e-health: mis challenges and opportunities in healthcare
TRANSCRIPT

Montgomery County AITP – April 2002
eHealth: IT and the Reinvention of Healthcare
Elliot B. Sloane, Ph.D.
With special thanks to presentation materials provided by:
Ted CohenDirector of Clinical EngineeringUniversity of California Davis
Health System Sacramento CA, USA
AND CDR Maria C. Horton NC, USNChief Information Officer
National Naval Medical CenterBethesda, Maryland
Tonight’s Goals• Provide a glimpse of how medical devices are
morphing into IT-interfaced systems• Identify the key regulatory issues emerging
– FDA – Registration and GMP– HIPAA – Healthcare Insurance Portability and
Accountability Act• “Paint” a bit of the (near) future landscape that
integrates the web-enabled hospital technologies to deliver care directly to the patient, “wherever!”
• Understand the major advantages & challenges ahead!

BioBrief: Elliot SloaneDual CE/IT citizen!
• 27 Years of CE and IT/IS Expertise– Vice President, ECRI – 15 years, CIO & CTO
• Medical device research, testing, and education
– Vice President, MEDIQ/PRN – 10 Years, COO & CTO • Medical device & drug distr’n, service, and manufacturing
– Ass’t Professor of Information Systems, Villanova U. • Teaching, research and publishing in health informatics.
• Member and Officer, Montco AITP/DPMA since 1980• President, American College of Clinical Engineering

Terminology Biomedical vs. Clinical Engineering?
• Biomedical Engineering (BME) departments have existed for over three decades; some are now called Clinical Engineering Departments
• Biomedical Engineering has expanded into a broad research field– Nowadays, BME includes genetic engineering,
nanotechnology, etc.• Clinical Engineering: a more recent term
– Has been used to identify engineers and technicians who apply their efforts directly to medical devices in the clinical care settings. Typically help design/purchase, install, calibrate, maintain, and repair patient care devices.

“Classic” Medical Devices • Infusion Pumps – motorized pumps to infuse
blood or drugs into a patient at a precise rate• Patient monitors – detect and record heartbeat,
breathing, blood oxygen levels• Ventilators – mechanical devices that breathe for a
patient following trauma, surgery, or major illness• Incubator – provides precise heat, humidity, and
oxygen levels to distressed newborn babies• Implanted pacemakers – provide electrical pulses
to help the patient’s heart maintain a normal rhythm.

The Convergence and Integration of Information and Medical Technology in the 21st Century is driving rapid change!
• Convergence definition:… moving toward uniformity …
• Integration definition:… process of incorporating as equals …

Computers in Medicine: History
– Minicomputers used in a variety of systems starting in the early 1970s.
– In the 1980s, shortly after the invention of the microprocessor, personal computers and computer peripherals (e.g. printers) became common place as a platform (with custom hardware) for medical devices
– New medical products are developed and some high-tech systems are totally dependent on computer technology (e.g., CT scanners)
Computers in Medicine: Today
– In the 1990s, standards-based information technology infrastructure started to be used for medical applications (e.g. 10- base-T ethernet)
– Today common infrastructure is often used simultaneously by medical devices and business computers ( 100 meg ethernet, smart hubs, routers)
– Microprocessors have become ubiquitous, and are found in medical and business devices as well as appliances of all forms
– Now: Gigabit ethernet, SAN, standard wireless networks (e.g. IEEE 802.11)

Computers in Medicine: Today continued
– Microprocessors used in many, many medical products:
– Simple examples• “smart” electric beds that weigh the patient• “smart” electric beds that sense when the patient is
out of the bed• implants (e.g. implanted cardiac defibrillators)
– Complex examples:• Automated defibrillators• Expert systems for diagnosis• Robotic “beating heart”surgery

Computerized Beds with built-in Networks
From bed manufacturer’s sales brochure:
… systems are controlled through a sophisticated … electronic network … with modules [that] will automatically download to the Graphical Computer Interface (GCI).

