workers
• BCG vaccination should be offered to healthcare
workers, irrespective of age, who:
• are previously unvaccinated (that is, without adequate
documentation or a characteristic scar), and
• will have contact with patients or clinical
materials, and
• are Mantoux (or interferon-gamma) negative.

BCG vaccination for contacts
of people with active TB
• BCG vaccination should be offered to Mantoux-
negative contacts of people with respiratory TB if
they are previously unvaccinated and are:
• Aged 35 or younger
• aged 36 and older and a healthcare or laboratory
worker who has contact with patients or clinical
materials

Infection control
Three levels of isolation for infection control in
hospital settings:
• Negative-pressure rooms
• Single rooms - not negative pressure but are vented
to the outside of the building
• Beds on a ward

Isolation guidelines( NICE)
• Should be given a single room. Preferably not
admitted
• Visitors to a child with TB in hospital - screened
as part of contact tracing, and kept separate from
other patients until they have been excluded as the
source of infection
• Isolation for 2 weeks of treatment

Barrier nursing
Healthcare workers caring for people with TB should
not use masks, gowns or barrier nursing techniques
unless:
MDR TB is suspected
Aerosol-generating/ cough inducing(
bronchoscopy/sputum production) procedures are
being performed.
?Long term follow up
Regular follow-up clinic visits after treatment
completion were unnecessary.
Patients should be advised to watch for symptoms of
relapse and to contact the TB service rapidly if the
symptoms occur.

Multidrug resistant Tuberculosis
• A minority of cases, 6–8% in England and Wales, are
resistant to one of the antibiotics.
• Isoniazid and rifampicin are ineffective in 1% of
cases.
• These are said to be cases of multidrug-resistant
(MDR) TB, which requires special treatment and
careful monitoring.

Summary
• Pathophysiology of childhood Tuberculosis
• Various clinical manifestations
• Management
• Treatment
• Preventive measures
• Surveillance

“Nothing in life is to be feared, it is only to be
understood. Now is the time to understand more, so that
we may fear less.”
― Marie Curie