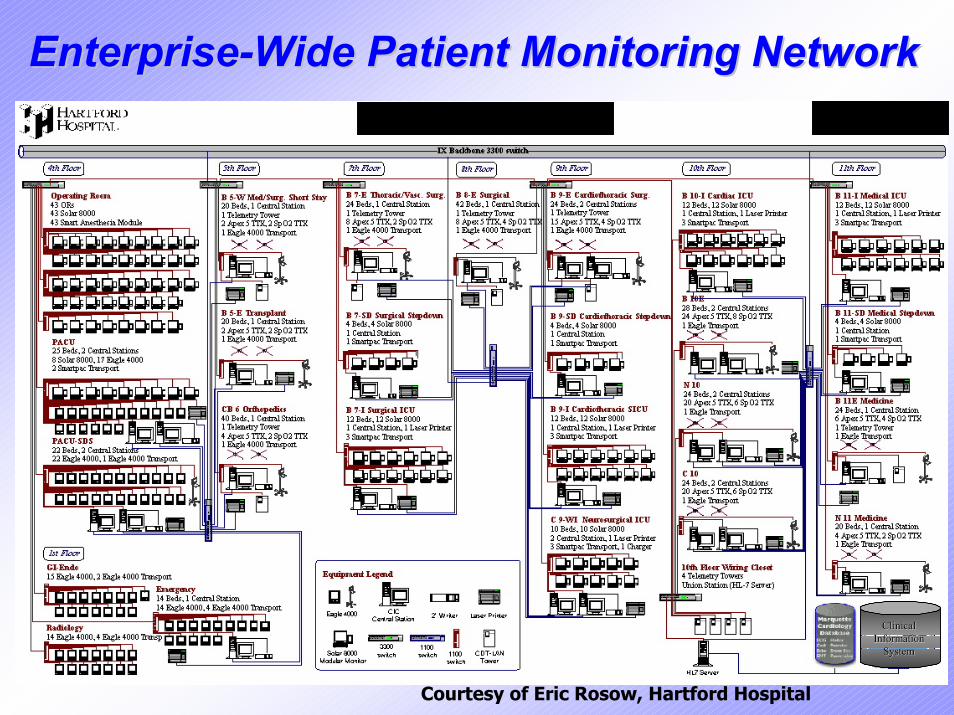
EnterpriseEnterprise--Wide Patient Monitoring NetworkWide Patient Monitoring Network
Clinical Clinical Information Information
System System
Courtesy of Eric Rosow, Hartford Hospital



Many new medical devices use standard Ethernet LAN adapters and/or are direct
Internet Protocol addressable
• Medical and business data can be intermixed on a single LAN
• Medical and business data can be run on separate LAN’s
• Medical and business data can share network gateways, print servers, etc

Example: Adding Wireless (802.11b) Monitors to an Existing Wireless LAN Network

Welch-AllynProtocol Systems Wireless(802.11b) portable patient monitor7.5 inches, 17 ouncesHeartbeat waveform display, rate detection, and oxygen level alarm capabilities in a patient-wearable device

Major Radio Frequency Issues in Hospitals
• If signals conflict, devices can be disabled.– Most hospitals outlaw personal cell phones
• New digital standards are emerging (WLAN 802.11 b, a, and g) and Bluetooth (low power, close proximity digital RF links)– Can be used with physician’s PDA’s too.
• How to safeguard privacy of patient data, hacking into hospital computer systems

Courtesy of Eric Rosow, Premis Corp/Hartford Hospital
Medical devices can now be virtual blends of HW & SW!
Devices can be reconfigured on the spot. For example, infant settings can replace adult settings for a monitor or ventilator, or a device can be reset to behave like an earlier version for easier deployment, or updated to newer specs.

The information system used to manage this network of medical
devices must be “aware.”• e.g., Devices must communicate their
configuration (just like printers, scanners, or other plug-and-play products do).
• The main system must adapt to the data needs – including bandwidth – and human interface requirements, as well as managing the information storage and retrieval.

Huge clinical databases result!
• e.g., One nearby hospital records ALL fetal heartbeat data from mothers in the delivery room, and ARCHIVES all records until the child is at least 21 years old!!!!!
– The system also analyzes all heartbeat data for possible problems, and sends out escalating alarms to central stations, pagers, portable phones, and 911 if needed!

Huge LAN data bandwidth capacity needs result, too.
• Medical images, like MRI or CT images from radiology department may each require 20+ Mbytes. A single study may have a hundred images, and the physicians in the hospital may expect to be able to see the images at any display on any floor or room at any time!

Capacity conflicts abound!• What is sacrificed first? Human data or
business data?– Smart, adaptive LAN and data server
management is needed• Life-critical data must get priority• Business critical functions must go second• General health-related data for record keeping can
go third• General business-related data… 4th
• …and how about general Internet access (personal, patient, and physician) and digital entertainment services????

In short, the healthcare facility has become HUGELY data intensive!
• Most new medical, business, and personal technologies being incorporated in hospitals are IT and IP aware!
• Responsibility for support is diffused among the CE and IT teams and management.

Regulatory Issues in this New World
• Food and Drug Administration: regulating IT systems and software as medical devices!
• HIPAA: Health Insurance Portability and Accountability Act (effective 6/2002 &2003)

Crossing over: From Information System to Medical Device
• A medical device is legally defined by the FDA as a device that directly affects the treatment or safety of a patient.– MEDICAL DEVICES MUST BE
REGISTERED WITH THE FDA AND THE REGISTRATION MUST PROVE THAT EITHER THE DEVICE IS THE SAME AS PRE-1976 DEVICES or HAS DOCUMENTED CLINICAL PERFORMANCE AND SAFETY.

Food for thought:• Will, or when will, portions of hospital information
systems be viewed as medical devices– Medical device is “hardware or software that can directly affect
patient diagnosis or therapy…”– What about a network, data warehouse, peripheral, or operating
system that interferes with telemetry, an alarm, drug administration, etc?
– How about a Decision Support System that “lost” a critical rule?
– What if an IS failure damages an electronic medical record?• FDA’s Final Software Validation guidance was just
released; required for legal Good Manufacturing Practice.

In the case of new, integrated and virtual IT/Medical Device systems:
• What separates the medical device (e.g., the fetal heart monitor on the mother’s stomach) from the information system (the file server with the heartbeat records and the alarm analysis software)???

HIPAA Issues – IT Focused!
• Require national coding standards for patients (you and me!), doctors, facilities, insurers, diagnoses, and treatments (Good news: can lead to reengineering healthcare, a la Dell and WalMart)
• BUT requires strict adherence to federal privacy regulations, or personal criminal prosecution and severe fines can result (new training, data and access security measures, radio frequency management, authentication technologies, etc, will be crucial.)

More food for thought:BMET/CE have HIPAA roles!
• Many current, and future, medical devices contain local copies of patient data.– Interlinked systems may also share copies of data– Devices “in the shop” can have patient data– Disks and EAROM chips that are swapped out can
still have readable data– Remote medical device support, including hospital
and OEM staff, may require secure access controls– BMET and CE staff may need to see patient-
specific data to diagnose and fix problems

Convergence of Clinical and Information Technologies
InternetInternetandand
World Wide World Wide WebWeb
InterapplicationInterapplicationCommunicationCommunication(SQL Toolkits)(SQL Toolkits)
“Fuzzy Logic”“Fuzzy Logic”ToolkitsToolkits
AdvancedAdvancedDAC & DSPDAC & DSP
VirtualVirtual
Medical DevicesMedical Devices
Courtesy of Eric Rosow, Premis Corp, Hartford Hosp

New opportunities/challenges of CE and IT working together:
• Both teams have roles that can affect patient safety and clinician effectiveness
• Both teams often share bandwidth, data warehouse capacity, CPU cycles, and peripherals
• Both teams require similar SW and HW configuration, management, and repair skills
• Each team has strengths (e.g. SW development vs. HW repair, different systems analysis skills)

Both teams have blind spots• Clinical engineering staff isn’t familiar with
software and system project management issues– Plus, historically the medical device mfrs operated in a
virtual vacuum. “System validation” should make sense to them, too, but in their prior world, the “system” was exclusively theirs, not shared!
• IT staff isn’t really comfortable in the direct patient care area, and not sensitive to clinician limitations, training– Plus, not used to crisis nature (urgency) of patient care,
and the need to make ad hoc temporary fixes.

As a Technology Leader or CIO….
How do you define the consumer and global aspects of eHealth?

E-Health• Often refers to Internet delivered
healthcare– medical records processing, virtual MD
offices, and on-line drug stores– extends the IP addressable technologies and
information OUTSIDE the hospital walls• Similar to E-commerce
– E-Health is web accessible and becoming transaction based

eHealth and Telemedicine
• The terms can be used interchangeably in some contexts– eHealth might be thought of as the consumer-
focused activities (e.g., WebMD)– Telemedicine might be used for the more
clinical and technical aspects (e.g., global consultation of physician experts, or robotic surgery as was done between France and US.)

Hospital Staff Web Literacy is IncreasingHospital Staff Access Soared in 1999
Staff Physicians 28% 82%Pharmacy 31% 80%
1998 1999Directors, Managers, and Supervisors 63% 91%Materials Management 35% 87%Human Resources 47% 86%
Business office 31% 75%Medical Records 22% 66%Radiology N/A 66%Laboratories N/A 60%Nurses 22% 56%Nursing Support Staff 17% 55%
Source: Delantten and Toothe; Study done through Hospital Access

AND SO IS PATIENT WEB LITERACY!!

The E-Health Umbrella
• “Telehealth” (like WebMD• PACs (Picture Archiving..)• Teleradiology • Listserves • E-mail• Web Enabled Systems• Computerized Data Repositories • Computerized Patient Records (EMR)• Personalized Health Records

e-E
eE-E
Patient Oriented E-Health
• e-information• e-consultation• e-prescribing• e-message boards• e-self-help• e-discussion groups• e-mail consultation

Internet Clinical Technology
• Changing patient relationship with nurses and physicians– more family and significant other interactions
• Increased patient information and education • Integration with personal and health records

E-Health Incentivesfor
Patients and Healthcare Organizations Patients and Healthcare Organizations
• More timely service• Reduced waiting time• Increased convenience• Reduced overhead• Improved communication

The Implication
E-Health has a varietyof definitions.
Execution strategies are nearly the same as other IT
projects, though.

Transitioning to E-Health
Strategic Readiness

E-Health – US Navy• Define E-Health for the organization
– articulating the potential– simple and complex terminology
“E-Health is the business of facilitating the electronic exchange of information within the Navy Medicine Healthcare community of interest to support Optimization, beneficiary care, and force health protection”

Technical Readiness
• Assess available resources– network capabilities
• upgrades – establishing/enlarging “DMZ” (i.e.,
accessible resources)– Security & legal (HIPAA) compliance
• firewall implementation• review of authentication/access• encryption• policy reviews

Evaluating NetworksTechnology or Function
Function•Convenient•Scaleable•Reliable•Consistent•Secure•Performance Based•Speed
Architecture•LAN•VLAN•WAN•VPN
Technology•ISDN•T-1•Fast Ethernet•Gigabit Ethernet•ATM

Enhancing Network Capabilities
• Use existing infrastructure• Augment existing infrastructure• Build to the requirement
– Government furnishes or vendor provides
E- health focus is instrumental in option selection

• Size and complexity of systems are growing• Simultaneous access for multiple web,
database, and PACS applications necessary– “Anytime, Anywhere”
• Poor network performance– results in sub-optimal or even non-performance
of application software– decreases clinical buy-in to E-Health
Why Emphasize Networking/Security?

Process redesign can save costs
• Just like other eCommerce experiences…

Online Routine Prescription Refill
• AudioCARE is Commercial-off-the-Shelf (COTS) product installed – web module product is in use to enhance
beneficiary access– allows for local customization by site for
specific satellite and branch pharmacies

Demonstrated Results
68%76%
81%83%87%
13%17% 19%
24%33%
0%10%20%30%40%50%60%70%80%90%
100%
Aug Sept Oct Nov Dec
Percent Phone Refills Percent Web Refills

eHealth & Internet Technologies – BPR for Healthcare
• Permit reconfiguration within an industry– especially helpful with high communication,
large data gathering, and huge transaction cost areas
• Changes the front end process– Internal and external customers
• Back end business requirements and construct require integration with vision/goals– CIO responsibility for planning and execution

Considerations when Selecting E-Health Applications
• Value for Patients and Physicians– Valuable interactions that do not interfere with
patient interaction, routine workflow, efficiency, portability, and support optimization
• Value to Management – Minimize lost revenue and reduce overhead and
rework costs– Leverage existing IT investments– Minimize upfront cost and hassle factor– Minimize maintenance and support costs

Considerations in eHealth implementation
• Regulatory compliance is severe challenge• Potential for systemic interference and overload is
significant and difficult to model or predict.– Multimedia and bandwidth issues are BIG!
• Legal issues of medical care, and prescriptions, are overreaching state, or national, laws– e.g., How can a US surgeon perform surgery by
remote-control robot in Africa if not licensed there? How can an African expert on tropical disease management prescribe a drug for a rare disease in Australia (and is the drug even legal for distribution in Australia?)
Virtual Home Health Agents
• Some predictions include virtual “health agents” in all homes by 2015– Will have to rely on Artificial Intelligence,
Expert System, and Decision Support Systems that a) are yet to be developed, b) will have to meet legal/regulatory scrutiny, c) tap into personal and technical data warehouses for decisions, and d) allow effective support for the diversity of humankind!

Practically speaking…
• Virtual home health agents will need to integrate with IP addressable medical and diagnostic devices to allow a remote clinician to obtain current information, and may also depend on 2-way VoIP and video links to succeed.

Challenges notwithstanding…• My prediction is that the economic savings,
and the moral imperatives behind improving the efficacy and efficiency of health care will ultimately ensure that IT continues to be a “prime mover” for tomorrow’s health care.
• The biggest resistance may become the physician; as standardized data can be “mined,” their latitude to practice as they see fit may be considerably curtailed.

Remember, too:
Sick people need “high touch,” not just high tech. Healing is a holistic process.
Everything we do to make the parts we control BETTER helps, but isn’t a “sole
source” solution!
(Further, global ethics and moral values differ. We’re going to be forced to “grow” to meet
the international needs.)

IT Career Tip:KEEP AN EYE ON HIPAA!
• Experts predict that if the government stays on course, the remediation effort will EXCEED Y2K.– Current deadline: Mid-2003!

A topic for another day…
• The critical road ahead for IT to help solve the medical error and patient injury crisis.– Government reports estimate as many as 90,000
Americans are severely injured or killed by medical errors.
• Drug and supply errors are claimed to be a major cause, but there isn’t even a national bar code (SKU) or nomenclature system for drugs and supplies! Industry doesn’t seem to want it, and gov’t hasn’t been willing to demand it.

Thank You!• Links you might find interesting:
– www.HIMSS.org– www.ACCEnet.org– www.AAMI.org– www.ECRI.org
QUESTIONS?